Embed Size (px)
Citation preview

52 JCN 2019, Vol 33, No 1
SKIN CARE
There are many treatments for moderate-to-severe psoriasis. All require assessment of
the condition to offer the most appropriate treatment to match the severity of the condition. National Institute for Health and Care Excellence (NICE) guidelines (NICE, 2017) were set out providing a logical patient treatment pathway to provide effective clearance to the skin (Figure 1). The pathway’s aim is to reduce troublesome symptoms, such as itch, as well as playing a huge emotional and psychological role in allowing patients to continue their daily lives without the embarrassment or other psychological pressures that come with a visual skin condition (Griffiths et al, 2004).
Psoriatic patient treatment pathway: systemic treatments
Tonia Goman
This series has assessed the forms of psoriasis and the impact this condition has on patients. Using NICE guidelines, these articles have focused on treatments such as simple emollient treatments, topical therapies including vitamin D derivatives, coal tar, dithranol and the varying strengths of steroid creams/ointments, as well as the use
phototherapy.
This article addresses the systemic options available and what is involved. Monitoring of these treatments is often shared by secondary and primary care. Table 1details how primary and secondary care practitioners come together to enable patients to manage their psoriatic symptoms.
WHAT ARE SYSTEMIC TREATMENTS FOR PSORIASIS?
Systemic treatments are usually tablet medications used to treat moderate-to-severe psoriasis. These treatments are prescribed by a dermatologist when the symptoms of psoriasis are
Tonia Goman, dermatology specialist nurse, (inflammatory skin conditions), Bristol Dermatology Centre, Bristol Royal Infirmary;
camouflage practitioner
This series has addressed the treatments for psoriasis as advised by the National Institute for Health and Care Excellence (NICE, 2017).
on mood, mental health, poor lifestyle choices (Cohen et al, 2016; Landriscina et al, 2016), reduced activities of daily living, and is
and cardiovascular disease (Rutter et al, 2016). NICE developed a
phototherapy, systemic medications and systemic non-biological and biologic therapy. In recent years, the latter options have increased dramatically. This article focuses on the more traditional systemic treatments, as advised by NICE.
KEYWORDS: Dermatology Systemic treatments Screening
Figure 1.The psoriasis treatment pathway (adapted from NICE, 201 ).
Person with psoriasis
Topical therapy
Specialist referral
Systemic biologic therapy
Systemictherapy
not controlled with topical treatments or phototherapy alone.
There are several options available, each with specific considerations when weighing up other comorbidities, lifestyle choices and practicalities. Some of these can be beneficial for those who have psoriatic arthritis as well as psoriasis. NICE (2012) recommends methotrexate (MTX) or ciclosporin as first treatment options. Acitretin is another option if the first two have failed, or are contraindicated by other
Wound
Care
People
Ltd
JCN 2019, Vol 33, No 1 53
SKIN CARE
health issues. These are the three main systemic options, although others are also available and will be discussed briefly.
As a part of the decision-making process, a thorough medical history should be taken. Hypertension (high blood pressure), liver and kidney impairment may prevent certain treatments being offered. Counselling is essential, providing specific information on each treatment form, dosage, regularity and blood testing.
METHOTREXATE
Methotrexate (MTX) is a disease-modifying antirheumatic drug, or DMARD. It has been used for over 50 years to treat psoriasis and psoriatic arthritis. It is an immunosuppressant that works by slowing down the rapid overproduction of skin cells that result in the increased scale and redness, which is classic of psoriasis (Oakley et al, 2015). It was initially used to treat specific types of cancer but was noted to help treat skin and joint pain in lower doses (British Association of Dermatologists [BAD], 2016a). It is appropriate to consider this option if the patient has a history of psoriatic arthritis or reports joint pain (Warren et al, 2016). Some of the contraindications for MTX are listed in Table 2.
ScreeningWhen the dermatologist suggests systemic treatment, baseline tests will also be requested. The patient will also be given information leaflets regarding the suitable options. Routine blood tests advised by BAD (2016a) include liver function tests (LFTs), full blood count (FBC), and urea and creatinine (U/Es), along with specialist tests, procollagen III peptide (blood test to assess for hepatic fibrosis), hepatitis B and C, human immunodeficiency virus (HIV), varicella zoster serology (chicken pox immunity) and chest x-ray (Warren et al, 2016).
CounsellingIt is recommended that all patients limit their alcohol intake to well below the national guidelines while taking MTX (Rajakulendran et al, 2008). Live vaccines must be avoided
while on MTX, but the annual flu vaccination is recommended due to immunosuppression. Contraception should be used throughout treatment and continued for a further three months after discontinuing treatment. Women are not to get pregnant while on this drug, as it can harm the foetus. Breastfeeding is also contraindicated (Visser et al, 2009; Oakley et al, 2015; BAD, 2016a). There are mixed opinions regarding whether men should father a child while on MTX, and it is therefore advised that men wait three months after stopping treatment before doing so. Fertility can be reduced, and on higher doses there is a risk of miscarriage or stillbirth (Warren et al, 2016).
If feeling unwell, or suffering with an infection, MTX should be withheld until symptoms have settled. As an immunosuppressant, symptoms can be prolonged or lower the system further. Avoiding live vaccines, such as yellow fever, is also recommended to prevent triggering symptoms of the disease (Arthritis Research UK, 2014).
The British National Formulary (BNF, 2017a) recommends taking note of other medications, including anti-folate drugs such as trimethoprim, as this, as well as age and renal impairment, can increase toxicity. Aspirin and ibuprofen, along with other non-steroidal anti-inflammatories can reduce how much MTX is safely eliminated by the kidneys (Oakley et al, 2015; BNF 2017a). Penicillin should be avoided
to enable the kidneys to excrete the MTX (National Psoriasis Foundation [NPF], 2015).
DosageMTX is prescribed as once a week only, and should be taken on the same day of the week. Dermatologists prescribe doses on a 2.5mg basis, enabling the dose to be titrated to a level that helps control the symptoms of psoriasis (BNF, 2017a). It is a slow treatment, taking up to 12 weeks before improvement may be noted.
During the initial 12-week period, the dermatologist will set the intended regimen and monitor the patient closely — monitoring blood results, assessing side-effects and noting symptom improvement. The regime generally starts on a low dose and is gently increased on a fortnightly basis.
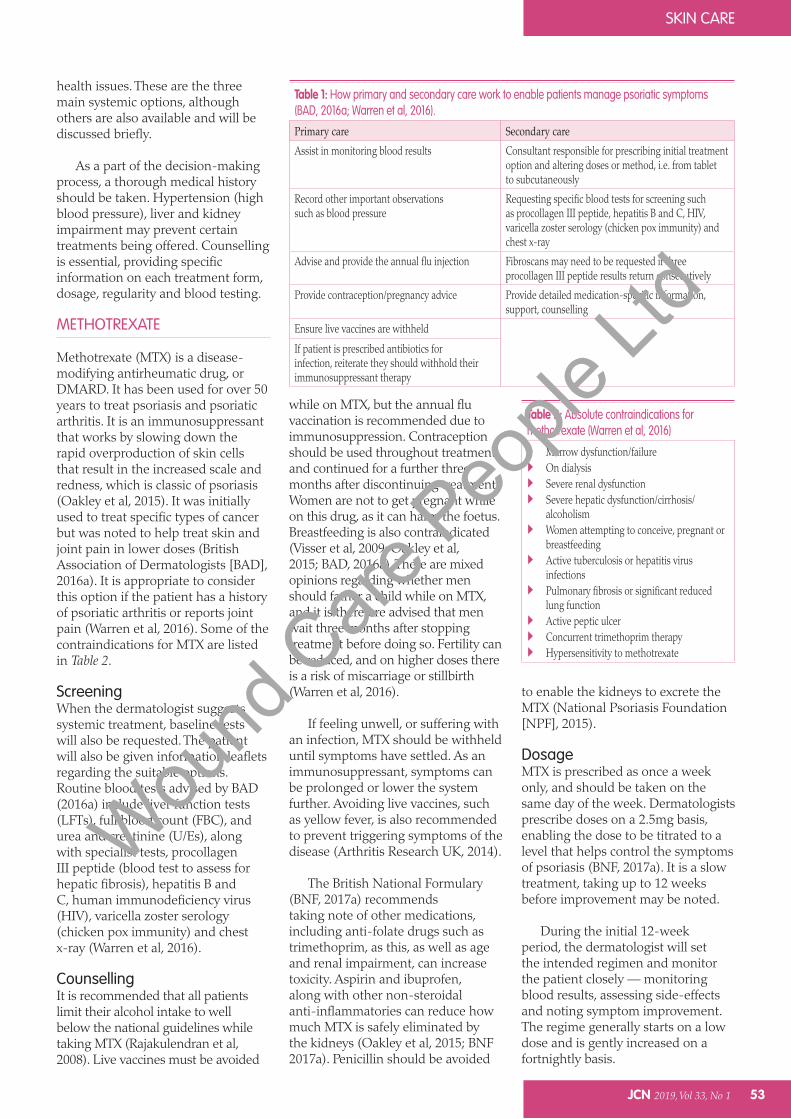
Table 2: Absolute contraindications for methotrexate (Warren et al, 2016)
Marrow dysfunction/failureOn dialysisSevere renal dysfunctionSevere hepatic dysfunction/cirrhosis/
alcoholismWomen attempting to conceive, pregnant or
breastfeedingActive tuberculosis or hepatitis virus
infectionsPulmonary fibrosis or significant reduced
lung functionActive peptic ulcerConcurrent trimethoprim therapyHypersensitivity to methotrexate
Table 1: How primary and secondary care work to enable patients manage psoriatic symptoms (BAD, 2016a; Warren et al, 2016).
Primary care Secondary careAssist in monitoring blood results Consultant responsible for prescribing initial treatment
option and altering doses or method, i.e. from tablet to subcutaneously
Record other important observations such as blood pressure
Requesting specific blood tests for screening such as procollagen III peptide, hepatitis B and C, HIV, varicella zoster serology (chicken pox immunity) and chest x-ray
Advise and provide the annual flu injection Fibroscans may need to be requested if three procollagen III peptide results return consecutively
Provide contraception/pregnancy advice Provide detailed medication-specific information, support, counselling
Ensure live vaccines are withheld
If patient is prescribed antibiotics for infection, reiterate they should withhold their immunosuppressant therapy
Wound
Care
People
Ltd
SKIN CARE
54 JCN 2019, Vol 33, No 1
Folic acid, a vitamin supplement, is prescribed alongside MTX (BAD, 2016a). It is not to be taken on the same day as MTX as it reduces the effectiveness but can assist in easing side-effects of nausea, fatigue or mouth ulcers. It is often prescribed once weekly, but if side-effects are problematic, this can be increased to six days a week via prescription (Shea et al, 2013).
MonitoringRegular blood tests are requested during initiation but can be moved to monthly or three-monthly, depending on how stable the results are (BAD, 2016a). After this point, a shared care contract is often arranged with the GP, so both can monitor blood results and provide prescriptions. Possible side-effects of MTX are listed in Table 3.
Whittle and Hughes (2004) state that approximately 30% of rheumatology patients stop MTX within one year due to adverse effects, and 60% experience mild adverse effects. Switching from tablet form to subcutaneous injection can often ease abdominal discomfort, allowing the patient to continue this treatment option.
Procollagen III peptide tests will be requested by the dermatologist
CICLOSPORIN
Ciclosporin (also spelt cyclosporine) is a substance produced by a fungus (BAD, 2018).Recommended as a first-line systemic option, ciclosporin was approved by the Food and Drug Administration for psoriatic patients in 1997. Before this, it was used specifically for prevention of rejection in organ transplant patients, (National Psoriasis Foundation, 2015). The brand used should remain consistent, as it is not bioequivalent (absorbed by the body in different amounts [BNF, 2018, MedLine Plus, 2018a]) to all other types of ciclosporin (Psoriasis Association, 2014).
NICE (2012) suggests patients can be considered for ciclosporin when: Symptoms are not being
controlled by topical therapies alone
Psoriasis covers 10% of the body area
Psoriasis has a significant impact on patient wellbeing — physical, psychological or social.
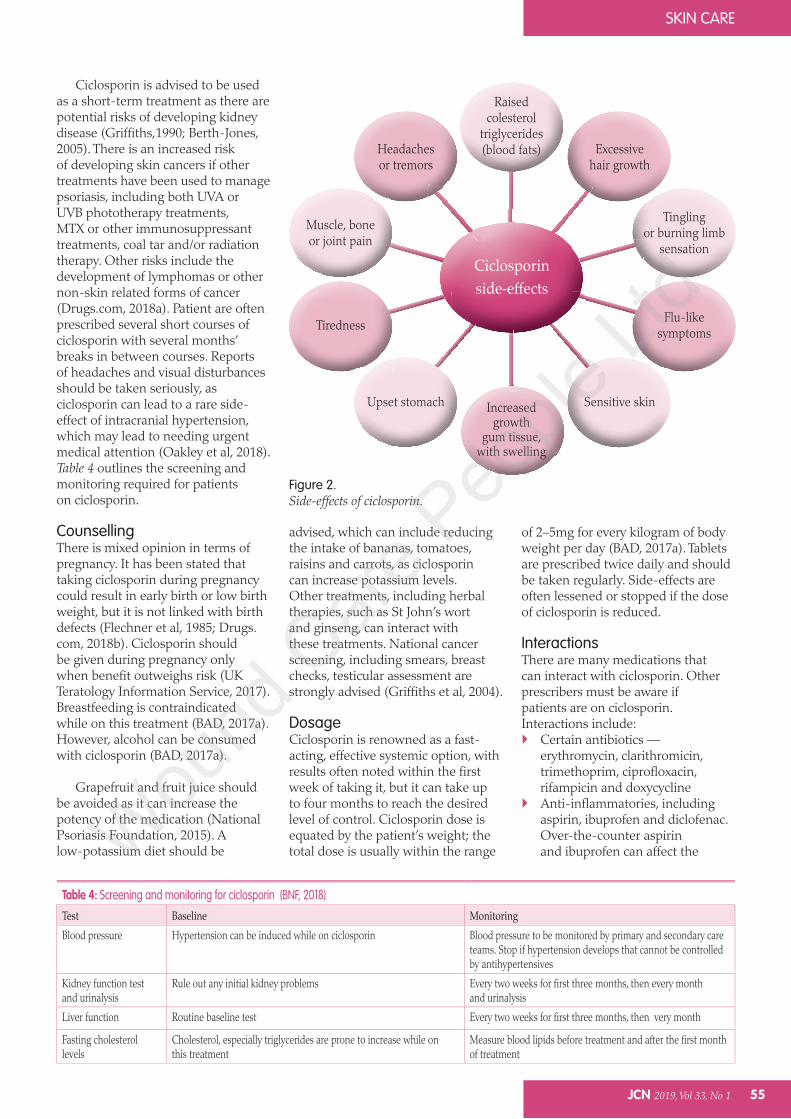
It can also be used if the psoriasis is not necessarily extensively covering the body, but affecting a localised area, such as scalp, hands and/or feet that causes significant distress. It can also be recommended when phototherapy has resulted in a rapid relapse (provided three months or less clearance), or ineffective. Palmoplantar pustulosis (pustular psoriasis to hands and/or feet) may require a short-term course to resolve a flare (Psoriasis Association, 2014). For side-effects, see Figure 2.
ContraindicationsThe BNF (2018) advises on the contraindications of ciclosporin being abnormal baseline renal/liver function, malignancy, uncontrolled hypertension and uncontrolled infections.
RisksThe risk of minor infections such as the common cold is not necessarily increased, however, resistance to infections such as tuberculosis will be lowered (BAD, 2017a). Anaemia/bleeding disorders, history of seizures, or eye/visual problems should be considered (Drugs.com, 2018a).
and should be carried out every three to six months. These results can take up to six weeks as they are sent away for analysis. If three raised results return consecutively, the clinician may need to request a fibroscan, a liver biopsy, and/or stop treatment and consider an alternative treatment (Oakley et al, 2015).
Fibroscan is a non-invasive procedure that measures the stiffness of the liver, and is used to detect cirrhosis (Kemp and Roberts, 2013). Other chronic liver diseases, including hepatitis B or C virus infection, alcohol and non-alcoholic liver disease may be indicated (Foucher et al, 2006). Occasionally, liver biopsies are required, although since the introduction of fibroscans, these are carried out less frequently. These are mainly requested to estimate the degree of liver damage or determine treatment options for liver disease (National Institute of Diabetes and Digestive and Kidney Disease, 2014).
Providing the symptoms continue to be held, side-effects are tolerable, and blood results show that the system is managing the medication, patients can successfully remain on this treatment for many years (Haustein and Rytter, 2000).
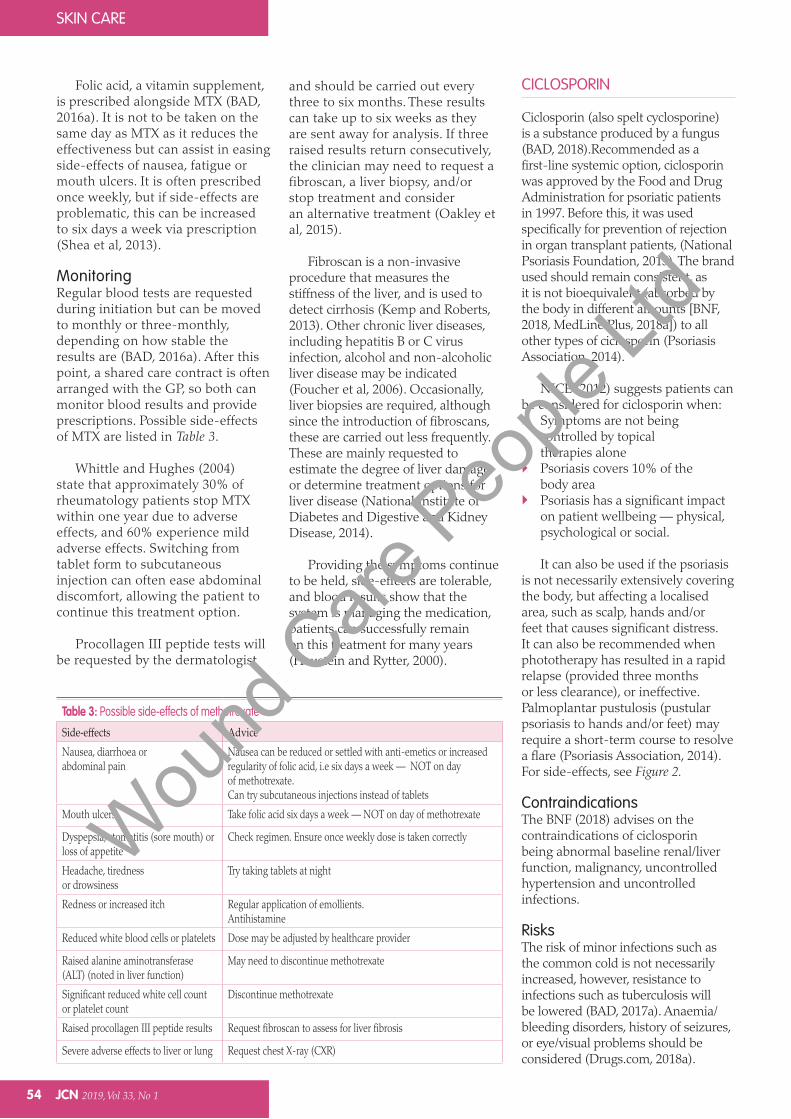
Table 3: Possible side-effects of methotrexate
Side-effects AdviceNausea, diarrhoea or abdominal pain
Nausea can be reduced or settled with anti-emetics or increased regularity of folic acid, i.e six days a week — NOT on day of methotrexate.Can try subcutaneous injections instead of tablets
Mouth ulcers Take folic acid six days a week — NOT on day of methotrexate
Dyspepsia, stomatitis (sore mouth) or loss of appetite
Check regimen. Ensure once weekly dose is taken correctly
Headache, tiredness or drowsiness
Try taking tablets at night
Redness or increased itch Regular application of emollients. Antihistamine
Reduced white blood cells or platelets Dose may be adjusted by healthcare provider
Raised alanine aminotransferase (ALT) (noted in liver function)
May need to discontinue methotrexate
Significant reduced white cell count or platelet count
Discontinue methotrexate
Raised procollagen III peptide results Request fibroscan to assess for liver fibrosis
Severe adverse effects to liver or lung Request chest X-ray (CXR)
Wound
Care
People
Ltd
JCN 2019, Vol 33, No 1 55
Ciclosporin is advised to be used as a short-term treatment as there are potential risks of developing kidney disease (Griffiths,1990; Berth-Jones, 2005). There is an increased risk of developing skin cancers if other treatments have been used to manage psoriasis, including both UVA or UVB phototherapy treatments, MTX or other immunosuppressant treatments, coal tar and/or radiation therapy. Other risks include the development of lymphomas or other non-skin related forms of cancer (Drugs.com, 2018a). Patient are often prescribed several short courses of ciclosporin with several months’ breaks in between courses. Reports of headaches and visual disturbances should be taken seriously, as ciclosporin can lead to a rare side-effect of intracranial hypertension, which may lead to needing urgent medical attention (Oakley et al, 2018). Table 4 outlines the screening and monitoring required for patients on ciclosporin.
CounsellingThere is mixed opinion in terms of pregnancy. It has been stated that taking ciclosporin during pregnancy could result in early birth or low birth weight, but it is not linked with birth defects (Flechner et al, 1985; Drugs.com, 2018b). Ciclosporin should be given during pregnancy only when benefit outweighs risk (UK Teratology Information Service, 2017). Breastfeeding is contraindicated while on this treatment (BAD, 2017a). However, alcohol can be consumed with ciclosporin (BAD, 2017a).
Grapefruit and fruit juice should be avoided as it can increase the potency of the medication (National Psoriasis Foundation, 2015). A low-potassium diet should be
advised, which can include reducing the intake of bananas, tomatoes, raisins and carrots, as ciclosporin can increase potassium levels. Other treatments, including herbal therapies, such as St John’s wort and ginseng, can interact with these treatments. National cancer screening, including smears, breast checks, testicular assessment are strongly advised (Griffiths et al, 2004).
DosageCiclosporin is renowned as a fast-acting, effective systemic option, with results often noted within the first week of taking it, but it can take up to four months to reach the desired level of control. Ciclosporin dose is equated by the patient’s weight; the total dose is usually within the range
of 2–5mg for every kilogram of body weight per day (BAD, 2017a). Tablets are prescribed twice daily and should be taken regularly. Side-effects are often lessened or stopped if the dose of ciclosporin is reduced.
InteractionsThere are many medications that can interact with ciclosporin. Other prescribers must be aware if patients are on ciclosporin. Interactions include:
Certain antibiotics — erythromycin, clarithromicin, trimethoprim, ciprofloxacin, rifampicin and doxycyclineAnti-inflammatories, including aspirin, ibuprofen and diclofenac. Over-the-counter aspirin and ibuprofen can affect the
SKIN CARE
Table 4: Screening and monitoring for ciclosporin (BNF, 2018)
Test Baseline MonitoringBlood pressure Hypertension can be induced while on ciclosporin Blood pressure to be monitored by primary and secondary care
teams. Stop if hypertension develops that cannot be controlled by antihypertensives
Kidney function test and urinalysis
Rule out any initial kidney problems Every two weeks for first three months, then every month and urinalysis
Liver function Routine baseline test Every two weeks for first three months, then very month
Fasting cholesterol levels
Cholesterol, especially triglycerides are prone to increase while on this treatment
Measure blood lipids before treatment and after the first month of treatment
Ciclosporin
Raisedcolesterol
triglycerides(blood fats)Headaches
or tremorsExcessive
hair growth
Upset stomach Sensitive skin
Muscle, boneor joint pain
Tinglingor burning limb
sensation
TirednessFlu-like
symptoms
Increasedgrowth
gum tissue,with swelling
Figure 2.Side-effects of ciclosporin.
Wound
Care
People
Ltd
56 JCN 2019, Vol 33, No 1
SKIN CARE
Reduced night vision Increased risk of skin infections,
especially with Staphylococcus aureus (impetigo, boils or nail fold paronychia)
Psoriasis can initially flare, but this is usually temporary and then steadily improves. However, a severe flare should be reported to the dermatology team
Hyperlipidaemia, raised cholesterol and triglyceride. This can be raised in people with diabetes and those prone to drinking a lot of alcohol. Statin treatment may be prescribed by the GP if cholesterol results remain high. A reduced fat and sugar diet should be advised. If lipids remain high, acitretin may be discontinued
Long-term use of acitretin can result in calcium deposits around the bones, leading to pain
Hepatitis, although rare, can develop when LFTs are disrupted. Treatment must be stopped immediately if LFTs, particularly ALT, are disrupted
(Ormerod, 2010; National Psoriasis Foundation, 2016; BAD, 2017b; Oakley, 2017).
FUMARIC ACID ESTERS
Fumaric acid esters (FAE; Fumaderm®), have been used for psoriasis since the late 1950s. They contain dimethylfumerate (DMF) and three monoethylfumerate (MEF) salts (Wollina, 2011). Although a popular drug in Europe, this medication is not licensed in the UK (BAD, 2018). As an unlicensed drug, it has not been awarded a marketing authorisation from the UK Medicines & Healthcare Products Regulatory Agency. However, the drug may still be prescribed in the UK, provided there is funding available locally to pay for it (BAD, 2018).
Fumaric acid esters work on the immune system, specifically t-cells. These cells produce chemicals called cytokines. When these chemicals are imbalanced, psoriasis is triggered. FAE can reduce the imbalance of the cytokines (Guy’s and St Thomas’ NHS Foundation Trust, 2014; BAD, 2018). Clearance may take several weeks to note, although treatment should be
metabolism of the drug, resulting in there being too much or little in the bloodstream
Antifungals — fluconazole, itraconazole, ketoconazole and amphotericin B
Gastrointestinal agents Digoxin Calcium channel blockers,
angiotensin-converting-enzyme (ACE) inhibitors, beta-blockers and calcium channel blockers
Anticonvulsants — phenytoin and carbamazepine (BAD, 2017a).
ACITRETIN
Acitretin is an oral retinoid, a synthetic vitamin A treatment used for pustular, erythrodermic and palmoplantar psoriasis, as well as a variety of other dermatological conditions. It is not effective for psoriatic arthritis (Oakley et al, 2015). It is recognised as a third systemic option in the NICE guidelines (NICE, 2017), if MTX or ciclosporin are not appropriate. Effectiveness can be noted relatively quickly from week two, with steady improvement continuing by week 12 (BAD, 2017b). This treatment can be used both in the short and long term.
Acitretin slows cell proliferation, and can be used conjunctively with other treatments, such as phototherapy, topical treatments and even some biologic treatments (National Psoriasis Foundation, 2016). Table 5 outlines the screening and monitoring required for patients on acitretin.
ContraindicationsAcitretin is highly teratogenic and is absolutely contraindicated for women who are, or may plan to get pregnant in the future. Pregnancy must not take place for three years after discontinuing this treatment (Ormerod, 2010).
CounsellingIt is essential that patients are aware of the side-effects. Lifestyle should be considered to ensure appropriateness of the treatment: Pregnancy — sperm is not
affected by acitretin and it is therefore safe for men to father a child. Due to the high risks of
damaging the foetus or causing deformities to an unborn baby, acitretin is very rarely prescribed for women of child-bearing age. In rare cases, women may be prescribed acitretin, but they should not be on the mini-pill as it decreases ovulatory effect, although this is not affected when on the combination pill (Ormerod, 2010)
Blood should not be donated by males or females while on acitretin, and for three years after stopping, as the recipient may be a female of child-bearing age (BAD, 2017b)
Alcohol — no alcohol should be consumed either as a drink or in food while taking acitretin and for two months after stopping. This is also true in the case of medication, whether prescribed or obtained over-the-counter. A substance that forms when alcohol and acitretin are combined can harm a foetus (MedLine Plus, 2018b).
DosageAcitretin will be prescribed according to the patient’s weight and extent of psoriasis. The dose is usually equated at 0.5–1mg/kg/day. The maximum recommended dose is 75mg daily, although lower doses can be prescribed if side-effects are problematic. Tablets come in 10mg and 25mg capsules (BAD, 2017b; BNF, 2017c). It is advised to take acitretin after a meal, as it is less effectively absorbed on an empty stomach.
Acitretin is generally safe with most other medications but should be avoided when on vitamin A (retinoids, such as isotretinoin), tetracycline, MTX or phenytoin, (Oakley, 2016). There is increased risk of hypoglycaemia when taken with antidiabetic medications and increased risk of hyperlipidaemia when taken with corticosteroids (Ormerod, 2010). Side-effects are listed in Table 6.
Other side-effects can involve: Temporary hair loss, thinning of
the hair, alteration in hair colour and/or texture
Gastrointestinal disturbance — nausea and abdominal pain
Wound
Care
People
Ltd
JCN 2019, Vol 33, No 1 57
SKIN CARE
DosageFumaderm comes in two strengths, low (Fumaderm Initial) and high dose (Fumaderm Full Strength). The dose is generally built up over a weekly basis, eventually leading to the planned dose. Maximum dose is two tablets three times a day (Guy’s and St Thomas’ NHS Foundation, 2014).
Side-effectsThese mainly include nausea, abdominal cramps, diarrhoea and flatulence, which can affect over two-thirds of patients. Flushing, feeling hot, redness to skin and irritation is also reported by one-third of patients. These side-effects are often overcome by starting on a low dose and steadily increasing over time (BAD, 2018; Menter et al, 2009). Headaches are also common when starting this treatment (BAD, 2018).
Rare side-effects include liver inflammation, kidney abnormalities with loss of protein in the urine and encephalogy (viral infection of the nervous system). This risk is increased when taken with a consistent low lymphocyte count, therefore regular blood checks should be made.
MYCOPHENOLATE MOFETIL
Mycophenolate mofetil (MMF) is a medication generally used post transplantation to prevent the organ from being rejected. In dermatology, it is used for a range of skin conditions. It is an immunosuppressant, lowering the body’s defence system (BAD, 2017c).
Mycophenolate mofetil is used alone, or in conjunction with other immunosuppressants such as ciclosporin and corticosteroids (Ngan, 2003).
ContraindicationsThese include pregnancy and breastfeeding, as well as gastrointestinal disease (BNF, 2017c).
ScreeningMonitoring should include a FBC, LFTs and U/Es within the first week of starting, then monthly.
Counselling Pregnancy — patients must
not be pregnant while on this treatment. A urine pregnancy test should be carried out within the first week of starting MMF. Two forms of contraception are advised during treatment, which should be continued for a further six weeks after stopping. Males should not consider fathering a child or sperm donation while on MMF and for a period of time after discontinuing treatment
Infection — there is a higher risk of developing infections and fighting off symptoms of infections. There is also increased risk of conditions such as progressive multifocal leukoencephalopathy (PML), HIV/AIDs, sarcoidosis (condition causing swelling in the lungs and other sites) and leukaemia
Alcohol within national limits is acceptable
Avoid antacids containing magnesium or aluminium
Avoid blood donation Higher risk of developing skin
cancers — follow sun protection advice
Avoid live vaccines. It is recommended to have the annual flu and pneumococcal vaccines. Avoid the new nasal flu vaccine as this is a live vaccination
(BAD, 2017c; BNF, 2017c).
discontinued if minimal improvement is seen within a six-month period (BAD, 2018). FAE should not be prescribed to those under the age of 18 years (BAD, 2018).
Contraindications These include: Pregnancy/breast-feeding Severe or chronic kidney disease Leukopenia and other
haematologic abnormalities Severe liver disease Cancer or history of cancer Severe or chronic GI disease (Menter et al, 2009).
Screening This should involve: Baseline bloods: routine LFTs,
UEs, FBC as well as HIV, hepatitis B and C
Urinalysis — checking for sugar and protein.
Routine bloods and urinalysis should be carried out fortnightly in the first three months and then reduced to monthly tests.
Counselling Pregnancy — it is advised to
avoid as there is increased risk of harming an unborn baby. FAE should also not be taken when breastfeeding. It does not interfere with the contraceptive pill or other hormonal contraception
Alcohol — drinking alcohol does not interact with FAE, but consumption should be within recommended limits. It is noted that strong alcoholic beverages can increase stomach irritation
Most medications can be taken alongside FAE. It is best to avoid nephrotoxic drugs, as kidney damage can be caused (BAD, 2018).
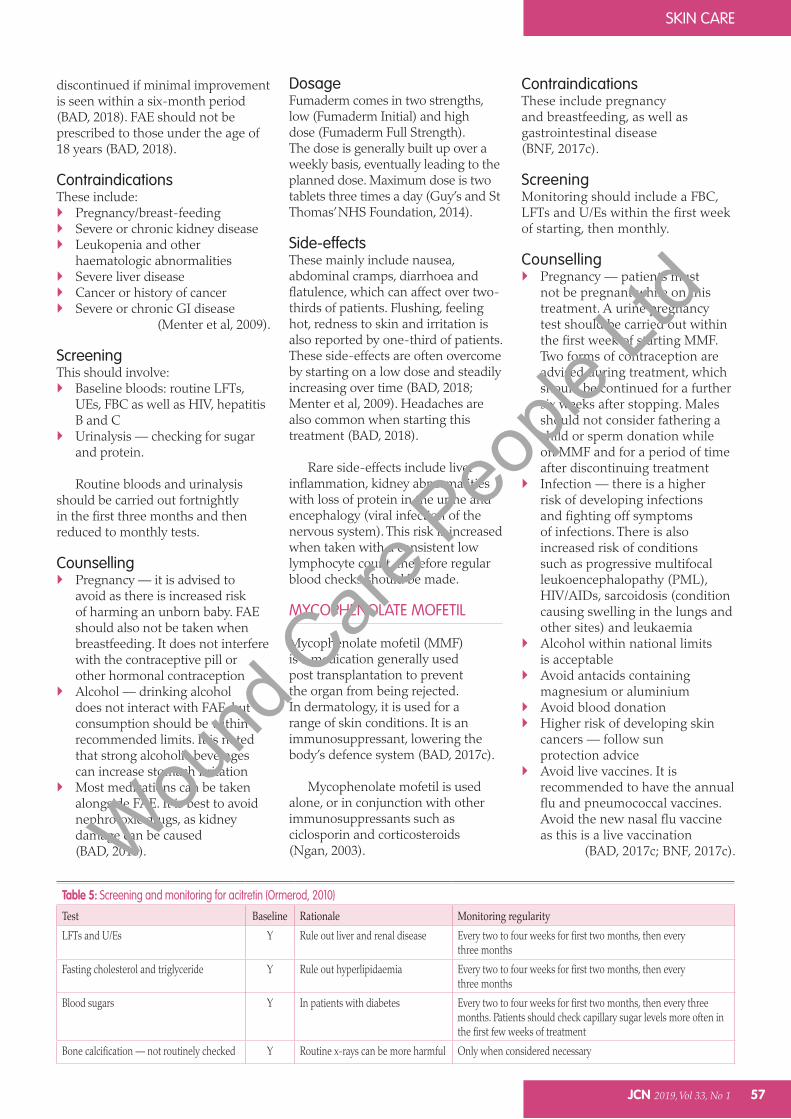
Table 5: Screening and monitoring for acitretin (Ormerod, 2010)
Test Baseline Rationale Monitoring regularityLFTs and U/Es Y Rule out liver and renal disease Every two to four weeks for first two months, then every
three months
Fasting cholesterol and triglyceride Y Rule out hyperlipidaemia Every two to four weeks for first two months, then every three months
Blood sugars Y In patients with diabetes Every two to four weeks for first two months, then every three months. Patients should check capillary sugar levels more often in the first few weeks of treatment
Bone calcification — not routinely checked Y Routine x-rays can be more harmful Only when considered necessary
Wound
Care
People
Ltd
SKIN CARE
58 JCN 2019, Vol 33, No 1
Antiepileptic drugs are not absorbed effectively
Clozapine — can result in lowering white blood cell count
Aciclovir interacts with MMF Certain antibiotics such as co-
amoxiclav and metronidazole can reduce the effect of MMF (Mydlarski, 2005; BAD, 2017c).
HYDROXYCARBAMIDE
This drug has been used since 1965. It is less frequently used than those already listed. It is often used in the treatment of cancer, and therefore is a cytotoxic drug. It slows the division of cell growth within the bone marrow (BAD, 2016b). It is not beneficial for pustular psoriasis, guttate psoriasis or psoriatic arthritis (Oakley, 2001).
It is a relatively quick-acting drug, with evidence of improvement to the skin noted within six to eight weeks. If tolerated and effective, it can be taken for many years.
ContraindicationsThese include pregnancy and breastfeeding, severe anaemia, reduced bone marrow function, as well as caution with kidney or liver damage.
ScreeningLiver function, U/Es and FBC pre-treatment and regularly
throughout time on the medication. Lymphadenopathy (lymph node checks) should be carried out at baseline and twice yearly (Menter et al, 2009). Monitoring these bloods should be carried out fortnightly for the first two months and then every two months (BNF, 2017d).
Counselling During treatment, females
should avoid pregnancy and males avoid fathering a child. Conception should be avoided for two months after stopping treatment. Breastfeeding is also contraindicated. Females should avoid handling this drug (BAD, 2017b)
• Avoidlivevaccines—theseasonal flu and pneumococcal vaccines are recommended.
DosageHydroxycarbamide is available in 500mg doses and generally prescribed as one to three capsules per day (BNF, 2017d). Side-effectsHydroxycarbamide slows cell growth and can alter the development of blood cells as they are formed in the bone marrow, which lowers the immune system. This can result in patients being more susceptible to picking up infections due to the reduced blood cell count. Other side-effects include: Breathlessness or fatigue due to
lowered red blood cells Bruising easily or increased risk
of bleeding Change in colour of skin pigment Temporary hair loss Loss of appetite with loose or
hard stools Leg ulcers Gout and drug-related lupus
(Oakley, 2001; BAD, 2016b; BNF, 2017d).
CONCLUSION
A variety of well-tried systemic treatments are readily available for moderate-to-severe psoriasis. They all carry their own range of side-effects and therefore require regular monitoring by both primary and secondary care teams. Patients need to be fully aware of these risks
DosageMycophenolate mofetil is often slow acting and can take up to three months to have a real effect on the skin, however, when it is effective, it can be used long term. Doses tend to range from 1–1.5g twice daily, with the maximum dose recommended at 3g. Tablets come in 250mg and 500mg (BNF, 2017c). MMF should be taken one to two hours before food at the same time of day, and taken even if feeling unwell, unlike most other immunosuppressant medications. The brand should not be switched. For best results, doses should not be missed.
Side-effectsThese can include: Nausea, vomiting, constipation,
diarrhoea, and indigestion, which generally reduce over time (Menter et al, 2009)
Anaemia — low red and/or white blood cell count
Low platelet count (thrombocytopenia)
Excessive bleeding or easy to bruise
Increased risk of developing skin cancers (BAD, 2017c).
Mycophenolate mofetil does
interact with a variety of other medications. These include: Antacids/iron/cholestytamine
(cholesterol reducing medication) reduce absorption of MMF
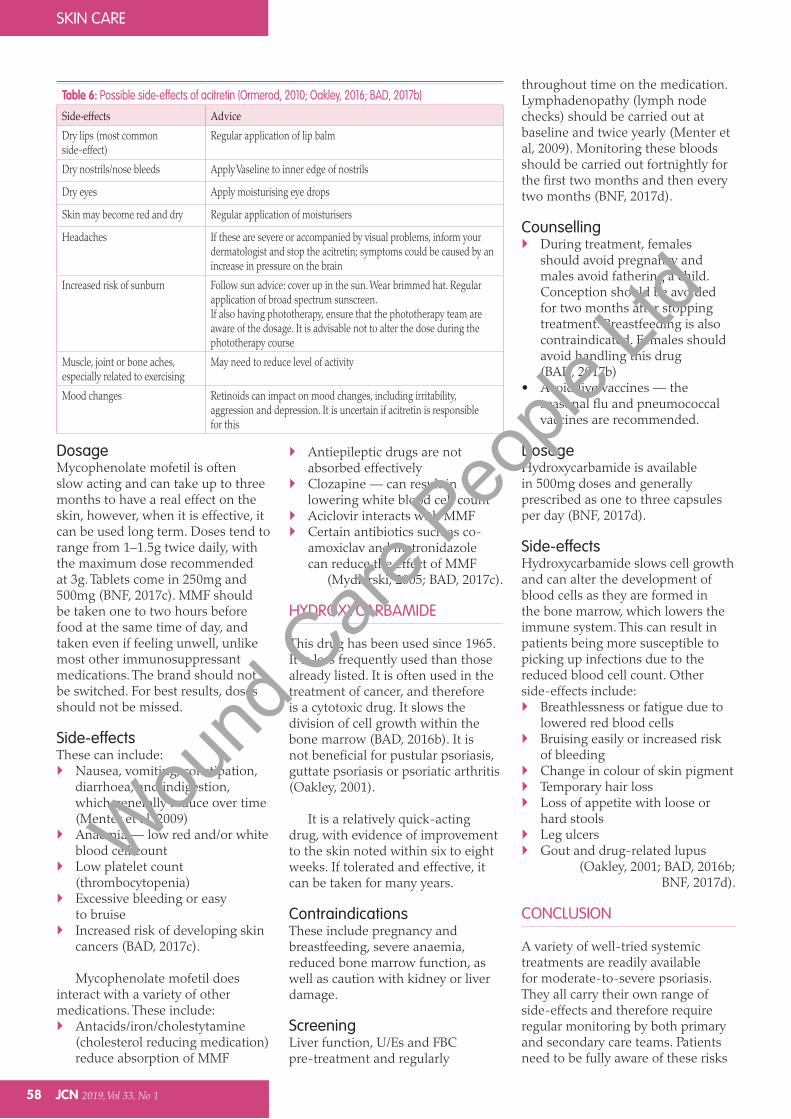
Table 6: Possible side-effects of acitretin (Ormerod, 2010; Oakley, 2016; BAD, 2017b)
Side-effects AdviceDry lips (most common side-effect)
Regular application of lip balm
Dry nostrils/nose bleeds Apply Vaseline to inner edge of nostrils
Dry eyes Apply moisturising eye drops
Skin may become red and dry Regular application of moisturisers
Headaches If these are severe or accompanied by visual problems, inform your dermatologist and stop the acitretin; symptoms could be caused by an increase in pressure on the brain
Increased risk of sunburn Follow sun advice: cover up in the sun. Wear brimmed hat. Regular application of broad spectrum sunscreen.If also having phototherapy, ensure that the phototherapy team are aware of the dosage. It is advisable not to alter the dose during the phototherapy course
Muscle, joint or bone aches, especially related to exercising
May need to reduce level of activity
Mood changes Retinoids can impact on mood changes, including irritability, aggression and depression. It is uncertain if acitretin is responsible for this
Wound
Care
People
Ltd
SKIN CARE
JCN 2019, Vol 33, No 1 59
and to weigh up the consequences versus the symptoms of their skin condition. Counselling is essential, as well as considering the holistic picture.
These treatments may lose their efficacy at some stage and so an alternative needs to be found, with further counselling specific to the chosen prescription.
Although side-effects should be considered seriously, these medications can relieve the symptoms and improve psoriasis. They cannot be guaranteed to entirely clear psoriasis, but often achieve an acceptable improvement, allowing patients to ‘claim back their lives’, which can have a significant positive psychological impact on both the patient and their family/carers.
REFERENCES
Armstrong AW, Harskamp CT, Armstrong EJ (2013) Psoriasis and the risk of diabetes mellitus: a systematic review and meta-analysis. JAMA Dermatol 149(1): 84–91
Arthritis Research UK (2014) Vaccinations and arthritis. Arthritis Research UK, Chesterfield. Available online: www.arthritisresearchuk.org/~/media/Files/Arthritis-information/Living-with-arthritis/2253-Vaccinations-and-Arthritis.ashx (accessed December 2018)
Berth-Jones J (2005) The use of ciclosporin in psoriasis. J Dermatolog Treat 16(5–6): 258–77
British Association of Dermatologists (2016a) Methotrexate. BAD, London. Available online: www.bad.org.uk/for-the-public/patient-information-leaflets/methotrexate/?showmore=1&returnlink=http%3a%2f%2fwww.bad.org.uk%2ffor-the-public%2fpatient-information-leaflets%3fgroup%3d00016001000200010003%26range%3dK-O#.WWuKD4jyvIU (accessed December 2018)
British Association of Dermatologists (2016b) Hydroxycarbamide (Formerly known as Hydroxyurea). BAD, London. Available online: www.bad.org.uk/shared/get-file.ashx?id=91&itemtype=document (accessed December 2018)
British Association of Dermatologists (2017a) Ciclosporin. BAD, London.
Available online: www.bad.org.uk/shared/get-file.ashx?id=288&itemtype=document (accessed December 2018)
British Association of Dermatologists (2017b) Acitretin. BAD, London. Available online: www.bad.org.uk/shared/get-file.ashx?id=1970&itemtype=document (accessed December 2018)
British Association of Dermatologists (2017c) Mycophenolate mofetil. BAD, London. Available online: www.bad.org.uk/shared/get-file.ashx?id=108&itemtype=document (accessed December 2018)
British Association of Dermatologists (2018) Fumaric Acid Esters. BAD, London www.bad.org.uk/shared/get-file.ashx?id=84&itemtype=document (accessed December 2018)
British National Formulary (2017a) BNF 74 September 2017 – March 2018. Methotrexate. National Institute for Health and Care Excellence, London. Available online: https://bnf.nice.org.uk/drug/methotrexate.html (accessed January 2019)
British National Formulary (2017b) BNF 74 September 2017 – March 2018. Acitretin. National Institute for Health and Care Excellence, London: 1156–57
British National Formulary (2017c) BNF 74 September 2017 – March 2018. Mycophenolate mofetil. National Institute for Health and Care Excellence, London: 796–7
British National Formulary (2017d) BNF 74 September 2017 – March 2018. Hydroxycarbomide. National Institute for Health and Care Excellence, London: 863
British National Formulary (2018) Ciclosporin. National Institute for Health and Care Excellence, London. Available online: https://bnf.nice.org.uk/drug/ciclosporin.html#monitoringRequirements
Cohen BE, Martirea KJ, Ho RS (2016) Psoriasis and the Risk of Depression in the US Population National Health and Nutrition Examination Survey 2009 – 2012. JAMA Dermatol 152(1):73–9
Drugs.com (2018a) Cyclosporine side-effects. Drugs.com, 7 June 2018. Available online: www.drugs.com/sfx/cyclosporine-side-effects.html (accessed January 2019)
Drugs.com (2018b) Cyclosporine: pregnancy and breastfeeding warnings. Drugs.com, Sept 25 2018. Available online: www.
drugs.com/pregnancy/cyclosporine.html (accessed January 2019)
Flechner SM, Katz AR, Rogers AJ, Van Buren C, Kahan BD (1985) The presence of cyclosporine in body tissues and fluids during pregnancy. Am J Kidney Dis 5(1): 60–3
Foucher J, Chanteloup E, Vergniol J, et al (2006) Diagnosis of cirrhosis by transient elastography (FibroScan): a prospective study. Gut 55(3): 403–8
Griffiths CE (1990) Systemic and local administration of cyclosporine in the treatment of psoriasis. J Am Acad Dermatol 2(6 pt2): 1242–7
Griffiths CE, Dubertret L, Ellis CN, et al (2004) Ciclosporin in psoriasis clinical practice: an international consensus statement. Br J Dermatol 150(S67): 11–23
Guy’s and St Thomas’ NHS Foundation Trust (2014) Taking Fumaderm (Fumaric Acid Esters) to treat psoriasis. Guys and St Thomas’ NHS Foundation Trust, London. Available online: www.guysandstthomas.nhs.uk/resources/patient-information/dermatology/fumaderm-to-treat-psoriasis.pdf (accessed December 2018)
Haustein UF, Rytter M (2000) Methotrexate in psoriasis: 26 years’ experience with low-dose long-term treatment. J Eur Acad Dermatol Venereol 14(5): 382–8
Kemp W, Roberts S (2013) FibroScan and transient elastography. Aust Fam Physician 42(7): 468–71
KEY POINTS Systemic treatments are
prescribed when the symptoms of psoriasis are not controlled with topical treatments or phytotherapy alone.
A thorough medical history must be taken as well as baseline tests to enable ongoing monitoring.
Patients should be made aware of the possible side-effects, lifestyle considerations and contraindications.
These medications can relieve symptoms and improve psoriasis, thereby reducing the psychological impact of the condition.
JCN
Wound
Care
People
Ltd
SKIN CARE
60 JCN 2019, Vol 33, No 1
Landriscina AL, Friedman AJ (2016) Integrating lifestyle approaches into psoriasis care: improving patient outcomes? Psoriasis (Auckl) 6: 1–5
MedLine Plus (2018a) Cyclosporine. Available online: https://medlineplus.gov/druginfo/meds/a601207.html (accessed December 2018)
MedLine Plus (2018b) Acitretin. Available online: https://medlineplus.gov/druginfo/meds/a601010.html (accessed January 2019)
Menter A, Korman NJ, Elmets CA, et al (2009) Guidelines of care for the management of psoriasis and psoriatic arthritis: section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am Acad Dermatol 451–85
Mydlarski PR (2005) Mycophenolate mofetil: A dermatologic perspective. Skin Therapy Lett 1–6
National Institute for Health and Care Excellence (2012) Psoriasis: assessment and management. Clinical guideline [CG153]. NICE, London. Available online: www.nice.org.uk/guidance/cg153 (accessed January 2019)
National Institute for Health and Care Excellence (2017) Psoriasis: Assessment and Management, Clinical Guidelines[CG153]. NICE, London. Available online: www.nice.org.uk/guidance/cg153/chapter/1-guidance#systemic-therapy
National Institute of Diabetes and Digestive and Kidney Disease (2014) Liver Biopsy. Available online: www.niddk.nih.gov/health-information/diagnostic-tests/liver-biopsy (accessed December 2018)
National Psoriasis Foundation (2015) Systemic Medications for psoriasis and psoriatic arthritis. National Psoriasis Foundation, Portland, USA: 1–29. Available online: www.psoriasis.org/sites/default/files/systemics_booklet.pdf (accessed December 2018)
National Psoriasis Foundation (2016)Fact Sheet. Soriatane (acitretin). National Psoriasis Foundation, Portland, USA. Available online: www.psoriasis.org/sites/default/files/soriatane_fact_sheet_2.pdf (accessed December 2018)
Ngan V (2003) Mycophenolate mofetil. Available online: www.dermnetnz.org/
topics/mycophenolate-mofetil/ (accessed December 2018)
Oakley A (2001) Hydroxyurea. Available online: www.dermnetnz.org/topics/hydroxyurea/ (accessed December 2018)
Oakley A, et al (2015) Methotrexate. Available online: www.dermnetnz.org/topics/methotrexate/ (accessed December 2018)]
Oakley A (2016) Acitretin. Available online: www.dermnetnz.org/topics/acitretin/ (accessed January 2019)
Oakley A, et al (2018) Ciclosporin. Available online: www.dermnetnz.org/topics/ciclosporin/ (accessed December 2018)
Ormerod AD, Campalani E, Goodfield MJD (2010) British Association of Dermatologists guidelines on the efficacy and use of acitretin in dermatology. Br J Dermatol 162(5): 952–63
Parisi R, Symmons DP, Griffiths CE, Ashcroft DM, Identification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) project team (2013) Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol377–85
Psoriasis Association (2014) Ciclosporin. Psoriasis Association, Northampton. Available online: www.psoriasis-association.org.uk/media/InformationSheets/Ciclosporin.pdf (accessed December 2018)
Psoriasis and Psoriatic Arthritis Alliance (2018) Methotrexate for psoriasis. Available online: www.papaa.org/immunosuppressant-therapies/methotrexate-psoriasis (accessed December 2018)
Rajakulendran S, Gadsby K, Deighton C (2008) Rheumatoid arthritis, alcohol, leflunomide and methotrexate. Can changes to the BSR guidelines for leflunomide and methotrexate on alcohol consumption be justified? Musculoskeletal Care 6(4): 233–45
Rutter MK, Kane K, Lunt M, et al (2016) Primary care-based screening for cardiovascular risk factors in patients with psoriasis. Br J Dermatol 175(2): 348–56
Shea B, Swinden MV, Tanjong Ghogomu E (2013) Folic acid and folinic acid for reducing side-effects in patients receiving methotrexate for rheumatoid
arthritis. Cochrane Database Syst Rev (5): doi: 10.1002/14651858.CD000951.pub2
UK Teratology Information Service (2017) Use of ciclosporin in pregnancy. Public Health England, London. Available online: www.medicinesinpregnancy.org/bumps/monographs/USE-OF-CICLOSPORIN-IN-PREGNANCY/?print=y (accessed December 2018)
Visser K, Katchamart W, Loza E, et al (2009) Multinational evidence-based recommendations for the use of methotrexate in rheumatic disorders with a focus on rheumatoid arthritis: integrating systematic literature research and expert opinion of a broad international panel of rheumatologists in the 3E Initiative. Ann Rheum Dis 68(7): 1086–93
Warren RB, Weatherhead SC, Smith CH, et al (2016) British Association of Dermatologists’ guidelines for the safe and effective prescribing of methotrexate for skin disease 2016. Br J Dermatol175(1): 23–44
Whittle SL, Hughes RA (2004) Folate supplementation and methotrexate treatment in rheumatoid arthritis: a review. Rheumatology (Oxford) 267–71
Wollina U (2011) Fumaric acid esters in dermatology. Indian Dermatol Online J 2(2): 111–19
Having read this article,
Your understanding of psoriasis and how and when to use treatments
If you are familiar with the guidelines set out by NICE
Your knowledge of the different products available and how they work.
Then, upload the article to the new, free JCN revalidation e-portfolio as evidence of your continued learning: www.jcn.co.uk/revalidation
RevalidationAlert
Wound
Care
People
Ltd





























