Embed Size (px)
Citation preview

Psychiatric Aspects of
Non-HIV Infectious Diseases
Robert K. Schneider, MD
Michael J. Robinson, MD
James L. Levenson, MD

Why Now?
• Global Society– Increased Travel– Increased Immigration/Emigration
• Broader Medical Management– HIV– Malignancies– Transplantation
• People living longer

Infectious Disease SyndromesChapter 52
Robert K. SchneiderJames L. Levenson

Risk Groups
Immune Status
Demographics

Risk Groups
• Immune Status– Elderly– Chronic Disease
• HIV
• Malignancy
• Transplant
• Diseases where immunosuppressants are used – (ie SLE, Psoriasis, IPF)
– Substance Abuse

Risk Groups
• Demographics– Children– Recreational Activities– Occupation– Region of origin or residence– Travel

Assessment
• Consider infectious causes when patient is in the risk group– Immune Status
– Demographics
• Activate an appropriate differential diagnosis
• Know the best tests to evaluate these patients
• Know the best treatments for these conditions

Case One
Postpartum Woman with Psychosis

Postpartum Woman with Psychosis
• 34 yo woman 4 weeks postpartum
• 3 week history of paranoid ideation and
auditory hallucinations
• Other points on history?

Postpartum Woman with Psychosis
• Recently emigrated from Mexico
• The family reports seizure disorder since
age 3
• Several family members have seizures
• Family reports no substance abuse

What’s the differential diagnosis?
• Postpartum psychosis
• Ictal or interictal psychosis
• Substance Abuse
• Malignancy
• Infectious causes– Brain Abscess– Toxoplasmosis– Neurocysticerosis– Tuberculosis

Postpartum Woman from Mexico
• EEG: “normal”• Urine Drug Screen: Negative
(collateral family hx supports this)
• CXR: normal• CBC: 7,000: 60 neut; 5 eos; 30 lymph; 5 mono• Hct: 40%• Biochemical Profile: WNL• HIV: negative

Postpartum Woman from Mexico
• Head CT with and without contrast: multiple cystic and calcified lesions
• CSF: – 24 WBC all lymphs– Protein and Glucose: wnl– Stains: negative– Cultures: pending
• Serology:– Pending


Differential Diagnosis:Toxoplasmosis
• Exceedingly common in general population
• Disease occurs only in
immunocompromized host
• Most common treatable cerebral lesion in HIV
• CT: ring enhancing lesions
• CSF: pleocytosis
• Serology: antibody positive 67%

Differential Diagnosis:Tuberculosis
• 15% extrapulomanry
• Most CNS TB is parameningeal– Cerebral TB is very rare
• CT scan: negative or meningeal granulomas
• CSF: almost always reactive– Depressed glucose– Increased WBC– Markedly elevated protein– Stains positive 25%/Cultures positive 75%

Differential Diagnosis:Brain Abscess
• Patient usually with evidence of systemic infection
• History of IVDA, Valvular heart disease or recent neurosurgery
• CSF: virtually always positive, particularly on stains showing organisms

Neurocysticercosis
• The “Pork Tapeworm”
• Caused by the larval form of Taenia solium
• Most widely disseminated neuroparasitosis
• CNS is the most frequently affected organ (92%)
• Most common cause of seizures in endemic areas
• Endemic in Latin America, sub-Saharan Africa, India and China




Classification
• Inactive disease
• Active disease– Parenchymal– Ventricular– Subarachnoid– Spinal and ocular

Neuroimaging
• CT scan is the primary means of diagnosis
• Most commonly reveals inactive disease– <1 cm calcifications– Hydrocephalus is evident secondary to obstructive
intraventricular disease
• Active Disease– Ring enhancing cystic lesions– Pathognomonic scolex is sometimes seen in the cyst– Meningeal disease is hard to detect on CT


How good is serology in NCC?
• CDC immunoblot assay• Acknowledged as immunodiagnositic by:
– World Health Organization – Pan American Health Organization
• 100% specific• Sensitivity varies:
– Multiple lesions: 90%– Single enhancing parenchymal cysts: <50%– Clinically defined patients with calcified cysts: 70%

What are the Psychiatric Aspects of NCC?
• Depression: >50% in outpatient setting
• Psychosis: 14% in outpatient, probably higher at presentation (inpatient)
• Delirium often present at presentation
• Cognitive decline and symptoms of hydrocephalus
• Headache is common but nonspecific

What’s the best treatment?
• If inactive disease, no treatment except for the seizure disorder.
• If active disease, corticosteroids and praziquantel is the main stay.
• However, praziquantel is toxic and recent RCT suggest no benefit over symptomatic treatment.
• In hydrcephalus (usually inactive, chronic NCC) surgically shunting is indicated.

What areas of the US is NCC rising?
• Prevalence in US is increasing, especially in areas with high immigrant populations – (eg Texas, California)
• Most cases occur among Latin American immigrants
• Local transmission is probably higher than expected

Does NCC occur in travelers?
• Yes
• Can occur with only brief contact
• Risk increases the longer the contact
Cysticercosis surveillance: Locally acquired and travel-rated infections and detection of intestinal tapeworm carriers in Los Angeles Count. Sorvillo FJ, Waterman SH, Richards FO, Schantz PM. Am J Trop Med Hyg. 1992;47(3),365-371.

Are you safe if you don’t eat pork?
• No• Most transmission occurs from eating food
that is fertilized with pork or human waste• Also carriers that are food handlers can
transmit T. solium• NCC occurred in an Orthodox Jewish
community in New York City. Infection was secondary to food handlers who were carriers of T soliumNeurocysticerosis in an Ortodox Jewish Community in New York city. Schantz PM, Moore AC, Munoz JL, et al. NEJM 1992;327:692-5

Wrap up and questions ?

Case Two
The Pediatric PatientThe Pediatric Patient

The CaseThe Case
• LR is a 5 year old girl who presents with the following complaints from her parents:
• HPI:– “she has recently started to obsess about
everything”– “she is constantly counting to four”– “everything has to be in its certain place or she
gets really upset”

The CaseThe Case
– “she repeatedly blinks” and “jerks her head the the side”
– “she later started to do things with her voice”
– Other associated behavior complaints
• Recent PMHx:– sick with a fever on and off for the last few months
– CXR - normal
– No other investigations have been performed

The CaseThe Case
• Past Psych Hx:– None; No emotional, behavioral, or school
problems noted
• Past Medical Hx:– early childhood recurrent otitis media, not
requiring myringotomy tubes or prophylactic antibiotics

The CaseThe Case
• Family hx:– first of 2 children; healthy younger brother
– maternal hx of depression responsive to antidepressant medications
– maternal grandmother with a hx of trichotillomania
– paternal hx of vocal tics as a child
– No OCD, No Sydenham’s chorea, No Rheumatic fever

Differential DiagnosisDifferential Diagnosis
• OCD• ADHD• Separation Anxiety• PANDAS• Sydenham’s Chorea• Transient Tic Disorder• Tourette’s Disorder / Chronic Motor or Vocal Tic
Disorder

Initial Work-Up?Initial Work-Up?
• Throat Culture Positive for GABHS
• Anything else?– MRI?– D8/17?– Anti-GABHS antibody titres? Which ones?

PANDASPANDAS
• PANDAS = ?
• Inclusionary Criteria:– Presence of OCD and/or tic disorder– Pediatric onset– Episodic course of symptom severity– Association with GABHS infection– Association with neurological abnormalities

PANDAS
• Proposed Pathogenesis:
– Pathogen + Susceptible Host Immune Response Sydenham’s Chorea or PANDAS

PANDASPANDAS
• Association with GABHS?– Positive throat culture
• Is a positive throat culture enough to demonstrate recent GABHS infection?
– Elevated ASO and/or AntiDNase-B titres• Are elevated titres enough to demonstrate recent
GABHS infection?
– Can a child have a relapse of symptoms without evidence for a recent GABHS infection?

PANDASPANDAS
• Any other investigations?– Is an MRI warranted?– What is the significance of B-lymphocyte
antigen D8/17? Should we test for it?

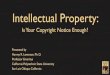
Example Relationship Between AntiDNAse-B titres and Ratings of OCD and Tourette's
0
10
20
30
40
50
0 2 4 6 8 10 12 14
Time (Months)
Rat
ing
s
0
200
400
600
800
1000
An
tib
od
y T
itre
(IU
/ml)
C-YBOCS Ratings Tourette Syndrome Unified Rating Scale AntiDNAse-B titres
IVIG Treatment

PANDAS - Treatment OptionsPANDAS - Treatment Options
• Antibiotics?– Acute treatment and/or prophylaxis?
• Plasma exchange/Plasmaphoresis
• Intravenous immunoglobulin

Discussion & QuestionsDiscussion & Questions

Case Three
Tick-bitten Hikers

• 35 year-old woman, hiked Appalachian Trail
• One week: flu-like symptoms, large rash on groin, facial palsy, Lyme serology negative
• Two months: headache, stiff neck, arm numb and burning
• One year: depression, fatigue, forgetful

• 36-year-old man, hiked Glacier National Park
• One week: flu-like symptoms, parethesias in hands and feet
• Two months: headache, stiff neck, fatigue, Lyme serology positive
• One year: depression, fatigue, diffuse myalgia

Lyme Disease
• Caused by spirochete, Borrelia burgdorfei
• Transmitted by deer ticks (<5% risk)
• Over 10,000 cases/year reported in U.S.
• Over 90% from 8 states (CT, RI, NY, NJ, PA, MD, WI, MN)

The Deer Tick

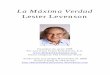
Incidence of Lyme per 100,000

Disease Onset (One week)
• Erythema migrans, >90%
• Central clearing, <40%

Erythema Migrans

Acute Disseminated Disease (First month)
• Fatigue, 54%
• Myalgia/arthralgia, 44%
• Headache, 42%
• Fever/chills, 39%
• Stiff neck, 35%

Subacute Disease (Months)
• Arthritis, oligoarticular, most often knee, 60%• Secondary skin lesions, 50%• Neurological, 15%
– Cranial neuropathy, most often VII
– Meningitis
– Painful radiculopathy
• Carditis (conduction disturbance), 5-10%

Chronic Disease (Years)
• Dermatitis
• Arthritis
• Neurological
– Mild sensory radiculopathy
– Cognitive dysfunction
– Depression

Chronic Neuroborreliosis – Diagnostic Tests
• CSF abnormal (>50%): protein, Ab positive
• MRI abnormal (25%): White matter lesions
• EEG normal
• Neuropsych testing abnormal

Lyme disease is a clinical diagnosis
Serology can support but not make diagnosis

Serology
• Two step
• Initial: ELISA (or IPA)
• If positive: Western blot

Serology Limitations
• False negative in early infection
• False negative after early antibiotics
• False positive in other infections, autoimmune diseases
• True positive uncorrelated with time or activity

Treatment
• Acute disease: – oral doxycycline or amoxicillin, 2-4 weeks
• Neuroborreliosis: – IV ceftriaxone, 2-4 weeks
• Complete recovery is the rule

Prevention
• Prophylaxis not recommended after tick bite
• Cover up and DEET
• Vaccine effective – 50-70% first year – 75-90% second year

• 35-year-old woman, hiked Appalachian Trail • One week: flu-like symptoms, large rash
on groin, facial palsy
• Two months: headache, stiff neck, arm numb and burning
• One year: depression, fatigue, forgetful

• 36-year-old man, hiked Glacier National Park
• One week: flu-like symptoms, parethesias in hands and feet
• Two months: headache, stiff neck, fatigue, Lyme serology positive
• One year: depression, fatigue, diffuse myalgia

Differential Diagnosis
• Fibromyalgia
• Chronic fatigue syndrome
• Other infections
• Somatoform disorders
• Depression
• Autoimmune diseases
• Multiple sclerosis

Consequences of Overdiagnosis & Overtreatment
• Somatization
• Invalidism
• Antibiotic side effects
“Lyme colitis” (Clostridia enteropathy)

Questions?