Embed Size (px)
Citation preview
INTERNATIONAL JOURNAL OF GERIATRIC PSYCHIATRY, VOL 10: 849-854 ( 1 995)
PSYCHIATRIC DIAGNOSES, OUTCOMES AND LENGTHS OF STAY OF PATIENTS ADMITTED
TO AN ACUTE PSYCHOGERIATRIC UNIT FRANCINE MOSS AND BRETT WILSON
Psychiatrists, Psychogeriatric Unit, Royal Park Hospital, Victoria, Australia
SUSAN HARRIGAN Stutistician, University of Melbourne Department of Psychiatry, Royal Purk Hospital, Parkville, Victoria, Australia
DAVID AMES Associate Professor of Psychiatry of' Old Age, University of Melbourne Department of Psychiatry, Royal Melbourne
Hospital, Parkville, Victoria, 3050, Australia
SUMMARY One hundred and ten consecutive patients admitted to an acute psychogeriatric unit were assessed with the Geriatric Mental State Schedule, assigned a DSM-111-R diagnosis and their length of stay in hospital and discharge destination noted. Forty-two per cent of patients had organic disorders (mainly dementia), 32% had affective disorders (mainly depression) and 23% had schizophrenia or a related disorder. The median length of stay was 29 days and bore little relation to diagnosis, age, sex or cognitive function. Patients with an organic mental disorder were more likely to enter long-term institutional care, but 78% of patients were able to return to the same level of accommodation (own home, hostel or nursing home) that they had occupied prior to admission. On a four-point non-blind outcome scale, 86% of patients were rated as improved at discharge.
KEY wow-psychiatric disorder; prevalence; elderly; psychogeriatric unit
In recent years specialist psychiatric services for the elderly have proliferated in several developed coun- tries, but randomized clinical trials to determine their effectiveness have not been performed (Cole, 1988). Epidemiological data and population projec- tions alone will not convince health planners of the need for maintenance o r expansion of services unless formal evaluations demonstrate their worth (Draper, 1990). Yet even straightforward published descriptions of the work of specialist acute psycho- geriatric units are few in number and flawed in design. We have traced six such studies published in the last 16 years. Two studies from Australia (Gil- Christ et d., 1985; Harrison et ul., 1988) and four from North America (Baribeau-Braun et al., 1979; Spar et al., 1980; Mei-Tal and Meyers, 1985; Rock- wood et al., 1991) assessed between 83 and 130
Address for correspondence: Dr. David Ames, University of Melbourne Department of Psychiatry, 7th Floor, Charles Con- nibere Building, Royal Melbourne Hospital, Parkville, Victoria, 3050. Australia
patients admitted to acute psychogeriatric units but none used a structured interview to assess the mental state, most report data based on chart diag- noses alone and the majority seem to have been retrospective. Affective illnesses accounted for be- tween 19% and 61% of admissions while dementia was the main diagnosis for between 23% and 58% of patients in these studies. Schizophrenic and para- noid illnesses were less prevalent, accounting for between 7% and 16Yo of admissions. Lengths of stay have not always been reported. Rockwood et al. (1991) found their patients stayed in hospital for a median period of 92 days, but studies reporting mean lengths of stay have a range from 32 to 44.5 days per patient. There has been variable success reported in returning patients to their original environments.
In order to document our inpatient work and to identify target areas for improved efficiency we have used a semi-structured interview to prospectively assess 1 10 consecutive admissions to Melbourne's
CCC 0885-6230/95/'100849-06 C 1995 by John Wiley & Sons, Ltd.
Received 21 September 1994 Accepted 19 January 1995

850 F. MOSS, B. WILSON, S. HARRIGAN AND D. AMES
largest acute psychogeriatric inpatient unit. We then attempted to relate diagnostic and demo- graphic variables to length of stay in hospital, dis- charge destination and outcome rated on a four-point scale.
METHOD
Setting and subjects
Royal Park Hospital is an acute psychiatric hos- pital which serves the northern and western suburbs of Melbourne, a city of nearly 3 million inhabitants. In 1991 census figures indicated that its 36-bed acute psychogeriatric unit (PGU) served a catchment area of 86 893 people aged 65 and over. Although a few elderly people with acute psychiatric illness are treated in private hospitals, the great majority who require admission are treated in the public sector and PGU is the only facility of this type in the region. One bed in the unit is set aside for planned family respite admissions while the other 35 beds are available at all times for both voluntary and invol- untary admissions of people aged above 65 with psychiatric illness. The unit also admits a few patients aged below 65 with presenile dementia, or multiple medical problems complicating functional psychiatric illness.
Because we aimed to assess 100 consecutively admitted patients a sampling period of 20 weeks was selected, as admission and discharge data from the previous year indicated that this would be the approximate time required to accumulate 100 ad- mission episodes.
Diagnoses All admitted patients were approached for inter-
view with the Geriatric Mental State Schedule (GMS) (Copeland et al., 1976) and the Mini Mental State Examination (MMSE) (Folstein et al., 1975). They were assessed by either FM or BW. FM con- sulted past admission notes, took historical details from patients, informants and members of staff and discussed each patient with the consultant psychia- trist in charge of his or her treatment. Together she and DA used all available data to make an admis- sion DSM-111-R diagnosis (American Psychiatric Association, 1987) for each patient. The date of admission, type of accommodation occupied prior
to admission and basic demographic data were re- corded. At a later date the length of stay in hospital and discharge destination were determined for each study participant and related to age, sex and initial psychiatric diagnosis. When a patient was trans- ferred to a general or geriatric hospital for treatment of an intercurrent medical condition and then returned to PGU for further psychiatric treatment, their length of stay in the unit was calculated as the number of days from initial admission to final dis- charge minus the number of days absent in another hospital. Patients who stayed in PGU awaiting the arrangement of accommodation after they were designated as fit to leave by the treating team were identified and classed as a group with ‘placement problems’. The treating medical officer was asked to rate each patient on discharge as greatly improved, somewhat improved, unchanged or worse with respect to the problem which had prompted the admission.
Statistical analysis Data analysis was performed using the statistical
package SPSS for Windows. Descriptive statistics on a range of sociodemographic and diagnostic variables were computed.
Non-parametric methods of analysis were employed to examine group differences on length of stay as this variable was non-normally distributed. Specifically, group differences on length of stay were assessed using the Mann-Whitney U test. Where more than two groups were compared, the Kruskal-Wallis one-way analysis of variance was applied. The relationship of diagnosis to outcome and destination was examined by cross-tabulating each of these variables with diagnosis and calculat- ing odds ratios and 95% confidence intervals.
Hierarchial multiple regression analysis was used to examine the relationship between length of stay and diagnostic and demographic variables. Evalu- ation of the assumptions of regression analysis necessitated a square root power transformation of the dependent variable, length of stay. As the amount of variance accounted for by the predictor variables was similar for both the transformed and untransformed length of stay variable, only the results for untransformed length of stay have been reported.
All statistical tests were two-tailed and outcomes were regarded as significant at or below the 0.05 probability level.

INPATIENT DIAGNOSES, STAY AND OUTCOMES 85 1
RESULTS
Patients
Over 20 weeks from the beginning of March 1993, there were 110 admissions of 99 patients. One de- mented female patient with recurrent depression was admitted five times for maintenance ECT, a male dementia patient had three respite admissions and five other patients had two admissions each. Results will be reported by admission episodes rather than as individual patients.
The 110 admissions included 45 males (41%). Ages were normally distributed with a mean of 74 years (SD 8 years, median 73, range 57-92). Forty- one per cent of admissions were of widowed patients, 29% were married or in de facto relation- ships, 17% divorced or separated and 12% were single. Seventy per cent of admitted patients spoke English as their first language, 8% Italian, 6% Polish, 5% Greek, 3% Arabic and 9% spoke eight other tongues. Of the 33 admitted patients whose first language was not English, 16 required an inter- preter for GMS and MMSE interviews.
The usual residence of 43 admitted patients was an institution (15 from nursing homes, 28 from hostels or special accommodation houses). Of the remainder, 26 lived alone in a house, flat or caravan, 22 lived with a spouse, 15 with other family and four in boarding houses or private hotels. Although most patients came directly from their usual abode to PGU, six were transferred from general hospital wards, five from casualty departments, three from a geriatric hospital, four from other wards at Royal Park and one from another psychiatric hospital.
Presenting problems and diagnoses Seven admissions eluded MMSE examination
and two could not be interviewed with the GMS, though they were allocated a diagnosis after dis- cussion with the treating team.
Thirty-seven admissions (34%) were for the management of disturbed behaviour in the context of dementia, 3 1 (28%) for treatment of depression, 22 (20%) for treatment of schizophrenia or other paranoid illness, nine (8%) for mania, seven (6%) for planned respite and four (4%) for other reasons.
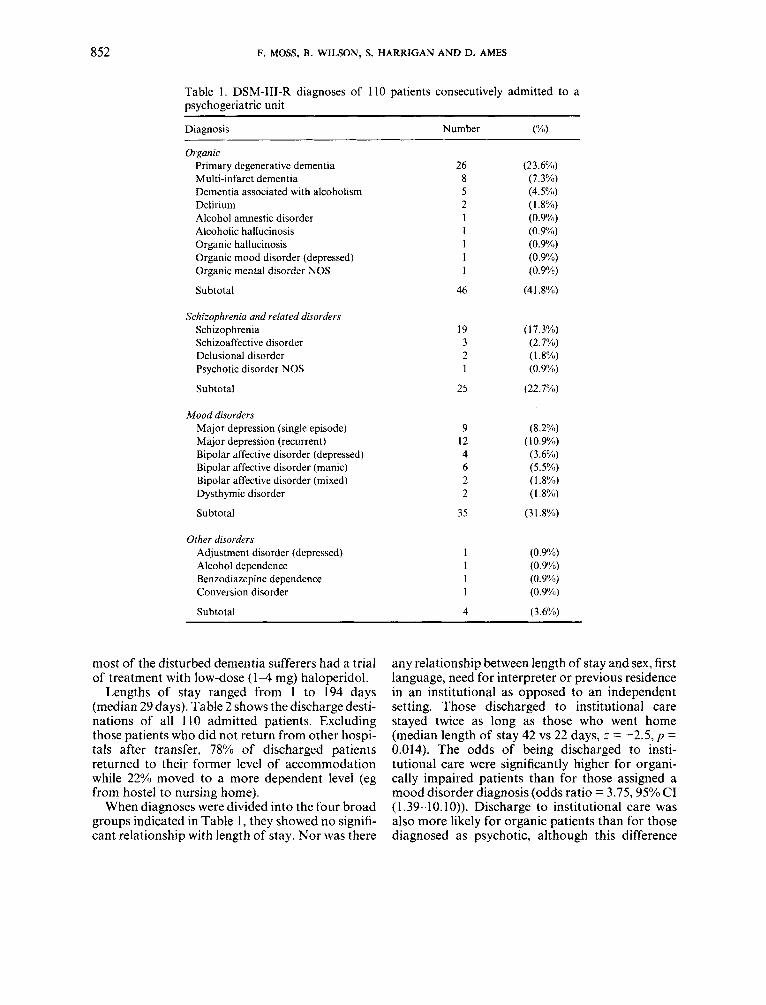
Table 1 shows the DSM-111-R diagnoses of the 110 admitted patients. Their MMSE scores ranged from 0 to 30 (median 20) and were not normally distributed. Thirty-nine patients (35%) were experi-
encing their first ever psychiatric admission, 12 (1 1%) were on their second and 30 (27%) on their third or subsequent admission to PGU, while 29 (26%) had never been to PGU but had been ad- mitted to other psychiatric facilities before. Eighty- two patients (75%) were detained involuntarily during their stay in PGU. All 39 patients with de- mentia, both delirious patients, the individuals with alcohol amnestic disorder and alcoholic hallucino- sis, 19 patients with schizophrenia or related dis- order, 13 with major depression (10 were psychotic and two others could not give consent for ECT), six patients with mania or mixed affective psychosis and the patient with conversion disorder comprised the 82 patients with involuntary status. Five de- mentia patients were on family respite admissions and the others had disturbed behaviours which in- cluded physical aggression, absconding, wandering, screaming and marked resistance to routine care interventions.
Intercurrent medical problems and transfers
Twenty-one patients (1 9y0) had to be transferred to a general or geriatric hospital, but 13 returned to PGU after treatment. The reasons for transfer were diverse and included four patients with compli- cations of ischaemic heart disease, three fractures or dislocations, two with neoplasms, two with delir- ium, and one each with dehydration, urinary tract infection, gynaecological surgery, seizures, Parkin- son’s disease, temporal artery biopsy, cataract sur- gery, stroke, for neuropsychiatric evaluation and neurosurgical assessment of a ventricular shunt. One patient from a remote area was transferred to a psychiatric hospital closer to home and one was transferred to the Royal Park rehabilitation unit.
Intercurrent medical problems not requiring transfer were extremely common as has been the case in earlier studies, but no formal record of these was maintained.
Treatments, lengths of stay and outcomes Treatments employed included conventional
physical therapies, a depression treatment group (Moffatt et al., 1995), other occupational therapy and support groups and a specific dementia management programme. Fifteen patients received ECT. All had depression as a primary or secondary diagnosis. All other depressed subjects received an- tidepressants or lithium, all schizophrenic and de- luded individuals received antipsychotic drugs and
852 F. MOSS, B. WILSON, S. HARRIGAN AND D. AMES
Table 1. DSM-111-R diagnoses of 110 patients consecutively admitted to a psychogeriatric unit
Diagnosis Number (%)
Organic Primary degenerative dementia Multi-infarct dementia Dementia associated with alcoholism Delirium Alcohol amnestic disorder Alcoholic hallucinosis Organic hallucinosis Organic mood disorder (depressed) Organic mental disorder NOS
Subtotal
Schizophrenia and related disorders Schizophrenia Schizoaffective disorder Delusional disorder Psychotic disorder NOS
Subtotal
Mood disorders Major depression (single episode) Major depression (recurrent) Bipolar affective disorder (depressed) Bipolar affective disorder (manic) Bipolar affective disorder (mixed) Dysthymic disorder
Subtotal
Other disorders Adjustment disorder (depressed) Alcohol dependence Benzodiazepine dependence Conversion disorder
Subtotal
26 8 5 2 1 1 1 1 1
46
19 3 2 1
25
9 12 4 6 2 2
35
1 1 I 1
4
(23.6%)) (7.3%) (4.5%) (1.8%) (0.9%) (0.9%) (0.9%1) (0.9%1) (0.9%)
(41.8%))
( 1 7.3%) (2.7%) (1.8%) (0.9%))
(22.7%))
(8.2%) (1 0.9%) (3.6%)) (5.5%) (1.8%) (1.8%1)
(3 1.8%)
(0.9%) (0.9'Yu) (0.9%) (0.99'0)
(3.6%))
most of the disturbed dementia sufferers had a trial of treatment with low-dose ( 1 4 mg) haloperidol.
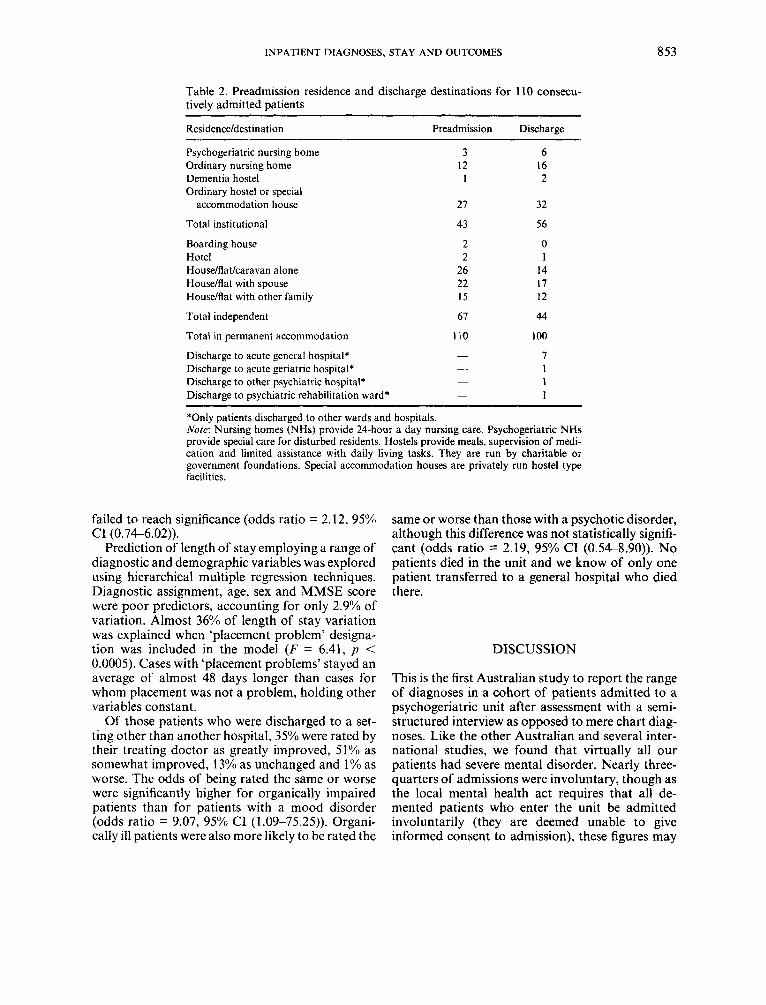
Lengths of stay ranged from 1 to 194 days (median 29 days). Table 2 shows the discharge desti- nations of all 110 admitted patients. Excluding those patients who did not return from other hospi- tals after transfer, 78% of discharged patients returned to their former level of accommodation while 22% moved to a more dependent level (eg from hostel to nursing home).
When diagnoses were divided into the four broad groups indicated in Table 1, they showed no signifi- cant relationship with length of stay. Nor was there
any relationship between length of stay and sex, first language, need for interpreter or previous residence in an institutional as opposed to an independent setting. Those discharged to institutional care stayed twice as long as those who went home (median length of stay 42 vs 22 days, z = -2.5, p = 0.014). The odds of being discharged to insti- tutional care were significantly higher for organi- cally impaired patients than for those assigned a mood disorder diagnosis (odds ratio = 3.75,950/0 CI (1.39-10.10)). Discharge to institutional care was also more likely for organic patients than for those diagnosed as psychotic, although this difference
INPATIENT DIAGNOSES, STAY AND OUTCOMES 853
Table 2. Preadmission residence and discharge destinations for 110 consecu- tively admitted patients
~ ~~~~~
Preadmission Discharge
Psychogeriatric nursing home Ordinary nursing home Dementia hostel Ordinary hostel or special
accommodation house
Total institutional
Boarding house Hotel House/flat/caravan alone House/flat with spouse House/flat with other family
Total independent
Total in permanent accommodation
Discharge to acute general hospital* Discharge to acute geriatric hospital* Discharge to other psychiatric hospital* Discharge to psychiatric rehabilitation ward*
3 12
I
21
43
2 2
26 22 15
61
110
6 16 2
32
56
0 1
14 17 12
44
100
7 1 1 1
*Only patients discharged to other wards and hospitals. Note: Nursing homes (NHs) provide 24-hour a day nursing care. Psychogeriatric NHs provide special care for disturbed residents. Hostels provide meals, supervision of medi- cation and limited assistance with daily living tasks. They are run by charitable or government foundations. Special accommodation houses are privately run hostel type facilities.
failed to reach significance (odds ratio = 2.12, 95% CI (0.74-6.02)).
Prediction of length of stay employing a range of diagnostic and demographic variables was explored using hierarchical multiple regression techniques. Diagnostic assignment, age, sex and MMSE score were poor predictors, accounting for only 2.9% of variation. Almost 36% of length of stay variation was explained when ‘placement problem’ designa- tion was included in the model ( F = 6.41, p < 0.0005). Cases with ‘placement problems’ stayed an average of almost 48 days longer than cases for whom placement was not a problem, holding other variables constant.
Of those patients who were discharged to a set- ting other than another hospital, 35% were rated by their treating doctor as greatly improved, 51% as somewhat improved, 13% as unchanged and 1940 as worse. The odds of being rated the same or worse were significantly higher for organically impaired patients than for patients with a mood disorder (odds ratio = 9.07, 95% C1 (1.09-75.25)). Organi- cally ill patients were also more likely to be rated the
same or worse than those with a psychotic disorder, although this difference was not statistically signifi- cant (odds ratio = 2.19, 95% CI (0.54-8.90)). No patients died in the unit and we know of only one patient transferred to a general hospital who died there.
DISCUSSION
This is the first Australian study to report the range of diagnoses in a cohort of patients admitted to a psychogeriatric unit after assessment with a semi- structured interview as opposed to mere chart diag- noses. Like the other Australian and several inter- national studies, we found that virtually all our patients had severe mental disorder. Nearly three- quarters of admissions were involuntary, though as the local mental health act requires that all de- mented patients who enter the unit be admitted involuntarily (they are deemed unable to give informed consent to admission), these figures may

8 54 F. MOSS, B. WILSON, S. HARRIGAN AND D. AMES
not be comparable with studies from places with more liberal mental health legislation. Most other involuntary patients were deluded and refusing necessary treatment.
It has been suggested that the low rates of neu- rotic disorder encountered in psychogeriatric ad- mission samples may reflect low base rates in the community or failure of primary care physicians to refer (Pitt, 1982). Our impression is that it simply relates to the constraints of available resources. The unit runs at close to 100% capacity and to be ad- mitted patients need to be very ill, very disturbed or both. Most are demented or deluded.
The main diagnostic difference between our sam- ple and those discussed in the introduction was the high rate of schizophrenia and related disorders. This may reflect referral patterns. While our unit does not object to general adult services continuing to manage schizophrenic patients after the age of 65, virtually all are referred on to us soon after their birthdays, again because of perceived resource limi- tations affecting the general adult services. In addition, there are no long-term psychiatric beds within our catchment area and the few that remain in two Melbourne hospitals are being closed rapidly.
It was impressive that such a high proportion of patients (78%) could return to their previous level of accommodation, particularly when one considers that over a third of the sample were suffering from dementia. We doubt that it would be ethical to conduct a trial to determine whether the treatments received in PGU determined the level of care re- quired on discharge but it is noteworthy that despite the non-blind nature of our crude outcome measures, only one patient was rated by the treating team as worse and 86% were thought to have im- proved by the time of discharge.
A large number of variables had little impact on length of stay when subject to a regression analysis. It was not surprising that a designation of ‘place- ment problem’ was associated with increased length of stay as patients moving to institutional care stayed twice as long as those returning to indepen- dent living. Streamlining of placement procedures could produce cost savings due to the earlier dis- charge of patients in this group.
ACKNOWLEDGEMENTS
The authors wish to thank the patients and staff of the psychogeriatric unit at Royal Park Hospital for
their assistance. Christ Martin, Anne Hassett, Rick Yeatman, Judith Adams, Carmen Clemente, Chris- tine Mercuri and Lorelle Drew provided help with consensus diagnoses and outcome ratings. Yvonne Liddicoat typed the manuscript.
REFERENCES
American Psychiatric Association (1987) Diagnostic and Statistical Manual of Mental Disorders, 3rd edition, revised. American Psychiatric Association, Washing- ton, DC.
Baribeau-Braun, J. , Goldstein, S. and Braun, C . (1979). A multivariate study of psychogeriatric readmissions. J. Gerontol. 34(3), 351-357.
Cole, M. G. (1988) Evaluation of psychogeriatric ser- vices. Can. J. Psychiat. 33, 57-58.
Copeland, J. R. M., Kelleher, M. J., Kellett, J. M., Gourlay, A. J., Gurland, B. J., Fleiss, J. L. and Sharpe, L., (1976) A semi-structured clinical interview for the assessment of diagnosis and mental state in the elderly: The Geriatric Mental State Schedule. Psychol. Med. 6, 439449.
Draper, B. (1990) The effectiveness of services and treat- ment in psychogeriatrics. Aust. N.Z. J. Psychiat. 24, 238-251.
Folstein, M. F., Folstein, S. E. and McHugh P. R. (1975) ‘Mini mental state’; A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189-198.
Gilchrist, P. N., Rozenbilds, U. Y., Martin, E. and Con- nolly, H. (1985) A study of 100 consecutive admissions to a psychogeriatric unit. Med. J. Aust. 143, 236- 237.
Harrison, A. S. Kernutt, G. J. and Piperoglou, M. V. (1988) A survey of patients in a regional geriatric psy- chiatry inpatient unit. Aust. N.Z. J. Psychiat. 22, 41241 7.
Mei-Tal, V. and Meyers, B. (1985) Empirical study of an inpatient psychogeriatric unit: Diagnostic complexi- ties. Int. J. Psychiat. Med. 15, 91-109.
Moffatt, F., Mohr, C. and Ames, D. (1995) A group therapy programme for depressed and anxious elderly inpatients. Int. J. Geriatr. Psychiat., 10, 3740.
Pitt, B. (1982) Psychogeriatrics-an Introduction to the Psychiatry of Old Age, 2nd edn. Churchill Livingstone, Edinburgh.
Rockwood, K., Stolee, P. and Brahim, A. (1991) Out- comes of admission to a psychogeriatric service. Can. J. Psychiat. 36, 275-279.
Spar, J . E., Ford, C. V. and Liston, E. H. (1980) Hospital treatment of elderly neuropsychiatric patients 11. Sta- tistical profile of the first 122 patients in a new teaching ward. J. Am. Geriatr. Soc. 28, 539-543.