Embed Size (px)
Citation preview
1055
fails; that all the hopes of patient and relatives are directedtowards a favourable result; that if there is no improvementthere may be despair and anger and that this may be a goodreason for not returning for follow-up. Of course, this is alsono more than hypothesis, but nevertheless it would be interest-ing to know how many of the not-followed-up patients weredischarged by the hospital and how many failed to keep anappointment. It would also be interesting to know how manypatients were being followed-up in hospitals other than theone by which the operation was recommended or performed.London, N.W.l1.
z
J. F. SHAW.J. F. SHAW.
INDIAN CHILDHOOD CIRRHOSIS
AMARJIT SINGHS. S. JOLLY.
Medical College,Patiala, India.
SIR,-We were very much interested in the commentsof Dr. Robinson (April 15) on our article (March 18).Undoubtedly a number of hepatotoxic plants have been
described in India, but our point is that such plants are neverused by the patients. But in Jamaica extracts of such plantsare used for preparing herbal medicines or in the form of abeverage-bush-tea. There are no such customs in the partof India from where we described our cases. The characteristiclocalisation of the disease to a particular sect of Hindus, theinvolvement of a number of siblings in the family, and theoverwhelming preponderance of boys are all too significantto be disposed of as due to " custom rather than inheritance ".There is hardly any doubt that Indian childhood cirrhosis is agenetically determined disease. A...—- <-....
SCIENCE, GOVERNMENT, AND DEMOCRACY
B. BARNETT.
SiR.—The fundamental problem posed in your leaderof April 22 might have been headed more correctlyScientists, Government, and Democracy. What in fact
you discussed was the relationship of these three aspectsof society, aspects with fairly well-known characteristics.Your final lament for democracy is hardly justified by theparticular starting-point of the debate or the issues raised.Of the original debate it is enough to say that had the
democratic tradition of this country been less effective the" cult of the individual" would have led to even greaterconcentration of power in fewer hands with results that havebeen noted, to some disadvantage, in other countries. Men ofscience are still very much men, and the central issue is towhat extent, and how, political leaders should delegate authorityinto the hands not of " science " but scientists and professionalsand how these can be directed and controlled, bearing in mindShaw’s dictum that every profession is a conspiracy against thecommunity, and the older, no less apposite fable of the giantAntius who, when he was not in touch with mother earth, soonlost his strength.Since scientists, Government, and democracy are not
independent variables (particularly the latter two), it is oftenlikely that Governments will choose for their committees thosewho represent the orthodox line (if no more), and by the factof being on such a committee the conformists will tend toconform even more. But however technical the problem thatis presented, the decisions in its resolution pass far beyond theexperts so that the scientist is often thrown back on to hisprejudices which are known to be no less strong than those ofthe non-expert. (It is after all only in a narrow sector of avery broad front that expert advice is what it claims to be.)It is therefore only by increasing the democratic cover at theapparent risk of diluting quality and increasing committeesthat this fundamental risk can possibly be avoided.Leaving aside those instances where Governments set up
committees with no greater object than that of marking time,excluding those instances where committees are so linked withvested interests of personal commitments (not uncommon inother parts of the world), the basic problem remains howthe community through its Government can best tackle the
very complex problems of politics and social organisation,using experts but avoiding possible prejudices of experts.(How attractive it is to believe that the expert is above the
battle, and that we can shed our own responsibility leaving it tothe leaders.)The thermodynamics of democracy are capable of varied
explanations, but there would seem to be more danger in nodebate than of the debate continuing. There can be no inbuiltcontrol which will absolve the community of keeping itselfwell informed and taking responsibility for final decisions. Itis probably true that the more informed the debate the moreseriously will the Government-and committees-attend totheir business.The problems of the N.H.S. do not spring least from the
fact that there has been little attempt to shoulder the com-munity with their responsibility and have an enlightenedand informed democracy. For this the Government andpossibly the committees must bear their share of responsi-bility, though in the final analysis you may be right in layingthe bulk of the blame on the public; but this is the result not oftoo much but of too little democracy.
Moseley, B BBirmingham. B. BARNETT.
PSYCHIATRY FIFTEEN YEARS AHEAD
SIR,-Having experience both of the very large mentalhospitals of the present day and of a 228-bed psychiatricunit (with a full complement of
" long-stay " patients)I should like to comment on Dr. Pilkington’s letter ofApril 15.
Since there are very few similar units in this country, forthose who have experienced only the very small observationward or mammoth mental hospital there may seem no greaturgency in creating more small comprehensive units. It maybe felt that the larger institution is simply a smaller one writlarge, or multiplied. I feel very strongly that despite thehighest standards and the most conscientious and energeticefforts, the massive mental hospital must always have an anti-therapeutic effect.
In a community of 228 patients, plus staff, such as the oneI know well, the team treating the patients has a far easiertask in effecting, continuing, and promoting therapy, and inmaintaining regular trained oversight for all patients.Coordination and effective work with local-health-authoritystaff, social workers, psychologist, and so on, is very mucheasier and more continuous with a tightly knit team.The discharge into the community of patients with certain
residual symptoms really requires intensive and often quitefrequent follow-up, for which in the present state of medicaland auxiliary staffing of most mental hospitals it is almostessential that the local-authority network of staff should bebrought in. This is much more readily obtained with medium-sized units, situated in the communities they serve.The disadvantages of the mammoth mental hospital are, of
course, well known, but I think underrated by most peoplewho have not experienced a small uncluttered comprehensiveunit of about the size I have mentioned. In large institutionsit seems almost unavoidable that from time to time staff willbe shifted around from ward to ward, often coming into contactwith patients that they do not or barely know. This dis-
continuity of ties tends to produce insecurity in the patientsand does not on the whole seem to be a good thing. In a
compact unit such changes are not nearly so upsetting sincethe staff will know all the patients reasonably well in everysection of the smaller unit they are on.The enormous and forbidding mass of buildings and
people; the labyrinthine corridors ; and the many unknownfaces, are the reverse of helpful to mentally ill and isolated
patients; of course subdivision into small units, wards, andvillas, on a more human scale, helps to mitigate this; but thelarge institution is always in the background.
Again, some of the most valuable staff of all departments andcategories are looking after and treating other staff; instead of
1056
patients. This appears an inevitable process with growth insize to really large proportions. In a unit of reasonable sizecommunications to all levels are much easier.
Lastly, let us not forget why these buildings were placedwhere they are and built as they are. The scale and site of thebuildings stand for, and must to some extent (whether we likeit or not) help to perpetuate, an attitude of mind. I writebecause I feel that Dr. Pilkington’s admirable letter, whilehaving the positive merit of encouraging the continuingimprovement of large mental hospitals, might tend to takethe steam out of the really urgent need for much smaller andmore human-sized units in the communities they serve.
H. JACOBS.Severalls Hospital,
Colchester.
1. Kapila, C. C., Kaul, S., Kapur, S. C., Kalayanam, T. S., Banerjee, D.Brit. med. J. 1958, ii, 1311.
2. Galagan, D. J., Lamson, G. G. J. publ. Hlth Rep., Wash. 1953, 68, 497.3. Medical-Dental Adhoc Committee on Evaluation of Fluoridation Report.
New York City, 1959.
EXTRAPULMONARY INFLUENZAL INFECTION
S. KAUL.Tata Main Hospital,Jamshedpur 1, India.
SIR,-I was interested to see from your annotation
(March 4) that visceral invasion by the influenza virus isbeing increasingly recognised.You did not refer to the 30 cases of encephalitis we reported
from India.l These were all associated with the influenza
epidemic of 1957. Several cases occurred almost simultaneouslyin small groups. Jaundice, presumably the result of liverinvolvement, was present in a third. The clinical course wascharacteristic. As against the negligible overall mortality in the1957 epidemic of Asian influenza in India, the mortality in thisgroup was very high: 17 of the 30 patients died. At necropsy,performed in all 17, typical pulmonary lesions of influenzawere invariably seen. The virus was isolated from the lungs in5 cases, and from the brain in 1.We were unable to find any reference to similar cases in the
literature. Symptoms and signs of this type may not be
uncommon, but may easily be missed because of pressure ofwork in epidemics.
SKELETAL FLUOROSIS
R. A. HOLMAN.Institute of Pathology,
Royal Infirmary,Cardiff.
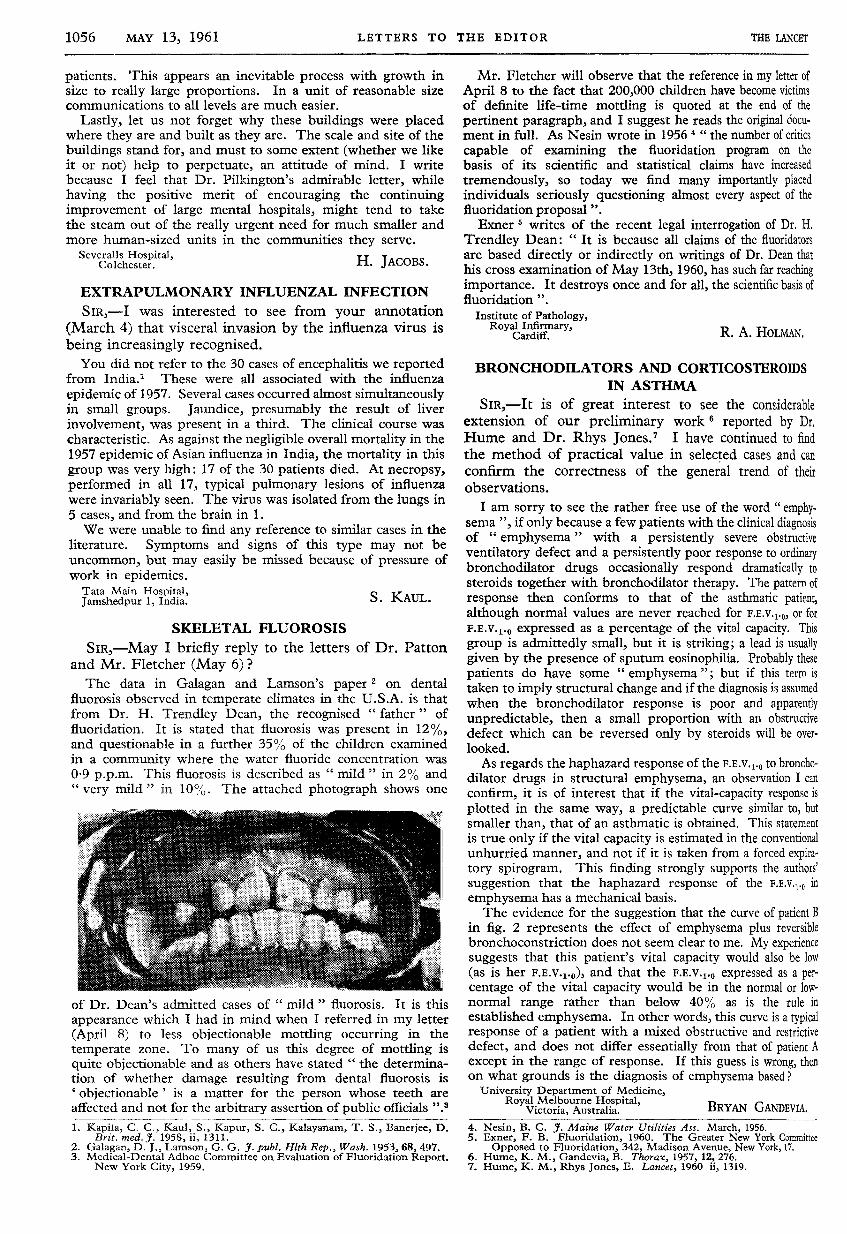
SIR,-May I briefly reply to the letters of Dr. Pattonand Mr. Fletcher (May 6) ?The data in Galagan and Lamson’s paper 2 on dental
fluorosis observed in temperate climates in the U.S.A. is thatfrom Dr. H. Trendley Dean, the recognised " father " offluoridation. It is stated that fluorosis was present in 12%,and questionable in a further 35% of the children examinedin a community where the water fluoride concentration was0-9 p.p.m. This fluorosis is described as " mild in 2% and"very mild " in 10%. The attached photograph shows one
of Dr. Dean’s admitted cases of " mild " fluorosis. It is this
appearance which I had in mind when I referred in my letter
(April 8) to less objectionable mottling occurring in the
temperate zone. To many of us this degree of mottling is
quite objectionable and as others have stated " the determina-tion of whether damage resulting from dental fluorosis is’ objectionable ’ is a matter for the person whose teeth areaffected and not for the arbitrary assertion of public officials ".3
Mr. Fletcher will observe that the reference in my letter ofApril 8 to the fact that 200,000 children have become victimsof definite life-time mottling is quoted at the end of the
pertinent paragraph, and I suggest he reads the original docu-ment in full. As Nesin wrote in 1956 4 " the number of critics
capable of examining the fluoridation program on thebasis of its scientific and statistical claims have increased
tremendously, so today we find many importantly placedindividuals seriously questioning almost every aspect of thefluoridation proposal".Exner 5 writes of the recent legal interrogation of Dr. H.
Trendley Dean: " It is because all claims of the fluoridatorsare based directly or indirectly on writings of Dr. Dean thathis cross examination of May 13th, 1960, has such far reachingimportance. It destroys once and for all, the scientific basis offluoridation ".
4. Nesin, B. C. J. Maine Water Utilities Ass. March, 1956.5. Exner, F. B. Fluoridation, 1960. The Greater New York Committee
Opposed to Fluoridation, 342, Madison Avenue, New York, 17.6. Hume, K. M., Gandevia, B. Thorax, 1957, 12, 276.7. Hume, K. M., Rhys Jones, E. Lancet, 1960 ii, 1319.
BRONCHODILATORS AND CORTICOSTEROIDSIN ASTHMA
BRYAN GANDEVIA.University Department of Medicine,
Royal Melbourne Hospital,Victoria, Australia.
SIR,-It is of great interest to see the considerableextension of our preliminary work reported by Dr,Hume and Dr. Rhys Jones.’ I have continued to findthe method of practical value in selected cases and canconfirm the correctness of the general trend of theirobservations.
I am sorry to see the rather free use of the word " emphy-sema ", if only because a few patients with the clinical diagnosisof " emphysema " with a persistently severe obstructiveventilatory defect and a persistently poor response to ordinarybronchodilator drugs occasionally respond dramatically to
steroids together with bronchodilator therapy. The pattern ofresponse then conforms to that of the asthmatic patient,although normal values are never reached for F.E.v.i.,, or forF.E.V.l.O expressed as a percentage of the vital capacity. This
group is admittedly small, but it is striking; a lead is usuallygiven by the presence of sputum eosinophilia. Probably thesepatients do have some " emphysema "; but if this term istaken to imply structural change and if the diagnosis is assumedwhen the bronchodilator response is poor and apparentlyunpredictable, then a small proportion with an obstructivedefect which can be reversed only by steroids will be over-looked.
As regards the haphazard response of the F.E,V’l’O to broncho-dilator drugs in structural emphysema, an observation I canconfirm, it is of interest that if the vital-capacity response isplotted in the same way, a predictable curve similar to, butsmaller than, that of an asthmatic is obtained. This statementis true only if the vital capacity is estimated in the conventionalunhurried manner, and not if it is taken from a forced expira-tory spirogram. This finding strongly supports the authors’suggestion that the haphazard response of the F.E.V.l.O in
emphysema has a mechanical basis.The evidence for the suggestion that the curve of patient B
in fig. 2 represents the effect of emphysema plus reversiblebronchoconstriction does not seem clear to me. My experiencesuggests that this patient’s vital capacity would also be low(as is her F.E.v.i.;,), and that the F.E.v.i.o expressed as a per-centage of the vital capacity would be in the normal or low-normal range rather than below 40% as is the rule inestablished emphysema. In other words, this curve is a typicalresponse of a patient with a mixed obstructive and restrictivedefect, and does not differ essentially from that of patient Aexcept in the range of response. If this guess is wrong, thenon what grounds is the diagnosis of emphysema based ?