Embed Size (px)
Citation preview

Psychological and Behavioral Psychological and Behavioral Responses to DisastersResponses to Disasters
Steve Bunney, MD Steve Bunney, MDDepartment of PsychiatryDepartment of PsychiatryYale School of MedicineYale School of Medicine


9-11-019-11-01
• Unique Disaster• First disaster in history
where in the aftermathpsychological repair wasmore important thanrepairing bodies orburying the dead
• Part of event waswatched live by millionsof people

Personal Experience Post 9-11Personal Experience Post 9-11
Day 1– Call from Walter Reed– Activation of Emergency Response Plan
Day 2– Call from Service Union
Day 7– Call from business CEO
Day 21– Call from airline unions
Day 30– Call from insurance company

PHASES of IMPACT and PHASES of IMPACT and RECOVERYRECOVERY
I. EMERGENCY/IMPACTSHOCK – first hours/daysHEROIC – first days/weeksII. EARLY POST-IMPACT
HONEYMOON – 1-3 Months DISILLUSIONMENT – 3-6 months
III. RESTORATION vs. BREAKDOWNRESTABILIZATION – 6-9 months
RECOVERY – 9-12 monthsPREPAREDNESS – 12+ months

What is Psychological What is Psychological Trauma?Trauma?
Overwhelming, unanticipated danger that cannot be mediated/processed in way that leads to fight or flight
Immobilization of normal methods for decreasing danger and anxiety
Neurophysiological dysregulation that compromises affective, cognitive and behavioral responses to stimuli

Psychological ShockPsychological Shock
Objective Exposure Exposure to threat of imminent/actual death Witnessing bodies and body parts Extreme exposure to fire, dust, exhaustion
Subjective Survival Responses Terror: fear, helplessness, impulsivity Horror: disbelief, revulsion, guilt, shame, rage Numbing: derealization, depersonalization, fugue,
amnesia.

Stress vs TraumaStress vs Trauma
Dealing with Problems
Heart Pounding
Rapid Breathing
Muscles Tense Up
Fight or Flight
Feel Excited or Worried
Seeing/Thinking Clearly
Acting Rapidly
Feel in Control
Trying to Survive
Heart Feels Like Bursting
Gasping, Feeling Smothered
Muscles Feel Like Exploding
Just Try to Get Through It
Feel Terrified of Panicked
Confused, Mentally Shut Down
Automatic Reflexes or Freezing
Feel Helpless or Out of Control

Neurobiology of Severe StressNeurobiology of Severe Stress
Responses are complex– Biological defenses against a threat– Mechanisms related to learning and adaptation– Responses to social cues– Reactions to loss and separation– Effects of cognitive disarray and chaotic
experience

Neurobiology of Severe StressNeurobiology of Severe Stress(cont.)(cont.)
Thalamus registers whether sensory input is familiar or novel and a threat or not
Threat triggers brain alarm system (amygdla) and release of corticosteroids and norepinephrine
Fight-flight responses (autonomic nervous system, sympathetic branch)
Peripheral resource conservation (autonomic nervous system, parasympathetic branch)

Neurobiology of Severe Stress Neurobiology of Severe Stress (cont.)(cont.)
Alarm: insula and amygdala coordinate body’s mobilization in response to threat
Attention: norepinepherine release by locus ceruleus (brain stem area) promotes focused attention
Reactivity: corticosteroids promote instinctual survival rather than goal-directed reflection
Information Processing: Hippocampus inhibited in spatial orientation and categorization of sensory inputs
Executive Decision Making: prefrontal cortex receives confusing/chaotic alarm signals and is down-regulated

Neurobiology of Severe StressNeurobiology of Severe Stress(cont.)(cont.)
Delayed responses Cascade of neuronal and genomic events including:
Increased synthesis of cortiotropin releasing hormone (CRH) and cortisol related receptors in areas of brain not directly in hormonal stress response
Increased protein synthesis in memory areas provides mechanism for two types of long term memory of stressful events :
Hippocampus Explicit - verbalizable and recallable
Amygdala Implicit - unconscious changes in habit and conditioned
responses (e.g. fear response when exposed to cues relevant to traumatic event

Neurobiology of Severe StressNeurobiology of Severe Stress(cont.)(cont.)
Summary– The early aftermath of a disaster is a critical time of
increased neuronal plasticity.– The perceived threat triggers intense bodily reactions
that shape the mental traces of adverse events.– Physiological and psychological factors can either
concur to cause chronic stress disorders or adaptation and resilience.
– Early interventions may reduce the risk of chronicity

Event Factors That Influence Event Factors That Influence Psychological ResponsesPsychological Responses
How directly events affect their lives:Physical proximity to event
Emotional proximity to event (threat to child, parent versus stranger)
Secondary effects-of primary importance (does event cause disruption in on-going life)

Individual Factors That Influence Individual Factors That Influence
Psychological ResponsePsychological Response Genetic vulnerabilities and capacities Prior history (i.e. consistent stress or one or
more stressful life experience/s) History of psychiatric disorder Familial health or psychopathology Family and social support Age and developmental level Other: Female, divorced or widowed, lower
IQ, lower income, lower education level

ChildrenChildren
Responses and TreatmentResponses and Treatment

Role of AdultsRole of Adults
For all children, especially younger children, experience and especially upsetting experience is mediated by adults.
Adults emotional response often as important as the actual event

Children’s Typical Initial ResponsesChildren’s Typical Initial ResponsesNormal reactions to abnormal situationsNormal reactions to abnormal situations
Emotional and SomaticEmotional and Somatic Sleep disturbance (nightmares etc.) Decreased or increased appetite Sad or anxious mood (withdrawn or more quiet) Irritable, fussy or argumentative Loss of recently achieved milestones Clingy or wanting to be close to parents Difficulty paying attention Daydreaming or easily distractible

ToddlersRely on ParentsRegression
PreschoolersHighly ImaginativeConcerned About Safety
School AgeSocial DifficultiesConcerned About Right/Wrong (Revenge)
AdolescentsStruggling With IndependenceConflict With Authority FiguresMinimize or ExaggerateIncreased Risk TakingSubstance Use
Older Adolescents & Young AdultsConcerns About FutureSubstance Use
Spectrum of Developmentally Determined Responses

Implications of Neurobiological Implications of Neurobiological Development for TreatmentDevelopment for Treatment
Hippocampus not fully functional until 4-5 years old
Prefrontal cortex not fully functional until around age 10

Treatment and InterventionTreatment and InterventionIn the immediate aftermathIn the immediate aftermath
Reunite children with important adults/ family members
Interventions for children include interventions for caretakers. If adults can not attend to children, outcome will be poor
Adults tend to underestimate impact on children or alternatively displace own feelings onto their children

Treatment and InterventionTreatment and InterventionIn the immediate aftermath (cont.)In the immediate aftermath (cont.)
Criteria for Referral
Presence of DissociationDecreased motor functionBlunted affectAbsence of speech
Decreased responsiveness to external stimuli Presence of Hyperarousal (heart rate and often
respiration increased) Avoidance/Withdrawal Symptoms Extreme Emotional Upset Symptoms of Acute Stress Disorder

Acute Stress DisorderAcute Stress Disorder
3+ of 5 Dissociative Sx (Detached, Dazed, Derealization, Depersonalization, Amnesia)
Recurrent Unwanted Memories Awake/Asleep or Biopsychological Distress Due to Reminders
Avoidance of Internal/External Reminders Hyperarousal (Anxious, Irritable, Insomnia, Poor
Concentration, Hypervigilant, Reactive) Significant psychosocial/healthcare impairment Duration 2-30 days

Treatment Issues 4-6 Months After Treatment Issues 4-6 Months After DisasterDisaster
Criteria For Referral
Extreme emotional upset Sleep disturbances Somatization Hyper-vigilance Severe distractibility Regressive behavior Blunted emotions Regression in social functioning and play Oppositional and aggressive behaviors
Classic PTSD not common in children but incidence increases with age (especially adolescents)

AdultsAdults
Responses and Treatment Responses and Treatment

Common FantasiesCommon Fantasies
to alter the precipitating event to interrupt the traumatic action to reverse the lethal or injurious consequences to gain safe retaliation (fantasies of revenge) to be able to anticipate or prevent future traumas to bring back lost loved ones, friends, places,
activities, or states of mind (trust) or body (peace)

Common Stress Reactions To DisasterCommon Stress Reactions To Disaster
Emotional EffectsShock
Anger
Despair
Emotional numbing
Terror
Guilt
Irritability
Helplessness
Loss of derived pleasure from regular activities
Dissociation (e.g., perceptual experience seems “dreamlike, “tunnel vision,” “spacey,” or on “automatic pilot”)
Physical EffectsFatigue
Insomnia
Sleep disturbance
Hyperarousal
Somatic complaints
Impaired immune response
Headaches
Gastrointestinal problems
Decreased appetite
Decreased libido
Startle response
Cognitive EffectsImpaired concentration
Impaired decision-making ability
Memory impairment
Disbelief
Confusion
Distortion
Decreased self-esteem
Decreased self-efficacy
Self-blame
Intrusive thoughts and memories
Worry
Interpersonal EffectsAlienation
Social withdrawal
Increased conflict within relationships
Vocational impairment
School impairment
Young, BH, et. al. Disaster Mental Health Services: A Guidebook For Clinicians and Administrators. The National Center for Post-Traumatic Stress Disorder, Department of Veterans Affairs

Acute Stress DisorderAcute Stress Disorder
3+ of 5 Dissociative Sx (Detached, Dazed, Derealization, Depersonalization, Amnesia)
Recurrent Unwanted Memories Awake/Asleep or Biopsychological Distress Due to Reminders
Avoidance of Internal/External Reminders Hyperarousal (Anxious, Irritable, Insomnia, Poor
Concentration, Hypervigilant, Reactive) Significant psychosocial/healthcare impairment Duration 2-30 days post traumatic event

Treatment and InterventionTreatment and InterventionIn the immediate aftermathIn the immediate aftermath
There is no one approach to treatment that current research singles out as effective
One time intervention models have been shown to be ineffective
Critical Incident Stress Management (CISM) has no proven effectiveness in prevention of late onset psychological disorders (e.g. PTSD)

Treatment and InterventionTreatment and InterventionIn the immediate aftermathIn the immediate aftermath
(cont.)(cont.)
Psychotherapeutic interventions in the the absence of structure and organization will not be effective.
Provide real and concrete information about event, explain actions of authorities
Provide basic necessities

Key Principles of Immediate Key Principles of Immediate InterventionIntervention
Engagement: Empathic, non directive inquiry( not what happened?, but, how are you feeling?, delving into detail can retraumatize)
Manage Overwhelming Feelings: agitation, pressured speech, uncontrollable crying, out of touch with reality Request person to look at you and listen to what
you are telling them Hold their attention, talk about positive or non-
emotional topics Ask them to describe the place they’re in and say
where they are Support: Confer control in therapeutic
contact

Key Principles of Immediate Key Principles of Immediate InterventionIntervention (cont.) (cont.)
Affect: Identify, label and link to ideation and somatic experience (noting differences from beginning to end of contact and with reports about pre-morbid functioning)
Cognition: Assess quality and nature of thought processes and link to affective impact of event and associated ideas

Key Principles of Immediate Key Principles of Immediate Intervention Intervention (cont.)(cont.)
Psycho-education: Explain the normal post-traumatic response (what to expect, what is normal and when additional support/intervention is needed)
Follow-up: Arrange for series of contacts to assess symptoms and adaptive functioning

4-6 Months After Disaster4-6 Months After Disaster
Persistent physical, mental, relational, and work problems are taking a toll
Helping professionals (behavioral health, medical/nursing, human services, clergy) and natural helpers are frayed and feeling the burden of answering the unanswerable
Delayed psychiatric sequel are emerging (unresolved bereavement, depression, PTSD, anxiety disorders, addictions)

Target Groups At Risk for Persistent Target Groups At Risk for Persistent Post-Traumatic SequelaePost-Traumatic Sequelae
On-Site Survivors
Bereaved Families/Primary Relationships
On-Site Rescue/Recovery Workers
Terror: Exposure to threat of imminent/actual death Horror: Witnessing death, destruction, terror & shockPhysical Insult: injury, exhaustion, toxic exposureTraumatic Reactivation (past & subsequent crisis work)Separation/Detachment from Family and Community

Target Groups At Risk for Persistent Target Groups At Risk for Persistent Post-Traumatic SequelaePost-Traumatic Sequelae
Helpers Caring for Survivors, the Bereaved, Workers (e.g., Behavioral Health, EAP, Health Care, Clergy)
Family/Community Members Living and Working with Survivors, the Bereaved & Rescue Workers
Vicarious Shock: Exposure to terror, helplessness, grief Uncertainty: Wanting to help but not knowing when/howPhysical/Workload Strain: Carrying the added load while
others are focused on coping with impairment or recoveryLoss: Disconnection from traumatized significant othersTraumatic Reactivation: Unresolved direct/vicarious trauma

Target Groups At Risk for Target Groups At Risk for Persistent Post-Traumatic SequelaePersistent Post-Traumatic Sequelae
People in Recovery from Behavioral Health Disorders
Vulnerable Groups
(e.g., children, elders, disenfranchised)

Treatment Issues 4-6 Months Treatment Issues 4-6 Months Later:Later:
Intrusive Re-experiencing: Overwhelming memories Numbing: Feeling stunned, empty, dead inside Hypervigilance: Prolonged Survival Alarm State Dissociation: Disconnection from Alarm Awareness Affect Dysregulation: Overwhelming emotions Somatization: Bodily exhaustion and breakdown Alienation: Loss of sustaining perceptions of future &
attachments Defeat: Loss of personal/spiritual trust & goals

Post Traumatic Disorders: Not Post Traumatic Disorders: Not Automatic & More than PTSDAutomatic & More than PTSD
Most adults and children recover without a lasting post-traumatic psychiatric disorder
10-20% develop depression or PTSD (often both) Alcohol/substance use disorders not prevalent Subclinical depression or substance use common

Posttraumatic Stress Disorder Posttraumatic Stress Disorder (PTSD)(PTSD)
Recurrent Unwanted Memories Awake/Asleep or Biopsychological Distress to Reminders
Avoidance of Internal/External Reminders, Emotional Numbing, Social Detachment, Amnesia
Hyperarousal (Anxious, Irritable, Insomnia, Poor Concentration, Hypervigilant, Reactive)
Significant psychosocial/healthcare impairment Duration 30+ days (may be delayed or chronic)

Issues to be Assessed in the Issues to be Assessed in the Treatment of Traumatic Sequelae of Treatment of Traumatic Sequelae of
DisasterDisaster
Criteria for Referral
Presence of depression, PTSD, panic attacks, disabling grief of six months duration and no improvement over time
Worsening of prior psychological problems Memories of prior traumatic experiences are now
causing distress Presence of sustained psychological or physical
stress Poor or absent social supports

Issues to be Assessed in the Issues to be Assessed in the Treatment of Traumatic Sequelae of Treatment of Traumatic Sequelae of
Disaster (cont.)Disaster (cont.)
Criteria for Immediate Referral
Suicidal thoughts with a plan and/or means Excessive substance use causing person or
others to be placed at risk Poor functioning to the point that individual’s
(or dependent’s) safety/welfare is in danger

Issues to be Assessed in the Issues to be Assessed in the Treatment of Traumatic Sequelae of Treatment of Traumatic Sequelae of
Disaster (cont.)Disaster (cont.)
Major Issues in Making Referrals Stigma
Explain feelings and behavior (note: not called symptoms) are normal under these circumstances and so is getting some help to deal with them
Take the “shrink” out of counseling Explain you are sending them for information and
potential support Explain they will get help in problem solving and
coping Tell them what you are doing to cope

A State Mental Health CareSystem Response to 9-11

A Statewide Network of Local Behavioral A Statewide Network of Local Behavioral Health Teams: Helping Communities with the Health Teams: Helping Communities with the
Stress of Disasters or Public Health CrisesStress of Disasters or Public Health CrisesCenter for Trauma Response, Recovery, and Preparedness
University of Connecticut Health Center
Julian D. Ford, Ph.D.CT Department of Mental Health and Addiction Services
Arthur C. Evans, Ph.D.James Siemianowski, MSW
Wayne Dailey, PhDCenter for Trauma Response, Recovery and PreparednessYale University School of Medicine, Dept. of Psychiatry
Steven Berkowitz, MDSteve Bunney, M.D
Steven Marans, PhD.Steve Southwick, MD
CT Department of Children and FamiliesThomas Gilman, MSW

What have we done since 9/11?What have we done since 9/11?
A Statewide Behavioral Health A Statewide Behavioral Health Preparedness PlanPreparedness Plan
800+ professionals trained to serve as volunteers on local behavioral health crisis response teams
150+ prevention providers and natural helpers trained as resources for community preparedness
50+ behavioral health consumer advocates trained to help communities support people in recovery
Local volunteer teams receiving ongoing technical assistance to prepare them for disaster response
Planning for mobilization and activation of these teams in the event of a major disaster
Behavioral health resources disseminated via www.ctrp.org and www.clearinghouse.org

Linking Behavioral Health to the OEM & DPH Linking Behavioral Health to the OEM & DPH Disaster/Crisis Response SystemDisaster/Crisis Response System
Statewide, Local
Incident Command
SystemMunicipal
officials, public health, fire,
police, emergency
management, EMS, health
care, schools, social service
agencies
Statewide, Regional,
Local Behavioral
Health System BH Agencies +
Professionals+ Natural Helpers
Local Behavioral
Health Response
Teams
OEM - Office of Emergency ManagementDPH - Department of Public HealthBH - Behavioral Health

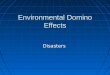
How does the state behavioral health How does the state behavioral health system support local crisis responses?system support local crisis responses?
Gov/OEM/DPH
DMHAS/DCF
CTRP
T T T TTTT T T T
Local teams comprised of specially trained state staff, Private Non-Profit and private volunteers, work closely with municipal and
community leaders, public health department directors, EMS, clergy, school officials, employers
RC = Regional Behavioral Health
Coordinators
DMHAS = Dept of Mental Health &
Addiction Svs
RC RCRC RC RC
Gov = Governor
OEM = Office of Emergency Mgmt
DPH = Dept of Public Health
CTRP = Ctr. for Trauma Response/Recovery & Preparedness
DCF = Dept of Children & Families

Taken in Part from aTaken in Part from aCenter for Trauma Response, Recovery Center for Trauma Response, Recovery and Preparedness (CTRP) Presentationand Preparedness (CTRP) Presentation
University of Connecticut School of Medicine Julian D. Ford, PhD
Yale University School of Medicine Steven Berkowitz, MD
Benjamin S. Bunney, MD Steven Marans, PhD Steve Southwick, MD
CT Department of Mental Health and Addiction Services Arthur C. Evans, PhD Wayne Dailey, PhD
James Siemianowski, MSW
CT Department of Children and Families Thomas Gilman, MSW