Embed Size (px)
Citation preview
This article was downloaded by: [McMaster University]On: 16 October 2014, At: 14:32Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH,UK
Clinical GerontologistPublication details, including instructions forauthors and subscription information:http://www.tandfonline.com/loi/wcli20
Psychological Resilience toSuicide Ideation Among OlderAdultsMarnin J. Heisel PhD a b & Gordon L. Flett PhD ca Departments of Psychiatry and Epidemiology andBiostatistics , The University of Western Ontario ,London, Ontario, Canadab Departments of Psychiatry , University ofRochester Medical Center , Rochester, New York,USAc Department of Psychology , York University ,Toronto, Ontario, CanadaPublished online: 11 Oct 2008.
To cite this article: Marnin J. Heisel PhD & Gordon L. Flett PhD (2008) PsychologicalResilience to Suicide Ideation Among Older Adults, Clinical Gerontologist, 31:4, 51-70,DOI: 10.1080/07317110801947177
To link to this article: http://dx.doi.org/10.1080/07317110801947177
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all theinformation (the “Content”) contained in the publications on our platform.However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness,or suitability for any purpose of the Content. Any opinions and viewsexpressed in this publication are the opinions and views of the authors, and

are not the views of or endorsed by Taylor & Francis. The accuracy of theContent should not be relied upon and should be independently verified withprimary sources of information. Taylor and Francis shall not be liable for anylosses, actions, claims, proceedings, demands, costs, expenses, damages,and other liabilities whatsoever or howsoever caused arising directly orindirectly in connection with, in relation to or arising out of the use of theContent.
This article may be used for research, teaching, and private study purposes.Any substantial or systematic reproduction, redistribution, reselling, loan,sub-licensing, systematic supply, or distribution in any form to anyone isexpressly forbidden. Terms & Conditions of access and use can be found athttp://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014

Clinical Gerontologist, Vol. 31(4) 2008Available online at http://cg.haworthpress.com
© 2008 by The Haworth Press. All rights reserved.doi:10.1080/07317110801947177 51
WCLI0731-71151545-2301Clinical Gerontologist, Vol. 31, No. 4, April 2008: pp. 1–29Clinical Gerontologist
Psychological Resilience to Suicide Ideation Among Older Adults
Marnin J. Heisel and Gordon L. FlettClinical Gerontologist Marnin J. Heisel, PhDGordon L. Flett, PhD
Marnin J. Heisel is affiliated with the Departments of Psychiatry and Epidemiologyand Biostatistics, Schulich School of Medicine and Dentistry, The University ofWestern Ontario; Lawson Health Research Institute London, Ontario, Canada; andthe Center for the Study and Prevention of Suicide, Department of Psychiatry,University of Rochester Medical Center, Rochester, New York.
Gordon L. Flett is affiliated with the Department of Psychology, York UniversityToronto, Ontario, Canada.
This study was part of Dr. Heisel’s doctoral dissertation conducted at YorkUniversity under Dr. Flett’s supervision. The authors acknowledge the assistanceof Drs. Kenneth Shulman, Robert van Reekum, Marcus Feak, Gary Challis,Howard Dombrower, Corinne Fischer, Alastair Flint, Rosemary Meier, Ivan Silver,David Streiner, Gary Teare, Fran Kleiner, M.S.W., and Earl Smith, M.S.W. inconducting this research, and thank Drs. Paul Kohn, Clarry Lay, Toyomasa Fusé,Joseph Levy, and Michael Kral for their helpful input. Thanks also are extendedto the study participants and to the Research Ethics Boards and staff of therecruitment sites (see Heisel & Flett, 2006). This research was funded by a SocialSciences and Humanities Research Council of Canada (SSHRC) DoctoralFellowship to Dr. Heisel, and by a grant from the SSHRC awarded to Dr. Flett.Dr. Heisel holds a Young Investigator award from the American Foundation forSuicide Prevention (AFSP), a Canadian Institutes for Health Research (CIHR)New Investigator Award through the Institute of Aging and Institute of Genderand Health, and research funding from The University of Western Ontario’sDepartment of Psychiatry and from the Lawson Health Research Institute.Dr. Flett holds a Canada Research Chair in Personality and Health.
Address correspondence to: Dr. Marnin J. Heisel, Department of Psychiatry,The University of Western Ontario, London Health Sciences Centre, 375 SouthStreet, Room #5054, London, Ontario, N6A-4G5, Canada (E-mail: [email protected]).
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014

52 CLINICAL GERONTOLOGIST
ABSTRACT. We investigated associations between suicide ideation and aset of potential risk and resiliency factors in a heterogeneous sample of 107older adults (mean age = 81.5 years, SD = 7.7 years; range, 67 to 98 years;76% female) recruited in community, residential, and healthcare settings.Participants completed the Geriatric Suicide Ideation Scale (GSIS; Heisel &Flett, 2006) and measures of depression, perceived physical health problems,domains of psychological well-being, perceived meaning in life, and indicesof social network and of religious affiliation and observance. The main find-ings indicated that suicide ideation was associated positively with depressionand with number of self-reported physical health problems and negativelywith domains of psychological well-being including positive relations withothers and self-acceptance, and with perceived meaning in life. Hierarchicalmultiple regression analyses indicated that the resiliency factors in general,and perceived meaning in life in particular, explained significant added vari-ance in suicide ideation over and above measures of mental and physicalhealth problems. These findings suggest potential value in attending to bothsuicide risk and resiliency when assessing late-life suicide ideation and whendeveloping interventions for older adults at risk for suicide.
KEYWORDS. Suicide ideation, resilience, meaning in life, depression,psychological well-being
INTRODUCTION
The North American older adult population is growing rapidly. Theaging of the baby-boom cohort will lead to a dramatic increase in the 65-pluspopulation over the next 50+ years, raising capacity concerns in thehealthcare system. Older adults have high rates of suicide, employ violentmeans of self-harm, and are more likely than younger adults to succumbto their injuries (Heisel, 2006). Suicide prevention strategies must be sen-sitive to late-life suicide risk and resilience. We investigated associationsbetween suicide ideation and potential risk and resiliency factors in a het-erogeneous sample of adults 65 years and older, using the Geriatric Sui-cide Ideation Scale (GSIS; Heisel & Flett, 2006), a multidimensionalinstrument assessing late-life suicide ideation.
Although many older adults enjoy good physical and mental health, asubstantial proportion do not, necessitating increased understanding ofmental health promotion and interventions to reduce negative mentalhealth outcomes. Late-life suicide prevention research has focused prima-rily on assessing risk, with far less research on resiliency factors (Heisel,
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014
Marnin J. Heisel and Gordon L. Flett 53
2006). Interdisciplinary guidelines highlight the need for exploration andenhancement of resiliency and assessment of suicide risk factors in clini-cal practice with older adults (Canadian Coalition for Seniors’ MentalHealth, 2006). Shneidman (1996) posited that intolerable psychologicalpain or “psychache” drives the risk for suicide. Research findings haveshown robust associations between late-life suicide ideation and indicesof intense psychological pain, including depression, poor social integra-tion, and experienced or anticipated health problems (Bartels et al., 2002;Heisel & Flett, 2006; Vanderhorst & McLaren, 2005). Late-life depres-sion is a common problem conferring risk for morbidity and for mortalityby all causes including suicide (Blazer, Hybels, & Pieper, 2001); how-ever, most depressed older adults do not die by suicide, suggesting thatsuicidal thoughts and behavior are instigated by the presence of risk andan absence of resilience.
Findings from case-controlled studies of suicidal deaths among olderadults suggest that positive health behaviors, presence of interests andhobbies, and involvement in social groups, organizations, and religiousactivities may lessen the risk for suicide (Juurlink et al., 2004; Rubenowitz,Waern, Wilhelmson, & Allebeck, 2001; Turvey et al., 2002). Durkheim(1966) reported an association between suicide and degree of religiouscommitment. Research has since indicated inverse associations betweenreligious affiliation and observance with suicidal ideation and behavior(Nelson, 1977; Stack & Lester, 1991). Although the capacity for spiritual-ity may increase with age (Braam et al., 2006; Nygren et al., 2005), not allolder adults find faith through religion, necessitating investigation ofadditional resiliency factors. We thus examined religious affiliation andobservance together with measures of psychological well-being, theoreti-cally consistent with research on successful aging, as potential resiliencyfactors to suicide ideation.
Erikson (1963) theorized that successful aging partly involves resolvingthe psychosocial challenge of striving for ego integrity versus despair.Fisher (1995) posited that successful aging involves interactions with oth-ers, a sense of purpose, self-acceptance, personal growth, and autonomy.Ryff’s (1989) review of the literature on psychological adjustment andsuccessful aging suggested a similar model of psychological well-being(PWB) comprising six domains: purpose in life (PIL), environmentalmastery, self-acceptance, positive relations with others, personal growth,and autonomy. Ryff’s six-factor model of PWB is well grounded in theory,and long- and short-forms of her multidimensional PWB measure havedemonstrated strong psychometric properties (Kafka & Kozma, 2002;
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014

54 CLINICAL GERONTOLOGIST
Ryff & Keyes, 1995). Researchers reporting on the 18-item PWB mea-sure administered to nearly 5000 older adults in the Canadian Study ofHealth and Aging confirmed the validity of the six-factor model of PWB,yet reported extremely low levels of internal consistency for PersonalGrowth, Autonomy, and Purpose In Life subscales (Clarke, Marshall,Ryff, & Wheaton, 2001). In the present study, we employed the PWBmeasure to test the hypothesis that several well-being variables are nega-tively associated with suicide ideation among older adults.
Research findings have documented a resiliency to suicidal despairamong older adults reporting reasons for living (Hirsch et al., 2006;Miller, Segal, & Coolidge, 2001) and perceiving meaning or purpose inlife (Heisel & Flett, 2007; Moore, 1997). Frankl (1985) provided an earlydescription of the salutary role of meaning in life (MIL) in preventing despairand suicide among prisoners of Nazi concentration camps. He theorizedthat the pursuit of MIL is a central human endeavor involving one’sresponses to objective challenges in everyday life experiences and thatrecognition of MIL might obviate pathological responses to negative situ-ations and reduce suicide risk (Frankl, 1985, 1988). Frankl posited thatmeaning can be discovered in creative pursuits, in life experiences, and inattitudes adopted toward both successes and challenges in life, and furtherproposed the existence of ultimate meaning in life referring to the percep-tion that one’s life serves a greater transcendent purpose. Older adultsreport more perceived MIL than do younger adults (Van Ranst & Marcoen,1997). MIL is significantly associated with adaptive psychological factors,including purpose in life, sense of coherence, resiliency, creativity, optimism,self-esteem, chronic pain management, life satisfaction, perceived socialsupport, and self-transcendence (Braam et al., 2006; Hickson & Housley,1997; Krause, 2003; Nygren et al., 2005). Perceived meaninglessness is,in turn, associated with stress, depression, and suicide ideation (Krause,2004; Petrie & Brook, 1992; Reker, 1997).
We have previously investigated risk and resiliency to suicide ideationin clinical adult and heterogeneous older adult samples, and reportedpositive associations between suicide ideation and risk factors, includingdepression and hopelessness, and negative associations between suicideideation and resiliency factors, including life satisfaction and meaning orpurpose in life (Heisel & Flett, 2004, 2007). Hierarchical multipleregression analyses indicated that the resiliency factors explained signif-icant variance in suicide ideation above and beyond the risk factorsalone, demonstrating value in attending to resiliency in addition tosuicide risk.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014
Marnin J. Heisel and Gordon L. Flett 55
In the present study, we sought to extend our previous research on riskand resiliency to late-life suicide ideation by investigating the associationsamong suicide ideation, depression, perceived physical health problems,psychological well-being, perceived meaning in life, social network, andreligious affiliation and observance. We hypothesized that suicide ideationwould be associated positively with depression and with number of self-reported health problems and negatively with domains of psychological well-being and with meaning in life. We predicted that suicide ideation wouldbe associated negatively with the size of one’s social network and withreligious affiliation and observance, and that the resiliency factors wouldexplain significant additional variance in suicide ideation scores afteraccounting for the risk factors.
METHODS
Participants
The present sample included 107 older adults (mean age = 81.5 years,SD = 7.7, range 67 to 98 years; 76% were female) who were living inde-pendently or in care-providing facilities. Voluntary participants wererecruited from community centers or senior’s programs (n = 10), retirementresidences (n = 9), nursing residences (n = 45), general hospital wards andgeriatric medicine clinics (n = 25), and from psychogeriatric outpatientpractices or inpatient units (n = 18). Most participants had at least attendedhigh school (78%), and 32% had attended college, university, or graduateor professional school. The majority reported being Protestant (50.5%),33% were Jewish, and 13% were Catholic. Over three-quarters wereunmarried (77%), the majority was either widowed (58%) or divorced orseparated (14%). Participants reported having an average of 2.4 children(SD = 1.5; range 0 to 9) and 4.4 grandchildren (SD = 3.8; range, 0 to 18).
Procedure
Participants were referred by a healthcare provider or self-referredduring residence community meetings or presentations to seniors groups.Providers were asked to refer patients who were ≥ 65 years of age andable to comprehend and respond to study measures. Individuals wereexcluded who were < 65 years of age, demonstrated extreme cognitiveimpairment (≤ 15 on the Mini-Mental State Examination or MMSE;Folstein, Folstein, & McHugh, 1975, or during the study interview), or
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014

56 CLINICAL GERONTOLOGIST
could not speak or understand English. Those with severe visual or motorlimitations were administered the measures verbally. Participants providedwritten consent, were debriefed fully upon completion of the study, andreferred for care if deemed necessary. This study was approved by univer-sity and hospital research ethics boards. Recruitment procedures andmethods are described more fully elsewhere (Heisel & Flett, 2006).
Measures
Suicide Ideation
Suicide ideation was assessed with the Geriatric Suicide Ideation Scale(GSIS), a 31-item multidimensional measure of suicide ideation developedand validated among older adults (Heisel & Flett, 2006). Scoring is on a 5-point Likert scale, ranging from 1 = Strongly Disagree to 5 = Strongly Agree.The GSIS assesses Suicide Ideation (e.g., “I want to end my life.”), DeathIdeation (e.g., “I welcome the thought of drifting off to sleep and never wak-ing up.”), Loss of Personal and Social Worth (e.g., “I generally feel prettyworthless.”), and Perceived Meaning in Life (e.g., “I am certain that I havesomething to live for.”). The GSIS has demonstrated strong internal consis-tency for total (a = 0.93) and subscale scores (a = 0.82 to 0.84), 1- to 2-monthtest-retest reliability for residents of long-term care facilities (r = 0.86 for thetotal scale and 0.75 to 0.78 for the subscales, p < 0.001), criterion validitydifferentiating mental health patients from nonpatients, construct validitywith hopelessness and suicide ideation, and nonconvergence with life satis-faction (Heisel & Flett, 2006). The GSIS Perceived Meaning in Life subscaleis reverse-scored, such that higher scores reflect less MIL.
Depression
Depression was assessed with the Geriatric Depression Scale (GDS), a30-item depression screening measure developed and validated among olderadults (Yesavage et al., 1983). The GDS has been used in hundreds ofstudies and has displayed strong internal consistency (α = 0.82 to 0.99), test-retest reliability (r = 0.85 to 0.94), and both construct and criterion validitywith respect to depression, suicide ideation, and related factors among olderadults across diverse settings and cultures (Stiles & McGarrahan, 1998).
Perceived Physical Health Problems
Perceived physical health problems were assessed with a self-reportitem instructing participants to “list any physical problems/illnesses
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014
Marnin J. Heisel and Gordon L. Flett 57
that you currently have,” in an open-ended fashion. The raw number ofself-reported physical problems was then treated as an outcome variable.We assessed this variable utilizing a self-report methodology, given asso-ciations between poor perceived health and morbidity, mortality, and useof healthcare services (Benyamini & Idler, 1999).
Psychological Well-Being
Psychological well-being was assessed with an 18-item short form ofRyff’s (1989) multidimensional Psychological Well-Being scale (PWB).In general, the 18-item version of the PWB has indicated acceptable psy-chometric properties, including correlations ranging from 0.70 to 0.89with the subscales of the longer form (Ryff & Keyes, 1995). Despite lowinternal consistency for the 3-item subscales, each of these scales wassignificantly associated with that scale alone, replicated the longer scale’s6-factor structure, and demonstrated excellent construct validity (Ryff &Keyes, 1995). For the purposes of the present study, we incorporated the9-item version of the Purpose in Life (PIL) scale into the PWB measure,given specific interest in exploring MIL and PIL.
Meaning in Life
Meaning in life was assessed broadly with the GSIS Perceived Meaning inLife subscale. We additionally conducted more focal analyses involving MILwith an item from the GSIS Perceived Meaning in Life subscale specificallyinvestigating MIL (“I feel that my life is meaningful”). For the purpose of thepresent analyses, we removed this item from total GSIS scores to reduce con-tent overlap and to facilitate examination of correlations between MIL andGSIS scores. We retained this item in analyses involving the GSIS PerceivedMeaning in Life subscale, because excluding the item did not significantlyalter associated findings (analyses available upon request).
Social Network
Social network was assessed with self-report items investigatingcurrent marital status, involvement in a “romantic relationship,” andnumbers of children and grandchildren.
Religious Affiliation and Observance
Religious affiliation and observance was assessed with an open-endedquestion investigating participant’s religion, a Yes/No question assessing
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014
58 CLINICAL GERONTOLOGIST
perceived religiosity (“Do you consider yourself a religious person?”), andopen-ended questions assessing frequency of attending religious services(“How often do you attend religious services?”) and frequency of conductingreligious rituals (“How often do you engage in religious rituals [e.g. prayer]?”).
RESULTS
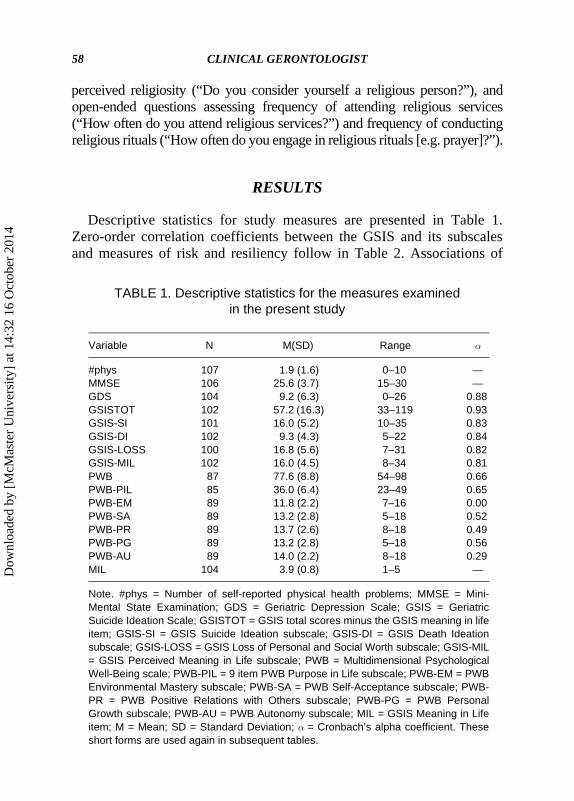
Descriptive statistics for study measures are presented in Table 1.Zero-order correlation coefficients between the GSIS and its subscalesand measures of risk and resiliency follow in Table 2. Associations of
TABLE 1. Descriptive statistics for the measures examined in the present study
Variable N M(SD) Range a
#phys 107 1.9 (1.6) 0–10 —MMSE 106 25.6 (3.7) 15–30 —GDS 104 9.2 (6.3) 0–26 0.88GSISTOT 102 57.2 (16.3) 33–119 0.93GSIS-SI 101 16.0 (5.2) 10–35 0.83GSIS-DI 102 9.3 (4.3) 5–22 0.84GSIS-LOSS 100 16.8 (5.6) 7–31 0.82GSIS-MIL 102 16.0 (4.5) 8–34 0.81PWB 87 77.6 (8.8) 54–98 0.66PWB-PIL 85 36.0 (6.4) 23–49 0.65PWB-EM 89 11.8 (2.2) 7–16 0.00PWB-SA 89 13.2 (2.8) 5–18 0.52PWB-PR 89 13.7 (2.6) 8–18 0.49PWB-PG 89 13.2 (2.8) 5–18 0.56PWB-AU 89 14.0 (2.2) 8–18 0.29MIL 104 3.9 (0.8) 1–5 —
Note. #phys = Number of self-reported physical health problems; MMSE = Mini-Mental State Examination; GDS = Geriatric Depression Scale; GSIS = GeriatricSuicide Ideation Scale; GSISTOT = GSIS total scores minus the GSIS meaning in lifeitem; GSIS-SI = GSIS Suicide Ideation subscale; GSIS-DI = GSIS Death Ideationsubscale; GSIS-LOSS = GSIS Loss of Personal and Social Worth subscale; GSIS-MIL= GSIS Perceived Meaning in Life subscale; PWB = Multidimensional PsychologicalWell-Being scale; PWB-PIL = 9 item PWB Purpose in Life subscale; PWB-EM = PWBEnvironmental Mastery subscale; PWB-SA = PWB Self-Acceptance subscale; PWB-PR = PWB Positive Relations with Others subscale; PWB-PG = PWB PersonalGrowth subscale; PWB-AU = PWB Autonomy subscale; MIL = GSIS Meaning in Lifeitem; M = Mean; SD = Standard Deviation; a = Cronbach’s alpha coefficient. Theseshort forms are used again in subsequent tables.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014
Marnin J. Heisel and Gordon L. Flett 59
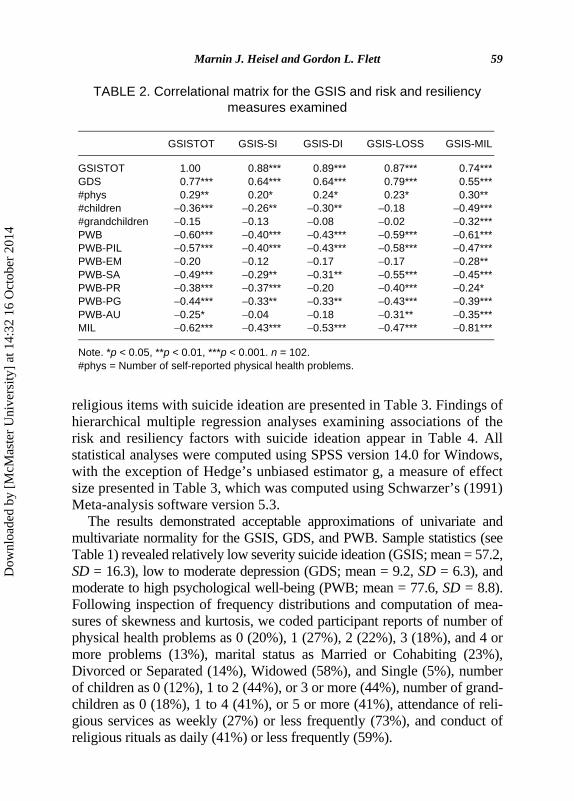
religious items with suicide ideation are presented in Table 3. Findings ofhierarchical multiple regression analyses examining associations of therisk and resiliency factors with suicide ideation appear in Table 4. Allstatistical analyses were computed using SPSS version 14.0 for Windows,with the exception of Hedge’s unbiased estimator g, a measure of effectsize presented in Table 3, which was computed using Schwarzer’s (1991)Meta-analysis software version 5.3.
The results demonstrated acceptable approximations of univariate andmultivariate normality for the GSIS, GDS, and PWB. Sample statistics (seeTable 1) revealed relatively low severity suicide ideation (GSIS; mean = 57.2,SD = 16.3), low to moderate depression (GDS; mean = 9.2, SD = 6.3), andmoderate to high psychological well-being (PWB; mean = 77.6, SD = 8.8).Following inspection of frequency distributions and computation of mea-sures of skewness and kurtosis, we coded participant reports of number ofphysical health problems as 0 (20%), 1 (27%), 2 (22%), 3 (18%), and 4 ormore problems (13%), marital status as Married or Cohabiting (23%),Divorced or Separated (14%), Widowed (58%), and Single (5%), numberof children as 0 (12%), 1 to 2 (44%), or 3 or more (44%), number of grand-children as 0 (18%), 1 to 4 (41%), or 5 or more (41%), attendance of reli-gious services as weekly (27%) or less frequently (73%), and conduct ofreligious rituals as daily (41%) or less frequently (59%).
TABLE 2. Correlational matrix for the GSIS and risk and resiliency measures examined
GSISTOT GSIS-SI GSIS-DI GSIS-LOSS GSIS-MIL
GSISTOT 1.00 0.88*** 0.89*** 0.87*** 0.74***GDS 0.77*** 0.64*** 0.64*** 0.79*** 0.55***#phys 0.29** 0.20* 0.24* 0.23* 0.30**#children −0.36*** −0.26** −0.30** −0.18 −0.49***#grandchildren −0.15 −0.13 −0.08 −0.02 −0.32***PWB −0.60*** −0.40*** −0.43*** −0.59*** −0.61***PWB-PIL −0.57*** −0.40*** −0.43*** −0.58*** −0.47***PWB-EM −0.20 −0.12 −0.17 −0.17 −0.28**PWB-SA −0.49*** −0.29** −0.31** −0.55*** −0.45***PWB-PR −0.38*** −0.37*** −0.20 −0.40*** −0.24*PWB-PG −0.44*** −0.33** −0.33** −0.43*** −0.39***PWB-AU −0.25* −0.04 −0.18 −0.31** −0.35***MIL −0.62*** −0.43*** −0.53*** −0.47*** −0.81***
Note. *p < 0.05, **p < 0.01, ***p < 0.001. n = 102.#phys = Number of self-reported physical health problems.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014
60 CLINICAL GERONTOLOGIST
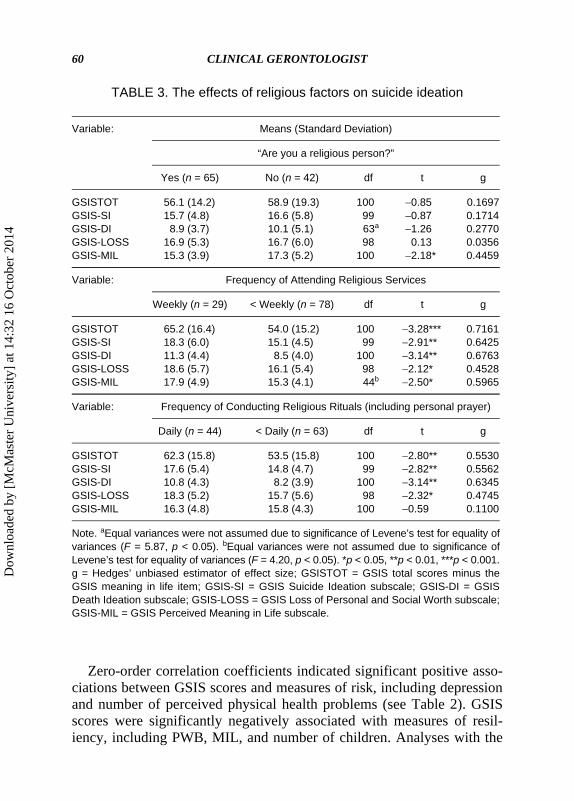
Zero-order correlation coefficients indicated significant positive asso-ciations between GSIS scores and measures of risk, including depressionand number of perceived physical health problems (see Table 2). GSISscores were significantly negatively associated with measures of resil-iency, including PWB, MIL, and number of children. Analyses with the
TABLE 3. The effects of religious factors on suicide ideation
Variable: Means (Standard Deviation)
“Are you a religious person?”
Yes (n = 65) No (n = 42) df t g
GSISTOT 56.1 (14.2) 58.9 (19.3) 100 −0.85 0.1697GSIS-SI 15.7 (4.8) 16.6 (5.8) 99 −0.87 0.1714GSIS-DI 8.9 (3.7) 10.1 (5.1) 63a −1.26 0.2770GSIS-LOSS 16.9 (5.3) 16.7 (6.0) 98 0.13 0.0356GSIS-MIL 15.3 (3.9) 17.3 (5.2) 100 −2.18* 0.4459
Variable: Frequency of Attending Religious Services
Weekly (n = 29) < Weekly (n = 78) df t g
GSISTOT 65.2 (16.4) 54.0 (15.2) 100 −3.28*** 0.7161GSIS-SI 18.3 (6.0) 15.1 (4.5) 99 −2.91** 0.6425GSIS-DI 11.3 (4.4) 8.5 (4.0) 100 −3.14** 0.6763GSIS-LOSS 18.6 (5.7) 16.1 (5.4) 98 −2.12* 0.4528GSIS-MIL 17.9 (4.9) 15.3 (4.1) 44b −2.50* 0.5965
Variable: Frequency of Conducting Religious Rituals (including personal prayer)
Daily (n = 44) < Daily (n = 63) df t g
GSISTOT 62.3 (15.8) 53.5 (15.8) 100 −2.80** 0.5530GSIS-SI 17.6 (5.4) 14.8 (4.7) 99 −2.82** 0.5562GSIS-DI 10.8 (4.3) 8.2 (3.9) 100 −3.14** 0.6345GSIS-LOSS 18.3 (5.2) 15.7 (5.6) 98 −2.32* 0.4745GSIS-MIL 16.3 (4.8) 15.8 (4.3) 100 −0.59 0.1100
Note. aEqual variances were not assumed due to significance of Levene’s test for equality ofvariances (F = 5.87, p < 0.05). bEqual variances were not assumed due to significance ofLevene’s test for equality of variances (F = 4.20, p < 0.05). *p < 0.05, **p < 0.01, ***p < 0.001.g = Hedges’ unbiased estimator of effect size; GSISTOT = GSIS total scores minus theGSIS meaning in life item; GSIS-SI = GSIS Suicide Ideation subscale; GSIS-DI = GSISDeath Ideation subscale; GSIS-LOSS = GSIS Loss of Personal and Social Worth subscale;GSIS-MIL = GSIS Perceived Meaning in Life subscale.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014
Marnin J. Heisel and Gordon L. Flett 61
PWB subscales identified few associations between GSIS scores andPWB Environmental Mastery and Autonomy subscales. Lower PWBAutonomy scores were associated with the GSIS subscales assessing Loss
TABLE 4. Summary of a hierarchical multiple regression analysis of risk and resiliency factors on suicide ideation (GSISTOT, n = 85)
Variable B SE B b t p
Step 1 (Intercept) 75.88 25.17 — 3.020.430.28
−1.963.816.80
−0.86−0.47−1.342.44
−3.761.723.64
−0.961.46
−3.374.33
−1.30−0.15−0.810.48
−1.130.903.47
−1.311.18
−3.174.750.12
0.003Sex 1.51 3.54 0.04 0.670Age 0.06 0.22 0.03 0.782MMSE −0.92 0.47 −0.22 0.054Psychogeriatric 7.02 1.84 0.39 0.000
Step 2 (Intercept) 146.49 21.54 — 0.000Sex −2.23 2.61 −0.07 0.396Age −0.08 0.16 −0.04 0.640MMSE −0.48 0.36 −0.12 0.185Psychogeriatric 3.42 1.40 0.19 0.017PWB −0.55 0.15 −0.34 0.000Attends 2.16 1.25 0.14 0.089Conducts 4.13 1.13 0.29 0.000#children −2.24 2.33 −0.10 0.340#grandchildren 3.10 2.13 0.15 0.150MIL −5.85 1.74 −0.29 0.001
Step 3 (Intercept) 95.08 21.94 — 0.000Sex −3.01 2.32 −0.09 0.198Age −0.02 0.15 −0.01 0.879MMSE −0.26 0.32 −0.06 0.423Psychogeriatric 0.66 1.38 0.04 0.635PWB −0.17 0.15 −0.11 0.261Attends 1.03 1.14 0.06 0.370Conducts 3.52 1.01 0.25 0.001#children −2.71 2.07 −0.12 0.195#grandchildren 2.23 1.89 0.11 0.243MIL −4.97 1.57 −0.25 0.002GDS 1.09 0.23 0.47 0.000#phys 0.09 0.76 0.01 0.908
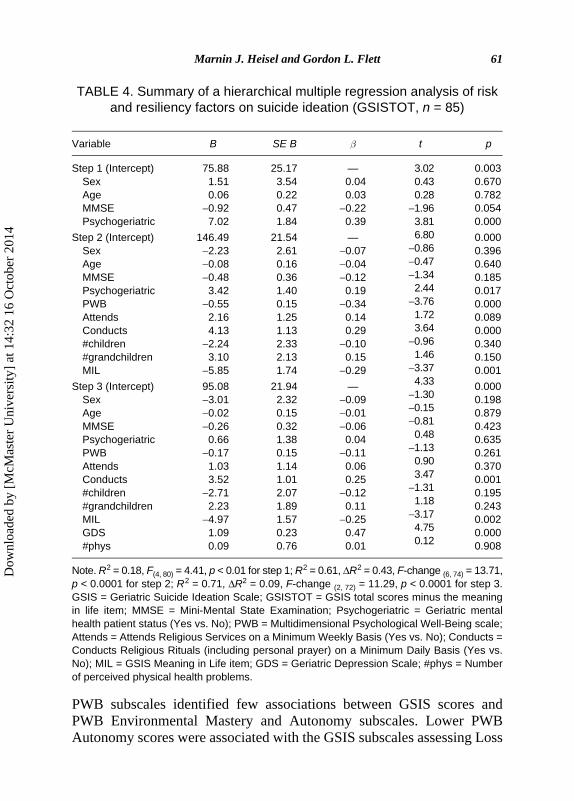
Note. R2 = 0.18, F(4, 80) = 4.41, p < 0.01 for step 1; R2 = 0.61, ΔR2 = 0.43, F-change (6, 74) = 13.71,p < 0.0001 for step 2; R2 = 0.71, ΔR2 = 0.09, F-change (2, 72) = 11.29, p < 0.0001 for step 3.GSIS = Geriatric Suicide Ideation Scale; GSISTOT = GSIS total scores minus the meaningin life item; MMSE = Mini-Mental State Examination; Psychogeriatric = Geriatric mentalhealth patient status (Yes vs. No); PWB = Multidimensional Psychological Well-Being scale;Attends = Attends Religious Services on a Minimum Weekly Basis (Yes vs. No); Conducts =Conducts Religious Rituals (including personal prayer) on a Minimum Daily Basis (Yes vs.No); MIL = GSIS Meaning in Life item; GDS = Geriatric Depression Scale; #phys = Numberof perceived physical health problems.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014
62 CLINICAL GERONTOLOGIST
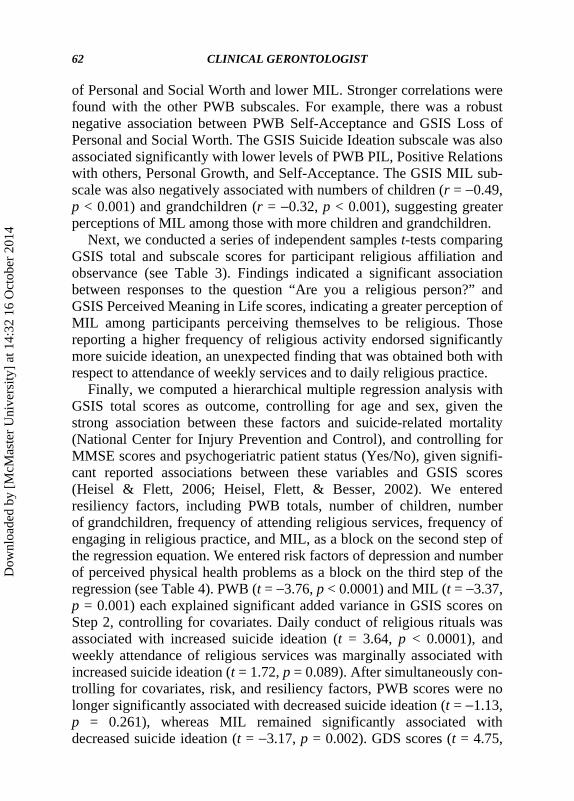
of Personal and Social Worth and lower MIL. Stronger correlations werefound with the other PWB subscales. For example, there was a robustnegative association between PWB Self-Acceptance and GSIS Loss ofPersonal and Social Worth. The GSIS Suicide Ideation subscale was alsoassociated significantly with lower levels of PWB PIL, Positive Relationswith others, Personal Growth, and Self-Acceptance. The GSIS MIL sub-scale was also negatively associated with numbers of children (r = −0.49,p < 0.001) and grandchildren (r = −0.32, p < 0.001), suggesting greaterperceptions of MIL among those with more children and grandchildren.
Next, we conducted a series of independent samples t-tests comparingGSIS total and subscale scores for participant religious affiliation andobservance (see Table 3). Findings indicated a significant associationbetween responses to the question “Are you a religious person?” andGSIS Perceived Meaning in Life scores, indicating a greater perception ofMIL among participants perceiving themselves to be religious. Thosereporting a higher frequency of religious activity endorsed significantlymore suicide ideation, an unexpected finding that was obtained both withrespect to attendance of weekly services and to daily religious practice.
Finally, we computed a hierarchical multiple regression analysis withGSIS total scores as outcome, controlling for age and sex, given thestrong association between these factors and suicide-related mortality(National Center for Injury Prevention and Control), and controlling forMMSE scores and psychogeriatric patient status (Yes/No), given signifi-cant reported associations between these variables and GSIS scores(Heisel & Flett, 2006; Heisel, Flett, & Besser, 2002). We enteredresiliency factors, including PWB totals, number of children, numberof grandchildren, frequency of attending religious services, frequency ofengaging in religious practice, and MIL, as a block on the second step ofthe regression equation. We entered risk factors of depression and numberof perceived physical health problems as a block on the third step of theregression (see Table 4). PWB (t = −3.76, p < 0.0001) and MIL (t = −3.37,p = 0.001) each explained significant added variance in GSIS scores onStep 2, controlling for covariates. Daily conduct of religious rituals wasassociated with increased suicide ideation (t = 3.64, p < 0.0001), andweekly attendance of religious services was marginally associated withincreased suicide ideation (t = 1.72, p = 0.089). After simultaneously con-trolling for covariates, risk, and resiliency factors, PWB scores were nolonger significantly associated with decreased suicide ideation (t = −1.13,p = 0.261), whereas MIL remained significantly associated withdecreased suicide ideation (t = −3.17, p = 0.002). GDS scores (t = 4.75,
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014

Marnin J. Heisel and Gordon L. Flett 63
p < 0.0001) were significantly associated with increased suicide ideation,as was daily conduct of religious rituals (t = 3.47, p = 0.001).
DISCUSSION
The present study assessed the impact of a set of risk and resiliencyfactors on late-life suicide ideation. Findings supported hypothesizednegative associations between suicide ideation and number of children,subjective religiosity, psychological well-being, and perceived meaningin life, and hypothesized positive associations between suicide ideationand both depression and number of perceived physical health problems.Support was also obtained for hypothesized negative associationsbetween suicide ideation and domains of PWB and MIL, as well asbetween suicide ideation and number of children and perceived religios-ity. These findings are consistent with research demonstrating close linksbetween depression, perceived health problems, and late-life suicideideation (Bartels et al., 2002; Duberstein et al., 2004b; Uncapher,Gallagher-Thompson, Osgood, & Bongar, 1998), and additionallysuggest the need to attend to the role of adaptive psychological factors inmitigating suicide risk among older adults.
The correlation obtained between GSIS scores and open-ended reportsof the number of physical health problems is in keeping with researchassociating health problems with late-life suicidal thoughts and behavior(Duberstein et al., 2004a; Erlangsen, Vach, & Jeune, 2005; Juurlink et al.,2004; Koponen et al., 2007), extends our previous research demonstratingan association of GSIS scores with severity of physical health problems(Heisel & Flett, 2007), and suggests the importance of assessing suicideideation among older adults struggling with health problems.
The findings suggest that domains of PWB protect against suicide ide-ation, even though our data confirmed previous findings of poor internalconsistency for the three-item PWB subscales, especially for the Environ-mental Mastery (EM) subscale. Visual inspection of the EM subscalereveals items reflecting a sense of control over one’s life, despair overlife’s demands, and success in managing one’s responsibilities. Althoughrelated to a general sense of mastery, these items appear to reflect possi-ble heterogeneous concerns among older adults, thereby partly accountingfor the low internal consistency of this subscale. The impact of these findingsmay be underestimated due to the low internal consistency of the PWBmeasures; however, findings were consistent with predicted negative
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014

64 CLINICAL GERONTOLOGIST
associations between PWB and suicide ideation. More fine-grainedanalyses indicated a protective role of specific domains of PWB: PIL,self-acceptance, autonomy, personal growth, and positive relations withothers. The pattern of correlations between the GSIS and PWB subscalesis in keeping with past accounts that emphasize the need for older adultsto remain connected with others and to maintain a positive self-image(Ryff, 1989). Our results indicated that both Positive Relations withOthers and Self-Acceptance were associated with lower scores on GSISsubscales assessing Suicide Ideation and Loss of Personal and SocialWorth. Environmental Mastery was significantly associated with MIL,but not with other aspects of late-life suicide ideation, indicating therobust role of MIL as a resiliency factor among older adults.
The present findings broadly support Frankl’s (1985) contention thatrecognition of meaning in life helps protect against despair and suicidalcontemplations. The results further replicate our findings with an adultclinical sample (Heisel & Flett, 2004), suggesting that MIL and PIL con-tribute to suicide resiliency among disparate populations at elevated sui-cide risk. Although intercorrelated, MIL and PIL are somewhat distinctconstructs that might differentially protect against suicide ideation in dif-ferent populations. PIL scores were significantly negatively associatedwith suicide ideation in the present analyses, but were not significantlyassociated with suicide ideation after accounting for MIL. MIL, in turn,significantly predicted suicide ideation scores above and beyond PIL.Inspection of the PIL items revealed an element of future orientation thatmay be less relevant to meaning perception among older adults. In laterlife, perception of MIL may turn from future possibilities to past accom-plishments (Frankl, 1988), corresponding to successful resolution ofErikson’s (1963) “ego integrity.”
Findings of a negative association between number of children and sui-cide ideation lend support to findings from Moore’s (1997) phenomeno-logical study among suicidal older adults linking perceived meaninglessnesswith psychache, social isolation, powerlessness, and alienation. Thesedata suggest the importance of perceived social support and of social inte-gration in protecting against late-life suicide (Duberstein et al., 2004b),and a potential role for interpersonally oriented forms of psychotherapy inhelping to reduce late-life suicide risk (Bruce et al., 2004). In addition,numbers of children and of grandchildren were significantly negativelyassociated with GSIS-MIL scores, suggesting that having a greater num-ber of offspring helps promote recognition of MIL and thus helps reducethe likelihood of contemplating suicide. Quality of relationships, rather
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014

Marnin J. Heisel and Gordon L. Flett 65
than size of one’s social network, may be more closely associated withresiliency to suicide ideation. Research is needed assessing older adults’perceptions of social support, frequency and/or quality of social interac-tions including presence of conflict, and degree of social integration asthey impact upon late-life suicide ideation.
A significant association emerged between GSIS Perceived MILscores and religiosity, as older adults reporting themselves to be a “reli-gious person” reported significantly more perceived MIL than thosedeclaring themselves to be nonreligious. These findings are consistentwith research demonstrating greater perceived MIL associated withreligiosity and gerotranscendence (Braam et al., 2006). Non-significantfindings between self-reported religiosity and GSIS totals and other sub-scale scores suggest a possible unique characteristic of this GSIS subscalethat is not captured by more standard measures of suicide ideation, deathideation, and perceived loss of worth. The significant association betweenheightened suicide ideation and both increased frequency of attendingreligious services and of engaging in religious rituals was unexpected.Although we cannot rule out the possibility that religiosity instigates orexacerbates suicide ideation for some older adults, a likelier interpretationof these findings is that older adults experiencing higher levels of suicideideation are more likely to turn to fervent religious observance for helpthan are less suicidal older adults. This finding is consistent with researchindicating that among secular older adults, higher levels of religiousobservance are associated with more severe depressive symptoms (Braamet al., 2007). This finding may also reflect underlying inter-religion differ-ences in frequency of religious practice. Sample characteristics restrictedexploration of associations between suicide ideation and religious factorsin more ethnically diverse, non-Judeo-Christian older adults, necessitatingfuture research.
The present study suggests that attending to both suicide resiliency andrisk may benefit theory and clinical practice with older adults at risk forsuicide. Research is needed exploring additional aspects of psychologicalresiliency among older adults, such as spirituality, perceived socialsupport, coping, optimism, creativity, and attitudinal characteristics. Ourfindings are limited by a cross-sectional methodology, and a largely cul-turally homogeneous sample.
Limited research exists exploring MIL and other resiliency variablesthat are potentially protective against suicide risk among diverse samplesof older adults. Researchers have suggested that sociocultural factors mayplay a key role in conferring risk for suicide or conversely in fomenting
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014

66 CLINICAL GERONTOLOGIST
resiliency among older adults, potentially helping to explain lower ratesof suicide among older women than older men (Canetto, 1992), and lowrates of suicide among Canadian Inuit elders despite elevated rates of sui-cide among young Inuit (Kral et al., 1998). A recent literature reviewindicated that religious and spiritual factors, social cohesion, and proso-cial behavior help decrease risk for suicide among African Americans(Utsey, Hook, & Stanard, 2007). Utsey and colleagues (2007) indicatedthat these factors are best considered in the context of African Americanculture, noting that cultural pride, identity, and consciousness all helpreduce risk for suicide, even in the face of racism and prejudice. Beckerand Newsom (2005) identified a similar set of variables associated withresilience to serious medical illness among chronically ill older AfricanAmericans. Research suggests that African Americans are less acceptingof suicide and euthanasia than are Whites, a finding partially reflective ofdifferences in degree of religious commitment (Cicirelli, 1997; Lichtenstein,Alcser, Corning, Bachman, & Doukas, 1997; Neeleman, Wessely, & Lewis,1998). Krause (2003) reported that African American older adults morefrequently report finding meaning in religion than do White older adults,and further reported stronger associations among religious MIL, optimism,self-esteem, and life satisfaction for African American older adults.Research is needed exploring suicide risk and resiliency factors amongdiverse samples of older adults.
Our findings suggest that MIL protects against late-life suicide ide-ation. We employed a single-item measure of MIL in some analyses inorder to disambiguate associations between GSIS total scores and theGSIS Perceived MIL subscale, and in order to focus upon the specificassociation of perceived MIL with suicide ideation. Although very briefscales can be quite appropriate (Burisch, 1984), psychometric limitationswith single-item measurement can include potential restriction of reliabil-ity and validity; these problems can be compounded among older adultsin whom hearing changes can increase the possibility of mishearing ormisunderstanding an item. Findings with this item were quite robust,however, lending general support to our results. Future research is neededemploying multi-item and multidimensional measures of MIL, in order toexplore the presence, degree, and manner by which creative, experiential,attitudinal, and ultimate sources of MIL protect against late-life suicideideation. Research is additionally needed exploring risk and resiliencyfactors associated with suicidal behavior and with death by suicide. Clini-cal implications include the importance of assessing for resiliency whenassessing late-life suicide risk, and the potential value in drawing on
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014
Marnin J. Heisel and Gordon L. Flett 67
seniors’ stores of life experience and potentially burgeoning existentialawareness (Nygren et al., 2005) when working to effect psychologicalchange, enhance health and well-being, and ultimately prevent suicide.Clinical intervention research is needed exploring the role of resiliencyfactors in potentially moderating or mediating treatment outcome witholder adults at risk for suicide, and interventions to directly enhanceperceptions of meaning in life and other resiliency factors among olderadults. Expanding our focus on resiliency factors, in addition to a risk-factorapproach, may enhance our understanding of late-life suicide risk andsuggest innovative approaches to preventing suicide among older adults.
REFERENCES
Bartels, S.J., Coakley, E., Oxman, T.E., Constantino, G., Oslin, D., Chen, H., Zubritsky,C., Cheal, K., Durai, U.N., Gallo, J.J., Llorente, M., & Sanchez, H. (2002). Suicidaland death ideation in older primary care patients with depression, anxiety, and at-riskalcohol use. The American Journal of Geriatric Psychiatry, 10, 417−427.
Becker, G., & Newsom, E. (2005). Resilience in the face of serious illness among chroni-cally ill African Americans in later life. Journal of Gerontology: Social Sciences, 60B,S214–S223.
Benyamini Y., & Idler E.L. (1999). Community studies reporting association betweenself-rated health and mortality: additional studies, 1995–1998. Research on Aging, 21,392–401.
Blazer, D.G., Hybels, C.F., & Pieper, C.F. (2001). The association of depression and mor-tality in elderly persons: A case for multiple, independent pathways. The Journals ofGerontology Series A: Biological Sciences and Medical Sciences, 56, M505–M509.
Braam, A.W., Bramsen, I., van Tilburg, T.G., van der Ploeg, H.M., & Deeg, D.J.H.(2006). Cosmic transcendence and framework of meaning in life: Patterns among olderadults in the Netherlands. Journal of Gerontology: Social Sciences, 61B, S121–S128.
Braam, A.W., Deeg, D.J.H., Poppelaars, J.L., Beekman, A.T.F., & van Tilburg, W. (2007).Prayer and depressive symptoms in a period of secularization: Patterns among older adultsin the Netherlands. The American Journal of Geriatric Psychiatry, 15, 273–281.
Bruce, M.L., Ten Have, T.R., Reynolds III, C.F., Katz, I.I., Schulberg, H.C., Mulsant,B.H., Brown, G.K., McAvay, G.J., Pearson, J.L., & Alexopoulos, G.S. (2004). Reduc-ing suicidal ideation and depressive symptoms in depressed older primary carepatients. A randomized controlled trial. JAMA, 291, 1081–1091.
Burisch, M. (1984). You don’t always get what you pay for: Measuring depression withshort and simple versus long and sophisticated scales. Journal of Research in Person-ality, 18, 81–98.
Canadian Coalition for Seniors’ Mental Health (2006). National guidelines for seniors’mental health: The assessment of suicide risk and prevention of suicide. Toronto:Author.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014

68 CLINICAL GERONTOLOGIST
Canetto, S.S. (1992). Gender and suicide in the elderly. Suicide and Life-ThreateningBehavior, 22, 80–97.
Cicirelli, V.G. (1997). Relationship of psychosocial and background variables to olderadults’ end-of-life decisions. Psychology and Aging, 12, 72–83.
Clarke, P.J., Marshall, V.W., Ryff, C.D., & Wheaton, B. (2001). Measuring psychologicalwell-being in the Canadian Study of Health and Aging. International Psychogeriatrics,13, 79–90.
Duberstein, P.R., Conwell, Y., Conner, K., Eberly, S., & Caine, E.D. (2004a). Suicide at50 years of age and older: Perceived physical illness, family discord and financialstrain. Psychological Medicine, 34, 137–146.
Duberstein, P.R., Conwell, Y., Conner, K., Eberly, S., Evinger, J.S., & Caine, E.D.(2004b). Poor social integration and suicide: Fact or artifact? Psychological Medicine,34, 1331–1337.
Durkheim, E. (1966). Suicide: A study in sociology. New York: Free Press.Erikson, E.H. (1963). Childhood and society (2nd ed.). New York: Norton.Erlangsen, A., Vach, W., & Jeune, B. (2005). The effect of hospitalization with medical
illnesses on the suicide risk in the oldest old: A population-based register study.Journal of the American Geriatrics Society, 53, 771–776.
Fisher, B.J. (1995). Successful aging, life satisfaction, and generativity in later life.International Journal of Aging and Human Development, 41, 239–250.
Folstein, M.F., Folstein, S.E., & McHugh, P.R. (1975). ‘Mini-mental state’: A practicalmethod for grading the cognitive state of patients for the clinician. Journal of PsychiatricResearch, 12, 189–198.
Frankl, V.E. (1985). Man’s search for meaning. New York: Simon & Schuster.Frankl, V.E. (1988). The will to meaning: Foundations and applications of Logotherapy.
New York: Penguin.Heisel, M.J. (2006). Suicide and its prevention among older adults. Canadian Journal of
Psychiatry, 51, 143–154.Heisel, M.J., & Flett, G.L. (2007). Meaning in life and resilience to suicidal thoughts
among older adults. In P.T.P. Wong, L.C.J. Wong, M. McDonald, & D. Klaassen(Eds.), The positive psychology of meaning and spirituality (pp. 183–196). Abbotsford,BC: INPM Press.
Heisel, M.J., & Flett, G.L. (2006). The development and initial validation of the GeriatricSuicide Ideation Scale. The American Journal of Geriatric Psychiatry, 14, 742–751.
Heisel, M.J., & Flett, G.L. (2004). Purpose in life, satisfaction with life and suicide ide-ation in a clinical sample. Journal of Psychopathology and Behavioral Assessment, 26,127–135.
Heisel, M.J., Flett, G.L., & Besser, A. (2002). Cognitive functioning and geriatric suicideideation: Testing a mediational model. The American Journal of Geriatric Psychiatry,10, 428–436.
Hickson, J., & Housley, W. (1997). Creativity in later life. Educational Gerontology, 23,539–547.
Hirsch, J.K., Duberstein, P.R., Conner, K.R., Heisel, M.J., Beckman, A., Franus, N., &Conwell, Y. (2006). Future orientation and suicide ideation and attempts in depressedadults ages 50 and over. The American Journal of Geriatric Psychiatry, 14, 752–757.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014

Marnin J. Heisel and Gordon L. Flett 69
Juurlink, D.N., Herrmann, N., Szalai, J.P., Kopp, A., & Redelmeier, D.A. (2004). Medi-cal illness and the risk of suicide in the elderly. Archives of Internal Medicine, 164,1179–1184.
Kafka, G.J., & Kozma, A. (2002). The construct validity of Ryff’s Scales of PsychologicalWell-Being (SPWB) and their relationship to measures of subjective well-being.Social Indicators Research, 57, 171–190.
Koponen, H.J., Viilo, K., Hakko, H., Timonen, M., Meyer-Rochow, V.B., Sarkioja, T., &Rasanen, P. (2007). Rates and previous disease history in old age suicide. InternationalJournal of Geriatric Psychiatry, 22, 38–46.
Kral, M.J., Arnakaq, M., Ekho, N., Kunuk, O., Ootoova, E., Papatsie, M., & Taparti, L.(1998). Stories of distress and healing: Inuit elders on suicide. In A.A. Leenaars,S. Wenckstern, I. Sakinofsky, R.J. Dyck, M.J. Kral, & R.C. Bland (Eds.),Suicide inCanada (pp. 179–188). Toronto, ON: University of Toronto Press.
Krause, N. (2003). Religious meaning and subjective well-being in late life. Journal ofGerontology: Social Sciences, 58B, S160–S170.
Krause, N. (2004). Stressors arising in highly valued roles, meaning in life, and the physi-cal health status of older adults. Journals of Gerontology Series B: Psychological Sci-ences & Social Sciences, 59, S287–S297.
Lichtenstein, R.L., Alcser, K.H., Corning, A.D., Bachman, J.G., & Doukas, D.J. (1997).Black/White differences in attitudes toward physician-assisted suicide. Journal of theNational Medical Association, 89, 125–133.
Miller, J.S., Segal, D.L., & Coolidge, F.L. (2001). A comparison of suicidal thinking andreasons for living among younger and older adults. Death Studies, 25, 357–365.
Moore, S.L. (1997). A phenomenological study of meaning in life in suicidal older adults.Archives of Psychiatric Nursing, 11, 29–36.
National Center for Injury Prevention and Control. 1999–2002, United States SuicideInjury Deaths and Rates per 100,000. Available from http://www.cdc.gov/ncipc/wisqars/
Neeleman, J., Wessely, S., & Lewis, G. (1998). Suicide acceptability in African- andWhite Americans: The role of religion. The Journal of Nervous and Mental Disease,186, 12–16.
Nelson, F.L. (1977). Religiosity and self-destructive crises in the institutionalized elderly.Suicide and Life-Threatening Behavior, 7, 67–74.
Nygren, B., Alex, L., Jonsen, E., Gustafson, Y., Norberg, A., & Lundman, B. (2005).Resilience, sense of coherence, purpose in life and self-transcendence in relation toperceived physical and mental health among the oldest old. Aging & Mental Health, 9,354–362.
Petrie, K., & Brook, R. (1992). Sense of coherence, self-esteem, depression and hopeless-ness as correlates of reattempting suicide. British Journal of Clinical Psychology, 31,293–300.
Reker, G.T. (1997). Personal meaning, optimism, and choice: Existential predictors ofdepression in community and institutional elderly. The Gerontologist, 37, 709–716.
Rubenowitz, E., Waern, M., Wilhelmson, K., & Allebeck, P. (2001). Life events and psy-chosocial factors in elderly suicides: A case-control study. Psychological Medicine,31, 1193–1202.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014

70 CLINICAL GERONTOLOGIST
Ryff, C.D. (1989). Happiness is everything, or is it? Explorations on the meaning of psy-chological well-being. Journal of Personality and Social Psychology, 57, 1069–1081.
Ryff, C.D., & Keyes, C.L.M. (1995). The structure of psychological well-being revisited.Journal of Personality and Social Psychology, 69, 719–727.
Schwarzer, R. (1991). Meta-analysis software. Version 5.3. Dubuque, IA: Brown Publishers.Shneidman, E.S. (1996). The suicidal mind. NY: Oxford University Press.Stack, S., & Lester, D. (1991). The effect of religion on suicide ideation. Social Psychiatry
and Psychiatric Epidemiology, 26, 168–170.Stiles, P.G., & McGarrahan, J.F. (1998). The Geriatric Depression Scale: A comprehen-
sive review. Journal of Clinical Geropsychology, 4, 89–110.Turvey, C.L., Conwell, Y., Jones, M.P., Phillips, C., Simonsick, E., Pearson, J.L., & Wal-
lace, R. (2002). Risk factors for late-life suicide: A prospective, community-basedstudy. The American Journal of Geriatric Psychiatry, 10, 398–406.
Uncapher, H., Gallagher-Thompson, D., Osgood, N.J., & Bongar, B. (1998). Hopelessnessand suicidal ideation in older adults. The Gerontologist, 38, 62–70.
Utsey, S.O., Hook, J.N., & Stanard, P. (2007). A re-examination of cultural factors thatmitigate risk and promote resilience in relation to African American suicide: A reviewof the literature and recommendations for future research. Death Studies, 31, 399–416.
Van Ranst, N., & Marcoen, A. (1997). Meaning in life of young and elderly adults: Anexamination of the factorial validity and invariance of the life regard index. Personal-ity and Individual Differences, 22, 877–884.
Vanderhorst, R.K., & McLaren, S. (2005). Social relationships as predictors of depressionand suicidal ideation in older adults. Aging & Mental Health, 9, 517–525.
Yesavage, J.A., Brink, T.L., Rose, T.L., Lum, O., Huang, V., Adey, M., & Leirer, V.O.(1983). Development and validation of a geriatric depression screening scale: Apreliminary report. Journal of Psychiatric Research, 17, 37–49.
Dow
nloa
ded
by [
McM
aste
r U
nive
rsity
] at
14:
32 1
6 O
ctob
er 2
014