Embed Size (px)
Citation preview

Psychosocial Impact for Health Care Workers
David S. Goldbloom, MD, FRCPC
Centre for Addiction and Mental Health
University of Toronto
April 19, 2004
Disaster Response Conference
Learning from SARS: The

Learning Objectives
• To understand the trajectory of SARS as it spread through hospitals and around the world
• To describe the psychosocial impact of SARS on health care workers
• To discuss interventions to minimize the impact of such outbreaks on health care workers

Health Care Professionals Who Died of SARS in Toronto
Tecla Lin, nurse
Nestor Yanga, physician
Nelia Laroza, nurse

Government Inquiry
• Learning from SARS: Renewal of Public Learning from SARS: Renewal of Public Health in CanadaHealth in Canada – A Report of the National Advisory Committee on SARS and Public Health, October 2003
• Committee chaired by Dean David Naylor, Faculty of Medicine, University of Toronto
• Full report available on-line at: www.hc-sc.gc.ca/english/pdf/sars/sars-e.pdf

SARS Overview• Caused by a novel coronavirus• Emerged in China (Guangdong) in November 2002• ~8500 people worldwide diagnosed with probable
SARS; 21% of them HCWs (43% in Canada)• >900 SARS deaths worldwide• Diagnosis in acute illness is clinical• Treatment is primarily supportive• Transmission by respiratory droplet contact with
eyes, nose & mouth (NOT airborne, says WHO)• Risk of transmission greatest at day 10

Virus is stable in feces and urine at room temp for 1-2 days Virus is stable in diarrheal stool for up to 4 days because of its higher pH Virus loses infectivity after exposure to common disinfectants

Emerging Infectious Diseases
• Since 1973, >30 infectious diseases of bacterial and viral origin have emerged that are new or increased in incidence and geography
• Ebola (1977); Legionnaire’s (1977); E. Coli-linked hemolytic uremic syndrome (1982); HIV (1983); Hepatitis C (1989); variant Creutzfeld-Jacob (1996); avian flu (1997); West Nile (1999)
• SARS: The first novel 21st century disease

Globalization• According to World Tourism Organization data,
~715 million international tourist arrivals were registered at borders in 2002
• The volume, speed and reach of human travel has accelerated the spread of infectious diseases; it took smallpox centuries to cross the Atlantic. It took weeks for SARS to travel to 30 countries on 5 continents
• Globalization includes the food and feed trades• This is compounded by the threat of intentional or
accidental release of biological agents as acts of terrorism

Globalization
• 40 verified flights on which one or more people with SARS traveled while symptomatic
• Five international flights have been associated with transmission of SARS from symptomatic probable cases to passengers or crew
• No evidence of confirmed transmission after March 27 travel advisory and implementation of screening measures– WHO Consensus Document on the Epidemiology of
SARS, October 2003 (www.who.int/csr/sars/en/WHOconsensus.pdf)

The Pace of Discovery
• It took almost 10 years to determine the complete genetic sequence of HIV
• It took 11 weeks from the identification of the corona virus as the likely cause of SARS to the determination of its complete genetic sequence

Anatomy of the Outbreak
• “Have you heard of an epidemic in Guangzhou? An acquaintance of mine from a teachers’ [Internet] chat room lives there and reports that the hospitals there have been closed and people are dying”– Dr. Stephen Cunnion, February 10, 2003
• WHO weekly newsletter February 14, 2003 describes unusual respiratory illness affecting 300 people, more than 100 of them HCWs, in Guangdong province, with 5 fatalities

Anatomy of the Outbreak
• Guangdong outbreak publicized by Health Canada on its Fluwatch bulletin summarizing activity Feb 9-15, 2003 – and the next week Fluwatch reported that Chinese authorities declared the outbreak over

Anatomy of the Outbreak
• February 19: Hong Kong officials report case of avian influenza and, in conference call with Health Canada’s Pandemic Influenza Committee, recommend that all all provinces be vigilant for influenza-like provinces be vigilant for influenza-like illnesses in returning travellers, illnesses in returning travellers, particularly from Hong Kong & Chinaparticularly from Hong Kong & China
• February 20: Health Canada issues alerts re avian flu to all Public Health and hospital infection control officers

Anatomy of the Outbreak – Hong Kong
• Dr. Liu Jianlun, a 65 year old MD who treated atypical pneumonia patients in Guangdong travels to Hong Kong for nephew’s wedding
• Feels unwell as he checks into room 911 of the Metropole Hotel
• Infects at least 12 other guests and visitors on 9th floor from several countries, including a 78 year old woman from Canada

Anatomy of an Outbreak- Patient Zero in Canada
• February 23 – Mrs. K returns to Canada
• February 25 – she develops high fever
• February 28 – she visits her FP, also complaining of muscle aches, dry cough
• March 5 – she dies at home
No autopsy
Heart attack listed as cause of death

Anatomy of the Outbreak – Son of Patient Zero
• March 7 –her 44 year old son arrives at Scarborough Grace ER with cough, fever, and dyspnea and is kept in an open ER for 18-20 hours awaiting admission; he is near other patients and has many visitors
• March 8- he deteriorates & needs intubation in ICU; clinical concern was that he might have TB. He had not been outside Canada in 8 years
• March 13 – he dies of SARS and his TB test was negative

Anatomy of the Outbreak – The Hospital Spread
• March 16 – patient who had been in adjacent ER bed returns to hospital with SARS symptoms; he dies of SARS on March 21
• His wife and 3 other family members were infected, including his 6-month old son
• His wife infected 7 visitors to ER, 6 hospital staff, 2 patients, 2 paramedics, a firefighter and a housekeeper
• The MD who intubated him in ICU wore mask, eye protection, gown and gloves but developed SARS, as did 3 nurses present at intubation

Anatomy of the Outbreak – The Inter-Hospital Spread
• March 13 -A second patient who had been in the ER on March 7 was brought back to ER with an MI. He had mild respiratory symptoms and was treated with standard infection control procedures and was transferred to York Central Hospital
• He became the source of a 2nd cluster that affected >50 people and closed the hospital

Anatomy of the Outbreak – The Government Response
• March 13 –Health Canada notified of the Toronto cluster and initiates daily federal/provincial public health teleconferences
• March 14 – Ontario Ministry of Health and Longterm Care (MOHLTC) holds press conference with Toronto Public Health and hospital officials re atypical pneumonia cluster

Anatomy of the Outbreak
• SARS continues to spread among staff, patients and visitors to Scarborough Grace
• March 23 – ICU and ER at Grace closed and hospital closed to admissions/transfers; outpatient clinics closed and employees barred from working at other hospitals. Anyone who had entered the hospital after March 16 asked to go on voluntary 10-day home quarantine. Stringent infection control implemented (N95 masks, etc; isolation/negative pressure rooms for SARS pts)

Anatomy of the Outbreak
• March 23 – West Park Hospital, a rehab facility, is re-commissioned to create 25-bed SARS unit. Staff can be found for only 14 patients
• March 25 – Ontario government designates SARS as reportable, communicable, and virulent disease under the Health Protection and Promotion Act, giving Public Health officials tracking authority as well as authority to prevent activities that might transmit the disease

Anatomy of the Outbreak• March 25 – Health Canada reports 19 cases of SARS in
Canada – but 48 presumptive cases were hospitalized by the end of that day
• March 25-27 – highest peak in epidemiol curve• March 26 – West Park unit and all negative pressure
rooms in Toronto are full; 10 ill staff from Scarborough Grace are in ER awaiting admission and more are at home
• March 26 - Provincial emergency declared and all hospitals required to create SARS units
• Within 48 hours, Sunnybrook & Women’s puts 40 negative pressure rooms into operation

Anatomy of the Outbreak• March 26 – multi-ministry Provincial Operations
Centre for emergency response activated• Code Orange implemented for all Toronto and
Simcoe County hospitals:– Non-essential services suspended
– Visitors limited
– Protective clothing for staff
– Isolation units for SARS patients
• March 30 – access restrictions extended to all Ontario hospitals

Anatomy of the Outbreak
Meanwhile, elsewhere in Canada…• March 13 –man who had stayed at Metropole
hotel arrived at Vancouver General Hospital with flu-like illness; he lived with wife, had not been in contact with family/friends, and went to hospital directly when he became symptomatic
• He was masked and isolated • No known secondary transmissions from this
case

Anatomy of the Outbreak
Meanwhile, elsewhere in the world…• February 26 -American man who had been at Metropole
hotel flew to Hanoi and went to hospital there; several nurses fell ill.
• Dr. Carlo Urbani of WHO sent to Vietnam to investigate• March 11 -Dr. Urbani develops symptoms• March 29 -Dr. Urbani dies of SARS• March 11 –23 HCWs admitted to isolation ward in
Hong Kong with SARS symptoms• March 12 –WHO issues global alert

Information Sharing and Data Technology
• April 1 – SARS surveillance system efforts initiated; provincial infectious disease tracking and outbreak management software described as “an archaic DOS platform used in the late ’80s”
• Public Health developed new software, but individual cases and contacts were maintained on paper charts with colour-coded Post-It notes
• Hospitals in daily teleconferences

Scientific Advisory Committee
• Volunteers (MDs, infection control practitioners, administrators) who worked 24/7 to develop guidelines and directives which were then passed on to the Hospitals branch of MOHLTC for “translation into ‘Hospitalese’” and implementation
• Nuances sometimes lost and meanings sometimes blurred as directives passed through multiple channels; some directives controversial and difficult to implement (e.g., N95 mask use and fit testing)

Leadership
• “We never knew who was in charge”• Provincial Operations Centre jointly led by
Dr. Colin D’Cunha, Chief Medical Officer and Commissioner of Public Health, and Dr. Jim Young, Commissioner of Public Safety and Security
• Both subsequently agreed a single leader “SARS czar” would have been preferable

SARS One
• February 23-April 23• Largely a hospital-based disease spread• Concerns re community spread:
– April 3 attendees at funeral home fell ill– Employee of I.T. company defied quarantine, infected 1 co-
worker, 200 on home isolation– School closed when 1 student, son of a nurse, fell ill– Screening of fellow passengers of a nurse on a commuter
train who fell ill– 31 cases in close-knit religious community
• ~10,000 people placed on home quarantine

SARS One• Public Health investigated >1900 reports in
addition to 220 cases• Guidelines for family MDs not issued until April 3• Lack of system to distribute protective gear to
family MDs until April 21• April 13 – difficult intubation of infected MD led to
infection of 11 HCWs at Sunnybrook and Women’s• April 20 – Sunnybrook & Women’s closed its ICU
and SARS unit; Canada’s largest trauma centre stopped taking trauma patients

SARS One
• CDC investigators help determine transmission and reveal risks of inadvertent spread even with protective gear
• Extremely difficult to recruit staff from other hospitals to assist S&W which had largest volume of SARS patients
• April 19 – a hospital ward in British Columbia closed following secondary transmission of SARS to a nurse – first such case in B.C; the other three B.C. cases were travel-acquired

SARS One
• Easter/Passover approaches and church-based practices change
• April 23 – despite the accumulation of SARS cases, only 1 new case in previous 2 weeks
• April 23 – WHO issues travel advisory, as they had already done for Guangdong and Hong Kong
• April 30 – WHO travel advisory withdrawn• May 14 – WHO removes Toronto from list of sites
with recent local transmission• May 17 – Provincial emergency lifted, Provincial
Operations Centre dismantled, Code Orange over

The Respite
• April 24 – May 22• All levels of government state SARS over• 140 probable and 178 suspect cases, and 24
deaths• Hospitals ease rules re protective
equipment, # of visitors, rules re distance sitting apart at meals
• BUT…North York General and St. John’s Rehabilitation Hospitals….

North York General Hospital
• April 20-May 7: 3 former inpatients on psychiatry unit present with pneumonia but no epidemiological links. Ruled out as new cluster
• Meanwhile, several elderly patients on orthopedic unit presented with what appeared to be post-op lung infections
• April 29: ICU nurse from NYGH admitted with respiratory symptoms which ultimately were SARs
• Mid-May: family members of orthopedic patient present to ER with SARS symptoms

St. John’s Rehabilitation Hospital
• Steady flow of patients from acute care hospitals, including NYGH
• 3rd week in May – 3 patients with SARS-like symptoms
• May 22 – Public Health visits hospital. No epidemiological link found

SARS Two
• May 23-June 30• May 23 – 5 new people under
investigation; anyone who had been in St. John’s Rehab or NYGH in preceding ~2 weeks ordered into quarantine
• NYGH open only to SARS admissions• Exact chain of events leading to SARS
Two remains a mystery

SARS Two
• All hospitals resume infection control rules• 4 hospitals declared SARS facilities• Problem of multiple leaders recurred• May 30 – 48 probable, 25 suspect cases• Mainly hospitalized patients, HCWs and their
families• Medical student became ill 2 days after completing
quarantine and during obstetrics rotation, leading to quarantine of mothers, newborns and staff

HCW Casualties
• June 30 – Nelia Laroza, nurse, first Canadian HCW to die of SARS
• July 19 – Tecla Lin, nurse, dies of SARS• August 13 – Nestor Yanga, physician, dies
of SARS• HCWs account for 40% of SARS cases in
Toronto outbreak, second only to Vietnam where HCWs accounted for 57% of cases

Communication
• SARS updates on websites of Health Canada, MOHLTC, Toronto Public Health
• Daily SARS televised press conferences• Dr. Donald Low, chief microbiologist at Mount
Sinai, became unofficial leader of SARS battle• Too many talking heads with different views• No coherent communications strategy evident

Research
• March 15 – WHO establishes network of labs to identify SARS agent and succeeds within a month
• March 31 – first scientific papers describing SARS from Hong Kong and Canada appear on New England Journal of Medicine website, and subsequently in Science (genetic sequence of Toronto SARS virus), BMJ, Lancet, JAMA (clinical features)
• July 26 – Lancet paper supporting coronavirus as cause of SARS had patient data from 6 countries

Clinical Challenges
• Non-specific symptoms• No unequivocally effective treatment• No previous clinical experience with it• Single SARS facility versus universal capacity• Learning on the fly: ribavirin. Both clinical
experience and in vitro evidence showed lack of benefit and clinical harm
• The race: by early April, there were already 91 probable and 135 suspect cases and 10 deaths

SARS in Canada
• Outside Asia, Canada hardest hit in world• In Canada, Toronto hardest hit• By August 2003, 438 probable and suspect
cases of SARS, mainly in greater Toronto area
• 44 deaths (all in Toronto)• >100 healthcare workers (HCWs)
developed SARS and 3 died of SARS (2 nurses and 1 physician)

SARS and Death
Case fatality ratios
• Canada: 16.7% of probable SARS cases and 9.3% of suspect and probable cases
• Median age 75 years; 83% > 60 years
• China: 349 deaths among 5,327 suspect and probable cases
• Global case fatality ratio 11%

SARS and Ethical Issues
• Public Health versus Civil Liberties: quarantine• Privacy of Information versus the Public’s Right
to Know: name of index patient released but not name of nurse on GO train
• Duty of Care of Health Professionals and Duty of Support and Protection for them by Institutions
• Collateral Damage: the consequences for non-SARS illnesses
University of Toronto Joint Centre for Bioethics; BMJ 2003; 327: 1342-1344

Ongoing Challenges
• Diagnosis
• Treatment
• Implications of mass outbreak
• Longterm sequelae of SARS and its treatment (early reports of avascular necrosis in 10% of 400 SARS patients in Hong Kong)

Impact on Healthcare Impact on Healthcare Workers – Doing the SARS Workers – Doing the SARS hophop

From the Front Lines• “Nobody ever thought this was the kind of job they
could potentially die from” – ICU nurse• “You cannot appreciate, I don’t believe, what the
feeling of isolation was. Physical isolation…you see nothing but people’s eyes for days on end” – I.D. physician
• “How terrible it is if you have to look after your own colleagues…[when word came down that several children of sick HCWs had come down with the disease] it broke people’s hearts” - MD
• “Emerg would just kind of fall apart because ‘oh no, it’s a staff member’” - nurse

Impact of SARS on HCWs
• Initial unstructured study by Maunder et al:– Concerns re personal safety, familial
transmission and stigmatization– Responses included fear, anxiety, anger and
frustration– Stressors included caring for colleagues as
patients, redeployment to unfamiliar tasks, workload changes
• Maunder R et al. CMAJ 2003; 168: 1245-1251

Impact of SARS on HCWs
• Subsequent cross-sectional, anonymous, self-report survey of HCWs at Mount Sinai Hospital, St. Michael’s Hospital & CAMH
• Data collection: – MSH: May 12-June 8– CAMH: May 22-June 20– SMH: May 13-May 28

Goal
• To identify constructs that may mediate the traumatic responses to the stress of SARS and are open to intervention in similar future outbreaks
• To determine the magnitude of the association of these constructs to outcome

Impact of SARS on HCWs
• Measures:– Impact of Event Scale – a measure of
traumatic stress (Horowitz et al, 1979)– Study of HCWs’ Perception of Risk and
Preventive Measures for SARS (Fones and Koh, 2003) – developed for use in Toronto and Singapore)
– Demographics, attitudes, and contact with SARS patients

Impact of Event Scale
• 15 items probing frequency of attitudes over past week related to a particular stressor (SARS outbreak)
• Items probe intrusive emotions and thoughts as well as avoidance
• Psychometric properties established• Score >19 considered high and of clinical
significance

Results
• 1,601 respondents
• SMH response rate 24%
• MSH/CAMH response rate 10%
• 571 HCWs had IES scores >19, above the cutoff for a stress response syndrome
• This represents 36% of all respondents, and 5% of all HCWs at these facilities

Responders
• Female: 75%• Doctors: 8%• Nurses: 28%• Other allied health professionals: 64%• Mean age: 40 (SD 11)• Mean years of hospital experience: 14.3 (SD
10.6)Sample is representative of staff discipline
distribution at hospitals studied

IES Scores
• No significant difference in mean scores (95% confidence intervals) between groups of HCWs caring for – Cases under investigation (n=72; IES 16-24)– Suspect or probable SARS (n=137; IES 18-23)– Both (n=187; IES 19-23)– These groups were thus collapsed into one
• IES for HCWs who did not care for cases under investigation, suspect or probable significantly lower (n=1207; IES 15-16)

IES Scores and Personal Characteristics
Higher IES scores predicted by:
• Exposure to SARS patients
• Having children• Having 5 or more
years of HCW experience
Higher IES scores NOT predicted by:
• Age• Gender• Marital status
Univariate ANOVA with Bonferroni correction

IES Scores and Professional Role
• Nurse (n=437; IES 19-21)
• MD (n=116; IES 9-13)
• Other HCW professional (SW, OT, RT, etc) (n=175; IES 14-18)
• HCW non-professionals with patient contact (clerical, housekeeping, etc) (n=192; IES 16-21)
• Administration (n=118; IES 13-18)

IES Scores and Ethnoracial Status
• Asian community in Toronto significantly stigmatized during SARS
• Asian HCWs in survey (n=238) reported significantly higher IES scores than caucasian HCWs but did not report higher stigma related to professional professional role; stigma based on ethnoracial status not probed





471539591N =
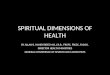
Job stress
highmed.low
Str
ess
sym
pto
ms
(Im
pa
ct o
f E
ven
t)
26
24
22
20
18
16
14
12
10
8

Risk Factors:
1. Care of SARS patients2. Being a nurse3.Having children4.Job stress5.Perceived social rejection6.Avoidance of crowds and colleagues7.Relationship insecurity
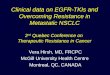
Interpersonal Isolation

number of risk factors
6 or 75432none or 1
% o
f H
CW
s w
ith h
igh
str
ess
sco
re
80
70
60
50
40
30
20
10
0

Mediating Factors
• For HCWs having contact with SARS patients and experiencing emotional distress, the mediating factors were:
1. Fear for own health/health of others
2. Social isolation
3. Increased job stress

Psychosocial effects of SARS on hospital staff (2004)
• 71 patients with SARS (23 of them HCWs) were admitted to Sunnybrook and Women’s College Health Sciences Centre (SWC) and >1,000 patients seen at their outpatient SARS assessment clinic
• Self-administered questionnaire distributed to employees April 10-22, 2003– Demographics, occupation, work history– SARS concerns and SARS precautions– General Health Questionnaire 12-item version (score
>3 = emotional distress/break from normal function) Nickell LA et al, 2004

Responders
• 2001 (27%) of the 7474 staff of SWC responded and 25% of responses included the GHQ
• 79% female• 9% physicians• 26% nurses• 33% allied health professionals• 32% non-clinical staff
This is representative of the hospital staff population as a whole

Concerns about health risks
• Concerns re own health during SARS: 65%
• Concerns re family health during SARS: 63%
• Nurses most frequently concerned: 76%
• Doctors least frequently concerned: 60%
• 94% of those who reported concerns felt they had friends, family, or others to talk to about those concerns

Increased level of concern for personal/family health
Logistic regression analysis identified 4 factors significantly associated with increased level of concern:
1. Perception of greater risk of death from SARS
2. Living with children3. Personal/family lifestyle affected by
SARS4.4. Being treated differently by other Being treated differently by other
people because of working in a hospitalpeople because of working in a hospital

Decreased level of concern for personal/family health
Logistic regression analysis identified 3 factors significantly associated with decreased level of concern:
1.1. Working in a management or Working in a management or supervisory positionsupervisory position
2. Believing precautions were sufficient
3. Being 50 years old or older

Implications of level of concern data
• Being stigmatized has been associated with increased level of concern in other outbreak studies
• Being in a management/supervisory position may provide some real or perceived level of control over a situation that reduces psychosocial effects

Emotional Distress
• Of the 510 GHQ respondents, 29% had scores >3 (more than double the rate in the general adult Canadian population), with highly significant differences between professional groups:– 45% of nurses– 33% of allied health professionals– 17% of physicians– 19% of non-clinical staff
• Study of nurses in 3 Singapore hospitals working under normal normal circumstances, 15% scored >3

Factors associated with Emotional Distress
Regression analysis identified 4 factors as significantly associated with emotional distress:
1. Being a nurse2. Being a part-time employee3. Lifestyle affected by SARS outbreak4. Ability to do one’s job affected by
precautionary measures

Reactions to SARS Precautions
• Workplace precautions were:– Sufficient (74%)– Insufficient (8%)– Don’t know (18%)
• Precautions affect ability to do job:– Yes (42%)– No (58%)

Reactions to SARS Precautions
• Most bothersome precaution:– Mask (70%)
– Access restriction to own hospital (14%)
– All others endorsed by 5% or fewer
• More on masks:– Particularly bothersome (85%)
– Physical discomfort (93%)
– Difficulty communicating (47%)
– Difficulty recognizing people (24%)
– Sense of isolation (13%)

Other Work/Life Implications
• Changes to regular job duties (52%)
• Working overtime (23%)
• Being treated differently because of working in a hospital (28%)
• Personal/family lifestyle impact (38%)

Positive Aspects of SARS
58% felt there were positive outcomes:• Increased awareness of disease control (41%)• Learning experience (26%)• Increased cohesion/cooperation (24%)• Less busy than usual (4%)• Greater appreciation of life and work (2%)• Other (3%; includes cancellation of student exams
and good business for mask and glove companies!)

Psychological Impact of SARS In Asia
• In Singapore, where 238 cases of SARS diagnosed, psychiatric morbidity was present among 21% of HCWs
• In Taiwan, up to 75% of HCWs experienced psychiatric morbidity– Drs. Kang Sim and Hong Choon Chua,
Institute of Mental Health, Woodbridge Hospital, Singapore, 2004

• Increased interpersonal contact– Attention to the interpersonal costs of infection
control protocols
– Extensive 2-way communication by e-mail and other means
– Clear communication of risk and non-risk to community & media to reduce stigma
What would reduce the psychological impact of an outbreak?


• Reduced job stress– Increased mastery
• Increased attention to training and support when redeployment is required
• Dedicated SARS wards
– Attention to workload issues• Including self-imposed!
What would reduce the psychological impact of an outbreak?

What would reduce the psychological impact of an outbreak?
• Reduced job stress– Financial security
• Employees in quarantine or ill
• Families of employees in quarantine or ill
• Part-time employees denied access to 2nd hospital

What would reduce the psychological impact of an outbreak?
• Responsive, protective authority– Clear communication– Response to concerns & questions– Advocacy in community and media


Agenda for Future Research
• Systematic evaluation of psychological impact more broadly on population
• Prospective research to evaluate longitudinal impact
• Rigorous evaluation of outcome of psychosocial interventions

The Future
• Why SARS Will Not Return: A Polemic– Dr. Donald Low, leading Toronto
microbiologist during SARS, CMAJ 2004; 170:
• SARS: Make No Mistake – There Will Be A Next Time– Dr. Alan Bernstein, President, Canadian
Institutes for Health Research, Hospital Quarterly 2003; 6: 21-22