Embed Size (px)
Citation preview

Psychotherapy and Psychosis
Prof Anthony Bateman
Roskilde December 2019

CBT Meta-analyses
CBT for psychosis compared with usual care significantly improved overall
psychotic symptoms (standard mean difference [SMD] -0.33, 95% confidence
interval [CI] -0.45 to -0.21)
positive symptoms overall (SMD -0.34, 95% CI -0.58 to -0.10)
auditory symptoms (SMD 0.39, 95% Cl not reported, P < .005),
delusions (SMD 0.33, 95% CI not reported, P < .05)
negative symptoms (e.g., blunt affect) (SMD -0.32, 95% CI -0.59 to -0.04) at
end of treatment.
No significant differences generally observed for social function, distress
associated with psychosis, relapse, or quality of life.

Cochrane Review of CBT and other
Psychosocial treatments for Psychosis (2018)
Thirty-six randomised controlled trials, randomising in total 3542 people with
schizophrenia to CBT and other psychosocial treatment.
The quality of evidence from these trials is very low to low.
No real differences were found between CBT compared with other psychosocial
treatments for:
Relapse
Rehospitalisation
mental state
Death
social functioning
quality of life.
Results were not robust enough to make firm conclusions.

Relative intervention + carer TAU vs. carer TAU for
psychosis (N=106)
Leavey,
Gulamhussein,
Papadopoulos et
al. Psychol Med
2004

Multiple-family group treatment for
schizophrenia (n=59)
Bradley,
Couchman,
Perlesz et al 2006

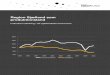
Psychoeducation vs. routine care for patients
with schizophrenia and their families (n=236)
Bauml,
Frobose,
Kraemer et
al., 2006
Rehospitalization rates after 1 year and 2 years (*p < .05)

Psychoeducation vs. routine care for patients
with schizophrenia and their families (n=236)
Bauml,
Frobose,
Kraemer et
al., 2006
Days in hospital after 1 year and 2 years (p < .05)

Family-focused psychoeducational treatment vs
crisis management for bipolar disorder (n=101)
Miklowitz, Simoneau,
George et al 2000

A different approach
to
Treatment

Impairment
Externalizing Internalizing
Male FemaleGendered
Style
Gendered
‘Neurotic’ conditions
Partially gendered
Personality disorder
Ungendered chronic
Psychotic conditions
The ‘P’ Factor (Caspi et al., 2013)

How appraisal shapes our experience
EnoughNot
Except our experience is social: not with physical objects but with people

Appraisal (higher order cognition) theory
Stimulus
Mental representation
Higher order cognition
Emotional response
…but by context-dependent evaluation of motivational relevance

Client
imagined self
representation
Therapist image
of the client self
representation
Client image of the
clinician image of the
client self
representation
Clinician Client
Therapist
image of own
self
representation

Higher Order RepresentationUs/We Representation

Alone
and
Lonely

Loneliness and Schizophrenia
Self-reported annual rates of loneliness among individuals
with schizophrenia and other psychotic disorders (80%) are
approximately 2.3 times higher than those in the general
population (35%) (Aust and NZ National Survey Stain et al 2012)
Loneliness reported as a significant contributor to worse
quality of life in schizophrenia (Roe D, Mashiach-Eizenberg M, Lysaker PH Schizophr
Res. 2011 Sep; 131(1-3):133-8
Individuals with psychotic disorders cite loneliness as one
of the most important challenges in their life, second only
to financial concerns (Morgan VA, et al Aust N Z J Psychiatry. 2017 Feb; 51(2):124-140.)

Social Isolation and Schizophrenia
People with schizophrenia tend to be more socially isolated than
other groups in the population.
Social isolation in turn is linked to higher levels of symptoms, poor
quality of life and worse treatment outcomes.
Specific symptoms may contribute to this social isolation: negative
symptoms can affect motivation and ability to socialise and positive
symptoms can lead to an active avoidance of social situations.
Social isolation may also be driven by social exclusion, prejudice
and a tendency for others to distance themselves.

The perils of isolation: Maintaining social
connections is required for self-
coherence and social isolation kills

Loneliness across the age range in representative sample of men
and women living with or without a partner (Beutel et al., 2017)
BMC Psychiatry, 17-97
n=15,010Prevalence of a feeling of loneliness in the general population of about 10.5%

Depression, anxiety and suicidality predicted by feeling of
loneliness (Beutel et al., 2017)
BMC Psychiatry, 17-97
90% more Depression 20% more Anxiety 30% more Suicidal Ideation

Loneliness and Social Isolation as Risk Factors for Mortality:
A Meta-Analysis (Holt-Lunstad, et al. 2015)
Across 70 studies the weighted average effect sizes for increased mortality:social isolation odds ratio (OR) = 1.29
loneliness OR = 1.26
living alone OR = 1.32
No differences between measures of objective and subjective social isolation
More predictive of death in samples with an average age younger than 65 years.(premature death)
Perspectives on Psychological Science 10(2) 227–237

Mortality in single fathers compared with single mothers
and partnered parents (Chiu et al., 2018)
Lancet Public Health 2018; 3: e115–23
40,000 parents aged 15 years or older,
living in a household with one or more
biological or adopted child < 25
younger than 25 years,

We underestimate importance of
social context e.g. for our health

Holt-Lunstad et al. (2010, p.14):
Physicians, health professionals, educators,
and the public media take risk factors such
as smoking, diet, and exercise seriously;
the data presented here make a compelling
case for social relationship factors to be
added to that list.
PLoS Med. 7, 2–20

The propensity to underestimate the importance of social factors for
health (Haslam et al., 2018)
Social Science and Medicine, 198 14-23

The propensity to underestimate the importance
of social factors for health (Haslam et al 2018)
Social Science and Medicine, 198 14-23
Only 15% of people perceive social factors such as connectedness to others as important to mortality

The ‘we-mode’ in social cognition (Gallotti &
Frith, 2013)
Human sociality is explained by the unique capacity to
share the mental states of others.
when people are poised to interact, they achieve
interpersonal awareness through a ‘meeting’ of minds
Intentional states that are assumed by individuals in the
system to be joint or shared by everyone.
Tuomela (2005) has named this category jointly seeing
to it (jstit).
Feeling of we-ness social collaboration
being part of a set of thoughts and feelings that are
beyond one’s own
minds shared by cognizing in an irreducibly collective
mode of cognition called the we-mode.Trends in Cognitive Sciences April 2013, Vol. 17, No. 4

Do we need to target social adjustment in schizophrenia?

Take Home MessageTreating developing and full-fledged Schizophrenia Spectrum
and other Psychosis related disorders (SSPDs) remains clinically
challenging.
These challenges stem from two main sources: comorbidity and
the symptom-disability gap, with social dysfunction
representing the no.1 clinical frontier.
MBT works on the hypothesis that morbidity associated to
psychotic disorders stem from core self disturbances
(underlying psychopathology).
Preliminary results suggest that MBT may help with the profound
impact of psychotic pathogenesis on interpersonal and social
functioning.

Outline
I. The Developmental Sequence of
Psychosis
I. Traits and States along Psychotic
Pathogenesis
I. MBT and Developing Psychosis

Clinical Trajectory in SSPD
Debbané et al., 2016

Comorbidity
Clinical Challenges in Emerging Psychosis
Symptom - Disability Gap

Clinical Challenges: Comorbidity
Mood disorders
Anxiety Disorders
Alcohol Dependance
Cannabis Dependance
Cocaine
Paranoid
Schizotypal
Schizoid
Borderline
Avoidant
Antisocial
Fusar-Poli et al, 2012, 2014; Armando, Hutsebaut, Debbané, 2019
Requires a clinical
approach which can
tackle comorbidity…
…or the P Factor!
Axis 1 disorders
Personality disorders

The Symptom – Disability Gap
CHR FEP
Social functioning principal cause of poor outcome
Armando, Hutsebaut, Debbané, 2019
- Social dysfunction is present along the clinical continuum (Debbané et al., 2016), and can be
resistant to treatment with antipsychotics or even increase during the course of illness (Carbon & Correll, 2014)
- Social dysfunction may be more invalidating:
-predicts poor vocational outcome (Bell et al., 2009)
-poor quality of life (Penn et al., 1997)
-increased risk of relapse into a psychotic episode (Hafner et al., 1999; Penn and
Roberts, 2006)

What is the nature of the underlying psychopathology sustaining social
dysfunctions in psychotic disorders ?

Working hypothesis: Core self disturbances
Debbané, Salaminios et al., 2016

Psychotic Pre-Mentalizing modes?
Psychotic
Pretend Mode
Hyper-
reflexivity
Psychotic
Pretend Mode
Hyper-
reflexivity
Psychotic
Teleological
Mode
Paranoid
phenomena
Psychotic
Teleological
Mode
Paranoid
phenomena
Psychotic
Psychic
Equivalence
Depersonalizati
on
Psychotic
Psychic
Equivalence
Depersonalizati
on
Experiences of disturbance in core self