Embed Size (px)
Citation preview

DEPRESSION AND ANXIETY 26:279–288 (2009)
Research Article
PSYCHOTHERAPY VERSUS THE COMBINATION OFPSYCHOTHERAPY AND PHARMACOTHERAPY IN THE
TREATMENT OF DEPRESSION: A META-ANALYSIS
Pim Cuijpers, Ph.D.,1� Annemieke van Straten, Ph.D.,1 Lisanne Warmerdam, M.A.,1
and Gerhard Andersson, Ph.D.2,3
Background: A large number of studies have shown that psychologicaltreatments have significant effects on depression. Although several studies haveexamined the relative effects of psychological and combined treatments, this hasnot been studied satisfactorily in recent statistical meta-analyses. Method: Weconducted a meta-analysis of randomized studies in which a psychologicaltreatment was compared to a combined treatment consisting of the samepsychological treatment with a pharmacological therapy. For each of thesestudies we calculated the effect size indicating the difference between thepsychological and the combined treatment. Results: All inclusion criteria weremet by 18 studies, with a total of 1,838 subjects. The mean effect size indicatingthe difference between psychological and combined treatment was 0.35 (95% CI:0.24�0.45; Po0.001), with low heterogeneity. Subgroup analyses indicatedthat the difference between psychological and combined treatments wassignificantly smaller in studies in which cognitive behavior therapy wasexamined. We also found a trend (Po0.1) indicating that the differencebetween psychological and combined treatment was somewhat larger in studiesaimed at specific populations (older adults, chronic depression, HIV patients)than in studies with adults, and in studies in which Trycyclic antidepressants orSSRIs were examined, compared to studies in which a medication protocol oranother antidepressant was used. At follow-up, no difference betweenpsychological and combined treatments was found. Conclusion: We concludethat combined treatment is more effective than psychological treatment alone.However, it is not clear whether this difference is relevant from a clinicalperspective. Depression and Anxiety 26:279–288, 2009. r 2008 Wiley-Liss,
Inc.
Key words: depression; major depression; psychotherapy; combined treatment;meta-analysis
Published online 21 November 2008 in Wiley InterScience (www.
interscience.wiley.com).
DOI 10.1002/da.20519
Received for publication 10 September 2007; Revised 10 February
2008; Accepted 20 March 2008
�Correspondence to: Pim Cuijpers, Ph.D., Professor of Clinical
Psychology, Department of Clinical Psychology, Chair Vrije
Universiteit, Amsterdam, Van der Boechorststraat 1, 1081 BT
Amsterdam, The Netherlands. E-mail: [email protected] of Clinical Psychology and EMGO Institute, VU
University, Amsterdam, The Netherlands2Department of Behavioural Sciences and Learning, Swedish
Institute for Disability Research, Linkoping University, Lin-
koping, Sweden3Department of Clinical Neuroscience, Psychiatry Section,
Karolinska Institutet, Stockholm, Sweden
rr 2008 Wiley-Liss, Inc.

INTRODUCTION
In the past three decades, at least 160 controlled andcomparative studies have examined the effects ofpsychological treatments compared to control condi-tions and to other treatments.[1] This large number ofstudies has clearly shown that most psychologicaltreatments studied in a trial have large effects ondepression. Psychological treatments that have provedeffective include cognitive-behaviour therapy,[2] beha-vioural activation treatments,[3] interpersonal psy-chotherapy,[4] problem-solving treatment[5,6], and lifereview for older adults.[7] These treatments are notonly effective in adults with depression, but also inolder adults,[8] in women with postpartum depres-sion,[9] and in patients with both depression andgeneral medical disorders, including multiple sclero-sis,[10], stroke patients,[11] and cancer patients.[12]
Psychological treatments can be delivered effectivelyin group format, individual format, or guided self-helpformat.[13,14] Probably, the latest contribution to thislist is the provision of treatment via the Internet.[15]
One group of studies has focused on the comparativeeffects of psychological and pharmacological treat-ments. This research has shown that the effects of bothtypes of treatment are comparable.[16] It is also clearthat a combined treatment is somewhat more effectivethan treatment with pharmacotherapy alone.[17,18] It isnot very clear, however, whether combined treatment ismore effective than a psychological treatment alone.Clinicians often have different views on this, inparticular when it comes to more severe depressionwhen combined treatments often are recommended
Although several studies have examined the effects ofcombined treatment, the results are not entirelyconclusive. Some studies find no significant differ-ence.[19–21] whereas others have found that combinedtreatment is significantly more effective than psycho-logical treatment alone.[23,24]There are even a fewstudies found that psychological treatment alone ismore effective than combined treatment.[25,26]
Because it can be expected that the differencebetween psychological and combined treatments aresmall, large sample sizes are required to find significantdifferences. When small effect sizes are expected inindividual studies, meta-analytical techniques can beused to integrate the results of individual studies and toincrease the statistical power. Although several sys-tematic reviews have examined the difference betweenpsychological and combined treatments,[27,28] thisquestion has not been examined in recent statisticalmeta-analyses using up-to-date methods. For example,one meta-analysis conducted in this area has includedonly a small portion of the available studies (8 of the 18studies we have identified, see below.[17] This meta-analysis also focused on several research questions, didnot pool the results of all studies together, and did notfor example conduct subgroup analyses to examine thecharacteristics of the studies, which were related to the
differential effects of the psychological and combinedtreatments. It did, however, find some indications thatcombined treatment was somewhat more effective thanpsychological treatment alone. Another small meta-analysis did examine the comparative effects ofpsychological versus combined treatment,[29] but fo-cused only on the seven studies that examined out-patients. This study also found that combinedtreatment was superior to psychological treatmentalone.
We decided to conduct a new, comprehensive meta-analysis in which all available studies are included. Wewanted to examine whether the small benefit ofcombined treatment, which was found in the earliermeta-analyses,[17,29] would also be found when thenumber of examined studies was increased. Finally, wewanted to examine whether study characteristics wererelated to the relative effects of psychological andcombined treatments.
METHODS
IDENTIFICATION AND SELECTION OF STUDIES
First, we used a large database of studies on the psychologicaltreatment of depression in general. This database has been describedin detail elsewhere.[3,5,6,8] It was developed through a comprehensiveliterature search (from 1966 to December 2007) in which weexamined 7,911 abstracts in Pubmed (1,403 abstracts), Psycinfo(2,097), Embase (2,207), and the Cochrane Central Register ofControlled Trials (2,204). We identified these abstracts by combiningterms indicative of psychological treatment (psychotherapy, psycho-logical treatment, cognitive therapy, behaviour therapy, interpersonaltherapy, counselling, family therapy, marital therapy, problem-solvingtherapy, psychodynamic therapy, psychoanalysis, relaxation, reminis-cence, life review) and depression (both MeSH-terms and textwords).For this database, we also collected the primary studies from 22 meta-analyses of psychological treatment of depression.[1] We retrieved atotal of 857 papers for further study. These papers were studied, andwe selected the ones which examined the relative effects ofpsychological and combined treatments of depression.
Second, references of earlier reviews and meta-analyses wereexamined.[1,16–18,27–28] Finally, the references of retrieved papers werechecked.
We included studies in which (1) a psychological intervention (2)was compared to a combined treatment (3) consisting of the samepsychological intervention plus an antidepressant, (4) in a rando-mized trial, (5) aimed at subjects with depression (as diagnosedthrough a clinical interview and/or a self-report questionnaire).Psychological interventions were defined as treatments in whichverbal communication between a therapist and a client was the coreelement and in which the communication of the therapist is based ona specific theoretical framework about the causes of depression andhow the communication can reduce it. Studies were included when allrandomized participants had a depressive disorder (or scored above acut-off point on a self-report instrument); comorbid general medicalor psychiatric disorders were not used as an exclusion criterion. Nolanguage restrictions or age limits were applied. We excluded studieson maintenance treatments and studies in which a psychologicaltreatment plus placebo were compared to a psychological treatmentplus active antidepressant, because it cannot be ruled out that theplacebo has an effect in itself.
280 Pim Cuijpers et al.
Depression and Anxiety

QUALITY ASSESSMENT
At least 25 scales have been used to assess the validity and qualityof RCTs,[30] but evidence of their reliability and validity is lacking.We adopted the Cochrane Handbook’s 4 criteria,[30] to assess studyvalidity: (1) randomization to conditions conducted by an indepen-dent (third) party; (2) concealment of randomization to conditions;(3) blinding of assessors of outcome; (4) completeness of follow-updata.
ANALYSES
We directly compared the psychological and combined treatmentson depressive symptomatology (continuous outcomes), recovery(dichotomous outcomes), and drop-out.
Effects on depressive symptomatology (continuousoutcomes). We calculated effect sizes indicating the differencebetween psychological and combined treatments. The effect sizes (d)were calculated by subtracting (at post-test) the average score of thepsychological treatment group (Mp) from the average score of thecombined treatment group (Mc) and dividing the result by the pooledstandard deviations of the experimental and control groups (SDpc).An effect size of .5 thus indicates that the mean of the psychologicaltreatment group is half a standard deviation larger than the mean ofthe combined treatment group. Effect sizes of .8 can be assumed to belarge, whereas effect sizes of .5 are moderate, and effect sizes of .2 aresmall.[31] In the calculations of effect sizes, only those instrumentswere used that explicitly measure depression (Table 1). If more thanone depression measure was used, the mean of the effect sizes wascalculated, so that each study (or contrast group) had only one effectsize. When means and standard deviations were not reported, weused other statistics (t-value, p-value) to calculate effect sizes.
To calculate pooled mean effect sizes, we used the computerprogram Comprehensive Meta-analysis (version 2.2.021), developedfor support in meta-analysis. We conducted all analyses using boththe fixed effects model and the random effects model.[25] As anindicator of homogeneity, we calculated the Q-statistic. We alsocalculated the I2-statistic, which is an indicator of heterogeneity inpercentages. A value of 0% indicates no observed heterogeneity, andlarger values show increasing heterogeneity, with 25% as low, 50% asmoderate, and 75% as high heterogeneity.
Subgroup analyses. We examined whether specific charac-teristics of the studies were related to the effect sizes by using theprocedures for subgroup analyses as implemented in ComprehensiveMeta-analysis. In these analyses we used the mixed effects model.This means that the random effects model is used to calculate theeffect size for each subgroup, whereas the fixed effects model tests thedifference between the subgroups of studies.
We conducted subgroup analyses on the selected characteristics ofthe three core elements of the studies: participants, interventions, andstudy characteristics. With regard to the participants we examinedthe recruitment method (clinical samples versus other samples) andtarget group (adults in general versus specific population). We alsoexamined the type of psychological intervention (CBT versus othertypes of psychological treatments) and the type of pharmacologicaltreatment (tricyclics, SSRIs, or other). General characteristics of thestudies we reviewed in subgroup analyses were: drop out rate (lessthan 20% drop-out versus 20% or more drop-out), type of analyses(intention-to-treat analyses versus completers-only analyses), and theperiod in which the study was conducted (before 1995 versus 1995 orlater).
Effects on recovery (dichotomous outcomes). Wecalculated the relative risk (RR) of recovery in subjects receivingpsychological treatment compared to subjects receiving combinedtreatment. Again, we conducted all meta-analyses both with the fixed
effects model and with the random effects model, using theComprehensive Meta-analysis (version 2.2.021) computer program,and we calculated the Q-statistic and the I2-statistic to estimateheterogeneity between study outcomes.
Publication bias. Publication bias was tested by inspectingthe funnel plot on primary outcome measures, and by Duval andTweedie’s trim and fill procedure, which yields an estimate of theeffect size after the publication bias has been taken into account (asimplemented in Comprehensive Meta-analysis, version 2.2.021).
We also calculated ‘‘Orwin’s fail safe N.’’ This number indicateshow many studies with an effect size of zero should be found toreduce the effect size that is found to a lower value (for example, .10).A larger N indicates that the effect size found can be furthergeneralized.
RESULTSDESCRIPTION OF INCLUDED STUDIES
All inclusion criteria were met by 19 studies, with atotal of 1,838 subjects (934 in the psychologicaltreatment groups, and 904 in the combined treatmentgroups). Selected characteristics of these studies aredescribed in Table 1.
Fourteen studies were aimed at adults in general, andfive at specific populations (two at adults with HIV; onefocused on multiple sclerosis patients; one on adultswith chronic depression; and one on older adults).Eleven studies were aimed at clinical populations, six atsubjects recruited from the community, and two didnot report the recruitment method or they usedsystematic screening to recruit patients. In all but onestudy only subjects who met diagnostic criteria for adepressive disorder (including two studies specificallyaimed at patients with dysthymia) were included. Ineight studies, CBT was used as psychological treat-ment. In three studies, amitryptiline was used as theantidepressant medication, in three other studiesimipramine was used, a further three had desipramine,two had fluoxetine, and the remaining 12 used anothermedication or used more than one type of medication.Six studies were conducted before 1990, five between1990 and 1999, and the remaining eight after 2000.Seventeen studies were published in English, one inSpanish, and one in German.
QUALITY OF THE INCLUDED STUDIES
The quality of the studies varied. Only four studiesreported that allocation to conditions was conductedby an independent party. Concealment of randomallocation to respondents was not possible or notreported in any of the studies, whereas blinding ofassessors was reported in 11 studies. Drop-out numbersranged from 6 to 55%.
CONTINUOUS OUTCOMES AT POST-TEST
In 17 studies (19 comparisons), effect sizes could becalculated which indicated the difference betweenpsychological and combined treatments at post-test.
281Research Article: Psychological Versus Combined Treatment of Depression
Depression and Anxiety

TA
BL
E1.
Sel
ecte
dst
ud
ies
of
ran
do
miz
edst
ud
ies
com
par
ing
the
effe
cts
of
psy
cho
logic
altr
eatm
ent
toth
eef
fect
so
fco
mb
ined
trea
tmen
t
Po
pu
lati
on
Psy
cho
logi
cal
trea
tmen
tC
om
bin
edtr
eatm
ent
Stu
dy
Stu
dy
Gen
eral
Rec
rD
efin
itio
nd
epre
ssio
nT
ype
Nse
sN
rsp
AD
Nrs
pM
easu
re-m
ents
Inst
rum
ents
Co
un
try
DO
(%)
Bec
ket
al.
[34]
Ad
ult
sC
om
m1
Cli
nB
DI4
201
HR
SD
414
1D
D(F
C)
CB
T20
18C
BT
1am
itri
pty
lin
e15
Pre
,p
ost
,6,
12
mn
BD
I,H
RS
DU
S24
Bla
ckb
urn
etal
.[3
5]
Ad
ult
sC
lin
MD
D(S
AD
S/
RD
C)
CB
T15
22C
BT
1d
rug
of
cho
ice
22
Pre
,p
ost
BD
I,H
RS
DU
K27
Bro
wn
eet
al.
[36]
Ad
ult
sC
om
DY
ST
(DS
M-I
V/
UM
-CID
I)IP
T10
178
IPT
1S
ertr
alin
e212
Pre
,p
ost
12,
24
mn
MA
DR
S,
CE
S-D
,V
AS
CA
N17
De
Jon
ghe
etal
.[2
2]
Ad
ult
sC
lin
MD
D(D
SM
-IV
)1
HR
SD
12-
24P
sych
od
ynth
er16
106
Psy
cho
dyn
ther
1A
D85
Pre
,p
ost
HR
SD
;S
CL
-90-d
NL
NR
Hau
tzin
ger
etal
.[3
2]
Ad
ult
sC
lin
MD
Do
rD
YS
T1
HD
RS4
201
BD
I4
20C
BT
2470
CB
T1
amit
ryp
tili
ne
68
Pre
,p
ost
12
mn
HR
SD
,B
DI
GE
R3
0
Ho
llo
net
al.
[37]
Ad
ult
sC
lin
MD
D(R
DC
)1
BD
I4
201
HR
SD
414
CB
T20
25C
BT
1im
ipra
min
e25
Pre
,p
ost
HR
SD
,B
DI,
RD
S,
MM
PI-
dU
S4
0
Kel
ler
etal
.[2
4]
Ad
ult
sw
ith
chro
nic
dep
ress
ion
Cli
nM
DD
1d
ysth
OR
recu
rrM
DD
(DS
M-I
V/
SC
ID)
1H
RS
D4
20
CB
AS
P18
228
CB
AS
P1
Nef
azo
do
ne
227
Pre
,p
ost
HR
SD
US
24
Lo
pez
-Ro
dri
guez
etal
.[3
8]
Ad
ult
sC
lin
DD
(DS
M-I
V)
Bel
laks
’p
sych
oth
erN
R10
Bel
laks
’p
sych
oth
er1
flu
oxe
tin
e10
Pre
,p
ost
HR
SD
ME
XN
R
Mar
kow
itz
etal
.[3
9]
Ad
ult
sw
ith
HIV
Co
mm
HR
SD
415
Su
pp
ort
ive
psy
cho
ther
8-16
24S
up
p.
Th
er1
imip
ram
ine
26
Pre
,p
ost
HR
SD
,B
DI
US
32
Mar
kow
itz
etal
.20
05A
du
lts
Co
mm
Dys
thym
ia(S
CID
)IP
T17
23IP
T1
Ser
tral
ine
21
HR
SD
,B
DI,
CD
RS
US
18
Mu
rph
yet
al.
[19]
Ad
ult
sC
lin
MD
D(F
eigh
ner
)1
BD
I4
201
HR
SD
414
CT
20
24
CT
1n
ort
rip
tyli
ne
22
Pre
,p
ost
,1
mn
HR
SD
,B
DI
US
26
Myn
ors
-Wal
lis
etal
.[3
3]
Ad
ult
sC
lin
–G
PM
DD
(RD
C)
PS
T(b
yG
PO
Rn
urs
e)6
391
41P
ST
1fl
uvo
xam
ine
OR
par
oxe
tin
e35
Pre
,p
ost
,1
2m
nH
RS
D,
BD
I,C
ISU
K6
Ro
thet
al.
[40]
Ad
ult
sC
om
mM
DD
(RD
C)
1B
DI
418
1H
RS
D4
15S
elf-
con
tro
lth
er.
1213
Sel
f-co
ntr
ol
ther
.1
des
ipra
min
e13
Pre
,p
ost
,3
mn
HR
SD
,B
DI
US
19
Ru
shan
dW
atki
ns
[41]
Ad
ult
sN
rM
DD
(DS
M-I
II)
1B
DI4
201
HR
SD
414
CB
T20
9C
BT
1A
D7
Pre
,p
ost
HR
SD
,B
DI,
MM
PI-
dU
S1
4
Sch
iffe
ran
dW
atki
ns
[42]
Mu
ltip
lesc
lero
sis
pat
ien
ts
Scr
een
ing
MD
D(S
AD
S/
RD
C)
Bri
ef psy
cho
ther
514
Bri
efp
sych
oth
er1
des
ipra
min
e14
Pre
,p
ost
HR
SD
,B
DI
US
12
Str
avyn
ski,
[43]
Ad
ult
sC
lin
MD
D(D
SM
-III
-R)
1
BD
I4
201
HR
SD
414
Gro
up
CB
T15
12G
rou
pC
BT
1
imip
ram
ine
12
Pre
,p
ost
HR
SD
,B
DI
CA
N25
Th
om
pso
net
al.
[21]
Old
erad
ult
s(4
60ye
ars)
Co
mm
MD
D(S
AD
S/
RD
C)
1
HR
SD
414
1B
DI4
16C
BT
1831
CB
T1
des
ipra
min
e36
Pre
,p
ost
HR
SD
,B
DI
US
30
Wei
ssm
ane
etal
.[4
4]
Ad
ult
sC
lin
MD
D(S
AD
S/
RD
C)
1
RD
S4
7IP
T16
24IP
T1
amit
rip
tyli
ne
24
Pre
,p
ost
RD
SU
S55
Zis
oo
ket
al.
[45]
HIV
pat
ien
tsC
lin
MD
D(D
SM
-III
-R/
SC
ID)
Gro
up
sup
p.
Th
er8
22G
rou
psu
pp
ther
1
flu
oxe
tin
e25
Pre
,p
ost
HR
SD
,B
DI
US
21
1] A
bb
revi
atio
ns
(alp
hab
etic
al):
Act
ivsc
hed
:ac
tivi
tysc
hed
uli
ng;
AD
:an
tid
epre
ssan
tm
edic
atio
n;
AU
S:A
ust
rali
a;C
AN
:Can
ada;
CB
AS
P:
cogn
itiv
eb
ehav
iou
ral-
anal
ysis
syst
emo
fp
sych
oth
erap
y;C
BT
:co
gnit
ive-
beh
avio
ur
ther
apy;
Cli
n:c
lin
ical
recr
uit
men
t;C
om
m:c
om
mu
nit
yre
cru
itm
ent;
DO
:dro
p-o
ut;
GE
R:G
erm
any;
GP
:gen
eral
pra
ctit
ion
er;I
PT
:in
terp
erso
nal
psy
cho
ther
apy;
Mar
ther
:m
arit
alth
erap
y;M
DD
:m
ajo
rd
epre
ssiv
ed
iso
rder
;M
EX
:M
exic
o;
Mn
:m
on
ths;
NL
:T
he
Net
her
lan
ds;
NR
:n
ot
rep
ort
ed;
Nrs
p:
nu
mb
ero
fre
spo
nd
ents
;N
ses:
nu
mb
ero
fse
ssio
ns;
PL
A:
pla
ceb
o;
PS
T:
pro
ble
m-s
olv
ing
ther
apy;
Psy
cho
dyn
:p
sych
od
ynam
ic;
Psy
cho
ther
:p
sych
oth
erap
y;R
ecr:
recr
uit
men
t;S
oc.
skil
lstr
:so
cial
skil
lstr
ain
ing;
Su
pp
:su
pp
ort
;T
her
:th
erap
y;U
K:
Un
ited
Kin
gdo
m;
US
:U
nit
edS
tate
so
fA
mer
ica.
282 Pim Cuijpers et al.
Depression and Anxiety

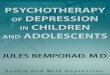
The mean effect size indicating the difference betweenpsychological and combined treatments was .35 (95%CI: .24�.45; Po.001) both in the fixed and the randomeffects model. Heterogeneity was very low (Q 5 15.85n.s.; I2 5 0). The results of these analyses are summar-ized in Table 2 and Figure 1.
Because the weight of one study was very high[21]
(28.50%), we also conducted a meta-analysis in whichthis study was removed. The results were almost thesame (fixed effects and random effects model: d 5 .27;95% CI: .15�.39, Po.001; I2 5 0).
Two studies contained more than one comparison ofa psychological versus a combined treatment.[32,33] Weincluded the four comparisons from these studies inour meta-analysis. Because these comparisons were notindependent of each other, we examined whether thisinfluenced the outcomes. We conducted a new meta-analysis in which only the smallest effect size from eachof these two studies was included, but found that thisscarcely influenced the results (fixed effects andrandom effects model: D 5 0.36; 95% CI: .25�.46;Z 5 6.56, Po.001; Q 5 15.39 n.s.; I2 5 0).
In 15 studies (17 comparisons), the Hamilton RatingScale for Depression (HRSD) was used. When onlythis scale was used for the calculation of the effect sizes,
a mean effect size of .35 (95% CI: .24�.46) was foundwith the fixed effects model, and .31 (95% CI: .18�.45)with the random effects model (with low heterogeneity:Q 5 19.73 n.s.; I2 5 18.91). The fifteen comparisonsusing the Beck Depression Inventory (BDI) resulted ina mean effect size of 0.28 (95% CI: 0.12�0.43), bothwith the fixed and the random effects model (Q 5 9.86,n.s.; I2 5 0).
SUBGROUP ANALYSES
We conducted several subgroup analyses (Table 2).No significant difference was found between the effectsize of studies in which clinically referred patients wereexamined and those in which subjects were recruited inother ways (mostly through community recruitment).We also found no difference between older (o1995)and newer (41995) studies; between studies whichused intention-to-treat analyses and those usingcompleters-only analyses; and between studies with adrop-out rate below 20% and those with a drop-outrate of 20% or higher.
We found a significant difference (Po.05) betweenstudies which used cognitive behavioural interventionand those in which other types of psychological
TABLE 2. Meta-analyses of studies comparing the effects of psychological treatments on depression compared tocombined treatments at post-test: continuous outcomes
Study Ncomp D 95% CI Z Qa I2 P
Overall effectsAll studies Fixed/random effectsb 19 0.35 0.24–0.45 6.67��� 15.85 0All studies without Keller Fixed/random effectsb 18 0.27 0.15–0.39 4.37��� 10.18 0Only HRSD Fixed effects 17 0.35 0.24–0.46 6.24��� 19.73 18.91
Random effects 0.31 0.18–0.45 4.59���
Only BDI Fixed/random effectsb 15 0.28 0.12–0.43 3.55��� 9.86 0Subgroup analysesc
Target group Adults 14 0.24 0.10–0.37 3.49��� 4.06 0 oSpecific groups 5 0.49 0.27–0.71 4.29��� 5.21 23.25
Recruitment Clinical 11 0.39 0.27–0.51 6.31��� 8.46 0 n.s.Other 8 0.24 0.05–0.43 2.53� 5.64 0
Psychological treatment CBT 8 0.15 �0.06–0.37 1.39 1.97 0 �
Other 11 0.40 0.29–0.52 6.82��� 9.95 0Year of publication Before 1995 7 0.22 �0.05–0.49 1.60 2.55 0 n.s.
1995 or later 12 0.35 0.23–0.47 5.62��� 12.35 10.92Drop-out rated o20% 7 0.24 0.06–0.43 2.59� 2.25 0 n.s.
4 20% 10 0.36 0.18–0.53 4.06��� 11.04 18.50Analyses Intention-to-treat 12 0.39 0.26–0.52 6.00��� 11.15 1.34 n.s.
Completers-only 7 0.25 0.08–0.43 2.82�� 3.04 0Medication category Tricyclics 10 0.22 0.02–0.41 2.21� 5.47 0 o
SSRIs 6 0.27 0.08–0.45 2.83�� 3.82 0Other 3 0.49 0.33–0.64 6.10��� 0.94 0
Effects at follow-up3–6 months Fixed 1 randomb 3 �0.15 �0.58–0.27 �0.71 n.s. 0.01 012 months Fixed 1 randomb 5 0.00 �0.26–0.26 0.01 n.s. 1.87 0
o: Po0.10; �Po0.05; ��Po0.01; ���Po 0.001.aThe results for the random effects model and the fixed effects model were identical.bAll subgroup analyses were conducted with mixed effects analyses.cNone of the Q-values was significant (P40.05).dthe two studies in which the drop-out rates were not reported were not included in these analyses.
283Research Article: Psychological Versus Combined Treatment of Depression
Depression and Anxiety

treatments were found (Table 2). For that comparisonthe advantage of combination was less when medica-tion was added to CBT. We also found a trend showingthat studies using tricyclic medications or SSRIs wereused had smaller effect sizes than studies using anothermedication (nefazodone)[24] or more than one type ofmedication.[22,41]
We found a trend (Po.1) indicating a significantdifference between studies aimed at adults withdepression and the effect size of studies targetingspecific populations (two studies on HIV-patients; onestudy on adults with chronic depression, one onpatients with multiple sclerosis, and one study on olderadults).
DICHOTOMOUS OUTCOMESAT POST-TEST
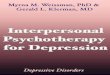
The RR indicating the difference between psycho-logical and combined treatments in recovery was .78(95% CI: .71�0.860; 17 comparisons; Z 5�4.91;Po.001), both in the fixed and the random effectsmodel. Heterogeneity was low (Q 5 12.90; n.s.; I2 5 0).The results of these analyses are summarized in Table 3and Figure 2.
We conducted the same subgroup analyses as withthe continuous outcomes (Table 3). However, none ofthe variables we examined in these analyses resulted ina significant difference between subgroups (includingthe three variables that were found to be significant inthe analyses with the continuous outcomes).
PUBLICATION BIAS
Neither the funnel plots nor Duval and Tweedie’strim and fill procedure pointed at a significantpublication bias. And this was true both in the analyseswith the continuous outcomes and in the analyses withthe dichotomous outcomes. The effect size indicatingthe difference in depressive symptomatology betweenpsychological treatment and combined treatment con-ditions did not change after adjustment for possiblepublication bias (the observed and adjusted d wereidentical), and this was also true for the RR indicatingthe difference between psychological and combinedtreatments.
We then calculated Orwin’s fail-safe N, which is thenumber of studies with an effect size of zero that shouldbe found to reduce the mean effect size (indicating thedifference between psychological and combined treat-ments) to .10; this was found to be 44. The number ofstudies (with an RR of 1) needed to reduce the RR from0.78 to 0.90 was found to be 24.
EFFECTS AT FOLLOW-UP
In seven studies (10 comparisons) the differencebetween psychological and combined treatments atfollow-up were presented. The results of these analysesare presented in Table 2. The follow-up periods rangedfrom 1 month to 2 years. As there was only one studywhich reported the results at 2-year follow-up, thisstudy was not included in the analyses. Nor did weinclude the study in which a follow-up of one monthwas used.
Figure 1. Standardized effect sizes of psychological treatment for depression compared to combined treatment at post-test:Continuous outcomes
284 Pim Cuijpers et al.
Depression and Anxiety

None of the analyses indicated a significant differ-ence between psychological and combined treatmentsat 3–6 months follow-up, and at 12 months follow-up.Because of the small number of comparisons and thedifferences in follow-up periods, we did not analyse theresults at follow-up any further.
DISCUSSION
We found clear evidence that a combined psycholo-gical and pharmacological treatment of depression issuperior to psychological treatment alone in the shortterm. This was true when we pooled different effect
TABLE 3. Meta-analyses of studies comparing the effects of psychological treatments on depression compared tocombined treatments at post-test: Dichotomous outcomes
Study N RR 95% CI Z Qa I2 P
Overall effectsAll studies Fixed/random effectsb 17 0.78 0.71–0.86 �4.91��� 12.90 0
Subgroup analysesc
Target group Adults 13 0.82 0.73–0.92 �3.50��� 8.78 0 n.s.Specific groups 4 0.67 0.55–0.82 �3.81��� 1.43 0
Recruitment Clinical 10 0.78 0.69–0.88 �4.02��� 3.21 0 n.s.Other 7 0.71 0.49–1.02 �1.86 9.68 38.04
Psychological treatment CBT 6 0.85 0.68–1.07 �1.40 5.78 13.44 n.s.Other 11 0.76 0.68–0.85 �4.76��� 6.11 0
Year of publication Before 1995 8 0.83 0.67–1.02 �1.81 6.73 0 n.s.1995 or later 9 0.77 0.68–0.86 �4.61��� 0
Drop-out rated o20% 7 0.80 0.68–0.93 �2.92�� 4.25 0 n.s.420% 9 0.77 0.67–0.90 �3.41�� 8.52 6.06
Analyses Intention-to-treat 10 0.74 0.64–0.85 �4.24��� 6.67 0 n.s.Completers-only 7 0.82 0.72–0.95 �2.69�� 5.06 0
Medication category Tricyclics 9 0.82 0.69–0.98 �2.15� 7.66 0 n.s.SSRIs 5 0.80 0.69–0.94 �2.82�� 2.76 0Other 3 0.70 0.58–0.85 �3.63��� 0.77 0
�Po0.05; ��Po0.01; ���Po0.001.aThe fixed effects model and the random effects model resulted in the same outcomes.bAll subgroup analyses were conducted with mixed effects analyses.cNone of the Q-values was significant.dThe study in which the drop-out rates was not reported, was not included in these analyses.
Study name Outcome Statistics for each study
Beck, 1985 2,08Blackburn, 1981 0,89Browne, 2002 0,81De Jonghe, 2004 0,76Hautzinger, 1996 0,82Hollon, 1992 0,62Keller, 2000 0,69Markowitz, 1998 0,39Markowitz, 2005 0,42Murphy, 1984 0,87Mynors, 2000 A 0,85Mynors, 2000 B 0,89Roth, 1982 0,83Rush, 1981 0,47Schiffer, 1990 0,50Weissman, 1979 0,75Zisook, 1998 0,71
0,78
0,1 0,2 0,5 1 2 5 10
RR lower upper Z p limit limit
RRand 95% CI
Favours COMB Favours PSY
Clinical judgement
> 50% decrease on BDI or HRSD> 40% decrease in MADRS
Remission (HRSD-17 < 7)BDI + HRSD < 9
HRSD < 6HRSD < 8
HRSD < 8
>50% impr + HRSD<7
HRSD < 6HRSD < 7
HRSD < 7BDI < 10
BDI < 9HRSD < 10
RDS < 8CGI-improvement
0,82 5,31 1,54 0,120,64 1,23 -0,71 0,470,67 0,98 -2,11 0,030,52 1,10 -1,47 0,140,57 1,20 -1,00 0,320,31 1,22 -1,39 0,160,55 0,87 -3,12 0,000,14 1,07 -1,82 0,070,17 1,00 -1,97 0,050,52 1,44 -0,55 0,580,57 1,29 -0,75 0,450,60 1,32 -0,56 0,580,34 2,06 -0,40 0,690,17 1,31 -1,44 0,150,15 1,61 -1,16 0,250,46 1,22 -1,15 0,250,41 1,22 -1,23 0,220,71 0,86 -4,91 0,00
Figure 2. Standardized effect sizes of psychological treatment for depression compared to combined treatment at post-test:Dichotomous outcomes
285Research Article: Psychological Versus Combined Treatment of Depression
Depression and Anxiety

sizes, but also when we examined specific outcomemeasures. Heterogeneity was low in these analyses,indicating that the studies, target populations, andinterventions are probably highly comparable to eachother. We found no indication of publication bias, andfail-safe analyses showed that a large number of studieswith no difference would have to be found to reducethe overall effects on a nonsignificant outcome. There-fore, there should be little doubt that there is indeed adifference in effects between psychological and com-bined treatments. Because the effect size indicating thedifference between psychological and combined treat-ments was small to moderate, several individual studiesfailed to find a significant difference, and it is a clearadvantage of a meta-analytic approach that makes itpossible to combine the results of multiple studies andvalidate such small effect sizes.
However, the effect size indicating the differencebetween psychological and combined treatments issmall to moderate. Effect sizes lower than 0.30 areusually considered to be small, and our effect size wasonly just above that threshold (d 5 0.35). Although ourfinding was statistically significant, it is not clearwhether this has any clinical relevance. To obtain anidea of the clinical relevance of these effect sizes, theuse of the binomial effect size display is recom-mended.[46,47] This displays the difference in successrate between the two treatments. When we comparepsychological treatment to combined treatment, thebinomial effect size display (based on d 5 .35) indicatesthat the success rate increases from .41 to .59. Thissuggests that combined treatment is superior for somepatients and that combined treatment should be offeredto patients before psychological treatment alone isconsidered.
However, these results should be considered withcaution. In our study, we did not examine thecomparative effects of pharmacotherapy and combinedtreatment. Several studies have found that combinedtreatment is more effective than pharmacotherapyalone.[21,33,48,49] If this is indeed the case, thencombined treatment should be considered as a firstline treatment, as it is superior to both psychologicaltreatment alone and pharmacological treatment alone.However, if pharmacotherapy appears to be equallyeffective as combined treatment, it may be better toconsider pharmacotherapy first and only offer com-bined treatment when pharmacotherapy alone does notwork. Because many patients prefer psychologicaltreatments and are not willing to take antidepres-sants,[50] psychological treatments (without additionalpharmacotherapy) will remain an important part ofroutine care, even when combined treatments areclearly superior. More (meta-analytic) research isneeded to examine these questions.
One reason why the suggested superiority ofcombined over psychological treatment alone shouldbe considered with caution is that no difference wasfound in the longer term. This is probably at least in
part related to the small number of available effect sizesat follow-up. It does mean that there is currently noevidence that combined treatment is superior topsychological treatment alone in the longer term.
Our findings should also be considered in the light ofthe study’s limitations. First, we found that the qualityof a number of the examined studies was not optimal.Although it is clearly inherent in studies of research onpsychological treatments that it is not possible toconceal to subjects to which condition they areassigned, many studies did not meet other majorquality criteria, such as assignment to conditions byan independent person, and blinding of assessors.Another important limitation of this meta-analysis isthat we were only able to include a relatively smallnumber of studies. Therefore, the results of ouranalyses should be considered very cautiously.
This meta-analysis only reports about averageeffects. However, the average patient does not exist,and it is entirely possible that different types of patientsare best served by different treatment strategies. Onefinding of this study is research on specific populationsfound significantly larger differences between psycho-logical and combined treatments than studies in adultoutpatients. It is possible that psychological treatmentsare less effective in some of these populations, whichincreases the effects of the added pharmacologicaltreatments. But it also possible that the relative effectsof psychological and combined treatments are relatedto severity, chronicity, and comorbid psychiatric orgeneral medical disorder. More research is needed toexamine these issues.
We found a trend indicating that the differencebetween psychological and combined treatments issmaller when cognitive behavioral therapy is usedcompared to other psychological treatments. It couldbe possible that cognitive behavioral treatments havestronger effects than other psychological treatments. Inthat case, the additional value of the pharmacologicaltreatment may be limited. Although there is someevidence that cognitive behavioral treatments are moreeffective than other treatments,[2,51] the evidence iscertainly not conclusive.[52]
Although we did find that combined treatment ismore effective than psychological treatment alone,more research is needed to examine this difference.Further research is called for on the relative efficacy ofpsychological and combined treatments in the longerterm. More basic research is needed required to explorethe mechanisms through which both treatments work.And more clinical research is necessary to examinewhich treatment or combination of treatments iseffective at in the longer term.
REFERENCES1. Cuijpers P, Dekker J. 2005. Psychologische behandeling van
depressie: een systematisch overzicht van meta-analyses. NedTijdschr Geneesk 149:1892–1897.
286 Pim Cuijpers et al.
Depression and Anxiety

2. Gloaguen V, Cottraux J, Cucherat M, Blackburn IM. A meta-analysis of the effects of cognitive therapy in depressed patients. JAffect Dis 1998;49:59–72.
3. Cuijpers P, van Straten A, Smit F. Psychological treatment oflate-life depression: a meta-analysis of randomized controlledtrials. Int J Geriatr Psychiatry 2006a;21:1139–1149.
4. Churchill R, Hunot V, Corney R, et al. A systematic review ofcontrolled trials of the effectiveness and cost-effectiveness ofbrief psychological treatments for depression. Health TechnolAssess 2001;5:35.
5. Cuijpers P, van Straten A, Warmerdam L. Problem solving therapiesfor depression: a meta-analysis. Eur Psychiatry 2007;22:9–15.
6. Cuijpers P, van Straten A, Warmerdam L. Behavioral treatmentof depression: a meta-analysis of activity scheduling. Clin PsycholRev 2007;27:318–326.
7. Bohlmeijer E, Smit F, Cuijpers P. Effects of reminiscence andlife-review on late-life depression: a meta-analysis. Int J GeriatrPsychiatry 2003;18:1088–1094.
8. Cuijpers P, van Straten A, Smits N, Smit F. Screening and earlypsychological intervention for depression in schools: systematicreview and meta-analysis. Eur Child Adol Psychiatry2006b;15:300–307.
9. Lumley J, Austin MP, Mitchell C. Intervening to reducedepression after birth: A systematic review of the randomizedtrials. Int J Technol Assess Health Care 2004;20:128–144.
10. Mohr DC, Goodkin DE. Treatment of depression in multiplesclerosis: review and meta-analysis. Clin Psychol Sc Pract1999;6:1–9.
11. Hackett ML, Anderson CS, House AO. Interventions fortreating depression after stroke. Cochrane Database of Systema-tic Reviews Issue 2004;2 Art No: CD003437pub2. DOI: 101002/14651858CD003437pub2.
12. Sheard T, McGuire P. The effect of psychological interventionson anxiety and depression in cancer patients: results of two meta-analyses. Br J Cancer 1999;80:1770–1780.
13. McDermut W, Miller IW Brown RA. The efficacy of grouppsychotherapy for depression: A meta-analysis and review of theempirical research. Clin Psychol Sc Pract 2001;8:98–116.
14. Cuijpers P. Bibliotherapy in unipolar depression. J Behav TherExp Psychiatry 1997;28:139–147.
15. Spek V, Cuijpers P, Nyklıeek I, Riper H, Keyzer J, Pop V.Internet-based cognitive behavior therapy for mood and anxietydisorders: a meta-analysis. Psychol Med 2007;37:319–328.
16. Robinson LA, Berman JS, Neimeyer RA. Psychotherapy for thetreatment of depression: a comprehensive review of controlledoutcome research. Psychol Bull 1990;108:30–49.
17. Friedman MA, Detweiler-Bedell JB, Leventhal HE, Horne R,Keitner GI, Miller IW. Combined psychotherapy and pharma-cotherapy for the treatment of major depressive disorder. ClinPsychol Sc Pract 2004;11:47–68.
18. Pampanolla S, Bollini P, Tibaldi G, Kupelnick B, Munizza C.Combined pharmacotherapy and psychological treatment fordepression; a systematic review. Arch Gen Psychiatry 2004;61:714–719.
19. Murphy GE, Simons AD, Wetzel RD, Lustman PJ. Cognitivetherapy and pharmacotherapy singly and together in thetreatment of depression. Arch Gen Psychiatry 1984;41:33–41.
20. Schmitz JM, Averill P, Stotts AL, Moeller FG, Rhoades HM,Grabowski J. Fluoxetine treatment of cocaine-dependent patientswith major depressive disorder. Drug Alc Dep 2001;63:207–214.
21. Thompson LW, Coon DW, Gallagher-Thompson, D, SommerBR, Koin D. Comparison of desipramine and cognitive/behavioraltherapy in the treatment of elderly outpatients with mild-to-moderate depression. Am J Geriatr Psychiatry 2001;9:225–240.
22. De Jonghe F, Hendricksen M, van Aalst G, et al. Psychotherapyalone and combined with pharmacotherapy in the treatment ofdepression. Br J Psychiatry 2004;185:37–45.
23. Ravindran AV, Anisman H, Merali Z, Charbonneau Y, Telner J,Bialik RJ, et al. Treatment of primary dysthymia with groupcognitive therapy and pharmacotherapy: clinical symptoms andfunctional impairments. Am J Psychiatry 1999;156:1608–1617.
24. Keller MB, McCullough JP, Klein DN, et al. A comparison ofnefazodone, the cognitive behavioral-analysis system of psy-chotherapy, and their combination for the treatment of chronicdepression. New Engl J Med 2000;342:1462–1470.
25. Hersen M, Bellack AS, Himmelhoch JM, Thase ME. Effects ofsocial skills training, amitriptyline, and psychotherapy inunipolar depressed women. Behav Ther There;15:21–40.
26. Friedman AS. Interaction of drug therapy with marital therapy indepressive patients. Arch Gen Psychiatry 1975;32:619–637.
27. Wexler BE, Cicchetti DV. The outpatient treatment of depres-sion implications of outcome research for clinical practice.J Nerv Ment Dis 1992;180:277–286.
28. Jindal RD, Thase ME. Integrating psychotherapy and pharma-cotherapy to improve outcomes among patients with mooddisorders. Psychiatr Serv 2003;54:1484–1490.
29. De Maat S, Dekker J, Schoevers RA, de Jonghe F. Relative efcacyof psychotherapy and combined therapy in the treatment ofdepression:a meta-analysis. Eur Psychiatry 2007;22:1–8.
30. Higgins JPT, Green S. Cochrane Handbook for SystematicReviews of Interventions 4.2.6 [updated September 2006]. In:The Cochrane Library, Issue 4, 2006. Chichester, UK: JohnWiley & Sons, Ltd; 2006.
31. Cohen J. Statistical Power Analysis for the Behavioral Sciences.2nd ed. Hillsdale, NJ: Erlbaum;1988.
32. Hautzinger M, de Jong-Meyer R, Treiber R, Rudolf,GAE, Thien U. Wirksamkeit Kognitiever Verhaltenstherapie,Pharmakotherapie und deren Kombination bei nicht-endogenen,unipolaren Depressionen. Zeitschr Klin Psychol 1996;25:130–145.
33. Mynors-Wallis, LM, Gath DH, Day A, Baker F. Randomisedcontrolled trial of problem solving treatment, antidepressantmedication, and combined treatment for major depression inprimary care. BMJ 2000;320:26–30.
34. Beck AT, Hollon SD, Young JE, Bedrosian RC, Budenz D.Treatment of depression with cognitive therapy and amitripty-line. Arch Gen Psychiatry 1985;42:142–148.
35. Blackburn IM, Bishop S, Glen AI, Whalley LJ, Christie JE. Theefficacy of cognitive therapy in depression: a treatment trial usingcognitive therapy and pharmacotherapy, each alone and incombination. Br J Psychiatry 1981;139:181–189.
36. Browne G, Steiner M, Roberts J, et al. Sertraline and/orinterpersonal psychotherapy for patients with dysthymic disorderin primary care: 6-month comparison with longitudinal 2-yearfollow-up of effectiveness and costs. J Affect Dis 2002;68:317–330.
37. Hollon SD, DeRubeis RJ, Evans MD, et al. Cognitive therapyand pharmacotherapy for depression: singly and in combination.Arch Gen Psychiatry 1992;49:774–781.
38. Lopez Rodriguez J, Lopez Butron MA, Vargas Terrez BE,Salcedo V. Estudio doble ciego con antidepresivo, psicoterapiabreve y placebo en pacientes con depresion leve a moderada.Salud Mental 2004;27:53–61. [Double blind study with anti-depressant, brief psychotherapy and placebo in patients with mildto moderate depression]
39. Markowitz JC, Kokcis JH, Fishman B, et al. Treatment ofdepressive symptoms in human immunodeficiency virus —positive patients. Arch Gen Psychiatry 1998;55:452–457.
287Research Article: Psychological Versus Combined Treatment of Depression
Depression and Anxiety

40. Roth D, Bielski R, Jones M, Parker W, Osborn G. A comparisonof self-control therapy and combined self-control therapy andanti-depressant medication in the treatment of depression. BehavTher 1982;13:133–144.
41. Rush AJ, Watkins JT. Group versus individual cognitive therapy:a pilot study. Cogn Ther Res 1981;5:95–103.
42. Schiffer RB, Wineman NM. Antidepressant pharmacotherapy ofdepression associated with multiple sclerosis. Am J Psychiatry1990;147:1493–1497.
43. Stravynski A, Verreault R, Gaudette G, Langlois R, Gagnier S,Larose M. The treatment of depression with group behavioural-cognitive therapy and imipramine. Can J Psychiatry1994;39:387–390.
44. Weissman MM, Prusoff BA, Dimascio A, Neu C, Goklaney M,Klerman GL. The efficacy of drugs and psychotherapy in thetreatment of acute depressive episodes. Am J Psychiatry1979;136:555–558.
45. Zisook S, Peterkin J, Goggin KJ, Sledge P, Atkinson JH, Grant I.Treatment of major depression in HIV-seropositive men. J ClinPsychiatry 1998;59:217–224.
46. Rosenthal R, Rubin DB. A simple, general purpose display ofmagnitude of experimental effect. J Educ Psychol 1982;74:166–169.
47. Rosenthal R. How are we doing in soft psychology? Am Psychol1990;45:775–777.
48. De Mello MF, Myczcowisk LM, Menezes PR. A randomizedcontrolled trial comparing moclobemide and moclobemideplus interpersonal psychotherapy in the treatment ofdysthymic disorder. J Psychother Pract Res 2001;10:117–123.
49. Macaskill ND, Macaskill A. Rational-emotive therapy pluspharmacotherapy versus pharmacotherapy alone in the treatmentof high cognitive dysfuntion depression. Cogn There Res1996;20:575–592.
50. Bedi N, Chilvers C, Churchill R, Dewey M, Duggan C, FieldingK. Assessing effectiveness of treatment of depression in primarycare: Partially randomised preference trial. Br J Psychiatry2000;177:312–318.
51. Gaffan EA, Tsaousis I, Kemp-Wheeler SM. Researcher alle-giance and meta-analysis: the case of cognitive therapy fordepression. J Consult Clin Psychol 1995;63:966–980.
52. Wampold BE, Minami T, Baskin TW, Callen Tierney S.A meta-(re)analysis of the effects of cognitive therapyversus ’other therapies’ for depression. J Affect Dis 2002;68:159–165.
288 Pim Cuijpers et al.
Depression and Anxiety