Embed Size (px)
Citation preview

Pubh 8482: Sequential Analysis
Joseph S. Koopmeiners
Division of BiostatisticsUniversity of Minnesota
Week 9

Course Summary
To this point...
• We have focused on sequential testing of a statistical hypothesis• We discussed sequential tests that have the same type-I error
rate and power as a fixed-sample test but smaller expectedsample size
• We then illustrated how inference is impacted by utilizing asequential testing procedure and we discussed approaches toinference after a group sequential test

Group Sequential Designs
• Group sequential methods are most often applied to large,confirmatory trials:
• After the safety of the new drugs has been carefully studied• The drugs biological mechanism is well-understood• We have a good understanding of what patients will most benefit
from the new drug
• In this case, our primary goal is to evaluate the new drug asquickly and efficiently as possible

Adaptive Designs
• In early phase designs, we are interested in a broader class ofmore basic questions
• Is the new drug safe?• What is the correct dose?• Who most benefits from the new drug?• How should the drug be administered?
• This motivates the use of a broader class of adaptive designs

Sequential vs. Adaptive Designs
• An adaptive design is a design that uses accumulating data fromthe ongoing trial to modify certain aspects of the study
• A sequential testing procedure is an example of an adaptivedesign
• We adapt the sample size based on interim analyses• More generally, we might consider adapting any number of
design features• Treatment dose• Randomization ratio• Study arms

Characteristics of Adaptive Designs
• Adaptive designs can be flexibly designed to accommodate awide variety of research questions
• The primary purpose of a clinical trial will be determined by thephase of drug development
• For the remainder of the semester, I will present an overview ofadaptive designs throughout the drug development process

Phases of Drug Development
• Phase 1: Safety trials• Phase 2: Efficacy trials• Phase 3: Confirmatory trials• Phase 4: Post-marketing surveillance

Phase 1 Clinical Trials
• Phase 1: Safety trials• Phase 2: Efficacy trials• Phase 3: Confirmatory trials• Phase 4: Post-marketing surveillance

Goals of Phase 1
• Establish safety profile of a new drug• Determine appropriate dosing for future studies• pharmacokinetics and pharmacodynamics

Safety
• The primary objective of a phase 1 clinical trial is to evaluate thesafety of a novel treatment
• Phase 1 clinical trials are often first-in-human trials and,therefore, the safety profile is unknown at the beginning of thetrial
• The goal is to determine if a safe dose exists

Dosing
• The efficacy of a novel agent will be evaluated through asequence of clinical trials after the completion of phase I
• Therefore, a secondary objective in phase 1 is to identify thecorrect dose for future clinical trials
• This is often the highest dose with acceptable toxicity• In some cases, we may choose a lower for future study from
among the set of doses with acceptable toxicity

pharmacokinetics and pharmacodynamics
• Phase 1 studies are often first-in-human trials• Prior to phase 1, we have little understanding as to how the drug
will be metabolized in the body• A secondary aim of phase 1 trials is to study the
pharmacokinetics and pharmacodynamics of a novel agent• pharmacokinetics: what the body does to the drug as it moves
through the body• pharmacodynamics: what the drug does to the body
• These are not clinical endpoints but provide useful informationfor understanding the basic biology of the new agent

Phase 1 Trials in Oncology
• We will use phase 1 clinical trials in oncology as the motivationfor this discussion
• Healthy volunteers are used when a new drug is expected to berelatively nontoxic
• Cytotoxic agents are known to beextremely toxic• Phase 1 oncology trials enroll patients for whom standard
treatments have failed instead of healthy volunteers

Patients vs. Health Volunteers
• Our primary motivation for running a clinical trial is to answer ascientific question
• We obviously would like to limit the number of subjectsexperiencing toxicities but we also have the responsibility ofproviding the best treatment available for subjects in the trial
• In this sense, there are two additional, competing objectives inphase 1 oncology trials:
• Limit toxicities• Maximize the number of patients that receive a therapeutic dose

The dose-toxicity curve
• We are interested in the probability of dose limiting toxicity (DLT)for each dose
• In general, we can assume that the probability of DLT increaseswith dose
• Traditionally, we assume that the probability of response alsoincreases with dose
• Goal is to find the maximum tolerated dose (MTD): Highest dosewith probability of DLT less than some pre-specified cut-off(usually 0.2 or 0.33)

The dose-toxicity curve
1 2 3 4 5
0.0
0.2
0.4
0.6
0.8
1.0
Dose Level
Pro
b(D
LT)
1 2 3 4 50.
00.
20.
40.
60.
81.
0
Dose Level
Pro
b(D
LT)

The dose-toxicity curve
• Scenario 1:• If maximum acceptable probability of DLT = 0.20, MTD = dose 3• If maximum acceptable probability of DLT = 0.20, MTD = dose 4
• Scenario 2:• MTD is dose 2 in both cases

How do we find the MTD?
• Ideally, we would complete a randomized trial to identify the MTD
• Randomize subjects to one of several dose levels• Estimate the probability of DLT at each dose level• Use estimated probabilities of DLT to identify the MTD
• In general, this is considered far too dangerous for afirst-in-humans study

Dose escalation Studies
• Instead, most phase I clinical trials are dose escalation studies• In a dose escalation study, the initial subjects are treated at the
lowest dose level and subsequent subjects are treatment atprogressively higher dose levels
• This process is continued until the MTD is identified• How should we design a dose-escalation study to identify the
MTD?

Classes of dose-escalation studies
• Phase I dose-escalation studies can be broadly classified asfollows:
• rule-based designs: dose escalation proceeds following apre-defined algorithm until the MTD is identified
• model-based designs: a statistical model is specified for theprobability of DLT and parameter estimates are used to guide doseescalation and identify the MTD

3+3 design
• The most popular rule-based design is the 3+3 proposed byStorer (1989)
• The 3+3 design enrolls subjects in cohorts of 3 and the doseescalates until we observe a dose with at least 2 DLTs out of 6subjects
• The MTD is the highest dose level with < 2/6 DLTs

3+3 design: basic algorithm
• Step 1: Enter first cohort of 3 patients at the lowest dose• Step 2: Observe toxicity outcomes
• if 0/3 DLT, treat next cohort of 3 patients at next highest dose• if 1/3 DLT, treat next cohort of 3 patients at same dose
• if 1/3 + 0/3 DLT, treat next cohort of 3 patients at next highest dose• if 1/3 + 1/3 DLT,define dose as MTD• if 1/3 + 2/3 or 3/3 DLT, dose exceeds MTD
• if 2/3 or 3/3 DLT, dose exceeds MTD
• Step 3: Repeat until MTD is reached.• Step 4: MTD is defined as a dose with ≤ 2/6 DLT

3+3 example
• Cohort 1: dose level 1, 0/3 DLT• Cohort 2: dose level 2, 0/3 DLT• Cohort 3: dose level 3, 1/3 DLT• Cohort 4: dose level 3, 0/3 DLT• Cohort 5: dose level 4, 2/3 DLT
Conclude that dose level 3 is the MTD

3+3 extensions
• The 3+3 has been modified over time to accommodate a varietyof settings:
• 2+4 design• 3+3+3 design• rolling 6 design
• In addition, an “expansion” cohort is often enrolled for PK and PD

Pros and Cons of the 3+3 design
• Pros• Simple!
• Cons• ad hoc• imprecise• only allows for a target DLT probability of .33• treats a maximum of 6 patients at the MTD

Continual Reassessment Method
• The continual reassessment method (CRM) was the firstBayesian adaptive phase 1 design (O’Quigley, Pepe and Fisher,1990)
• The CRM uses a simple, usually one-parameter, parametricmodel for the probability of DLT at each dose
• Dose escalation and MTD are determined by posteriordistributions for the probability of DLT at each dose

Probability of DLT: Power model
Let p(dj)= P
(DLT |dose = dj
), for j = 1, . . . , J
p(dj)= dexp(a)
j
where (d1, . . . ,dJ) is a pre-specified “skeleton” for the probability ofDLT at each dose

Probability of DLT: Hyperbolic tangent model
Let p(dj)= P
(DLT |dose = dj
), for j = 1, . . . , J
p(dj)=
(exp
(dj)
exp(dj)+ exp
(−dj
))a
where (d1, . . . ,dJ) are standardized doses.

Probability of DLT: Logistic model
Let p(dj)= P
(DLT |dose = dj
), for j = 1, . . . , J
p(dj)=
exp(α+ βdj
)1 + exp
(α+ βdj
)where (d1, . . . ,dJ) are standardized doses. In some cases, α is fixedat -3, otherwise, this is a two-parameter model.

Estimating the probability of DLT for each dose
As a model based method, we are able to estimate the probability ofDLT for each dose using standard Bayesian methods. Assuming priordistribution, π (a),
π (a|~y) ∝ L (~y |a)π (a) ,
where,
L (~y |a) =n∏
i=1
p (di)yi (1− p (di))
1−yi .
The posterior is generally not available in closed form and must beestimated using numerical methods (i.e. MCMC)

CRM algorithm
• Step 1: Assume a vague or fully non-informative prior for a• Step 2: Treat 1 patient at the level closest to the current estimate
of MTD• Step 3: Observe toxicity outcome• Step 4: Update posterior for a• Step 5: Treat next patient at the level closest to the current
estimate of MTD based on posteior for a• Step 6: Repeat 1-5 until maximum sample size is reached

CRM Example
• Consider a phase I clinical trial with 5 dose levels• We will model the probability of DLT using the power model with
skeleton(0.1,0.2,0.3,0.5,0.65)
• We will use a vague normal priori for a• The first subject will be enrolled at dose level 3 and we will
continue until 20 subjects have been enrolled• The maximum acceptable probability of toxicity is 0.30

CRM Example
5 10 15 20
01
23
45
subject
dose
x
x
x x x

CRM Example
• The final estimates of the probability of DLT are• Dose 1: 0.048• Dose 2: 0.219• Dose 3: 0.409• Dose 4: 0.701• Dose 5: 0.841
• Declare dose 2 the MTD• 15 subjects treated at MTD• 5 total toxicities

3+3 vs. CRM
• Traditional concepts of type-1 error rate and power do not applyin phase 1 clinical trials
• Instead, designs are compared by considering the followingquantities:
• probability of correctly identifying the MTD• number or percent of subjects experiencing DLT• total sample size

3+3 vs. CRM
• It is not usually possible to evaluate the CRM or 3+3 analytically• Instead, we evaluate the operating characteristics of our design
using simulation• We simulate the trial under a variety of scenarios and compute
the empirical operating characteristics• The following simulation results are from Berry, Carlin, Lee and
Muller (2011)

3+3 vs. CRM: Scenario 1
Dose Ave %1 2 3 4 5 N DLT
P (DLT ) 0.05 0.15 0.30 0.45 0.603+3 %MTD 20.5 42.7 27.5 5.7 0.0 15.2 21.1
%patients 26.0 32.5 27.2 12.1 2.3CRM %MTD 1.0 21.4 52.4 23.0 2.2 18.5 27.0
%patients 15.6 24.1 34.7 19.0 6.7

3+3 vs. CRM: Scenario 2
Dose Ave %1 2 3 4 5 N DLT
P (DLT ) 0.05 0.10 0.20 0.30 0.503+3 %MTD 9.5 28.5 33.0 21.1 0.0 16.9 18.3
%patients 21.6 25.7 26.4 18.9 7.3CRM %MTD 0.1 6.4 25.6 49.4 18.5 18.6 25.7
%patients 13.0 13.2 23.3 30.4 20.2

3+3 vs. CRM: Scenario 3
Dose Ave %1 2 3 4 5 N DLT
P (DLT ) 0.15 0.30 0.45 0.60 0.853+3 %MTD 65.4 27.9 6.3 0.4 0.0 11.6 27.0
%patients 43.9 36.4 16.3 3.2 0.2CRM %MTD 24.5 52.8 19.9 2.8 0.1 18.5 28.7
%patients 40.5 35.4 17.7 6.1 0.3

3+3 vs. CRM: Summary
• The CRM correctly identifies the MTD more often than 3+3• The CRM treats more patients at the MTD than 3+3• The CRM requires a larger sample size than 3+3• The CRM is more likely to overdose, resulting in a higher rate of
DLTs

Modifications to the CRM
The standard CRM dose-escalation can be too aggressive. Thefollowing modifications have been suggested as as remedy:
• Start at the lowest dose and do not skip untried doses• Treat patients in cohorts greater than 1 (2 or 3)• No dose escalation until all treatment in patients from previous
doses are completed• More aggressive stopping rules for safety

Modified CRM Example
• Consider a phase I clinical trial with 5 dose levels• We will model the probability of DLT using the power model the
same skeleton as before
(0.1,0.2,0.3,0.5,0.65)
• We will use a vague normal priori for a• We will enroll subjects in cohorts of 3, starting at dose 1 and we
will not skipped untried dose levels when escalating• The maximum sample size will be 30 (i.e. 10 cohorts) and the
maximum acceptable probability of toxicity is 0.30

CRM Example
0
1 0
0 0 1 0 0 1 2
2 4 6 8 10
01
23
45
cohort
dose

CRM Example
• The final estimates of the probability of DLT are• Dose 1: 0.007• Dose 2: 0.086• Dose 3: 0.235• Dose 4: 0.562• Dose 5: 0.755
• Declare dose 3 the MTD• 21 subjects treated at MTD• 5 total toxicities

Modified CRM: Scenario 1
Dose Ave %1 2 3 4 5 N DLT
P (DLT ) 0.05 0.15 0.30 0.45 0.603+3 %MTD 20.5 42.7 27.5 5.7 0.0 15.2 21.1
%patients 26.0 32.5 27.2 12.1 2.3CRM %MTD 1.0 21.4 52.4 23.0 2.2 18.5 27.0
%patients 15.6 24.1 34.7 19.0 6.7M-CRM %MTD 1.5 22.6 49.8 23.7 2.4 19.0 23.3
%patients 21.3 31.4 29.1 15.8 2.5

Modified CRM: Scenario 2
Dose Ave %1 2 3 4 5 N DLT
P (DLT ) 0.05 0.10 0.20 0.30 0.503+3 %MTD 9.5 28.5 33.0 21.1 0.0 16.9 18.3
%patients 21.6 25.7 26.4 18.9 7.3CRM %MTD 0.1 6.4 25.6 49.4 18.5 18.6 25.7
%patients 13.0 13.2 23.3 30.4 20.2M-CRM %MTD 0.2 5.5 25.4 48.3 20.5 19.1 20.8
%patients 19.3 19.8 25.2 25.2 10.5

Modified CRM: Scenario 3
Dose Ave %1 2 3 4 5 N DLT
P (DLT ) 0.15 0.30 0.45 0.60 0.853+3 %MTD 65.4 27.9 6.3 0.4 0.0 11.6 27.0
%patients 43.9 36.4 16.3 3.2 0.2CRM %MTD 24.5 52.8 19.9 2.8 0.1 18.5 28.7
%patients 40.5 35.4 17.7 6.1 0.3M-CRM %MTD 23.6 53.7 19.6 3.0 0.1 18.5 27.3
%patients 41.5 39.0 15.3 4.1 0.1

Modified CRM: Summary
• The modified CRM reduces the rate of DLTs to a rate similar to3+3
• The modified CRM correctly identifies the MTD more likely than3+3
• The modified CRM treats fewer patients at the MTD than theoriginal CRM

Advantages of CRM vs. 3+3
• In general, the CRM is more likely to find the true MTD than 3+3• Can be adapted for target probabilities other than .33• Model-based methods uses all date to model the dose-toxicity
curve• Treats more patients with doses close to the MTD (i.e. patients
more likely to receive efficacious dose)

Disadvantages of CRM vs. 3+3
• More complicated (for clinicians, at least)• Model misspecification is a potential concern

Model Miss-specification in the CRM
• One of the primary concerns about model-based designs inphase 1 is model miss-specification
• Model-based phase 1 designs usually rely on fully parametricmodels for the probability of DLT
• This will be optimal if the model is correct but our estimates canbe badly biased if the model is incorrect
• In general, we are not able to perform model diagnostics duringan adaptive clinical trial
• How do we address this problem?

Accounting for model miss-specification
• Several authors have proposed model-based phase 1 designsthat are robust to model miss-specification
• Gasparini and Eisele (2000) proposed a curve-free method thatonly assumes that the probability of DLT increases with dose
• Yin and Yuan (2009) proposed a Bayesian model averageapproach that averages over several different skeletons using thepower model
• In both cases, their results are robust to miss-specification withonly a small loss of efficiency when the model is correct

CRM Extensions
• One advantage to model-based designs is that they can beeasily extended to more complicated scenarios
• In general, a Bayesian adaptive phase 1 design requires thefollowing:
• A parametric probability model• An algorithm for adapting the dose level throughout the study
• We will consider the two following extensions:• The two competing outcomes of efficacy and toxicity• Combination therapy

Limitations to Standard Phase I Trials
• Standard Phase I designs only consider toxicity• In this case, we are assuming that the probability of DLT and the
probability of response increases with dose• This may not be a reasonable assumptions in all cases
• MTD has unacceptable efficacy• Efficacy does not continue to increase as dose increases

Simultaneously Considering Efficacy and Toxicity
• An alternate approach is to simultaneously consider efficacy andtoxicity
• In this case, dose-finding is guided by considering the trade-offbetween efficacy and toxicity
• This allows us to identify situations where the MTD hasinadequate efficacy or when efficacy does not continue toincrease as dose increases
• This requires the following:• A bivariate probability model for efficacy and toxicity• A dose-finding algorithm that considers an efficacy/toxicity trade-off

Outcomes
• We will now consider two, binary outcomes• Toxicity: YT - DLT, defined as before• Efficacy: YE - usually defined as tumor response
• Define the following two marginal probabilities• Let πT (x , θ) be the marginal probability of DLT at dose x• Let πE (x , θ) be the marginal probability of response at dose x

Modeling the marginal probabilities
• Toxicity and efficacy are thought to be positively correlated• Therefore, we must specify a joint probability distribution that
allows for correlation between YT and YE
• This is usually accomplished using a copula model• A copula model specifies a joint distribution on the unit square
and uses the fact that Fx (x) is a uniform random variable todevelop a joint density for any two random variables
• Several different copula models have been used for specifyingjoint models for YT and YE

Arnold and Strauss Copula
• Braun (2002) models YT and YE jointly using the copulaspecified by Arnold and Straus
πT ,E = k (πT , πE , ψ)πyTT (1 − πT )
1−yT πyEE (1 − πE)
1−yE ψyT yE (1 − ψ)1−yT yE

Properties of the Arnold and Strauss Copula
• ψ/ (1− ψ) is the odds ratio between yT and yE
• yT and yE are independent if ψ = 1/2• In this specification, πT and πE are no longer the marginal
probabilities of YT and YE
• Instead, πT is the conditional probability of YT conditional onYE = 0 and vice-versa

Gumbel Copula
• Thall and Cook (2004) model the joint probability of YT and YEusing the Gumbel Copula
πT ,E = πyEE (1 − πE )
1−yE πyTT (1 − πT )
1−yT +(−1)yE +yT πE (1 − πE )πT (1 − πT )eψ − 1eψ + 1

Properties of the Gumbel Copula
• ψ characterizes the correlation between efficacy and toxicity• ψ = 0 indicates that efficacy and toxicity are independent• πE and πT retain their original interpretations

Estimating the parameters
The likelihood, L (YE ,YT |x , θ), for a patient at dose x is
π1,1 (x , θ)YE YT π1,0 (x , θ)YE (1−YT ) π0,1 (x , θ)(1−YE )YT π0,0 (x , θ)(1−YE )(1−YT )
• Specify priors for all parameters• Proceed with standard Bayesian inference using MCMC

Identifying the optimal dose
• We must now consider and efficacy/toxicity trade-off to identifythe optimal dose
• This is far more complicated than identifying the MTD in astandard phase I design
• Several approaches for considering this trade-off have beendiscussed in the literature

Identifying the optimal dose: Euclidean Distance
• Braun (2002) considered the euclidean distance between theestimated probability of efficacy and toxicity and targetprobabilities of efficacy and toxicity
dj =
√(πE(xj , θ
)− π∗
E
)2+(πT(xj , θ
)− π∗
T
)2
• An obvious limitation to this approach is that it imposes a penaltyif πE is too high or πT is too low

Identifying the optimal dose: Euclidean Distance
• Alternately, a weighted euclidean distance can be used instead
dj =
√wE(πE(xj , θ
)− π∗
E
)2+ wT
(πT(xj , θ
)− π∗
T
)2
• Finally, we could only penalize for πE < π∗E or πT > π∗
T
dj =
√(πE(xj , θ
)− π∗
E
)2 1[πE<π∗E ]+(πT(xj , θ
)− π∗
T
)2 1[πT>π∗T ]

Efficacy/Toxicity trade-off contour
• Thall and Cook (2004) proposed an efficacy/toxicity trade-offcontour for identifying the optimal dose
• They require clinicians to specify three points• (π∗
E , 0) - minimum efficacy with no toxicity• (1, π∗
T ) - maximum toxicity with perfect efficacy•
(π′E , π
′T
)- a point that is equally desirable to the first two
• This defines an efficacy/toxicity trade-off contour

Desirability Index
• A dose with probability of efficacy, πE , and probability toxicity, πT ,has desirability δ = 1− r where
r =
((1− πE
1− π∗E
)p
+
(πT
π∗T
)p)1/p
where p is found by plugging(π′
E , π′
T
)in for (πE , πT ), setting
r = 1 and solving for p.• The collection of points with δ = 0 defines an efficacy/toxicity
contour• Higher values of δ represent a more favorable trade-off and the
optimal combination (1,0) has δ = 1

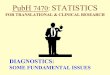
Efficacy/Toxicity trade-off contour: Example
• Let π∗E = 0.30, π∗
T = 0.40 and(π′
E = 0.60, π′
T = 0.20)
• In this scenario, we find that p = 1.11

Efficacy/Toxicity trade-off contour: Example
0.0 0.2 0.4 0.6 0.8 1.0
0.0
0.2
0.4
0.6
0.8
1.0
Probability of Efficacy
Pro
babi
lity
of T
oxic
ity

Early Termination for Futility
• Throughout the trial, we will assign subjects to the currentestimate of the optimal dose
• In some cases, it may be that there are no acceptable doselevels, in which case, we would like to terminate for futility
• A dose is unacceptable if:• There is high posterior probability of the probability of toxicity
exceeding the maximum or target probability of DLT• There is high posterior probability of the probability of efficacy
being less than the minimum or target probability of efficacy
• If all doses are unacceptable, we terminate early for futility

Dose Finding Algorithm
• Step 1: Treat the first cohort (2 or 3 patients) at the lowest doselevel
• Step 2: Observe the efficacy and toxicity outcomes• Step 3: Update posterior and calculate posterior means,
E (πE (x , θ) |YE ,Yt) and E (πT (x , θ) |YE ,Yt) for each dose level• Step 4: Determine the acceptable doses• Step 5: Terminate the trial if no doses are acceptable, otherwise,
treat the next cohort at the current estimate of the optimal doseunder the restriction that no untried doses may be skipped
• Step 6: Continue until the maximum sample size is reached. Theoptimal dose at study completion is selected for furtherevaluation

Advantages and Disadvantages of Efficacy/toxicitytrade-off designs
• Advantages• Efficacy and toxicity considered simultaneously• Considers MTD undesirable if the MTD has unacceptable efficacy• Does not escalate unless there is an efficacy benefit
• Disadvantages• Complicated!• Requires a larger sample size than standard phase 1 designs• We may not be able to determine a desirable level of efficacy this
early in drug development

Combination Therapy
• It is increasingly common that our interest lies in the safetyprofile for a combination of two drugs
• This requires dose finding with two agents• Yin and Yuan (2009) describe a Bayesian adaptive design for
two-agent dose finding

Combination Therapy
• Let A1, . . . ,AJ be the dose levels for drug A and B1, . . . ,BK bethe dose levels for drug B
• Let Xjk and Yjk be binary indicators for whether or not a patientexperienced a toxicity from drugs A and B, respectively, fromcombination Aj and Bk
• Yin and Yuan use a similar approach to the EffTox design in thatthey directly model the marginal probabilities and combine themusing a copula model

Modeling the marginal probabilities
• Yin and Yuan use the one-parameter power model for themarginal probabilities
P (DLT from Drug A|dose = j) = pαj
andP (DLT from Drug B|dose = j) = qβk

Modeling the joint probabilities
The joint probability of efficacy and toxicity is modeled using a copulamodel
π(x,y)j,k = pαx
j(1 − pαj
)1−x qβyk (1 − qk )
1−y+(−1)x+y pαj(1 − pαj
)qβk (1 − qk )
eψ − 1eψ + 1
• ψ characterizes the correlation between drug A and drug B• ψ = 0 indicates that drug A and drug B are independent

Estimating the parameters
The Likelihood for Yin and Yuan’s model is
J∏j=1
K∏k=1
(π(0,0)j,k
)n(0,0)j,k(π(0,1)j,k
)n(0,1)j,k(π(1,0)j,k
)n(1,0)j,k(π(1,1)j,k
)n(1,1)j,k
• Specify priors for α, β and ψ• Proceed with standard Bayesian inference using MCMC

Problem
• A problem arises if we are unable to assign DLTs to a specificdrug
• In this case, we only observe whether or not a DLT occurs• To accommodate, we alter the likelihood to
J∏j=1
K∏k=1
(π(0,0)j,k
)n(0,0)j,k(
1− π(0,0)j,k
)nj,k−n(0,0)j,k

Combination dose-finding algorithm
• Step 1: Treat patients in the first cohort at the lowest dosecombination
• Step 2: If for the current dose (j , k) we have
P(πj,k > π∗|Data
)< ce
escalate to an adjacent dose level with probability of toxicitygreater than that for the current dose level.
• Step 3: If for the current dose (j , k) we have
P(πj,k > π∗|Data
)> cd
de-escalate to an adjacent dose level with probability of toxicitylowerr than that for the current dose level.
• Step 5: The MTD is the dose level with probability of DLT closestto the target when the maximum sample size is reached.

Summary
• The goal of a phase 1 clinical trial is to assess the safety profileof a new drug and determine the optimal dose for furtherinvestigation
• Phase 1 oncology trials are unique for enrolling cancer patientswho’s previous treatments have failed
• We would like to treat as many patients as possible attherapeutic dose levels while identifying the MTD
• Bayesian adaptive designs allow us to treat more patients attherapeutic dose levels while identifying the true MTD at a higherrate than standard designs
• Bayesian adaptive designs provide the flexibility to accommodatedeviations from standard phase 1 designs (toxicity and efficacy,two drugs, etc.)