Embed Size (px)
Citation preview

PulmonaryFunctionTestingRamezSunnaMD,FCCP

LectureOverview
• GeneralIntroduction• IndicationsandUses• Technicalaspects• Interpretation• PatternsofAbnormalities

WhentoperformaPFT1. Evaluationofapulmonarycomplaintorsigntoassessforanyimpairmentinfunction
2. Quantificationofaknownimpairment(whetherpartofinitialeval.orfollowup/assessingdz.progression)
3. Preoperativeassessment4. Disabilityevaluation5. Screenpeopleexposedtoinhalational/toxic
agentsordrugeffects

Caution• Myocardialinfarctionwithinthelastmonth• UnstableAngina• RecentThoraco-abdominalsurgery• Recentophthalmicsurgery• ThoracicorabdominalAneurysm• CurrentPneumothoraxWildeM,NairS,Madden B.PulmonaryFunctiontests- areview.CareoftheCrit Ill.2007;Dec23(6):173-7
PFT- Components• Spirometry• Bronchodilatorchallenge• LungVolumes• DLCO• MaximalRespiratoryPressures• MaximalVoluntaryVentilation• Bronchoprovocation

LungVolumes

Volume-TimeSpirogram• Tidalvolumerespirations
• Atendexpirationpt.performsamaximalinspirationfollowedby
• Exhalationashardandfastaspossible
• ExhalingtheFVC
Volume (L )
FVC
RV

Volumetimecurve Flowvolumeloop

EquipmentPerformance
QualityControl
PatientManeuvers
AcceptabilityCriteria
ReproducibilityCriteria
TestsforAnalysisReferenceValuesInterpretation
• Volumeswithin±5%or50ml;flowswithin±5%or200ml/s
• Checkaccuracy&linearitydailywith3Lsyringe
• Explainanddemonstratemaneuver;properpatientposition;repeattestsuntil3acceptabletestsorpatienthasmade8attempts
• Goodquickstartwithvigorouseffort;nocoughorpauseinfirstsec;6secminimumorgoodplateauwithoutglottic closure
• For3acceptabletests,differencebetweenlargesttwoFVC’sandlargesttwoFEV1’sshouldbewithin150mlofeachother
• AnalyzelargestFVCandFEV1fromacceptabletests&selectappropriatereferencevalues
• Useestablishedguidelinesforinterpretation

GeneralApproachtoInterpretingaPFT• Confirmdemographicdata• IsthetestAcceptable/Reproducible• Aretheresultsnormal• Whatisthepatternofabnormality• Whatistheseverityofabnormality• Whatdoesthismeanforthepatient-comparisontoprevioustests
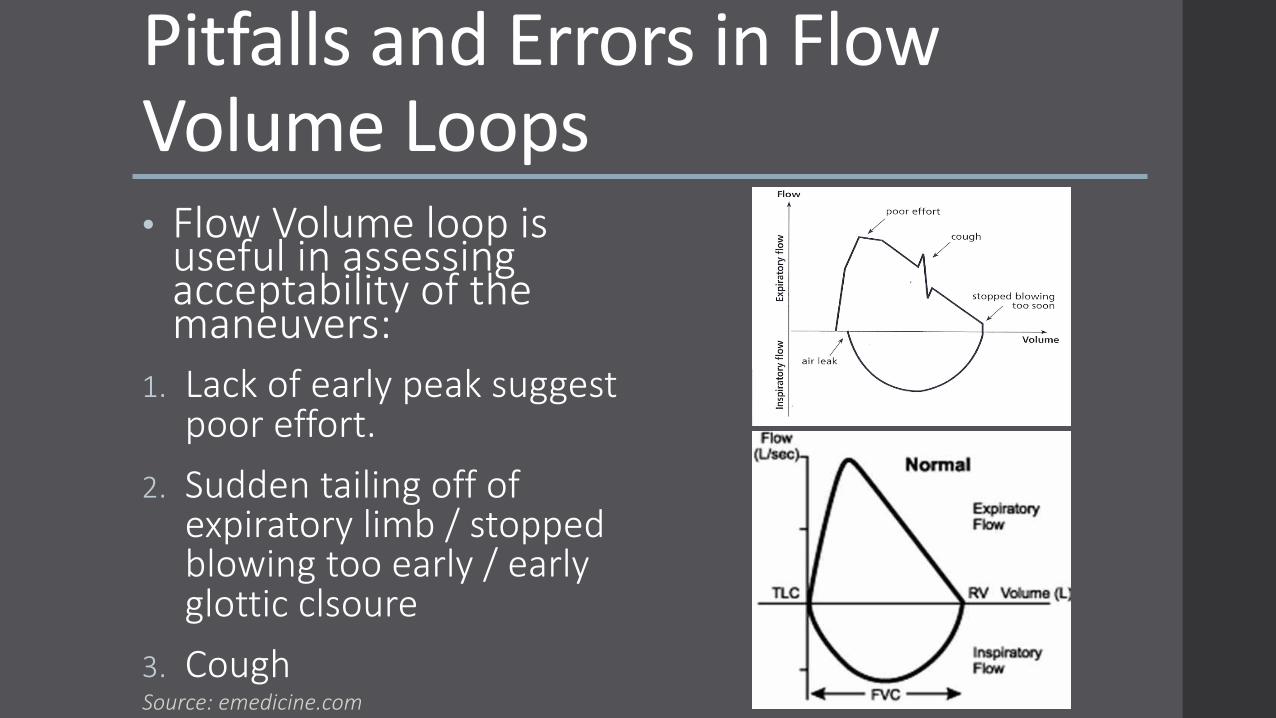
PitfallsandErrorsinFlowVolumeLoops• FlowVolumeloopisusefulinassessingacceptabilityofthemaneuvers:
1. Lackofearlypeaksuggestpooreffort.
2. Suddentailingoffofexpiratorylimb/stoppedblowingtooearly/earlyglottic clsoure
3. CoughSource:emedicine.com
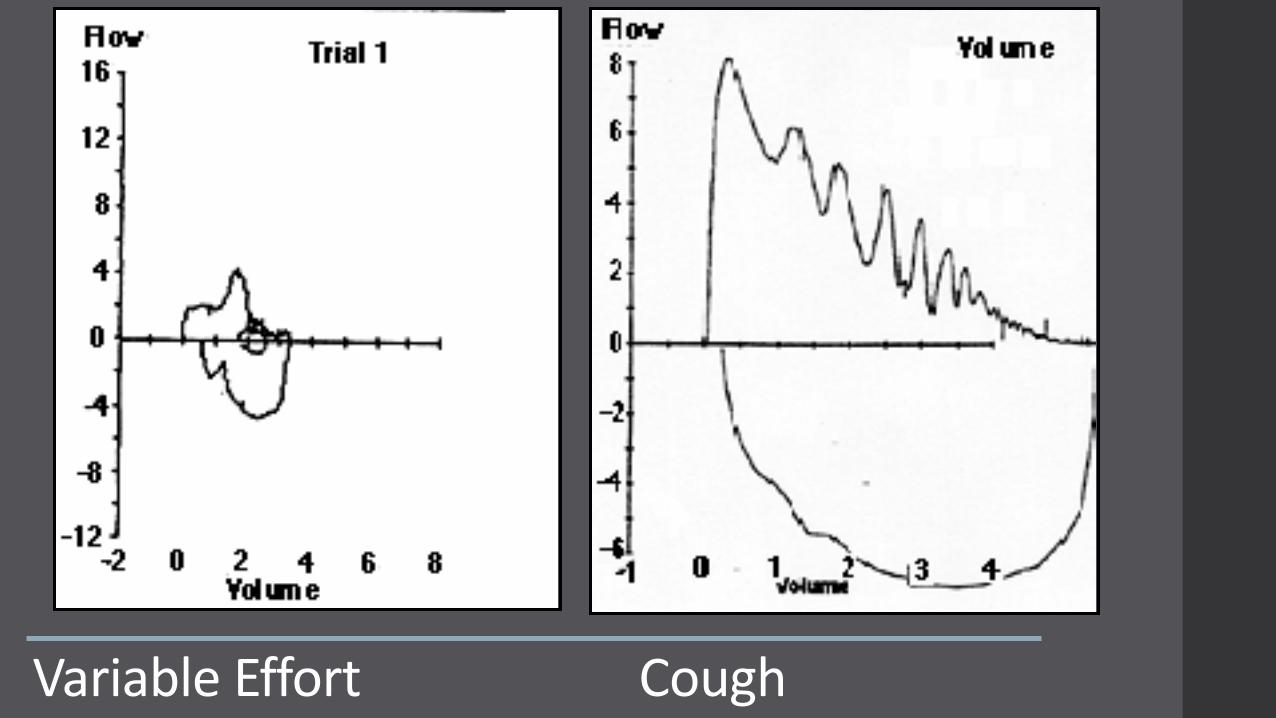
VariableEffortCough

NormalValues• AppropriateReferenceStandardsmustbeusedforcomparison• BasedonAge,Height,SexandRace• IntheUS:NHANESIIIstandardforadults• DifferentadjustmentfactorsfordifferentvaluesforCaucasian,AfricanAmerican,Asian,easternIndian• Shouldbeupdatedatleastevery10years

PercentPredictedasNormalRange• Resultsareexpressedas%Predictedofapredictednormalvalueofapersonthesameage,sex,raceandheight
• NormalRanges:ü FVC>80%
ü FEV1 >80%
ü FEV1/FVClessthan5th percentile(LLN),>0.70
ü FEF25-75:65%;50%
ü DLCO80-120%
ü TLC80-120%
ü RV80-120%
• UseofLLNbelow5thpercentileofthenormaldistributioninsteadof%predicted

PatternsofAbnormality• Obstructivepattern• Restrictivepattern• Mixedpattern• Vascularpattern• Neuromuscularpattern• Pooreffortpattern• NonSpecificPattern

ObstructiveVentilatory Defect• Limitationofexpiratoryflow• ThehallmarkisareducedFEV1/FVCratio<0.7• FEF25-75<?50%
ü Asthmaü COPDü CysticFibrosisü Bronchiectasis

TheFlowVolumeLoop• Theusuallineardescentoftheflow-volumecurveisdisruptedbyanexaggeratedupwardconcavityofthedescendinglimbofthecurve
BronchodilatorResponse• Physiologicresponseinvolvingairwayepithelium,nerves,mediatorsandsmoothmuscle• Bronchodilatortobeheldpriortotesting• IncreaseineitherFEV1orFVCfrombaseline
ü Byatleast12%and200mL• ThecorrelationbetweenbronchoconstrictionandBDresponseisimperfect


RestrictiveVentilatory Defect• ThehallmarkisreducedLungvolumes
• ReducedTLCbydefinition
• Theflowvolumeloopoftenmaintainsanearlynormalshapethoughminiaturized.

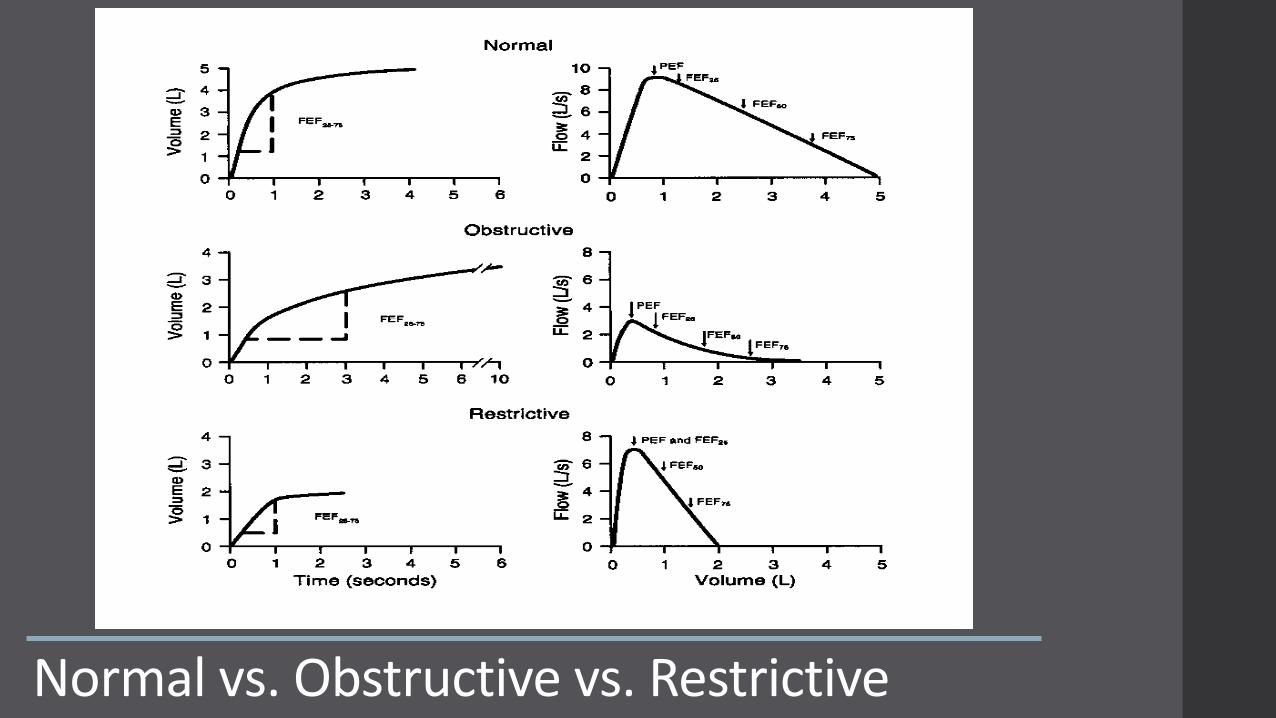
Normalvs.Obstructivevs.Restrictive

MixedObstructiveandRestrictivePattern• ReducedFEV1/FVCratiowithareducedTLC• Couldbetwodiseaseprocesses:AmiodaroneDrugToxicityinapatientwithCOPD…• Sarcoidosis,Lymphangiomleiomyomatosis,cryptogenicorganizingpneumonia,langerhans cellhistiocytosis,respiratorybronchiolitis

RatingofSeverity
• Basedonstatement/guidelinesfromtheAmericanThoracicSociety(ATS)- FEV1• ObstructivePattern- FEV1• RestrictivePattern– TLC(lungvolumes)
ü Iflungvolumesnotobtained– FVC

ATS/ERSStandardizationofLungTesting:InterpretativeStrategiesforLungFunctionTests- 2005

IsolatedReductioninDiffusionCapacity• Single-breathDLCOmeasuresthecapacityofthelungtotransfergas
• PatientexhalestoRVthenrapidlyinhalesgasmixturewithaminuteamountofCO.After,10secondbreath-holdatTLC,thepatientrapidlyexhales&theexhaledgasisanalyzedtomeasuretheamountofCOtransferredintothecapillarybloodduringthemaneuver
CausesofDecreasedDLCO• Anemia,highCOlevels
• ObstructiveLungDiseaseü Emphysema
ü CysticFibrosis
• ParenchymalLungDiseaseü InterstitialLungDisease
ü Sarcoidosis
• PulmonaryVascularDiseaseü PrimaryPulmonaryHypertension
ü AcuteandChronicPulmonaryThromboembolism

NeuromuscularPattern• RestrictivepatternwithnormalDLCO
Lungcompliance(microatelectasis)greaterlossofVCwithchronicMuscleweakness
Chestwallcompliance(stiffligaments,ankylosedjoints,kyphoscoliosis)
• ChangeinFVCbetweenuprightandsupineü Normalfall- average8%;upperlimit19%ü >20%fallsuggestsdiaphragmaticparalysis
Estenne M,DeTroyerATheRespiratoryMuscles1990;360AllenSMetalBrJDisChest1985;79:267

MeasurementofMIPandMEP
HyattREetalInterpretationofPulmonaryFunctionTests,LippincottWilliamsandWilkins1997,p90

MaximumAirwayPressures• %predictedvaluesareavailable,decreaseswithage,lowervaluesinfemales
• Variabilityofaround24cmH2Opressuresinsamedaymeasurements
• NormalMIPgood–ve predictivevalue• MIP<1/3NLpredictshypercarbia• MEP<60cmH2Opredictsweakcough• correlatespoorlywithseverityoflimbmuscleweakness
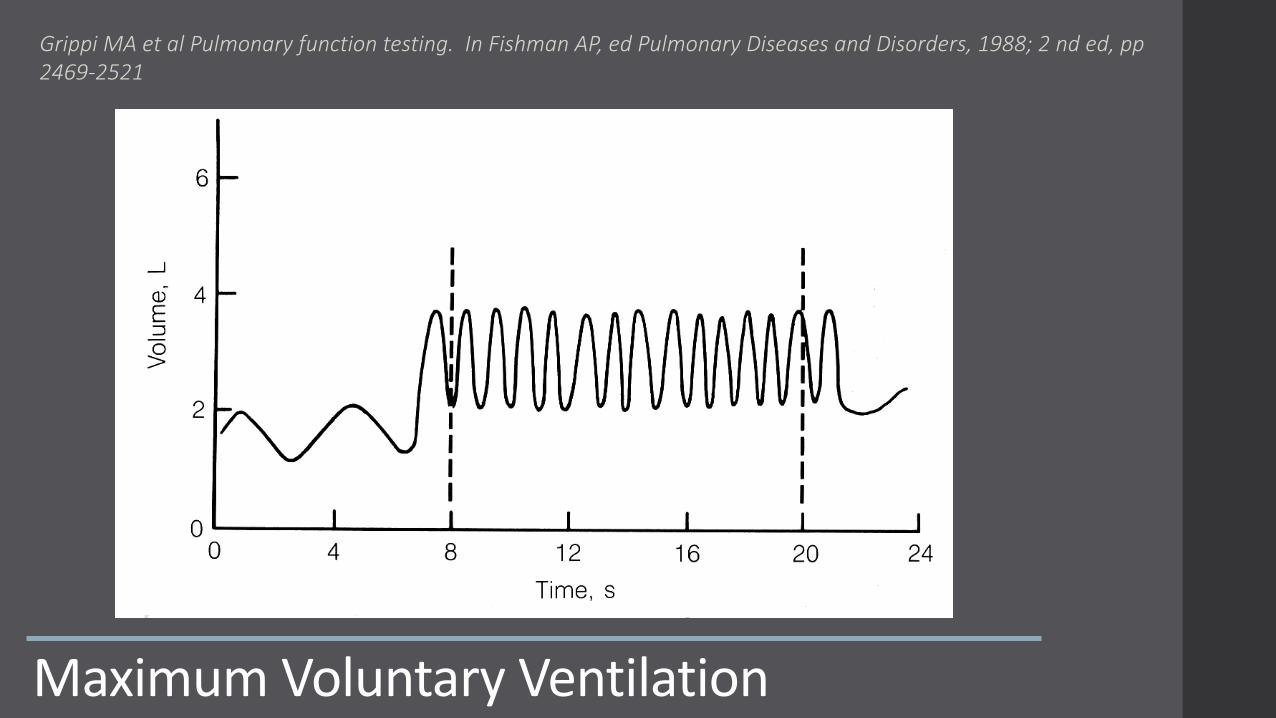
MaximumVoluntaryVentilation
Grippi MAetalPulmonaryfunctiontesting.InFishmanAP,ed PulmonaryDiseasesandDisorders,1988;2nd ed,pp2469-2521

MaximalVoluntaryVentilation• Originallycalledmaximalbreathingcapacity• Themaximalvolumeofairthatcanbemovedbyvoluntaryeffortin1minute• Technique:breatherapidlyanddeeplyfor15to30seconds,ventilatory volumesarerecorded

MVV• Heavilydependentonpatientcooperationandeffort
• Nonspecific:Lossofcoordinationofrespiratorymuscles,musculoskeletaldiseaseofthechestwall,neurologicdisease,anddeconditioningfromanychronicillness,aswellasventilatory defectsdecreaseMVV
• Itcorrelateswellwithsubjectivedyspnea
• Usefulinevaluatingexercisetolerance
• Hasaprognosticvalueinpreoperativeevaluation
• Itprovidesameasureofrespiratorymuscleenduranceandventilatoryreserve
• MVV=FEV1*35-40

NonspecificAirwayDiseasePattern
CentralandUpperAirwayObstruction
• Flowvolumeloopscanprovideinformationonupperairwayobstruction• Characteristicsofthelesion
ü Locationofthelesion:intrathoracicvsextrathoracic
ü Behaviorofthelesioninrapidinspirationandrapidexhalation:fixedvsvariable

FixedObstruction
Trachealstenosis/strictureBilateralvocalcordparalysis
Extrinsiccompression
Levitzky MGPulmonaryPhysiology,McGrawHill4thed,1995,p50

VariableExtrathoracic Obstruction
VocalcordparalysisGoiterTumor
Levitzky MGPulmonaryPhysiology,McGrawHill4thed,1995,p50

VariableIntrathoracicObstruction
TracheomalaciaIntratracheal tumor
Levitzky MGPulmonaryPhysiology,McGrawHill4thed,1995,p50

ThankYou!RamezSunnaMD,[email protected]


![Shrinking Lung Syndrome: A Pulmonary Manifestation of ... · scan]) and pulmonary function tests (PFTs). Pulmonary function tests were carried out in our pulmonary function laboratory,](https://img.pdfslide.net/doc/110x75/5f03189c7e708231d40783f1/shrinking-lung-syndrome-a-pulmonary-manifestation-of-scan-and-pulmonary-function.jpg)