Embed Size (px)
Citation preview

Accepted for publication Sept 10, 2013.
Address correspondence to Dr Tzao, Division of Thoracic Surgery,Department of Surgery, Tri-Service General Hospital, 325, Section 2,Cheng Gong Rd, Nei Hu, Taipei 114, Taiwan; e-mail: [email protected].
329Ann Thorac Surg CASE REPORT CHEN ET AL2014;98:329–31 LUNG CYST WITH METASTATIC GASTRIC CANCER
FEATUREARTIC
LES
Comment
Fungal infections in the lung transplant population areincreasingly recognized, with major functional morbidcomplications, notably an increased risk of bronchiolitisobliterans syndrome [4]. Of these, pulmonary mucormy-cosis is uncommon, but has an extraordinarily poor prog-nosis across all organ transplant recipient populations. Theextant literature on pulmonary mucormycosis clearlydemonstrates that a combined strategy of surgical resectionand amphotericin B yields the best survival outcomes. Thelargest series, which also reviewed previous reports withinthe literature, reported a mortality of 11% in patients un-dergoing combined surgical therapy, in contrast to 68% inpatients treated with antifungal agents alone, althoughhigh-risk patientsmay have been denied surgical treatment[5]. Consequently, with clearly donor-derived bronchiallyinvasive infection in the absence of disseminated disease,we chose an aggressive strategy of bilateral retrans-plantation. Our review of the literature suggests that this isthe first reported case of donor-derived pulmonarymucormycosis successfully managed with reoperative lungtransplantation. Two previous cases of allograft mucormy-cosis manifesting in the peritransplant period have beenreported [6, 7]; thesepatientsweremanagednonoperativelywith successful outcomes.
Obtaining donor organs in the DCD setting is commonin abdominal organ transplantation, but comparativelyrare in thoracic organ transplantation. However, recentresults regarding the use of DCD lungs from centers in theUnited States [1], Canada [8], and Australia [2] are prom-ising. We obtained a well-functioning donor organ block,but given possible ischemic injury and pulmonary edemain the DCD setting, we chose to evaluate the lungs usingEVLP. In EVLP, donor lungs are ventilated mechanicallyand perfused with crystalloid-based Steen solution in aclosed circuit [3]. EVLP can serve as a diagnostic tool forallograft functional assessment and to rehabilitate mar-ginal donor lungs [8]. Thus, salient features of this caseinclude reoperative bilateral lung transplantation as thecritical element of the treatment strategy, the use of a DCDlung donor subjected to EVLP, and continued adjunctivesystemic and local antifungal therapies.
References
1. Wigfield CH, Love RB. Donation after cardiac death lungtransplantation outcomes. Curr Opin Organ Transplant2011;16:462–8.
2. Snell GI, Levvey BJ, Oto T, et al. Early lung transplantationsuccess utilizing controlled donation after cardiac death do-nors. Am J Transplant 2008;8:1282–9.
3. Sanchez PG, Bittle GJ, Burdorf L, Pierson RN 3rd, Griffith BP.State of art: clinical ex vivo lung perfusion: rationale, currentstatus, and future directions. J Heart Lung Transplant 2012;31:339–48.
4. Lease ED, Zaas DW. Update on infectious complicationsfollowing lung transplantation. Curr Opin Pulm Med 2011;17:206–9.
5. Tedder M, Spratt JA, Anstadt MP, Hegde SS, Tedder SD,Lowe JE. Pulmonary mucormycosis: results of medical andsurgical therapy. Ann Thorac Surg 1994;57:1044–50.
6. McGuire FR, Grinnan DC, Robbins M. Mucormycosis ofthe bronchial anastomosis: a case of successful medical
� 2014 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
treatment and historic review. J Heart Lung Transplant2007;26:857–61.
7. Brugiere O, Dauriat G, Mal H, et al. Pulmonary mucormycosis(zygomycosis) in a lung transplant recipient: recovery afterposaconazole therapy. Transplantation 2005;80:2061–2.
8. Cypel M, Yeung JC, Machuca T, et al. Experience with the first50 ex vivo lung perfusions in clinical transplantation. J ThorCardiovasc Surg 2012;144:1200–6.
Pulmonary Metastatic GastricCancer Mimicking A GiantMediastinal CystWun-Lin Chen, MD, Chih-Lung Shen, MD,Yi-Ming Chang, MD, Chih-Ming Hsieh, MD,Cheng-Kuang Chang, MD, Hsian-He-Hsu, MD, andChing Tzao, MD, PhD
Division of Thoracic Surgery, Department of Surgery,Department of Pathology, and Department of Radiology,Tri-Service General Hospital, National Defense MedicalCenter, Taipei, Taiwan
Cysts and cavities are common radiologic abnormalities.Pulmonary metastasis comprises a rare entity of thoraciccystic diseases. We reported a case of giant cyst at the leftanterior mediastinum that was pathologically confirmedas a lung metastasis from previously resected gastriccancer. The cyst was completely removed with wedgeresection of the surrounding lung through a left anteriorthoracotomy. One should always keep in mind the pos-sibility of an intrathoracic cyst near or at the mediastinalregion that may originate from metastatic lesions to thelungs when patients have previous cancer history.
(Ann Thorac Surg 2014;98:329–31)� 2014 by The Society of Thoracic Surgeons
ysts and cavities are common abnormalities on chest
Cradiographs and chest computed tomography (CT).Confirmation of the nature of thoracic cystic or cavitarylesions may be challenging. Differential diagnoses of suchlesions range from congenital to the acquired cystic dis-eases but very rarely cases of metastatic cancer [1, 2]. Wereport a case of lung metastasis from gastric cancer pre-senting as a giant cyst at the left anterior mediastinumthat mimics a cyst of thymic origin.A 73-year-old man was hospitalized on account of epi-sodes of hemoptysis with a large mass abutting from theleft anterior mediastinum on chest radiograph (Fig 1A).He had been treated for a stage II gastric cancer by sub-total gastrectomy half of year prior to this admission. Thechest radiograph taken before gastrectomy appeared tobe normal. Chest computed tomography (CT) revealed awell-defined thin-walled cyst, 10 cm in diameter, at the
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2013.09.063
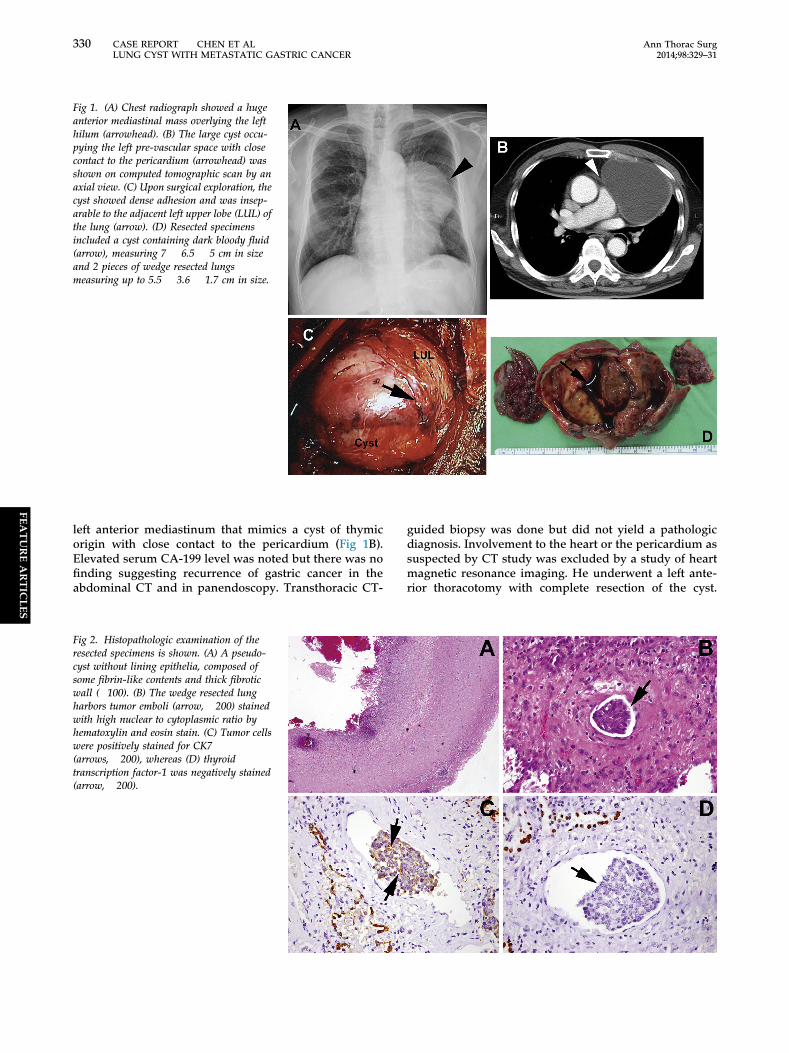
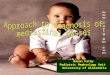
Fig 1. (A) Chest radiograph showed a hugeanterior mediastinal mass overlying the lefthilum (arrowhead). (B) The large cyst occu-pying the left pre-vascular space with closecontact to the pericardium (arrowhead) wasshown on computed tomographic scan by anaxial view. (C) Upon surgical exploration, thecyst showed dense adhesion and was insep-arable to the adjacent left upper lobe (LUL) ofthe lung (arrow). (D) Resected specimensincluded a cyst containing dark bloody fluid(arrow), measuring 7 � 6.5 � 5 cm in sizeand 2 pieces of wedge resected lungsmeasuring up to 5.5 � 3.6 � 1.7 cm in size.
330 CASE REPORT CHEN ET AL Ann Thorac SurgLUNG CYST WITH METASTATIC GASTRIC CANCER 2014;98:329–31
FEATUREARTIC
LES
left anterior mediastinum that mimics a cyst of thymicorigin with close contact to the pericardium (Fig 1B).Elevated serum CA-199 level was noted but there was nofinding suggesting recurrence of gastric cancer in theabdominal CT and in panendoscopy. Transthoracic CT-
Fig 2. Histopathologic examination of theresected specimens is shown. (A) A pseudo-cyst without lining epithelia, composed ofsome fibrin-like contents and thick fibroticwall (�100). (B) The wedge resected lungharbors tumor emboli (arrow, �200) stainedwith high nuclear to cytoplasmic ratio byhematoxylin and eosin stain. (C) Tumor cellswere positively stained for CK7(arrows, �200), whereas (D) thyroidtranscription factor-1 was negatively stained(arrow, �200).
guided biopsy was done but did not yield a pathologicdiagnosis. Involvement to the heart or the pericardium assuspected by CT study was excluded by a study of heartmagnetic resonance imaging. He underwent a left ante-rior thoracotomy with complete resection of the cyst.

331Ann Thorac Surg CASE REPORT CHEN ET AL2014;98:329–31 LUNG CYST WITH METASTATIC GASTRIC CANCER
Upon exploration, a dense adhesion was observed be-tween the cyst and the adjacent left upper lung (Fig 1C)that mandated wedge resections to allow a completeremoval of the cyst. Resected specimens are shown as alarge blood-containing cyst along with wedge resectedlungs (Fig 1D). Microscopic examination of the resectedspecimens revealed a pseudocyst without lining epithelia,composed of some fibrin-like contents and thick fibroticwall (Fig 2A), with lung parenchyma harboring multiplesmall tumor emboli of gastric origin (Fig 2B). Immuno-histochemical stains of the tumor part concluded positivestaining for CK7 (Fig 2C) but negative for TTF-1 (Fig 2D)that excluded primary adenocarcinoma of the lung. Hehad led an uneventful postoperative course with adjuvantchemotherapy being offered toward metastatic gastriccancer. He has continued to do well at a follow-up of7 months without disease progression at the time of thisreport.
FEATUREARTIC
LES
Comment
Cystic masses at the anterior mediastinum comprisea heterogeneous group of asymptomatic or symptom-atic conditions including congenital, infectious, orneoplastic entities [1]. Common anterior mediastinalcystic masses include cystic teratoma, pericardial cyst,lymphangioma, thymic cyst [1]. Metastatic carcinoma tothe mediastinum is rare and may present as cyst-likelesions [2, 3]. Anterior mediastinal tumors can un-dergo cystic degeneration presenting as mixed solidand cystic lesions at CT or magnetic resonance imagingand these cystic lesions are almost indistinguishablefrom those of a congenital cyst if degeneration isextensive [4].
Depending on the location of the cyst, it may origi-nate from the adjacent lung that has close contact to theanterior mediastinum. Among them, cystic or cavitarylung masses such as tumor with necrosis or lung ab-scess may appear as an anterior mediastinal cyst [4].Many cystic and cavitary lesions of the lungs occurfrequently in bronchogenic carcinoma (10% to 15%)and are associated more often with squamous cellcarcinoma [3]. Occasionally, they also occur with sar-coma, transitional cell carcinoma of the bladder, and,less commonly, with lymphoma and metastasis [3, 5].The frequency of cavitation or cystic change in pul-monary metastases is approximately 4%, as opposed to9% in primary bronchogenic carcinoma [5]. Pulmonarymetastases may present radiologically with a spectrumof unusual appearance including cavitation or cystformation, calcification, and surrounding ill-definedhemorrhage [5]. It is essential to detect pulmonarymetastases in the treatment of patients with cancer.Modern immunohistochemistry studies using specialmarkers, such as thyroid transcription factor 1 (TTF-1),can help make this distinction between primary pul-monary adenocarcinoma and metastatic adenocarci-noma from another site [6].
It is challenging to differentiate a thymic cyst from theone reported in this case. Hemorrhage in metastatic
lesions can be depicted on CT images and it is consideredto be caused by rupture of the vessels within the fragileneovascular tissue [3]. One should keep in mind that acyst in the thymic region may not be a thymic cyst as itcan originate from the adjacent lungs that harbor otherpathologies such as metastasis, especially when bloodycyst content is present. Based on the patient’s history ofprevious gastric cancer, intraoperative findings, and ob-servations from histopathologic examinations with anegative immunohistochemical stain for TTF-1, it sug-gests that the cyst reported herein may be a hemorrhagiccyst arising from the lungs with metastatic gastric cancer.Further, the majority of thymic cysts present with solidcomponents and usually do not grow as fast as in thiscase.Lung metastases from a primary extrapulmonary
malignancy are often a manifestation of widespreaddissemination. Aggressive pulmonary metastasectomy ina number of different cancers may substantially prolongpatients’ survival [7]. It has been reported that patientswith lung metastasis of gastric cancer can potentiallyenjoy long-term survival by metastasectomy [8]. Never-theless, the presence of tumor emboli in our patientsuggests that it may not be a localized process, whichneeds continued follow-up for possible disease progres-sion with treatment being offered accordingly.In conclusion, we reported an extremely rare case of
metastatic gastric cancer to the lung that mimics ananterior mediastinal cyst. One should always keep inmind the possibility of an intrathoracic cyst near or at themediastinal region that may originate from metastaticlesions to the lungs when patients have previous cancerhistory. An aggressive diagnostic procedure such as bi-opsy or surgical exploration should be warranted to avoiddelay in the diagnosis and treatment for potential cancermetastasis.
References
1. Odev K, Arıbas BK, Nayman A, Arıbas OK, Altınok T,K€uc€ukapan A. Imaging of cystic and cyst-like lesions of themediastinum with pathologic correlation. J Clin Imaging Sci2012;2:33.
2. Moran CA, Suster S, Silva EG. Low-grade serous carcinoma ofthe ovary metastatic to the anterior mediastinum simulatingmultilocular thymic cysts: a clinicopathologic and immuno-histochemical study of 3 cases. Am J Surg Pathol 2005;29:496–9.
3. Topal NB, Oruc E, Gokalp G, Topal U. Atypical pulmonarymetastases: Radiologic appearances. Indian J Radiol Imaging2007;17:181–5.
4. Jeung MY, Gasser B, Gangi A, et al. Imaging of cystic massesof the mediastinum. RadioGraphics 2002;22:S79–93.
5. Godwin JD, Webb WR, Savoca CJ, Gamsu G, Goodman PC.Multiple, thin-walled cystic lesions of the lung. AJR Am JRoentgenol 1980;135:593–604.
6. Jagirdar J. Application of immunohistochemistry to the diag-nosis of primary and metastatic carcinoma to the lung. ArchPathol Lab Med 2008;132:384–96.
7. Hornbech K, Ravn J, Steinbr€uchel DA. Outcome after pul-monary metastasectomy: analysis of 5 years consecutive sur-gical resections 2002-2006. J Thorac Oncol 2011;6:1733–40.
8. Kemp CD, Kitano M, Kerkar S, et al. Pulmonary resection formetastatic gastric cancer. J Thorac Oncol 2010;5:1796–805.

![Diagnosis and treatment of cystic lung diseasekjim.org/upload/kjim-2016-242.pdf · · 2017-03-07Features of cyst and cyst-mimicking lucencies [1] ... tion of the mammalian target](https://img.pdfslide.net/doc/110x75/5ad657ab7f8b9a6d708e07bc/diagnosis-and-treatment-of-cystic-lung-of-cyst-and-cyst-mimicking-lucencies-1.jpg)