Embed Size (px)
Citation preview

Pulsed Electromagnetic Field Therapy Improves Tendon-to-BoneHealing in a Rat Rotator Cuff Repair Model
Jennica J. Tucker,1 James M. Cirone,1 Tyler R. Morris,1 Courtney A. Nuss,1 Julianne Huegel,1 Erik I. Waldorff,2 Nianli Zhang,2
James T. Ryaby,2 Louis J. Soslowsky1
1McKay Orthopaedic Research Laboratory, University of Pennsylvania, 424 Stemmler Hall, 3450 Hamilton Walk, Philadelphia, Pennsylvania19104-6081, 2Department of Research and Clinical Affairs, Orthofix Inc., Lewisville, Texas
Received 25 December 2015; accepted 5 June 2016
Published online in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/jor.23333
ABSTRACT: Rotator cuff tears are common musculoskeletal injuries often requiring surgical intervention with high failure rates.Currently, pulsed electromagnetic fields (PEMFs) are used for treatment of long-bone fracture and lumbar and cervical spine fusionsurgery. Clinical studies examining the effects of PEMF on soft tissue healing show promising results. Therefore, we investigated therole of PEMF on rotator cuff healing using a rat rotator cuff repair model. We hypothesized that PEMF exposure following rotator cuffrepair would improve tendon mechanical properties, tissue morphology, and alter in vivo joint function. Seventy adult male Sprague–Dawley rats were assigned to three groups: bilateral repair with PEMF (n¼30), bilateral repair followed by cage activity (n¼30), anduninjured control with cage activity (n¼10). Rats in the surgical groups were sacrificed at 4, 8, and 16 weeks. Control group wassacrificed at 8 weeks. Passive joint mechanics and gait analysis were assessed over time. Biomechanical analysis and mCT wasperformed on left shoulders; histological analysis on right shoulders. Results indicate no differences in passive joint mechanics andambulation. At 4 weeks the PEMF group had decreased cross-sectional area and increased modulus and maximum stress. At 8 weeksthe PEMF group had increased modulus and more rounded cells in the midsubstance. At 16 weeks the PEMF group had improved bonequality. Therefore, results indicate that PEMF improves early tendon healing and does not alter joint function in a rat rotator cuffrepair model. � 2016 Orthopaedic Research Society. Published by Wiley Periodicals, Inc. J Orthop Res
Keywords: PEMF; supraspinatus repair; animal model
Rotator cuff tears are common musculoskeletal injurieswhich often require surgical intervention. Unfortu-nately, post-repair prognosis is poor, with surgicalrepairs that fail in up to 94% of cases.1 Repaired tissuetends to be fibrotic, disorganized, and reattaches poorlyto the bony insertion. To improve tendon-to-bone heal-ing, many non-invasive therapeutic devices have beenutilized post-operatively including therapeutic ultra-sound and shock wave therapy.2,3
In orthopaedics, the use of these non-invasivetherapeutic devices has become increasingly popularduring the post-operative recovery period in an effortto enhance tissue healing. These devices tend to berelatively inexpensive and easily obtainable. They arerelatively easy to use, and are especially enticing asthey can be brought into the patient’s home and do notrequire frequent visits to the clinic. Additionally, non-invasive therapeutic devices can be used for a varietyof applications, including promoting tissue healingprior to surgical intervention or in lieu of surgicalintervention all together.
Although there are numerous advantages to usingnon-invasive therapeutic devices, their efficacy has notyet been maximized. For example, a recent studycomparing shock wave therapy and corticosteroid injec-tion found corticosteroids significantly reduced pain inpatients with plantar fasciitis.4 Although corticoste-roids are commonly used as anti-inflammatory painreducers in orthopaedics, their safety is controversial,
and they do not play a role in tissue healing. Therefore,the investigation of alternative non-invasive therapeu-tic technologies is desirable.
Currently, non-invasive devices emitting pulsed elec-tromagnetic fields (PEMFs) have been approved by theFDA for treatment of long-bone fracture non-unions andas an adjunct to lumbar and cervical spine fusionsurgery.5–9 Several pre-clinical studies have been con-ducted examining the effect of PEMF in various biologicalmodels including a study examining the effect of PEMFin a rat fibular osteotomy model which found increasedbone callus volume, stiffness, and modulus in the PEMFtreated group.10 Another study examining whetherPEMF would improve vertebral bone mass in a ratosteoporosis model found that PEMF exposure improvedtrabecular bone volume in osteoporotic rat vertebrae.11
Because PEMF therapy is commonly used in bonefracture healing, there may be a potential therapeuticapplication using PEMF therapy to enhance soft tissuehealing as PEMF has also been shown to decreaseinflammatory markers.12 PEMF has been utilized inclinical studies to treat epicondylitis and to improvehealing after rotator cuff repair. When compared to shamtreatment, patients with epicondylitis receiving PEMFtherapy saw improvements in multiple pain parametersfor up to 3 months following the onset of treatment.13
Patients with small to medium rotator cuff tears hadimproved range of motion 3 months post-op after 6 weeksof PEMF therapy when compared to those receivingplacebo.14 Pre-clinical studies also suggest that PEMFincreases tensile strength of repaired Achilles transectionin a rat model.15 However, investigation of the structuraland functional effects of PEMF on tendon-to-bone healinghas not yet been evaluated.
Grant sponsor: Orthofix, Inc.Correspondence to: Louis J. Soslowsky (T: þ1-215-898-8653;F: þ1-215-537-2133; E-mail: [email protected])
# 2016 Orthopaedic Research Society. Published by Wiley Periodicals, Inc.
JOURNAL OF ORTHOPAEDIC RESEARCH MONTH 2016 1

Therefore, the objective of this study was toinvestigate the effect of PEMF exposure on rotatorcuff healing using an established rat rotator cuffacute detachment and repair model.16–21 In thisstudy, we asked whether PEMF exposure for 3 h aday, 7 days per week would improve tissue mechani-cal and morphologic properties, as well as jointfunction. We hypothesized that PEMF exposurefollowing rotator cuff detachment and repair would:(i) improve healing tendon mechanical properties; (ii)improve tissue morphology including cell shape,cellularity, and collagen fiber organization; and (iii)alter in vivo joint function including ambulation andpassive joint mechanics.
METHODSStudy DesignSeventy adult male Sprague–Dawley rats (400–450 g) wereused in this University of Pennsylvania Institutional AnimalCare and Use Committee approved study. Animals werehoused in a conventional facility in 12-h light/dark cyclesand were fed standard rat chow ad libitum. Animals wererandomized into one of three treatment groups: (1) acuteinjury and repair followed by cage activity with PEMF; (2)acute injury and repair followed by cage activity alone; and(3) uninjured control with no surgical intervention. Animalsin groups 1 and 2 were sacrificed at 4, 8, and 16 weeks(n¼ 10 per time point) and animals in group 3 (control) weresacrificed at 8 weeks (n¼ 10). Additionally, animals in the16 week time point (8 week for control group) underwentlongitudinal in vivo ambulatory assessment and passiveshoulder joint mechanics assessments as described below. Atthe time of sacrifice, left shoulders (n¼ 10 per group andtime point) remained intact for subsequent mechanicaltesting while right shoulders (n¼ 7 per group and time point)were immediately dissected and processed for histologicalanalysis. The remaining right shoulders were left intact toserve as additional mechanical testing specimens. The ani-mals were then frozen at �20˚C and later thawed fordissection at the time of mechanical testing.
Detachment and Repair SurgeryAnimals in groups 1 and 2 were subjected to identicalbilateral supraspinatus detachment and repair asdescribed.17 For analgesia, buprenorphine (0.05mg/kg) wasadministered subcutaneously 30min prior to surgery, 6–8hpost-operatively, and then every 12h for the next 48h.Briefly and as described previously,17 with the arm held inexternal rotation and adduction, the deltoid muscle was splitin the transverse plane to expose the supraspinatus tendon.The tendon was grasped using double-armed 5–0 polypropyl-ene suture (Surgipro II, Covidien, Mansfield, MA) and wassharply transected from its bony insertion. For repair, a5mm diameter high speed bur (Multipro 395, Dremel, Mt.Prospect, IL) was used to remove remaining fibrocartilagefrom the footprint of the tendon insertion site. A 0.5mm bonetunnel was drilled from anterior to posterior through thegreater tuberosity of the humerus. The suture was passedthrough the bone tunnel and tied down, affixing the tendonto the greater tuberosity using a modified Mason–Allentechnique. The wound was flushed with saline, and thedeltoid and skin sutured closed.
PEMF ExposureAnimals in group 1 received daily 3h PEMF exposure untilthe time of sacrifice using a commercial PEMF signal (Physio-Stim1, Orthofix, Inc., Lewisville, TX). The maximum ampli-tude, fundamental frequency and slew rate of the Physio-Stim1 PEMF signal are 0.5mT, 3.85kHz, and 15.4T/s,respectively. Treatment regime was determined based on theFDA approved Physio-Stim1 device currently used to treatfracture non-unions.6 Specifically, 24h after surgery, animalswere placed on a custom built PEMF rack (Orthofix, Inc.,Lewisville, TX) with sets of Helmholtz coils for each standardcage (for a total of 16 cages). The PEMF rack was equippedwith a timer, which automatically turned off the PEMF signalafter 3h. For quality assurance, the slew rate (dB/dt) for eachPEMF coil module were tested twice per week using atransverse search coil placed at the center of each modulebetween the two coils connected to an amplifier and signalintegrator and interfaced with an oscilloscope (Orthofix, Inc.).The quality assurance check ensured that the PEMF fielduniformity within the entire volume of each cage was withinthe allowed �30% of the average slew rate.
Quantitative Ambulatory AssessmentGround reaction forces (medial/lateral, vertical, braking,propulsion) and temporal spatial parameters (step lengthand width) were measured using an instrumented walk-way.22 Measurements were taken at baseline and 7, 14, 21,28, 42, 56, 84, and 112 days (excluding 84 and 112 days inthe 8 week control group). Parameters were averaged acrosswalks on a given day and measurements were normalized tobody weight.
Passive Joint MechanicsPassive range of motion and stiffness were measured using acustom device.23 Briefly, animals were anesthetized and theforearm was placed in a rotating clamp at 90˚ elbow flexionand 90˚ glenohumeral forward flexion. The scapula wasstabilized manually to isolate glenohumeral motion and thearm was rotated through the full range of internal andexternal rotation three times. Range of motion was calcu-lated by the average of the three maximum values forinternal and external rotation. Joint stiffness was measuredin both the toe and linear regions for both internal andexternal rotation. Measurements were recorded at baselineand at 4, 8, and 16 weeks (excluding 16 weeks in the 8 weekcontrol group). All parameters measured were normalized tobaseline values.
Tendon Mechanical TestingSupraspinatus and humerus tendon-bone units were dis-sected from the shoulder and cleaned of excess soft tissueunder a stereomicroscope. Stain lines were placed along thelength of the tendon using Verhoeff’s stain for optical strainmeasurement. Cross sectional area was measured using acustom laser device as previously described.24 The humeruswas embedded in polymethylmethacrylate (PMMA) andheld in a custom fixture. The tendon was affixed betweenfine grit sand paper using cyanoacrylate and then fixed ina custom grip. Samples were immersed in a 37˚C PBS bathand subjected to a mechanical testing protocol consisting ofa preload to 0.08N, 10 cycles of preconditioning (0.1–0.5Nat 1% strain/s), a stress relaxation to 5% strain (5%/s)followed by a 600 s hold, and finally a ramp to failure at0.3%/s. Following mechanical testing, humeri were wrapped
2 TUCKER ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH MONTH 2016

in PBS-soaked gauze and frozen at �20˚C for subsequentmCT analysis. Stress was calculated as force divided bycross sectional area and 2D Lagrangian optical strain wasdetermined from stain line displacements measured fromimages taken throughout the test using custom trackingsoftware.25,26 Maximum stress and maximum load werecalculated only from samples undergoing physiologicalfailure, including failure at the site of injury or in themidsubstance of the tendon.
Histological AnalysisHistological analysis was performed to assess cell shape,cellularity, and collagen fiber organization at the injury siteand midsubstance of the repaired supraspinatus tendon. Theinjury site was defined as the central portion of the fibrousscar tissue, and the midsubstance as the region proximal tothe myotendinous junction. At the time of sacrifice, supra-spinatus-humerus units were immediately dissected, fixed informalin, and processed using standard paraffin techniques.7mm sections were stained with hematoxylin and eosin(H&E) to assess cell shape, cellularity, and collagen fiberorientation. Cell shape and cellularity were evaluated bythree blinded graders using a semi-quantitative method.Images were graded between 1 and 3 (1¼higher number ofcells and more rounded shape and 3¼ fewer cells and morespindle shaped). A grading scale was created within the setof images at each time point, and at least two images perregion were assessed per specimen. To define the gradingscale, images were blinded and sorted from most to leastnumber of cells (for cellularity) and roundest to most spindleshaped (for cell shape). The ranked images were divided intothree equal groups (Grades 1–3), and the median image fromeach group was assigned as a “standard” for the correspond-ing grades (1–3). Circular standard deviation of collagenfibers was determined by images taken with a polarizingmicroscope and analysis with custom software as describedpreviously.21,26,27
m-Computed TomographymCT scans were performed on the proximal humerus of asubset of humeri (n¼ 6 per group and time point) (vivaCT
40, Scanco Medical AG, Bruttisellen Switzerland). The proxi-mal growth plate was identified, and the region of interestwas defined as the 5mm proximal from the growth plate,which included the greater tuberosity. Scans were performedat 10.5mm resolution. Parameters included bone mineraldensity, bone mineral content, bone volume fraction, totalbone volume, connectivity density, trabecular number, tra-becular spacing, and trabecular thickness.
Statistical AnalysisSample sizes were determined using a priori power analyses.All statistical comparisons were made between the PEMFand non-PEMF groups at the same time points. Mechanicaltesting, mCT, and collagen fiber organization comparisonswere made using student’s t-tests with significance set ap� 0.05. Semi-quantitative histological comparisons weremade using Mann–Whitney U-tests with significance set atp� 0.05. Ambulatory assessment comparisons were madeusing a two-way ANOVA with repeated measures on timewith follow-up t-tests between groups at each time point.Multiple imputations were calculated for a repeated mea-sures analysis for missing data points (�10% per day).Significance was set at p� 0.05.
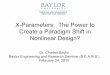
RESULTSQuantitative Ambulatory AssessmentResults indicate no significant difference between thePEMF and non-PEMF groups (Fig. 1).
Passive Joint MechanicsResults indicate no significant difference between thePEMF and non-PEMF groups (Fig. 2).
Tendon Mechanical PropertiesAt 4 weeks, the PEMF group had a significantlysmaller cross-sectional area compared to the non-PEMF group (Fig. 3A). No differences were detected incross-sectional area at 8 and 16 weeks. There were nosignificant differences in percent relaxation at anytime point (Fig. 3B). At 4 and 8 weeks, the PEMF
Figure 1. Ambulatory assessment of left limbs before and after injury and repair did not detect any significant differences in A:braking force, B: propulsion force, C: medial/lateral force, D: stance time, E: stride length, or F: rate of loading at any time point. Datarepresented as mean�SD.
PEMF IMPROVES RAT ROTATOR CUFF HEALING 3
JOURNAL OF ORTHOPAEDIC RESEARCH MONTH 2016

group had significantly increased modulus (100% at4 weeks, 60% at 8 weeks) compared to the non-PEMFgroup, with no differences detected at 16 weeks(Fig. 3C). No differences were detected in stiffness atany time point (Fig. 3D). At 4 weeks, the PEMF grouphad significantly increased maximum stress comparedto the non-PEMF group, with no differences at 8 and16 weeks (Fig. 3E). No differences were detected inmaximum load at any time point (Fig. 3F). At 8 and16 weeks, tendons often failed at a non-physiological
location, primarily at the mechanical testing gripfixture due to high stress concentration. Maximumstress and maximum load data for tendons which didnot fail physiologically (i.e., fail at the injury site) wereexcluded, resulting in a smaller sample size for thesemeasurements. Therefore, remaining right shoulders(n¼3/group/time point) were tested, but failure loca-tion in these samples was also variable. Maximumstress and maximum load for control samples were notcalculated for the same reason. There were no
Figure 2. Shoulder joint stiffness and range of motion. No significant differences were noted in A: internal toe stiffness, B: internallinear stiffness, C: internal range of motion, D: external toe stiffness, E: external linear stiffness, or F: external range of motion at anytime point. Data represented as mean�SD.
Figure 3. Tendon mechanical properties. A: Cross-sectional area was significantly decreased in the PEMF group compared to thenon-PEMF group at 4 weeks. No differences were noted at 8 and 16 weeks (Control area¼ 1.34mm2). B: No differences in percentrelaxation were noted at any time point (Control % relaxation¼47%). C: Modulus was significantly increased by 100% at 4 weeks and60% at 8 weeks in the PEMF group compared to the non-PEMF group. No differences were noted at 16 weeks (Controlmodulus¼ 290.3MPa). D: No differences were noted in stiffness at any time point (Control stiffness¼ 31.15N/mm). E: Maximum stresswas significantly increased at 4 weeks in the PEMF group compared to the non-PEMF group. No differences were noted at 8 and16 weeks. No error bar is present in the PEMF group at 8 weeks due to small sample size with physiological failure (n¼2). F: Nodifferences were noted in maximum load at any time point. Data represented as mean�SD. Due to non-physiological failure location(typically at 8 and 16 weeks); maximum stress and maximum load data points which did not fail physiologically (i.e., at the injury site)were excluded. Control maximum stress and maximum load were not calculated for a similar reason.
4 TUCKER ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH MONTH 2016

differences in failure location for PEMF and non-PEMFspecimens (data not shown).
Histological AnalysisRepresentative images of the injury and midsub-stance locations for PEMF and non-PEMF treatedtendons display similarities in histological charac-teristics at all time points (Fig. 4). At the injurysite, no differences were detected between thePEMF and non-PEMF group in both cell shape andcellularity at any time point (Fig. 5A and B).Additionally, no differences were observed in colla-gen fiber organization at the injury site (Fig. 6A). Inthe midsubstance, at 8 weeks the PEMF group hadsignificantly more rounded cells compared to thenon-PEMF group (Fig. 5D). For collagen fiber orga-nization, the PEMF group had trends towardssignificantly decreased circular standard deviationat both 8 and 16 weeks (Fig. 6B). No other differ-ences were observed in the midsubstance at anytime point.
m-Computed TomographyAt 4 weeks, trabecular thickness was significantlydecreased in the PEMF group compared to the non-PEMF group (Fig. 7H). Additionally, at 4 weeks,connectivity density was significantly increased in thePEMF group compared to the non-PEMF group(Fig. 7E). At 8 weeks, no differences were observed inany parameter. At 16 weeks, the PEMF group hadsignificantly increased bone volume fraction, trabecu-lar thickness, and bone mineral density, and a trendtoward increased bone mineral content compared tothe non-PEMF group (Fig. 7).
DISCUSSIONThis study examined the effect of exposure of acommercially available and FDA approved PEMFwaveform on tendon-to-bone healing in a rat rotatorcuff model. Overall, results suggest that PEMF expo-sure has a positive effect on early rat rotator cuffhealing. Specifically, mechanical properties were dras-tically improved in the PEMF group at both 4 and8 weeks. Of note, modulus was increased by 100% at4 weeks and 60% at 8 weeks, which is a significantimprovement in tissue properties. Histological analysisshowed a more rounded cell shape in the PEMF groupat 8 weeks in the midsubstance. This slight butsignificant finding might suggest inferior tissue, al-though this difference did not result in inferiormechanical properties and was not noted histologicallyat 16 weeks. The more rounded cell shape in thePEMF group at 8 weeks also suggests the cells aremetabolically active due to the PEMF exposure, whichmight support improved mechanical properties at thattime point. Additionally, collagen fiber organization inthe midsubstance at 8 and 16 weeks showed thePEMF group had trends toward significantlydecreased circular standard deviation, suggesting thetissue might be more organized in the PEMF group,which may be related to the improved mechanicalproperties due to previous findings indicating a strongstructure-function relationship in tendon, where fiberalignment was found to correlate significantly withmechanical parameters.28 Lastly, in vivo ambulatoryassessment and shoulder joint function showed mini-mal differences between groups. Particularly, whencomparing to the control group (although no statisticalcomparisons were made), it is apparent that the two
Figure 4. Representative histological images. Injury and midsubstance regions were evaluated at 4, 8, and 16 weeks, andrepresentative images selected (n¼6/group/time point). Scale bar: 100mm.
PEMF IMPROVES RAT ROTATOR CUFF HEALING 5
JOURNAL OF ORTHOPAEDIC RESEARCH MONTH 2016

surgical groups were similar to the control (Figs. 1and 2). This finding implies that the PEMF and non-PEMF groups recover function concurrently and thatPEMF does not negatively affect ambulation andshoulder function. Overall, results suggest that PEMFimproves early tendon-to-bone healing specificallythrough an improvement of tendon mechanical proper-ties. We speculate that PEMF treatment may increasetendon cell metabolism, in turn increasing matrixproduction and collagen remodeling, reflected in im-proved mechanical properties and increased collagenalignment. A small rotator cuff repair clinical trialutilizing a different PEMF signal demonstrated earlyincreases in range of motion and functional scores.14
Our findings provide further evidence of improvementsin mechanical properties and matrix organization,
supporting further investigation into clinical use ofthis therapy for various PEMF waveforms.
Results from this study may support previouslyreported findings using Physio-Stim
1
PEMF therapyto treat healing bone fractures.10,11 mCT analysisshows improved bone properties in the PEMF group(Fig. 7) after transosseous supraspinatus repair, whichfurther supports findings of PEMF exposure leading toimproved bone growth and healing. Therefore, thecurrent study supports the use of PEMF for a rotatorcuff tendon-to-bone healing in both tendon and bone.
This study is not without limitations. Although therat rotator cuff repair model is well established andpublished in over 140 full-length papers to date,animal models do not exactly mimic the clinicalscenario. Additionally, this study utilized an acute
Figure 5. Histological analysis. A: No differences were noted at the injury site in cellularity or B: cell shape at any time point. C: Nodifferences were noted in cellularity in the midsubstance. D: At the midsubstance, cells were more rounded at 8 weeks in the PEMFgroup compared to the non-PEMF group. Shapes denote individual sample scores. Bars denote median score (�p< 0.05).
Figure 6. Collagen fiber alignment. No differ-ences were noted at the injury site in collagenfiber alignment. At the midsubstance, circularstandard deviation trended toward lower values(more organized) at 8 and 16 weeks in the PEMFgroup compared to the non-PEMF group.
6 TUCKER ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH MONTH 2016

supraspinatus detachment and repair whereas clini-cally rotator cuff tears are typically chronic conditionsresultant from repeated overhead motions and over-use. Mechanical analysis was limited by the occur-rence of non-physiological failure during testing, andhistological analysis was limited by the semi-quantita-tive nature of the evaluation. Lastly, animals wereexposed to a systemic PEMF signal. Current FDAapproved devices deliver PEMF locally to the healingtissue. Although systemic PEMF exposure did notseem to negatively affect the animals, future studiesmight examine the effects of localized PEMF exposure.
As this is the first known study to examine andsupport the effect of PEMF exposure on tendon-to-bonehealing in a well-accepted animal model, many futureavenues of study can be investigated. First, the PEMFsignal intensity, frequency, and duration are variable,and the PEMF signal might be optimized to even furtherenhance tendon-to-bone healing. Second, this study onlyexamined supraspinatus tendon-to-bone healing. Investi-gating the effects on other commonly injured tissuesincluding Achilles tendon, patellar tendon, anteriorcruciate ligament, joint replacement, and many otherorthopaedic applications may be advantageous. Addition-ally, PEMF therapy might also be evaluated in tendonsand ligaments with diagnosed tendinitis, tendinopathy,or partial tears to avoid or postpone surgical interven-tion. This application could help to reduce health carecosts and potential morbidities associated with anesthe-sia and surgical procedures.
In conclusion, PEMF exposure improves earlytendon-to-bone healing in an acute rat supraspinatus
detachment and repair model supporting the use in aclinical scenario of rotator cuff healing.
AUTHORS’ CONTRIBUTIONSAll authors have read and approved final version of manu-script. Contributions are as follows: JJT—research design,acquisition of data, data analysis and interpretation, draftingand revision of paper, approval of submitted and final versions;JMC—acquisition of data, data analysis and interpretation,approval of submitted and final versions; TRM—acquisition ofdata, approval of submitted and final versions; CAN—acquisi-tion of data, data analysis, approval of submitted and finalversions; JH—data analysis and interpretation, revision ofpaper, approval of submitted and final versions; EIW—research design, revision of paper, approval of submitted andfinal versions; NZ—research design, revision of paper, ap-proval of submitted and final versions; JTR—research design,revision of paper, approval of submitted and final versions;LJS—research design, data interpretation, revision of paper,approval of submitted and final versions.
REFERENCES1. Galatz LM, Ball CM, Teefey SA, et al. 2004. The outcome
and repair integrity of completely arthroscopically repairedlarge and massive rotator cuff tears. J Bone Joint Surg Am86-A:219–224.
2. Lovric V, Ledger M, Goldberg J, et al. 2013. The effects oflow-intensity pulsed ultrasound on tendon-bone healing in atransosseous-equivalent sheep rotator cuff model. Knee SurgSports Traumatol Arthrosc 21:466–475.
3. Springer J, Badgett RG. 2015. Optimized extracorporealshock-wave therapy improved pain and functioning inchronic plantar fasciitis. Ann Intern Med 163:JC8.
4. Mardani-Kivi M, Karimi Mobarakeh M, Hassanzadeh Z,et al. 2015. Treatment outcomes of corticosteroid injection
Figure 7. mCT analysis. A: No differences were noted in bone mineral density at 4 and 8 weeks. At 16 weeks bone mineral densitywas significantly increased in the PEMF group compared to the non-PEMF group. B: No differences were noted in bone mineralcontent at 4 and 8 weeks. At 16 weeks bone mineral content trended toward a significant increase in the PEMF group compared to thenon-PEMF group. C: No differences were noted in bone volume fraction at 4 and 8 weeks. At 16 weeks bone volume fraction wassignificantly increased in the PEMF group compared to the non-PEMF group. D: No differences were noted in bone volume at any timepoint. E: At 4 weeks connectivity density was significantly increased in the PEMF group compared to the non-PEMF group. Nodifferences were noted at 8 and 16 weeks. F: No differences were noted in trabecular number at any time point. G: No differences werenoted in trabecular spacing at any time point. H: At 4 weeks trabecular thickness was significantly decreased in the PEMF groupcompared to the non-PEMF group. No differences were noted at 8 weeks. At 16 weeks trabecular thickness was significantly increasedin the PEMF group compared to the non-PEMF group. Data represented as mean�SD.
PEMF IMPROVES RAT ROTATOR CUFF HEALING 7
JOURNAL OF ORTHOPAEDIC RESEARCH MONTH 2016

and extracorporeal shock wave therapy as two primarytherapeutic methods for acute plantar fasciitis: a prospectiverandomized clinical trial. J Foot Ankle Surg 54:1047–1052.
5. Foley KT, Mroz TE, Arnold PM, et al. 2008. Randomized,prospective, and controlled clinical trial of pulsed electro-magnetic field stimulation for cervical fusion. Spine J 8:436–442.
6. Garland DE, Moses B, Salyer W. 1991. Long-term follow-upof fracture nonunions treated with PEMFs. Contemp Orthop22:295–302.
7. Goodwin CB, Brighton CT, Guyer RD, et al. 1999. A double-blind study of capacitively coupled electrical stimulation asan adjunct to lumbar spinal fusions. Spine (Phila Pa 1976)24:1349–1356; discussion 1357.
8. Linovitz RJ, Pathria M, Bernhardt M, et al. 2002. Combinedmagnetic fields accelerate and increase spine fusion: adouble-blind, randomized, placebo controlled study. Spine(Phila Pa 1976) 27:1383–1389; discussion 1389.
9. Mooney V. 1990. A randomized double-blind prospectivestudy of the efficacy of pulsed electromagnetic fields forinterbody lumbar fusions. Spine (PhilaPa 1976) 15:708–712.
10. Midura RJ, Ibiwoye MO, Powell KA, et al. 2005. Pulsedelectromagnetic field treatments enhance the healing offibular osteotomies. J Orthop Res 23:1035–1046.
11. Midura RJ. 2013. The effects of bone growth stimulatortreatments on vertebral bone mass in an osteoporosis model.New Orleans, Louisiana: North American Spine Society 28thAnnual Meeting.
12. Willardson R, Coughlin D, El Naga A, et al. 2013. Pulsedelectromagnetic fields have an acute anti-inflammatoryeffect on intervertebral disc cells. San Antonio, Texas, USA:Orthopaedic Research Society.
13. Uzunca K, Birtane M, Tastekin N. 2007. Effectiveness ofpulsed electromagnetic field therapy in lateral epicondylitis.Clin Rheumatol 26:69–74.
14. Osti L, Del Buono A, Maffulli N. 2015. Pulsed electromag-netic fields after rotator cuff repair: a randomized, controlledstudy. Orthopedics 38:e223–e228.
15. Straugh B, Patel MK, Rosen DJ, et al. 2006. Pulsedmagnetic field therapy increases tensile strength in a ratAchilles’ tendon repair model. J Hand Surg 31A:1131–1135.
16. Soslowsky LJ, Carpenter JE, DeBano CM, et al. 1996.Development and use of an animal model for investigationson rotator cuff disease. J Shoulder Elbow Surg 5:383–392.
17. Beason DP, Connizzo BK, Dourte LM, et al. 2012. Fiber-aligned polymer scaffolds for rotator cuff repair in a ratmodel. J Shoulder Elbow Surg 21:245–250.
18. Beason DP, Tucker JJ, Lee CS, et al. 2014. Rat rotator cufftendon-to-bone healing properties are adversely affected byhypercholesterolemia. J Shoulder Elbow Surg 23:867–872.
19. Caro AC, Tucker JJ, Yannascoli SM, et al. 2014. Efficacy ofvarious analgesics on shoulder function and rotator cufftendon-to-bone healing in a rat (Rattus norvegicus) model.J Am Assoc Lab Anim Sci 53:185–192.
20. Connizzo BK, Yannascoli SM, Tucker JJ, et al. 2014. The detrimen-tal effects of systemic Ibuprofen delivery on tendon healing aretime-dependent. Clin Orthop Relat Res 472:2433–2439.
21. Gimbel JA, Van Kleunen JP, Williams GR, et al. 2007. Longdurations of immobilization in the rat result in enhancedmechanical properties of the healing supraspinatus tendoninsertion site. J Biomech Eng 129:400–404.
22. Sarver JJ, Dishowitz MI, Kim SY, et al. 2010. Transientdecreases in forelimb gait and ground reaction forces follow-ing rotator cuff injury and repair in a rat model. J Biomech43:778–782.
23. Sarver JJ, Peltz CD, Dourte L, et al. 2008. After rotator cuffrepair, stiffness-but not the loss in range of motion-increasedtransiently for immobilized shoulders in a rat model.J Shoulder Elbow Surg 17:108S–113S.
24. Favata M. 2006. Scarless healing in the fetus: implicationsand strategies for postnatal tendon repair. Philadelphia:University of Pennsylvania.
25. Bey MJ, Song HK, Wehrli FW, et al. 2002. A noncontact,nondestructive method for quantifying intratissue deforma-tions and strains. J Biomech Eng 124:253–258.
26. Thomopoulos S, Williams GR, Gimbel JA, et al. 2003.Variation of biomechanical, structural, and compositionalproperties along the tendon to bone insertion site. J OrthopRes 21:413–419.
27. Gimbel JA, Van Kleunen JP, Mehta S, et al. 2004. Supra-spinatus tendon organizational and mechanical properties ina chronic rotator cuff tear animal model. J Biomech37:739–749.
28. Lake SP, Miller KS, Elliott DM, et al. 2009. Effect of fiberdistribution and realignment on the nonlinear and inhomo-geneous mechanical properties of human supraspinatustendon under longitudinal tensile loading. J Orthop Res27:1596–1602.
8 TUCKER ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH MONTH 2016