Embed Size (px)
Citation preview

! The Northern Ohio Foot and Ankle Journal Official Publication of the NOFA Foundation
Purpura Fulminans in the Lower Extremity: A Case Report and Review by Dustin Huntsman DPM1, Chad Knight, DPM2 and Michael Maier, DPM3
The Northern Ohio Foot and Ankle Journal 4(22): 1-4
Abstract: Purpura fulminans (PF) is an extremely rare condition that is associated with very high mortality rates secondary to severe multi-systemic thrombotic events. The mechanism by which this occurs is poorly understood but is often associated with bacterial infections. Patients who survive are often faced with extensive skin necrosis, resulting in amputations and significant scarring. Early recognition, treatment with anticoagulation, transfusion of deficient proteins, eradication of infection, and delayed surgical debridement are essential in management of PF. In this case report we discuss the case of PF in a 34-year-old intravenous drug user (IVDU).
Key words: purpura fulminans, disseminated intravascular coagulation, protein C deficiency
Accepted: February, 2018 Published: March, 2018
This is an Open Access article distributed under the terms of the Creative Commons Attribution License. It permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ©The Northern Ohio Foot and Ankle Foundation Journal. (www.nofafoundation.org) 2014. All rights reserved.
Purpura fulminans is a rare disorder
characterized by rapid skin necrosis and disseminated
intravascular coagulation (DIC). It is postulated that a
deficiency of protein C and dysfunction of the
protein C-thrombomodulin pathway, as well as other
systems, exert a negative regulatory effect on
coagulation but overall the mechanism is still poorly
understood [1]. Acute sepsis, viral or bacterial
infections and coagulopathy have been found to
trigger PF [5]. PF occurs most frequently in pediatrics
with a history of meningococcemia. Purpuric lesions
on the upper and lower extremities are characteristic
of PF. Skin necrosis is a result of acute thrombotic
events in small Address correspondence to: [email protected]. 1Podiatric Medicine and Surgical Resident, Mercy Regional Medical Center. 2Podiatric Medicine and Surgical Resident, CCF-Oklahoma City. 3Podiatric Medicine Physician, Cleveland Clinic.
to medium sized blood vessels [4]. In severe instances,
multi-systemic thrombotic events can lead to multi-
The Northern Ohio Foot & Ankle Foundation Journal, 2018

Volume 4, No. 22, March 2018 Huntsman, Knight, Maier
organ failure and/or death [5]. There is no consensus
on the most appropriate treatment because there are
only a few studies, with limited sample sizes, to draw
from. Early recognition and aggressive supportive
management have been essential in decreasing the
mortality rates. It is estimated that greater than 50%
of patients will undergo surgical debridement and/or
partial/total limb amputation [6]. Surgical timing is of
debate in the literature and can be controversial. Some
authors suggest early surgical debridement while
others recommend delaying surgical intervention until
demarcation to maintain maximum limb length and
prevent unnecessary surgeries [8]. Clinicians should
use caution and clinical judgment when treating
patients with PF. The goal of treatment is to preserve
maximal functionality without causing additional
systemic inflammatory insult [4].
Methods
A search of the literature was conducted regarding PF until February 2018. References from the appropriate articles were also reviewed to find all reports and outcomes of PF in the literature.
Case Report
A 34-year-old female IVDU was transferred from an outside hospital after sustaining a fall at home. She reported several episodes of nausea, vomiting, and anterior chest pain. Her past medical history was significant for hepatitis C and acute MRSA tricuspid valve endocarditis. Her past surgical history was
positive for tricuspid valve repair and permanent pacemaker placement one year ago.
Patient was transferred to the intensive care unit (ICU) febrile and intubated. She had profound septic shock with acute respiratory failure, and acute kidney injury. On physical exam, the patient had palpable radial pulses and audible dorsalis pedis and posterior tibial pulses upon Doppler ultrasound bilaterally. Dermatologically, cyanotic to violaceous hues were noted to the nose, ears, arms and legs. Stellate purpuric plaques were also noted on the arms and legs along with scattered bullae to the lower extremities. Skin temperature was warm to cold, from the tibial tuberosity to the lesser digits. Neurologically, protective sensation was absent distal to the midfoot on the left and intact on the right. Musculoskeletal examination was deferred due to pain.
! ! Figure 1. Diffuse purpura and bullae formation Laboratory findings were significant for leukocytosis, low fibrinogen and protein C, elevated aPPT, PT, and D-Dimer. Given her clinical presentation and laboratory findings the diagnosis of PF was made and heparin and protein C concentration were administered.
Several imaging studies were performed. Radiographs of bilateral feet were unremarkable. Transesophageal echocardiography showed vegetations on the repaired tricuspid valve, which later required a subsequent repair of her tricuspid valve. Bilateral lower extremity venous duplex ultrasounds were positive for deep vein thromboses in bilateral popliteal veins.
Throughout her hospitalization, her dermatological
exam continued to worsen. On the right lower
extremity, necrotic lesions were noted to the
The Northern Ohio Foot & Ankle Foundation Journal, 2018

Volume 4, No. 22, March 2018 Huntsman, Knight, Maier
anterolateral and posterior aspect of the leg. The
distal tufts of toes 3-5 developed gangrenous
changes. On the left lower extremity, necrosis was
noted to the anterolateral aspect of the leg, to the
entire forefoot and to the plantar lateral aspect of the
midfoot and rearfoot. All wounds appeared to be dry
and stable with mild peri-wound erythema.
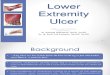
! Figure 2a. Increased necrosis, after 30 days, to the right lower extremity.
!
Figure 2b. Increased necrosis, after 30 days, to the
left lower extremity.
A multi-specialty decision was made to delay surgical
debridement and continue conservative treatment,
which consisted of betadine wet to dry dressings and
semi-occlusive Vaseline gauze to areas of necrosis, to
allow for full demarcation of all wounds. The patient
was discharged and will undergo a below-the-knee
amputation on the left and distal symes amputations
to the affected digits on the right.
!Figure 3. Progressive necrosis noted after 60 days
Discussion
The prevalence and incidence of PF is not exactly known but is rare, especially in the adult population. PF presents acutely with painful skin lesions, erythematous macules, and purpuric rashes with vesicles and bullae. There are other conditions with purpuric entities such as calciphylaxis, necrotizing fasciitis, thrombotic thrombocytopenic purpura, meningococcemia, and toxic shock syndrome [4].
The mechanism of infectious causes is not well understood. Treatment of sepsis-induced PF is centered on supportive management, usually in the ICU. Early recognition is key. Typical management includes ventilation, fluid resuscitation, pressor support, and blood transfusions [4]. Heparin infusion has shown a 12% mortality reduction in sepsis and DIC [12]. Evidence of the use of activated protein C and high-dose anti-thrombin have failed to show a decrease in the mortality rates and is reserved for severe cases [13]. Many physicians are faced with the decision to use vasopressors, which are known to significantly increase the risk of acral necrosis in patients with sepsis, endocarditis, DIC and vasculitis. It is recommended that pressor support be used with caution in these patients. Modern medicine has increased the survival rates and early recognition of
The Northern Ohio Foot & Ankle Foundation Journal, 2018

Volume 4, No. 22, March 2018 Huntsman, Knight, MaierPF throughout recent years, which has changed the timing of surgical intervention.
With decreasing mortality rates, there is increasing controversy of surgical debridement and sequel management. Surgical treatment is aimed at preserving maximum functionality and limb length. Davis et al. performed early fasciotomies in 9 pediatric patients without evidence of preventing amputation in those patients. There has been controversy over acute intervention versus delayed surgical intervention. The trend throughout the literature is towards delayed surgical debridement, to allow the soft tissue to fully demarcate before intervening. However, there is a report of 7% of patients with PF having compartment syndrome requiring early fasciotomies [9].
Most of the literature represents cases in the pediatric population. There are few reported cases in adult patients, such as ours. In the pediatric population skin grafts, free flaps, and advanced wound care products have been described with success. Many studies, such as Pino et al., report the success of semi-occlusive material in preserving length of digits, when treating these wounds conservatively.
PF is an extremely rare and complex condition. Patients present with extensive past medical histories and severe systemic illnesses including systemic shock, multi-organ failure, DIC and extensive soft tissue necrosis. Due to the impending and extensive necrosis, the morbidity associated with PF is crippling. Mortality rates vary throughout the literature and may range from 25-44%. Roughton et al. reported a 44% mortality rate in nine patients with PF [5, 12]. Treatment should be focused on early recognition, supportive treatment, delayed surgical debridement, and semi-occlusive dressings for conservative management, in order to maximize functional outcomes.
References 1. Colling, Meaghan E., and Pavan K. Bendapudi. "Purpura Fulminans: Mechanism and Management of
Dysregulated Hemostasis." Transfusion medicine reviews (2017).
2. Chalmers E, Cooper P, Forman K, Grimley C, Khair K, Minford A, Morgan M, Mumford AD (2011). "Purpura fulminans: recognition, diagnosis and management". Arch Dis Child. 96 (11): 1066–1071.
3. Ghosh SK, Bandyopadhyay D, Dutta A (2009). "Purpura fulminans: a cutaneous marker of disseminated intravascular coagulation". West J Emerg
4. Pino, Paula A., Javier A. Román, and Felipe Fernández. "Delayed Surgical Debridement and Use of Semiocclusive Dressings for Salvage of Fingers After Purpura Fulminans." HAND 11.4 (2016): NP34-NP37.
5. Davis, Mark DP, Katrina M. Dy, and Steven Nelson. "Presentation and outcome of purpura fulminans associated with peripheral gangrene in 12 patients at Mayo Clinic." Journal of the American Academy of Dermatology 57.6 (2007): 944-956.
6. Davies, MS, Nadel, S, Habibi, P, Levin, M, Hunt, DM. The orthopaedic management of peripheral ischaemia in meningococcal septicaemia in children. J Bone Joint Surg Br. 2000;82(3):383-386
7. MacLennan, SE, Kitzmiller, WJ, Yakuboff, KP. Free-tissue transfer for limb salvage in purpura fulminans. Plast Reconstr Surg. 2001;107(6):1437-1442
8. Warner, PM, Kagan, RJ, Yakuboff, KP Current management of purpura fulminans: a multicenter study. J Burn Care Rehabil. 2003;24(3):119-126
9. Childers, Ben J., and Brando Cobanov. "Acute infectious purpura fulminans: a 15-year retrospective review of 28 consecutive cases." The American Surgeon 69.1 (2003): 86-90.
10. Edlich, Richard, et al. "Modern concepts of the diagnosis and treatment of purpura fulminans." Journal of Environmental Pathology, Toxicology and Oncology 27.3 (2008).
11. Roughton, Michelle C., Shailesh Agarwal, and Lawrence J. Gottlieb. "Surgical management of acute infectious purpura fulminans." Journal of Burn Care & Research 32.2 (2011): 231-236.
The Northern Ohio Foot & Ankle Foundation Journal, 2018

Volume 4, No. 22, March 2018 Huntsman, Knight, Maier12. Yamakawa K, Ogura H, Fujimi S, et al. Recombinant human soluble thrombomodulin in sepsis-induced disseminated intravascular coagulation: a multicenter propensity score analysis. Intensive Care Med. 2013;39(4):644-652
13. Warren BL, Eid A, Singer P, et al. Caring for the critically ill patient. High-dose antithrombin III in severe sepsis: a randomized controlled trial. JAMA. 2001;286(15):1869-1878.
The Northern Ohio Foot & Ankle Foundation Journal, 2018