Embed Size (px)
Citation preview

Putting Prevention and Health Promotion into Practice in EU Regions
North West England
Dominic HarrisonDeputy Regional Director for Public Health
Department of Health

Issues
• Paradigm Shifts – – Public Sector, NHS, Regions, Performance
Management systems.• NHS Reform
– The Darzi Review of NHS– World Class Commissioning– Future Scenario Testing
• Wider Health Strategy – Local Area Agreements/ Multi Area Agreements– Investment for Health / Health Inequalities– Health and well-being as economic development

Paradigm ShiftsFor the public sector
– From “detect and manage to predict and prevent”– From “How do we best make use of health sector resources to
secure health outcomes” to “How do we best mobilise all public sector investment (on this footprint) to secure the shared aspirations of this community (across all sectoral outcomes)”
– From “public as consumer to public as co-producer”
For the NHS– From a focus on “effective management of service delivery” to
effective commissioning of health outcomes.– From “commissioning services to commissioning outcomes”
For Regions– From “how do we command and control this system to deliver
health outcomes” to “how do we assure this system functions to deliver outcomes”.
For Performance Assessment – From “How well does this institution deliver its own target” to
“how well does this partnership deliver all agreed targets. (CAA)

Local Area Agreements
• Agreement between Central and local government for 3 years following Comprehensive Spending Review
• 35 targets agreed (out of a national indicator set of about 198)
• Negotiated by regions with Local Strategic Partnerships LSPs at local level
• Signed off by all Ministers with rewards for delivery.

Local priorities and targets
~35 targets
LAA
Local accountability to citizens
Local consultation through the LSP with Partners and Stakeholders
Better outcomesfor citizens
CSR07 national priority outcomes & 198 national
indicatorsLSP view of local priorities
Local targets monitored by LSP
'Designated’ targets monitored by LSP and GO
new LAAs
Local Challenges and AmbitionsSustainable Community
Strategy
Negotiation and agreementCross-Govt view through GOs on priorities
16 statutory education and early years targets

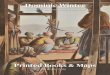
PRINCIPAL RELATIONSHIPS INTHE NEW LOCAL PERFORMANCE FRAMEWORK
LOCAL DELIVERY PARTNER
LOCAL DELIVERY PARTNER
LOCAL AUTHORITY
CENTRAL GOVERNMENT DEPARTMENT
CENTRAL GOVERNMENT DEPARTMENT
CENTRAL GOVERNMENT DEPARTMENT
CENTRAL GOVERNMENT DEPARTMENT
CENTRAL GOVERNMENT DEPARTMENT
GOVERNMENT OFFICE
Agree local priorities through a Sustainable Communities Strategy, informed by local context, national priorities and engagement with local citizensand business
Negotiate and agree proposed LAAs , selected MAAsand how they will deliver outcomes, through ongoing, evidence-based, system-wide dialogue
Agree national priorities through the Comprehensive Spending Review , PSAs and National Indicator Set
5
3
Deliver LAAs and MAAs, adapting to changing national and local contexts
4
OUTCOMES FOR PEOPLE AND PLACES
Audit Commission and other inspector-
ates
6
LGAIDeA
Leadership CentreRIEPs
CLG
GO Network
PMDU
LOCAL DELIVERY PARTNER
LOCAL DELIVERY PARTNER
1
2
Build system-wide capacity and capabilities
•National Improvement and Efficiency Strategy
•Government Office transformation
•Capability reviews of central government departments
Carry-out effective performance management and inspection
•Local performance management
•Government Office performance dialogues
•System leadership and oversight
•Risk-based assessment through CAA
CLG
GOs
Local Area Agreements

MAAs
7
Tyne and Wear
Hull and Humber
Tees Valley
Leeds
South Yorks
Leicester/Leicestershire
Bournemouth, Dorset and Poole
Fylde Coast
Pennine Lancs
Manchester
Liverpool
Black Country
West of England
PUSH – Partnership for Urban South Hampshire
South Essex
Olympic Boroughs
North Staffordshire
North Kent
Bedfordshire and Luton
Partnerships in discussion with Govt- no specified signing date
Partnerships negotiating MAAswith Govt- sign-off likely Spring 09
Partnerships negotiating MAAswith Govt- sign-off likely Autumn 08
MAAs signed off
Nottingham/Nottinghamshire

2000 2002 2004 2006 2008 2010 2012
The NHS journey
Targets and
performance management
Commissioning organisations
Autonomous providers
Payment by results
Patient choice
‘REFORM’Journey
Local Capability & Self-improvement
Breakthrough & Innovation
Social Movements
Co-creation
Some keyoutcomes
• key illnesses• throughput
• capacity
• health priorities• waiting times
• financial stability
• quality, safety• responsiveness•Joined up care
• health & well-being• equity
‘LEADERSHIP’ Journey
Technical LeadershipAdaptive Leadership
Target setter +
Performance manager +
Delivery leader
Regulator +
National Standards +
System leader
Transforming the service
Introducing the reform levers
Building capacity in the system
‘SERVICE” Journey

New National /Regional NHS Strategy
Healthier Horizons for the North West

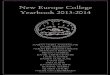
We have designed a stratified approach to long-term conditions. If we successfully prevent & treat, equally
according to need, we would reduce the inequalities morbidity gap
Case-Management of vulnerable people most at
riskPreventing escalation to
emergency admission
Improved disease management
Preventing escalation to high complexity condition
Improved self-care
Preventing escalation to high risk condition
Level 3: High
ComplexityConditions
Level 2: High risk
Conditions
Level 1: 70-80% of LTC population
Have a LTC
EmergencyAdmission
Cost o
f Tre
atm
en
t
Distre
ss to P
atie
nt
Managing LTC Conditions
£
££££Case-Management of
vulnerable people most at risk
Preventing escalation to emergency admission
Improved disease management
Preventing escalation to high complexity condition
Improved self-carePreventing escalation to
high risk condition
Level 3: High
ComplexityConditions
Level 2: High risk
Conditions
Level 1: (70 -80% of LTC population)
Have a LTC
EmergencyAdmission
Cost o
f Tre
atm
en
t
Distre
ss to In
div
idu
al
Managing LTCs
£
££££

10.2 m
19.9 m
2.6 m
17.1 m
High Risk Have LTC (aware and unaware)
Aware of LTC
Eligible for treatment
Optimal treatment
Compliant with treatment
5.7m
2.6m 2.3m1.3m 1m
2.8m1.8m 1.8m
0.4m Not known
0.9m 0.48m 0.21m 0.1m 0.08m
2.9m
0.9m0.52m 0.26m 0.14m
DiseasePrevention
Patient identification and diagnosis
Treatment and ongoing management
CHD
Diabetes
CHF
COPD
Long-term conditions/Chronic Disease Management (England)

SHA/DHPCT DH
Our strategic ambition is becoming clearer – and should all be connected
Regional
Regional enablement, assurance and system management
‘Healthier horizons’NHS NW Strategic Framework
National
Darzi review
World class commissioning assurance process/guidance
System management paradigm and tools
Local
PCT as local leaders of the NHS
World class commissioners
Local system managers
Local delivery of strategic ambition for NHS in region, and national Darzi commitments

Effectiveness
Time business as usual reformed system transformed system
•‘big is best’, •User adapts to provider characteristics•Standardisation rules
•Example: mainframe computers
The ‘Three Horizons’ Model – Improving the present while preparing for the Future
•‘small can sometimes be beautiful•Greater user choice•Less uniformity•Focus on greater efficiency and on outputs
-Example: growth of market for personal computers
- Small is best •dispersed, flexible, local models •Services moulded around users•Dynamic user engagement•Focus on changed relationship between service/product and those who use it
Example: the digital revolution, internet

I will be living a healthier lifestyleI will receive more
personalised care
My NHS will maintain a
healthy financial position andperform the
best in class
I will have betterCustomer care
and an improved patient experience
I will receive the most informed technologies
as part of my care
I will be more involved in
decisions madeby the NHS
I will be givenhigher qualityclinical care My family will have
a better opportunityto live a longer and
healthier life
I will get more integrated seamless
care, when I need helpfrom more than one
organisation10 Public
TouchstonesI will receive more of my care closer
to my home

PCTs have to improve the present whilst simultaneously preparing for
the future
Improving the Present:
• PCTs have to manage the health care ‘machine’ more effectively.
Preparing for the Future:
• PCTs also have to lead their local health ‘system’
• NHS has to get smarter at enabling prevention and foster health in different environments
PCTs must learn to use the healthcare ‘machine’ to prepare for the future more effectively - prevention; consciously promoting independence and reducing dependency
Health care and prevention are not mutually exclusive

VISION AND COMPETENCIESVISION AND COMPETENCIES
ASSURANCE SYSTEMASSURANCE SYSTEM
SUPPORT ANDDEVELOPMENT MODEL
SUPPORT ANDDEVELOPMENT MODEL

PCTs as local leaders of the NHS
• The World Class Commissioning vision is to create self improving health commissioning organisations, responsive to the needs and aspirations of citizens, drawing on the best of public, private and third sector provision.
• Focused on, and held accountable for delivering outcomes for local people
• Freed from top-down ‘push’

Assess needs
Assess needs
Review current service
provision
Review current service
provisionDecide
prioritiesDecide
priorities
Strategic planningDesign serviceDesign service
Shape structure of
supply
Shape structure of
supply
Specify outcomes &procure services
Manage demand
and ensure appropriate access to
care
Manage demand
and ensure appropriate access to
care
Clinical decision making
Clinical decision making
Managing performance
(quality, performance,
outcomes)
Managing performance
(quality, performance,
outcomes)
Managing demand and performance

11 World Class Commissioning Competencies

CONTROL OVER MEANS OF DELIVERY?
The Four Scenarios
PO
LIC
Y E
MP
HA
SIS
?
Curing Sickness
Improving Health & Wellbeing
Co
mm
erc
ial P
rovid
ers
Are
D
om
inan
t
Lo
cal C
om
mu
nitie
s A
re D
om
inan
t
Scenario 1
“Corporate Cures”
Scenario 2
“CommunityCures”
Scenario 4
“Living for Health”
Scenario 3
“Shopping for Health”
Strategic Scenarios


www.internationalfuturesforum.com

Societal influencesIndividual psychology
Biology
Activity environment
Individual activityFood
ConsumptionFood Production

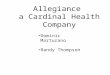
Male Life Expectancy Gaps
-7%
-6%
-5%
-4%
-3%
-2%
-1%
0%
1%
2%
1995-1997 1996-1998 1997-1999 1998-2000 1999-2001 2000-2002 2001-2003 2002-2004 2003-2005
three years (pooled_
Per
cen
tag
e d
iffe
ren
ce f
rom
En
gla
nd
Bolton
Bury
Manchester
Oldham
Rochdale
Salford
Stockport
Tameside
Trafford
Wigan

Components of the Male GapMale Reduced Life Expectancy - compared to E&W average
Persons under 75 dying in Manchester: trend 1995-97 through to 2003-2005
-8 -3 2 7 12
other causes
diabetes
other cancer
lip, oral and oesophagus cancer
colorectal cancer
prostate cancer
lung cancer
digestive disease (inc. cirrhosis)
other circulatory disease
stroke
coronary heart disease
other respiratory disease
bronchitis and copd
other accidents
self harm
violence
accidental overdose and poisoning
infant mortality
ca
teg
ory
of
de
ath
gap between local and national life expectancy in months of life lost (plus values indicate higher mortality)
1995-97
1998-00
2001-03
2003-05

Health and productivity costs of alcohol misuse are around £4 billion.
8%
24%
27%
33%
3%5%
0%
Inpatient
A & E
Outpatient
GPs
Other primary care
Dependency drugs
Alcohol services
Estimated annual cost of alcohol misuse (2003)
A&E
£510m
Inpatient
£618m
Alcohol Services
£96m
The Alcohol Harm Reduction Strategy (2003) estimated total annual healthcare
costs related to alcohol misuse to be up to £1.8bn. The bulk of these costs are born
by the NHS.
Estimated cost of alcohol-related productivity lost (2003)
Sou
rce:
Alc
oh
ol C
on
cern
(2
00
2);
Bri
tton
an
d m
acp
hers
on
(2
00
1);
WH
O
(20
00
); N
ett
en
an
d C
urt
is (
20
02
); H
AD
& M
OR
I (2
00
3);
Leon
tari
di (2
00
3)
all
qu
ote
d in
PM
SU
In
teri
m A
naly
tica
l R
ep
ort
Other
£64mGeneral Practice
£146m
Outpatient
£445m
Sickness absence
Reduced employment
Premature mortality
Alcohol-related premature death costs £2.4bn in productivity
foregone
Excess drinking is associated with unemployment. Costs arising from such
reduced employment are estimated to be in the region of £1.9bn per year.
Sickness absence costs
£1.5bn

A newnew attempt to make an impactimpact on
healthhealth in the North WestNorth West
To achieve:
• a public motivated and able to protect its own health
• an environment that supports healthy lifestyle choices.

• “Coalitions for better health” - Darzi
• “Social movement for health” - DH
• Social movements and large scale change in the NHS – Helen Bevan
• Public empowerment - Darzi
A new language for the public sector

1. Significant interest in Our Life from public sector and business leaders
2. Big Drink Debate – 33,000 responses
3. Enormous buy-in from NHS, police, fire, ambulance, local government and voluntary sector to the need for this new approach
Progress

We are the culture
We need to consider how our actions and decisions as leaders, parents, and role models establish and reinforce cultural norms
“We need a culture change”

A movement of “leaders”
From the public sector, businesses, faith groups, community groups and among the public
People willing to commit themselves and their organisations and networks to action to change cultural norms
Leading by example