Embed Size (px)
Citation preview

QOL AND OTHER PATIENT-RELATED OUTCOMES IN PSYCHIATRY OF ID
Marco BertelliPsychiatrist, Psychotherapist
Consultant for Intellectual Disability and Autistic Spectrum Disorders
CREA (Centro di Ricerca ed Evoluzione AMG) Director
WPA-SPID (World Psychiatric Association – Section Intellectual Disability) Chair
SIRM (Società Italiana per lo studio del Ritardo Mentale)

Dott. Marco BertelliDeclaration of Interest
Medico ChirurgoPsichiatra – Psicoterapeuta
Libero Professionista
Consulente AMG FirenzeConsulente Consorzio Zenit FirenzeResponsabile Sanitario Cooperativa Sociale WORK 2000 Castiglion Fiorentino (AR)Direttore MAPPsi (Medici Associati per la Psichiatria e la Psicoterapia) FirenzeDirettore CREA (Centro di Ricerca ed Evoluzione AMG), Firenze
Presidente della sezione Psichiatria della Disabilità Intellettiva dell’Associazione Mondiale di Psichiatria (WPA-SPID)Segretario della Società Italiana per lo studio del Ritardo Mentale (SIRM)Segretario e Fondatore dell’Associazione Italiana per lo studio della Qualità di Vita (AISQuV)
Ha avuto rapporti di collaborazione con le seguenti case farmaceutiche:FarmadesNovartisJanssenAttualmente è consulente ad incarico di Eli Lilly Italia

Effectiveness
Quality of Life
Subjective Wellbeing
Long-term cost/benefits
ASSESSING USEFULNESS OF MEDICATION:NEW OUTCOME MEASURES
Efficacy on symptoms / PBs
Normalization
Clinical improvement
Short-term costs
Bertelli M., 2006

MEETING EVERYDAY CHALLENGES:ANTIPSYCHOTIC THERAPY
IN THE REAL WORLD
• Methanalysis of RCT
• RCT with large sample
• RCT with small sample
• Non-randomized trials controlled with current control group
• Non-randomized trials controlled with historical control group
• Non-randomized trials without control group
• Expert consensus
• Case report
Bertelli 2006, modified from Sackett, 1989
REAL WORLD
IDEAL EXPERIMENTAL EFFICACY

IL CONCETTO DI EFFICIENZA DI TRATTAMENTO
Efficacy Tolerability and Safety
Adeherence/Stay on treatment
Effectiveness
Lieberman JA, et al. N Engl J Med. 2005;353(12):1209-1223; Lehman AF, et al. Am J Psychiatry. 2004;161(2 suppl):1-56; Swartz MS, et al. Schizophr Bull. 2003;29(1):33-43.

SCHIZOPHRENIA PATIENTS STAYING ON TREATMENT SHOW BETTER TREATMENT
RESPONSE COMPARED TO PATIENTS DISCONTINUING TREATMENT
Liu-Seifert H, et al. Schizophr Bull 2005;31(2):487.
† Early response predicted study completion: A 20% improvement in PANSS total score by 2 weeks was associated with an approximately 80% greater likelihood of study completion (odds ratio 1.76, confidence interval (1.4, 2.21), p<.0001).
50
60
70
80
90
100
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
Weeks
Completers
Discontinued
*
**
** * *
*p<.001
Mean P
AN
SS
Tota
l S
core
(O
C)
Impro
vem
ent
Study Methodology
♦ 4 clinical trials, duration of 24 to 28 weeks
♦ N=1627
♦ Diagnosis
• Schizophrenia 78.5%
• Schizoaffective 20.84%
• Schizophreniform 0.6%
♦ Mean age 39.53 ± 10.85
♦ Age of onset of illness:
23.48 ± 8.26
♦ 64.4% Male
♦ 53.3% Caucasian

SCHIZOPHRENIC PATIENTS COMPLETINGTHE TREATMENT HAVE A QoL IMPROVEMENT
Zhao F, et al. Schizophr Bull 2005;31(2):508.
45
50
55
60
65
0 4 8 12 16 20 24
Weeks on Antipsychotic Therapy
QLS
Tota
l S
core
(O
C)
Completers
Discontinued
Number of patients at each time point:
Completers: 856 851 844 838
Discontinued:
961 707 274 83
*
*p<.05

WHAT IS QUALITY OF LIFE?
A. a sociological concept
B. a media phenomenon
C. a new outcome measure for medical and rehabilitative interventions
D. a new definition of health
E. all the previous
F. none of the previous

QoL: PRINCIPLES AND IMPLICATIONS
• human entitlement to a life of quality
• Universality of human characteristics
• Uniqueness of human needs, behaviours and
performances (choice)
• Human attitude to self-fulfilment (self
perception, self image)
• Holism in human life
• Dynamic nature of human life (growth,
improvement, life-span)
R.I. Brown and I.Brown. Principles of quality of life and their application: an overview. JIDR, 2004, 48; 4-5; 447

1. Burns T. and Patrick D. Acta Psychiatr Scand, 2007; Patterson TL. and Leeuwenkamp OR. Schiz Res, 2008 2. Wehmeier P. et al. Pr Neu Biol Psych, 2007; Dunayevich E. et al., J Cl Psych, 2007
social skills (1)
quality of life (2)
- subjective well-being
- clinician-rated measures
ANTIPSYCHOTIC TREATMENT:NEW OUTCOME MEASURES

QoL: A POLYSEMIC CONCEPT
Mass-Media meaninga universal ideal of high quality of most material and most marketableareas of life (i.e. objects owned, success in career, money to spend,social environment, holidays and free-time, physical performances)
the individual perception of satisfaction with the ‘being in the world’.It can be evaluated only trough the person’s opinion. Auto-evaluation.
Medicalmeaning
objective
subjective
a person’s life conditions as they appear to an external observer.Hetero-evaluation.
the patient’s perception of his own health status(aspects of life related to wellbeing and functionement)
Bertelli M. e Brown I. Quality of Life for PWID. Current Opinion in Psychiatry, 2006; 19:508-513

WHO FOR QoL
Quality of life is defined as individual’s perceptions of their position in life in the
context of the culture and value system where they live, and in relation to their
goals, expectations, standards and concerns.
Orley J., Saxena S., Herrman H. BJP, 1998Health Promotion Glossary. World Health Organization, 1998Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, 19-22 June, 1946
HEALTH: a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.(WHO, 1948)

QoL vs SUBJECTIVE WELL-BEING
Subjective well-being concerns itself primarily with affective states, positive or negative.
QOL implies a broader assessment and although affect-laden, it represents a subjective evaluation of oneself and one's social and material world.The exploration refers to those areas of life that are applicable to anybody’s life.
Orley J., Saxena S., Herrman H. Quality of life and mental illness. Reflections from the perspective of the WHOQOL. BJP, 1998

HEALTH AS A WAY OF BEING
It is not a given status but a conquest; it is not a definitive achievement but a pursue, a task, a life-style, enriched by that ethical dimension which encompasses all other human dimensions (physical, psychic,and ecological)
HEALTH DISEASE
capacity to live in a mindful and free way, increasing the
value of all one's own energies
incapacity to live in a mindful and free way, and to increase the value
of one's own skills and energies
National (Italian) Committee for Bioethics. Bioetica e Riabilitazione. Governo Italiano, marzo 2006

ETHICS OF CARE/REHABILITATION
Functionalist approach
Health practice aimed at restoring physical ability and autonomy
Contractualistic approach
Health practice aimed at adding further ability or autonomy (i.e. self-sufficiency, self-consciousness, or self-determination)
THERAPEUTIC ABANDON
OVERTREATMENT
approach based on Human Rights QoL
QoLIntegral approach
National (Italian) Committee for Bioethics. Bioetica e Riabilitazione. Governo Italiano, marzo 2006

restitution of all the structures damaged by the illness and their normal functioning
help to be satisfied with one’s own life
Normalization
Quality of Life approach
A NEW APPROACH TO THESYSTEM PATIENT-PERSON
Bertelli M. e Brown I. Quality of Life for PWID. Current Opinion in Psychiatry, 2006; 19:508-513

SOCIO-DEMOGRAPHIC AND CLINICAL DETERMINANTSOF QUALITY OF LIFE IN SCHIZOPHRENIA
Xiang YT, Wang CY, Wang Y, et al. Socio-demographic and clinical determinants of quality of life in Chinese patients with schizophrenia: a prospective study. Qual Life Res. 2010 Apr;19(3):317-22. Epub 2010 Feb 5.
AbstractPURPOSE: The aim of the study was to assess the changes in the quality of life
(QOL) of Chinese schizophrenia patients and to identify their predictors over a 1-
year follow-up. METHODS: A cohort of 116 schizophrenia patients was recruited,
and their socio-demographic and clinical characteristics including psychotic and
depressive symptoms, drug-induced side effects, social functioning, and QOL
were assessed with standardized rating instruments. The patients received
standard psychiatric care and were followed up for 1 year. RESULTS: The
psychotic and depressive symptoms, extrapyramidal side effects, and QOL
domains of physical functioning, role limitations due to physical problems, social
functioning, and role limitations due to emotional problems all improved
significantly. Social functioning was a predictor of baseline QOL and change at 1-
year follow-up. CONCLUSIONS: Routine clinical management was effective in
improving schizophrenia patients' psychopathology and several domains of QOL.
QOL was related to the level of social functioning and had only a weak
association with socio-demographic factors.

GENERIC QOL VS HR QOL
Generic: subjective modulation in those areas of life that are applicable to anybody’s life
Health-Related: mixture of clinical or dysfunctioning aspects, compared to normality
Bertelli M. e Brown I. Quality of Life for PWID. Current Opinion in Psychiatry, 2006; 19:508-513

ESEMPI DI ITEM IN STRUMENTI HR QOL
CCD HRQOL-141
Number of days in which you felt sad or depressed ___Number of days in which you felt worry or anxious ___
Functional Assessment of Cancer Therapy (FACT-G – 27 item)2
Physical Well-Being:I feel lack of energyI have nauseaI feel painI feel sickI’m obliged to spend my time in bed
AIDS QoL Assessment Questionnaire – AIDS-HAQ3
Area Item Descrption
Disabilities 23/116 Misures of the level to wich health status impact on 9 activities of basic autonomy (i.e. to stand up, to eat, to handle)
Symptoms 68/116 presence/absence during last week
1. U.S. Center for Chronic Disease Prevention and Health Promotion; 2. Cella DF., et al. Journal of Clinical Oncology, 1993; 11(3): 570-579; 3. Ludeck DP. and Fries JF. Quality of Life Research, 1992; 1: 359-366

INSTRUMENTS TO ASSESS QoL IN SCHIZOPHRENIA
GENERIC
WHOQoL;
SF-36 (HR-QdV);
EQ-5D (HR-QdV).
SPECIFIC
Instrument conceptual model items rater
QLS deficit syndrome 21 clinicians
QoLI general QoL model 143 patient
LQoLP general QoL model 105 patient
SQLQ sub. sick person’s life 59 patient
PETiT symptoms, SE and perf. 30 patient
S-QoL Calman’s approach 41 patient
Bobes J. et al. Quality of life measures in schizophrenia. Eur Psychiatry, 2005; 20 (3): S313-7

LIMITS OF THE INSTRUMENTS TO ASSESS QoL IN SCHIZOPHRENIA
• Lack of a specific theoretic basis
• Unclear and overlapped definitions
• Lack of data on measures sensitivity, as treatment outcome
• Confounding potential with symptomatology and
functionement
• Lack of a normative reference for target population
Bobes et al., 2005


SATISFACTION MODEL(Lehman et al., 1982; Baker e Intagliata, 1982)Calman’ gap between what one is and what he would like to be.
FUNCTIONALITY OF ROLE (Bigelow, 1982)Happiness and satisfaction are strictly related to the achievement of those social and environmental conditions (role) that human being needs.
IMPORTANCE / SATISFACTION MODEL (Becker, 1993)Satisfaction is related to importance.
THEORETICAL MODEL OF QoL
Bertelli M. e Brown I. Quality of Life for PWID. Current Opinion in Psychiatry, 2006; 19:508-513

Variables indicator of Subjective Well-Being should be considered as the least sensitive subjective measures
AFFECTIVE-COGNITIVEHOMEOSTATIC SYSTEM
OVERLOADUNDERLOAD
THE BALANCE OF SWB
Cummins R.A. Moving from the quality of life concept to a theory. Journal of Intellectual Disability Research 2005; 49(10):699-706

“…there is good agreement that the measurement should be based on both qualitative and quantitative variable from both subjective and objective positions
also dependently on the aim an evaluation is conducted to”.
Bertelli M. e Brown I. Quality of Life for PWID. Current Opinion in Psychiatry, 2006; 19:508-513
QUALITY OF LIFE:SUBJECTIVE OR OBJECTIVE?

• Importance attribuited by the individue
• Satisfaction perceived by the individue
• Opportunities available
• Choises made by the individue
QoL: CHARACTERISTICS
Brown I. et al., Centre of Public Health, University of Toronto, 1995
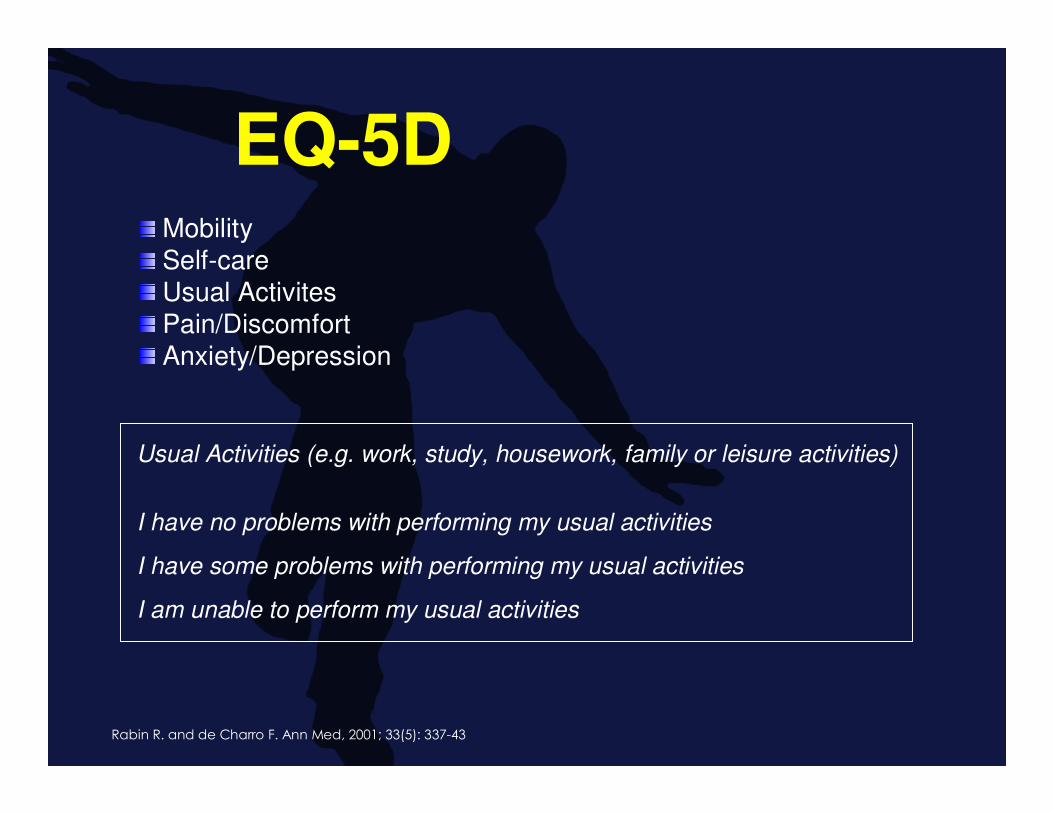
EQ-5D
Rabin R. and de Charro F. Ann Med, 2001; 33(5): 337-43
Mobility
Self-care
Usual Activites
Pain/Discomfort
Anxiety/Depression
Usual Activities (e.g. work, study, housework, family or leisure activities)
I have no problems with performing my usual activities �
I have some problems with performing my usual activities �
I am unable to perform my usual activities �
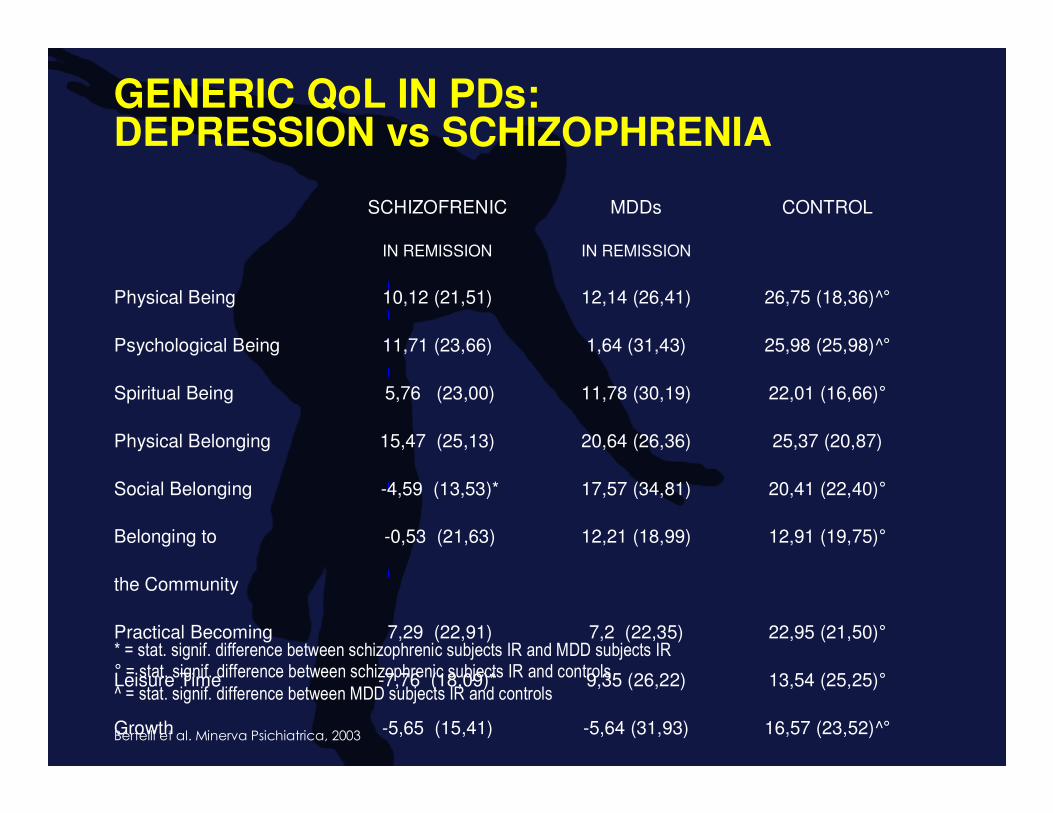
GENERIC QoL IN PDs:DEPRESSION vs SCHIZOPHRENIA
* = stat. signif. difference between schizophrenic subjects IR and MDD subjects IR° = stat. signif. difference between schizophrenic subjects IR and controls^ = stat. signif. difference between MDD subjects IR and controls
Bertelli et al. Minerva Psichiatrica, 2003
SCHIZOFRENIC MDDs CONTROL
IN REMISSION IN REMISSION
Physical Being 10,12 (21,51) 12,14 (26,41) 26,75 (18,36)^°
Psychological Being 11,71 (23,66) 1,64 (31,43) 25,98 (25,98)^°
Spiritual Being 5,76 (23,00) 11,78 (30,19) 22,01 (16,66)°
Physical Belonging 15,47 (25,13) 20,64 (26,36) 25,37 (20,87)
Social Belonging -4,59 (13,53)* 17,57 (34,81) 20,41 (22,40)°
Belonging to -0,53 (21,63) 12,21 (18,99) 12,91 (19,75)°
the Community
Practical Becoming 7,29 (22,91) 7,2 (22,35) 22,95 (21,50)°
Leisure Time -7,76 (18,09)* 9,35 (26,22) 13,54 (25,25)°
Growth -5,65 (15,41) -5,64 (31,93) 16,57 (23,52)^°
QoL Total 31,82 (126,53) 86,92 (178,44) 185,85 (113,90)^°

1. physical (e.g. energy, fatigue)
2. psychological (e.g. positive feelings)
3. level of independence (e.g. mobility)
4. social relationships (e.g. practical social support)
5. environment (e.g. Accessibility of health care)
6. personal beliefs/spirituality (e.g. meaning in life)
WHO CROSS-CULTURAL CORE DOMAINSFOR QUALITY OF LIFE
The domains of health and quality of life are complementary and overlapping
Health Promotion Glossary. World Health Organization, 1998What Quality of Life? The WHOQOL Group. In: World Health Forum. WHO, Geneva, 1996.

BEINGWho the patient is as a person.
PHYSICAL BEINGIt concerns such things as physical health, personal hygiene, nutrition, exercise, grooming and clothing, and general physicalappearance.
PSYCHOLOGICAL BEING It concerns such things as psychological health and adjustment, cognition, feelings, self-esteem, self-concept and self-control.
SPIRITUAL BEINGIt concerns such things as personal values, personal standards of conduct, and spiritual beliefs.
Brown I. et al., Centre of Public Health, University of Toronto, 1995
THE 9 AREAS OF LIFE OF THE QOL-IP

BELONGINGBelonging relates to connections with one's environments.
PHYSICAL BELONGINGPhysical Belonging concerns such places as in the home, workplace, school, neighborhood and community.
SOCIAL BELONGINGSocial Belonging concerns relationships with intimate others, family, friends, co-workers, neighborhood and community.
COMMUNITY BELONGINGCommunity Belonging concerns having an adequate income, health and social services, employment, educational programs, recreational programs, community events and activities.
Brown I. et al., Centre of Public Health, University of Toronto, 1995
THE 9 AREAS OF LIFE OF THE QOL-IP

BECOMINGBecoming relates to achieving personal goals, hopes and aspirations.
PRACTICAL BECOMINGPractical Becoming concerns domestic activities, paid work, school or volunteer activities, seeing to health or social needs.
LEISURE BECOMINGLeisure Becoming concerns activities that promote relaxation andstress reduction.
GROWTH BECOMINGGrowth Becoming concerns activities that promote the maintenance or improvement of knowledge and skills, as well as adapting to change.
Brown I. et al., Centre of Public Health, University of Toronto, 1995
THE 9 AREAS OF LIFE OF THE QOL-IP

QUALITY OF LIFE: FOR WHO?
A. The individue
B. The community
C. The family
D. The individue within the family
E. all the previous
F. none of the previous

• Importance• Satisfaction• Attainment• Initiative• Stability• Opportunity
FAMILY QOL
Werner S. et al. J Intellect Disabil Res, 2009; 53(6): 501-11

ASSESSING QoL: BY WHO?
A. the person herself
B. their relatives
C. their friends
D. their acquaintances
E. their health professionals
F. all the previous
G. a specific combination of the previous

• Direct interview
• Proxy Questionnaire
• External Assessor Questionnaire
person herself
other person
other person
QoL: ARTICULATION OF THE ASSESSMENT
Bertelli M. e Brown I. Quality of Life for PWID. Current Opinion in Psychiatry, 2006; 19:508-513

• le persone con DIG esprimono i loro vissutiattraverso repertori di comportamenti ricorrenti
• questi comportamenti possono essere organizzati ed interpretati dai familiari e dalle altre persone più vicine
• questi comportamenti possono essere confermati da altri osservatori esterni
• i repertori comportamentali permettono di individuare preferenze
Life Satisfaction Matrix
Lyons G. J Intellect Disabil Res, 2000; 49(10): 766-9