Embed Size (px)
Citation preview

QUALITY AND SAFETY POLICY
DOCUMENT NO. SKMCA/QD002_04_0618
FIRST ISSUE DATE: 29 MARCH 2017
DATE APPROVED: 27 JUNE 2018 NEXT REVIEW DATE: 01 MAY 2021
________________________________________________________________________________________________________
Accessed 27JUNE 2018 12:00 AM SKMCA/QD002_04_0618 Approved by Erik Wassberg CEO Page 1 of 10
1.Purpose
-The purpose of the Quality, safety and improvement efforts at SKMCA is to ensure delivery of the best possible care for our patients. The purpose of this document to provide a framework and to identify opportunities to improve care and services by measuring and assessing in a systematic and ongoing manner.
2. Policy Statement
2.1 At SKMCA, the roadmap to quality and performance improvement begins with strategic planning. The SKMCA quality and patient safety framwork is aligned with the hospitals strategic plan and TMO Quality and patient safety regulatory standards. The quality framwork is also aligned with the TMO /SKMCA strategic objectives to provide integrated high quality and patient centered/customer focused, cost effective and outcome oriented services to the population, ensured with superior operational execution from leadership level/ department level and hospitals wide level: by implementing the updated Joint Commission International (JCI) standards , as well as (TMO) Regulatory Standards which provides guidelines for systematic evaluation of systems, processes, functions, and outcomes to ensure excellence in delivering quality health care. 2.2 Information and data is aggregated and used in a consistent manner to improve systems and processes based on priorities identified by leadership and approved by the governing body. Systems and processes are designed and redesigned using a multidisciplinary approach and coordinated through all the hospital quality and safety programs and plans guided with an organizational culture of quality and patient safety with the evidences of frontline staffs engagement .
3. Scope SKMCA SKH-G SKH-WC SKH-M RCDR
4.Target audience
Core Relevant
All SKMCA Staff
C suite
Hospital Directors
Head of Department only
Line Manager Only
Physicians Specific Departments (specify)
……………………………….. ………………………………..
Nurses Specific Departments (specify)
………………………………….. ………………………………..
AHPs Specific Departments (specify)
………………………………….. ………………………………..
Admins Specific Departments (specify)
Quality Department ………………………………..
Others (specify) …………………………………….. ……………………………………..
QUALITY AND SAFETY POLICY
DOCUMENT NO. SKMCA/QD002_04_0618
FIRST ISSUE DATE: 29 MARCH 2017
DATE APPROVED: 27 JUNE 2018 NEXT REVIEW DATE: 01 MAY 2021
________________________________________________________________________________________________________
Accessed 27JUNE 2018 12:00 AM SKMCA/QD002_04_0618 Approved by Erik Wassberg CEO Page 2 of 10
5. Abbreviations SKMCA: Sheikh Khalifa Medical City Ajman SKH-G: Sheikh Khalifa Hospital - General SKH-WC: Sheikh Khalifa Hospital - Women and Children SKH-M: Sheikh Khalifa Hospital - Masfoot RCDR: Rashid Centre for Diabetes and Research GHP: Global Health Partner TMO: The Medical Office
6. Definitions 6.1 Quality Department: Department with assigned responsibility for Continuously improve and maintain quality and patient safety in all areas of care by adapting and/or adopting international best practices. The Quality Department operates under the direction of the CQO that reports to the CEO. The objective to achieve best care will be coordinated by the Quality Department with the support of the management and all coworkers at SKMCA. The Quality Department is organized as a shared service to ensure more flexibility and support the use of common work-principles and methods within SKMCA. Coordination and dissemination are organized through common committees for all SKMCA-hospitals.
7. Responsibilities
7.1 C-suite members
Are responsible to appoint necessary resources and staff to continuously improve and maintain quality and patient safety in all areas of care. Also, for actively taking measures for improvement and corrective actions.
7.2 Hospital Director:
Is responsible for providing support for the proper functioning of hospital wide Quality, safety and Improvement activities.
Provides support, direction and or assists with the resolution of problems or opportunities to improve care or services as needed.
7.3 Quality Department:
Has overall responsibility for quality improvement and patient safety in the hospitals.
Provides oversight for the continuous improvement and patient safety activities identified in the required and desired measures.
Fostering a culture that promotes a commitment to continually improve the quality of patient care and services;
Providing education to key personnel, as needed, on the approaches and methods of Quality Improvement activities;
Assessing and prioritizing process improvement projects;
Reporting Quality Improvement activities to C-suite members
Participate actively in RCA, FMEA, process mapping…etc. (lead, educate, guide, facilitate…etc.).
7.4 SKMCA Committees:
Supports and provides participation on interdisciplinary teams as needed based on the activities of the team.
Relevant findings, conclusions, recommendations and actions taken to improve care are communicated to the appropriate individuals.
Medical and non-medical cases with medical care concerns will undergo appropriate audit. The concerns will be forwarded to the appropriate committee for review and any
QUALITY AND SAFETY POLICY
DOCUMENT NO. SKMCA/QD002_04_0618
FIRST ISSUE DATE: 29 MARCH 2017
DATE APPROVED: 27 JUNE 2018 NEXT REVIEW DATE: 01 MAY 2021
________________________________________________________________________________________________________
Accessed 27JUNE 2018 12:00 AM SKMCA/QD002_04_0618 Approved by Erik Wassberg CEO Page 3 of 10
further action will be taken based upon recommendation of the committee.
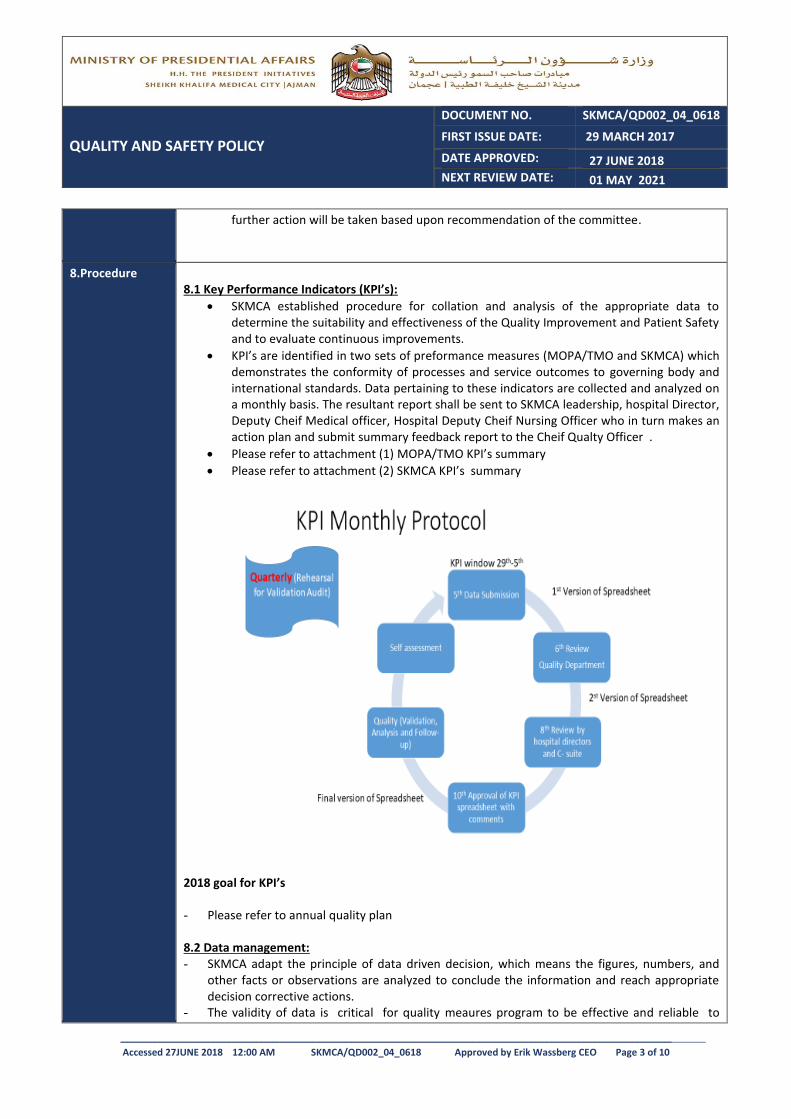
8.Procedure 8.1 Key Performance Indicators (KPI’s):
SKMCA established procedure for collation and analysis of the appropriate data to determine the suitability and effectiveness of the Quality Improvement and Patient Safety and to evaluate continuous improvements.
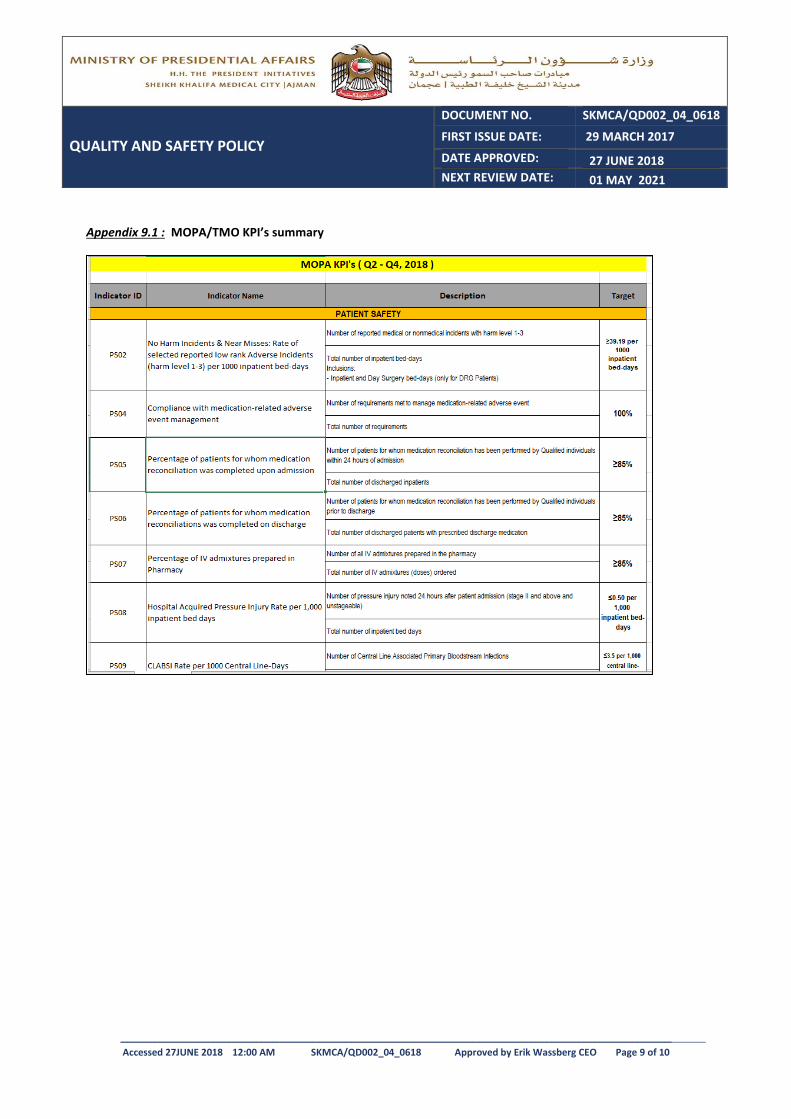
KPI’s are identified in two sets of preformance measures (MOPA/TMO and SKMCA) which demonstrates the conformity of processes and service outcomes to governing body and international standards. Data pertaining to these indicators are collected and analyzed on a monthly basis. The resultant report shall be sent to SKMCA leadership, hospital Director, Deputy Cheif Medical officer, Hospital Deputy Cheif Nursing Officer who in turn makes an action plan and submit summary feedback report to the Cheif Qualty Officer .
Please refer to attachment (1) MOPA/TMO KPI’s summary
Please refer to attachment (2) SKMCA KPI’s summary
2018 goal for KPI’s - Please refer to annual quality plan 8.2 Data management: - SKMCA adapt the principle of data driven decision, which means the figures, numbers, and
other facts or observations are analyzed to conclude the information and reach appropriate decision corrective actions.
- The validity of data is critical for quality meaures program to be effective and reliable to
QUALITY AND SAFETY POLICY
DOCUMENT NO. SKMCA/QD002_04_0618
FIRST ISSUE DATE: 29 MARCH 2017
DATE APPROVED: 27 JUNE 2018 NEXT REVIEW DATE: 01 MAY 2021
________________________________________________________________________________________________________
Accessed 27JUNE 2018 12:00 AM SKMCA/QD002_04_0618 Approved by Erik Wassberg CEO Page 4 of 10
ensure that relble and useful data have been collected, when deemed nessessary an internal data validation shall be conducted.
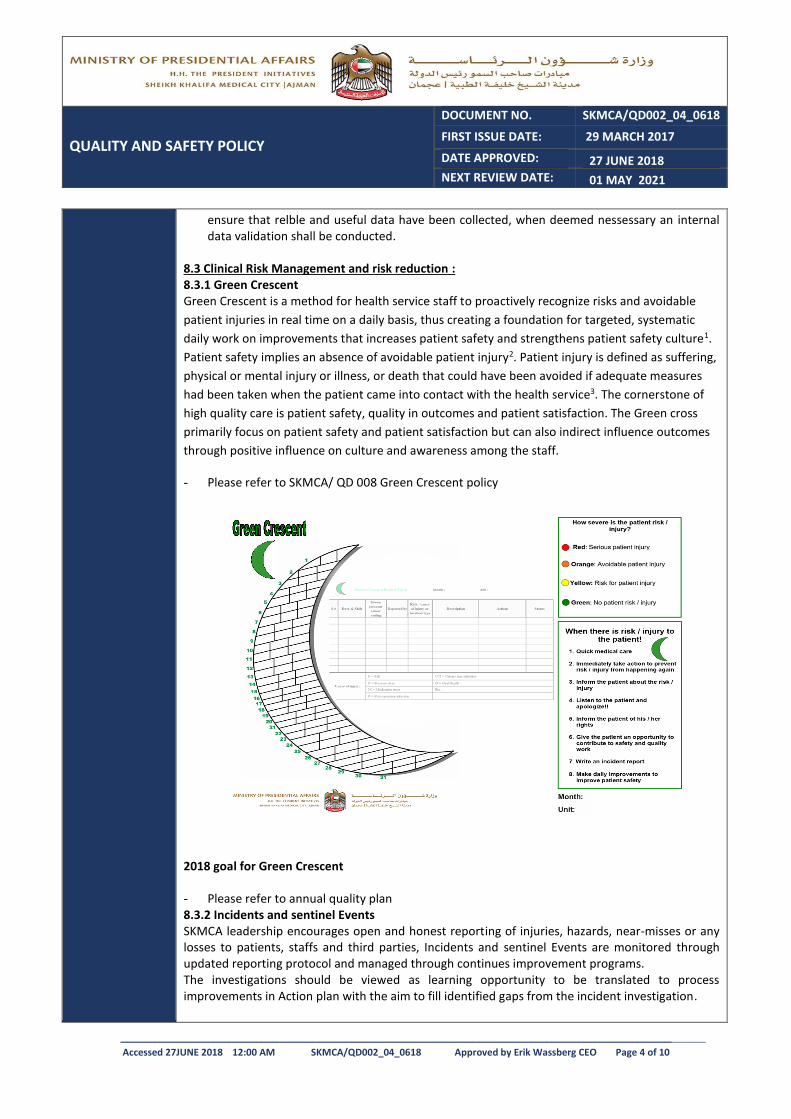
8.3 Clinical Risk Management and risk reduction : 8.3.1 Green Crescent Green Crescent is a method for health service staff to proactively recognize risks and avoidable
patient injuries in real time on a daily basis, thus creating a foundation for targeted, systematic
daily work on improvements that increases patient safety and strengthens patient safety culture1.
Patient safety implies an absence of avoidable patient injury2. Patient injury is defined as suffering,
physical or mental injury or illness, or death that could have been avoided if adequate measures
had been taken when the patient came into contact with the health service3. The cornerstone of
high quality care is patient safety, quality in outcomes and patient satisfaction. The Green cross
primarily focus on patient safety and patient satisfaction but can also indirect influence outcomes
through positive influence on culture and awareness among the staff.
- Please refer to SKMCA/ QD 008 Green Crescent policy
2018 goal for Green Crescent - Please refer to annual quality plan 8.3.2 Incidents and sentinel Events SKMCA leadership encourages open and honest reporting of injuries, hazards, near-misses or any losses to patients, staffs and third parties, Incidents and sentinel Events are monitored through updated reporting protocol and managed through continues improvement programs. The investigations should be viewed as learning opportunity to be translated to process improvements in Action plan with the aim to fill identified gaps from the incident investigation.
QUALITY AND SAFETY POLICY
DOCUMENT NO. SKMCA/QD002_04_0618
FIRST ISSUE DATE: 29 MARCH 2017
DATE APPROVED: 27 JUNE 2018 NEXT REVIEW DATE: 01 MAY 2021
________________________________________________________________________________________________________
Accessed 27JUNE 2018 12:00 AM SKMCA/QD002_04_0618 Approved by Erik Wassberg CEO Page 5 of 10
All incidents are handled in a confidential manner to ensure that patients, staff and third parties are supported and treated respectfully
All incidents at respectively hospital is reported in the Quality and Risk sub-committees.
Relevant incidents are shared to other Quality and Risk sub-committees within SKMCA. These are chosen by the Quality Department.
Please refer to SKMCA/QD 003 Incident reporting policy and SKMCA/ QD 004 Sentinel Event Policy
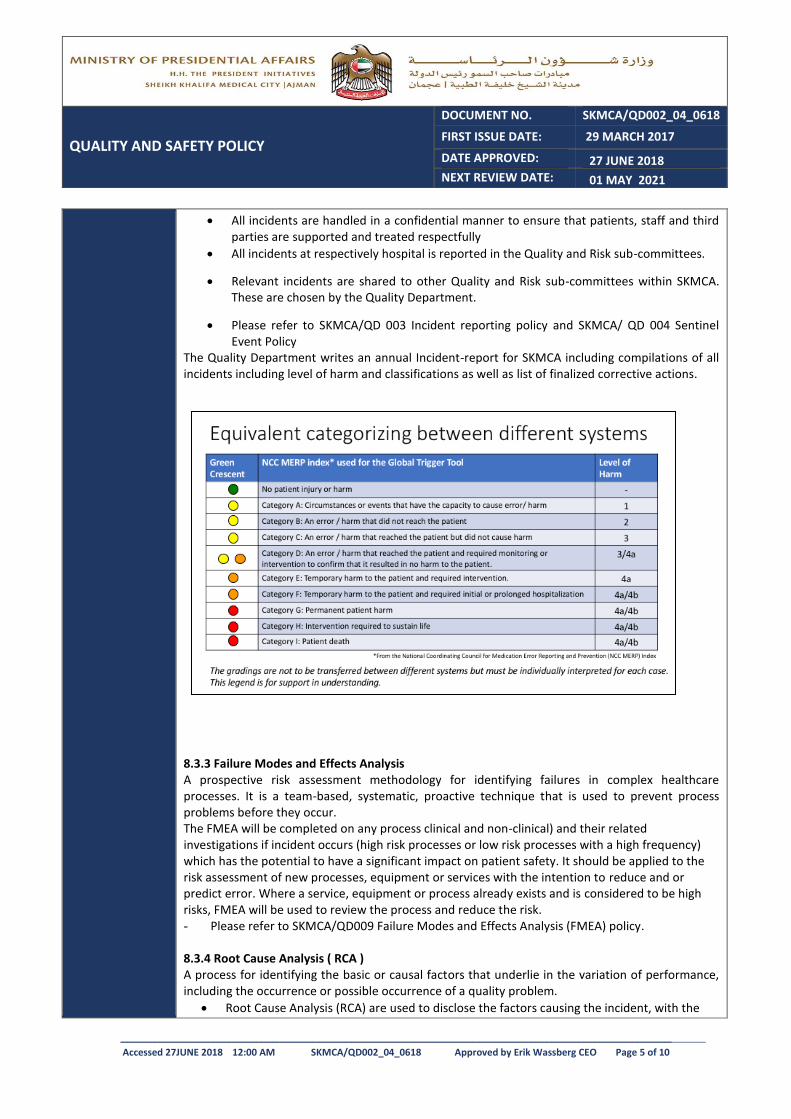
The Quality Department writes an annual Incident-report for SKMCA including compilations of all incidents including level of harm and classifications as well as list of finalized corrective actions.
8.3.3 Failure Modes and Effects Analysis A prospective risk assessment methodology for identifying failures in complex healthcare processes. It is a team-based, systematic, proactive technique that is used to prevent process problems before they occur. The FMEA will be completed on any process clinical and non-clinical) and their related investigations if incident occurs (high risk processes or low risk processes with a high frequency) which has the potential to have a significant impact on patient safety. It should be applied to the risk assessment of new processes, equipment or services with the intention to reduce and or predict error. Where a service, equipment or process already exists and is considered to be high risks, FMEA will be used to review the process and reduce the risk. - Please refer to SKMCA/QD009 Failure Modes and Effects Analysis (FMEA) policy. 8.3.4 Root Cause Analysis ( RCA ) A process for identifying the basic or causal factors that underlie in the variation of performance, including the occurrence or possible occurrence of a quality problem.
Root Cause Analysis (RCA) are used to disclose the factors causing the incident, with the
QUALITY AND SAFETY POLICY
DOCUMENT NO. SKMCA/QD002_04_0618
FIRST ISSUE DATE: 29 MARCH 2017
DATE APPROVED: 27 JUNE 2018 NEXT REVIEW DATE: 01 MAY 2021
________________________________________________________________________________________________________
Accessed 27JUNE 2018 12:00 AM SKMCA/QD002_04_0618 Approved by Erik Wassberg CEO Page 6 of 10
purpose to reduce the risk and prevent reoccurrence of a similar incidents by suggesting corrective actions, Please refer to SKMCA/ QD 011 Root Cause Analysis ( RCA ) Policy.
The RCA will be completed on any incident having the potential to have a significant impact on patient safety and a significant risk of re-occurrence, please refer to SKMCA/QD009 FMEA policy.
The outcomes of all RCA’s will be shared across the SKMCA- Ajman facilities to prevent incident reoccurrence and to ensure that lessons are learnt.
8.4 Hospital Accreditation: The UAE Vision agenda aims to achieve a world-class healthcare system by 2021. The mission of the GHP´s operation of the SKMCA is in line with Vision 2021 through a program to develop cost-effective and high quality healthcare.
TMO decide to mandate Joint commission international (JCI) accreditation standard as fist choice for evidence of compliance with international best practice.
JCI accreditation as its core is a risk reduction activity
SKMCA utilises Tracer methodology to monitor SKMCA performance and compliance with international standards, all noncompliant areas (partially met and not met) as opportunities to improve care processes and develops subsequent improvement action plans.
The Quality department communicates the result of the monthly tracer with the hospital leadership through an official report.
The hospital leadership monthly shares the progress status of improvement action plan with the Quality department.
The CEO and other leaders of SKMCA shall be informed the result of tracer activity including tracer result and action plan progress in a quarterly basis.
Please refer to SKMCA/ QD 010 JCI Tracer Policy
2018 goals for JCI.
- - Please refer to annual quality plan 8.5 Further assignments for the Quality Department are:
Organize teams and task force for implementation of the quality strategy on a regular basis, with an agenda and follow up on actions.
Development of methods and organizing for collection of clinical results such as KPI´s, indicators and outcome measurements.
Over all responpiity of the Document Management System
Coordinating of accreditation for the Joint Commission International
Active partnership with Strategy department in audits, e.g. TMO/MOPA quarterly audit and other reviews.
9. Appendices
Appendix 9.1 : MOPA/TMO KPI’s summary
Appendix 9. 2 : SKMCA KPI’s summary
QUALITY AND SAFETY POLICY
DOCUMENT NO. SKMCA/QD002_04_0618
FIRST ISSUE DATE: 29 MARCH 2017
DATE APPROVED: 27 JUNE 2018 NEXT REVIEW DATE: 01 MAY 2021
________________________________________________________________________________________________________
Accessed 27JUNE 2018 12:00 AM SKMCA/QD002_04_0618 Approved by Erik Wassberg CEO Page 7 of 10
10.References http://sas.vgregion.se/contentassets/c26d2a29e940433db9a1c7c6f2f0dee1/2079---folder-grona-korset-eng-version-2016.pdf
http://www.who.int/patientsafety/en/
http://www.socialstyrelsen.se/patientsakerhet/vardskada
Evaluation of the Green Cross at the Sheikh Khalifa Hospital General, (2017). Joacim Stalfors MD, Ph.D, Associate professor, CQO SKMCA, Report from 24 April 2017
Joint Commission International: Joint Commission International Standards, 6th Edition (2017). QPS.1
Joint Commission International (2017). Survey Process Guide for Hospitals 6th Edition. Illinois: Joint Commission Resources.
Riskanalys och händelseanalys. Analysmetoder för att öka patientsäkerheten. Sveriges Kommuner och Landsting 2015. ISBN 978-91-7585-237-9.
SOSFS 2011:9 Ledningssystem för systematiskt kvalitetsarbete - chapter 5
Systematiskt förbättringsarbete, chapter 7 – Dokumentationsskyldighet GHP References:
B Kvalitet.doc – page 2,3
Review Cycle One year Three years
12. Amendment History
Superseded Documents
Description of Amendment
(Compared to previous version)
Page
Date
QD002 - The policy is rewritten and
modified to SKMCA template with
the new structure and format of
policies and procedure.
All
SKMCA/QD002_02_1216 - The Policy have been reviewed as
recommended by TMO with
respect to linguistic and structure.
Also changes have been done to
meet the standards described in
the updated Document
Management Policy.
All
SKMCA/QD002_03_0317 - The policy has been rewritten addition of procedure, Green Crescent and Key Performance Indicators (KPI’s), 3 Clinical Risk Management and risk reduction
- Addition of appendixes
All
QUALITY AND SAFETY POLICY
DOCUMENT NO. SKMCA/QD002_04_0618
FIRST ISSUE DATE: 29 MARCH 2017
DATE APPROVED: 27 JUNE 2018 NEXT REVIEW DATE: 01 MAY 2021
________________________________________________________________________________________________________
Accessed 27JUNE 2018 12:00 AM SKMCA/QD002_04_0618 Approved by Erik Wassberg CEO Page 8 of 10
13. Approvals Date: 27 JUNE 2018
Title Name Signature
Author:
Quality Director Hisham H Siddig
First Reviewer:
Chief Quality Officer Joacim Stalfors
Second Reviewer:
Quality Department Joacim Stalfors (CQO) Aysha Alshehhi
TEAM
Endorsed by:
Hospital Director Deputy Chief Medical Officer Deputy Chief Nursing Officer Chief Quality Officer
Policy Committee Member
24 June 2018
Approved by:
CEO Erik Wassberg
QUALITY AND SAFETY POLICY
DOCUMENT NO. SKMCA/QD002_04_0618
FIRST ISSUE DATE: 29 MARCH 2017
DATE APPROVED: 27 JUNE 2018 NEXT REVIEW DATE: 01 MAY 2021
________________________________________________________________________________________________________
Accessed 27JUNE 2018 12:00 AM SKMCA/QD002_04_0618 Approved by Erik Wassberg CEO Page 9 of 10
Appendix 9.1 : MOPA/TMO KPI’s summary

QUALITY AND SAFETY POLICY
DOCUMENT NO. SKMCA/QD002_04_0618
FIRST ISSUE DATE: 29 MARCH 2017
DATE APPROVED: 27 JUNE 2018 NEXT REVIEW DATE: 01 MAY 2021
________________________________________________________________________________________________________
Accessed 27JUNE 2018 12:00 AM SKMCA/QD002_04_0618 Approved by Erik Wassberg CEO Page 10 of 10
Appendix 9. 2 : SKMCA KPI’s summary





























