Embed Size (px)
Citation preview

Quality Assurance Manual GMERSGHH/CQI/A Quality Manual G.M.E.R.S General Hospital, Himmatanagar, Gujarat

INDEX
S. No. Pages
1. Responsibility for Implementation 4-4
2. Amendment sheets 5-6
3. Services available at GMERSGHH 7-8
4. Quality Management System
Quality Assurance Committee
Our Vision
Our Mission
Quality Policy Statement
Objectives
Service Standards
8-14
5. Structure for Quality Assurance
Documentation System
Quality Assurance Committee
Accreditation Coordinator
Departmental Coordination
14-17
6. Quality Assurance Programme 17-36

RESPONSIBILITY FOR IMPLEMENTATION:
The overall responsibility for formulating, revising, implementing,
provisioning of education material to patients/ workers, training of trainers/
supervisors/ concerned hospital personnel and monitoring for this manual
is the responsibility of the Co-Chairperson Quality Assurance Committee
and its committee members.
Also the top management is responsible for implementation of this
manual.
All individual Incharges of the related units are directly responsible for the
implementation / training of supervisors / concerned hospital personnel
and monitoring / reporting for this policy in their respective areas of work.
For this they shall take guidance from and coordinate with the Co-
Chairperson Quality Assurance Committee.
ABBREVIATIONS USED:
CRBSI – CR Blood Stream Infection
SSI – Surgical Site Infection
VAP – Ventilator Associated Pneumonia
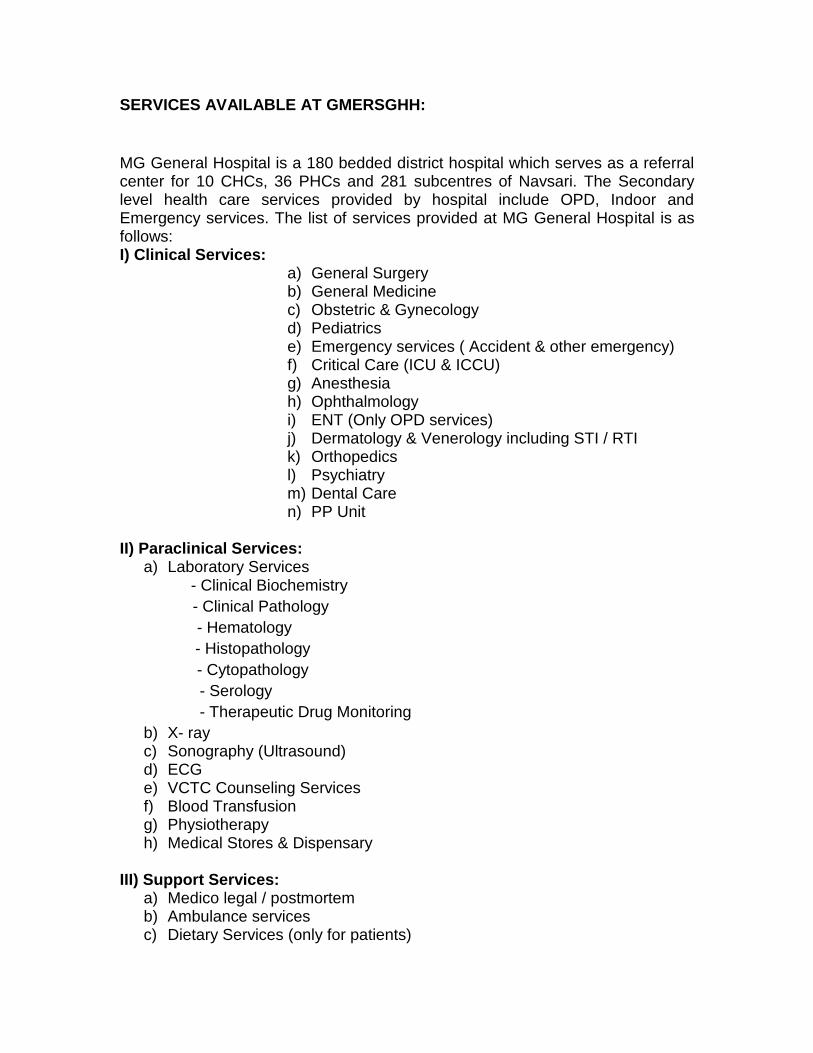
SERVICES AVAILABLE AT GMERSGHH:
MG General Hospital is a 180 bedded district hospital which serves as a referral center for 10 CHCs, 36 PHCs and 281 subcentres of Navsari. The Secondary level health care services provided by hospital include OPD, Indoor and Emergency services. The list of services provided at MG General Hospital is as follows: I) Clinical Services:
a) General Surgery b) General Medicine c) Obstetric & Gynecology d) Pediatrics e) Emergency services ( Accident & other emergency) f) Critical Care (ICU & ICCU) g) Anesthesia h) Ophthalmology i) ENT (Only OPD services) j) Dermatology & Venerology including STI / RTI k) Orthopedics l) Psychiatry m) Dental Care n) PP Unit
II) Paraclinical Services:
a) Laboratory Services - Clinical Biochemistry
- Clinical Pathology
- Hematology
- Histopathology
- Cytopathology
- Serology
- Therapeutic Drug Monitoring
b) X- ray c) Sonography (Ultrasound) d) ECG e) VCTC Counseling Services f) Blood Transfusion g) Physiotherapy h) Medical Stores & Dispensary
III) Support Services: a) Medico legal / postmortem b) Ambulance services c) Dietary Services (only for patients)
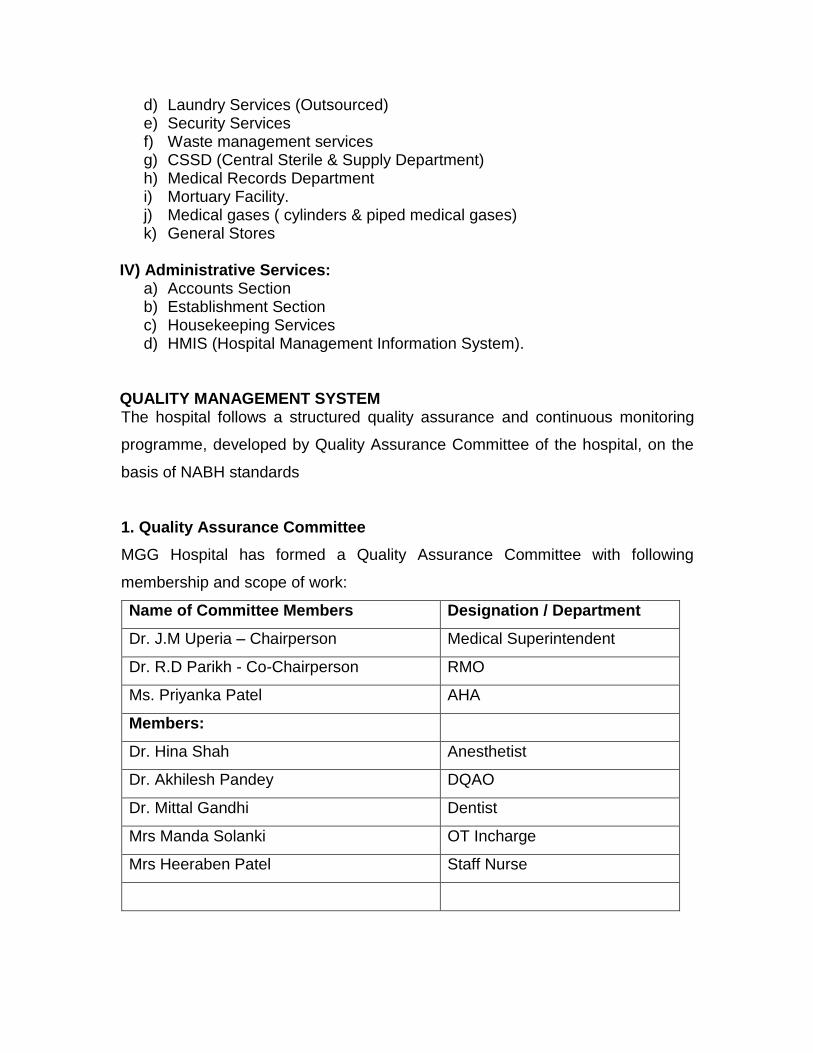
d) Laundry Services (Outsourced) e) Security Services f) Waste management services g) CSSD (Central Sterile & Supply Department) h) Medical Records Department i) Mortuary Facility. j) Medical gases ( cylinders & piped medical gases) k) General Stores
IV) Administrative Services:
a) Accounts Section b) Establishment Section c) Housekeeping Services d) HMIS (Hospital Management Information System).
QUALITY MANAGEMENT SYSTEM The hospital follows a structured quality assurance and continuous monitoring
programme, developed by Quality Assurance Committee of the hospital, on the
basis of NABH standards
1. Quality Assurance Committee
MGG Hospital has formed a Quality Assurance Committee with following
membership and scope of work:
Name of Committee Members Designation / Department
Dr. J.M Uperia – Chairperson Medical Superintendent
Dr. R.D Parikh - Co-Chairperson RMO
Ms. Priyanka Patel AHA
Members:
Dr. Hina Shah Anesthetist
Dr. Akhilesh Pandey DQAO
Dr. Mittal Gandhi Dentist
Mrs Manda Solanki OT Incharge
Mrs Heeraben Patel Staff Nurse

Scope of Work:
Issue Quality Policy
Documentation of policy
Deal with all matters concerning quality management system, quality
improvement, accreditation of the health care service.
To provide support and guidance to other committees and department in
developing indicators.
Function as apex committee for monitoring performance indicators /
parameters of QMS and medical statistics
Standardization of procedures and systems
Credentialing and Privileging of medical and nursing staff.
Provision of resources for successful implementation of quality program at
MGG hospital.
Evaluate sentinel events related to patient care.
Conducting regular meetings of all respective committee chairpersons to
keep a track of the activities carried out by them and trouble shooting if
any in implementation in their respective areas.
Plan and act for Continuous Quality improvement of hospital
NABH Chapter Ref: CQI, HRM -10, 12
In line with our goal of providing quality services in our hospital, we have
developed and set our vision, mission, quality policy, and service standards.
2. OUR VISION:
"To be the part of network of finest public health care institutions in the State of
Gujarat, providing quality medical care services with the state of art technology
with easy accessibility, affordability and equity to the people of Gujarat and
beyond."

3. OUR MISSION:
The GMERS General Hospital is dedicated to carry forward the dream of
government of Gujarat to provide quality care of national standards to all in a
caring & compassionate environment.
4. QUALITY POLICY STATEMENT:
GMERSGHH is committed to provide Health Care par excellence at reasonable
cost. This would be achieved through:
a. Complying with National and International Quality standards
b. To provide services within the framework of Regulatory requirements
c. Up gradation of Technology and Facilities on regular basis
d. Training the manpower in the relevant discipline
e. Continuous Quality improvement in the processes
f. Striving to increase external and internal customer satisfaction level.
5. OBJECTIVES:
To provide high quality care according to the health needs of the
catchment population
To facilitate patient satisfaction by service and ensuring the dignity and
rights of patients and other stakeholders.
To provide a safe and conducive work environment for staff.
To ensure accountable, consultative and transparent management
process.
To provide basic and continuing education for staff.
To integrate with district and state health system, by providing referral
systems, technical, and logistic support to primary and community health
care.

6. SERVICE STANDARDS:
GMERS General Hospital has:
11 Specialists
5 Medical Officers and 37 Nurses
Standards of service and adequate degree of patient care can be provided
to the extent proper and workable ratio between doctor to patient, nurse to
patient and beds to patients are maintained, as also the extent of
availability of resources and facilities. Consistent with this every possible
effort will be made by this hospital to provide standard services.
To provide access to hospital and professional medical care to all patients
who visit the hospital.
To prescribe a workable maximum waiting time for outpatients, before
they are attended to by a qualified doctor and I or specialists and
continuously strive to improve upon it.
To ensure that all equipment in the hospital are maintained efficiently in
proper working order.
To ensure availability of beds and operation theatres facilities as freely as
possible.
To ensure treatment of emergency cases with utmost promptitude and
attention.
Every outpatient seeking treatment at the hospital will be registered and
issued a case for recording various details of the symptoms, diagnosis
and treatment being provided. Efforts will be made to computerize the
record system in the hospital, to provide better service to the patients.
The patients' and families' rights are in consonance to accreditation
standards and are documented separately in this charter.
All patients and visitors to the hospital will receive courteous and prompt
attention from the staff and officials of the hospital in the use of its various
services.

Reliability and promptness of diagnostic investigation results is ensured
and whenever possible such reports will be made available.
Operation theatre is maintained on a regular basis to ensure that they are
serviceable all the time and every effort will be made to keep the hospital
and its surroundings, clean, infection-free and hygienic.
A regular system of obtaining feedback from the users is in place through
periodic surveys. The inputs from these are continuously used for
improving the service standards.
The hospital has necessary equipments required for provision of service
mentioned in 'scope of services and system to ensure proper maintenance
and working of various equipments.
When things go wrong or fail, appropriate action is taken on those
responsible for such failures and action taken to rectify the deficiencies.
Complainants will also be informed of the action taken, if requested.
In case of likely persistence of the deficiency, the reasons for the delay in
rectifying the deficiency and the time taken for rectifying the same will be
displayed prominently for the information of the public.
Special directions are given to the non-medical staff to deal with the
patients and public courteously. Any breach in this regard when brought to
the notice of the hospital authorities shall be dealt with appropriately.
Hospital encourages the patients and the public to inform the authorities
when things go wrong. Suggestion I complaint boxes alongwith complaint
tracking forms and registers are provided at the reception, at each ward
level, RMO office, Matron Office, sanitary inspector and administrator.
To resolve patient complaints the hospital has formed a Patient Complaint
Cell.
Hospital follows all policies, processes, programmes, committee meetings;
regulatory guidelines, which have been prepared to meet the standards of
accreditation as, set by NABH.
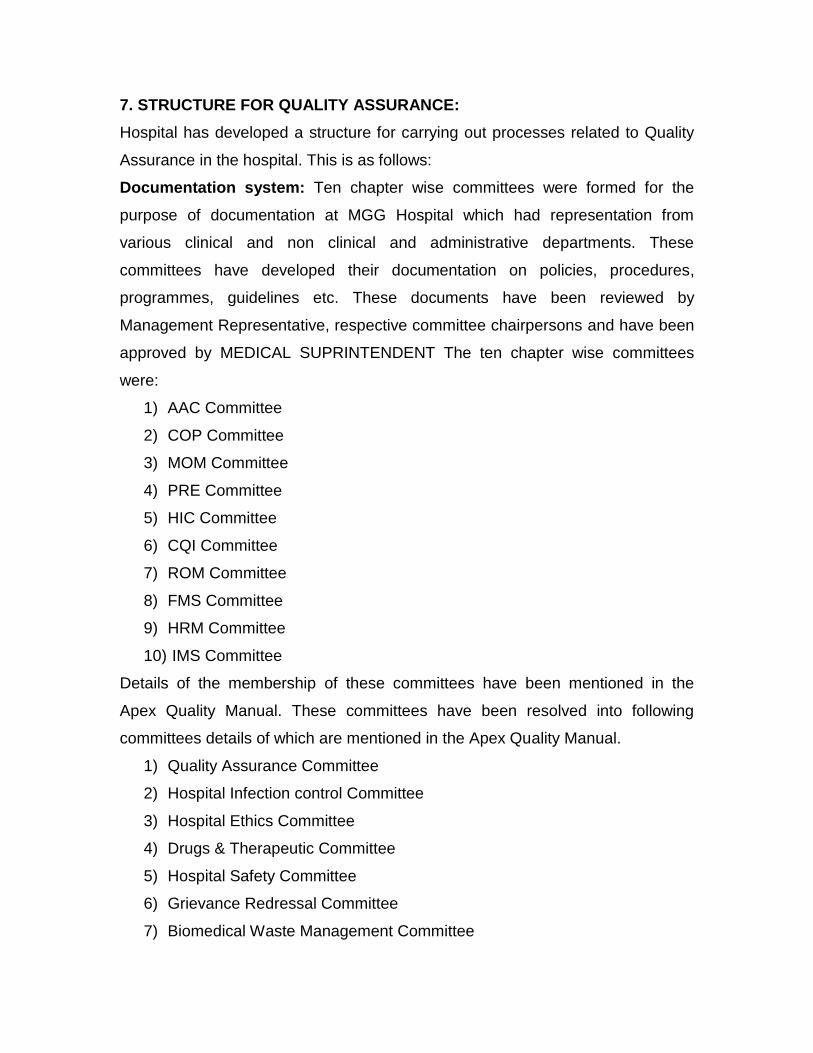
7. STRUCTURE FOR QUALITY ASSURANCE:
Hospital has developed a structure for carrying out processes related to Quality
Assurance in the hospital. This is as follows:
Documentation system: Ten chapter wise committees were formed for the
purpose of documentation at MGG Hospital which had representation from
various clinical and non clinical and administrative departments. These
committees have developed their documentation on policies, procedures,
programmes, guidelines etc. These documents have been reviewed by
Management Representative, respective committee chairpersons and have been
approved by MEDICAL SUPRINTENDENT The ten chapter wise committees
were:
1) AAC Committee
2) COP Committee
3) MOM Committee
4) PRE Committee
5) HIC Committee
6) CQI Committee
7) ROM Committee
8) FMS Committee
9) HRM Committee
10) IMS Committee
Details of the membership of these committees have been mentioned in the
Apex Quality Manual. These committees have been resolved into following
committees details of which are mentioned in the Apex Quality Manual.
1) Quality Assurance Committee
2) Hospital Infection control Committee
3) Hospital Ethics Committee
4) Drugs & Therapeutic Committee
5) Hospital Safety Committee
6) Grievance Redressal Committee
7) Biomedical Waste Management Committee

8) Medical Audit Committee
9) Disaster Management Committee
10) Biomedical equipment management & medical gases management
committee.
11) Blood Transfusion Reaction monitoring Committee.
Quality Assurance Committee: Quality assurance related activities is planned,
undertaken, and controlled by Quality Assurance Committee which is a
multidisciplinary committee having representation from various clinical, non-
clinical and administrative departments.
Accreditation Coordinator: The hospital designated Accreditation, Co-
ordinator, will have overall responsibility of coordinating the work of NABH
accreditation. His I her responsibility will include:
To issue various documents to departments from time to time.
To keep a record of all the documentation of the hospital, in relation to
accreditation.
To delegate the activities in departments and ensure its timely
completion.
To regularly receive feedbacks from departments regarding status of their
work related to accreditation preparation.
To coordinate all such activities required for quality assurance and
continuous monitoring of the hospital.
Departmental Coordination:
Each department of the hospital has been appointed with one NABH coordinator.
The responsibility of these coordinators will be:
a) To receive and retain all the documents and official correspondence
related to NABH accreditation from time to time
b) To inform and orient the staff of their department on policies and
procedures developed for their department

c) To ensure the completion of all the work assigned to their department
for NABH accreditation preparation.
d) To coordinate with NABH assessors for their departmental assessment.
QUALITY ASSURANCE PROGRAM
a) The program is comprehensive and covers quality assurance of input,
process and outcome. This has been developed by quality assurance
committee and implemented by various committees, accreditation
coordinator and other personnel.
b) Quality assurance and continuous monitoring programme is developed for
following areas
i. Applicable hospital wide (Table 1)
ii. Applicable for laboratory (Table 2)
iii. Applicable for radiology (Table 3)
iv. Applicable for intensive care areas (Table 4)
v. Applicable for surgical services (Table 5)
Vi.Other Clinical & Managerial Indicators used for quality assurance and
continuous monitoring. (Table 6)
c) Procedure for implementing the programme is as follows:
i. The programme which is applicable hospital wide and which is
applicable for infection control is explicitly tabulated. Quality
Assurance committee and Hospital Infection committee shall
implement, monitor and improve the programme.
ii. The hospital has developed medical indicators which are monitored on
monthly basis and recorded in HMIS. Report on these indicators is
generated for hospital through HMIS. This report gives the figures for
all indicators, which is reviewed and subsequent actions shall be
taken based on adherence to standard value, by Hospital
administration and QAC.

iii. The program applicable for laboratory, radiology, intensive care area
and surgical services shall be implemented through departmental in
charge under the vigilance of QAC. Each of these departments shall
maintain a quality assurance register. The record shall be endorsed in
the register as 'C I PC I NC' (C for Compliance, PC for partial
compliance and NC for non-compliance). The record shall be entered
at frequency defined in the table.
i. Quality assurance programme applicable hospital wide (Table 1)
Purpose Methodology Responsibility Remark
Setting goals
and objectives
Setting of mission,
vision, objectives,
quality policy and
service standards
through committee
discussion and
approval of MEDICAL
SUPRINTENDENT
QAC Refer S. No 1 to 7 of
this document
Infrastructure Identifying
infrastructural
requirement including
Physical facility
Manpower
Equipments
This is determined on
the basis of workload
and change in scope
of service
Hospital
Administration and
State government
Reference is taken
from Bureau of Indian
Standards and IPH
standards.
Policies
procedures
and other
This documentation is
done to develop
systems and
Various
committees,
accreditation

documentation
requirement
processes that are
necessary to provide
uniform service of
desired level of quality
and communicate it to
relevant personnel.
coordinator and
MEDICAL
SUPRINTENDENT
Compliance
monitoring
Compliance is
monitored and non-
conformity is tracked
for taking corrective
and preventive actions.
This is done through
compliance monitoring
registers kept in
various departments
All the staff of the
hospital and
Quality Assurance
Committee
Walk through
monitoring
Walk through
monitoring or physical
monitoring is done by
designated member of
QAC, Hospital
infection control
committee, hospital
safety committee
Accreditation co-
ordinator, RMO, AO
and MEDICAL
SUPRINTENDENT.
QAC, Hospital
infection control
committee,
hospital safety
committee,
Accreditation
coordinator, RMO
Matron, Sanitary
inspector and
MEDICAL
SUPRINTENDENT
Following aspects are
specially looked for
Infection
control
Hospital safety
Record
maintenance
Policy
compliance
Indicator
monitoring
A list of indicators has
been developed to
monitor the key
features necessary for
QAC Refer Tables 2, 3, 4 5
& 6.

quality assurance.
These are developed
for structure process,
clinical and managerial
activities. A monthly
report is generated
with all these
indicators which is
reviewed for necessary
action by Quality
Assurance committee.
Training and
orientation
Necessary instructions
to the staff for quality
assurance are
communicated through
their departmental in
charges. Quality
Assurance is also
included as one of the
training needs, on
which training is
organized at regular
intervals.
QAC and hospital
administration
Continuous
process
The contents of this
programme are
reviewed every year by
Quality Assurance
Committee for
adequacy.
QAC Following aspects is
reviewed every year.
Objective and
service standards
Adequacy of
documentation
Monitoring
systems
Various indicators
and their
standards
Structure for
implementation of
quality assurance
programme
Any other system
required for
quality
improvement
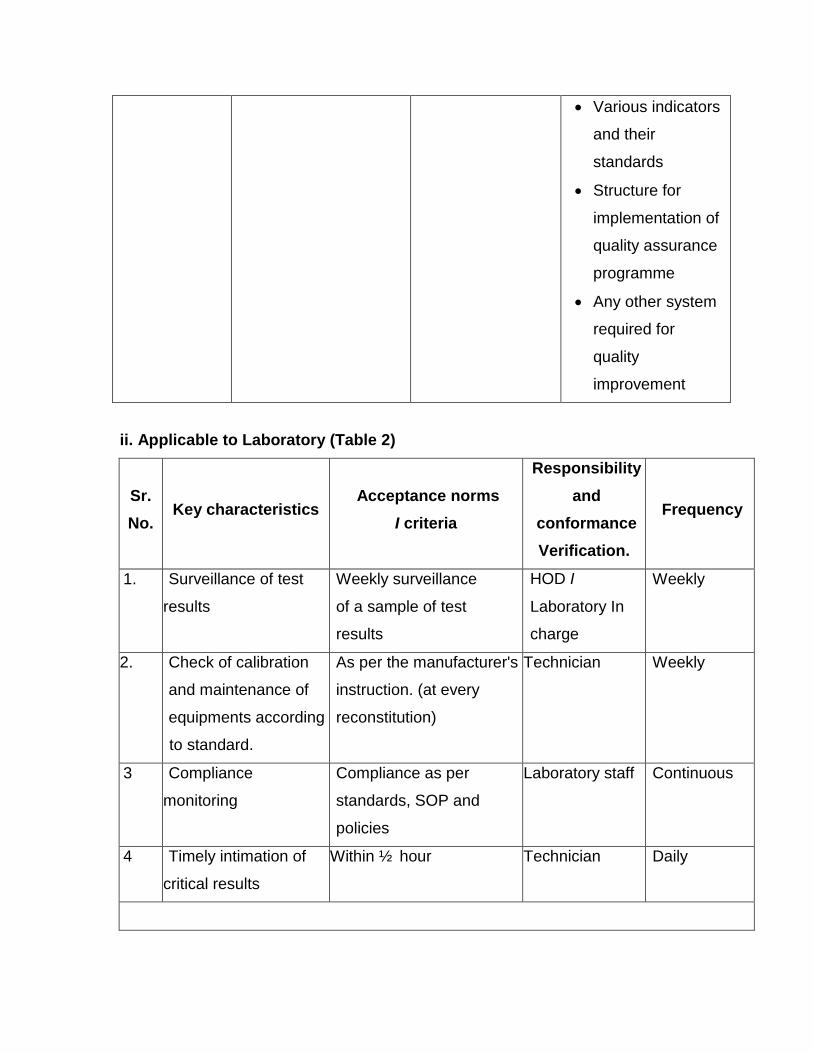
ii. Applicable to Laboratory (Table 2)
Sr.
No. Key characteristics
Acceptance norms
I criteria
Responsibility
and
conformance
Verification.
Frequency
1. Surveillance of test
results
Weekly surveillance
of a sample of test
results
HOD I
Laboratory In
charge
Weekly
2. Check of calibration
and maintenance of
equipments according
to standard.
As per the manufacturer's
instruction. (at every
reconstitution)
Technician Weekly
3 Compliance
monitoring
Compliance as per
standards, SOP and
policies
Laboratory staff Continuous
4 Timely intimation of
critical results
Within ½ hour Technician Daily

Biochemistry
1. Calibration through
control ( Biochemistry
Kit)
As per the manufacturer's
instruction.
Technician Quarterly
Haematology
1. Maintenance of
equipment
As per the instruction in
operation manual.
Technician Daily
2. Calibration through
Control.
(Heamatology kit)
As per the
manufacturer's
instruction.
Service
Engineer
of the company.
Once in
three
months
Pathology
1. Tests to be done on
fresh specimens
received in
containers with lids.
Proper covering of
sample with lid
Technician Daily
iii. Applicable for Radiology (Table - 3)
sr.
No.
Key Characteristics Acceptance
Norms I
Criteria
Responsibility
And
Conformance
Verification
Frequency
1. Compliance monitoring Compliance as per
standards, SOP and
policies
Imaging Staff Continuous
2. Waiting time for
investigation.
X ray: 30 mins or
less (90% cases)
Ultrasound: 40 min
after preparation
(90% cases)
Technician
I
Radiologist
Weekly

3. Report delivery time 90% x-ray and
ultrasound
reports delivery on
time as per policy
Technician
I
radiologist
Weekly
4. Wastage of film because
of repeat process
Less than 7% Technician /
Radiologist
Monthly
5. Uptime of equipment 95 % - 98 % Supervisor
Technician
I
Radiologist
Monthly
iv. Applicable to Intensive care department (Table 4)
S.
No.
Key
Characteristics
Acceptance
Norms
/
Criteria
Responsibility
And
Conformance
Verification
Frequency
1 Infection control and
sterility
Weekly swab
culture
In charge / staff Once in a
week
2 Monitoring and
measurement of life
saving equipment and
other equipments
Functional status
check.
Calibration -
Yearly/as and
when required
AMC/Preventive
Maintenance -
Yearly/as and
when required
In charge I staff Monthly

v. Applicable to surgical services department (Table 5)
S.
No.
Key
Characteristics
Acceptance Norms I
Criteria
Responsibility
And
Conformance
Verification
Frequency
1. Punctuality of O. T staff Start functioning at
time
OT in charge Once in a week
2. Complete pre operative
preparation before patient
is shifted to O.T
Part preparation
Removal of all
ornaments.
Consent for
procedure
Change of
clothes.
Ward staff &
O.T. Staff
Daily
3. Anesthesia induced after
17.00 hrs.
Acceptable only during
emergency
Anesthetist Once in a week
4. Cases continuing beyond
19.00 hrs.
Acceptable only when
necessary
Anesthetist Once in a week
5. Infection Control and
sterility of O. T
Weekly air culture
Weekly fumigation
Hypochlorite
treatment of
infected linen /
instruments for 3 –
4 hrs before
autoclaving.
Restricted entry of
visitors into O.T.
complex
OT incharge /
OT
Staff
Once in a
week.

vi. Other Clinical & Managerial Indicators used for quality assurance and
continuous monitoring: (Table 6)
Following indicators are measured and monitored by quality assurance
committee as a part of quality assurance and continuous monitoring programme
Indicators for clinical & managerial structure, process and outcome.
S No.
Indicator NABH Std.
Definition Numerator Denominat
or
Source of Data /
Responsibility
Patient Assessment
1 Allergy Documentation
IMS.7 (CQI -
2.a)
Appropriate documentation of all the drugs and other agents to which a patient is allergic is called allergy documentation
No. of cases where allergy was recorded in History & Physical Examination Sheet
No. of discharged files checked
MRD
2
Completion of History & Physical Examination (Initial Assessment Form)
AAC.5
Completion of History & Physical Examination Sheet implies that on admission, the doctor has done the initial assessment of the patient and filled up all fields of H & P Sheet
No. of complete H & P sheets
No. of discharged files.
MRD
S No.
Indicator NABH Std.
Definition Numerator Denominat
or
Source of Data /
Responsibility
3
Completion of Nursing Admission Assessment
AAC.2
Completion of Admission Assessment form by filling up all fields
No. of cases where assessment were completed
No. of discharges
MRD

4 Nutritional Assessment AAC.5
Assessment of patient’s nutritional status at the time of admission of the patient is called nutritional assessment
No. of cases where assessment was completed
No. of discharges
MRD
5 Pre Anesthesia Check up
(CQI - 2.e)
Pre Anesthetic Assessment completed for patients undergoing any kind of anesthesia
No. of cases where assessment was completed
No. of surgeries
MRD
Anesthesia Use
6 Adverse Anesthesia Events
COP.11 (CQI - 2-e)
Adverse Anesthesia Events are the incidents which occur directly or indirectly due to administration of Anesthesia in the form of Drug, Procedure, Invasive monitoring or position of the patient, which has resulted in unpleasant outcome.
No. of adverse anesthesia events
Total no. of surgeries done
Medical Record of
patient
S No.
Indicator NABH Std.
Definition Numerator Denominat
or
Source of Data /
Responsibility
Blood and Blood Products
8. Hemolytic Reactions
Any Serious adverse reactions arising after blood & blood products transfusion
Total Number of Such Reactions
Total Number of units transfused
BTR Committee
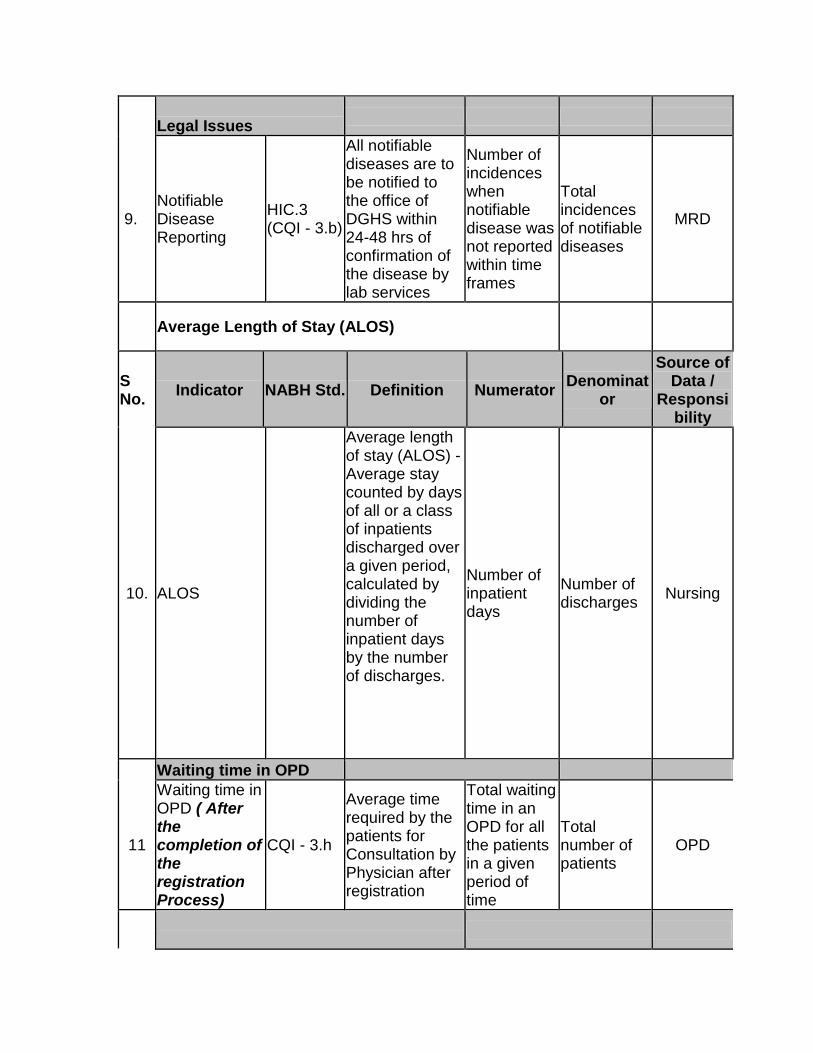
Legal Issues
9. Notifiable Disease Reporting
HIC.3 (CQI - 3.b)
All notifiable diseases are to be notified to the office of DGHS within 24-48 hrs of confirmation of the disease by lab services
Number of incidences when notifiable disease was not reported within time frames
Total incidences of notifiable diseases
MRD
Average Length of Stay (ALOS)
S No.
Indicator NABH Std. Definition Numerator Denominat
or
Source of Data /
Responsibility
10. ALOS
Average length of stay (ALOS) - Average stay counted by days of all or a class of inpatients discharged over a given period, calculated by dividing the number of inpatient days by the number of discharges.
Number of inpatient days
Number of discharges
Nursing
Waiting time in OPD
11
Waiting time in OPD ( After the completion of the registration Process)
CQI - 3.h
Average time required by the patients for Consultation by Physician after registration
Total waiting time in an OPD for all the patients in a given period of time
Total number of patients
OPD

Discharge Time
S No.
Indicator NABH Std.
Definition Numerator Denominat
or
Source of Data /
Responsibility
12 Discharge
Time
Average time required by the organization to discharge the patient after the decision to discharge has been conveyed to the patient & documented
Total time taken for discharge process of all the patients in a day
Total number of patients discharged in that day
Discharge Register
Infection Control
13 UTI HIC.4 (CQI - 2.h)
Urinary tract infection includes symptomatic UTI asymptomatic bacteriuria & other infections of urinary tract.
No. of Catheterized patients developing UTI in the hospital
Total no of urinary catheter days
Infection Control Team
14 CRBSI HIC.4
CR Blood Stream infection includes positive cultures from patients with central lines(after 48 hrs of infection)
No. of patients with central lines developing BSI in the hospital
Total central line days
Infection Control Team
S No.
Indicator NABH Std.
Definition Numerator Denominat
or
Source of Data /
Responsibility
15 SSI HIC.4
Involves patients developing SSI within 30 days of surgery
No. of patients developing SSI after surgery
No. of patients undergoing same surgeries
Infection Control Team

16 VAP HIC.4
Pneumonia involves a combination of clinical, radiological & lab evidence of infection. Any new progressive lesion that develops after 48 hrs of hospital admission or subsequent to ventilator use is labeled as VAP
Patient with 3 out of 4 criteria for hospital onset pneumonia
Total ventilator days
Infection Control Team
17 Hand Hygiene HIC.5
Hand Hygiene is defined as either using soap and water to wash hands or use of Hand rubs before and after opportunities as indicated in Infection Control Manual
Total number of times hands have been washed for the activities defined
Total number of hand hygiene episodes defined for the activities included
Infection Control Team
S No.
Indicator NABH Std.
Definition Numerator Denominat
or
Source of Data /
Responsibility
Utilization Management
18 OT utilization FMS.3 (CQI - 3.d)
It is the no. of hours per day for which the OT is utilized for Operative purposes.
No. of hrs OT is utilized
Operational hrs of OT
OT registers, OT Staff
Patient Satisfaction
20 Patient satisfaction
Number of patients satisfied with the organization's services and
No. of patients who gave very satisfied score in Patient
Total no. of discharge feedbacks collected
Data assistants, Patient Satisfaction Survey

award a grading of very satisfied in the patient satisfaction survey
satisfaction survey
Staff Satisfaction
21 Nursing staff satisfaction
HRM (CQI - 3.f)
Being the largest group in hospital, this group's satisfaction measurement will give a representation of staff satisfaction
No. of staff scored above average
Total no. of feedbacks
HR Manager
22 Other Staff Satisfaction
Do
The satisfaction index of the other employees is also required to foresee the organizational climate
No. of staff scored above average
Total no. of feedbacks
HR Manager
Safety Issues
23 Needle Stick Injury Reporting
HIC.5
Sustenance of injury due to accidental needle stick by any health care worker at the workplace resulting in inoculation of infectious material.
No. of incidents Occurred & Reported
Nursing





























