Embed Size (px)
Citation preview

Quality improvement initiatives of mental health services in Japan
Hiroto Ito, Ph.D.Department of Social Psychiatry
National Institute of Mental HealthNational Center of Neurology and Psychiatry

Japan, a leader of high quality products
High quality productsKaoru Ishikawa (1915‐1989), Fishborn diagramTaichi Ono (1912‐1990), TOYOTAAkio Morita (1921‐1999), Sony
1986: Imai M. “KAIZEN”1989: Berwick DM. N Engl J Med 320: 53‐6.2004: Liker J. “THE TOYOTA WAY”

“Quality” is a new conceptin Japanese healthcare organization*
1980’s: Self‐check manuals for hospitals
1987: A committee of Tokyo JCAHO (Joint Commission on
Accreditation of Healthcare Organizations)
1990: Japan Society for Quality in Health Care (JSQua)
1995: Japan Council for Quality Health Care (JCQHC)
1997: JCQHC start formal accreditation activities
*Ito H, et al. Int J Qual Health Care 10:361‐363, 1998.

Examples of Quality Improvement Initiatives
• Japan Council for Quality Health Care (JCQHC), 1997
• JCI Accreditation (2009‐)
• Clinical Indicators by National Hospital Organization (2010‐)

Challenges
• Bench‐marking systems in mental health field–“multi‐centre” quality improvement programs–especially for the process of care and outcomes
• Clarifying process of care–Using management techniques in Japan

Outline of my talk
1. “Mental Health Care KAIZEN projects”• Suicide prevention program in psychiatric inpatient care• Infection control initiative in psychiatric hospitals• Feedback system of quality of mental health care
2. Process‐visualization project in psychiatric services
3. Conclusions

Nation‐Wide Suicide Prevention Project in Stress‐Care Units
Shiranui Hospital(Fukuoka, 1989)
Nishi Hachioji Hospital(Tokyo, 1998)
*Soutce: Tokunaga Y (personal communication)
Matsubara Hospital(Fukui, 1997)
Kusatsu Hospital(Hiroshima, 2000)
Welfare Kyushu Hospital(Kagoshima, 1996)
Kansai Kinen Hospital(Osaka, 2003)
Kaya Hospital(Fukuoka, 2001)
Asaka Hospital(Fukushima, 2002 & 2008)
Iwaki Hospital(Kagawa, 1988)
Sawa Memorial Hamamatsu Hospital(Shizuoka, 2002)
Jindai Hospital(Aichi, 2002)
Toda Hospital(Saitama, 1986)
Nishiwaki Hospital(Nagasaki, 2001)
Narimasu Kosei Hospital(Tokyo, 2008)
Yonan Hospital(Gifu, 2006)
Hannan Hospital(Osaka, 1997)
Shinoda‐no‐mori Hospital(Chiba, 2007)
Uji‐Obaku Hospital(Kyoto, 2001 & 2008)
Goryokai Hospital(Hokkaido, 2004)
Iougaoka Hospital(Ishikawa prefecture)
Yahata Kosei Hospital(Fukuoka)
Hijiyama Hospital(Hiroshima, 2011)

Nosocomial Infection in Patients with Mental Disorders
1. Vulnerability to nosocomial infection– Poor self‐care– Closed environment– Older age
2. Potential transmitter of nosocomial infection– Delayed diagnosis– Uncooperative attitudes
Hayato Yamauchi, MD. (Saiki Hoyoin Hospital)

45 members from 36 hospitals
Infection Control Initiative by theInfection Control Association for Psychiatry (ICAP)*
• Various training programs on Infection Control– Tuberculosis and scabies**– Appropriate use of antibiotics– Controlling the spread of infections
• Outcomes– Improved prevention of nosocomial infection – More infection control rounds
*Professor Noriaki Nukanobu (Hiroshima International University), et al. IHI, 2016**Others include HBV, HCV, HIV (acute patients) , influenza, norovirus, and O157 (long‐term care patients)

Feedback system of quality of mental health care: Concept
Diagnosis, Functioning level (eg. GAF), etc.
Seclusion/Restraint, etc.
Your hospital
Average
Controlledrange
Your hospital Average*Feedback using eCODO system (seclusion/restraint and other quality
indicators) NCNP: National Center of Neurology and Psychiatry
Every 3 months Time
Benchmark(international)
Data inpu
t at h
ospital
Second
ary an
alysis of “an
onym
ized
” da
ta
Feed
back to
hospital
Goa
l settin
g at hospital
percen
tage

A ten-year activity using electronic Coercive measures Database for Optimization (eCODO)
2006
2007
2008
2009
2010
2011
2012(3 hospitals)
2013(6 hospitals)
2014(6 hospitals)
2015
Multi-center peer review(February)
Regional exchange in Osaka(November)
Training program(June)
International exchange(Finland)
Start of the project
eCODO edge server (ver.1)
eCODO edge server (ver .2.0)
NCNP introduced eCODO system (October)
eCODO edge server (ver .2.1)
eCODO edge server (ver .3.1)
Psychiatric Electronic Clinical Observation(PECO)

Outline of my talk
1. “Mental Health Care KAIZEN projects”• Suicide prevention program in psychiatric inpatient care• Infection control initiative in psychiatric hospitals• Feedback system of quality of mental health care
2. Process‐visualization project in psychiatric services
3. Conclusions

Tools for Standardization‐ Clinical Pathway for inpatient ‐
Phase 1 Phase 2 Phase 3
Outcome
Pharmacological intervention
Psycho-social intervention
Preparation for discharge
…

“Chain model” clinical pathway
Overview pathway
Clinical Pathwayfor early stage after discharge
Clinical Pathway for
maintenance stage
Clinical Pathway for inpatient
Phase1 Phase2 Phase3
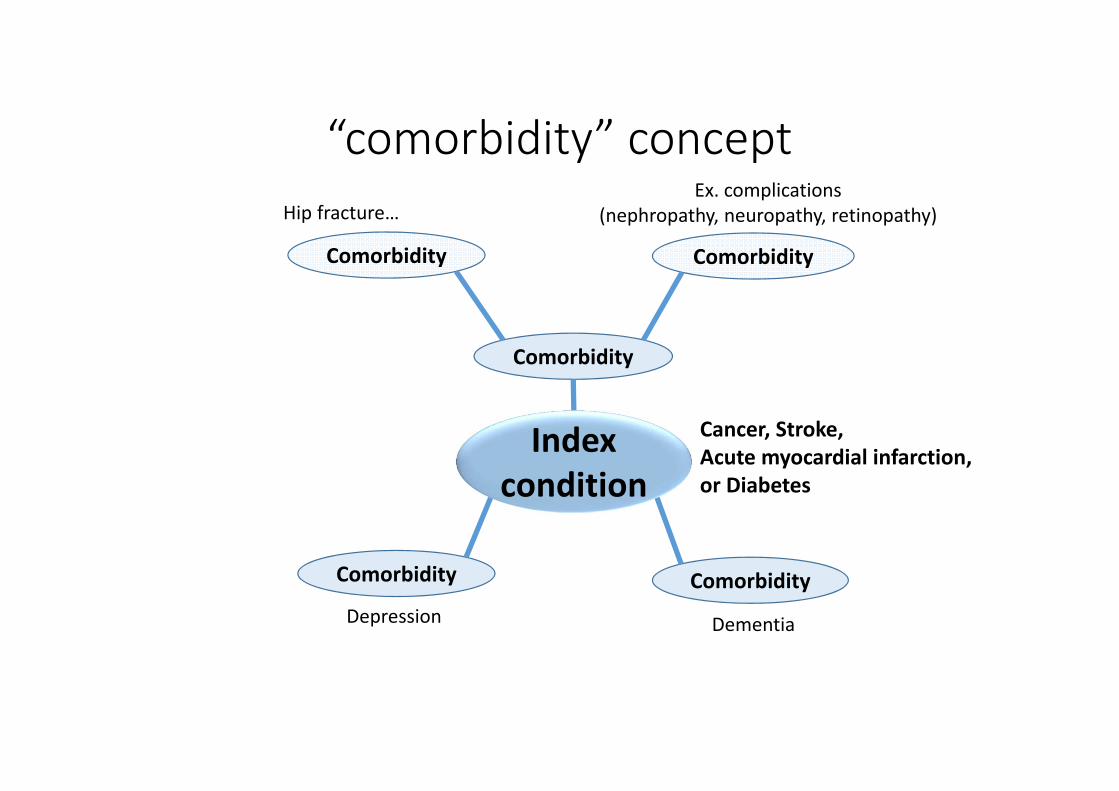
“comorbidity” concept
Index condition
Comorbidity
Comorbidity ComorbidityDepression Dementia
Comorbidity Comorbidity
Hip fracture…Ex. complications
(nephropathy, neuropathy, retinopathy)
Cancer, Stroke,Acute myocardial infarction,or Diabetes

Multimorbidity in ageing societyCombinations of 3 diseases*
Diabetes (774,100: 56.9%)
Hypertension(1,090,200人: 80.1%)
Hyperlipidemia(838,200人: 61.6%)
30,200 (2.2%)
391,600(28.8%) 139,900
(10.3%)
212,400(15.6%)
457,300(33.6%)
101,400(7.4%)
[Total] 1,361,400
28,600(2.1%)
*Japan Patient Survey (2008)Tsushita K, et al. 2014 (in Japanese)
1 disease: 11.7%2 diseases: 78.0% 3 diseases: 10.3%
“Clinical care is often fragmented, involving both primary care and multiple secondary care specialists who may not be communicating effectively” with each other, and “there is a clear need for integrated care of multiple conditions” [1, 2‐5].
1. Smith SM, et al. BMJ 345: e5205, 2012. 2. Stange KC. Ann FamMed 10: 2‐3, 20123. Bayliss EA. Simplifying care for complex patients. Ann FamMed 10: 3‐5, 2012.4. Kamerow D. BMJ 344: e1487, 2012. 5. Smith SM, et al. Br J Gen Pract 60: 285‐294, 2010.

“Web model” needed for integrated care*
Low
High
High Low
Chain model
Hub model
Web model
Level of predictability
Ex. internal medicine, rehabilitation, psychiatry, palliative care processesCase manager coordinates sub‐processes
Ex. chemotherapy processesGantt charts
Ex. multimorbidityChange from ‘time’–task matrix
into a ‘goal’–task matrix
*Modified figure by Kris Vanhaecht, et al. Int J Care Pathways 14: 117–123, 2010.
Level of agreemen
t
Index condition

Web model: Personalized Notebook for patients with multimorbidity*
・・・
PersonalizedNotebook
using
Initially registered as
<Dementia><Depression><Diabetes><Heart disease><Schizophrenia><Stroke><…>
Hypertension
DepressionDiabetes
Cancer
Heart disease
Schizophrenia
Stroke
Dementia*Developed in collaboration with<Six national centers>NCC: National Cancer Center NCCV: National Cerebral and Cardiovascular CenterNCNP: National Center of Neurology and Psychiatry NCGM: National Center for Global Health and MedicineNCCHD: National Center for Child Health and Development NCGG: National Center for Geriatrics and GerontologySource: Ito H, et al. Shakai Hoken Jyunpo 2531: 10‐14, 2013 (in Japanese).
+Life style monitoring+Advance directives

Depression and other chronic diseases (meta‐analysis)*
Unh
ealth
y lifestyle
Dementia
Vascular
Alzheimer type
Diabetes Depression
StrokeLacunar infarction
Atrial fibrillation
Hypertension1.59 [1.29‐1.95] 2)
2.52 7)
1.657)
1.39 [1.17‐1.66] 1)
2.38 [1.79‐3.18]1)
10% (recurrent: 1/3) 8)
10%8)
*Meta analysis/systematic review.1)Lu FP, et al. 2009 2)Sharp SI, et al. 2011 3)dChang‐Quan H, et al., 2011 4)McGuinness B et al., 2009 5)Power MC, et al. 2011 6)Kalantarian S, et al., 2013 7)Diniz BS, et al. 2013 8)Pendlebury et al., 2009 9)Makin SD, et al., 2013 10) Mezuk B et al., 2008 11)Pan A et al., 2012 12)Nouwen A, et al., 2010 13) Rotella F, et al., 2013 14)Ayerbe L, et al., 2013 15)Dong JY, et al., 2012 16) Nicholson A, et al., 2006 17) Van der Kooy K, et al., 2007 18) Peters SA et al., 2014 19)Peters SA, et al., 2014 20)Petgen T, et al., 2012
20 [9‐33] %9)
1.38[1.22‐1.56] 6)
Not significant5)
1.4~1.610‐11)
1.15 (2008)10)1.24 (2010)12)1.29 (2013)13)
1.29 [1.25‐1.32]14)1.34[1.17‐1.54]15]
Myocardial infarction
1.81 [1.53‐2.15]16)1.60 [1.34‐1.92]17)
Coronary artery18)F: 2.82 [2.35‐3.38]M: 2.16 [1.82‐2.56]
F: 2.28 [1.93‐2.69]M: 1.83 [1.60‐2.08]19)
Adherence/ exercise / diet/ alcohol consumption/ sleep/ other lifestyles
Decline of renal function
CKD guide2012
1.39 [1.15‐1.68]20)
Death

Fishbone (or Ishikawa*) diagram
Polypharmacyof
Antipsychotics
PatientNursePhysician
MethodSystem
Insufficient timeto assess patients
Insufficient physician
Insufficient supervision
ReluctantTo change
Reluctantto changemedications
Chronicdisease
Fear of relapse
Attitudes not to follow guidelines
Ito H, Koyama A, Higuchi T. Br J Psychiatry 2005.Goh YL, Seng KH, Su A, et al. Permanente Journal 15: 52‐56, 2011.
Rotation of physicians
Fee‐for‐service
Limited incentives
Limited alternatives
No practical guideline how to decrease numberof antipsychotics
*Kaoru Ishikawa, PhD. (1915 ‐ 1989)
Professor, Faculty of Engineering The University of Tokyo
Quality Management Innovations

Unit transition of 10 inpatients*
A: Main routI: Sub rout(seclusion/restraint)
Case [1]:Unit A1→A2→I2→A2→A5[2]:A1→A2→I1→A2→I1→I4→A2→A4→A5[3]:A1→I2→I3→I2→I3→I4→I3→I4→A2→A5[4]:A1→I3→I4→I3→I2→I4→A2→A5[5]:A1→I2→I3→I4→A2→I2→I4→A2→A5[6]:A1→I2→I3→I4→I3→I4→A2→A4→A5[7]:A1→I2→I1→I2→I4→A2→A3→A5[8]:A1→I2→I1→I2→I3→I4→A2→A5[9]:A1→I3→I4→I3→I4→A2→A3→A4→A5[10]:A1→I2→I3→I4→I3→I4→A2→A4→A5
*Satoko Tsuru (University of Tokyo)

Conclusions
• Quality issues: multi‐dimensional
• Quality improvement stages
1. In‐hospital quality improvement
2. Multi‐centre activities
3. International platform