Embed Size (px)
Citation preview

Quality of Maternal Health Services and their Utilization in Five States of Nigeria
Anastasia J. Gage, Ph.D.a, Onyebuchi Ilombu, MPH a, and Akanni Ibukun Akinyemi, Ph.D. b a Tulane University, b Obafemi Awolowo University
August 13, 2013
Corresponding author: Anastasia J. Gage, Department of Global Health Systems and Development, Tulane University, 1440 Canal Street, Suite 2200 TB-46, New Orleans, LA 70112, Phone: 504-988-3647, Fax: 504-988-3653, Email: [email protected]; [email protected]
Acknowledgments
The data analyzed in this paper was funded by the U.S. Agency for International Development (USAID) through Cooperative Agreement GHA-A-00-08-00003-00. The authors’ views expressed in this publication do not necessarily reflect the views of USAID or the United States Government. USAID played no role in the study design; in the collection, analysis and interpretation of data; in the writing of the article; and in the decision to submit it for consideration for presentation.

Abstract Using linked data from the 2009 COMPASS health facility and household surveys, this paper
examines the association of the quality of maternal health services with their use in the past five
years in five states of Nigeria. The results of multilevel logistic regression models revealed a strong
positive association between the availability of essential delivery care equipment and supplies and
the odds of initiating antenatal care in the first trimester of pregnancy. The odds of institutional
delivery were significantly higher in Local Government Areas (LGAs) that scored higher on
management practices that were supportive of quality maternal health services than in LGAs that
scored lower, after controlling for other factors. More comprehensive provider training on maternal
health had a significant negative association with skilled attendance at birth and institutional
delivery. The findings suggest that efforts to increase the utilization of maternal health services
should improve health facility management practices, ensure the availability of essential equipment
and supplies, and conduct further research to better understand how provider training may
influence service use.

1
Introduction
Although substantial progress has been made in reducing maternal mortality worldwide, the
World Health Organization estimates that in 2010, 287,000 women died from potentially avoidable
or preventable problems in pregnancy or childbirth (WHO, 2012). Sub-Saharan Africa accounted for
more than half of the global burden of maternal deaths, with women in the region having a 1 in 39
chance of dying in pregnancy or child birth compared to a 1 in 3,800 risk in developed countries
(WHO, 2012) – the largest difference between poor and rich countries on any health indicator.
Nigeria, which constitutes less than 1 percent of the world population, had an estimated maternal
mortality ratio of 630 maternal deaths per 100,000 live births in 2010 and accounted for 14 percent
of global maternal deaths. Uptake of maternity care is relatively low in Nigeria. Data from the 2008
Nigeria Demographic and Health Surveys revealed that 58 percent of women who had a live birth in
the five years preceding the survey sought antenatal care from a skilled provider (doctor, nurse,
midwife or auxiliary nurse/midwife) and 48 percent reported visiting antenatal clinics at least four
times during pregnancy. Thirty-five percent of births occurred in a health facility and 39 percent
were assisted by a skilled provider (National Population Commission and ICF Macro, 2009). In light
of achieving the Millennium Development Goal of reducing the maternal mortality ratio by three-
quarters and improving access to reproductive health, there is an urgent need to examine how the
quality of care and other factors may improve the utilization of maternal health services.
It is widely acknowledged that the quality of health services has significant implications for
health outcomes. Empirical studies have confirmed that poor quality services may be associated
with low uptake of care and non-effective and non-timely management of life-threatening
complications of pregnancy and childbirth (Althabe et al., 2008; Fauveau and de Bernis, 2006; Raven
et al., 2012). The lack of sufficient drugs, reagents and instruments often prevents health workers
from preventing fatal outcomes and poor patient-provider interaction often may leave women
uninformed with little understanding of the importance of maternal health services (Conrad et al.,
2012). By comparison, receipt of good quality antenatal care has been found to significantly
2
increase the chances of delivery attendance by skilled medical personnel (Adanu, 2010). It has also
been noted that the availability of quality services may not produce desired health outcomes if there
is little possibility for individuals to make healthy decisions and act on those decisions (World Health
Organization, 2010), suggesting the need for examining the relative contributions of supply and
demand-side factors to maternal health outcomes.
There is no consensus on the definition of the quality of maternal health care, partly due to
the inherent complexities of measuring the concept (Raven et al., 2012). Early attempts to define
and measure the quality of maternal health services were based on the quality of health framework
developed by Donabedian (1988), which focused on three aspects of health service delivery:
structure, process, and outcome. Structure refers to characteristics of the setting in which health
services are delivered, including the physical equipment, infrastructure, human resources, as well as
organizational characteristics, staff training, and remuneration. Process refers to the technical and
interpersonal aspects of provider-client interactions in health service delivery. This includes
diagnosis, patient education, communication and preventive care. Outcomes include health status,
health behaviour, knowledge, and client satisfaction. Hulton et al.’s (2005) quality of care
framework is instructive as it separates quality into two constituent parts: quality of the provision of
care within the institution and quality of care as experienced by users. The framework identifies 10
elements in assessing the quality of maternal health services, six of which relate directly to the
provision of care (human and physical resources; referral system; maternity information systems;
use of appropriate technologies; internationally recognized good practice; and management of
emergencies). The other four elements are related to women’s experience and include cognition;
respect; dignity and equity; and emotional support).
Studies in sub-Saharan Africa have used different methodologies for evaluating the quality of
care in maternal health, including facility audit and clinical records (Sharan et al., 2011), exit
interviews (Osungbade et al., 2008), and community-based surveys (Galadanci, 2007). Such
evaluations have focused on assessing infrastructure, equipment, and supplies; type of care
3
provided; provider-client experiences (Conrad et al., 2012); the availability of skilled providers
(Rockers et al., 2009); the actual services that are performed during antenatal care visits such as
abdominal examinations, blood pressure measurement, blood and urine examinations (Galadanci et
al., 2007); and the availability of services such as emergency obstetric care and neonatal health care;
referral systems; and transportation (Kongnyuy et al., 2009). The interpersonal dimensions of care
are often overlooked, partly due to lack of data. These aspects include the social and psychological
aspects of care – welcoming of clients, staff helpfulness and friendliness, provider communication,
and patient understanding.
Studies have generally shown that maternal health services in some countries of sub-
Saharan Africa are deficient in terms of providing basic emergency obstetric care (Conrad et al.,
2012; Ijadunola et al., 2010) and lack the capacity to perform tests for syphilis and bacteriuria or
address the effects of severe anemia and malaria in pregnancy (Osungbade et al., 2008). Maternal
health services have also been noted to lack essential drugs, reagents and instruments, to have poor
quality patient education, to lack timely referral and transportation services, and to have an
inadequate number and mix of skilled providers (Kongnyuy et al., 2009). Poor record keeping in
maternal health facilities has also been noted to hinder patient monitoring (Sarker et al., 2010).
Many studies have also evaluated maternal health care utilization outcomes in their assessment of
the quality of maternal health services and have concluded that in many parts of sub-Saharan Africa,
levels of maternal health care are poor (Ijadunola et al., 2010). However, few studies have linked
the supply aspects of maternal health care to demand for maternal health services.
Tremendous resources have been expended on health facility surveys in sub-Saharan Africa.
However, few of them are conducted in tandem with or designed to be linked to household surveys,
making it difficult to assess the influence of service quality on the utilization of maternal health
services. The objectives of this study were to examine the association between the quality of
maternal health services and their use in five states of Nigeria. It is hypothesized that women would
be more likely to use maternal health services in local government areas (LGAs) with higher indices
4
of (a) provider training in maternal health care; (b) supportive maternal health care management
practices; (c) availability of basic equipment and supplies for the provision of antenatal and
delivery/newborn care services.
Data
The data for the present study were drawn from the 2009 end-of project survey for the
Community Participation for Action in the Social Sectors (COMPASS) project in Nigeria. The study,
which consisted of a health facility survey, a household survey, and a school survey, was
implemented by MEASURE Evaluation/Tulane University and the Center for Research, Evaluation
and Resource Development (CRERD). The survey was conducted in 51 local government areas
(LGAs) in the Federal Capital Territory (FCT) and the states of Bauchi, Kano, Lagos, and Nasarawa
where the COMPASS project was implemented. The purpose of COMPASS was to integrate health
and education by enhancing FP/RH services, promoting child survival and improving basic literacy
and numeracy. The Institutional Review Board of Tulane University and CRERD granted ethical
approval for the study.
The household survey used a multi-stage stratified sampling design and collected
information on reproductive and maternal health, child health, and primary school education among
a representative sample of women aged 15-49 and men aged 15-64. At the first stage of sampling,
enumeration areas were selected within each state, with probability proportional to the number of
LGAs per state as follows: 1:1:2:2:1 for Bauchi, FCT, Kano, Lagos, and Nasarawa, respectively. At the
second stage of sampling, 25 households were selected within each sample enumeration area using
systematic random sampling. Fieldwork for the household survey started in mid-June 2009 and was
completed by early July, 2009.
The survey of primary health care facilities (comprehensive health care centers, public
primary health care centers, health clinics, maternity clinics, private clinics, uniformed services
clinics, health posts, and dispensaries) and patent medicine vendors (PMVs) was implemented at the
same time as the household survey. The sample for the facility survey was drawn from a list of all

5
public and primary health care facilities and PMVs serving the population interviewed in the
household survey. As a result, the facility survey included some service delivery points that were
located outside of the enumeration areas selected for the household survey. Due to sample size
considerations, the LGA (as opposed to the enumeration area) was used to link the facility and
household survey in order to determine the influence of maternal health service quality on
individual health outcomes. To the extent possible, all primary health care facilities and PMVs were
included when defining LGA-based measures of HF readiness and the quality of care.
Outcomes
Four outcomes were examined: initiation of antenatal care (ANC) in the first trimester of
pregnancy; receipt of four or more ANC visits; delivery assistance by a skilled provider; and delivery
in a health facility. All outcomes were dichotomous.
LGA-level Variables
Four variables measured the quality of maternal health care at the LGA-level: (a) index of
provider training in maternal health care; (b) index of supportive management practices; (c) index of
the availability of basic equipment and supplies for the provision of antenatal services; and (d) index
of the availability of basic equipment and supplies for the provision of delivery/newborn care
services.
Index of provider lifetime in-service training in maternal health (antenatal care (ANC)/ postpartum
care (PPC) and delivery/newborn care): Eight items measured whether the ANC/PPC provider had
ever received in-service training in each of the following subjects: (a) antenatal care; (b)
counseling/health education for maternity clients; (c) management of risk pregnancies; (d) mother-
to-child transmission of HIV/AIDS; (e) postnatal care; (f) family planning; (g) sexually transmitted
infection; (h) other subjects. Each component was a dichotomous variable measuring whether
training in a given subject had been received. An additional 8 items measured whether the
delivery/newborn care provider had ever received in-service training in each of the following
subjects: (whether the health care provider had ever received training on the following subjects: (a)

6
care during labor and delivery; (b) use of partograph; (c) life-saving skills/emergency complications;
(d) other delivery care subject; (e) neonatal resuscitation; (f) mother-to-child transmission of
HIV/AIDS; (g) exclusive breastfeeding; and (h) other newborn care training. Cronbach’s alpha for the
resulting index was 0.9539. The index ranged from 0 to 16. The LGA-based index represented the
mean provider MH training index per facility in the LGA. The LGA-based index ranged from 0 to 9,
with an average of 2.689 [SD = 2.324] per LGA surveyed.
Index of management practices supportive of quality maternal health (ANC/PPC or
delivery/newborn care) services: Components of this 28-item measured the presence of observed
up-to-date client registers with entry in the past 7 days; availability of systems for client feedback;
content of supervisory visits of ANC service provision in the past 6 months; and routine use of quality
assurance methods. Questions on use of quality assurance methods asked non-PMVs whether any
of the following methods of quality assurance were routinely used by the facility: (a) supervisory
checklist for health system components (e.g., service-specific equipment, medications and records)
based on standards and protocol; (b) supervisory checklist for health service provision (e.g.,
observation checklist) based on standards and protocol; (c) system for identifying and addressing
quality of care that is implemented by staff or specific service level; (d) facility-wide review of
mortality; (e) periodic audit of medical records or service registers; (f) quality assurance
committee/team; (g) regional/district health management teams; and (h) other method.
Components pertaining to ANC supervision measured (h) number of times in the last six
months the provider’s ANC and/or PPC work has been supervised and for the most recent
supervisory visit, whether the supervisor (i) checked the provider’s records/reports; (j) observed
his/her work; (k) provided feedback on his/her performance; (l) provided updates on administrative
or technical issues related to his/her work; (m) discussed problems the provider had encountered;
(n) discussed job expectations; and (n) anything else.
Components pertaining to supervision of delivery/newborn care measured (h) number of
times in the last six months the provider’s delivery/newborn care was supervised and for the most
7
recent supervisory visit, whether the supervisor (i) checked the provider’s records/reports; (j)
observed his/her work; (k) provided feedback on his/her performance; (l) provided updates on
administrative or technical issues related to his/her work; (m) discussed problems the provider had
encountered; (n) discussed job expectations; and (n) anything else.
Components pertaining to the availability of systems for client feedback asked whether the
health facility had the following systems for determining client opinion about the health facility or its
services: (o) suggestion box; (p) client survey form; (q) client interview; (r) other system. The variable
measuring up-to-date ANC client registers consisted of four categories: no register, register not seen,
register seen – last entry more than 7 days ago, and register seen – entry in past 7 days.
Components pertaining to supervision measured (h) number of times in the last six months the
provider’s delivery/newborn care was supervised and for the most recent supervisory visit, whether
the supervisor (i) checked the provider’s records/reports; (j) observed his/her work; (k) provided
feedback on his/her performance; (l) provided updates on administrative or technical issues related
to his/her work; (m) discussed problems the provider had encountered; (n) discussed job
expectations; and (n) anything else.
The variable measuring up-to-date birth registers consisted of four categories: no register,
register not seen, register seen – last entry more than 7 days ago, and register seen – entry in past 7
days. One component of the index measured whether a skilled birth attendant (doctor, nurse or
midwife) was present at the facility or on call 24 hours a day, including weekends to provide delivery
care and their actual involvement in conducting deliveries. This variable was coded as follows: 4 if a
skilled attendant was present and always conducted deliveries; 3 if a skilled attendant was present
but deliveries were sometimes conducted by primary or auxiliary level staff; 2 if a skilled attendant
was on call and always conducted deliveries; 1 if a skilled attendant was on call but deliveries were
sometimes conducted by primary or auxiliary level staff; and 0 if a skilled attendant was not present
or on call 24 hours a day, including weekends, to provide delivery care. The resulting additive
8
facility-based index ranged from 0 to 23 and had a Cronbach’s alpha of 0.9109. Our LGA-based
index was the mean management practices index per MH non-PMV in the LGA.
Index of essential equipment and supplies for quality ANC and PPC services: The index comprised the
following essential equipment: (a) blood pressure gauge; (b) stethoscope; (c) fetal stethoscope.
These components of the index were binary and measured the availability of the equipment. Other
components of the scale measured:
Availability of the following medicines for treating pregnancy complications: (f) amoxicillin; (g) contrimoxazole;
Availability of the following first line antimalarials: (h) Artemisine (Cotecin); (i) Coartem; and (j) Quinine;
Availability of the following (additional) medications for treating the three common STIs, namely, gonorrhea, chlamydia, and syphilis: (k) Cotrimoxazole (Septrin); (l) Doxycycline PO (Vitadar); (m) Erythromycin oral; (n) Benzathine benzyl penicillin injection (IM); (o) Benzyl Penicillin (Procaine) injection (IM/IV); (p) Streptomycin injection.
Availability of Sulphadoxine-Pyrimethamine: (q) Amalar; (r) Fansidar;
Availability of tetanus toxoid vaccine (in stock)
With the exception of tetanus toxoid vaccine, which was binary, each of the other components of
the scale comprised three categories: observed, reported and not available, which were coded 2, 1,
and zero, respectively. No data were collected on medication for treating trichomoniasis or on
equipment and supplies for conducting diagnostic tests for anemia, urine protein, urine glucose or
syphilis. The resulting 16-item facility-based index had a Cronbach’s alpha of 0.9269 and ranged
from 0 to 28. Our measure of the LGA index of essential equipment and supplies was the mean index
per health facility in the LGA and ranged from 0 to 23, with a mean of 8.956 [SD = 5.209] per LGA
surveyed.
Index of essential equipment and supplies for quality delivery and newborn care services: The index
comprised the following essential equipment and supplies for delivery: (a) skin antiseptic (e.g.,
chlorhexidine, savlon, detol); (b) intravenous infusion set; (c) injectable ergometrine; (d) syringes
and needles; (e) suture material with needle; (f) sterile scissors/blade; (g) needle holder; (h) manual
vacuum aspirator; and (i) dilation and curatage kit. Other components of the index measured the
availability of the following supplies for the baby: (j) bag and mask or tube and mask for baby
9
resuscitation; (k) baby scale; (l) baby height scale; (m) tape rule; (n) mucous extractor; and (o) cord
ties or clamps. All components of the index were binary and measured the availability of a given
item. The resulting 15-item facility-based index had a Cronbach’s alpha of 0.9739 and ranged from 0
to 15. Our measure of the LGA index of essential equipment and supplies for delivery and newborn
care was the mean index of delivery/newborn care health facility in the LGA and ranged from 0 to
15, with a mean of 6.4 [SD = 5.237] per LGA surveyed. Each of the above-listed indices was
categorized into a binary variable indicating whether the LGA was at/above or below the median
value of the index of interest for all LGAs included in the analysis.
Individual-level variables
The analysis also controlled for the following individual-level variables: age (as reported in
continuous years); highest level of school attended (none (reference group), primary, or secondary
or higher); marital status (married (reference group); living together; or not in union); type of place
of residence (rural (reference group) versus urban/semi-urban); state (Lagos (reference group);
Bauchi, Kano, Federal Capital Territory, or Nasarawa); household wealth (low (reference group),
medium or high); and perception of distance as a big problem in accessing health services (yes or
no). Household wealth represented terciles of an index constructed from the presence of the
following amenities or items in the household, using principal components analysis: refrigerator,
electricity, piped water, flush toilet, a bicycle, a motorcycle, a car, television, radio, and a
telephone/cellular phone). The first component was used as the measurement of household wealth
since it explained the major part of the common variances of all ten components (44.2 percent) and
the scree plot inspection revealed a distinct one-factor solution. The Kaiser-Meyer Olkin measure of
sampling adequacy was 0.867 for the household wealth index.
Methods
We used F-tests to examine the differences between LGAs in prevalence of the outcomes of
interest by measures of the quality of maternal health care. Multilevel logistic regression was used
to estimate the association of LGA-based quality of care measures with the outcomes of interest,
10
thereby accounting for the hierarchical clustered structure of the data, which if ignored, could
generate improper estimates of the standard errors. Multilevel models also incorporate random
effects at the LGA and individual levels in the regressions to account for unobserved individual and
LGA-level factors. Separate regression models were estimated for each outcome using the
generalized latent and mixed model command (GLLAMM) in Stata 11.0 (Rabe-Hesketh and Skrondal,
2008).
We estimated odds ratios (ORs) and 95percent confidence intervals (CIs) from regression
statistics. To test for multicollinearity, we calculated variance inflation factors (VIFs) for explanatory
variables included in each regression. The mean VIF was 1.92 and the highest was 2.73, signifying
that each independent variable was not highly correlated with the other independent variables in
the regressions. Intra-class correlation coefficients (ICC) were used to evaluate how the outcomes of
interest varied between LGAs and may be interpreted as the proportion of variation in a given
outcome that can be explained at the LGA level. If most of the variation in a given outcome is
explained by individual-level measures, the ICC would be close to 0. The intra-class correlation for
our two-level logistic random intercept models with an intercept variance of σ2µ, is calculated as:
ρ = (σ2µ / (σ2
µ + π2/3))
where π2/3 = 3.29 and represents the level-1 residual variance for a logit model
The analytical sample consisted of 1,394 last births that occurred to women in the five years
preceding the survey and that had no missing data on the variables of interest.
Results
Sample Characteristics
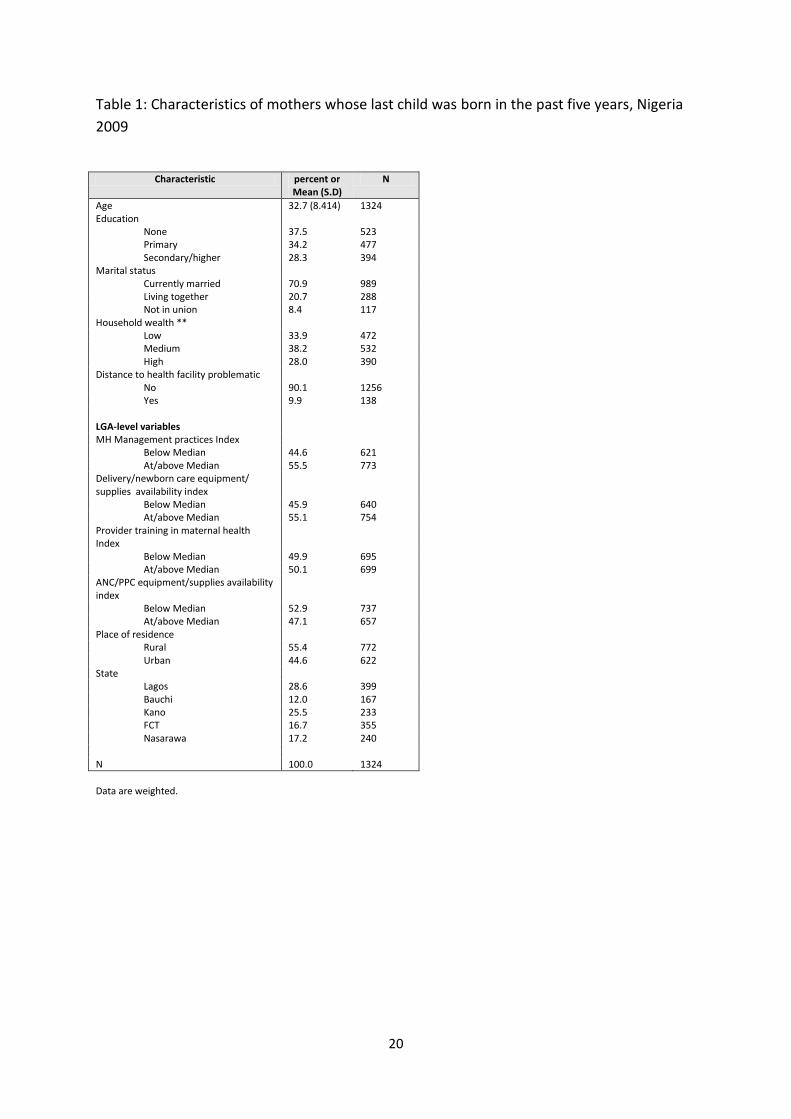
Table 1 presents the socio-demographic characteristics of mothers in the sample as well as
measures of maternal health service quality in their LGAs of residence. Mothers were 32.1 years old
on average and nearly a third had never been to school. The vast majority of mothers were
currently married at the time of the interview, with one out of five being in a cohabiting union. A
third of mothers lived in poor households and nearly ten percent perceived distance to the health
11
facility as a big problem in accessing care. Slightly more than half of mothers resided in LGAs that
were at/above the median in terms of the management practices that were supportive of quality
maternal health services and in terms of the availability of equipment and supplies for quality
delivery and newborn care.
Table 1 about here
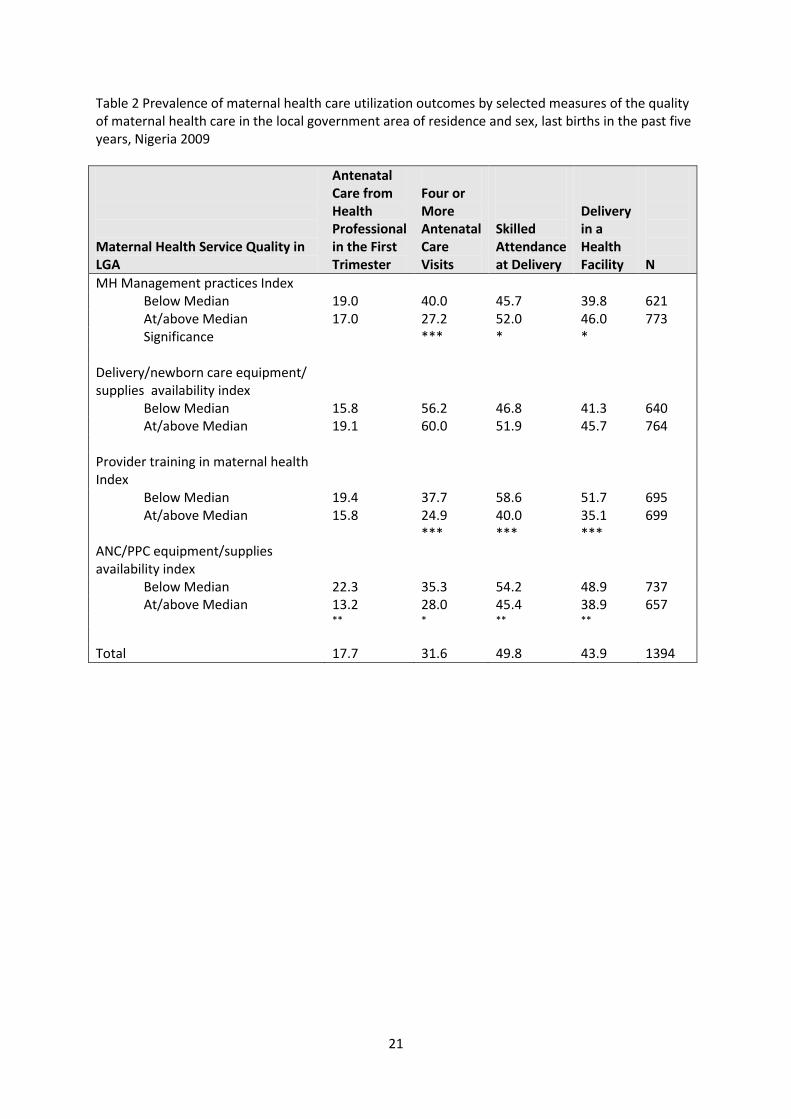
Bivariate Associations
Eighteen percent of women in the sample received antenatal care from a health professional
in the first trimester and 32 percent made four or more antenatal visits to a skilled provider. Half of
deliveries were assisted by skilled medical personnel (doctor, nurse or midwife) and 44 percent
occurred in a health facility (see Table 2). There was a positive association between residing in an
LGA with stronger maternal health care management practices and the delivery care utilization
rates. For example, the proportion of mothers whose most recent delivery in the past five years was
attended by skilled personnel was 46 percent in LGAs that were below the median on the index of
maternal health care management practices compared to 52 percent in LGAs that were at/above the
median. Maternal health care utilization rates did not vary according to the ranking of the LGA in
terms of the availability of delivery/newborn care equipment and supplies in its health facilities.
Table 2 about here
For the two other measures of maternal health care quality, differentials in maternal health
care utilization outcomes were contrary to expectations. A significantly higher proportion of women
made four or more antenatal care visits, were assisted by skilled personnel at delivery, and delivered
in a health facility in LGAs that were below (as opposed to at/above) the median index of provider
training in maternal health-relevant topics. A similar pattern is observed with regard to the
availability of ANC/PPC equipment and supplies in health facilities in the LGA. For example, the
institutional delivery rate was 49 percent in LGAs that were below the median in terms of the
availability of ANC/PPC equipment and supplies compared to 39 percent in LGAs that were at/above
the median on this measure. This pattern could reflect the fact that clients of maternal health
12
services may seek care in other LGAs if the availability of quality services in their LGAs of residence is
poor.
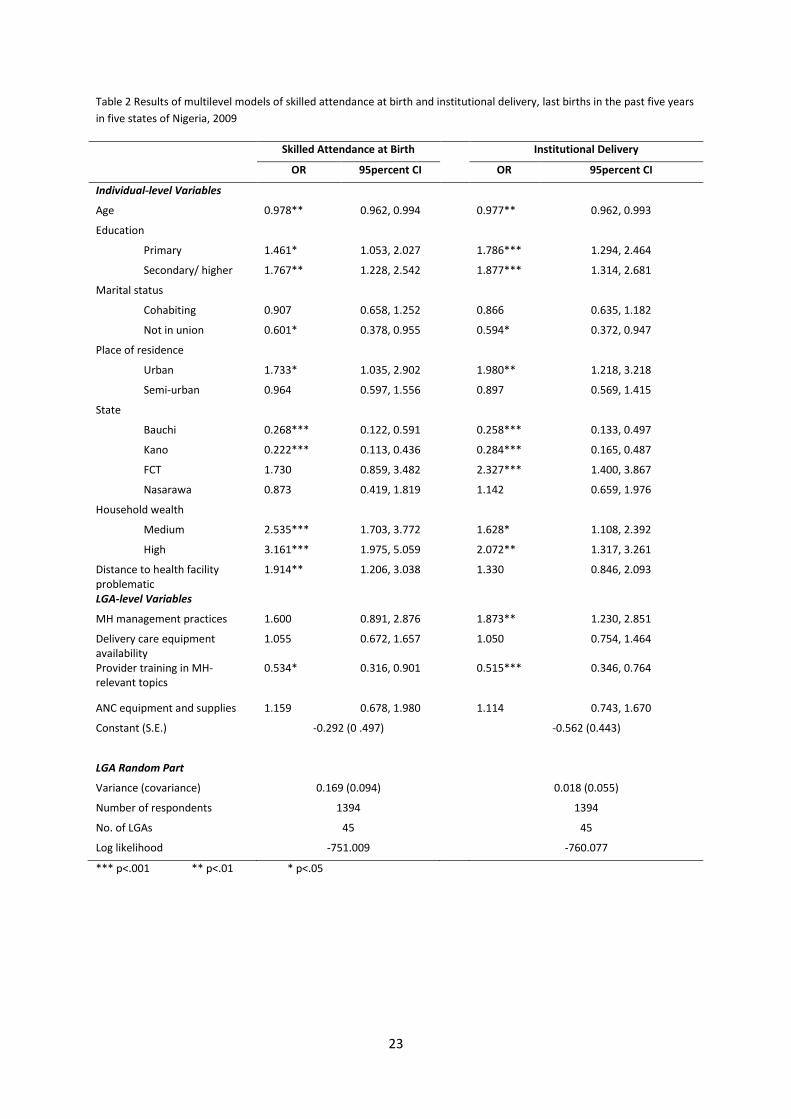
Multivariate Results
LGA level
Tables 3 and 4 show the multilevel regression results for the ANC and delivery care
outcomes, respectively. Greater availability of essential equipment and supplies for quality delivery
and newborn care services was associated with increased odds of initiating ANC with a health
professional in the first trimester of pregnancy (OR = 1.527; 95 percent CI = 1.031, 2.262). The odds
of institutional delivery were higher in LGAs with more supportive management practices for quality
delivery/newborn care services (OR = 1.873; 95 percent CI = 1.230, 2.851). Contrary to expectations,
the odds of skilled attendance at birth and institutional delivery were significantly lower in LGAs in
which providers had received lifetime training on a wider range of maternal health care topics than
in LGAs where providers had been trained on a narrower range of topics.
Table 3 about here
Individual Level
The individual-level results were worthy of note. The odds of initiating antenatal care in the
first trimester, making four or more antenatal care visits, being assisted at delivery by skilled
personnel and delivering in a health facility were significantly lower for respondents who were older.
Women with primary education and those with secondary/higher education had significantly higher
odds for all four outcomes than those who were uneducated. Place of residence was not
significantly associated with the antenatal care outcomes. However, as expected, urban women had
odds of skilled attendance at delivery and institutional delivery that were significantly higher than
those of rural women. Household wealth was not associated with the odds of initiating antenatal
care in the first trimester. The odds of four or more antenatal care visits, skilled attendance at
delivery, and institutional delivery were at least twice as high among mothers from households with
high as opposed to low levels of wealth.
13
Table 4 about here
Although state was not associated with the odds of making four or more antenatal care
visits, mothers from the states of Bauchi and Kano had significantly lower odds of receiving antenatal
care in the first trimester, skilled attendance at delivery and institutional delivery than those from
Lagos state. In addition, the odds of institutional delivery were 2.327 (95 percent CI = 1.400, 3.867)
times as high in FCT as in Lagos State. Women who reported that distance to the health facility was
a big problem had significantly higher odds of receiving antenatal care in the first trimester, making
four or more antenatal care visits and being attended at delivery by skilled personnel than those
who did not report distance to be a big problem in accessing health care.
The relative importance of individual-level and LGA-level variables in accounting for variation
in the maternal health care utilization outcomes of interest was estimated by calculating the ratio of
the LGA-level variance to the total variance (the intra-class correlation), a measure of the degree to
which the outcomes were clustered at the LGA-level. Using the estimates from the null model (with
just a multilevel constant term, the LGA-specific random effect and no explanatory variables), we
obtained an intra-LGA correlation of 0.209 for initiation of antenatal care in the first trimester of
pregnancy, 0.152 for four or more antenatal care visits, 0.365 for skilled attendance at birth, and
0.359 for institutional delivery. These estimates implied that even though more than half the
variation in maternal health care utilization outcomes is explained by individual-level characteristics,
more than a third of the explained variance in the delivery care utilization outcomes is attributable
to LGA-level measures of the quality of maternal health services.
Cross-level interactions
We also examined how aspects of the maternal health care service delivery environment interacted
with individual characteristics to result in use or non-use of maternal health services (results
available upon request). None of the interaction terms between the following LGA-based measures
of the quality of maternal health services and respondent’s education and age were statistically
significant: (a) maternal health care management practices; (b) provider training in maternal health

14
topics; and (c) availability of equipment and supplies for the delivery of quality antenatal care and
postpartum care services. The only significant interaction was found between the availability of
essential equipment and supplies for quality delivery and newborn care services (OR=0.967; 95
percent CI =0.938, 0.997; p = 0.033) and respondent’s age in the regressions for four or more
antenatal care visits (not shown). This interaction term suggested that increasing age was
associated with significantly lower odds of having four or more ANC visits in LGAs that ranked higher
than others in terms of the availability of equipment and supplies for delivery and newborn care.
Random Effects
To test the significance of the random intercept, the likelihood ratio test was applied by
calculating the difference in the observed deviances between the random intercept models
presented here and ordinary logistic regression models with the same explanatory variables. A
deviance difference of zero was obtained for timely initiation of ANC, 5.34 for four or more ANC
visits, 3.78 for skilled attendance at delivery, and 0.06 for institutional delivery. Halving the tail
probability associated with the chi-squared distribution with 1 degree of freedom (the difference in
parameters between the two types of models) yielded p<.05 for four or more ANC visits and skilled
attendance at birth. These results imply that the differences between LGAs were statistically
significant for these outcomes and that the odds of making four or more ANC visits and skilled
attendance at birth were determined by factors not captured by the observed covariates. Important
unmeasured factors could have included variations in cultural beliefs surrounding delivery, road
conditions, and factors underlying the placement of maternal health services.
Discussion
Previous studies on maternal health care utilization have given much emphasis on
household and individual determinants (i.e., the demand elements). Although many researchers
believe that the collection of household and individual information on service use should be
combined with information about the characteristics of health facilities that are available to the
population (i.e., the supply elements), few surveys permit service environment data to be linked to
15
population data. The current study is one of few to contribute to the knowledge of how aspects of
the structure of maternal health care services are associated with individual-level outcomes. The
study assessed the association between elements of maternal health service provision and key
population behaviors – timely initiation of antenatal care, four or more antenatal care visits, skilled
attendance at birth, and institutional delivery – by linking data from facility inventories and provider
interviews with household survey data.
The study found a strong positive association between the availability of essential delivery
care equipment and supplies in health facilities in the LGA of residence and women’s odds of
initiating prenatal care in the first trimester of pregnancy. The odds of institutional delivery were
significantly higher in LGAs that scored higher on management practices supportive of quality
maternal health services than in LGAs that scored lower, after controlling for other factors. Two
findings were contrary to expectations and call for further research. More comprehensive provider
training on maternal health in a LGA had a significant negative association with skilled attendance at
birth and institutional delivery. Furthermore, in LGAs that scored higher on the availability of
essential delivery and newborn care equipment and supplies, the odds of four or more ANC visits
were more negative as respondent’s age increased than in LGAS that scored lower on this indicator.
The study has raised important methodological issues as to how best to measure the quality
of maternal health services and how best to link population and facility data. In the survey,
household responses were used to generate a list of health facilities and a sample of facilities was
derived from this list. Although the survey identified the universe of facilities actually used by the
household, the administrative boundaries of the LGA of residence were artificially imposed on the
data for the purposes of identifying level 2 units for the multilevel regressions. The question arises
as to whether the sampled facilities that fell within a given LGA characterized well where residents
were obtaining maternal health care. There are two caveats. Even though the set of facilities
actually used by the population was identified, there were many individuals in the population who
did not use any facilities for maternal health. Thus, limiting the study to facilities used by the
16
population likely introduced biases. Second, imposing the artificial boundaries of the LGA on the
facility data mixes two concepts: “Where LGA residents could go” and “where LGA residents do go”
for health services. Alternative approaches that allow one to draw a catchment area around a
facility and draw a random sample of facilities within this radius may have been more appropriate,
and are quite feasible with GIS maps of enumeration areas and surrounding facilities. While GPS
codes were obtained for health facilities in the survey, they were not obtained for the households or
the enumeration area, an important omission.
An important question surrounds whose definition of quality matters for the use of maternal
health services in low-income settings: the individual, the community, or the profession? In a
landmark article by Haddad et al. (1998) on what quality means to lay people, the following
components pertaining to the structure of the facility were identified: availability of drugs;
availability of facility services; accessibility of the facility; presence of health worker; conditions of
buildings and rooms; availability of hospital beds; delivery of services not conditional upon prior
payments; cleanliness of rooms; availability of diagnostic equipment/devices; availability of running
water; free drugs and services; availability and state of washrooms; availability of roads, bridges,
and electricity; availability of in-patient food, quality of meals; availability of phone or shortwave
radio, and availability of integrated services. Future analysis will consider these issues explicitly and
assess their associations with maternal health care utilization. An additional consideration is that
the service supply environment (and lay people’s perceptions of quality) could differ by type of place
of residence and the condition of transportation networks. In areas with good transportation
networks, facilities located far away from a given household could still be accessible, making the
quality of care in the LGA of residence less salient for determining the maternal health outcomes of
interest.
Another issue in evaluating the quality of maternal health services in the present study had
to do with sample size – ensuring that there were enough facilities and service providers that were
interviewed in order to characterize the quality of maternal health service provision in areas that
17
were smaller than the LGA. That was a challenge. Other limitations of the data stemmed from their
cross-sectional nature, which made it difficult to establish causality. Endogeneity was also of
concern. If maternal health services were placed where the demand for them and fertility levels
were high, failure to consider this factor could lead to an overstatement of some of the results.
Temporal ordering was also of concern as it was not clear that measures of the service delivery
environment for maternal health preceded the utilization outcomes of interest. Structural and
process aspects of quality may have changed over the 2-5 year period preceding the survey, making
earlier facility surveys conducted in 2005 and 2007 potentially more relevant than the 2009 facility
survey data analyzed in the present study. It is also to be noted that the health facility and
household surveys were conducted in the 51 LGAs that were targeted at the start of the COMPASS
project and the results of the analysis are not representative of Bauchi, FCT, Lagos, Kano and
Nasarawa states. No provider-client observations were conducted during the health facility survey,
which prevented an assessment of the association between process components of the quality of
maternal health care and utilization outcomes.
Program and Policy Implications
The findings call for interventions that target specific elements of maternal health service
delivery. Efforts to increase the utilization of maternal health care services should improve health
facility management practices, ensure the availability of essential equipment and supplies, and
conduct further research to better understand the linkages between provider training and the
utilization of maternal health services. As this study focused on the structural aspects of the quality
of maternal health services, research is needed to elucidate the linkages between the social-
psychological aspects of care and the utilization of maternal health services.
18
References
Adanu R. M. K. Utilization of Obstetric Services in Ghana between 1999 and 2003. African Journal of Reproductive Health. 2010; 14(3):153. Althabe, F., Bergal, E., Cafferta, M., et al. (2008). Strategies for improving the quality of health care in maternal and child health in low- and middle-income countries: an overview of systematic reviews. Paediatric and Perinatal Epidemiology, 22 (S1), 42–60. Conrad, P., De Allegri, M., Moses, A., Larsson, E. C., Neuhann, F., Müller, O., & Sarker, M. (2012). Antenatal Care Services in Rural Uganda: Missed Opportunities for Good-Quality Care. Qualitative Health Research, 22, 619-629. Donabedian, A. (1988). The quality of care. How can it be assessed? Journal of the American Medical Association,260, 1743-8. Fauveau, V., & de Bernis, L., 2006. Good obstetrics revisited: too many evidence based practices and devices are not used. International Journal of Gynaecology and Obstetrics, 94, 179–184. Galadanci, H. S., C. L. Ejembi, et al. (2007). Maternal health in Northern Nigeria: a far cry from ideal. British Journal of Obstetrics and Gynaecology, 114, 448-452. Haddad, S., Fournier, P., Machouf, N., & Yatara, F. (1998). What does quality mean to lay people? Community perceptions of primary health care services in Guinea. Social Science & Medicine, 47, 381-94. Hulton, Louisa, A., Matthews, Zoe and Stones, R.W. (2005) A framework for assessing quality of
maternal health services and preliminary findings form its application in Urban India. Southampton,
UK: Southampton Statistical Sciences Research Institute. (S3RI Applications and Policy Working
Papers, (A05/03).
Ijadunola, K. T., Ijadunola, M. Y., Esimai, O. A, & Abiona, T. C. (2010). New paradigm old thinking: The case for emergency obstetric care in the prevention of maternal mortality in Nigeria. BMC Women’s Health, 10, 6. Kongnyuy, E. J., Hofman, J., Mlava, G., Mhango, C., & Van der Broek, N. (2009). Availability, utilization and quality of basic and comprehensive emergency obstetric care services in Malawi. Maternal Child Health Journal, 13, 687-694. National Population Commission (NPC) [Nigeria] and ICF Macro. (2009). Nigeria Demographic and Health Survey 2008. Abuja, Nigeria: National Population Commission and ICF Macro. Osungbade, K., Oginni, S., & Olumide, A. (2008). Content of antenatal care services in secondary health care facilities in Nigeria: Implication for quality of maternal health care. International Journal for Quality in Health Care, 20, 346-351. Raven, J. H., Tolhurst, R. J., Tang, S., van den Broek, N. (2012). What is quality in maternal and neonatal health care? , 28, e676-83.
19
Rockers, P. C., Wilson, M. L., Mbaruku, G., Kruk, M. E. (2009). Source of antenatal care influences facility delivery in rural Tanzania: A population-based study. Maternal Child Health Journal, 13, 879-888. Sarker, M., Schmid, G., Larrson, E., Kirenga, S., De Allegri, M., Neuhann, F., Mbnda, T., Lekule, I., & Muller, O. (2010). Quality of antenatal care in rural southern Tanzania: A reality check. BMC Research Notes, 3, 209. Sharan, M., Ahmed, S., Ghebrehiwet, M., & Rogo, K. (2011). The quality of the maternal health
system in Eritrea. International Journal of Gynaecology and Obstetrics, 115, 244-250.
National Population Commission (NPC) [Nigeria] and ICF Macro (2009). Nigeria Demographic and
Health Survey 2008. Abuja, Nigeria: National Population Commission and ICF Macro.
World Health Organization (2010). Working with Individuals, Families and Communities to Improve
Maternal and Newborn Health. Geneva, Switzerland: WHO.
World Health Organization (2012). Trends in Maternal Mortality: 1990-2010. Geneva, Switzerland:
WHO.
20
Table 1: Characteristics of mothers whose last child was born in the past five years, Nigeria
2009
Characteristic percent or
Mean (S.D) N
Age 32.7 (8.414) 1324 Education
None 37.5 523 Primary 34.2 477 Secondary/higher 28.3 394
Marital status Currently married 70.9 989 Living together 20.7 288 Not in union 8.4 117
Household wealth ** Low 33.9 472 Medium 38.2 532 High 28.0 390
Distance to health facility problematic No 90.1 1256 Yes 9.9 138
LGA-level variables MH Management practices Index
Below Median 44.6 621 At/above Median 55.5 773
Delivery/newborn care equipment/ supplies availability index
Below Median 45.9 640 At/above Median 55.1 754
Provider training in maternal health Index
Below Median 49.9 695 At/above Median 50.1 699
ANC/PPC equipment/supplies availability index
Below Median 52.9 737 At/above Median 47.1 657
Place of residence Rural 55.4 772 Urban 44.6 622
State Lagos 28.6 399 Bauchi 12.0 167 Kano 25.5 233 FCT 16.7 355 Nasarawa 17.2 240
N 100.0 1324
Data are weighted.
21
Table 2 Prevalence of maternal health care utilization outcomes by selected measures of the quality of maternal health care in the local government area of residence and sex, last births in the past five years, Nigeria 2009
Maternal Health Service Quality in LGA
Antenatal Care from Health Professional in the First Trimester
Four or More Antenatal Care Visits
Skilled Attendance at Delivery
Delivery in a Health Facility
N
MH Management practices Index Below Median 19.0 40.0 45.7 39.8 621 At/above Median 17.0 27.2 52.0 46.0 773 Significance *** * *
Delivery/newborn care equipment/ supplies availability index
Below Median 15.8 56.2 46.8 41.3 640 At/above Median 19.1 60.0 51.9 45.7 764
Provider training in maternal health Index
Below Median 19.4 37.7 58.6 51.7 695 At/above Median 15.8 24.9 40.0 35.1 699
*** *** *** ANC/PPC equipment/supplies availability index
Below Median 22.3 35.3 54.2 48.9 737 At/above Median 13.2 28.0 45.4 38.9 657
** * ** **
Total 17.7 31.6 49.8 43.9 1394

22
Table 3 Results of multilevel logit models of initiation of antenatal care in the first trimester and four or more antenatal visits, last births in the past five years in five states of Nigeria, 2009
Received Antenatal Care in First Trimester
Four or More Antenatal Care Visits
OR 95percent CI OR 95percent CI
Individual-level variables
Age 0.975* (0.956, 0.994) 0.976** (0.961, 0.992)
Education
Primary 2.034*** (1.346, 3.072) 1.843*** (1.325, 2.563)
Secondary/ higher 2.024** (1.292, 3.169) 2.007*** (1.389, 2.901)
Marital status
Cohabiting 0.855 (0.600, 1.217) 0.884 (0.647, 1.208)
Not in union 0.470* (0.247, 0.896) 0.851 (0.537, 1.349)
Place of residence
Urban 0.961 (0.539, 1.714) 1.027 (0.618, 1.710)
Semi-urban 0.693 (0.401, 1.196) 0.666 (0.412, 1.076)
State
Bauchi 0.231*** (0.101, 0.530) 0.917 (0.425, 1.977)
Kano 0.237*** (0.124, 0.454) 0.605 (0.308, 1.192)
FCT 1.256 (0.727, 2.169) 1.475 (0.735, 2.957)
Nasarawa 1.565 (0.838, 2.921) 1.824 (0.868, 3.833)
Household wealth
Medium 1.277 (0.801, 2.035) 1.526* (1.025, 2.272)
High 1.633 (0.949, 2.810) 2.361*** (1.481, 3.765)
Distance to health facility problematic
2.633*** (1.637, 4.233) 1.997*** (1.305, 3.054)
LGA-level Variables
MH management practices 0.894 (0.545, 1.468) 0.596 (0.329, 1.079)
Delivery care equipment availability
1.527* (1.031, 2.262) 1.155 (0.728, 1.832)
Provider training in MH-relevant topics
0.908 (0.590, 1.395) 0.708 (0.414, 1.208)
ANC equipment and supplies 0.749 (0.482, 1.164) 1.384 (0.805, 2.382)
Constant (S.E.) -1.138 (0.519) * -0.668 (0.479)
LGA Random Part
Variance (covariance) 1.038e-21 (1.061e-11) 0.185 (0.092)
Number of respondents 1394 1394
No. of LGAs 45 45
Log likelihood -582.246 -798.047
*** p<.001 ** p<.01 * p<.05
23
Table 2 Results of multilevel models of skilled attendance at birth and institutional delivery, last births in the past five years
in five states of Nigeria, 2009
Skilled Attendance at Birth Institutional Delivery
OR 95percent CI OR 95percent CI
Individual-level Variables
Age 0.978** 0.962, 0.994 0.977** 0.962, 0.993
Education
Primary 1.461* 1.053, 2.027 1.786*** 1.294, 2.464
Secondary/ higher 1.767** 1.228, 2.542 1.877*** 1.314, 2.681
Marital status
Cohabiting 0.907 0.658, 1.252 0.866 0.635, 1.182
Not in union 0.601* 0.378, 0.955 0.594* 0.372, 0.947
Place of residence
Urban 1.733* 1.035, 2.902 1.980** 1.218, 3.218
Semi-urban 0.964 0.597, 1.556 0.897 0.569, 1.415
State
Bauchi 0.268*** 0.122, 0.591 0.258*** 0.133, 0.497
Kano 0.222*** 0.113, 0.436 0.284*** 0.165, 0.487
FCT 1.730 0.859, 3.482 2.327*** 1.400, 3.867
Nasarawa 0.873 0.419, 1.819 1.142 0.659, 1.976
Household wealth
Medium 2.535*** 1.703, 3.772 1.628* 1.108, 2.392
High 3.161*** 1.975, 5.059 2.072** 1.317, 3.261
Distance to health facility problematic
1.914** 1.206, 3.038 1.330 0.846, 2.093
LGA-level Variables
MH management practices 1.600 0.891, 2.876 1.873** 1.230, 2.851
Delivery care equipment availability
1.055 0.672, 1.657 1.050 0.754, 1.464
Provider training in MH-relevant topics
0.534* 0.316, 0.901 0.515*** 0.346, 0.764
ANC equipment and supplies 1.159 0.678, 1.980 1.114 0.743, 1.670
Constant (S.E.) -0.292 (0 .497) -0.562 (0.443)
LGA Random Part
Variance (covariance) 0.169 (0.094) 0.018 (0.055)
Number of respondents 1394 1394
No. of LGAs 45 45
Log likelihood -751.009 -760.077
*** p<.001 ** p<.01 * p<.05





























