Embed Size (px)
Citation preview

The 4th
generation IGRA
L. Masae Kawamura, M.D.Senior Director, Medical and Scientific Affairs, TB Diagnostics, QIAGEN
August 2017
QuantiFERON-TB Gold Plus
Sample to Insight
Disclaimers - QuantiFERON-TB Gold Plus (QFT Plus)
2
QFT-Plus is CE-IVD marked and FDA approved.
It will be available in the US this fall.
QFT-Plus is an in vitro diagnostic aid for detection of Mycobacterium
tuberculosis infection (including disease) and is intended for use in
conjunction with risk assessment, radiography, and other medical and
diagnostic evaluations. QFT-Plus results alone cannot distinguish active TB
disease from latent infection. QFT-Plus Package Inserts, available in multiple
languages, as well as up-to-date licensing information and product-specific
disclaimers can be found at www.QuantiFERON.com.

Sample to Insight
3
Tuberculin skin test (TST) QuantiFERON-TB (QFT)
Can be fully automated
Highly specific, not affected by BCG
Results with one patient visit
No inter-reader variability
Electronic results (straight to EMR)
Quality-assured laboratory test
Manual placement, reading and data entry
Two patient visits required, high no-show rate
Significant inter-reader variability
Poor surveillance tool
Often no quality control after initial training
In-vivo test---causes boosting
TST is not patient or program-centered and least effective in most vulnerable:
“hard to reach” groups
Sample to Insight
Evolution of QFT Technology
4
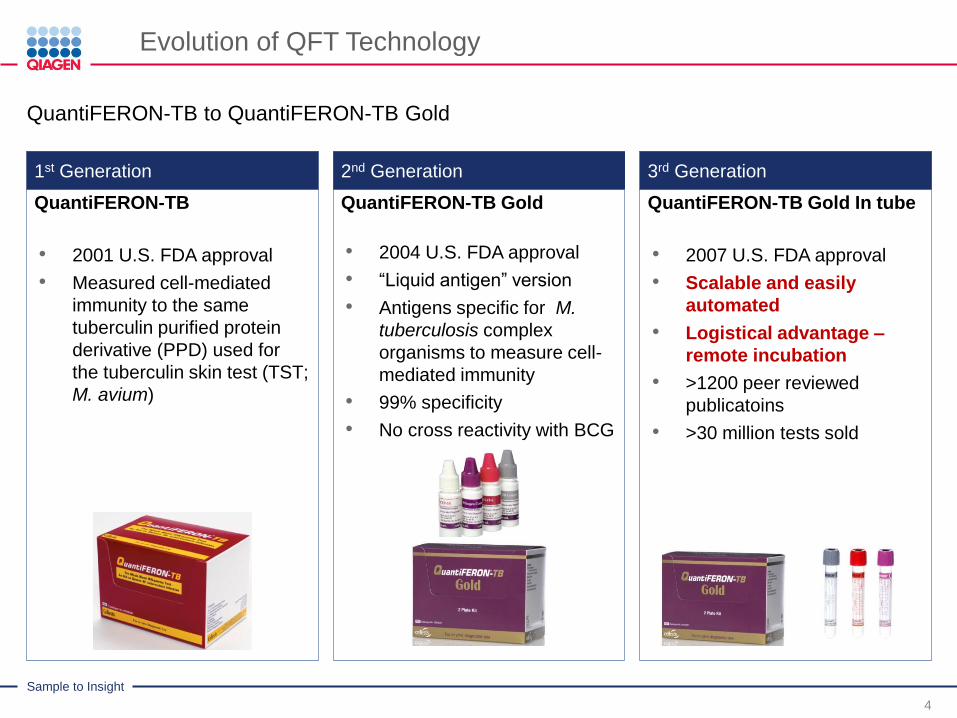
QuantiFERON-TB to QuantiFERON-TB Gold
1st Generation 2nd Generation 3rd Generation
QuantiFERON-TB Gold In tube
• 2007 U.S. FDA approval
• Scalable and easily
automated
• Logistical advantage –
remote incubation
• >1200 peer reviewed
publicatoins
• >30 million tests sold
QuantiFERON-TB Gold
• 2004 U.S. FDA approval
• “Liquid antigen” version
• Antigens specific for M.
tuberculosis complex
organisms to measure cell-
mediated immunity
• 99% specificity
• No cross reactivity with BCG
QuantiFERON-TB
• 2001 U.S. FDA approval
• Measured cell-mediated
immunity to the same
tuberculin purified protein
derivative (PPD) used for
the tuberculin skin test (TST;
M. avium)
5
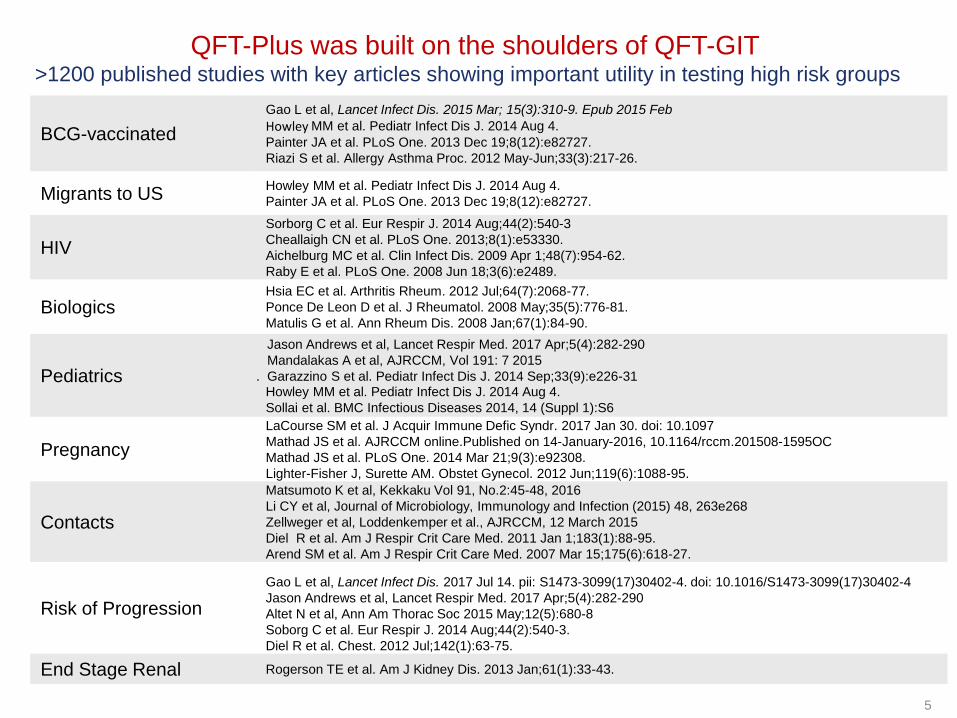
QFT-Plus was built on the shoulders of QFT-GIT
BCG-vaccinated
Gao L et al, Lancet Infect Dis. 2015 Mar; 15(3):310-9. Epub 2015 Feb
Howley MM et al. Pediatr Infect Dis J. 2014 Aug 4.
Painter JA et al. PLoS One. 2013 Dec 19;8(12):e82727.
Riazi S et al. Allergy Asthma Proc. 2012 May-Jun;33(3):217-26.
Migrants to USHowley MM et al. Pediatr Infect Dis J. 2014 Aug 4.
Painter JA et al. PLoS One. 2013 Dec 19;8(12):e82727.
HIV
Sorborg C et al. Eur Respir J. 2014 Aug;44(2):540-3
Cheallaigh CN et al. PLoS One. 2013;8(1):e53330.
Aichelburg MC et al. Clin Infect Dis. 2009 Apr 1;48(7):954-62.
Raby E et al. PLoS One. 2008 Jun 18;3(6):e2489.
BiologicsHsia EC et al. Arthritis Rheum. 2012 Jul;64(7):2068-77.
Ponce De Leon D et al. J Rheumatol. 2008 May;35(5):776-81.
Matulis G et al. Ann Rheum Dis. 2008 Jan;67(1):84-90.
Pediatrics
Jason Andrews et al, Lancet Respir Med. 2017 Apr;5(4):282-290
Mandalakas A et al, AJRCCM, Vol 191: 7 2015
. Garazzino S et al. Pediatr Infect Dis J. 2014 Sep;33(9):e226-31Howley MM et al. Pediatr Infect Dis J. 2014 Aug 4.
Sollai et al. BMC Infectious Diseases 2014, 14 (Suppl 1):S6
Pregnancy
LaCourse SM et al. J Acquir Immune Defic Syndr. 2017 Jan 30. doi: 10.1097
Mathad JS et al. AJRCCM online.Published on 14-January-2016, 10.1164/rccm.201508-1595OC
Mathad JS et al. PLoS One. 2014 Mar 21;9(3):e92308.
Lighter-Fisher J, Surette AM. Obstet Gynecol. 2012 Jun;119(6):1088-95.
Contacts
Matsumoto K et al, Kekkaku Vol 91, No.2:45-48, 2016
Li CY et al, Journal of Microbiology, Immunology and Infection (2015) 48, 263e268
Zellweger et al, Loddenkemper et al., AJRCCM, 12 March 2015
Diel R et al. Am J Respir Crit Care Med. 2011 Jan 1;183(1):88-95.
Arend SM et al. Am J Respir Crit Care Med. 2007 Mar 15;175(6):618-27.
Risk of Progression
Gao L et al, Lancet Infect Dis. 2017 Jul 14. pii: S1473-3099(17)30402-4. doi: 10.1016/S1473-3099(17)30402-4
Jason Andrews et al, Lancet Respir Med. 2017 Apr;5(4):282-290
Altet N et al, Ann Am Thorac Soc 2015 May;12(5):680-8
Soborg C et al. Eur Respir J. 2014 Aug;44(2):540-3.
Diel R et al. Chest. 2012 Jul;142(1):63-75.
End Stage Renal Rogerson TE et al. Am J Kidney Dis. 2013 Jan;61(1):33-43.
>1200 published studies with key articles showing important utility in testing high risk groups

Sample to Insight
6
Sample to Insight
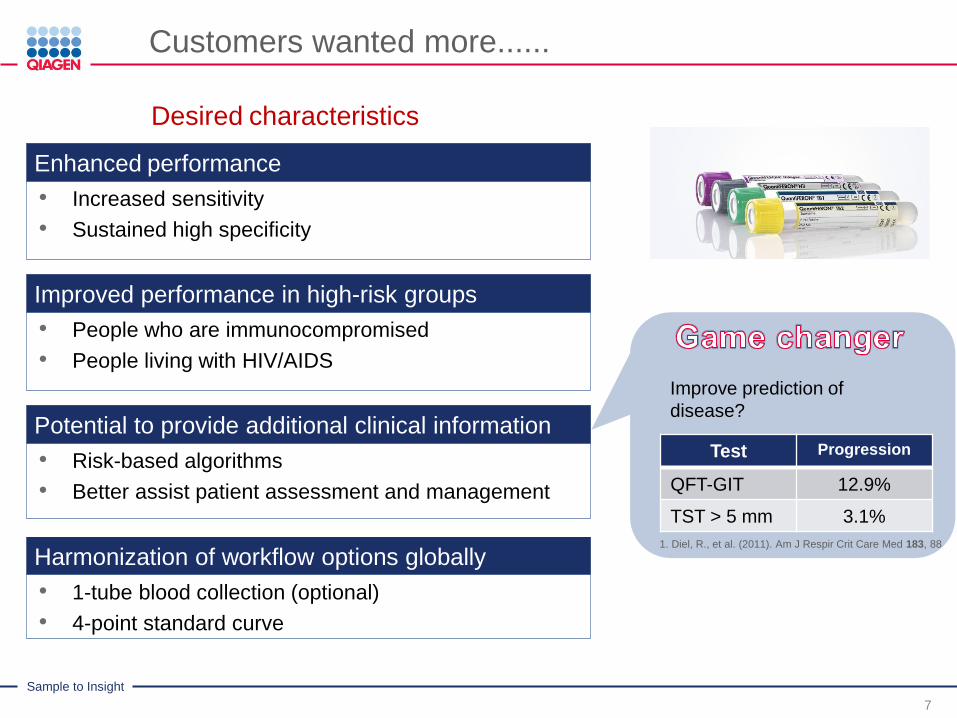
Customers wanted more......
7
Desired characteristics
Enhanced performance
Improved performance in high-risk groups
Potential to provide additional clinical information
Harmonization of workflow options globally
• Increased sensitivity
• Sustained high specificity
• People who are immunocompromised
• People living with HIV/AIDS
• Risk-based algorithms
• Better assist patient assessment and management
• 1-tube blood collection (optional)
• 4-point standard curve
Test Progression
QFT-GIT 12.9%
TST > 5 mm 3.1%
Improve prediction of
disease?
1. Diel, R., et al. (2011). Am J Respir Crit Care Med 183, 88

Sample to Insight
8

Sample to Insight
New CD8+ antigens: WHY?
9
CD8+ T cells and role in TB immunity:
MTB-specific CD8+ T cells secrete IFN- and other soluble factors to (1–3):
• Suppress MTB growth
• Kill infected cells
• Directly lyse intracellular MTB
BIOMARKER for intracellular burden
TB-specific CD8+ T cells that produce IFN- have been:
• More frequently detected in those with active TB disease vs. latent infection (4, 5)
• Associated with recent exposure to TB (6)
• Detectable in active TB subjects with HIV co-infection and young children (7, 8)
• Observed to decline when patients are exposed to anti-tuberculosis treatment (9)
References: 1. Turner, J. et al. (1996) Immunology 87, 339. 2. Brookes, R.H. et al. (2003) Eur. J. Immunol. 33, 3293. 3. Stenger, S. et al. (1998)
Science 282, 121. 4. Day, C.L. et al. (2011) J. Immunol. 187, 2222. 5. Rozot, V. et al. (2013) Eur. J. Immunol. 43, 1568. 6. Nikolova, M. et al. (2013)
Diagn. Microbiol. Infect. Dis. 75, 277. 7. Chiacchio, T. et al. (2014) J. Infect. http://dx.doi.org/10.1016/j.jinf.2014.06.009. 8. Lanicioni, C. et al. (2012)
Am. J. Respir. Crit. Care Med. 185, 206. 9. Nyendak M. Et al. (2014) PLoS ONE 8, e81564. Epub.
Sample to Insight
QFT-Plus Product Format
10
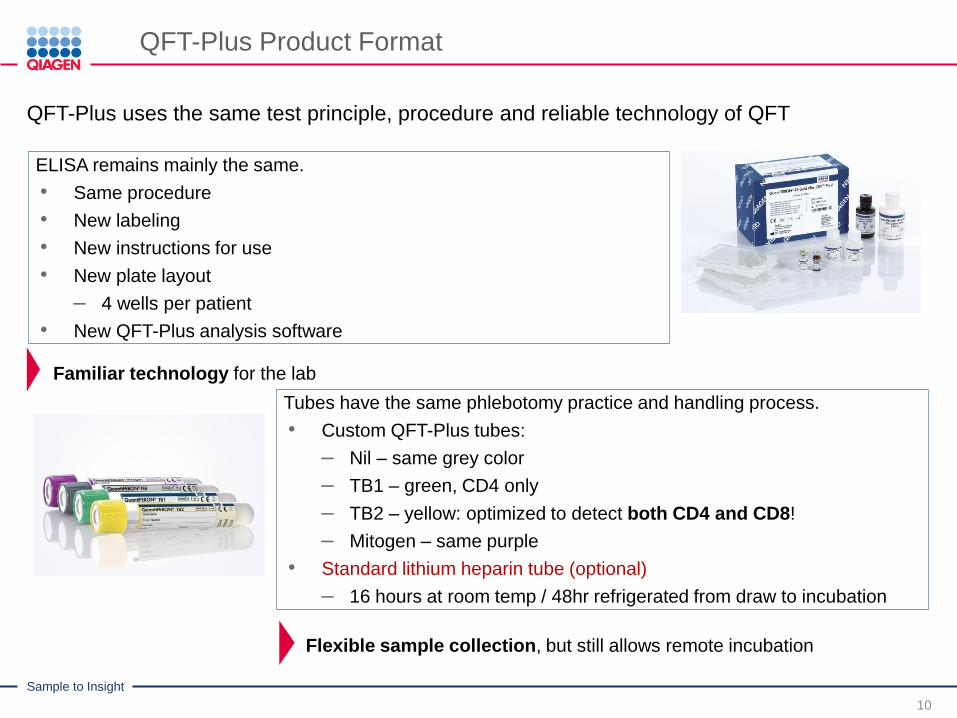
QFT-Plus uses the same test principle, procedure and reliable technology of QFT
ELISA remains mainly the same.
• Same procedure
• New labeling
• New instructions for use
• New plate layout
– 4 wells per patient
• New QFT-Plus analysis software
Tubes have the same phlebotomy practice and handling process.
• Custom QFT-Plus tubes:
– Nil – same grey color
– TB1 – green, CD4 only
– TB2 – yellow: optimized to detect both CD4 and CD8!
– Mitogen – same purple
• Standard lithium heparin tube (optional)
– 16 hours at room temp / 48hr refrigerated from draw to incubation
Flexible sample collection, but still allows remote incubation
Familiar technology for the lab
Sample to Insight
11
Sample to Insight
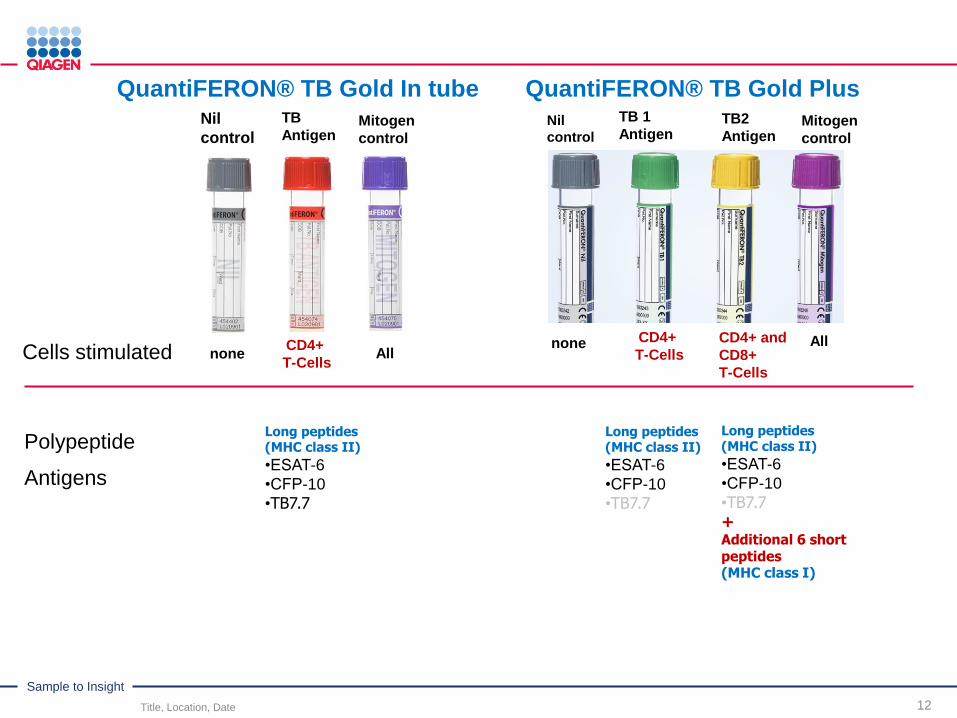
QuantiFERON® TB Gold In tube QuantiFERON® TB Gold Plus
Title, Location, Date 12
Cells stimulated
Nil
controlMitogen
control
Nil
controlMitogen
control
noneCD4+ and
CD8+
T-Cells
CD4+
T-Cells
TB
Antigen
TB 1
AntigenTB2
Antigen
CD4+
T-Cells
none AllAll
Long peptides (MHC class II)
•ESAT-6
•CFP-10
•TB7.7+Additional 6 short peptides(MHC class I)
Long peptides (MHC class II)
•ESAT-6
•CFP-10
•TB7.7
Long peptides (MHC class II)
•ESAT-6
•CFP-10
•TB7.7
Polypeptide
Antigens
Sample to Insight
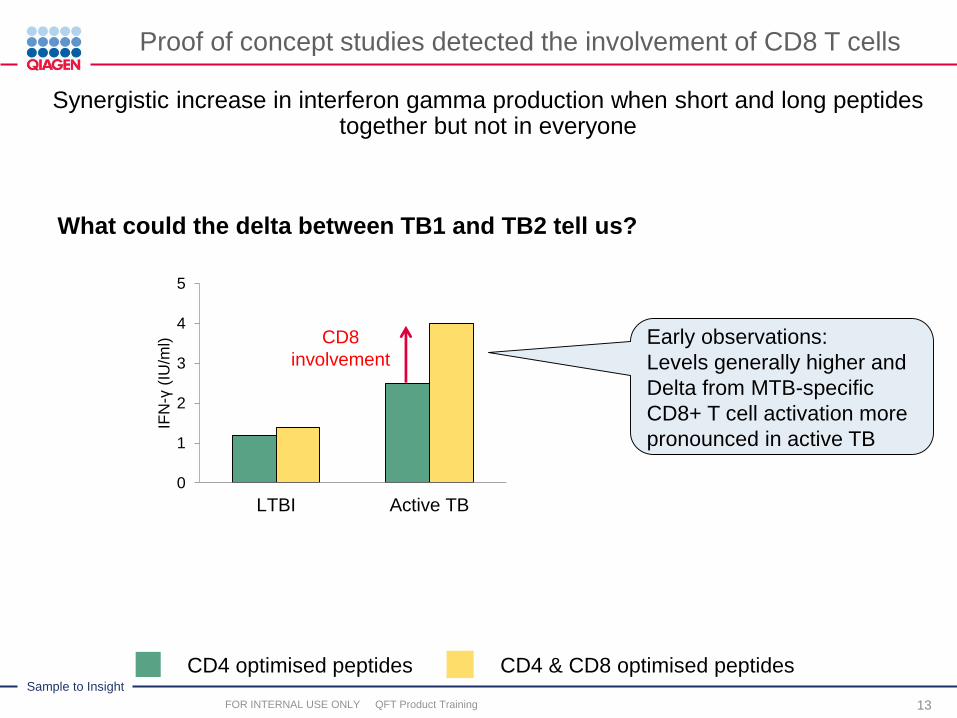
Proof of concept studies detected the involvement of CD8 T cells
13
Synergistic increase in interferon gamma production when short and long peptides together but not in everyone
What could the delta between TB1 and TB2 tell us?
0
1
2
3
4
5
LTBI Active TB
IFN
-γ(I
U/m
l) CD8
involvementEarly observations:
Levels generally higher and
Delta from MTB-specific
CD8+ T cell activation more
pronounced in active TB
CD4 optimised peptides CD4 & CD8 optimised peptides
FOR INTERNAL USE ONLY QFT Product Training

Sample to Insight
14
Sample to Insight
Sensitivity of QFT-Plus- FDA approved US Package Insert
15
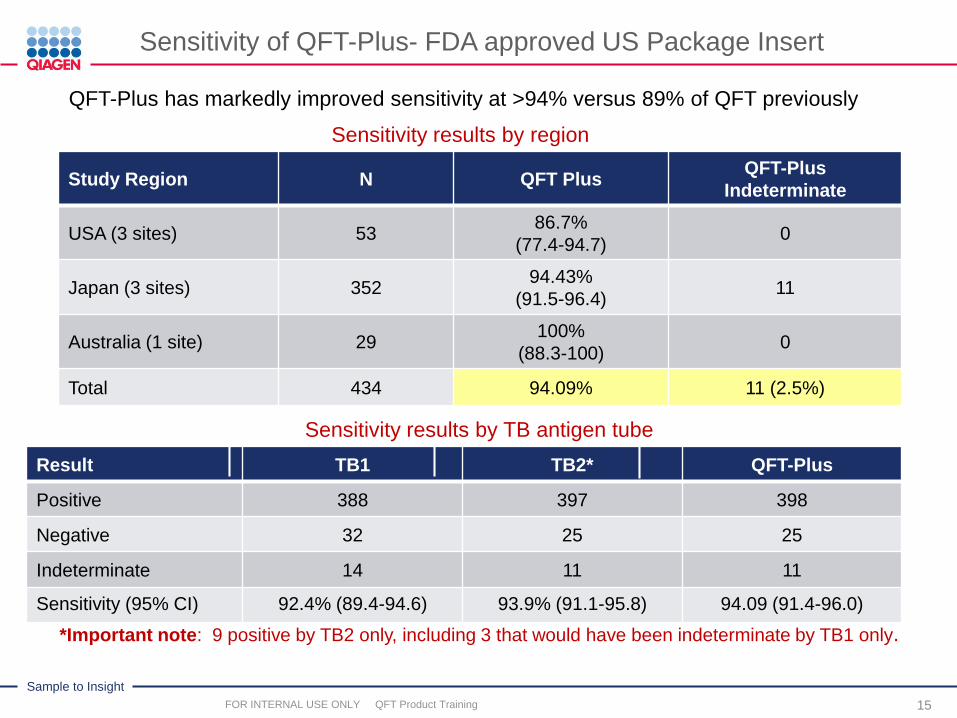
QFT-Plus has markedly improved sensitivity at >94% versus 89% of QFT previously
Sensitivity results by region
Sensitivity results by TB antigen tube
*Important note: 9 positive by TB2 only, including 3 that would have been indeterminate by TB1 only.
Study Region N QFT PlusQFT-Plus
Indeterminate
USA (3 sites) 5386.7%
(77.4-94.7)0
Japan (3 sites) 35294.43%
(91.5-96.4)11
Australia (1 site) 29100%
(88.3-100)0
Total 434 94.09% 11 (2.5%)
Result TB1 TB2* QFT-Plus
Positive 388 397 398
Negative 32 25 25
Indeterminate 14 11 11
Sensitivity (95% CI) 92.4% (89.4-94.6) 93.9% (91.1-95.8) 94.09 (91.4-96.0)
FOR INTERNAL USE ONLY QFT Product Training

Sample to Insight
Sensitivity of QFT-Plus – Independent data
16
Sensitivity (culture confirmed TB) results from Independent QFT-Plus studies
.
Publication Indeterminate Sensitivity
BARCELLINI et al, ERJ 2016 2.6% (3/116) 87.93% (102/116)
Includes 4/4 HIV infected
HOFFMAN et al, CMI 2016 0 95.8% (23/24)
YI et al, Scientific Reports 3.1% (5/162) 91% (147/162)
1. QuantiFERON-TB Gold Plus (QFT-Plus) ELISA Package Insert. Rev. 02. February 2015.1083163.
Sample to Insight
QFT-Plus: Clinical performance – Specificity Studies
17
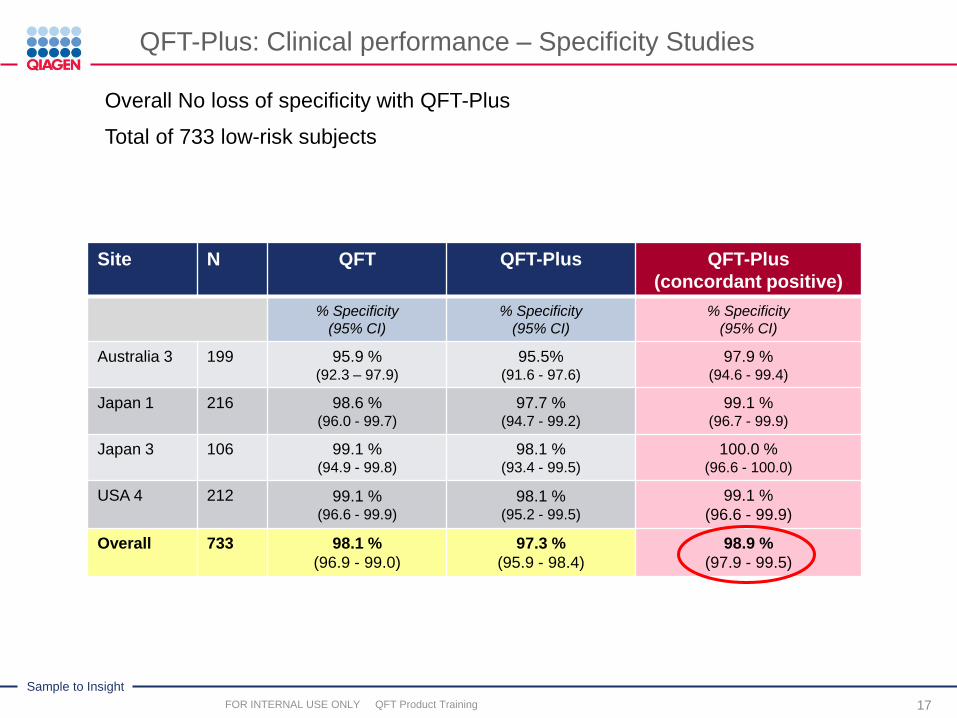
Overall No loss of specificity with QFT-Plus
Total of 733 low-risk subjects
Site N QFT QFT-Plus QFT-Plus
(concordant positive)
% Specificity
(95% CI)
% Specificity
(95% CI)
% Specificity
(95% CI)
Australia 3 199 95.9 %(92.3 – 97.9)
95.5%(91.6 - 97.6)
97.9 %(94.6 - 99.4)
Japan 1 216 98.6 %(96.0 - 99.7)
97.7 %(94.7 - 99.2)
99.1 %(96.7 - 99.9)
Japan 3 106 99.1 %(94.9 - 99.8)
98.1 %(93.4 - 99.5)
100.0 %(96.6 - 100.0)
USA 4 212 99.1 %(96.6 - 99.9)
98.1 %(95.2 - 99.5)
99.1 %
(96.6 - 99.9)
Overall 733 98.1 %
(96.9 - 99.0)
97.3 %
(95.9 - 98.4)
98.9 %
(97.9 - 99.5)
FOR INTERNAL USE ONLY QFT Product Training
Sample to Insight
Additional analysis of TB Antigen Tube values – Package Insert data
18
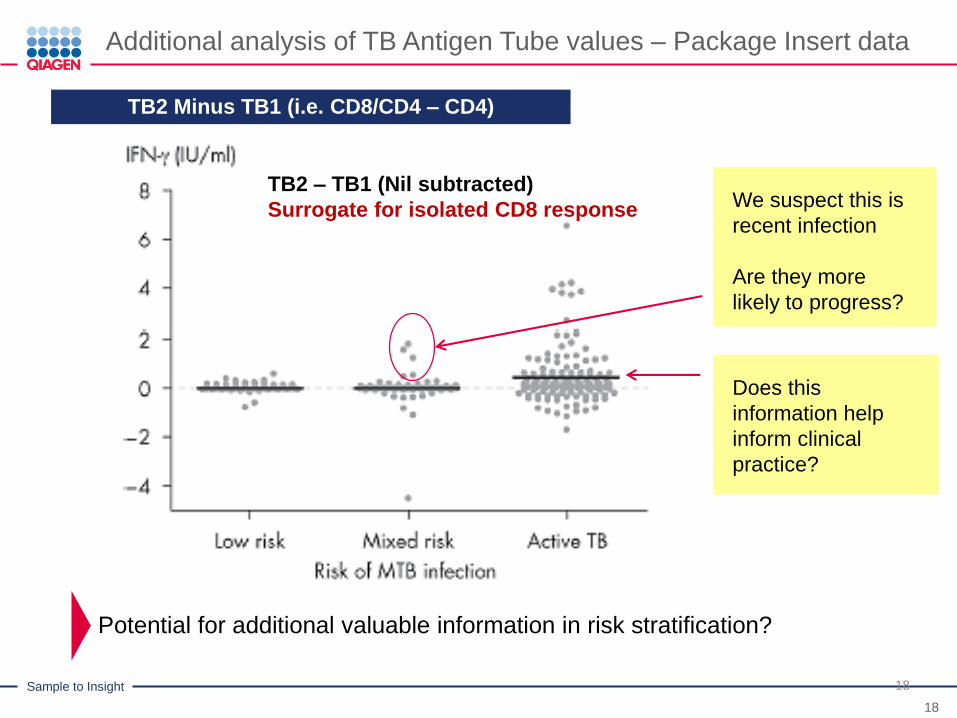
TB2 Minus TB1 (i.e. CD8/CD4 – CD4)
18
TB2 – TB1 (Nil subtracted)
Surrogate for isolated CD8 response
Potential for additional valuable information in risk stratification?
Does this
information help
inform clinical
practice?
We suspect this is
recent infection
Are they more
likely to progress?
Sample to Insight
19

Sample to Insight
QFT PLUS Publications
20
Title/Authors
First independent evaluation of QuantiFERON-TB Plus performance
BARCELLINI et al
Published – ERJ 2016
Equal sensitivity of the new generation QuantiFERON-TB Gold plus in direct comparison with the previous
test version QuantiFERON-TB Gold IT.
HOFFMANN et al.
Published – CMI 2016
First evaluation of QuantiFERON-TB Gold Plus performance in contact screening
BARCELLINI et al
Published – ERJ 2016
Preliminary data on precision of QuantiFERON-TB Plus (QFT-Plus) performance.
GALLAGHER et al
Published- ERJ 2016
CD8 response is associated to active TB and to the response to TB2 in the QuantiFERON-TB Plus kit.
PETRUCCIOLI et al
Published– J of Infection 2016
Evaluation of QuantiFERON-TB Gold Plus for Detection of Mycobacterium tuberculosis
infection in Japan
YI et al
Published-Scientific Reports
2016
QuantiFERON-TB® Gold Plus as a potential tuberculosis treatment monitoring tool
KAMADA et al
Published –ERJ 2017
The sensitivity of the QuantiFERON®-TB Gold Plus assay in Zambian adults with active tuberculosis
TELISINGHE et al
Published–IJTLD 2017
QFT-Plus: a plus in variability? – Evaluation of new generation IGRA in serial testing of students with a
migration background in Germany
KNIERER et al
Published – J of Occ Med and
Tox
Evaluation of QuantiFERON®-TB Gold-Plus in Healthcare Workers in a Low-Incidence Setting.
MOON et alJCM 2017
Prevalence of latent tuberculosis infection among foreign students in Lübeck, Germany tested with
QuantiFERON-TB Gold In-Tube and QuantiFERON-TB Gold Plus
MORALES et al
Journal of Occ Med and
Toxicology 2017
Sample to Insight
QFT PLUS 2016-2017 Key Publications
21
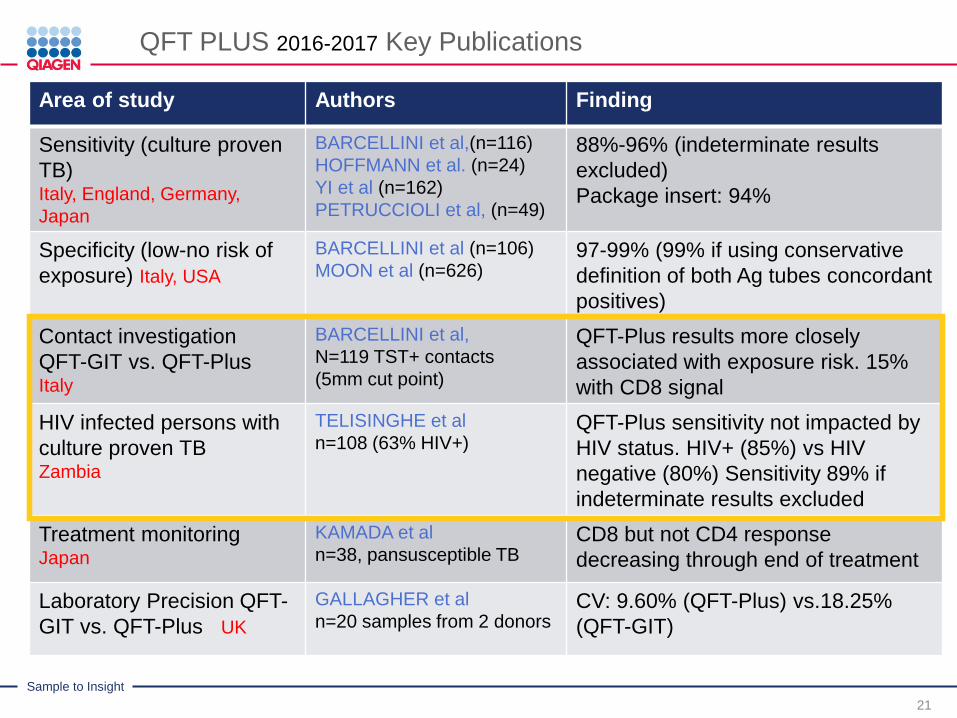
Area of study Authors Finding
Sensitivity (culture proven
TB)Italy, England, Germany,
Japan
BARCELLINI et al,(n=116)
HOFFMANN et al. (n=24)
YI et al (n=162)
PETRUCCIOLI et al, (n=49)
88%-96% (indeterminate results
excluded)
Package insert: 94%
Specificity (low-no risk of
exposure) Italy, USA
BARCELLINI et al (n=106)
MOON et al (n=626)97-99% (99% if using conservative
definition of both Ag tubes concordant
positives)
Contact investigation
QFT-GIT vs. QFT-PlusItaly
BARCELLINI et al,
N=119 TST+ contacts
(5mm cut point)
QFT-Plus results more closely
associated with exposure risk. 15%
with CD8 signal
HIV infected persons with
culture proven TBZambia
TELISINGHE et al
n=108 (63% HIV+)QFT-Plus sensitivity not impacted by
HIV status. HIV+ (85%) vs HIV
negative (80%) Sensitivity 89% if
indeterminate results excluded
Treatment monitoringJapan
KAMADA et al
n=38, pansusceptible TBCD8 but not CD4 response
decreasing through end of treatment
Laboratory Precision QFT-
GIT vs. QFT-Plus UK
GALLAGHER et al
n=20 samples from 2 donorsCV: 9.60% (QFT-Plus) vs.18.25%
(QFT-GIT)

Sample to Insight
First evaluation of QuantiFERON-TB Gold Plus performance in contact screening
Study design: Prospective recruitment of TST-positive adult contacts (TST ≥5 mm)
• Average age of 39 (30-79)
• 26%(n=61) non-European born, 78.85% (n=82) BCG vaccinated
• 9.24% (n=11) were immunocompromised (HIV and other)
• Contact screening based on NICE TB guidelines 2011 and Italian guidelines
Results
RESULTS
Barcellini et al, Eur Respir J. 2016 Jul 7. pii: ERJ-00510-2016. doi:
10.1183/13993003.00510-2016. Epub ahead of print]

Sample to Insight
Barcellini et al, 2016: Results continued…
23
Strong overall agreement: ĸ = 0.8
◦ Discordant results N=12
All 12 results were negative QFT and positive QFT-Plus
All but one discordant result had positive TST result >10 mm
Two conversions occurred with QFT upon retesting at 10–12 weeks.
Both initially positive by QFT-Plus
QFT-Plus with stronger risk association
• QFT-Plus showed a stronger risk association to aggregate exposure time than QFT:
Odds ratio 6 QFT vs. 14 QFT-Plus
• QFT-Plus showed a stronger risk association to index case proximity than QFT:
Odds ratio 4 QFT vs. 6 QFT-Plus
“…our data show that QFT-Plus in contact screening has improved
performance compared to QFT-GIT...”
Barcellini et al, Eur Respir J. 2016 Jul 7. pii: ERJ-00510-2016. doi:
10.1183/13993003.00510-2016. Epub ahead of print]
Sample to Insight
TB2:TB1 differential as a surrogate measure for CD8 stimulation
24
15% of QFT+ contacts had TB2-TB1 values >0.6 IU/mL
• Significantly associated with proximity to the index case
◦ p = 0.0029
• Significantly associated with European origin
◦ p = 0.043
“[QFT-Plus performance] suggests a role for the differential value
between the two tubes as a proxy for recent infection.”
Barcellini et al, Eur Respir J. 2016 Jul 7. pii: ERJ-00510-2016. doi:
10.1183/13993003.00510-2016. Epub ahead of print]
Barcellini et al, 2016: Results continued…

Sample to Insight
1st evaluation of QFT-Plus performance in PLHIV (high-burden setting)
Study design: Prospective recruitment of Zambian patients with pulmonaryTB• Mean age of 32, 73% male; 63% HIV infected, BMI <18.5 (>50%)
• 108 consecutive smear or Xpert +
Results
RESULTS
Telisinghe et al, INT J TUBERC LUNG DIS 21(6):690–696
Sample to Insight
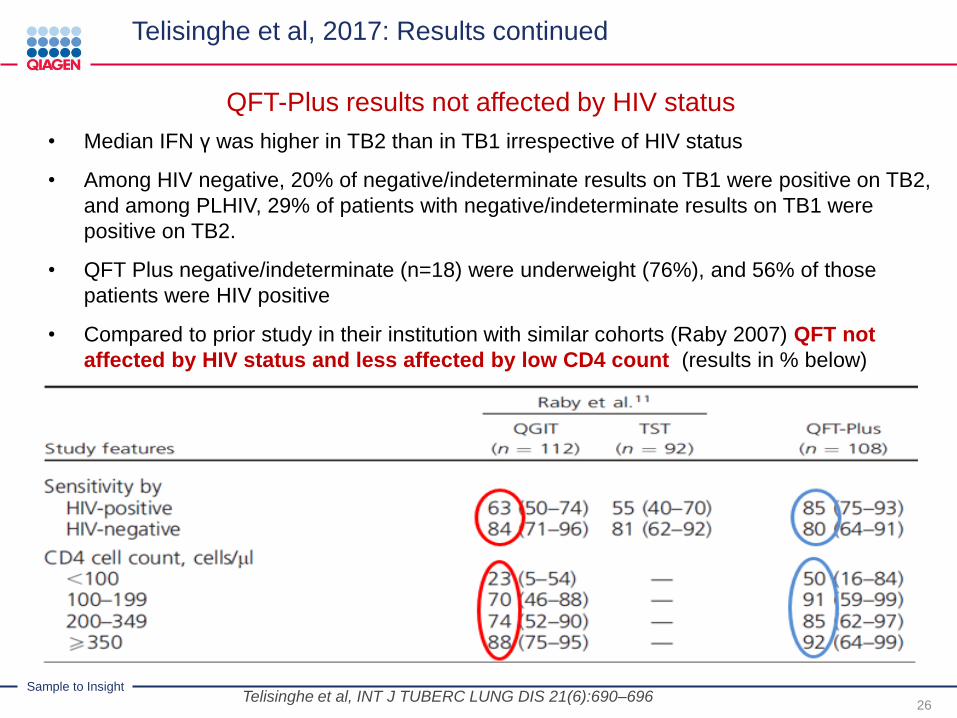
QFT-Plus results not affected by HIV status
26
• Median IFN γ was higher in TB2 than in TB1 irrespective of HIV status
• Among HIV negative, 20% of negative/indeterminate results on TB1 were positive on TB2,
and among PLHIV, 29% of patients with negative/indeterminate results on TB1 were
positive on TB2.
• QFT Plus negative/indeterminate (n=18) were underweight (76%), and 56% of those
patients were HIV positive
• Compared to prior study in their institution with similar cohorts (Raby 2007) QFT not
affected by HIV status and less affected by low CD4 count (results in % below)
Telisinghe et al, INT J TUBERC LUNG DIS 21(6):690–696
Telisinghe et al, 2017: Results continued
Sample to Insight
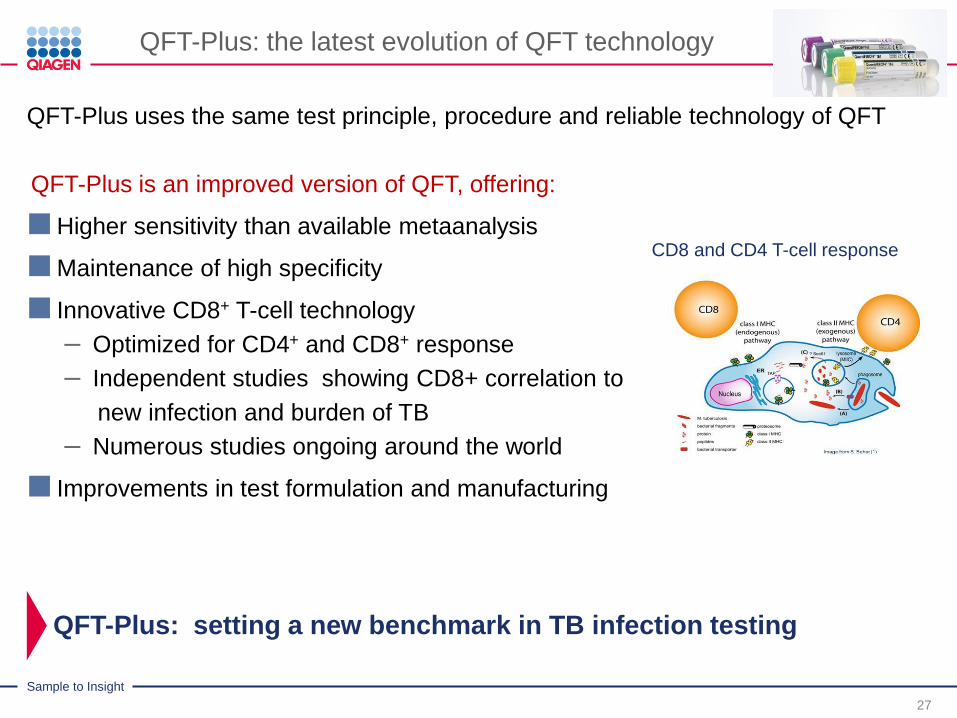
QFT-Plus: the latest evolution of QFT technology
27
QFT-Plus uses the same test principle, procedure and reliable technology of QFT
QFT-Plus is an improved version of QFT, offering:
Higher sensitivity than available metaanalysis
Maintenance of high specificity
Innovative CD8+ T-cell technology
– Optimized for CD4+ and CD8+ response
– Independent studies showing CD8+ correlation to
new infection and burden of TB
– Numerous studies ongoing around the world
Improvements in test formulation and manufacturing
QFT-Plus: setting a new benchmark in TB infection testing
CD8 and CD4 T-cell response


























![LIAISON QuantiFERON-TB Gold Plus ( [REF] 311010) 1](https://img.pdfslide.net/doc/110x75/61b26a9e529835162559e41c/liaison-quantiferon-tb-gold-plus-ref-311010-1-.jpg)

