Embed Size (px)
Citation preview

�������� ����� ��
Quantitative in vivo longitudinal nerve excursion and strain in responsoe tojoint movement: a systematic literature review
Ana Silva, Andre Manso, Ricardo Andrade, Vanessa Domingues, MariaPiedade Brandao, Anabela G. Silva
PII: S0268-0033(14)00192-2DOI: doi: 10.1016/j.clinbiomech.2014.07.006Reference: JCLB 3825
To appear in: Clinical Biomechanics
Received date: 15 April 2014Revised date: 30 July 2014Accepted date: 30 July 2014
Please cite this article as: Silva, Ana, Manso, Andre, Andrade, Ricardo, Domingues,Vanessa, Brandao, Maria Piedade, Silva, Anabela G., Quantitative in vivo longitudinalnerve excursion and strain in responsoe to joint movement: a systematic literature review,Clinical Biomechanics (2014), doi: 10.1016/j.clinbiomech.2014.07.006
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
1
Quantitative in vivo longitudinal nerve excursion and strain in response to joint
movement: a systematic literature review
Ana Silvaa, BSc, André Mansoa, BSc, Ricardo Andradea MSc, Vanessa Dominguesa,
BSc, Maria Piedade Brandãoa, b, PhD, Anabela G. Silvaa, b, PhD
Affiliations
a School of Health Sciences, University of Aveiro, Portugal
Address: Escola Superior de Saúde da Universidade de Aveiro, Campus Universitário
de Santiago, 3810-193 Aveiro - Portugal
bCenter for Health Technology and Services Research (CINTESIS), Piso 2, edifício
nascente, Rua Dr. Plácido da Costa, s/n, 4200-450 Porto, Portugal
Corresponding author Anabela G. Silva (PhD) –
School of Health Sciences, University of Aveiro, Portugal
Address: Escola Superior de Saúde da Universidade de Aveiro, Campus Universitário
de Santiago, 3810-193 Aveiro - Portugal
Telephone: +351 234247119, extension: 27120 Fax: +351 234 401597
e-mail: [email protected]
Abstract word count – 245
Manuscript word count - 4594
Number of figures – 4
Number of tables - 2
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
2
Abstract
Background – Neural system mobilization is widely used in the treatment of several
painful conditions. Data on nerve biomechanics is crucial to inform the design of
mobilization exercises. Therefore, the aim of this review is to characterise normal
nervous system biomechanics in terms of excursion and strain.
Methods - Studies were sought from Pubmed, Physiotherapy Evidence Database,
Cochrane Library, Web of Science and Scielo. Two reviewers’ screened titles and
abstracts, assessed full reports for potentially eligible studies, extracted information on
studies’ characteristics and assessed its methodological quality.
Findings – Twelve studies were included in this review that assessed the median nerve
(n=8), the ulnar nerve (n=1), the tibial nerve (n=1), the sciatic nerve (n=1) and both the
tibial and the sciatic nerves (n=1). All included studies assessed longitudinal nerve
excursion and one assessed nerve strain. Absolute values varied between 0.1 mm and
12.5 mm for median nerve excursion, between 0.1 mm and 4.0 mm for ulnar nerve
excursion, between 0.7 mm and 5.2 mm for tibial nerve excursion and between 0.1 mm
and 3.5 mm for sciatic nerve excursion. Maximum reported median nerve strain was
2.0%.
Interpretation - Range of motion for the moving joint, distance from the moving joint to
the site of the lesion, position of adjacent joints, number of moving joints and whether
joint movement stretches or shortens the nerve bed need to be considered when
designing neural mobilization exercises as all of these factors seem to have an impact
on nerve excursion.
Key words: Biomechanics, Neural mobilization, Excursion, Strain
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
3
1. Introduction
Body movements and postures induce tensile, shear, and compressive stresses to the
nervous system. The normal nervous system is able to adapt to these stresses through
a variety of mechanisms, such as gliding (excursion) relative to adjacent structures,
stretching (increasing strain) and its capacity to tolerate compression from adjacent
structures, while maintaining its main function, the transmission of neural impulses
[1,2]. If something interferes with the normal biomechanical responses of the nervous
system to body movements and postures, imposed stresses may reach levels that
compromise the nervous system functioning, for example, reducing axonal transport
and intraneural blood supply [3,4].
Changes in the normal biomechanics of the nervous system have been associated with
painful disorders such as carpal tunnel syndrome, thoracic outlet syndrome, cubital
tunnel syndrome or diabetes [5–8]. This has contributed to a greater popularity of
nervous system mobilization as part of a conservative treatment approach aiming at
restoring the normal biomechanics of the nervous system [9–11]. In fact, it has been
shown that mobilizing the nerve in relation to the surrounding structures contributes to
reverse behavioral and cellular changes associated with neuropathic pain in rats [12]
and favours intraneural fluid dispersion in cadavers [13]. Furthermore, nervous system
mobilization has been shown to result in immediate C-fiber mediated hypoalgesia and
increased range of motion [14]. However, the mechanisms behind nervous system
mobilization are not completely clear [13]. There are several theories, including
physiological effects, such as reduction of edema, central effects, such as the reduction
of the central sensitization as well as mechanical effects such as the excursion of the
nervous system [15].
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
4
Individual studies investigating the effect of neural mobilization are either unclear or
very different in terms of the specific procedures of neural mobilization used [16,17].
However, previous studies have suggested that the joints mobilized, the sequence of
joint movement or the position of adjacent joints influence the quantity of nervous
system strain and gliding and the direction of gliding [5,15,18–20]. Therefore,
effectiveness of nervous system mobilization might depend on these factors. An
important step to help define protocols for clinical trials and inform the interpretation of
results is to clarify how different patterns of movement impact the normal biomechanics
of the nervous system. This will help define the most appropriate pattern of movement
to attain a specific treatment aim and inform studies aiming to assess the efficacy of
different patterns of nervous system mobilization.
Thus the aims of this systematic review are i) to determine quantity and direction of
normal nervous system longitudinal excursion and tension in response to joint
movement and ii) to identify which factors are likely to impact nerve longitudinal
excursion and tension.
2. Methods
2.1. Data sources and searches
Studies were sought using Pubmed, Physiotherapy Evidence Database (PEDro),
Cochrane Library, Web of Science and Scielo. The search was conducted on May
2010 and updated on February 2013 and included references published since 1975.
Combinations of the following key words were used for all databases with the exception
of Scielo database: neural mobilization, mobilization, nerve mobilization, neural
manipulative physical therapy, nerve glide, nerve biomechanics, nerve gliding
exercises, nerve mobilization exercises, neural treatment, neural stretching,
neurodynamics, neural physiotherapy, upper limb neurodynamic test, straight leg
raising, slump, prone knee bend. Equivalent key words in Portuguese were used for
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
5
Scielo database. The reference list of retrieved articles was also screened for reports
not identified through electronic searches.
To be included in this review studies must have:
Been published as a full article or an abstract with sufficient detail to extract the
main attributes of the study;
Been written either in English or in Portuguese;
Assessed either longitudinal excursion or tension (or both) of any component of
the peripheral nervous system in response to any movement of one or several
segments of the body;
Been conducted in human participants (in vivo) without known nervous system
pathology;
Reported the position of at least one joint adjacent to the one being mobilized.
Studies were excluded if:
Participants had been submitted to a surgery or any other invasive event likely
to affect nerve biomechanics.
2.2. Assessment of methodological quality of studies
Two authors (AGS and MPB) independently evaluated the quality of the studies using a
modified version of the quality assessment tool by Downs and Black [21], previously
used in a study aiming to synthesise the biomechanical characteristics of peripheral
diabetic neuropathy [22]. Individual items were scored either 1, if appropriately
addressed in the study, or 0, if not addressed in the study or if assessors were unable
to determine it. The total quality scores were reported as an average score between
the two assessors for a maximum score of 17 (Table 1). The scoring system for the tool
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
6
was that described by Fernando et al. [22]: a score of 7 or less was considered low
quality, 8–11 as fair quality and greater than 11 as good quality.
2.3. Data extraction, synthesis and analysis
Titles and abstracts were screened by at least two of the first four authors (AS, AM, RA
and VD). Potentially eligible studies were identified and their respective full reports
obtained. Full reports were also assessed separately by at least two of the first four
authors (AS, AM, RA and VD) against the eligibility criteria. Discrepancies in judgement
were discussed with a third reviewer (AGS) who acted as arbiter.
The reviewers independently extracted the following information from each included
study: i) sample characteristics (number of participants, age and sex); ii) involved joint
and movement performed; iii) position of participant and position of joints adjacent to
the moving joint; iv) site where measurements of excursion and/or strain were taken
and v) mean values for excursion and/or strain in millimetres and percentage of change
from baseline, respectively. Data were described using counts, minimum and maximum
values and presented using tables and graphs. Graphs were used only for data on the
median nerve due to the limited number of data on the other nerves. Additionally, the
95% confidence interval (CI) of the minimal detectable change (MDC) was calculated
for individual measurements of nerve gliding. This calculation was only performed for
studies reporting the standard error of measurement (SEM). The equation used was
MDC95%= SEM * √2 * 1.96 [23].
3. Results
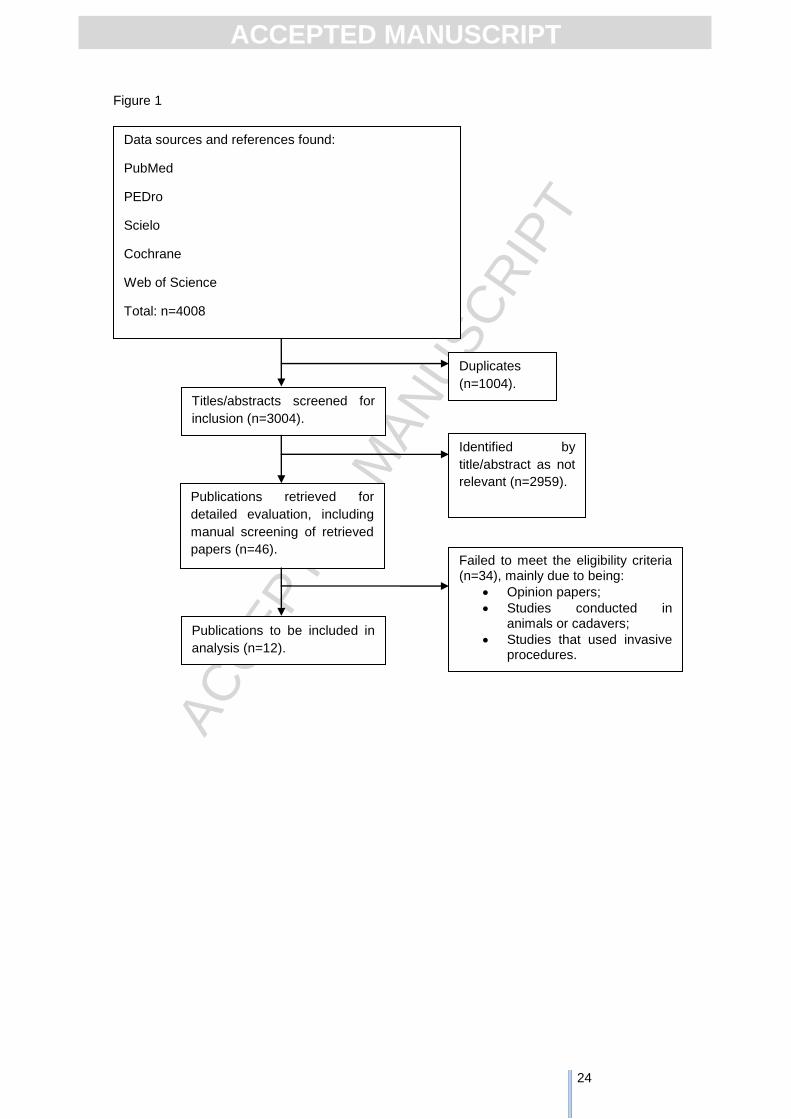
The search strategy retrieved 4008 references. After excluding for duplicates (n=1004),
a total of 3004 references were screened by title and/or abstract for relevance. Of
these, 2958 were excluded for not meeting the inclusion criteria and 46 full reports
were retrieved for further analysis. No study was excluded based on language of
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
7
publication. The reference lists of the 46 full reports were also screened for potential
eligible studies. A total of 12 studies were included in this systematic review (Figure 1).
3.1. Included studies
Of the 12 studies included in this review, eight reported on the median nerve
[11,19,24–29], one on the ulnar nerve [30], one on the tibial nerve [5], one on the
sciatic nerve [15] and one on both the tibial and the sciatic nerves [31]. All included
studies used ultrasound to acquire nerve images and 10 out of the 12 included studies
reported to use the cross correlation analysis as described by Dilley et al [32] to
analyse these images and quantify nerve movement [5,11,15,19,26–31]. Of the 10
studies that used this method of image analysis, 5 reported on its reliability and found
an intra-class correlation coefficient (ICC) of 0.75 or greater [5,11,15,19,26–31]. Hough
et al [24] used the Scion Image program (www.scioncorp.com) for quantification of nerve
gliding and reported an ICC of 0.92. Hough et al. [25] used the Java-based image
processing program (ImageJ) and reported an ICC of 0.89. These ICC values indicate
that measurement procedures had excellent reliability [33].
3.2. Study quality
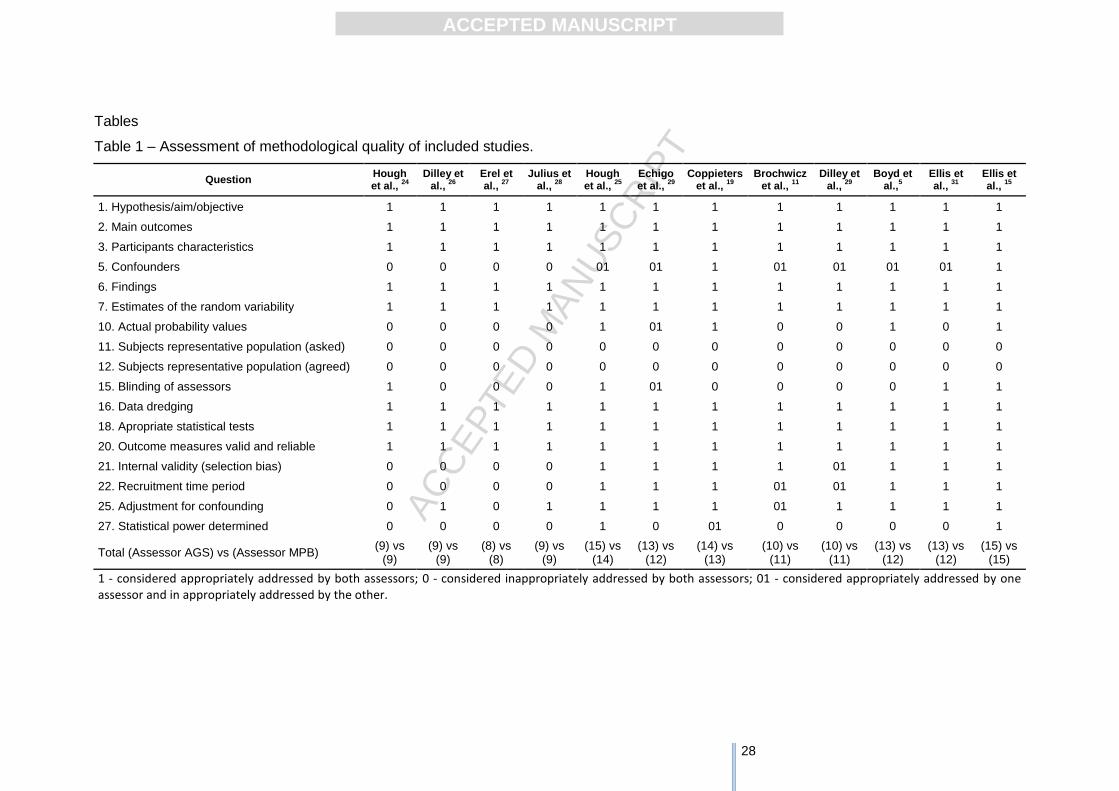
There were minor differences in ratings between assessors for included studies
(maximum difference in the final score between assessors is 1) as illustrated in Table
1. No study scored 7 or less. Six studies were of fair quality (scored 8 to 11) and
another six were of good quality (>11). Included studies failed mostly in terms of
reporting of actual p values, sample representativeness, blinding of the assessors and
a priori sample size calculation.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
8
3.3. MDC 95% for individual measurements of nerve gliding
MDC 95% was calculated for individual measurements of nerve gliding for nine out of
the 12 included studies (Table 2). MDC 95% values varied between 0.03 mm and 2.2
mm across measurements and studies. Overall, the MDC 95% for individual
measurements of nerve gliding was less than or equal to nerve gliding mean values.
For example, in the study of Brochwicz et al. [11] mean nerve gliding varied between
1.9 mm and 3.3 mm and the MDC 95% associated with these measurements varied
between 0.3 mm and 0.8 mm. These results suggest that nerve gliding measurements
were above the measurement error associated with it. In addition, we used the MDC
95% associated with nerve gliding measurements to inform the comparison between
different combinations of joint movement and positioning described in section 3.4. We
considered that differences between nerve gliding measurements induced by different
combinations of joint movement and positioning were attributed to random error if <
MDC 95% [34].
3.4. Median nerve longitudinal gliding
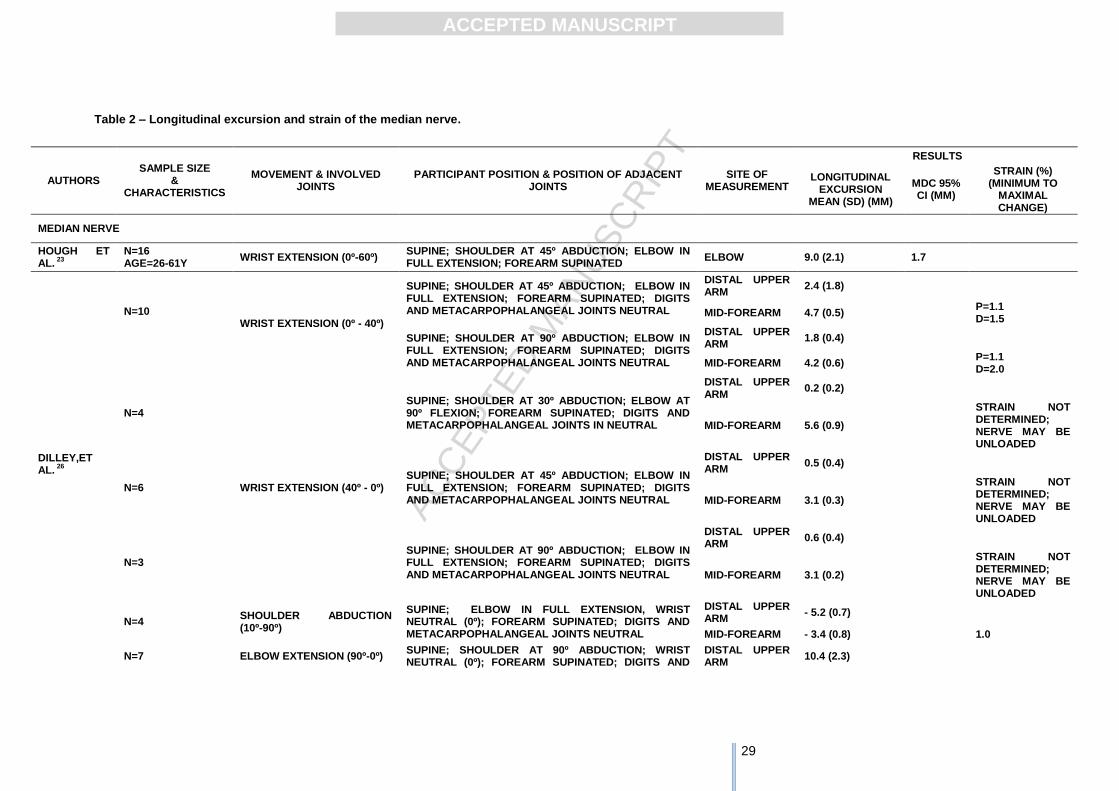
The eight studies assessing the median nerve reported on longitudinal excursion in
response to joint movement [11,19,24–29]. Additionally, Dilley et al. [26] also reported
on nerve strain. All studies assessed nerve excursion and/or strain in response to the
movement of a single body segment while adjacent joints were stationary. Additionally,
one study also reported on nerve excursion in response to simultaneous movement of
two body segments [19]. Detailed characterization of each study and results are
presented in Table 2.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
9
3.4.1. Impact of finger movement on median nerve gliding
One study assessed the effect of finger flexion on median nerve gliding at the forearm
and reported mean values for proximal longitudinal gliding of 0.8 mm and 1.3 mm [29].
Measurements were taken with the shoulder at 30º abduction, elbow extended and
forearm supinated. The effect of finger extension was assessed in two studies [25,27].
Erel et al. [27] measured median nerve gliding at the forearm with the shoulder at
45º/90º abduction, elbow extended and forearm supinated. They reported a mean
distal nerve gliding of 2.6 mm. Hough et al. [25] measured median nerve gliding at the
wrist. The mean distal nerve gliding was 12.5 mm when finger extension was
performed with the elbow flexed, and 11.2 mm when finger extension was performed
with the elbow extended. The mean difference between measurements of nerve gliding
with the elbow extended and flexed is within the MDC 95% (0.9 mm and 1.4
mm).Taken together, these results suggest that finger flexion and finger extension
induce median nerve gliding in opposite directions and that gliding increases with
proximity to the finger joints.
3.4.2. Impact of wrist movement on median nerve gliding
Three studies reported on the impact of wrist extension on median nerve gliding
[24,26,29] and measured it in the arm (mean values between 0.2 mm and 2.4 mm), in
the elbow (mean value for the only measurement made - 9 mm) and in the forearm
(mean values between 1.9 mm and 4.7 mm). The direction of the median nerve gliding
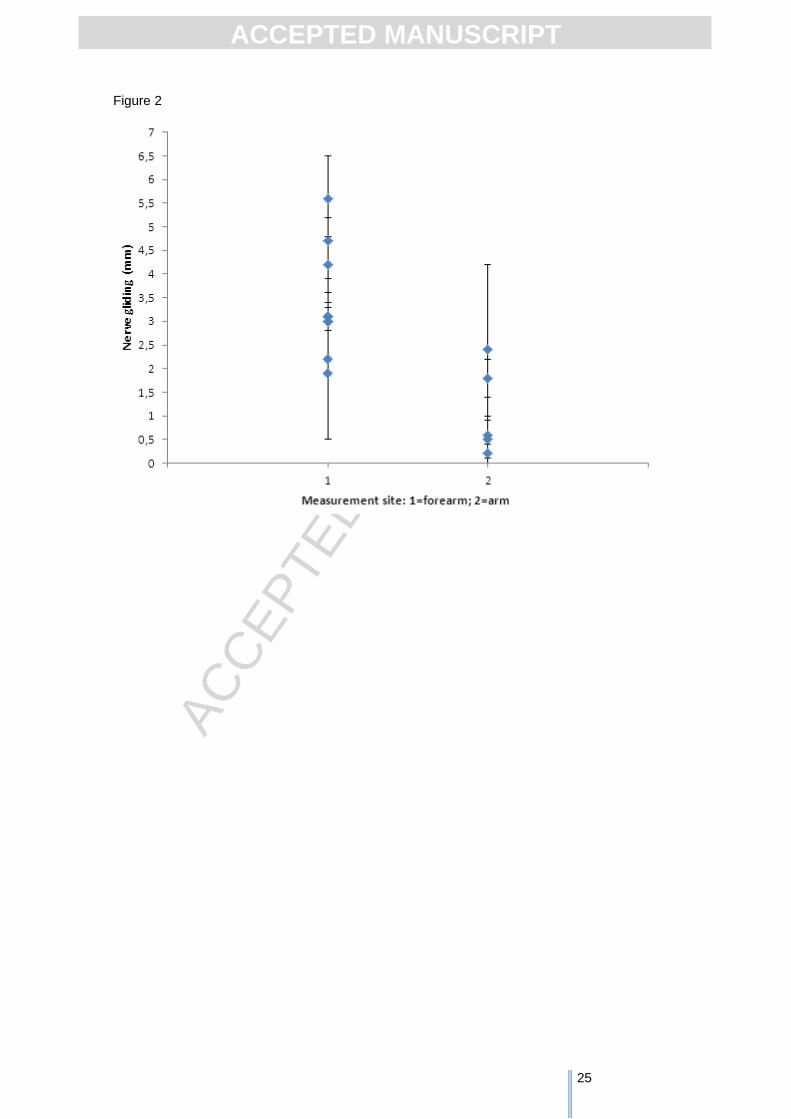
was distal for all measurements. When considering similar combinations of wrist
movement and adjacent joint positioning, data suggest that nerve gliding is higher at
the forearm compared to the arm (as illustrated in Figure 2).
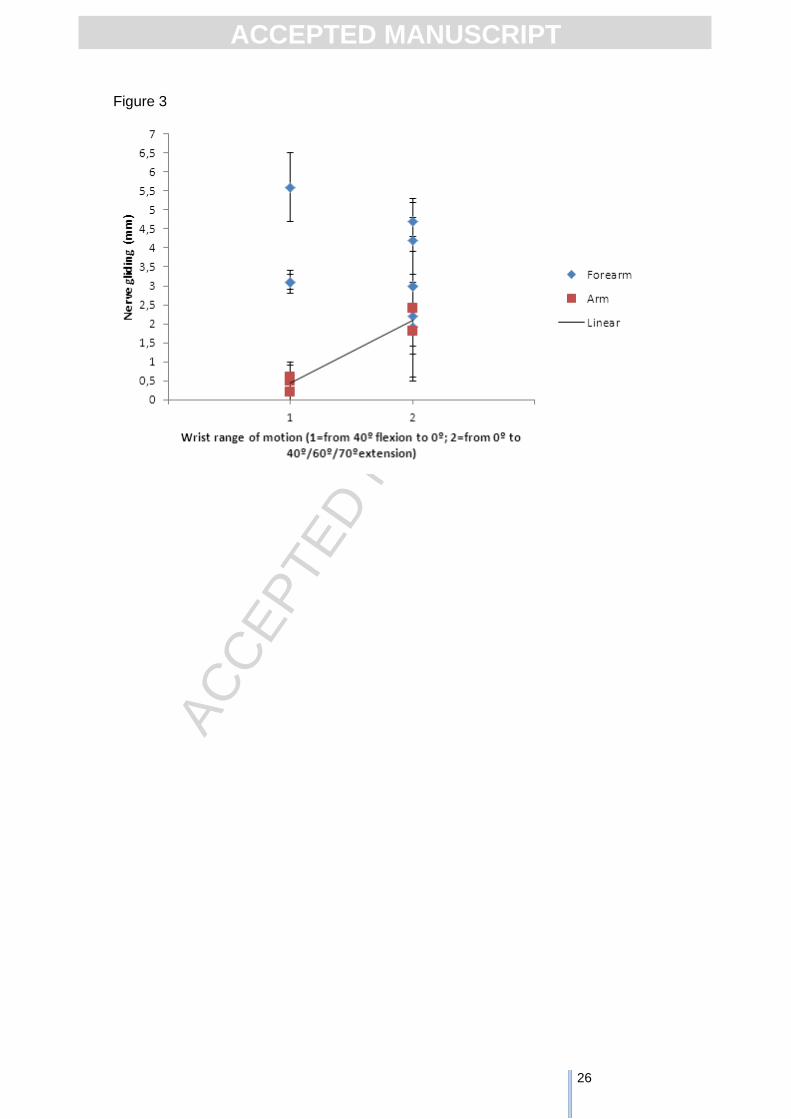
Wrist movements from 40º flexion to 0º extension induce less median nerve gliding,
particularly in the arm (arm: 0.2 mm to 0.6 mm; forearm: 3.1 mm to 5.6 mm), than wrist
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
10
movements from 0º to 40º/60º/70º extension (arm: 1.8 mm to 2.4 mm; forearm: 1.9 mm
to 4.7 mm; elbow: 9.0 mm) [24,26,29] (Figure 3). The MDC 95% was only calculated
for measurements taken at the elbow and was 1.7 mm [24]. Performing wrist extension
with the forearm supinated seems to favour nerve gliding when the shoulder is at 30º
abduction and the elbow is extended (supination: 3 mm; pronation: 1.9 mm) and also
when the shoulder is at 30º abduction and the elbow is flexed (supination: 3 mm;
pronation: 2.2 mm) [29]. No study assessed the impact of wrist flexion on median nerve
gliding.
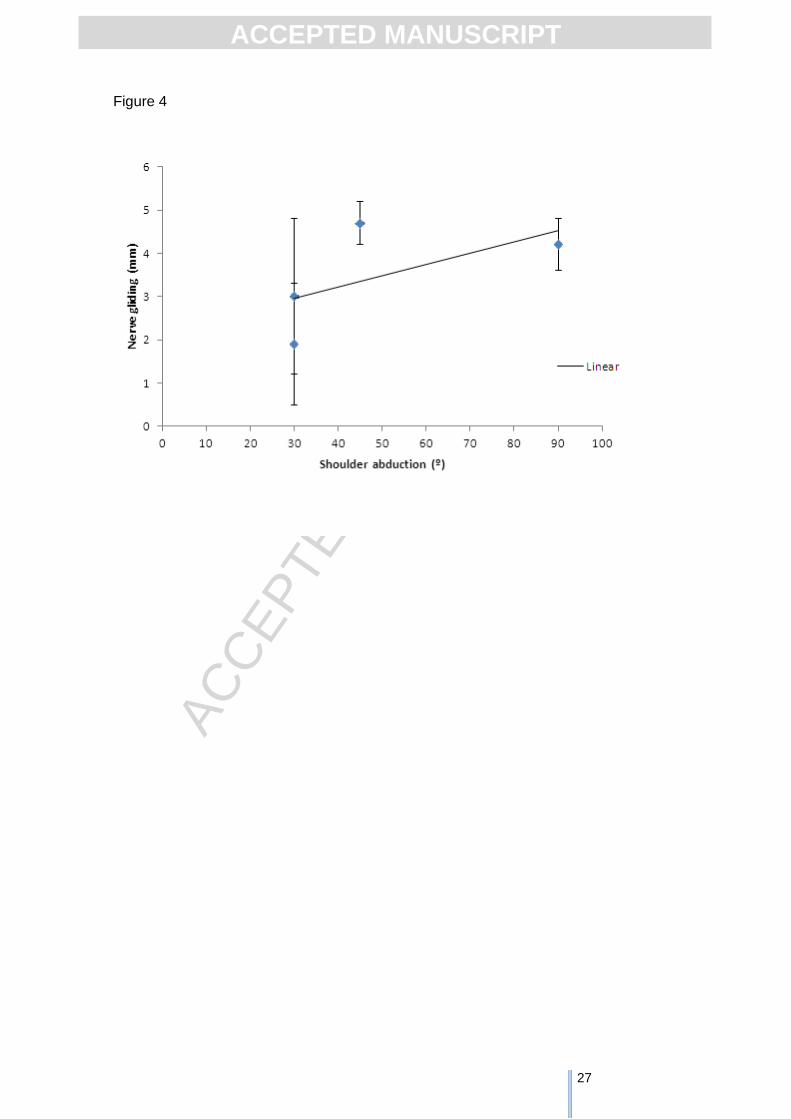
In addition, 45º and 90º of shoulder abduction seem to facilitate nerve gliding at the
forearm when wrist extension was performed from 0º to 40º/70º compared to 30º of
shoulder abduction (30º abduction: 1.9 mm to 3.0 mm; 45º abduction: 4.7 mm; 90º
abduction: 4.2 mm) [26,29]. This is illustrated in Figure 4.
3.4.3. Impact of elbow movement on median nerve gliding
Two studies assessed how elbow extension affected the median nerve gliding [19,26].
Elbow extension with the wrist in neutral position induced a mean of 10.4 mm of distal
gliding in the arm and 3.0 mm of proximal gliding in the forearm. Elbow extension with
the wrist at 45º extension induced a mean of 4.2 mm of proximal gliding in the forearm
[26].
Elbow extension with the neck in either ipsilateral or contralateral lateral flexion induced
similar distal median nerve gliding (ipsilateral=5.5 mm, contralateral=5.6mm; MDC 95%
=1.8 mm) [19]. However, elbow extension performed simultaneously to ipsilateral
lateral neck flexion induced more gliding than elbow extension performed
simultaneously to contralateral lateral neck flexion (elbow extension+ipsilateral neck
flexion=10.2 mm; elbow extension+contralateral neck flexion= 1.8 mm; MDC 95%=1.8
mm) [19].
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
11
Taken together, results suggest that when performing elbow extension: i) the median
nerve glides in opposite directions in the arm and forearm, ii) positioning the wrist in
extension increases median nerve gliding compared to positioning the wrist in neutral,
iii) simultaneously performing a movement of the neck that shortens nerve bed
increases nerve gliding, and iv) simultaneously performing a movement of the neck that
elongates nerve bed decreases nerve gliding.
No study assessed the impact of elbow flexion on median nerve gliding.
3.4.4. Impact of shoulder movement on median nerve gliding
Two studies assessed the effect of shoulder movements on median nerve gliding
[26,28]. Shoulder abduction (10º-90º) and shoulder protraction induced proximal gliding
of the median nerve both at the arm and forearm. Mean values were similar for both
movements (abduction: 5.2 mm in the arm and 3.4 mm in the forearm; protraction: 5.9
mm in the arm and 3.5 mm in the forearm; MDC 95% for shoulder protraction = 1.7 mm
in the arm and 0.8 mm in the forearm).
3.4.5. Impact of neck movement on median nerve gliding
The impact of neck contralateral lateral flexion on median nerve gliding was
investigated in three studies [11,19,28]. Mean values for proximal nerve gliding varied
between 0.9 mm and 3.4 mm in the arm and between 0.6 mm and 2.3 mm in the
forearm. Cervical contralateral lateral flexion induced slightly less gliding than a cervical
lateral glide (away from the side to be tested) at C5/C6 both at the middle (glide=3.3
mm; lateral flexion=2.3 mm; MDC 95% = 0.3 mm and 0.8 mm) and at the distal forearm
(glide=2.5 mm; lateral flexion=1.9 mm; MDC 95%= 0.6) [11].
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
12
Performing cervical contralateral lateral flexion with the shoulder abducted or in a
neutral position seems to increase median nerve gliding compared to performing the
same movement with the shoulder protracted (protraction: arm = 0.9 mm, forearm = 0.6
mm; neutral: arm = 2.3 mm, forearm = 1.5 mm; abduction: forearm = 1.9 mm to 2.3
mm; MDC 95% ≤ 0.8 mm) [11,28]. Elbow position does not seem to affect the gliding of
the median nerve in response to lateral flexion of the neck (flexion = 3.4 mm; extension
= 3.3 mm; MDC 95%=1.8 mm) [19].
The impact of neck flexion on median nerve gliding was assessed in one study [26].
Mean values for gliding of the median nerve in the arm were higher than mean values
in the forearm and at 90º of shoulder abduction compared to 30º of shoulder abduction
(30º abduction: arm=0.5 mm, forearm=0.3 mm; 90º abduction: arm=1.3 mm,
forearm=0.8 mm).
Forward head posture seems to induce virtually no nerve gliding at both the arm and
forearm [28].
3.4.6. Impact of trunk movement on median nerve gliding
Trunk flexion seems to have virtually no effect on median nerve excursion at the
forearm [28]. Key findings in relation to median nerve gliding are summarized in Table
2.
3.5. Median nerve strain
Dilley et al. [26] was the only study that reported on median nerve strain.
Measurements were taken at the forearm in response to wrist, elbow, shoulder and
neck movements. Wrist extension from neutral to 40º induced similar strain when the
shoulder was at 45º and at 90º abduction (between 1.1 % and 2.0%). Study authors
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
13
reported that it was not possible to calculate strain induced by wrist extension from 40º
flexion to neutral and they suggested that the nerve might be unloaded in these
positions. Shoulder abduction (10º - 90º) when the elbow and wrist were in neutral
positions was associated to an increase in strain of 1%. Elbow extension from 90º
flexion to neutral when the shoulder was at 90º abduction and the wrist was neutral
was associated to an increase in strain of 0.6%. Neck flexion induced virtually no
increase in strain.
3.6. Ulnar nerve longitudinal gliding
One study reported on ulnar nerve gliding [30]. The ulnar nerve glided distally at the
forearm with wrist extension (1.1 mm to 3.0 mm; MDC 95% ≤ 1.4 mm). Elbow flexion
induced proximal gliding at the forearm (0.8 mm; MDC 95%=0.6 mm) and virtually no
movement at the upper arm. Shoulder abduction (40º to 90º) induced virtually no
longitudinal excursion of the ulnar nerve (Table 2).
3.7. Tibial nerve longitudinal gliding
Two studies assessed the tibial nerve gliding at the popliteal fossa and in response to
ankle dorsiflexion either alone [5] or performed simultaneously to neck extension [31].
The tibial nerve glided distally in both studies. Nerve gliding in response to ankle
dorsiflexion alone was assessed in side lying and mean values decreased with an
increase in hip flexion (hip at 20º flexion=2.2 mm hip at 62º flexion=0.7 mm) [5]. Nerve
gliding in response to ankle dorsiflexion performed simultaneously to neck extension
was assessed in a seated position and induced a mean gliding of 5.2 mm (MDC 95% =
1.4 mm) [31] (Table 2).
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
14
3.8. Sciatic nerve longitudinal gliding
Two studies measured gliding of the sciatic nerve at the mid-thigh when participants
were in a seated position [15,31]. Performing neck extension simultaneously to ankle
dorsiflexion (sitting upright) induced similar gliding of the sciatic nerve to performing
neck extension simultaneously to knee extension (slumped spinal posture) (neck
extension+ankle dorsiflexion=3.5 mm; neck extension+knee extension=3.3 mm; MDC
95% ≤ 2.2 mm) [15,31]. Neck flexion performed simultaneously to knee extension
induced a similar amount of gliding to knee extension with the neck in a neutral position
(neck flexion+knee extension=knee extension=2.6 mm; MDC 95% = 0.6 mm) [15].
Neck flexion alone with the knee also in flexion induced virtually no nerve movement
[15].
4. Discussion
This systematic review showed that there are a limited number of in vivo studies
investigating the effect of joint movement on normal nerve longitudinal excursion for
nerves other than the median nerve. Furthermore, we found one study only that
investigated the impact of joint movement on nerve strain. Despite this, this systematic
review also shows that different combinations of movement and adjacent joint
positioning impact differently on the biomechanics of the peripheral nervous system.
Simultaneous joint movements that elongate the nerve bed at one end and shorten it at
the other, i.e. sliding techniques, seem to promote the greatest nerve excursion. In
contrast, combinations of joint movements that elongate the nerve at both ends,
tensioning techniques, seem to induce the least amount of nerve excursion. For
example, simultaneous elbow extension and cervical ipsilateral lateral flexion induced
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
15
10.2 mm of median nerve gliding while simultaneous elbow extension and cervical
contralateral lateral flexion induced 1.8 mm of median nerve gliding [19]. A similar
behavior was reported by Ellis et al. [15] for the sciatic nerve: simultaneous knee
extension and neck extension induced 3.3 mm of gliding while knee extension with
neck flexion induced 2.6 mm of gliding. In addition, joint movements performed at
different angles seem to impact nerve biomechanics differently. For example, there is
less median nerve gliding in response to wrist extension when wrist movement is
performed from 40º flexion to a neutral position compared to when it is performed from
neutral to 40º extension (e.g. 3.1 mm vs. 4.7 mm at the forearm) [26]. Furthermore,
findings of the same authors [26] showed that strain for the median nerve varied
between 1.1% and 2.0% when wrist extension was performed from 0º to 40º and that
the nerve was unloaded when wrist extension was performed from 40º flexion to
neutral.
Results also suggest that nerve gliding decreases as the distance from the moving joint
increases. For example, wrist extension from 0º to 40º induced nerve gliding between
0.2 mm and 2.4 mm in the arm and between 4.6 mm and 5.6 mm in the forearm [26]
and a cervical lateral glide induced 2.5 mm of nerve gliding in the distal forearm and
3.3 mm in the middle forearm [11]. This highlights the need to accurately describe the
site of measurement in future studies. For example, 7 to 10 cm proximal to the medial
epicondyle as described by Coppieters et al. [19]. Additionally, it suggests that nerve
bed length should be considered when defining the site of measurement.
The direction of nerve gliding (proximal or distal nerve excursion) seems to be
influenced by the joint movements being performed. Finger flexion induces proximal
median nerve gliding at both the arm and the forearm, while finger extension induces
distal median nerve gliding. Wrist extension induces distal nerve gliding at the arm the
elbow and the forearm. These findings suggest that wrist and finger movements that
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
16
elongate the nerve bed are associated with median nerve distal excursion through the
whole upper limb, while movements that shorten the nerve bed are associated with
proximal median nerve excursion. The nerve behaves slightly differently with elbow
movement. Elbow extension induces distal median nerve gliding at the arm and
proximal median nerve gliding at the forearm, suggesting that the median nerve
converges towards the elbow. This is in accordance with the convergence mechanism,
according to which when the nerve bed lengthens at the elbow the nerve sections
above and below the joint converge towards it [2]. Shoulder abduction and neck
contralateral lateral flexion seem to induce proximal median nerve gliding at both the
arm and the forearm when adjacent joints are stationary, suggesting that shoulder and
neck movements that elongate the nerve bed are associated with proximal excursion of
the nerve through the whole upper limb. How nervous structures behave in response to
movement between the shoulder and the neck was not measured in any of the studies
included in this systematic review and needs to be investigated as it is of relevance to
nerve entrapments located in this body segment. Taken together the results suggest
that nerves glide towards the joint if the movement elongates the nerve bed and away
from the joint if the movement shortens it, in line with the conclusions of a previous
review [2].
The MDC is an estimate of the amount of change between two points in time that
indicates a true change and, therefore, could be used to inform the clinical significance
of measurements [23]. MDC 95% for individual measurements of included studies was
smaller than the respective nerve gliding. Additionally, differences between the mean
values of nerve gliding induced by different joint movements were also above the MDC
95%. Both findings suggest that joint movement induces nerve gliding above
measurement error.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
17
The findings of this systematic review identify a set of variables that affect nerve
gliding. We believe that this information will help clinicians in their rationale when
selecting a specific combination of movements to perform neural mobilization, justifying
the progression of treatment or judging its outcome. Similarly, the findings of this
systematic review will inform researchers when designing studies aiming to compare
different techniques of nervous system mobilization or assess its effectiveness. The
variables likely to influence nerve gliding are: i) range of movement, ii) moving joint, iii)
distance from the moving joint to the site of the lesion, iv) position of adjacent joints, v)
number of moving joints and vi) whether joint movement stretches or shortens nerve
bed. Therefore, these variables need to be considered when designing and justifying
neural mobilization based interventions. Furthermore, they can be manipulated in order
to suit patients’ needs. The number of variables that need to be considered make
neural mobilization very flexible and adaptable to patients’ conditions, but also
challenges standardization.
Included studies failed mostly in terms of sample representativeness, blinding of the
assessors and a priori sample size calculation. No study was considered to include a
sample that was representative of the population. Studies either use convenience
samples, or fail to identify the source population for participants and describe how they
were selected. Only five studies were considered to use a blinded assessor (out of the
12 included studies). Sample sizes varied between 1 and 37 participants, but 8 studies
had a sample size of less than 20 participants. These methodological limitations may
compromise the validity of the findings and the precision of the estimates. To improve
the evidence-base, these factors should be taken into consideration during the design
of future studies.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
18
Future research needs to investigate whether combinations of joint movements that
impact nerve biomechanics differently also have different physiological consequences,
are more efficient in certain stages of disease or for certain patients. More research is
also needed investigating the relationship between gliding and strain so that clinicians
are informed on how to induce the highest gliding without considerable increases in
strain. For example, Coppieters and Butler [35] have found that sliding techniques
result in a substantially larger excursion of the nerves than tensioning techniques and
that this larger excursion is associated with a much smaller increase in strain. High
levels of strain may affect neural function, in particular vascularization and axonal
transport [36]. However, both studies were conducted in embalmed cadavers [35,36].
Furthermore, it has been shown that a strain of 5%-10% affects vascularization and at
15% intraneural vascularization is completely blocked in rats [37]. Strain levels for the
median nerve reported by Dilley et al. [26] were below the harmful levels of strain
previously reported in cadaver studies [20,36,38], suggesting that nervous system
mobilization is unlikely to reach strain levels that affect nerve functioning. However, this
was the only study found investigating strain in human healthy participants [26].
Whether personal factors such as sex or age affect nerve gliding was not explored in
included studies and might be considered in future studies.
Review limitations
This review should be seen in light of its limitations. Heterogeneity of included studies,
in particular in terms of moving joints, positioning of adjacent joints and measurement
site prevented meta-analysis. Additional limitations were the small number of included
studies and the small number of participants in some studies. We used USA spelling
for databases’ search (e.g. mobilization) and this might have influenced the outcome of
the search.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
19
5. Conclusions
This systematic review showed that joint movement might induce up to 12. 5 mm of
nerve gliding, which seem to vary according to range of motion for the moving joint,
distance from the moving joint to the site of the lesion, position of adjacent joints,
number of moving joints and whether joint movement stretches or shortens nerve bed.
Therefore, these factors need to be considered when designing neural mobilization
exercises for both clinical practice and research.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
20
References
1. Butler D. Adverse Mechanical Tension in the Nervous System: A model for Assessment and Treatmen. Aust J Physiother.35 (1989) 12.
2. Topp K, Boyd BS. Structure and Biomechanics of Peripheral Nerves: Nerve Responses to Physical Stresses and Implications for Physical Therapist Practice. Phys Ther. 86 (2006) 92–109.
3. Wall E, Massie J, MK K, Rydevik B, Myers R, Garfin S. Experimental stretch neuropathy: changes in nerve conduction under tension. J Bone Jt Surg Br. 74 (1992) 126–9.
4. Rydevik B, Lundborg G, Bagge U. Effects of graded compression on intraneural blood blow. An in vivo study on rabbit tibial nerve. J Hand Surg. 6 (1981) 3–12.
5. Boyd B, Gray A, Dilley A, Wanek L, Topp K. The pattern of tibial nerve excursion with active ankle dorsiflexion is different in older people with diabetes mellitus. Clin Biomech. 27 (2012) 967–71.
6. Yoshii Y, Ishii T, Tung W, Sakai S, Amadio P. Median nerve deformation and displacement in the carpal tunnel during finger motion. J Orthop Res. 31 (2013)1876–80.
7. Ozoa G, Alves D, Fish D. Thoracic outlet syndrome. Phys Med Rehabil Clin N Am. 22 (2011) 473–83.
8. Green J, Rayan G. The cubital tunnel: anatomic, histologic, and biomechanical study. J Shoulder Elbow Surg. 8 (1999) 466–70.
9. Godoi J, Kerppers I, Rossi L, Corrêa F, Costa R, Corrêa J, et al. Electromyographic analysis of biceps brachii muscle following neural mobilization in patients with stroke. Electromyogr Clin Neurophysiol. 50 (2010) 55–60.
10. Saban B, Deutscher D, Ziv T. Deep massage to posterior calf muscles in combination with neural mobilization exercises as a treatment for heel pain: a pilot randomized clinical trial. Man Ther. 19 (2014) 102–8.
11. Brochwicz P, von Piekartz H, Zalpour C. Sonography assessment of the median nerve during cervical lateral glide and lateral flexion. Is there a difference in neurodynamics of asymptomatic people? Man Ther. 18 (2013) 216–9.
12. Santos FM, Silva JT, Giardini AC, Rocha P A, Achermann APP, Alves AS, et al. Neural mobilization reverses behavioral and cellular changes that characterize neuropathic pain in rats. Mol Pain. Molecular Pain. 8 (2012) 57.
13. Brown C, Gilbert K, Brismee J, Sizer P, Roger C, Smith M. The effects of neurodynamic mobilization on fluid dispersion within the tibial nerve at the ankle: an unembalmed cadaveric study. J Man Manip Ther.19 (2011) 9.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
21
14. Beneciuk J, Bishop M, George S. Effects of upper extremity neural mobilization on thermal pain sensitivity: a sham-controlled study in asymptomatic participants. J Orthop Sport Phys Ther. 39 (2009) 428–38.
15. Ellis RF, Hing W a, McNair PJ. Comparison of longitudinal sciatic nerve movement with different mobilization exercises: an in vivo study utilizing ultrasound imaging. J Orthop Sports Phys Ther. 42 (2012) 667–75.
16. Page M, O’Connor D, Pitt V, Massy-Westropp N. Exercise and mobilisation interventions for carpal tunnel syndrome. Cochrane Database Syst Rev. 13 (2012) CD009899.
17. Ellis R, Hing W. Neural mobilization: a systematic review of randomized controlled trials with an analysis of therapeutic efficacy. J Man Manip Ther. 16 (2008) 8–22.
18. Alshami AM, Babri AS, Souvlis T, Coppieters MW. Strain in the tibial and plantar nerves with foot and ankle movements and the influence of adjacent joint positions. J Appl Biomech. 24 (2008) 368–76.
19. Coppieters MW, Hough AD, Dilley A. Different nerve-gliding exercises induce different magnitudes of median nerve longitudinal excursion: an in vivo study using dynamic ultrasound imaging. J Orthop Sports Phys Ther. 39 (2009) 164–71.
20. Coppieters MW, Alshami AM, Sciences R. Longitudinal Excursion and Strain in the Median Nerve during Novel Nerve Gliding Exercises for Carpal Tunnel Syndrome. J Orthop Res. 25 (2006) 972–80.
21. Downs S, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Heal. 52 (1998) 377–84.
22. Fernando M, Crowther R, Lazzarini P, Sangla K, Cunningham M, Buttner P, et al. Biomechanical characteristics of peripheral diabetic neuropathy: A systematic review and meta-analysis of findings from the gait cycle, muscle activity and dynamic barefoot plantar pressure. Clin Biomech. 28 (2013) 831–45.
23. Donoghue D, Stokes EK. How much change is true change? The minimum detectable change of the Berg Balance Scale in elderly people. J Rehabil Med. 41 (2009) 343–6.
24. Hough AD, Moore AP, Jones MP. Peripheral nerve motion measurement with spectral Doppler sonography: a reliability study. J Hand Surg Br. 25 (2000) 585–9.
25. Hough AD, Moore AP, Jones MP. Reduced longitudinal excursion of the median nerve in carpal tunnel syndrome. Arch Phys Med Rehabil. 88 (2007) 569–76.
26. Dilley A, Lynn B, Greening J, DeLeon N. Quantitative in vivo studies of median nerve sliding in response to wrist, elbow, shoulder and neck movements. Clin Biomech. 18 (2003) 899–907.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
22
27. Erel E, Dilley A, Greening J, Morris V, Cohen B, Lynn B. Longitudinal sliding of the median nerve in patients with carpal tunnel syndrome. J Hand Surg Br. 28 (2003) 439–43.
28. Julius A, Lees R, Dilley A, Lynn B. Shoulder posture and median nerve sliding. BMC Musculoskelet Disord. 5 (2004) 23.
29. Echigo A, Aoki M, Ishiai S, Yamaguchi M, Nakamura M, Sawada Y. The excursion of the median nerve during nerve gliding exercise: an observation with high-resolution ultrasonography. J Hand Ther. 21 (2008) 221–7.
30. Dilley A, Summerhayes C, Lynn B. An in vivo investigation of ulnar nerve sliding during upper limb movements. Clin Biomech. 22 (2007) 774–9.
31. Ellis R, Hing W, Dilley A, McNair P. Reliability of measuring sciatic and tibial nerve movement with diagnostic ultrasound during a neural mobilisation technique. Ultrasound Med Biol. 34 (2008) 1209–16.
32. Dilley A, Greening J, Lynn B, Leary R, Morris V. The use of cross-correlation analysis between high-frequency ultrasound images to measure longitudinal median nerve movement. Ultrasound Med Biol. 27 (2001) 1211–8.
33. Fleiss J. The design and analysis of clinical experiments. New York: John Wiley and Sons; 1986.
34. Haley S, Fragala-Pinkham M. Interpreting change scores of tests and measures used in physical therapy. Phys Ther. 86 (2006) 735–43.
35. Coppieters MW, Butler DS. Do “sliders” slide and “tensioners” tension? An analysis of neurodynamic techniques and considerations regarding their application. Man Ther. 13 (2008) 213–21.
36. Coppieters MW, Alshami AM, Babri AS, Souvlis T, Kippers V, Hodges PW. Strain and Excursion of the Sciatic , Tibial , and Plantar Nerves during a Modified Straight Leg Raising Test. J Orthop Res.24 (2006) 1883–9.
37. Ogata K, Naito M. Blood flow of peripheral nerve effects of dissection stretching and compression. J Hand Surg Br. 11 (1986) 4.
38. Wright TW, Glowczewskie F, Wheeler D, Miller G, Cowin D. Excursion and strain of the median nerve. J Bone Joint Surg Am. 78 (1996) 1897–903.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
23
Figure 1 – Flow chart for the systematic review.
Figure 2 – Mean and standard deviation for median nerve gliding during wrist extension
in relation to measurement site (data from Dilley et al. 26 and Echigo et al. 29).
Figure 3 – Mean and standard deviation for median nerve gliding during wrist extension
in relation to wrist range of motion and measurement site (data from Dilley et al. 26).
Figure 4 – Mean and standard deviation for median nerve gliding measured at the
forearm during wrist extension in relation to shoulder abduction (data from Dilley et al. 26 and Echigo et al. 29).
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
24
Figure 1
Data sources and references found:
PubMed
PEDro
Scielo
Cochrane
Web of Science
Total: n=4008
Titles/abstracts screened for
inclusion (n=3004).
Duplicates
(n=1004).
Publications retrieved for
detailed evaluation, including
manual screening of retrieved
papers (n=46).
Identified by
title/abstract as not
relevant (n=2959).
Publications to be included in
analysis (n=12).
Failed to meet the eligibility criteria (n=34), mainly due to being:
Opinion papers;
Studies conducted in animals or cadavers;
Studies that used invasive procedures.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
25
Figure 2
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
26
Figure 3
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
27
Figure 4
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
28
Tables
Table 1 – Assessment of methodological quality of included studies.
Question Hough et al.,
24
Dilley et al.,
26
Erel et al.,
27
Julius et al.,
28
Hough et al.,
25
Echigo et al.,
29
Coppieters et al.,
19
Brochwicz et al.,
11
Dilley et al.,
29
Boyd et al.,
5
Ellis et al.,
31
Ellis et al.,
15
1. Hypothesis/aim/objective 1 1 1 1 1 1 1 1 1 1 1 1
2. Main outcomes 1 1 1 1 1 1 1 1 1 1 1 1
3. Participants characteristics 1 1 1 1 1 1 1 1 1 1 1 1
5. Confounders 0 0 0 0 01 01 1 01 01 01 01 1
6. Findings 1 1 1 1 1 1 1 1 1 1 1 1
7. Estimates of the random variability 1 1 1 1 1 1 1 1 1 1 1 1
10. Actual probability values 0 0 0 0 1 01 1 0 0 1 0 1
11. Subjects representative population (asked) 0 0 0 0 0 0 0 0 0 0 0 0
12. Subjects representative population (agreed) 0 0 0 0 0 0 0 0 0 0 0 0
15. Blinding of assessors 1 0 0 0 1 01 0 0 0 0 1 1
16. Data dredging 1 1 1 1 1 1 1 1 1 1 1 1
18. Apropriate statistical tests 1 1 1 1 1 1 1 1 1 1 1 1
20. Outcome measures valid and reliable 1 1 1 1 1 1 1 1 1 1 1 1
21. Internal validity (selection bias) 0 0 0 0 1 1 1 1 01 1 1 1
22. Recruitment time period 0 0 0 0 1 1 1 01 01 1 1 1
25. Adjustment for confounding 0 1 0 1 1 1 1 01 1 1 1 1
27. Statistical power determined 0 0 0 0 1 0 01 0 0 0 0 1
Total (Assessor AGS) vs (Assessor MPB) (9) vs
(9) (9) vs
(9) (8) vs
(8) (9) vs
(9) (15) vs
(14) (13) vs
(12) (14) vs
(13) (10) vs
(11) (10) vs
(11) (13) vs
(12) (13) vs
(12) (15) vs
(15)
1 - considered appropriately addressed by both assessors; 0 - considered inappropriately addressed by both assessors; 01 - considered appropriately addressed by one assessor and in appropriately addressed by the other.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
29
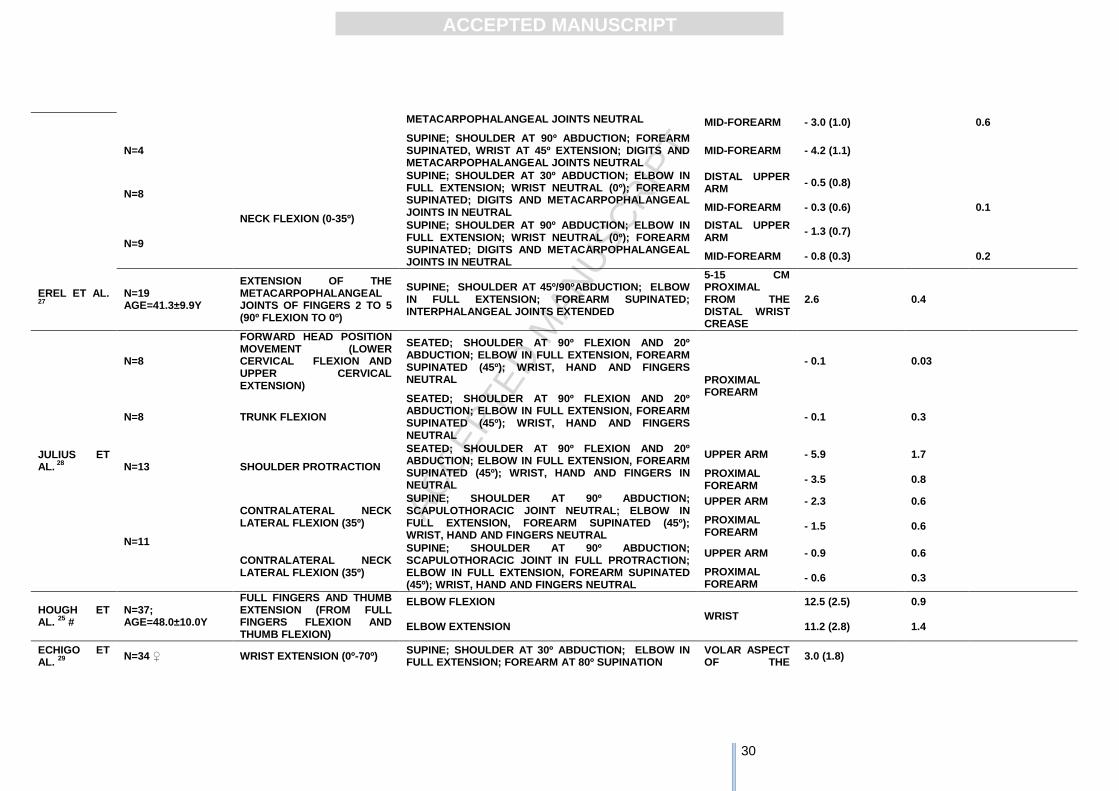
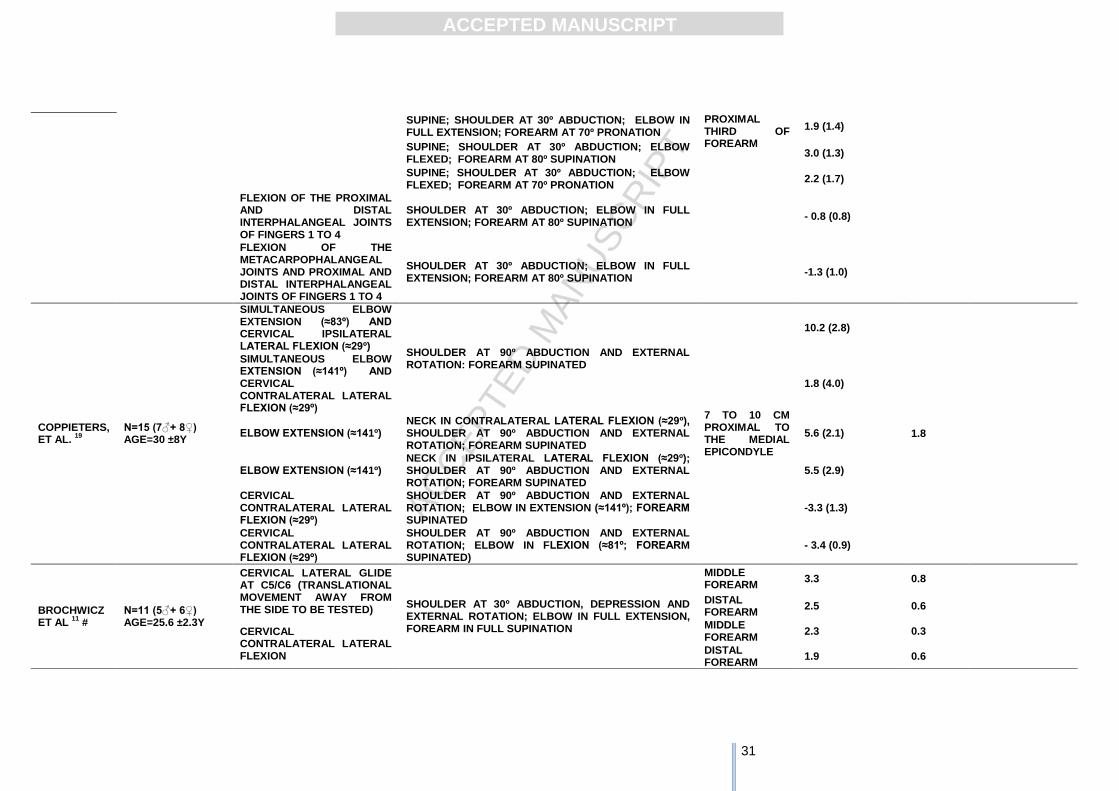
Table 2 – Longitudinal excursion and strain of the median nerve.
AUTHORS SAMPLE SIZE
& CHARACTERISTICS
MOVEMENT & INVOLVED JOINTS
PARTICIPANT POSITION & POSITION OF ADJACENT JOINTS
SITE OF MEASUREMENT
RESULTS
LONGITUDINAL EXCURSION
MEAN (SD) (MM)
MDC 95% CI (MM)
STRAIN (%) (MINIMUM TO
MAXIMAL CHANGE)
MEDIAN NERVE
HOUGH ET AL.
23
N=16 AGE=26-61Y
WRIST EXTENSION (0º-60º) SUPINE; SHOULDER AT 45º ABDUCTION; ELBOW IN FULL EXTENSION; FOREARM SUPINATED
ELBOW 9.0 (2.1) 1.7
DILLEY,ET AL.
26
N=10
WRIST EXTENSION (0º - 40º)
SUPINE; SHOULDER AT 45º ABDUCTION; ELBOW IN FULL EXTENSION; FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
DISTAL UPPER ARM
2.4 (1.8)
MID-FOREARM 4.7 (0.5) P=1.1 D=1.5
SUPINE; SHOULDER AT 90º ABDUCTION; ELBOW IN FULL EXTENSION; FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
DISTAL UPPER ARM
1.8 (0.4)
MID-FOREARM 4.2 (0.6) P=1.1 D=2.0
N=4
WRIST EXTENSION (40º - 0º)
SUPINE; SHOULDER AT 30º ABDUCTION; ELBOW AT 90º FLEXION; FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS IN NEUTRAL
DISTAL UPPER ARM
0.2 (0.2)
MID-FOREARM 5.6 (0.9)
STRAIN NOT DETERMINED; NERVE MAY BE UNLOADED
N=6 SUPINE; SHOULDER AT 45º ABDUCTION; ELBOW IN FULL EXTENSION; FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
DISTAL UPPER ARM
0.5 (0.4)
MID-FOREARM 3.1 (0.3)
STRAIN NOT DETERMINED; NERVE MAY BE UNLOADED
N=3 SUPINE; SHOULDER AT 90º ABDUCTION; ELBOW IN FULL EXTENSION; FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
DISTAL UPPER ARM
0.6 (0.4)
MID-FOREARM 3.1 (0.2)
STRAIN NOT DETERMINED; NERVE MAY BE UNLOADED
N=4 SHOULDER ABDUCTION (10º-90º)
SUPINE; ELBOW IN FULL EXTENSION, WRIST NEUTRAL (0º); FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
DISTAL UPPER ARM
- 5.2 (0.7)
MID-FOREARM - 3.4 (0.8) 1.0
N=7 ELBOW EXTENSION (90º-0º) SUPINE; SHOULDER AT 90º ABDUCTION; WRIST NEUTRAL (0º); FOREARM SUPINATED; DIGITS AND
DISTAL UPPER ARM
10.4 (2.3)
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
30
METACARPOPHALANGEAL JOINTS NEUTRAL MID-FOREARM - 3.0 (1.0) 0.6
N=4 SUPINE; SHOULDER AT 90º ABDUCTION; FOREARM SUPINATED, WRIST AT 45º EXTENSION; DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
MID-FOREARM - 4.2 (1.1)
N=8
NECK FLEXION (0-35º)
SUPINE; SHOULDER AT 30º ABDUCTION; ELBOW IN FULL EXTENSION; WRIST NEUTRAL (0º); FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS IN NEUTRAL
DISTAL UPPER ARM
- 0.5 (0.8)
MID-FOREARM - 0.3 (0.6) 0.1
N=9
SUPINE; SHOULDER AT 90º ABDUCTION; ELBOW IN FULL EXTENSION; WRIST NEUTRAL (0º); FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS IN NEUTRAL
DISTAL UPPER ARM
- 1.3 (0.7)
MID-FOREARM - 0.8 (0.3) 0.2
EREL ET AL. 27
N=19 AGE=41.3±9.9Y
EXTENSION OF THE METACARPOPHALANGEAL JOINTS OF FINGERS 2 TO 5 (90º FLEXION TO 0º)
SUPINE; SHOULDER AT 45º/90ºABDUCTION; ELBOW IN FULL EXTENSION; FOREARM SUPINATED; INTERPHALANGEAL JOINTS EXTENDED
5-15 CM PROXIMAL FROM THE DISTAL WRIST CREASE
2.6 0.4
JULIUS ET AL.
28
N=8
FORWARD HEAD POSITION MOVEMENT (LOWER CERVICAL FLEXION AND UPPER CERVICAL EXTENSION)
SEATED; SHOULDER AT 90º FLEXION AND 20º ABDUCTION; ELBOW IN FULL EXTENSION, FOREARM SUPINATED (45º); WRIST, HAND AND FINGERS NEUTRAL PROXIMAL
FOREARM
- 0.1 0.03
N=8 TRUNK FLEXION
SEATED; SHOULDER AT 90º FLEXION AND 20º ABDUCTION; ELBOW IN FULL EXTENSION, FOREARM SUPINATED (45º); WRIST, HAND AND FINGERS NEUTRAL
- 0.1 0.3
N=13 SHOULDER PROTRACTION
SEATED; SHOULDER AT 90º FLEXION AND 20º ABDUCTION; ELBOW IN FULL EXTENSION, FOREARM SUPINATED (45º); WRIST, HAND AND FINGERS IN NEUTRAL
UPPER ARM - 5.9 1.7
PROXIMAL FOREARM
- 3.5 0.8
N=11
CONTRALATERAL NECK LATERAL FLEXION (35º)
SUPINE; SHOULDER AT 90º ABDUCTION; SCAPULOTHORACIC JOINT NEUTRAL; ELBOW IN FULL EXTENSION, FOREARM SUPINATED (45º); WRIST, HAND AND FINGERS NEUTRAL
UPPER ARM - 2.3 0.6
PROXIMAL FOREARM
- 1.5 0.6
CONTRALATERAL NECK LATERAL FLEXION (35º)
SUPINE; SHOULDER AT 90º ABDUCTION; SCAPULOTHORACIC JOINT IN FULL PROTRACTION; ELBOW IN FULL EXTENSION, FOREARM SUPINATED (45º); WRIST, HAND AND FINGERS NEUTRAL
UPPER ARM - 0.9 0.6
PROXIMAL FOREARM
- 0.6 0.3
HOUGH ET AL.
25 #
N=37; AGE=48.0±10.0Y
FULL FINGERS AND THUMB EXTENSION (FROM FULL FINGERS FLEXION AND THUMB FLEXION)
ELBOW FLEXION
WRIST
12.5 (2.5) 0.9
ELBOW EXTENSION 11.2 (2.8) 1.4
ECHIGO ET AL.
29
N=34 ♀ WRIST EXTENSION (0º-70º) SUPINE; SHOULDER AT 30º ABDUCTION; ELBOW IN FULL EXTENSION; FOREARM AT 80º SUPINATION
VOLAR ASPECT OF THE
3.0 (1.8)
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
31
SUPINE; SHOULDER AT 30º ABDUCTION; ELBOW IN FULL EXTENSION; FOREARM AT 70º PRONATION
PROXIMAL THIRD OF FOREARM
1.9 (1.4)
SUPINE; SHOULDER AT 30º ABDUCTION; ELBOW FLEXED; FOREARM AT 80º SUPINATION
3.0 (1.3)
SUPINE; SHOULDER AT 30º ABDUCTION; ELBOW FLEXED; FOREARM AT 70º PRONATION
2.2 (1.7)
FLEXION OF THE PROXIMAL AND DISTAL INTERPHALANGEAL JOINTS OF FINGERS 1 TO 4
SHOULDER AT 30º ABDUCTION; ELBOW IN FULL EXTENSION; FOREARM AT 80º SUPINATION
- 0.8 (0.8)
FLEXION OF THE METACARPOPHALANGEAL JOINTS AND PROXIMAL AND DISTAL INTERPHALANGEAL JOINTS OF FINGERS 1 TO 4
SHOULDER AT 30º ABDUCTION; ELBOW IN FULL EXTENSION; FOREARM AT 80º SUPINATION
-1.3 (1.0)
COPPIETERS, ET AL.
19
N=15 (7♂+ 8♀) AGE=30 ±8Y
SIMULTANEOUS ELBOW EXTENSION (≈83º) AND CERVICAL IPSILATERAL LATERAL FLEXION (≈29º)
SHOULDER AT 90º ABDUCTION AND EXTERNAL ROTATION: FOREARM SUPINATED
7 TO 10 CM PROXIMAL TO THE MEDIAL EPICONDYLE
10.2 (2.8)
1.8
SIMULTANEOUS ELBOW EXTENSION (≈141º) AND CERVICAL CONTRALATERAL LATERAL FLEXION (≈29º)
1.8 (4.0)
ELBOW EXTENSION (≈141º) NECK IN CONTRALATERAL LATERAL FLEXION (≈29º), SHOULDER AT 90º ABDUCTION AND EXTERNAL ROTATION; FOREARM SUPINATED
5.6 (2.1)
ELBOW EXTENSION (≈141º) NECK IN IPSILATERAL LATERAL FLEXION (≈29º); SHOULDER AT 90º ABDUCTION AND EXTERNAL ROTATION; FOREARM SUPINATED
5.5 (2.9)
CERVICAL CONTRALATERAL LATERAL FLEXION (≈29º)
SHOULDER AT 90º ABDUCTION AND EXTERNAL ROTATION; ELBOW IN EXTENSION (≈141º); FOREARM SUPINATED
-3.3 (1.3)
CERVICAL CONTRALATERAL LATERAL FLEXION (≈29º)
SHOULDER AT 90º ABDUCTION AND EXTERNAL ROTATION; ELBOW IN FLEXION (≈81º; FOREARM SUPINATED)
- 3.4 (0.9)
BROCHWICZ ET AL
11 #
N=11 (5♂+ 6♀) AGE=25.6 ±2.3Y
CERVICAL LATERAL GLIDE AT C5/C6 (TRANSLATIONAL MOVEMENT AWAY FROM THE SIDE TO BE TESTED)
SHOULDER AT 30º ABDUCTION, DEPRESSION AND EXTERNAL ROTATION; ELBOW IN FULL EXTENSION, FOREARM IN FULL SUPINATION
MIDDLE FOREARM
3.3 0.8
DISTAL FOREARM
2.5 0.6
CERVICAL CONTRALATERAL LATERAL FLEXION
MIDDLE FOREARM
2.3 0.3
DISTAL FOREARM
1.9 0.6
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
32
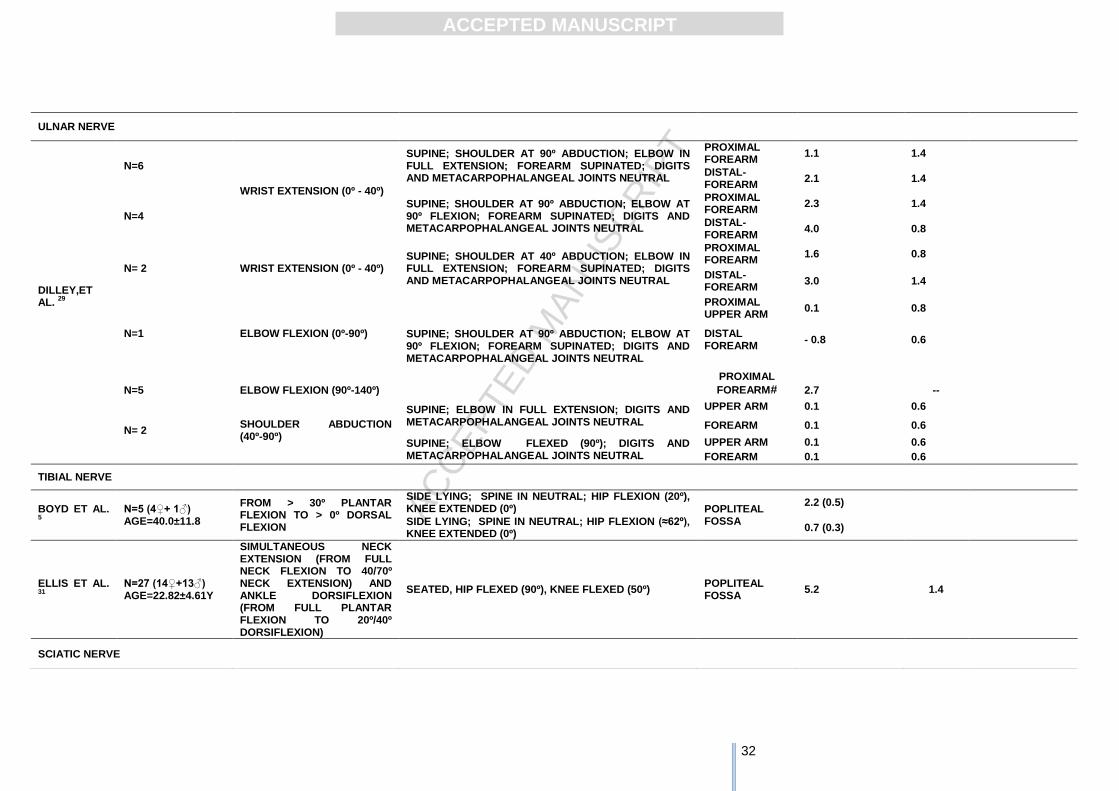
ULNAR NERVE
DILLEY,ET AL.
29
N=6
WRIST EXTENSION (0º - 40º)
SUPINE; SHOULDER AT 90º ABDUCTION; ELBOW IN FULL EXTENSION; FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
PROXIMAL FOREARM
1.1 1.4
DISTAL-FOREARM
2.1 1.4
N=4 SUPINE; SHOULDER AT 90º ABDUCTION; ELBOW AT 90º FLEXION; FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
PROXIMAL FOREARM
2.3 1.4
DISTAL-FOREARM
4.0 0.8
N= 2 WRIST EXTENSION (0º - 40º) SUPINE; SHOULDER AT 40º ABDUCTION; ELBOW IN FULL EXTENSION; FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
PROXIMAL FOREARM
1.6 0.8
DISTAL-FOREARM
3.0 1.4
N=1 ELBOW FLEXION (0º-90º) SUPINE; SHOULDER AT 90º ABDUCTION; ELBOW AT 90º FLEXION; FOREARM SUPINATED; DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
PROXIMAL UPPER ARM
0.1 0.8
DISTAL FOREARM
- 0.8 0.6
PROXIMAL
FOREARM# 2.7 -- N=5
ELBOW FLEXION (90º-140º)
N= 2 SHOULDER ABDUCTION (40º-90º)
SUPINE; ELBOW IN FULL EXTENSION; DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
UPPER ARM 0.1 0.6
FOREARM 0.1 0.6
SUPINE; ELBOW FLEXED (90º); DIGITS AND METACARPOPHALANGEAL JOINTS NEUTRAL
UPPER ARM 0.1 0.6
FOREARM 0.1 0.6
TIBIAL NERVE
BOYD ET AL. 5
N=5 (4♀+ 1♂) AGE=40.0±11.8
FROM > 30º PLANTAR FLEXION TO > 0º DORSAL FLEXION
SIDE LYING; SPINE IN NEUTRAL; HIP FLEXION (20º), KNEE EXTENDED (0º) POPLITEAL
FOSSA
2.2 (0.5)
SIDE LYING; SPINE IN NEUTRAL; HIP FLEXION (≈62º), KNEE EXTENDED (0º)
0.7 (0.3)
ELLIS ET AL. 31
N=27 (14♀+13♂) AGE=22.82±4.61Y
SIMULTANEOUS NECK EXTENSION (FROM FULL NECK FLEXION TO 40/70º NECK EXTENSION) AND ANKLE DORSIFLEXION (FROM FULL PLANTAR FLEXION TO 20º/40º DORSIFLEXION)
SEATED, HIP FLEXED (90º), KNEE FLEXED (50º) POPLITEAL FOSSA
5.2 1.4
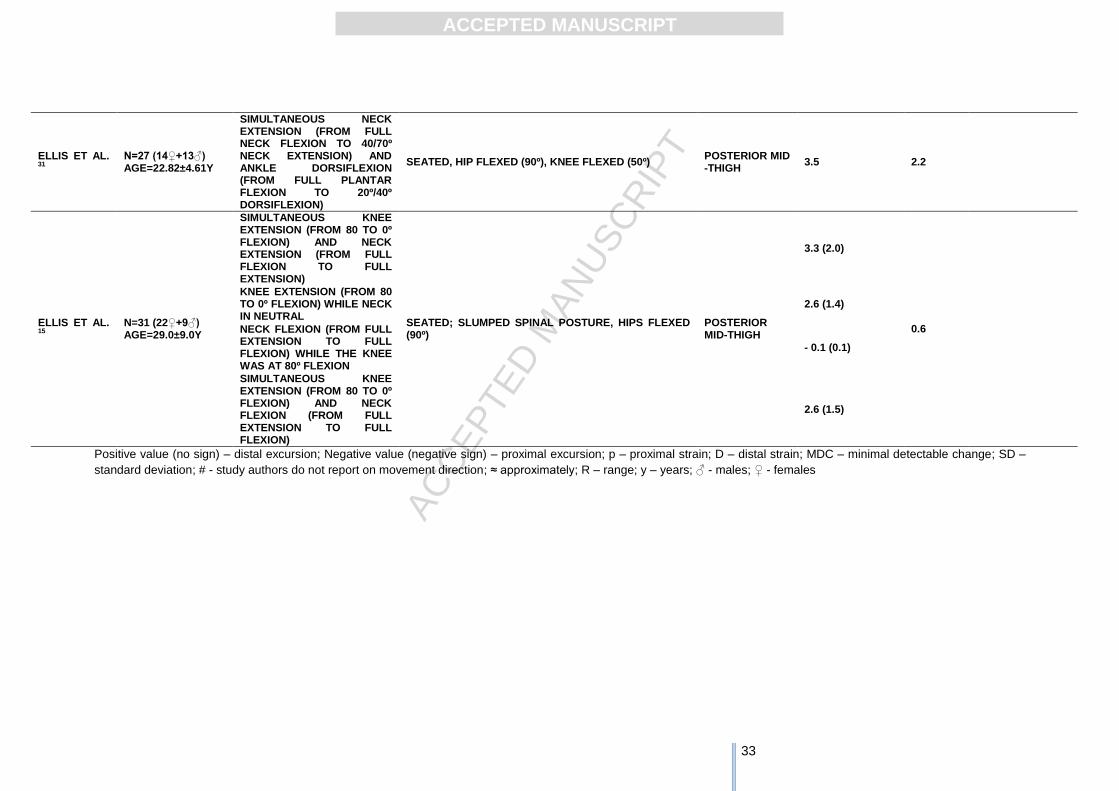
SCIATIC NERVE
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
33
Positive value (no sign) – distal excursion; Negative value (negative sign) – proximal excursion; p – proximal strain; D – distal strain; MDC – minimal detectable change; SD –
standard deviation; # - study authors do not report on movement direction; ≈ approximately; R – range; y – years; ♂ - males; ♀ - females
ELLIS ET AL. 31
N=27 (14♀+13♂) AGE=22.82±4.61Y
SIMULTANEOUS NECK EXTENSION (FROM FULL NECK FLEXION TO 40/70º NECK EXTENSION) AND ANKLE DORSIFLEXION (FROM FULL PLANTAR FLEXION TO 20º/40º DORSIFLEXION)
SEATED, HIP FLEXED (90º), KNEE FLEXED (50º) POSTERIOR MID -THIGH
3.5 2.2
ELLIS ET AL. 15
N=31 (22♀+9♂) AGE=29.0±9.0Y
SIMULTANEOUS KNEE EXTENSION (FROM 80 TO 0º FLEXION) AND NECK EXTENSION (FROM FULL FLEXION TO FULL EXTENSION)
SEATED; SLUMPED SPINAL POSTURE, HIPS FLEXED (90º)
POSTERIOR MID-THIGH
3.3 (2.0)
0.6
KNEE EXTENSION (FROM 80 TO 0º FLEXION) WHILE NECK IN NEUTRAL
2.6 (1.4)
NECK FLEXION (FROM FULL EXTENSION TO FULL FLEXION) WHILE THE KNEE WAS AT 80º FLEXION
- 0.1 (0.1)
SIMULTANEOUS KNEE EXTENSION (FROM 80 TO 0º FLEXION) AND NECK FLEXION (FROM FULL EXTENSION TO FULL FLEXION)
2.6 (1.5)
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
34
Highlights
Overall mean gliding varies between virtually no gliding to 12.5 mm
Gliding is greatest proximal to the moving joint
Nerves glide towards the moving joint when the nerve bed is elongated and
away from the moving joint when the nerve bed is shortened
When there is only one moving joint: movements that elongate the nerve bed
seem to increase nerve gliding
When there are two moving joints moving simultaneously: combinations of joint
movements that elongate the nerve bed at one end and shorten it at the other
end (sliding techniques) seem to promote the greatest nerve excursion





























