Embed Size (px)
Citation preview

Question: Should genome sequencing of multiple oncogenes surplant BRAF V600
mutation testing by an FDA approved test?
Answer: Yes
Jeffrey A Sosman MDIngram Chair for Cancer Research- Professor of Medicine,
Director, Melanoma Program

Why Melanoma? • 2012- Target therapy
– Therapy for BRAFV600E melanoma
– Therapy for CKIT mutated melanoma (exon 11 mutations)
• Other BRAF mutations- V600K,M,R,D,E’ (20% of V600 mutations), L597 mutations
• Expansion in NRAS melanoma 15-20% of all melanoma- targeted therapy in development– MEK inhibitor+AKT inhibitor, MEK inhibitor+CDK4 inhibitor
• Expansion into alternate genes- NF1, MEK1, MEK2, HRAS, CRAF (all components of MAP kinase pathway)
• RAC1, PPP6C, GRIN2A, targets?? Or modulating• Other mutations which are activating same genes
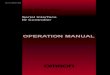
Melanoma is Comprised of Clinically Relevant Molecular Subsets
Curtin et al. NEJM 2005; Curtin et al. JCO 2006
Arising from SkinWithout Chronic
Sun Damage
Arising from SkinWith Chronic Sun Damage
Arising from MucosalSurfaces
Arising fromAcral
Surfaces
50% BRAF20% NRAS
1-2% KIT
10% BRAF10% NRAS
5% KIT
5% BRAF15% NRAS
20% KIT
15% BRAF15% NRAS
15%KIT
Goals of the VICC PCMI
• To establish ‘reflex’ testing of ‘common’ clinically relevant genetic alterations in lung cancers and melanomas.
• To develop a clinically-applicable high-throughput molecular genotyping facility for ‘rarer’ genetic variants.
• To develop bioinformatic algorithms to report genetic results in the electronic medical record in ways that are clinically useful for practicing oncologists.
– Collaboration among Depts of Medicine, Pathology, BioInformatics, and VICC
– Sounds simple, but…requires high level of collaboration/coordination

S37p.S37F c.110C>Tp.S37Y c.110C>A
S45p.S45P c.133T>Cp.S45F c.134C>Tp.S45Y c.134C>A
Q209p.Q209P c.626A>Cp.Q209L c.626A>Tp.Q209R c.626A>G
GNAQ
Position AA mutant Nucleotide mutant
G12
p.G12C c.34G>Tp.G12S c.34G>Ap.G12R c.34G>Cp.G12V c.35G>Tp.G12A c.35G>Cp.G12D c.35G>A
G13
p.G13A c.38G>Cp.G13V c.38G>Tp.G13R c.37G>Tp.G13D c.38G>A
Q61
p.Q61E c.181C>Gp.Q61H c. 183A>Tp.Q61H c.183A>Cp.Q61L c.182A>Tp.Q61L c.182_183AA>TGp.Q61K c.181C>Ap.Q61P c.182A>Cp.Q61R c.182A>Gp.Q61R c.182_183AA>GG
NRAS
CTNNB1
W557p.W557R c.1669T>Cp.W557R c.1669T>A
V559p.V559A c.1676T>Cp.V559D c.1676T>A
L576 p.L576P c.1727T>CK642 p.K642E c.1924A>GD816 p.D816H c.2446G>C
KIT
Q209p.Q209P c.626A>Cp.Q209L c.626A>T
GNA11
Position AA mutant Nucleotide mutant
V600
p.V600R c.1798_1799GT>AGp.V600K c.1798_1799GT>AAp.V600E c.1799T>Ap.V600E c.1799_1800TG>AAp.V600M c.1798G>Ap.V600G c.1799T>Gp.V600D c.1799_1800TG>AT
BRAF
43 Somatic Point Mutations in 6 Genes Relevant to Targeted Therapy in Melanoma
43 Somatic Point Mutations in 6 Genes Relevant to Targeted Therapy in Melanoma

BRAF _V6001799T>A/G
NRAS_Q61182A>T/C/G
NRAS_G13 (R)38 G>A/T/C
BRAF_V600 (R)1800 G>A/T
KIT_V5591676 T>C/A
B-CAT_S45 (R)133 T>C
NRAS_G1235 G>T/C/A
BRAF _V600 (R)1799 T> G/A
B-CAT_S37110C>A/G/T
B-CATS45 (R)134R C>A/T
BRAF_V6001798G>A
NRAS_G13 (R)37G>T/C
NRAS_Q61 (R)183 A>G/T/C
NRAS_G12 (R)34G>A/T/C
KIT_K6421924A>G
NRAS_Q61181C>A/G GNA11_Q209 (R)
626A/T/C
KIT_W5571669T>A/C
KIT_L5761727T>C
KIT_D8162446G>C
GNAQ_Q209626A>T/C/G
Fig 1B

First 150 Patients: 20% of BRAF V600 Mutations Would Have Been Missed by Allele-Specific PCR
Lovly, Dahlman, Fohn, Su et al ‘12

Vanderbilt-Ingram Cancer Center
Gene # of metastatic cases # patients placed on a
genotype-driven clinical trial (%) BRAF 32 12 (38%)
CTNNB1 1* 1 (100%)
GNAQ/GNA11 6 3 (50%)
KIT 1 1 (100%)
NRAS 15 4 (27%)
No mutation detected 28 N/A
Total cases 82 21/54 (39%)
* This CTNNB1 mutation (CTNNB1 S45P) occurred concurrently with an NRAS Q61L mutation.
First 150 Patients: 40% of Pts with Mutant Metastatic Disease Genotype-Driven Treatment
Lovly, Dahlman, Fohn, Su et al ‘12

Melanoma SNaPshot genotyping in CLIA Lab (652 samples, from Jul 2010 to June 2012)
Distribution of BRAF V600 mutations
Distribution of all mutations detected

Melanoma7/1/2010-11/1/2012
• 759 Specimens– 65% specimens with mutation detected– 16 specimens with 2 mutations– 3 specimens with 3 mutations
• 715 patients– 64% patients with mutation detected

11
Vemurafenib(PLX4032)

100
90
80
70
60
50
40
30
20
10
0
Ove
rall
surv
ival
(%
)
0 6 12 18 24
Vemurafenib (n=337)
Median f/u 12.5 months
Dacarbazine (n=338)
Median f/u 9.5 months
338
337
173
280
79
178
24
44
0
1
244
326
111
231
50
109
4
7
9.7 13.6
Overall survival (February 01, 2012 cut-off) censored at crossover
Hazard ratio 0.70 (95% CI: 0.57–0.87)p<0.001 (post-hoc)
Time (months)No. at riskDacarbazine
Vemurafenib
15.9
BRIM2

c-KIT Mutations in Melanoma• 4q12
– Selectively amplified in acral/mucosal– Candidate genes → c-Kit amplifications
→ point mutations
• C-Kit by Subtype– Acral 11% Mt 25% Amp– Mucosal 21% Mt 29%
Amp– Cutaneous
• +CSD 1-18% Mt 6% Amp
• C-Kit: Melanoma vs GIST– Point mutations
– ↑ Exon 13 & 17 mutations
– Amplified wild-type c-KIT
– Lack of 2ndary mutations
Woodman, BCP, 2010

Phase II Studies of Imatinib 400 mg BID in Advanced Melanoma
kit
c-abl
PDGFR-α
PDGFR-β
Imatinib
Three “large” studies have been embarked upon include both KIT mutated and amplified
Hodi- DFCC central with imatinib, sunitinib, or nilotinib for imatinib fail Carvajal- MSKCC central with imatinib Guo-. Peking Univ, Beijing, China- imatinib

. Treatment Response Over Time by Melanoma Subtype and Genetic Alteration of KIT
Carvajal, R. D. et al. JAMA 2011;305:2327-2334
Copyright restrictions may apply.

Kit Inhibition in Melanoma
Kit Inhibitors can produce dramatic effects in patients with melanomas containing a variety of C-kit mutations
Kit mutations are seen in 2% of all melanomas Role of Kit inhibition in Kit amplified tumors has yet to
be established Multiple studies currently underway
Imatinib, sunitinib, dasatinib, nilotinib International Phase II trial (nilotinib )- comp[leted
Exciting, but not the answer for the majority of patients with melanoma

Vanderbilt-Ingram Cancer Center
Index Case: Using NGS to Find Novel Drivers
• 75 year old male presented with ulcerated right ear melanoma resected
• 4 mos later – local recurrence re-resection and radiation; BRAF V600E and KIT mutations not detected
• 12 mos later – widespread mets palliative thyroidectomy; no mutations detected by SNaPshot
• Whole genome sequencing performed on thyroid metastasis (90% tumor) and matched normal blood
Dahlman, Xia, Hutchinson et al ‘12

WGS Analysis of “Pan-Negative” Melanoma
GAIIxPaired-endSAMtoolsPindelCRESTFREEC
Dahlman, Xia, Hutchinson et al ‘12

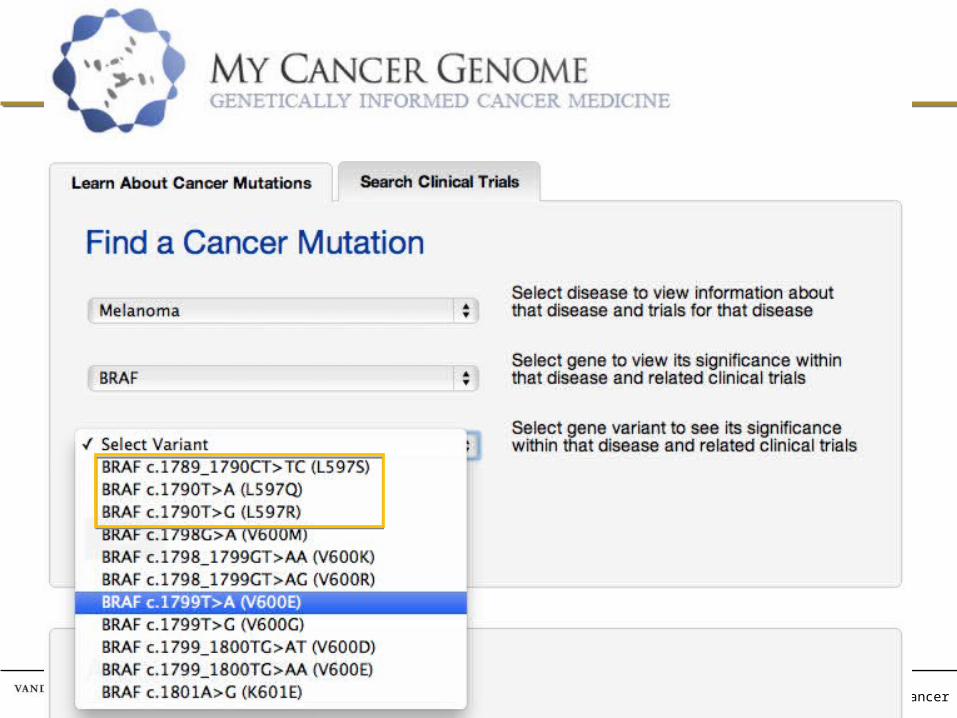
• Melanoma SNaPshot Negative Patient• Whole-genome sequencing BRAF L597R• Sensitive to MEK inhibition in vitro
SNaPshot Limitation Example:Melanoma Patient with BRAF L597 Mutation
Dahlman, Xia, Hutchinson et al, Cancer Discov, 2012)
Patient with BRAF L597S, treated with TAK-733

Vanderbilt-Ingram Cancer Center
Of 49: 2 L597,1 D594, 1 K601(8%)
8% of “Pan-Negative” Samples Harbor non-V600E BRAF Exon 15 Mutations
Melanoma Panel: 538 Samples
7/1/10-12/31/11
Dahlman, Xia, Hutchinson et al ‘12
Cosmic: 0.1% of BRAF mutations

Mutations in the BRAF gene
PRESENTED BY:

MEK 162: Best percentage change from baseline and best overall response (NRAS mut)
*Patients with missing best % change from baseline and unknown overall response are not included.
N=28*Progressive Disease (PD)
Stable Disease (SD)
Partial Response (PR)
Unconfirmed PR
45 mg NRAS
Ongoing pts
Ascierto, Berking, Agarwala et al. ASCO 2012
Response rate: 21% (6 of 28 pts)Disease control rate: 68%
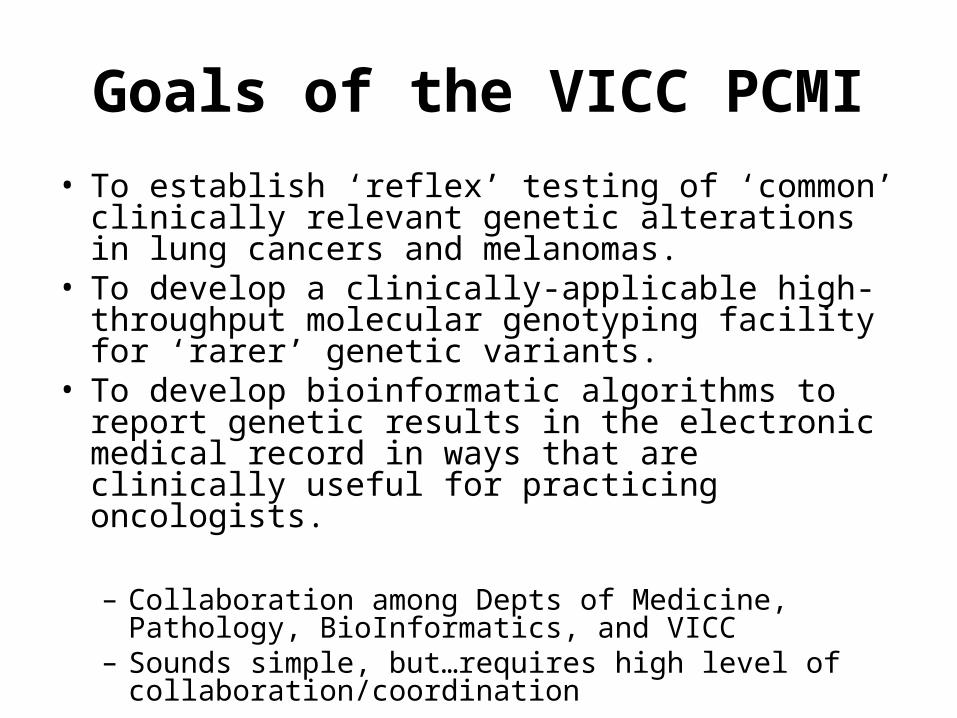
Actionable Mutations- MAPKinase Pathway


Vanderbilt-Ingram Cancer Center
Summary
• Routine multiplex mutational profiling of melanoma with a disease-specific panel– Identifies patients with clinically relevant driver
mutations– Enables genetically-informed cancer medicine in the
clinic– Facilitates clinical trial enrollment– Allows for rapid discovery of potentially targetable
novel drivers in ‘pan-negative’ cases• BRAF L597 mutations and MEK inhibitors

Vanderbilt-Ingram Cancer Center
16 CancersALL
ALCLBasal Cell Carcinoma
BreastColorectal
GastricGISTIMTLung
MedulloblastomaMelanoma
NeuroblastomaOvarian
RhabdomyosarcomaThymicThyroid
24 Genes
271 Disease-Gene-Variant Relationships
16 CancersALL
ALCLBasal Cell Carcinoma
BreastColorectal
GastricGISTIMTLung
MedulloblastomaMelanoma
NeuroblastomaOvarian
RhabdomyosarcomaThymicThyroid
24 Genes
271 Disease-Gene-Variant Relationships
Vanderbilt-Ingram Cancer Center

More Comprehensive Profiling with Illumina MiSeq
Illumina.com
Amplicon Target Enrichment
1000x read coverageAutomated Alignment & Analysis

“Vanderbilt Cancer Panel” for MiSeq
Panel 1 = 34 genesTargets = 594 (exons)Target bp = 195838 bp# Amplicons = 1494 (max 1536)Coverage = 95%Low-Scoring Targets = 13
AKT1 IDH1 NF1ALK IDH2 NF2BRAF KIT NRASCDK4 KRAS PDGFRADDR2 MAP2K1 PIK3CAEGFR MAP2K2 PTENERBB2 MET RICTORFGFR1 MLH1 RPTORFGFR2 MLH3 SMOFGFR3 MSH2 TSC1GNA11 MTOR TSC2GNAQ
Panel 2 = 32 genesTargets = 457 (exons)Target bp = 210570 bp# Amplicons = 1448 (max 1536)Coverage = 93%Low-Scoring Targets = 13
AKT2 JAK3 NTRK3AKT3 KDR PTCH1ARAF MCL1 PTCH2BCL2 MYC RAF1BCL2L1 MYCL1 RB1ERBB3 MYCN RETERBB4 NOTCH1 SMAD4FGFR4 NOTCH2 STK11HRAS NOTCH3 TP53
JAK1 NTRK1 IGF1RJAK2 NTRK2
• Design: Illumina Design Studio• Targets: All exons of 66 genes

• Validate with samples with known mutations:– FFPE Patient Tissue– Frozen Patient Tissue– Cell Lines
• Expand to SNaPshot-negatives/unknowns
• Design a capture method/panel for fusion genes
• Now seeking interesting clinical samples! Please contact me ([email protected])
• Implement into Clinical Molecular Diagnostics Lab??? (Cindy Vnencak-Jones)
Vanderbilt Cancer Panel Plans
The major issues critical to personalized cancer care in melanoma
• Acquired resistance to BRAF inhibitors- – mechanisms and overcoming resistance
• Targeting other mutations (NRAS) effectively with new or old drugs
• Defining new genetic mutations, amplifications, or translocations
• Need for both clinical and translational collaboration to speed up the discoveries needed for clinical progress
• Transmitting genetic information to the oncologist in a clinically relevant language