Embed Size (px)
DESCRIPTION
R isk factors for maternal mortality in Delhi slums: A community-based case-control study. Aggarwal A, Pandey A, Bhattacharya BN. Risk factors for maternal mortality in Delhi slums: A community-based case-control study. Indian J Med Sci 2007;61:517-26. Learning objectives. - PowerPoint PPT Presentation
Citation preview
RISK FACTORS FOR MATERNAL MORTALITY IN DELHI SLUMS: A COMMUNITY-BASED CASE-CONTROL STUDY.
Aggarwal A, Pandey A, Bhattacharya BN. Risk factors for maternal mortality in Delhi slums: A community-based case-
control study. Indian J Med Sci 2007;61:517-26

LEARNING OBJECTIVES To learn about maternal mortality indicators.
INTRODUCTION: In order to develop, implement and evaluate
policy for reducing maternal mortality, it is essential to study risk factors.
Pregnancy complications and childbirth-related complications are the major causes.
MMR in India is far from the desired level of 100 by 2012 set by the National Rural Health Mission (NRHM) and 109 by 2015 as per millennium development goals (MDG).

OBJECTIVE OF STUDY: To determine the epidemiological risk factors
and its related causes associated with maternal deaths in Delhi slums.
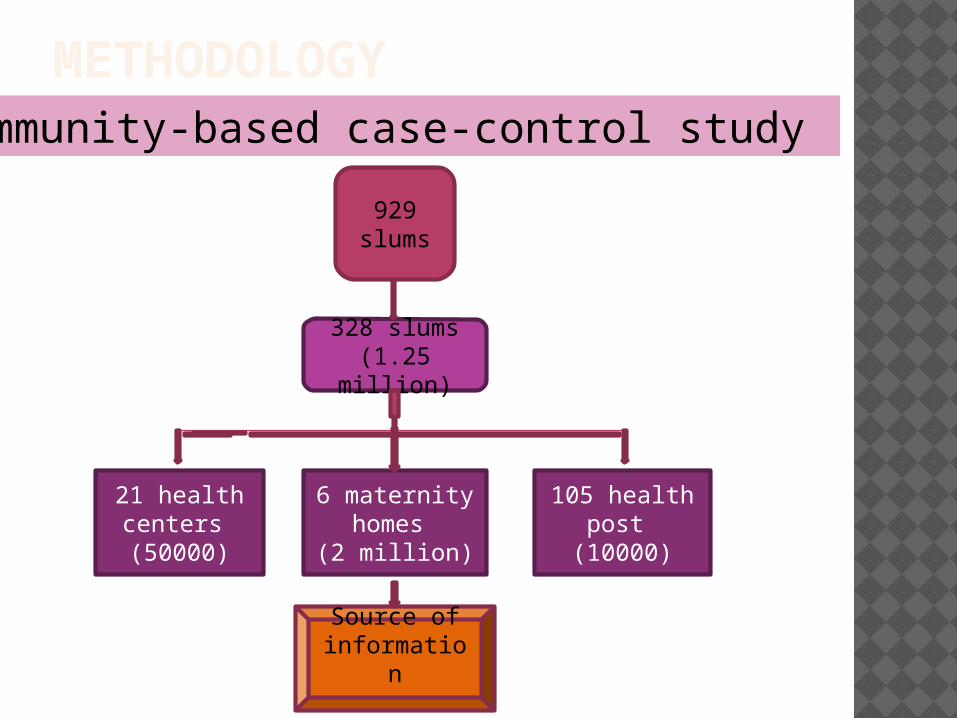
METHODOLOGY
929 slums
328 slums(1.25 million)
21 health centers (50000)
105 health post (10000)
6 maternity homes
(2 million)
Source of information
Community-based case-control study

Definitions of Cases and Controls: Case : A woman who was pregnant and whose
pregnancy's outcome was a live birth but the woman died within 42 days of delivery.
Control: A woman who was pregnant and whose pregnancy's outcome was a live birth and the woman was surviving at the time of survey.
Method of identifying Cases and Controls: Cases: Snowball-sampling method was used to identify
the maternal deaths (cases) in the community and hospital recods.
Controls: Circular systematic random sampling procedure was used to select the controls from the same area where a maternal death was found.
Exclusion criteria: pregnancy outcome SB/abortion.
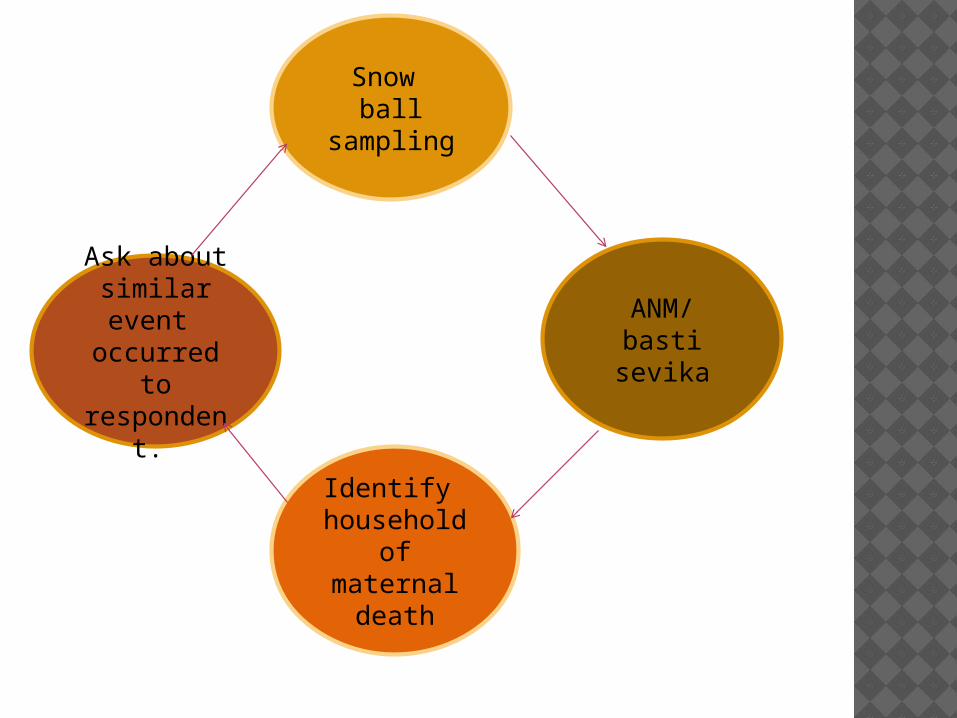
Identify household of
maternal death
Ask about similar event occurred to respondent.
ANM/ basti sevika
Snow ball sampling
Circular systematic random sampling for selection of controls:
1 case= 3 controls
1.1Total no of households with a live birth/ no of controls(384)
1.2 controls were found i.e. 3 times cases .
Then every kth household of live birth was selected as control.
STUDY POPULATION:
131
70(61)
cases
393
384(9)
controls
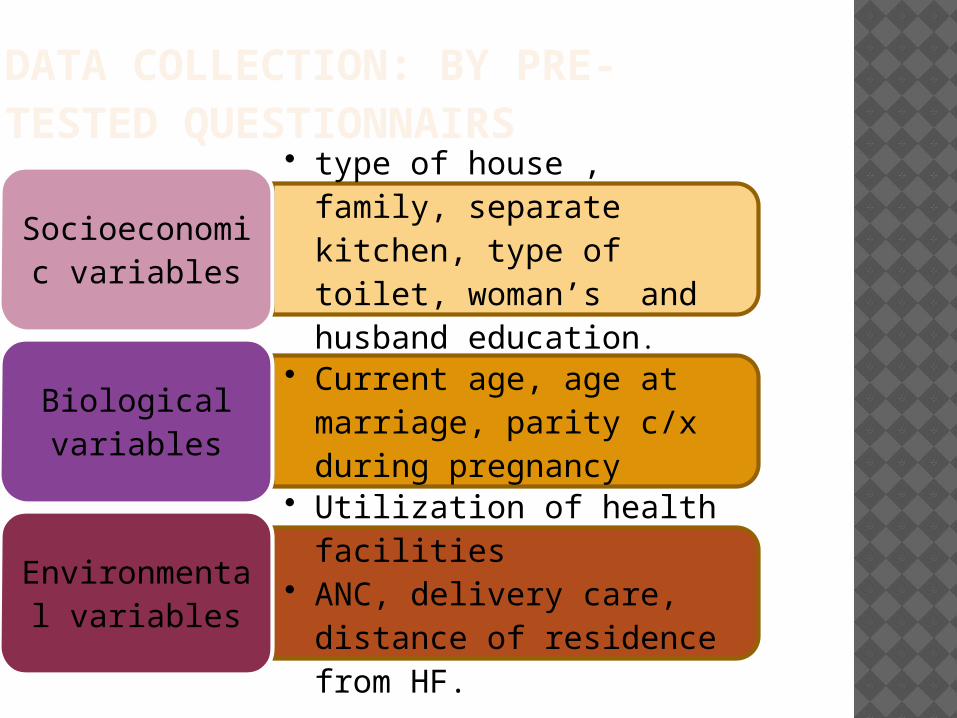
DATA COLLECTION: BY PRE-TESTED QUESTIONNAIRS
• type of house , family, separate kitchen, type of toilet, woman’s and husband education.
Socioeconomic variables
• Current age, age at marriage, parity c/x during pregnancy
Biological variables
• Utilization of health facilities • ANC, delivery care, distance of
residence from HF.
Environmental variables

RESULTS
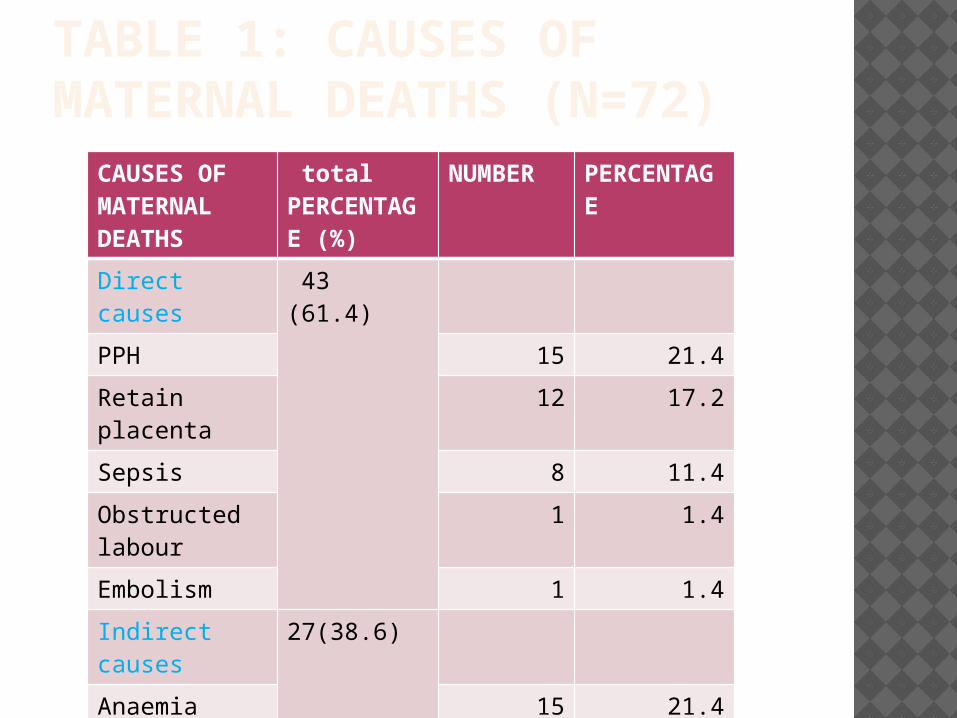
TABLE 1: CAUSES OF MATERNAL DEATHS (N=72)
CAUSES OF MATERNAL DEATHS
total PERCENTAGE (%)
NUMBER PERCENTAGE
Direct causes 43 (61.4)
PPH 15 21.4
Retain placenta
12 17.2
Sepsis 8 11.4
Obstructed labour
1 1.4
Embolism 1 1.4
Indirect causes
27(38.6)
Anaemia 15 21.4
Post op 6 8.6
Other 12 17.2
TABLE 2
No significant difference was found in household characteristics.

TABLE 3:SE & REPRODUCTIVE CHARACTERSTICSVariables Case (%)
(n=70)Control( %)(n=384)
P Value
Education Level
Illiterate 54 (77.1) 234(60.9) 0.005
Literate 16(22.9) 150(39.1) Ns
Husband’s Education
Illiterate 31(44.3) 113(29.5) 0.007
Literate 39(55.7) (70.5) Ns
Type of Family
Nuclear 40(57.1) 262(68.2) 0.03
Joint 30(42.9) 122(31.8) Ns
Current Age
> 35 13(18.6) 26(6.8) 0.0006
Parity
2 10(14.3) 106(27.6) 0.0107
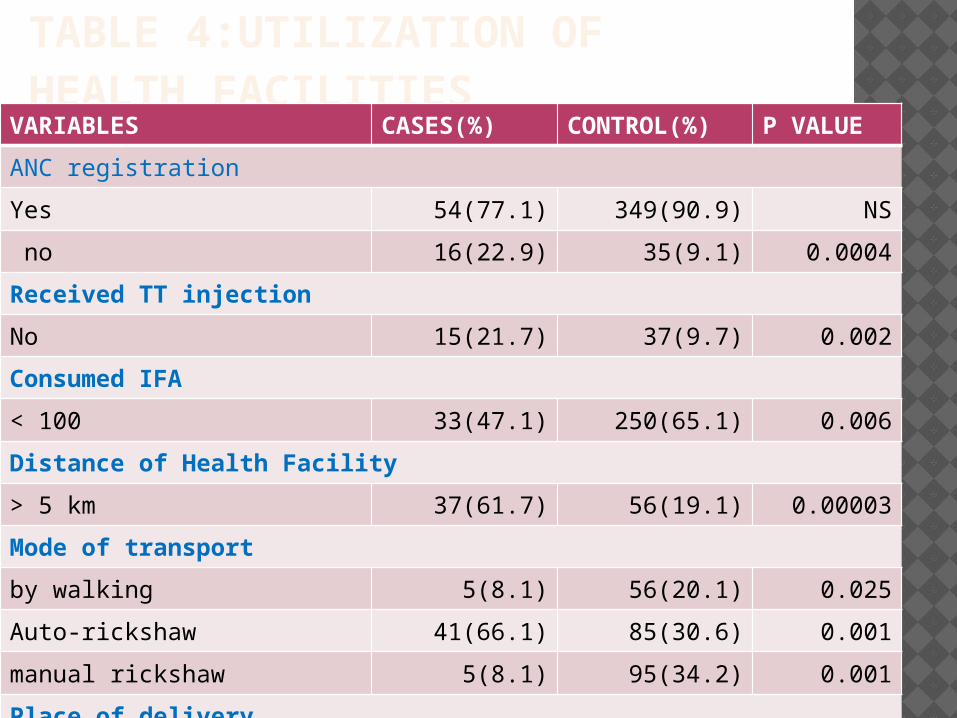
TABLE 4:UTILIZATION OF HEALTH FACILITIES
VARIABLES CASES(%) CONTROL(%) P VALUE
ANC registration
Yes 54(77.1) 349(90.9) NS
no 16(22.9) 35(9.1) 0.0004
Received TT injection
No 15(21.7) 37(9.7) 0.002
Consumed IFA
< 100 33(47.1) 250(65.1) 0.006
Distance of Health Facility
> 5 km 37(61.7) 56(19.1) 0.00003
Mode of transport
by walking 5(8.1) 56(20.1) 0.025
Auto-rickshaw 41(66.1) 85(30.6) 0.001
manual rickshaw 5(8.1) 95(34.2) 0.001
Place of delivery
home 39(55.7) 268(69.8) 0.02
hospital 31(44.3) 116(30.2) 0.02

TABLE 5: C/X DURING PREG & DELIVERYVARIABLE CASE(%) CONTROL
(%)P VALUE
Complications during pregnancy
Anaemia 33(47.1) 27(7.0) <0.001
High BP 3(4.3) 4(1) NS
Jaundice 6(8.6) 5(1.3) <0.001
Fever 13(18.6) 50(13.0) 0.1062
Abn +nt of child 14(20.0) 20(5.2) <0.001
Complications during delivery
Exce. bleeding 5(7.1) 2(0.5) <0.001
Retained placenta 5(7.1) 1(0.3) <0.001
Delivery by untrained dai 37(94.9) 194(72.4) <0.001
Institutional death 47(67.2)
Death <24 hrs 23(48.9)
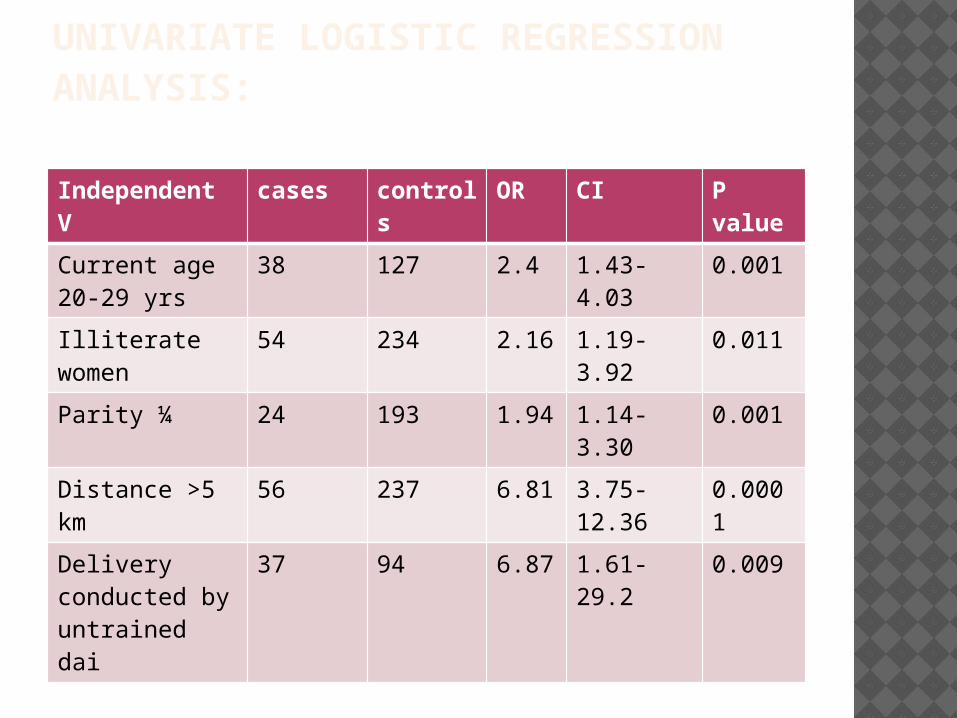
UNIVARIATE LOGISTIC REGRESSION ANALYSIS:
Independent V cases controls OR CI P value
Current age 20-29 yrs
38 127 2.4 1.43-4.03 0.001
Illiterate women 54 234 2.16 1.19-3.92 0.011
Parity ¼ 24 193 1.94 1.14-3.30 0.001
Distance >5 km 56 237 6.81 3.75-12.36 0.0001
Delivery conducted by untrained dai
37 94 6.87 1.61-29.2 0.009
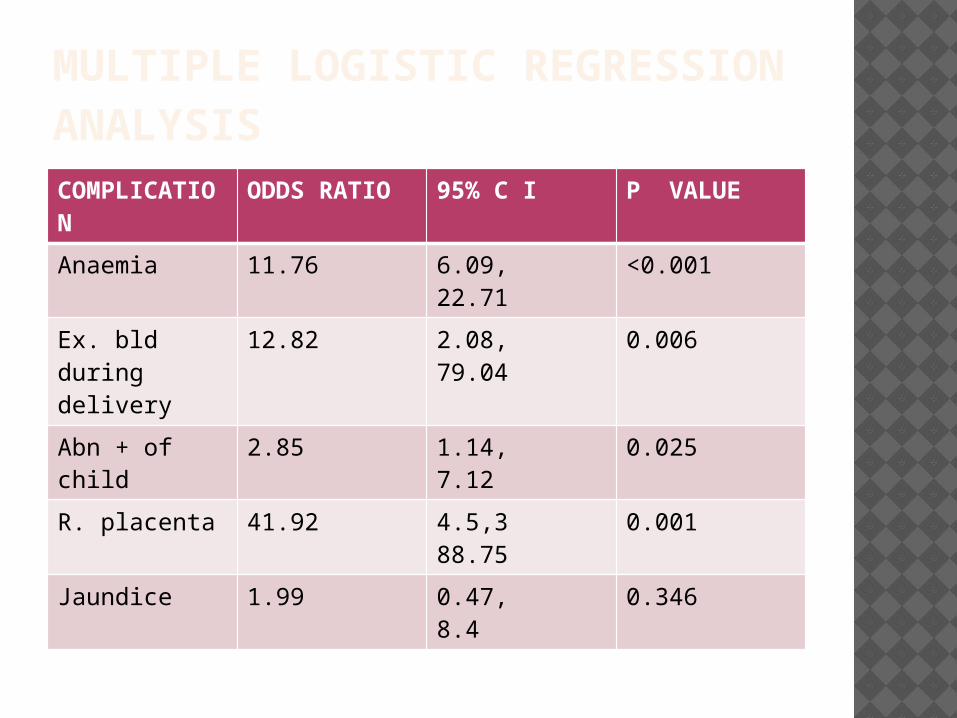
MULTIPLE LOGISTIC REGRESSION ANALYSISCOMPLICATION
ODDS RATIO 95% C I P VALUE
Anaemia 11.76 6.09, 22.71 <0.001
Ex. bld during delivery
12.82 2.08, 79.04 0.006
Abn + of child 2.85 1.14, 7.12 0.025
R. placenta 41.92 4.5,3 88.75 0.001
Jaundice 1.99 0.47, 8.4 0.346
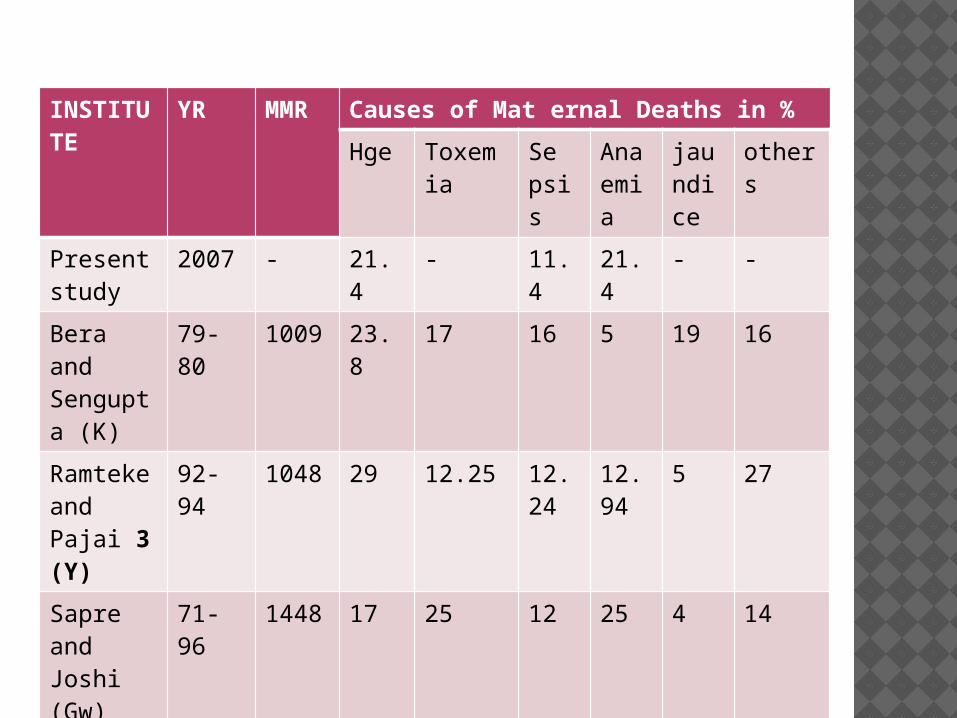
RESULTS FROM OTHER STUDIES :INSTITUTE
YR MMR Causes of Mat ernal Deaths in %
Hge Toxemia Se psis
Anaemia
jaundice
others
Present study
2007 - 21.4 - 11.4 21.4 - -
Bera and Sengupta (K)
79-80 1009 23.8 17 16 5 19 16
Ramteke and Pajai 3 (Y)
92-94 1048 29 12.25 12.24
12.94
5 27
Sapre and Joshi (Gw)
71-96 1448 17 25 12 25 4 14
Pal and ray (WB)
94-04 623 9.7 50 18 4 2 15
SRS 1998 540(NFHS)
30 8 16 19 - 8
WHO report
2005 - 25 - 15 20 - 8

DISCUSSION:
Use of a cost-effective snowball-sampling technique. The major direct causes - PPH, F.B. retained placenta
and sepsis. As per the report of the sample registration system
(SRS) –hemorrhage 38%, which is much higher than this study’s estimate.
Hypertensive disorders are one of the causes of maternal deaths, our study did not find any such case.
Maternal deaths d/t retained placenta was found to be marginally higher than those reported elsewhere. Anemia -major cause of maternal death in the present study

CONT….. Entire study population was from urban slums,
socioeconomic characteristics do not show statistically significant differences between cases and controls.
Investing in training of untrained dies should be considered by policy makers and donor agencies.
A high proportion of maternal deaths occurred in hospital set up - deliveries were conducted at home by untrained dais and were rushed to a hospital at the last minute.

CONCLUSION: Mass education about the importance of
antenatal registration and regular ANC checkups.
Focus on training of dais. Encouragement for institutional
deliveries to reduce maternal mortality at the community level.

THANKS…….