Embed Size (px)
Citation preview

This article was downloaded by: [University of Toronto Libraries]On: 09 October 2014, At: 03:23Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH,UK
Ethnicity & HealthPublication details, including instructions for authorsand subscription information:http://www.tandfonline.com/loi/ceth20
Racial Differences in Symptomsand Complications in Adultswith Type 2 Diabetes MellitusJoseph C. Konen , John H. Summerson , Ronny A. Bell& Laura G. CurtisPublished online: 01 Jul 2010.
To cite this article: Joseph C. Konen , John H. Summerson , Ronny A. Bell & Laura G.Curtis (1999) Racial Differences in Symptoms and Complications in Adults with Type 2Diabetes Mellitus, Ethnicity & Health, 4:1-2, 39-49, DOI: 10.1080/13557859998182
To link to this article: http://dx.doi.org/10.1080/13557859998182
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all theinformation (the “Content”) contained in the publications on our platform.However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness,or suitability for any purpose of the Content. Any opinions and viewsexpressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of theContent should not be relied upon and should be independently verified withprimary sources of information. Taylor and Francis shall not be liable for anylosses, actions, claims, proceedings, demands, costs, expenses, damages,and other liabilities whatsoever or howsoever caused arising directly orindirectly in connection with, in relation to or arising out of the use of theContent.
This article may be used for research, teaching, and private study purposes.Any substantial or systematic reproduction, redistribution, reselling, loan,

sub-licensing, systematic supply, or distribution in any form to anyone isexpressly forbidden. Terms & Conditions of access and use can be found athttp://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014

Ethnicity & Health 1999; 4(1/2): 39±49
Racial Differences in Symptoms and Complications inAdults with Type 2 Diabetes Mellitus
JOSEPH C. KONEN MD, MSPH,1 JOHN H. SUMMERSON MS,2 RONNY A.BELL PHD, MS3
AND LAURA G. CURTIS PA2
1Department of Family Medicine, Carolinas Medical Center, Charlotte, NC28232, USA. 2Department of Family and Community Medicine and 3Department
of Public Health Sciences, Wake Forest University School of Medicine,Winston-Salem, NC 27157, USA
ABSTRACT
Objective. To compare the frequency of common symptoms and complications betweenAfrican- and white American adults with type 2 diabetes mellitus in a primary caresetting, and to examine associations of these conditions with glycemic control.
Design. Three hundred and four adults with type 2 diabetes participated in thiscross-sectional analysis; 142 of whom were African-Americans. Patients were recruitedfrom a family practice ambulatory care unit and a community health center.
Results. Both male and female African-Americans had higher mean diastolic bloodpressure and poorer metabolic control than their white counterparts. After adjustmentfor diabetes duration, glycosylated hemoglobin and diastolic blood pressure, African-American females were signi® cantly more likely to experience constipation and hyper-tension but less likely to experience chest pain, claudication, peripheral neuropathy orhave peripheral vascular disease. Among male subjects, African-Americans weresigni® cantly more likely to experience blurred vision and hypertension but less likely tohave peripheral atherosclerotic disease. Poor glycemic control was more stronglyassociated with the occurrence of common diabetic symptoms in African-Americansubjects.
Conclusions. Both African- and white Americans with type 2 diabetes are likely toexperience a wide variety of symptoms and vascular complications. African-Americansubjects appear more likely than whites to experience symptoms related to glycemiccontrol but less likely to have, or experience symptoms and complications of, cardiovas-cular disease. That nearly half of these subjects seen in a primary care setting hadmicroalbuminuria suggests that vascular complications are likely to be present in themajority of adults with type 2 diabetes, even in these currently asymptomatic. These® ndings may have implications for screening and preventive strategies for the treatmentof this disease.
Keywords: Diabetes mellitus, African-American , glycemic control , ethnicity .
INTRODUCTION
The prevalence of diabetes mellitus among African-Americans, regardless of gender, isapproximately twice that of white Americans and is increasing even though its preva-
Correspondenc e to: Joseph C. Konen MD MSPH, Department of Family Medicine, Carolinas MedicalCenter , PO Box 32861, Charlotte, NC 28232, USA.
ISSN 1355-7858 (print) ISSN 1465-3419 (online) /99/01/2039-11 Ó 1999 Taylor & Francis Ltd 39
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014

J. C. KONEN ET AL.40
lence has remained fairly constant for whites over the last decade.1 Diabetes presentlyaffects more than 10.3 million Americans; 1.4 million of whom are African-American,and contributes substantially to the development of premature mortality and morbidityfrom cardiovascular diseases. This disease is also the leading cause of both newblindness and end-stage renal disease (ESRD) in the USA.2 Symptoms and otherlimitations imposed by diabetes and its complications are a signi® cant cause of disabilityand have enormous economic impact with total costs for diabetes and its complicationsexceeding 90 billion dollars per year.2
Common diabetic complications such as retinopathy and nephropathy havebeen more frequently examined in white populations, and in subjects with type 1diabetes. These studies show that the prevalence of complications often appearrelated to duration of diabetes and degree of glycemic control and that other co-morbidities such as hypertension may be important in their development. However,there are few reports of the types of symptoms and complications experienced byAfrican-Americans, a population which suffers a disproportionate burden fromthis disease. We compared by race and gender the types and frequencies ofsymptoms and complications experienced by adults with type 2 diabetes in a primarycare setting.
METHODS
All 433 of the adult patients with type 2 diabetes listed in the computerized encounterdatabase of the Family Practice Ambulatory Care Unit of the Wake Forest UniversitySchool of Medicine were invited to a free screening program to determine the prevalenceand risk factors for cardiovascular and renal disease. The recruitment procedures havebeen described previously.3 Two hundred and twenty subjects agreed to participate andcompleted the screening process. Using similar procedures, an additional 84 subjectsfrom a community health clinic were recruited, giving a total of 304 subjects. Of these304 individuals, 142 were African-American. Demographic and clinical data for all studypatients were comparable to our entire Family Practice population of diabetics and didnot differ signi® cantly by age and gender compared to data from type 2 diabetic patientsfrom the State of North Carolina4 and to national data compiled by the Centers forDisease Control (CDC).1
Height and weight data were measured during a physical examination and a bodymass index (BM 5 kg/ht2) was derived for each subject. Blood pressure was measuredon the left arm of subjects after a 5-minute, seated rest. Mean arterial pressure (MAP)was de® ned as (1/3 3 systolic) 1 (2/3 3 diastolic).
Participants were given a written questionnaire asking whether or not during thepast 6 months they had experienced any speci® c symptoms from a list of commoncardiovascular, genitourinary, nervous system, or general diabetic symptoms. Thoseresponding positively were asked how long ago the symptom ® rst appeared. Similarlyall subjects were asked if and when any de® nite co-morbid condition or potentialcomplication from their diabetes ® rst appeared. Either a physician or physicianassistant used a checklist to record categories of signi® cant past histories of complica-tions. A physical examination was performed on each subject, recording all positive® ndings on an objective criteria-based form. Special attention was paid to thoseexamination maneuvers that might detect diabetic vascular complications. The presenceof complications were de® ned if evidence existed on the physical examination to makea diagnosis of a given complication, or if physical signs existed that would verify eachpatient’ s history. Past medical histories were veri® ed through the patient’ s medicalrecords.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014

RACIAL DIFFERENCES IN SYMPTOMS IN NIDDM 41
The following de® nitions were used for speci® c complications or co-morbidities:HypertensionÐ de® ned as either a past history of treatment for hypertension with eitherdiet, exercise, or medication or prior documentation of elevated blood pressures (greaterthan 160 mmHg systolic or 90 mmHg diastolic) on more than one occasion, and anelevated pressure at the time of examination. Atherosclerotic cardiac diseaseÐ historyof classical angina and any abnormal electrocardiogram, signi® cant ® ndings on angiog-raphy, previous coronary artery bypass or angioplasty. Cerebral vascular diseaseÐ his-tory of previous transient ischemic attack and signs of carotid bruits or asymmetricalpulses, or history of completed stroke and presence of neurological abnormality inmemory, verbal, motor or sensory examination. Peripheral vascular diseaseÐ history ofclaudication or asymmetrical or diminished dorsalis pedes, or posterior tibial pulses.Clinical proteinuriaÐ history of excess protein in the urine veri® ed by more than oneoccasion of the ® nding of at least 1 1 protein on dipstick. MicroalbuminuriaÐ urinaryalbumin excretion ratios (UAER) between 0.02 and 0.2 g albumin/g creatinine. Blind-nessÐ a visual abnormality resulting in visual acuity in either eye of less than 20/200.CataractsÐ any cataracts seen on physical examination with indirect ophthalmoscopy orhistory of cataract removal and evidence of iridectomy or arti® cial lens implant.RetinopathyÐ any history of retinopathy, excluding retinal detachment, veri® ed byretinal abnormalities, including retinal laser burns, seen on examination with indirectophthalmoscopy. Since it was dif® cult to adjudicate severity of retinopathy on indirectophthalmoscopy without fundal photographs, all types of retinopathy were collapsed intoone category. Peripheral neuropathyÐ history of glove and stocking numbness in handsand feet and diminished perception of vibration using a vibrating 256 Hz tuning forkapplied to nails of middle ® nger or great toe. In addition, all subjects had fasting blooddrawn for a determination of glucose and glycosylated hemoglobin (HbA1c). UAER wasdetermined from an overnight urinary collection.5
Means and standard deviations were calculated for each study variable. Analyses ofvariance and chi-square procedures were used to evaluate differences in demographicand clinical variables. Logistic regression was used to compare the presence ofsymptoms and complications by race after adjustment for diabetes duration, diastolicblood pressure and HbA1c. These analyses were run separately for males and females.Signi® cance levels of p , 0.05 are used unless otherwise stated. All statistical analyseswere performed using the Statistical Package for the Social Sciences for PersonalComputers (SPSS, Inc., Chicago, IL, USA).
RESULTS
Thirty-six percent of African-Americans had a diastolic blood pressure greater than90 mmHg compared to 21% of white subjects (p , 0.05), and 32% of African-Amer-icans had a MAP greater than 110 mmHg compared to 18% of whites (p , 0.05).Forty-three percent of African-Americans had a glycosylated hemoglobin greater than8% compared to 29% of white subjects. African-American subjects were twice as likelyto have had type 2 diabetes for more than 5 years duration compared to the whitesubjects (p , 0.05), but no more likely to have had type 2 diabetes for greater than 10years (data not shown).
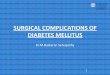
Table 1 gives anthropometric and physiological characteristics of the population bygender and race. While white males were older than black males, both male and femaleAfrican-Americans had higher mean diastolic blood pressures than their white counter-parts. African-American females had higher MAP and mean HbA1c levels compared towhite females. There were no signi® cant difference found for systolic blood pressure,diabetes duration, BMI, or fasting glucose level.
As expected, symptoms often associated with diabetes such as polydipsia, polyuria,and fatigue occurred in more than a third of all subjects. The most frequent symptoms
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014

J. C. KONEN ET AL.42
TABLE 1. Anthropometri c and physiologi c characteristic s of patients with type 2 diabetes by gender andrace
Female Male
Blacks Whites Blacks WhitesN 5 100 N 5 76 N 5 42 N 5 86
AnthropometricsAge, years 57 6 13 56 6 12 57 6 10 61 6 11*Body mass index 32.3 6 7 30.8 6 6 30.5 6 6 29.6 6 5Diabetes duration , years 8.5 6 8 7.6 6 8 8.1 6 9 8.3 6 8
Blood pressure, mmHgSystolic 139 6 21 132 6 28 141 6 21 137 6 23Diastolic 84 6 13 76 6 13** 85 6 11 80 6 13*Mean arterial 102 6 14 95 6 16* 104 6 13 99 6 15
Metabolic parametersBlood glucose, mg/dl 206 6 79 190 6 75 209 6 91 184 6 64HbA1c% 7.6 6 2 6.9 6 2* 7.6 6 3 7.1 6 2
*p , 0.05, **p , 0.01.
among African-Americans were in descending order with a prevalence greater than athird of subjects: fatigue, polyuria, blurred vision, polydipsia and palpitations. Amongwhite subjects the most frequent symptoms were fatigability, palpitations, polyuria,blurred vision, and polydipsia (data not shown).
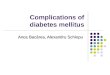
Table 2 gives the frequencies of symptoms and complications by gender and race.After adjustment for diabetes duration, diastolic blood pressure and HbA1c, African-American females compared to whites were signi® cantly more likely to experienceconstipation and hypertension but less likely to have claudication, peripheral atheroscle-rotic disease or peripheral neuropathy. African-American females were more likely thanwhites to experience polyphagia compared to white females but the difference was notstatistically signi® cant. Among male subjects after adjustment for covariates, African-Americans were signi® cantly more likely to experience blurred vision and hypertensionbut less likely to experience peripheral atherosclerotic disease. They were more likelythan white males to experience polyphagia, polydipsia, polyuria, and fatigue but thesedifferences were not statistically signi® cant.
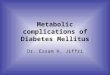
When the data were strati® ed by gender and race and odds ratios determined forsymptoms and complications of diabetes versus poor glycemic control (glycosylatedhemoglobin . 8%) as in Tables 3 and 4, African-American females with poor controlwere signi® cantly more likely to have polyphagia, polydipsia, and peripheral neuropathy.This group was also less likely to have cataracts than those with improved glycemiccontrol. Among white females the presence of poor glycemic control was associated withthe presence of microalbuminuria and retinopathy. Both African- and white Americanmales with poor glycemic control were signi® cantly more likely to have experiencedpolydipsia.
DISCUSSION
Data from the National Health Interview,6 and National Health and Nutritional Examin-ation Surveys7 show that the prevalence of known diagnosed diabetes over the last threedecades has increased markedly among African-Americans. From 1963 to 1985, rates ofdiabetes increased three-fold among African-Americans, while doubling in US whites.2
Since estimates suggest that only two-thirds of those with diabetes have been diagnosedwith the condition,8 diabetes is likely to occur in 25±30% of African-Americans by age
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014

RACIAL DIFFERENCES IN SYMPTOMS IN NIDDM 43
TA
BL
E2.
Com
pari
son
ofth
efr
eque
ncy
ofsy
mpto
ms
and
com
plic
atio
nsduri
ngth
epa
st6
mon
ths
for
pati
ents
with
type
2di
abet
es,ove
rall
and
by
race
and
gen
der
Fre
quen
cy(%
)F
emal
esM
ales
Over
all
Bla
cks
Whit
esO
R(9
5%
CI)
Bla
cks
Whites
OR
(95%
CI)
(N5
100)
(N5
76)
(N5
42)
(N5
86)
Sym
pto
ms
Gen
eral
Poly
phag
ia19
30
18
1.4
0(0
.94,
2.1
0)
12
12
1.1
7(0
.61,
2.2
4)
Poly
dip
sia
36
40
47
0.7
6(0
.54,
1.0
7)
36
21
1.3
6(0
.88,
2.1
0)
Poly
uri
a40
44
41
1.0
8(0
.77,
1.5
1)
45
33
1.3
5(0
.90,
2.0
1)
Fat
igab
ility
53
55
66
0.7
6(0
.54,
1.0
7)
45
43
1.2
0(0
.80,
1.7
9)
Const
ipat
ion
25
31
18
1.4
8*
(1.0
1,
2.2
0)
24
23
1.1
1(0
.69,
1.7
7)
Dysu
ria
14
89
0.8
6(0
.47,
1.5
6)
17
22
0.7
8(0
.47,
1.3
3)
Blu
rred
vis
ion
47
50
54
1.0
5(0
.75,
1.4
5)
55
31
1.6
2*
(1.0
9,
2.3
9)
Car
dio
vas
cula
rC
hes
tpai
n/a
ngin
a26
22
33
0.6
6*
(0.4
5,
0.9
7)
29
23
1.2
1(0
.77,
1.8
9)
Pal
pit
atio
ns
42
45
55
0.7
5(0
.53,
1.0
4)
36
31
1.1
5(0
.76,
1.7
3)
Com
plic
atio
ns/c
o-m
orb
idit
yC
ardio
vas
cula
rH
yper
tensi
on
61
75
50
1.8
0**
(1.3
0,
2.5
0)
71
49
1.6
4*
(1.1
0,
2.4
5)
Tra
nsi
ent
Isch
emic
Attac
ks/
CV
A4
55
1.3
1(5
8,3.0
2)
52
1.4
8(0
.27,
8.0
9)
Cla
udic
atio
n18
14
25
0.6
3*
(0.4
1,
0.9
8)
17
19
0.8
8(0
.53,
1.4
9)
Ath
erosc
lero
tic
Dis
ease
card
iac
28
24
30
0.8
2(0
.56,
1.2
1)
24
31
0.8
4(0
.53,
1.3
1)
AS
Dce
rebra
l10
13
91.1
2(0
.65,
1.9
2)
10
81.0
1(0
.45,
2.4
6)
AS
Dper
ipher
al18
921
0.5
5**
(0.3
3,
0.9
1)
12
29
0.5
6*
(0.3
2,
0.9
8)
Gen
itouri
nar
yP
rote
inuri
a12
17
11
1.1
0(0
.64,
1.8
8)
15
71.1
3(0
.57,
2.2
3)
Mic
roal
bum
inuri
a39
44
35
1.0
4(0
.72,
1.5
0)
41
38
1.0
1(0
.65,
1.5
6)
Vis
ual
Bli
ndnes
s.
20/2
00
68
41.3
0(0
.59,
2.8
4)
75
1.1
0(0
.46,
2.6
5)
Any
cata
ract
s25
30
28
1.0
3(0
.71,
1.5
0)
17
22
0.8
3(0
.51,
1.3
7)
Any
reti
nopat
hy
19
20
24
0.7
3(0
.48,
1.1
1)
21
14
1.1
3(0
.68,
1.8
9)
Ner
vous
syst
emP
erip
her
alneu
ropat
hy
51
46
57
0.6
9*
(0.4
9,
0.9
7)
52
50
1.0
3(0
.69,
1.5
3)
*p
,0.0
5,**p
,0.0
1.
OR
,odds
rati
o;
CI,
confi
den
cein
terv
al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014

J. C. KONEN ET AL.44
TA
BL
E3.
Odd
sra
tios
(95%
con®de
nce
inte
rval)
for
dia
bete
ssy
mpt
om
s,st
rati®ed
by
gen
der
,ra
ce,
and
gly
cem
icco
ntr
ol
Fem
ales
Mal
es
HbA
1c
.8%
HbA
1c
.8%
Bla
cks
Whit
esB
lack
sW
hit
es
Gen
eral
Poly
phag
ia2.7
3*
(1.0
3,
7.2
8)
1.6
3(0
.40,6.5
5)
2.3
0(0
.26,23.2
5)
5.2
1*
(1.1
0,25.8
0)
Poly
dip
sia
4.2
2**
(1.6
5,
10.9
7)
1.0
5(0
.34,3.2
4)
6.2
9**
(1.3
3,32.1
1)
2.0
7(0
.59,7.1
6)
Poly
uri
a1.5
4(0
.63,
3.7
7)
2.6
0(0
.82,8.3
2)
1.2
7(0
.31,5.1
9)
2.4
8(0
.82,7.5
7)
Fat
igue
2.0
5(0
.83,
5.1
1)
1.1
1(0
.34,3.7
0)
1.5
0(0
.37,6.1
8)
1.6
6(0
.57,4.8
8)
Const
ipat
ion
0.9
5(0
.36,
2.4
7)
1.6
3(0
.40,6.5
5)
0.9
0(0
.17,4.7
4)
1.6
8(0
.50,5.6
5)
Dysu
ria
0.4
8(0
.06,
2.9
1)
2.1
7(0
.34,13.3
3)
2.1
0(0
.32,14.5
7)
1.3
6(0
.38,4.7
2)
Blu
rred
vis
ion
0.9
4(0
.39,
2.2
7)
0.9
1(0
.29,2.8
1)
1.1
5(0
.28,4.7
0)
1.6
1(0
.52,4.9
3)
Car
dio
vas
cula
rA
ngin
a0.6
5(0
.21,
1.9
7)
0.7
2(0
.21,2.4
4)
1.5
8(0
.34,7.5
3)
0.8
9(0
.24,3.1
8)
Pal
pit
atio
ns
1.0
3(0
.42,
2.5
0)
0.4
9(0
.15,1.5
2)
0.5
8(0
.13,2.5
6)
0.7
1(0
.21,2.3
1)
*p
,0.0
5,**p
,0.0
1.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014

RACIAL DIFFERENCES IN SYMPTOMS IN NIDDM 45
TA
BL
E4.
Odd
sra
tios
(95%
con®de
nce
inte
rval
)fo
rdia
bete
sco
mpli
cati
ons,
stra
ti®ed
by
gen
der,
race
,and
gly
cem
icco
ntr
ol
Fem
ales
Mal
es
HbA
1c
.8%
HbA
1c
.8%
Bla
cks
Whit
esB
lack
sW
hit
es
Car
dio
vas
cula
rH
yper
tensi
on
0.6
1(0
.22,1.6
9)
0.5
3(0
.17,1.6
8)
1.0
7(0
.22,5.1
7)
0.7
5(0
.25,2.1
8)
TIA
/CV
A1.5
7(0
.23,10.6
)U
UU
Cla
udic
atio
n3.2
5(0
.88,12.6
)2.5
2(0
.73,8.7
9)
0.5
0(0
.06,3.6
2)
2.6
3(0
.73,9.5
0)
AS
Dca
rdia
c0.3
3*
(0.0
9,0.9
7)
0.6
1(0
.16,2.1
7)
0.8
6(0
.16,4.5
1)
0.3
7(0
.09,1.3
6)
AS
Dce
rebra
l0.4
2(0
.08,1.8
7)
1.0
7(0
.13,7.2
3)
0.4
1(0
.01,5.3
1)
2.2
1(0
.35,13.4
0)
AS
Dper
ipher
al1.2
8(0
.26,6.0
9)
1.2
8(0
.32,4.9
3)
0.8
8(0
.09,7.8
0)
1.4
4(0
.46,4.5
4)
Gen
itouri
nar
yP
rote
inuri
a0.9
6(0
.30,3.0
8)
3.0
6(0
.55,17.1
0)
1.4
7(0
.19,11.1
2)
3.0
0(0
.43,21.0
7)
Mic
roal
bum
inuri
a1.1
8(0
.49,2.8
7)
3.8
9*
(0.1
9,13.1
2)
1.5
0(0
.37,6.1
8)
2.2
6(0
.77,6.7
5)
Vis
ual
Blindnes
s0.9
1(0
.16,4.8
0)
5.7
9(0
.37,174.8
)U
UA
ny
cata
ract
s0.2
8*
(0.0
9,0.8
5)
1.5
0(0
.44,5.1
2)
2.0
0(0
.30,13.9
6)
0.6
7(0
.16,2.6
0)
Any
retinopat
hy
1.3
6(0
.45,4.1
2)
5.4
5**
(1.5
1,20.2
5)
1.9
2(0
.35,11.0
1)
0.9
0(0
.17,4.2
5)
Ner
vous
syst
emP
erip
her
alneu
ropat
hy
2.6
6*
(1.0
7,6.6
4)
2.5
0(0
.75,8.6
1)
1.3
5(0
.33,5.5
3)
1.1
3(0
.39,3.2
8)
*p
,0.0
5,
**p
,0.0
1.
U,
odds
rati
oco
uld
not
be
det
erm
ined
.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014

J. C. KONEN ET AL.46
65, compared to 15% for whites.9 The excess prevalence of diabetes among African-Americans is likely due to both a genetic predisposition towards diabetes as well as thetendency towards marked obesity for a larger proportion of African- than whiteAmericans. While Cowie et al.10 suggest that the strong interaction between African-American racial grouping and obesity may be responsible for the excess prevalence oftype 2 diabetes in this population, we found no signi® cant differences in BMI betweenthe two racial groups.
While the prevalence, characteristics, and risk factors for type 2 diabetes in African-and white Americans have been reviewed by Harris,6 most available data are fromnational surveys, and little from clinical observations that compare these two sub-popu-lations. To our knowledge there are no reports of racial differences of commonsymptoms and complications experienced by type 2 diabetic adults from the primary careperspective. Since three-fourths of all diabetic patients are cared for by primary carephysicians,11 understanding the similarities and differences of these major racial groupswill be important for the primary care physician to anticipate, suspect, recognize andeffectively manage complications.
Similar to white Americans, African-Americans with diabetes are at increased risk forcardiovascular disease compared to non-diabetics. However, the prevalence of cardiovas-cular disease in those with diabetes appears to be lower in blacks versus whites. The1976±1980 NHANES II cohort found that African-Americans were less likely thanwhites to report angina and to have had a prior myocardial infarction.7 The incidence ofangina has also been found to be lower in European blacks of African descent.12 Inaddition, coronary heart disease (CHD) mortality from diabetes has been found to belower in African-Americans. In older age groups ( . 45 for men, . 55 for women),diabetes was associated with lower risk of CHD mortality among blacks [odds ratio(OR) 5 1.6] than among whites (OR 5 2.5).13 Age-adjusted death rates with cardiovascu-lar disease as the underlying cause of death are also lower for both black males andfemales.1 The present study also found a similar pattern, with a lower prevalence ofsymptoms related to, and a lower incidence of, cardiovascular disease among African-Americans. We found that black women were less likely to experience angina andclaudication. In addition, while African-Americans with type 2 diabetes were more likelythan whites to have hypertension and poor glycemic control, they were less likely thanwhites to have atherosclerotic cardiac or peripheral vascular disease. It has beensuggested that the lower CHD mortality risk among blacks is due to a higher prevalenceof an insulin-sensitive variant of type 2 diabetes in the black population.14 Data indicatethat blacks with insulin-sensitive diabetes have a lower CHD risk factor pro® le,14 themajority of which is probably due to improved lipid and lipoprotein levels in thispopulation.15
There are data that indicate that African-Americans with diabetes are more likely tosuffer visual impairment than US whites. The National Health Interview Survey usingself-reported data showed a 40% higher rate of visual impairment among blacks.17 Theprevalence of retinopathy in blacks from the 1988±91 phase of NHANES III was foundto be higher than in non-Hispanic whites.16 Studies on visual complications fromdiabetes have found that the prevalence of blindness from retinopathy was twice as highamong African-Americans compared to whites.17 Although we found no difference byrace in blindness, de® ned as visual acuity greater than 20/200, we did ® nd thatAfrican-American males were more likely to complain of blurred vision. Our black malesubjects also tended to be more likely to have signs of any retinopathy, but thisdifference was not statistically signi® cant.
End-stage renal disease (ESRD) is also more likely to occur among African-than whiteAmericans. In general, black sub-populations are nearly four times more likely todevelop ESRD than their white counterparts.18 It has been suggested that this associationoccurs because diabetes and hypertension are less well controlled among African-Amer-
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014

RACIAL DIFFERENCES IN SYMPTOMS IN NIDDM 47
icans than among whites.19 However, Brancati et al.20 found that diabetic ESRDappears to occur at a higher prevalence among African-Americans possibly becauseof an increased susceptibility among this population, and not simply from ahigher prevalence of diabetes or hypertension or because of possible racialdifferences in socioeconomic status or access to health care. While differences inrenal function between blacks and whites may explain some of the excess risk ofnephropathy among African-Americans with type 2 diabetes, the path to ESRD may notbe inevitable if early detection and treatment of vascular complications becomes moreeffective.21
The detection of abnormal urinary excretion of albumin has been proposed as amarker for underlying diabetic vascular pathology.22 The appearance of microalbumin-uria, levels of albuminuria below that detected on routine dipstick, is predictive ofESRD23 and is associated with cardiovascular disease and mortality in patients with type2 diabetes23 and in the elderly.24 So powerful is this marker, that diabetic individualswithout microalbuminuria appear to have no greater risk of atherosclerotic outcomesthan individuals without diabetes.25 In our population we found no signi® cant racialdifferences in mean excretion of urinary albumin or in the proportion of individuals withmicroalbuminuria.
Constipation is a common complaint of individuals with diabetes mellitus.26 Fre-quent constipation is believed to contribute to DNA and other cellular damage in thecolon and rectum27 and it has been shown that diabetics are at greater risk forcolorectal cancer compared to non-diabetics.28 In our sample we found that a highpercentage of our subjects reported constipation (25%). In addition, African-Americanfemales were signi® cantly more likely than white females to report this symptom, onewhich is seldom reported in diabetic subjects. Since there is data that African-Americans have a slightly higher incidence of colon and rectum cancers comparedto whites,29 screening for constipation in this population may have importantimplications.
There is evidence that African-American patients, particularly women, have poorerglycemic control than white individuals with type 2 diabetes even after controlling forduration of diabetes, physical activity, and BMI.19,30 In the present study, poor long-termglycemic control was associated with traditional diabetic symptoms/complications ofpolyphagia, polydipsia and peripheral neuropathy among African-American females andpolydipsia among African-American males. However, there were no signi® cant associa-tions with poor glycemic control for the common symptoms of polyuria, blurred visionand fatigue for either race, even though African-American males complained of blurredvision more often than white males.
This study is limited by its cross-sectional nature and the possibility that these resultsare not generalizable. However, the characteristics of our diabetic subjects are notsigni® cantly different from surveys of North Carolina as a whole, or from nationalestimates made by the CDC. Additional studies based on multiple sites and with largersample sizes will be necessary to establish whether the differences observed by race area function of biological differences, differences in glycemic control and/or bloodpressure levels, or differences than can be largely explained by access to care, educationand income.
Regardless, clinicians should be aware that our results indicated that both African- andwhite Americans with type 2 diabetes appear to suffer from a wide variety of symptomsand complications and that racial differences in these conditions exist. African-Ameri-cans with diabetes appear to have a greater probability of experiencing poor metaboliccontrol and hypertension than whites while suffering less cardiovascular disease. These® ndings may have important implications concerning screening and preventive strategiesin this high risk population.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014

J. C. KONEN ET AL.48
ACKNOWLEDGEMENT
This study was supported in part by a cooperative agreement from the Centers forDisease Control (U32CCU-403318) .
REFERENCES
1. Centers for Disease Control and Prevention . Diabetes Surveillance 1997. US Dept of Health andHuman Services, National Center for Chronic Disease Prevention and Health Promotion, Division ofDiabetes Translation , 1997.
2. Harris MI. Summary. In: Diabetes in America, 2nd edn, National Diabetes Data Group, NationalInstitutes of Health, NIH publicatio n #95±1468, 1995: 1±14.
3. Konen JC, Curtis LG, Shihabi ZK & Dignan MB. Screening diabetic patients for microalbuminuria .J Fam Prac 1990; 31: 505±10.
4. Diabetes in North Carolina. Diabetes in North Carolina. Diabetes Control Program, Division ofAdult Health, Department of Environment , Health, and Natural Resouces , 1993 (publicatio n no.14G±2/93).
5. McCormick CP, Shihabi ZK & Konen JC. Microtransferrinuri a and microalbuminuria : enhancedimmunoassay. Ann Clin Lab Sci 1989; 19: 444±51.
6. National Center for Health Statistics. The National Health Interviews Survey Design 1974± 84 andProcedures 1973± 83, 1985 (NCHS Vital Statistics Series 1, no. 18).
7. National Center for Health Statistics . Plan and Operation of the Second National Health andNutritiona l Examination Surveys, 1981 (NCHS Vital and Health Statistics Series 1, no. 15).
8. Centers for Disease Control and Prevention. National Diabetes Fact Sheet: national estimates andgeneral information on diabetes in the United States. Atlanta, GA: US Department of Health andHuman Services, Centers for Disease Control and Prevention , 1997.
9. Harris MI. Non-insulin dependen t diabetes mellitus in black and white Americans. Diabetes/MetabRev 1990; 6: 71±90.
10. Cowie CC, Harris MI & Silverman RE. Are blacks at greatest risk of diabetes after considerin g otherdiabetic risk factors? (Abstract) . American Diabetes Association 50th annual meeting, Atlanta, GA,1990, 39 Suppl 1: 74A.
11. Schappert SM. Of® ce Visits for Diabetes Mellitus, United States, 1989. Hyattsville, MD: NationalCenter for Health Statistics, 1992.
12. Weijers RN, Goldschmidt HM & Silverbusch J. Vascular complications in relation to ethnicity innon-insulin-dependen t diabetes mellitus. Eur J Clin Invest 1997; 27: 182±8.
13. DeStefano F & Newman J. Comparison of coronary heart disease mortality risk between black andwhite people with diabetes. Ethnicity Dis 1993; 3: 145±51.
14. Banerji MA & Lebovitz HE. Coronary heart disease risk factor pro® les in black patients withnon-insulin-dependen t diabetes mellitus: paradoxic patterns. Am J Med 1991; 91: 51±8.
15. Summerson JH, Konen JC & Dignan MB. Racial differences in lipid and lipoprotein levels indiabetes. Metabolism 1992; 41: 851±5.
16. Klein RK & Klein BEK. Vision disorders in diabetes. In: Diabetes in America, 2nd edn, NationalDiabetes Data Group, National Institutes of Health, NIH publicatio n #95±1468, 1995: 293±338.
17. Kahn HA & Hiller R. Blindness caused by diabetic retinopathy . Am J Ophthal 1981; 78: 58±67.18. Cowie CC, Port FK, Wolfe RA, Savage PJ, Moll PP & Hawthorne VM. Disparities in incidence of
diabetic end-stage renal disease according to race and type of diabetes. N Engl J Med 1889; 321:1074±9.
19. Eberhardt MS, Lackland DT, Wheeler FC & Teutsch SM. Glycemic control in blacks and whiteswith diabetes in two South Carolina communities. Diabetes 1990; 39 (Suppl 1) 205A.
20. Brancati FL, Whittle JC, Whelton PK, Seider AJ & Klag MJ. The excess incidence of diabeticend-stage renal disease among blacks. JAMA 1992; 268: 3079±84.
21. Rostand SG. Diabetic renal disease in blacksÐ inevitabl e or preventable ? N Engl J Med 1989; 321:1121±2.
22. Deckert T, Feld-Rasmussen B, Borch-Johnse n K, Jensen T & Kofoed-Enevoldse n A. Albuminuriare¯ ects widespread vascula r damage. The Steno hypothesis . Diabetologia 1989; 32: 219±26.
23. Mogensen CE. Microalbuminuri a predicts clinical proteinuri a and early mortality in maturity-onse tdiabetes. N Engl J Med 1984: 310: 356±60.
24. Damsgaard EM, Froland A, Jorgensen OD & Mogensen CE. Microalbuminuri a as predicto r ofincreased mortality in elderly people. Br Med J 1990; 300: 297±300.
25. Schmitz A & Vaeth M. Microalbuminuria : a major risk factor for non-insuli n dependen t diabetes.A 10-year followup study of 503 patients. Diabetic Med 1988; 5: 126±34.
26. Hartford JD, Skyler JS & Barkin JS. Diabetes and the gastrointestina l system. In: Rifkin H & PorteD Jr. Eds. Diabetes Mellitus: theory and practice, 4th edn. New York: Elsevier, 1990: 824±37.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014

RACIAL DIFFERENCES IN SYMPTOMS IN NIDDM 49
27. Potter JD. Reconciling the epidemiology , physiology , and molecular biology of colon cancer . JAMA1992; 268: 1573±7.
28. Cancer Facts and FiguresÐ 1997. American Cancer Society, 1997, 20.29. Will JC, Galuska DA, Vinicor F & Calle EE. Collorectal cancer: another complication of diabetes
mellitus? Am J Epidemiol 1998; 147: 816±25.30. Summerson JH, Konen JC & Dignan MB. Race-related differences in metabolic control among
adults with diabetes. S Med J 1992; 85: 953±6.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
oron
to L
ibra
ries
] at
03:
23 0
9 O
ctob
er 2
014