-
8/9/2019 Radio Graphic Caries Diagnosis
1/50
The following slides describe the radiographic
diagnosis of caries.
0
Caries Diagnosis
In navigating through the slides, you should click
on the left mouse button when you see the
mouse holding an x-ray tubehead or you are
done reading a slide. Hitting Enter or Page
Down will also work. To go back to the previous
slide, hit backspace or page up.
-
8/9/2019 Radio Graphic Caries Diagnosis
2/50
Caries
Caries is the breakdown of tooth structure
caused by acid-producing bacteria in the mouth.These bacteria
are found in the white or pale
yellow plaque that builds up on the teeth if they
are not cleaned properly on a regular basis. The
bacteria break down carbohydrates (sugars) toform the acid that
demineralizes tooth structure,
leading to caries.
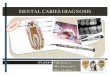
The diagnosis of caries is made through a
combination of the clinical examination andradiographs.
Unless fairly large, interproximal caries in the
posterior region usually requires radiographs to
make a diagnosis.
-
8/9/2019 Radio Graphic Caries Diagnosis
3/50
The bitewing film is primarily used for caries
identification, but the periapical film is also helpful.The
difference in angulation between the two films
gives two different perspectives and can be especially
helpful in diagnosing recurrent caries around existing
restorations.There is a lot of discussion on which film speed (D
or
F) should be used. Many dentists use D-speed film
because they feel it provides sharper images as a
result of the smaller grain size. Most educators, on theother
hand, recommend the F-speed film (Insight)
because of the significant reduction in x-ray exposure
to the patient (approximately 60% less than when using
D-speed film).
Radiographs
-
8/9/2019 Radio Graphic Caries Diagnosis
4/50
Approximately 40-50 % demineralization is required
for radiographic detection of a lesion. As seen in the
occlusal view, above right, the thickness of the tooth
buccolingually masks the carious lesion when it is
small.
The actual depth of penetration of a carious lesion
is actually deeper than it appears on the radiograph.
Proximal caries susceptible zone
caries
0
-
8/9/2019 Radio Graphic Caries Diagnosis
5/50
Buccolingual thickness of tooth.The thicker the
tooth, the more difficult it is to see the extent ofthe
caries.
Limitations of two-dimensional film.The extent of
carious involvement can not be seen in a
buccolingual (cheek to tongue) direction.
Factors affecting appearance of caries
on radiographs:
-
8/9/2019 Radio Graphic Caries Diagnosis
6/50
X-ray beam angle(horizontal or vertical). This isespecially
important when trying to identifyrecurrent caries, since changes in
angulation maycause the superimposition of the existingrestoration
with the carious lesion. Overlap due toimproper horizontal
angulation makes it verydifficult to diagnose early interproximal
caries.
Exposure factors. Caries detection is improvedwith a lower kVp
setting, which provides a higher
contrast. If the overall density of the film is too
light or too dark, the diagnostic potential of the
film is limited.
Factors affecting appearance of caries
on radiographs (continued):
-
8/9/2019 Radio Graphic Caries Diagnosis
7/50
0
In the anterior region,interproximal caries can
often be diagnosed using
transillumination, which
involves directing a brightlight through the contact
areas. Combining
transillumination with
radiographs enhances the
diagnostic information
obtained.
Transillumination
transilluminator
-
8/9/2019 Radio Graphic Caries Diagnosis
8/50
I
M = Moderate (Stage II)
I = Incipient (Stage I)
A = Advanced (Stage III)
S = Severe (Stage IV)
Caries Classification
S
AMA
-
8/9/2019 Radio Graphic Caries Diagnosis
9/50
Interproximal Caries(Incipient)
I
Up to half the thickness of enamel
Usually not restored unless patient
has high level of caries activity (high
risk). Treat with fluoride.
-
8/9/2019 Radio Graphic Caries Diagnosis
10/50
The arrow points to incipient lesions on the
mesial of # 19 and the distal of # 20.
-
8/9/2019 Radio Graphic Caries Diagnosis
11/50
Incipient
Moderate
Advanced
-
8/9/2019 Radio Graphic Caries Diagnosis
12/50
M
Interproximal Caries(Moderate)
More than halfway through the
enamel (up to DEJ)
-
8/9/2019 Radio Graphic Caries Diagnosis
13/50
The bottom arrow points to a moderate lesion
on the distal of # 20. The upper arrow points to
one of several incipient lesions on the molar
and premolars.
-
8/9/2019 Radio Graphic Caries Diagnosis
14/50
-
8/9/2019 Radio Graphic Caries Diagnosis
15/50
Moderate lesion seen on previous film
-
8/9/2019 Radio Graphic Caries Diagnosis
16/50
Class III moderate lesion seen in the
anterior region
-
8/9/2019 Radio Graphic Caries Diagnosis
17/50
AA
Interproximal Caries
(Advanced)
-
8/9/2019 Radio Graphic Caries Diagnosis
18/50
Advanced lesion identified by arrows.
-
8/9/2019 Radio Graphic Caries Diagnosis
19/50
Advanced lesions seen on previous film
-
8/9/2019 Radio Graphic Caries Diagnosis
20/50
Advanced lesion
-
8/9/2019 Radio Graphic Caries Diagnosis
21/50
Advanced lesion
-
8/9/2019 Radio Graphic Caries Diagnosis
22/50
More than halfway
through the dentin
S
Interproximal Caries
(Severe)
-
8/9/2019 Radio Graphic Caries Diagnosis
23/50
Severe lesion
-
8/9/2019 Radio Graphic Caries Diagnosis
24/50
Severe lesion
-
8/9/2019 Radio Graphic Caries Diagnosis
25/50
Must have penetrated into dentin
Diagnosed from clinical exam
May be seen as thin radiolucent line orcup-shaped zone
underlying occlusal
enamel, but difficult to see on
radiographs unless lesion is large.
Some feel that a sharp explorer used tooforcefully may
contribute to spread
of caries by opening up pit or fissure
Occlusal Caries
-
8/9/2019 Radio Graphic Caries Diagnosis
26/50
Occlusal caries
-
8/9/2019 Radio Graphic Caries Diagnosis
27/50
Occlusal caries
-
8/9/2019 Radio Graphic Caries Diagnosis
28/50
Should be identified from clinical
exam. Sometimes seen as well-defined circular area in middle
of
tooth, although it is not very
radiolucent. Depth can not bedetermined radiographically.
Buccal/Lingual
Caries
-
8/9/2019 Radio Graphic Caries Diagnosis
29/50
Lingual caries (Cant tell whether its buccal
or lingual from one radiograph
-
8/9/2019 Radio Graphic Caries Diagnosis
30/50
Buccal caries with severe interproximal
caries on # 12
-
8/9/2019 Radio Graphic Caries Diagnosis
31/50
Saucer-like cratering on the roots of the
teeth, involving the cementum. Usually
found on older individuals withprominent recession and/or
periodontitis. May have xerostomia due
to medications. May be confused with
cervical burnout (discussed on later
slide).
RootCaries
-
8/9/2019 Radio Graphic Caries Diagnosis
32/50
Root caries
-
8/9/2019 Radio Graphic Caries Diagnosis
33/50
Root caries
-
8/9/2019 Radio Graphic Caries Diagnosis
34/50
Cervical Burnout
Cervical burnout is an apparent radiolucency
found just below the CE junction on the rootdue to anatomical
variation (concave root
formation posteriorly) or a gap between the
enamel and bone covering the root(anteriorly). Mimica root
caries. Posteriorly,
this radiolucency usually disappears when
another film of the region is examined. Caries
does not occur on the root of the tooth unlessthere is loss of
alveolar bone and gingival
tissue due to recession or periodontitis.
P t i i l b t Th i i ti
-
8/9/2019 Radio Graphic Caries Diagnosis
35/50
Posterior cervical burnout. The invagination
of the proximal root surfaces allow more x-
rays to pass through this area, resulting in a
more radiolucent appearance on theradiograph. X-rays directed at
a different
angle usually pass through more tooth
structure and the radiolucency disappears.
-
8/9/2019 Radio Graphic Caries Diagnosis
36/50
Radiolucency seen at left (arrow)disappears on periapical film
of
same tooth. This is cervical burnout.
-
8/9/2019 Radio Graphic Caries Diagnosis
37/50
bone level
Anterior cervical burnout. The space between
the enamel and the bone overlying the tooth
will appear more radiolucent than either the
enamel or the bone-tooth combination.
-
8/9/2019 Radio Graphic Caries Diagnosis
38/50
Cervical burnout in theanterior region due to
gap between enamel
(red arrows) and
alveolar bone over root(blue arrows).
-
8/9/2019 Radio Graphic Caries Diagnosis
39/50
Found around the margins of existing
restorations. May be due to unusualsusceptibility to caries,
poor oral
hygiene, failure to remove all of the
caries during cavity preparation, adefective restoration or a
combination
of the above.
Recurrent Caries
-
8/9/2019 Radio Graphic Caries Diagnosis
40/50
Recurrent caries
-
8/9/2019 Radio Graphic Caries Diagnosis
41/50
Recurrent caries
-
8/9/2019 Radio Graphic Caries Diagnosis
42/50
Recurrent caries
-
8/9/2019 Radio Graphic Caries Diagnosis
43/50
Rampant Caries
Extensive and rapidly progressingcaries usually found in
children
and teens with poor diet and
inadequate oral hygiene
-
8/9/2019 Radio Graphic Caries Diagnosis
44/50
-
8/9/2019 Radio Graphic Caries Diagnosis
45/50
Found in head/neck radiation
therapy patients with xerostomia
Fluoride used for control
Radiation Caries
-
8/9/2019 Radio Graphic Caries Diagnosis
46/50
-
8/9/2019 Radio Graphic Caries Diagnosis
47/50
Before radiation
-
8/9/2019 Radio Graphic Caries Diagnosis
48/50
1 year after radiation
M h B d
-
8/9/2019 Radio Graphic Caries Diagnosis
49/50
Mach BandOptical illusion giving appearance of increased
radiolucency at the junction of differing tissuedensities, such
as enamel and dentin. If you block
off the enamel with a fingernail, the radiolucency
will disappear if due to the mach band effect. If the
radiolucency persists, it may be caries.
0
-
8/9/2019 Radio Graphic Caries Diagnosis
50/50
This concludes the section on Caries.
Additional self-study modules are availableat:
http://dent.osu.edu/radiology/resources.htm
If you have any questions, you may e-mail
me at:[email protected].
Robert M. Jaynes, DDS, MS
Director, Radiology Group
College of DentistryOhio State University
0