Embed Size (px)
Citation preview

Progress in
Cardiovascular Diseases VOL. XV, NO. 1 JULY/AUGUST 1972
Radioactive Tracers in Diagnosis of Cardiovascular Disease
Henry N. Wagner, Jr. and Buck A. Rhodes
A LMOST HALF A CENTURY AGO, Blumgart and Weiss used radioactive tracers to study circulation in patients with rheumatic and syphilitic heart
disease.‘+2 A radium salt solution was the radioactive tracer, and a cloud chamber was the detection instrument. Modern radiopharmaceuticals, such as 99mTc-labeled microsphereq3 and the scintillation camera exemplify some of the advances that have been made since these pioneering studies.
Although tracers such as radioactive sodium and radioiodinated albumin had been used occasionally in research studies of patients with edema, the first clinically useful study of cardiovascular disease was the scanning of patients sus- pected of pericardial effusion after the intravenous injection of radioiodinated albumin, a procedure first proposed by Rajali et al. in 1958.4
Lung scanning was introduced 5 yr later for the diagnosis of pulmonary em- bolism5*6 and is now widely used throughout the world, not only in the differen-
tial diagnosis of pulmonary embolism, but also in evaluating regional lung func- tion in lung cancer, infections, and obstructive lung disease.
The scintillation camera, invented by Anger7 and commercially available in 1963, soon had a profound effect on tracer studies in the diagnosis of cardiovas- cular disease. In contrast to the rectilinear scanner, which has a radiation de- tector that moves back and forth across the region of the body being studied, the scintillation camera has a circular field of view approximately 11 inches in di- ameter. The detector does not move, spatial localization of the tracer being achieved by an array of 19 photomultiplier tubes that are attached to the scintil- lation detector. Because the spatial distribution of the radioactive tracer is mea- sured continuously, serial images of a bolus passage of tracers intravenously in- jected through the heart and great vessels could be made, a procedure referred to as nuclear angiocardiography.
With “9mTc-labeled human serum albumin the intracardiac distribution of
From the Deparrmenr of Radiological Sciertces. The Johns Hopkins Medical Insrirurion.\. Bal- timore, Md.
Supported by USPHS Granr GM 1054X. Henry N. Wagner, Jr., M.D.: Professor ofRadiological Sciences, Radiology. and Medicitlr. Thr
Johns Hopkins Medical Iturirulions. Baltimore, Md. Buck A. Rhodes. Ph.D.: ds.~i.~[anr Profes.wr
ofRadiological Sciences. The Johns Hopkins Medical Institutions. Baltimore, Md.
Progress in Cardiovascular Diseases, Vol. XV, No. 1 (July/August), 1972 1

2 WAGNER AND RHODES
Table 1. Circulatory Diseases in Which Radioactive Tracers Are Useful in Diagnosis
Cerebral thromboembolism
Arteriovenous malformations of bram
Aneurysms of brain
Thyrotoxic heart dwase
Aneurysms of great vessels
Pencardral effusion
Pericardial cysts
Myocardial infarction
Ventricular aneurysm
Cyanotrc congenital heart disease
Left-to-right intracardiac shunts
Pulmonary venous hypertension
Hypoplastrc pulmonary arteries
Dextrocardia
Asplenia
Primary aldosteronism
Unilateral renal disease
Pulmonary thromboembc
Congestive heart failure
Anemia
Hypovolemia
Polycythemia
Venous obstruction
Arterial insufficrency
Leg ulcers
Gangrene
the tracer during specific parts of the cardiac cycle can be monitored with the scintillation camera, using electrocardiographic voltages such as the QRS com- plex to activate the camera only during systole or diastole, a procedure called “gating” the camera.B Ejection fraction can be measured and areas of myocar- dial akinesis documented in patients who have had a myocardial infarction.
Other areas in which advances were made included the use of the particle dis- tribution principle to study the systemic as well as the pulmonary circulation. The distribution of blood flow to the legs in patients with peripheral vascular or Paget’s disease was examined. lo Regional myocardial blood flow was measured
with radioactive gases,” particles, 12-16 and ionic tracers such as 43K17 and ‘zgCs.‘8 Finally, anatomic arteriovenous shunting across the lungslg and in the systemic circulation could be determined with microspheres, as well as with soluble tracers. Table 1 lists the major uses of radioactive tracers in cardiovascular disease. Some of these will be reviewed in this article.
COMPARTMENTAL VOLUMES
The volume of blood within a given part of the circulatory system can be de- termined by injecting a radioactive tracer, such as albumin, red blood cells, or a substance (e.g. ionic l131n) that is bound by plasma proteins, and measuring the spatial distribution of radioactivity within the area of interest. In such studies, time is relatively umimportant unless we wish to relate the circulatory volumes to particular parts of the cardiac cycle. It is necessary only that the tracer be allowed sufficient time to distribute itself throughout the circulation prior to making the measurements, although the spatial resolution of the mea- surements is also an important consideration. To measure total plasma or blood volume, it is necessary only to draw a sample of blood and relate the plasma or red blood cell radioactivity to the amount of radioactive tracer injected. Total plasma or red blood cell volume is computed by the principle of indicator dilu- tion.
Among the earliest clinical uses of radioactive tracers was the measurement of total red blood cell and plasma volumes. Such procedures are useful in the differential diagnosis of patients with high hematocrits to distinguish between true and relative polycythemia, and occasionally in the pre- and post-operative evaluation of blood loss. The relative number of such studies remains low, prob- ably related to the reliability of other signs of polycythemia Vera, such as

RADIOACTIVE TRACERS 3
splenomegaly and increased platelet count, and the common use of central venous pressure measurements in surgical patients.
To measure the volume of blood within a specific region, such as the left ven- tricle, the radiation detection system must be able to resolve adequately the radioactivity within the ventricle from the radioactivity in surrounding struc- tures that contain blood. A specific diagnostic problem can be viewed in terms of the spatial and temporal resolution required for its solution. If we are in- terested in a fast process, such as the fraction of the left ventricular volume ejected with each beat of the heart, the temporal resolution of the detection system must be a fraction of a second, whereas if we are only concerned with the volume of blood within a region such as the leg, the temporal resolution need not be great. Functional resolution, a third type, is the selection of the par- ticular functions that we wish to measure. To diagnose pulmonary embolism, we select a tracer that will measure regional pulmonary arterial blood flow, while in patients suspected of alpha-i antitrypsin deficiency, we are interested in re- gional ventilation and select a tracer such as ‘33Xe.
At present, the instruments used to obtain spatial resolution are the rectilinear scanner and the scintillation camera. While adequate for many purposes, the spatial resolution is still quite poor. Rectilinear scanners and cameras can re- solve two parallel lines about 1.5 cm apart, although special devices such as the pinhole collimator can increase the spatial resolution so that lines 0.75 cm apart can be distinguished. Resolution in depth is even poorer, but can be improved by the use of multiple views, and tomographic techniques which are now being evaluated.
Figure 1A illustrates the improvement in image quality that results from the use of improved radiopharmaceuticals and instruments. Figure 1B is a rec- tilinear scan performed in 1960 with a 3-inch diameter sodium iodide crystal and 100 &i of 1311 human serum albumin injected intravenously. The black areas represent the distribution of the tracer within the blood pool of the heart. Al- though we see a clear zone of decreased radioactivity surrounding the heart, little else is discernable. A typical image obtained today with a scanner with a 5-inch diameter crystal and 99mTc-albumin is of better quality. We can identify left ventricular hypertrophy, an enlarged left atria1 appendage and probably a giant left atrium. The improved image quality is the result of the increased number of photons making up the image as the result of the use of 99mTc. Be- cause of its rapid radioactive decay, millicurie rather than microcurie amounts can safely be administered.
The use of a radioactive tracer to detect a pericardial effusion requires only an intravenous injection and the result is available within minutes. Little training is required in interpreting the images, although experience is required in distinguishing effusions superimposed on cardiac dilatation from ventricular hypertrophy without effusion. Pericardial effusions resulting from infections, such as tuberculosis or myxedema, are readily apparent because they are characterized by an abnormally small intracardiac blood pool, together with the zone of decreased activity surrounding the heart. Pericardial cysts or tu- mors usually result in displacement of the cardiac blood pool to one side in a manner that can be distinguished from an effusion. Many use the scintillation camera together with 99mTc-pertechnetate to diagnose pericardial effusion.

4 WAGNER AND RHODES

RADIOACTIVE TRACERS 5
Since pertechnetate diffuses promptly out of the vascular compartment into the interstitial fluid, observations are made of the tracer’s passage through the great vessels immediately after intravenous injection, rather than letting the tracer distribute itself throughout the vascular compartment as with an intra- vascular tracer such as 99mTc-albumin or ionic 113mIn. The latter substance binds to plasma transferrin and remains within the vascular compartment. For the diagnosis of pericardial effusion, we prefer the use of rectilinear scanner and an intravascular tracer. The zone of best resolution with the scanner is several inches below the chest wall, rather than at the surface, as is the case with the scintillation camera. Even normal persons may have an apparent zone of decreased activity surrounding the cardiac blood pool when examined with the scintillation camera.
The relative blood volume in the venous pools of the legs and the rates in which these volumes change with position and exercise can be used in the diagnosis of peripheral vascular disease. 2o--22 In a group of 19 volunteers, 21-38 yr old without clinical evidence of venous disease, we used a radioactive blood pool label and external radiation detectors to measure the relative changes in calf blood volumes and the times required for these changes. In the rapid change from horizontal to 45” upright position, there is a gradual rise in the volume to 145% f 14% (1 SD) the horizontal volume, taking an average of 21 set to reach one-half of this volume, and more than 14 min to reach equilibrium. With exer-
cise, the volume of blood within the calf falls to 76% A 6% (1 SD) of the volume prior to exercise. On inverting the subjects to 45” head-down position, the calf blood pool is reduced to 70% & 12% (1 SD) of the horizontal volume.
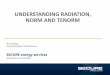
Occlusive venous disease both alters the magnitude of these relative volume changes and decreases the rate of change in volume when the subject is tilted to the 45” head-down position. In a subject with acute unilateral venous thrombosis (Fig. 2). the relative calf blood volume of her diseased leg increased to only
u.w.- acut. L venous thrombosis
/ I -1 / I u
T;E- sue
Fig. 2. Peripheral blood pool dynamic study. After intravenous administration of 3 mCi of ssmTc- albumin gamma ray detectors ere focused over calf muscles of each leg and counts are recorded as patient is tilted or exercised. Tracings show relative right (R) and left f L) calf muscle blood volumes as subject is tilted from horizontal to 45” head-up position. Note that thrombosed leg
drains blood more slowly than normal leg; 30 set v. 5 set T ) E is time required for the count rate to decrease from upright value to upright value minus one-half change of volume in going from up- right to horizontal.

6 WAGNER AND RHODES
Table 2. Changes in Peripheral Blood Pool Dynamics Indicative of Venous Disease
Abnormallry Calf Blood Pool
Incompetence of venous system
Incompetent perforating vessels
(ankle blow-out syndrome)
Venous thrombosis or congestive
heart failure
Increased pool we with more rapld
flllmg and large volume changes wth
posmon
Pool volumes may be normal except
m speclflc areas affected by the I”-
competent vessels-during exenxe
the volume mcreases m the affected
areas
Decreased pool size with slowed drainage
and reduced volume changes wth
posltion: thrombosis - unilateral
abnormahttes: congestive heart fallwe
-. bilateral abnormalmes
104% of the horizontal volume when tilted 45” to upright. Her normal leg in- creased to 125%. She required 70 set to drain her thrombosed leg, compared to 15 set for her normal leg.
Peripheral venous disease due to incompetent valves is also detected by the radiometric monitoring of changes in the relative blood volumes. Subjects with postphlebitic legs show rapid filling when tilted from horizontal to 45” head up. During exercise they show little or no decrease in relative calf volume. Areas affected by incompetently perforating vessels (ankle blow-out syndrome) show increased volume during exercise.
Table 2 shows changes in peripheral blood pool dynamics which are indicative of venous disease. The safety and simplicity of measuring changes in muscle blood volumes with radioactive tracers is useful in the initial diagnostic workup of patients, as well as in the evaluation of response to therapy.
GATED STUDIES OF INTRAVASCULAR VOLUMES
Instead of simply depicting the intravascular volumes of the heart averaged over the entire cardiac cycle, to look for pericardial effusion, it is possible to use the electrical events of the patient’s own electrocardiogram to activate the scintillation camera only during specific parts of the cardiac cycle. In such stud- ies we may look at the left ventricular contour during systole or diastole only. The patient is viewed in the right anterior oblique position, so that the boundaries of the left ventricle lie outside those of the right ventricle. As in the search for a pericardial effusion, the tracer used is Y9mTc albumin which is first allowed to distribute itself throughout the vascular compartments prior to ex- amination of the patient.
The purpose of such studies is to determine the contractility of the heart and to obtain information such as ejection fraction or to detect areas of myocardial akinesis. Figure 3 is the study of a patient with myocardial infarction in whom the apex of the heart did not contract during systole, while the rest of the left ventricle did. The advantage of this type of study relative to contrast angiog- raphy is its safety and simplicity; it can be performed at daily or even hourly intervals. The radiation dose is far less than that with fluoroscopy. At present it is being evaluated in patients with acute myocardial infarction.

RADIOACTIVE TRACERS
Fig. 3. Gated heart scan. A and C, diastole; B and D. systole. Drawing on right shows how images are analyzed.
CARDIAC STRUCTURE
When a child or young adult has unexplained cyanosis or a cardiac murmur, the differential diagnosis includes the possibility of congenital heart disease. The definitive diagnosis may require cardiac catheterization and contrast angiography, but such procedures are not without risk, particularly in newborn cyanotic infants. If the physician could be reasonably certain that the infant were suffering from respiratory distress syndrome, myocardial disease, or central nervous system disease, cardiac catheterization and contrast angiography might be avoided and the child’s chance of survival would probably be increased. On the other hand, prompt diagnosis of patients with certain types of cyanotic con- genital heart disease and congestive heart failure during the first month of life may be life saving.
At Johns Hopkins Hospital, nuclear angiocardiography has been shown to be of value in the differentiation of cardiac and noncardiac cyanosis in newborn infants.23 The technique consists of continuous monitoring with the scintillation camera of the passage of an intravenously injected bolus of sodium pertechne- tate (99mTc) or human serum ablumin (99mT~) as it passes through the cardiac chambers and lungs. The types of images that are obtained are shown in Fig. 4. Although the structural detail is poor compared to contrast angiography, we can usually identify the superior vena cava, right atrium and ventricle, pulmo- nary artery and lungs, and finally, the left ventricle and aorta. To identify a structurally normal heart, we look particularly for a clear space between the su- perior vena cava and pulmonary artery in the early frames, which will subse- quently be filled as activity fills the ascending aorta. We look for filling of the lungs immediately after visualization of the pulmonary artery without any evi- dence of activity in the abdominal aorta. In normal persons, activity is not seen in the region of the left ventricle until after the lungs have begun to fill.
The characteristic findings in a 7-mo-old infant with transposition of the great

WAGNER AND RHODES
Fig. 4. Nuclear angiocardiogrv, normal study. Upper frames: right heart phase. Lower frames: left heart phase. Lower right: equilibration image.
arteries is shown in Fig. 5. In the anterior view, a vessel can be seen arising from the right ventricle, instead of the usual separation of the pulmonary ar- tery from the superior vena cava 3.1 set after intravenous injection. Activity can also be seen in an abdominal vessel (the aorta) prior to the filling of the lungs. The latter sign is seen particularly well in the lateral view which is obtained immediately after the anterior view.
Other abnormalities that can be detected by nuclear angiocardiography are summarized in Table 3. Table 4 gives the nuclear angiocardiographic findings useful in the differential diagnosis of certain cardiac malformations. In infants suspected of serious heart disease but with a structurally normal heart, the tracer study correctly demonstrates normal anatomy. Major advantages of such studies are safety and simplicity. The entire study can be completed within min- utes with only an intravenous injection. The radiopharmaceuticals used have no pharmacological effect. Prompt demonstration of abnormalities such as trans- position of the great arteries can expedite cardiac catheterization and, at times, balloon septostomy. With a provisional diagnosis made prior to catheterization, the time required and irradiation associated with fluoroscopy and catheteriza- tion can be reduced.
Although in properly selected cyanotic infants, the tracer procedure has been shown to be of value, we have not yet had the opportunity to explore another potential use of nuclear angiocardiography: the differentiation of patients with so-called innocent murmurs from those with potentially serious heart disease.

RADIOACTIVE TRACERS
TcV RV
Fig. 5. Nuclear angiocardiogram in 7-mo infant with transposition of great arteries with spetal defect; tine frames, anterior view. Aorta (Ao) arises from right ventricle (RV), filling the space beside the superior vena cava (SVC); right-to-left interventricular shunt; faint visualization of pulmonary artery (PA) and lung after left ventricle ILV).
A hypothetical example is a teenager who, during a school physical examina- tion, is found to have a cardiac murmur. When this occurs, the physician must decide whether to permit vigorous sports, or to recommend procedures such as cardiac catheterization to clarify the diagnosis. We postulate that nuclear angio- cardiography may be able to fill an important role between the clinical examina- tion of the patient and the more complicated, invasive procedures, in a manner analogous to the screening role of lung scanning in the diagnosis of pulmonary embolism.24~25
REGIONAL MYOCARDIAL BLOOD FLOW
Myocardial imaging after intravenous administration of the radioactive tracer 43KC1 shows decreased concentration of the nuclide in areas of myocardial
Table 3. Abnormalities That Can Be Detected by Nuclear Angiocardiography
(1 I Ddferentiation of cardiac from pulmonary
disease m newborn patients with cyanosis
(2) Prelimmary identification of transposmon
of great arteries, truncus artenosus. and
hypoplastvz right or left ventricle
(3) Differential diagnosis of “Innocent” murmurs
(4) Detection of aneurysms of great vessels
(5) DetectIon of pulmonary arteriovenous
flstulas

Table
4.
Su
mm
ary
of
Nucle
ar An
gioca
rdiog
raph
ic Fin
dings
in
Diffe
renti
al Di
agno
ses
of
Certa
in Ca
rdiac
M
alfor
mati
ons
RA
RV
PA
Lung
LA
. LV
A0
Norm
al he
ari
Norm
al siz
e
Tran
spos
ition
of
grea
t
arter
ies
Norm
al siz
e
Trun
cus
arten
osus
Norm
al siz
e
Pulm
onar
y
atres
ia wi
th
intac
t ve
ntricu
lar
sept
um,
hypo
-
plasti
c RV
Larg
e, wi
th
reflu
x int
o
WC
Aortic
atr
esla
Norm
al appe
aranc
e
Outlin
e of
bo
dy
and
pulm
onar
y ou
tflow
tract
RV
body
no
rmal
size;
no
pulm
onar
y
outflo
w tra
ct
RV
body
no
rmal
size.
No
pulm
onar
y
outflo
w tra
ct
Small
Norm
al ap
peara
nce
Origi
n fro
m
RV:
empt
y
spac
e be
side
svc
Not
visua
lized
afte
r RV
filling
: fai
nt
outlin
e af
ter
LV
filling
Not
visua
lized
afte
r RV
filling
No
visua
lizatio
n
Norm
al appe
aranc
e
Abno
rmal
persi
stenc
e of
ac
tivity
du
e to
lar
ge
L +
R sh
unt
Visua
hzati
on
afte
r RV
an
d PA
Faint
ac
tivity
afte
r LV
an
d PA
Visua
hzati
on
afte
r fill
ing
of
trunc
us.
Visua
lizatio
n
afte
r ao
rtic
filling
via
PD
A
Norm
al ap
peara
nce
Outlin
e af
ter
lung
phas
e
Outlin
e be
fore
lung
phas
e via
intra
card
iac
R -
Lshu
nt
Outlin
e be
fore
lung
phas
e via
inter
ventr
icular
R -
Lshu
nt
Outlin
e be
fore
lung
phas
e via
inter
atnal
R 4
Lshu
nt
No
visua
lizatio
n
Arise
s fro
m
LV;
later
al vie
w:
poste
rior
origi
n. fro
m
LV.
Anter
ior
view
outlin
es
afte
r RV
.
fills
spac
e be
slde
SVC:
lat
eral
view.
arise
s an
terior
ly.
from
RV
Outlm
e of
tru
ncus
afte
r LV
. fill
ing
spac
e be
slde
SVC
Later
al vie
w
anse
s po
sterio
rly
from
LV
Asce
ndm
g ao
rta
not
seen
; ac
tivity
in
abdo
mina
l ao
rta
afte
r PA
, via
PD
A
Abbre
viatio
ns
RA.
right
at
num
. RV
. rig
ht
ventr
icle.
PA.
pulm
onar
y ar
tery
; LA
. lef
t am
um;
LV.
left
ventr
icle:
Ao.
aorta
. PD
A.
paten
t du
ctus
aTten
osus
. IV
C.
Infer
ior
vena
0
cava
: SC
V.
supe
rior
vena
ca
va
z 0 -

RADIOACTIVE TRACERS 11
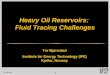
Fig. 6. Myocardial scan ob- tained after injection of ‘3KC1, showing decreased radioactiv- ity in infarcted region of myo-
cardium.
ischemia or infarction. Figure 6 shows the left anterior gamma camera image of a patient with extensive anterior and inferior myocardial infarction.
The particle distribution principle used for lung scanning has aIso been used to study regional myocardial blood flow. Compared to lung scanning, such stud- ies are more complex since the particles must be injected into the systemic cir- culation via cardiac catheter. The potential toxicity is also much greater. In lung scanning, intravenous injection of approximately 100,000 microspheres has a wide margin of safety because we obstruct only a fraction of a per cent of the pulmonary arterioles, and the collateral circulation is rich. There is cor- respondingly greater risk in myocardial scanning with particles.
The principal use of regional myocardial blood flow measurements to date has been in the pre- and postoperative evaluation of patients with myocardial infarc- tion treated with saphenous vein bypass. A typical study is illustrated by a 68- year-old man with angina pectoris and congestive heart failure studied at the Loma Linda University Medical Center. Arteriogram revealed occlusion of the right coronary artery. In order to evaluate the status of the capillary bed distal to the occluded artery, radioiodinated human serum albumin particles were in- jected via cardiac catheter into the right coronary artery and technetium-labeled albumin particles were injected into the left coronary artery. Anterior, right anterior oblique, left anterior oblique and lateral views of the particles’ distribu- tion was determined. Figure 7 shows typical views. There was persistently ab- sent perfusion to the area supplied by the posterior descending artery, mark- edly impaired perfusion in the area supplied by the circumflex system, and impaired perfusion in the distal left anterior descending artery. Because of the poor status of the collateral circulation, as demonstrated in the radioactive particle study, the decision was made that the patient would probably not benefit from a surgical procedure.

12 WAGNER AND RHODES

RADIOACTIVE TRACERS 73
Although these studies are still investigational, preliminary results attest to their safety and the usefulness of the data provided. It is likely that they will be used more and more in the future.
PULMONARY ARTERIAL BLOOD FLOW
Since its introduction in 1963, lung scanning has become the most widely performed radioactive tracer study of the cardiovascular system in clinical medicine. Why has lung scanning become so popular, when prior tracer methods for measuring regional pulmonary arterial blood flow, such as the use of radioactive 133Xe, remained restricted primarily to research laboratories‘? One reason is that lx3Xe studies were used chiefly in patients with obstructive lung disease rather than pulmonary embolism. Another reason is that, in 1963, rectilinear scanners were available in embryonic nuclear medicine depart- ments throughout the country. Thus, lung scanning with radioactive particles could be performed with equipment at hand. A final reason is related to the techniques themselves. With the original 133Xe method, blood flow measure- ments were made in a limited number of regions depending on the number of detectors employed, and the data were presented in numerical form, rather than as images. With the lung scan, regional blood flow was depicted in the form of an image, and the spatial resolution of the perfusion defects was greatly improved. Lesions as small as 2 cm in diameter could be detected and their size, shape, and position could be depicted in an easily understood form. A typical lung scan in a patient with pulmonary embolism is depicted in Fig. 8. The patient was injected with 2 FCi of 99mTc-labeled human serum albumin microspheres intravenously. Since the microspheres have an average diameter of 25 cc, they are removed from the circulation by the first capillary bed which they en- counter (the average diameter of capillaries is about 8 P). After intravenous in- jection, the microspheres are removed by the lung, and the regional concentra-
Fig. 8. Lung scan posterior view in patient with pulmonary embolism.

14 WAGNER AND RHODES
tion of radioactivity is directly proportional to regional pulmonary arterial blood flow.
One of the most important findings of lung scanning is that patients with all types of lung disease whether infectious, neoplastic, obstructive, or thrombo- embolic have decreased pulmonary arterial blood flow in the involved regions. Such lesions are not avascular or even hypovascular, but pulmonary arterial blood flow is reduced, and nutrient blood flow is provided chiefly by the bronchial arteries, which in the absence of right-to-left intracardiac shunting, do not con- tain radioactive particles injected intravenously.
Why is regional pulmonary arterial blood flow reduced in all pulmonary dis- eases? At times there is mechanical obstruction, e.g., a bronchogenic carcin- oma obstructing one of the pulmonary veins, or fibrosis resulting from pul- monary infection. At times, reduction in regional pulmonary arterial blood flow is related to alveolar hypoxia which results in arteriolar constriction and redis- tribution of unoxygenated blood to the more normal areas of lung.
The universality of perfusion defects in all types of lung disease has led to con- fusion in the interpretation of lung scans. How, one might ask, can lung scanning be helpful in the diagnosis of pulmonary embolism when all focal lung disease results in perfusion defects? The importance of this question justifies a detailed description of how lung scanning can be used in the differential diagnosis of pul- monary embolism.
First, let us consider a common error. A patient is referred to the nuclear medicine department because of suspected pulmonary embolism, and the nu- clear medicine physician sees a perfusion defect in the lung scan. He reports to the referring physician that the findings are “compatible with pulmonary em- bolism.” When the referring physician receives this report time after time he begins to wonder why he keeps referring patients since he can predict the report. Belief in his own omniscience is shattered, however, when he orders a pulmonary arteriogram for such patients and no evidence of pulmonary embolism is found. Should he rely only on the arteriogram for the diagnosis of pulmonary embo- lism? This policy is unsatisfactory because of the great number of patients with suspected pulmonary embolism. Performing cardiac catheterization and pul- monary arteriography in all these patients is not only undesirable but impossible. When interpreted properly, lung scanning can play an important role.
Before discussing interpretation of lung scans, a word about measurement of arterial oxygen saturation as a screening procedure for pulmonary embolism is needed. This test is not specific, since congestive heart failure, chronic obstruc- tive pulmonary disease and other cardiopulmonary abnormalities can result in low arterial oxygen saturation. What about its sensitivity in pulmonary em- bolism? In the large series of patients with proven pulmonary embolism studied in Phase I of the Urokinase Pulmonary Embolism Trial conducted by the Na- tional Institutes of Health, 12% of the patients with proven pulmonary embolism had arterial oxygen saturation over 80 mm Hg.
Is lung scanning more sensitive? Several years ago, we studied a series of 21 patients in whom the clinical diagnosis of pulmonary embolism was sufficiently certain that a pulmonary arteriogram was performed despite a normal four- view (anterior, posterior and both lateral) lung scan. None of the patients had

RADIOACTIVE TRACERS
Fig. 9. Lung scan posterior view in patient with pulmonary 1
venous hypertension. I
arteriographic evidence of pulmonary embolism. On the other hand, when the multiple view lung scan was interpreted as “high probability of pulmonary em- bolism,” 75% of the patients had filling defects in the contrast media at sub- sequent arteriography, and the remainder were abnormal, although the arterio- graphic findings were less specific. What criteria were used in the interpretation of the lung scans? All perfusion defects were not interpreted as being due to pul- monary embolism. Attention was paid to the characteristics of the perfusion defect in order to increase the relative specificity of diagnosis.
The criteria that we use to interpret lung scans are as follows: (1) If the four- view scan is completely normal, it is interpreted as having “no evidence of pulmonary embolism.” (2) If the blood flow to the tops of the lungs is greater than to the bases, with no evidence of perfusion defects in corresponding seg- mental arteries, the interpretation is “probable pulmonary venous hypertension without evidence of pulmonary embolism” (Fig. 9). (3) If a zone of decreased perfusion corresponds to one or more fissures, at times associated with increased blood flow at the top half of the lungs compared to the bases, without seg- mental perfusion defects, the interpretation is “probable pulmonary congestion or pleural effusion without evidence of pulmonary embolism” (Fig. 10). (4) Gen- erally decreased activity in one entire lung, seen best in the posterior compared to the anterior view, without segmental defects, is interpreted as “probable pleu- ral effusion without evidence of pulmonary embolism.” (5) Symmetrical perfusion defects, e.g., at both apices or at both bases, are interpreted as “probable paren- chymal lung disease, rather than pulmonary embolism.” (6) If there are one or more perfusion defects corresponding with segmental arteries either in associa- tion with a normal chest radiograph or a radiograph showing abnormalities, such as an elevated diaphragm, linear densities, small pleural effusions or hemispheral

16 WAGNER AND RHODES
Fig. 10. Lung scan right
lateral view of patient with pleural effusion.
densities at the periphery of the lungs, the interpretation is “high probability of pulmonary embolism,” provided the patient does not have obstructive lung dis- ease. The clinical history, timed vital capacity (FEV,), and regional ventilation measurements using *33Xe help determine whether the patient has obstructive lung disease. If he does, the interpretation is either “obstructive lung disease; we cannot say whether the patient has superimposed pulmonary embolism”; or “ob- structive lung disease; no evidence of pulmonary embolism.” This depends on whether or not the perfusion defects are segmental (first interpretation) or non- segmental (second interpretation). (7) If activity is seen in both kidneys after the injection of radioactive particles or microspheres, the interpretation is “right-to- left intracardiac shunt.” Such patients, if young adults, frequently are suffering from tetralogy of Fallot and have regional perfusion defects due to hypoplastic arteries (Fig. 1 I). (8) If all perfusion defects correspond with areas of infiltration, such as consolidation, the interpretation is “probable pulmonary infection.” Of course, the clinical manifestations are of great importance in the differential diag- nosis of pneumonia and pulmonary embolism. (9) If blood flow to one entire lung is absent, the interpretation is “high probability of neoplasm,” since hilar bron- chogenic carcinoma is more likely than pulmonary embolism. (10) If the perfu- sion defects follow a nonsegmental distribution with decreased blood flow in the medial parts of the lung, the interpretation is “pulmonary edema.” These find- ings are often seen in association with increased relative blood flow to the tops of the lungs and decreased blood flow along the fissures. If the patient has segmental perfusion defects superimposed on this or other patterns, the interpretation may be “pulmonary embolism superimposed on the underlying congestive heart dis- ease.”
Serial studies are often helpful. Nearly all patients with acute pulmonary em- bolism have a changing perfusion pattern within several days. Defects may im- prove or disappear while new ones may appear. If the perfusion defects remain unchanged, it is unlikely that the patient has acute pulmonary embolism, al-

RADIOACTIVE TRACERS 17
Fig. 11. Lung scan poste- .;: ; rior view in patient with tetral-
ogy of Fallot.
though he may have had embolism that occurred more than 3 mo prior to study. Parenchymal lung disease is often stable, although changing patterns may be ob- served in diseases, such as acute or chronic bronchitis.26
PERIPHERAL ARTERIAL BLOOD FLOW
Over the past decade, peripheral arterial reconstructive surgery such as femoral to popliteal artery bypass grafts have transformed treatment of femoral- popliteal occlusive disease. The selection of suitable patients remains a problem. The failure of arteriography to successfully predict the success of surgery in particular patients has led to an attempt to use radioactive tracer techniques to supplement the structural information obtained by arteriography with measure- ments of regional capillary perfusion. There are two general methods using radioactive tracers for determining capillary perfusion. One approach is the measurement of the rate of clearance of a diffusable tracer to determine blood flow to a localized area. The other approach is the microsphere distribution method to determine relative regional perfusion. Table 5 lists current and po- tentially useful studies of the peripheral circulation using radioactive tracers.
Local muscle or skin blood flow is determined from the disappearance rate of locally injected diffusible materials such as “.?Kr or laaXeT27.2x or by measuring the accumulation of radioactivity following intravenous injection of nondiffusible radiopharmaceuticais such as ‘“1I-albumin.2” It is necessary in assessing the de-

18 WAGNER AND RHODES
Table 5. Current and Potentially Useful Studies of Peripheral Circulation
lh.ease
Occlusive arterial
disease
Leg ulcers
Varicose veins
Gangrene
A-V fistula
Thrombosis
Type of Study
Intravenous radionuclide
artenography
Leg scan
Peripheral blood pool
dynamrc study
Leg scan
Peripheral blood pool
dynamic study
Leg scan
A-V shunt quantification
Peripheral blood pool
dynamic study
Scanning for thromboemboli
Use
lnitlal diagnosis when
contrast anglography
IS contramdicated
Differential diagnosis and
evaluation of revascularation
Detection of Incompetent
perforators as cause
To estimate prognosis
of healing
Evaluation of management
Planning of surgery
Detection and evaluation
of surgery
Initial dragnosis and
differentation from
cellulitis
Detection of thrombi
gree of arterial circulatory impairment to make measurements both at rest and at maximum vasodilation. Vasodilation is induced by whole-body warming, tem- porary sympathetic blockade, as with anesthesia, using 1% procaine, voluntary or electrically induced exercise,30 or by occluding the arterial inflow for 3-5 min prior to the test to induce reactive hyperemia. Normally, blood flow at rest lies
between 1.8 and 4 ml / 100 ml tissue / mm and increases by a factor of IO-20 during maximum vasodilation if there is no arterial insufficiency.
Relative regional perfusion is determined from radioisotope scans of the extremities following intraarterial injections of 99mTc or “3mIn-albumin micro- spheres or 13*1 macroaggregates of albumin.31
Initially, injections were made into each femoral artery, but it soon became apparent that a preferable technique was to inject microspheres labeled with 99mTc into the abdominal aorta via a translumbar needle. In this way, compari- son of the blood flow between the two legs, as well as within each leg, could be more readily made. In addition to delineating the regional distribution of blood flow, measurements of anatomic arteriovenous shunting could be made by mon- itoring the fraction of the injected dose that traversed the peripheral circulation to be eventually taken up by the pulmonary capillary bed.
The normal perfusion to the resting limb in a comfortable environment is expected to be distributed in proportion to the muscle masses. In patients with- out evidence of peripheral vascular disease in at least one leg, the scan showed radioactivity distributed chiefly to muscle. The normal perfusion scan is also seen in patients whose vascular disease is not severe enough to alter resting blood flow.‘0,3’
Abnormal leg scans include (I) diffuse distribution of radioactivity associated with generalized occlusive disease. In this case the blood flow is distributed primarily to skin rather than muscle masses. (2) Focal areas of decreased radio- activity as seen in patients with occlusive disease affecting primarily the distri-

RADIOACTIVE TRACERS 19
bution of certain branch arteries. (3) Focal areas of increased radioactivity. This is seen in areas of bone diseases such as Paget’s disease,32 fibrous dysplasia or osteoarthritis. Also hyperperfusion is seen in skin affected with dermatitis or in association with healing ulcers or wounds. One of the most promising uses of leg scanning is in patients with ischemic lesions of the lower extremities. In 21 patients whose limbs were in jeopardy, 13 showed increased activity, i.e.. hyperemia associated with the lesion. All of these healed with conservative therapy. Eight did not show hyperemia, and seven of these eventually required amputation because of nonhealing.
Figure 12 shows the leg scan of a man with arteriosclerosis, which is not signif- icantly altering the distribution of his blood flow at rest, i.e., this radioactivity is distributed proportionally to the muscle masses as is seen in the normal scan. Skin lesions in the areas of the knee show up as hot spots on the scan. Figure 13 shows more severe occlusive vascular disease, but the lesion on the left foot shows hyperemia, which indicates that there is probably enough blood supply to the area to permit healing with conservative treatment.
Perfusion scans of the extremities and quantification of arteriovenous shunt- ing with YqmTc microspheres have contributed to our understanding of Paget’s
Fig. 12. Leg and lung
scans anterior and posterior views obtained after injections of ssmlc-microspheres into each femoral artery and into a superficial vein. Venous injection was made in order to quantitate peripheral arterio- various shunting.

20 WAGNER AND RHODES
R Fig. 13. Leg scan after aortic injection of ssmTc-mi- crorpheres. Patient has arterio- sclerosis and hyperemia sur-
rounding ulcer on left foot.
disease of bone.32 The increased venous oxygen concentrations and increased cardiac output were formerly thought to be due to arteriovenous shunting through the diseased bone. By comparing the scans with x-rays, we see that the diseased bone is indeed hyperperfused. No significant arteriovenous shunting was detected in the seven patients whom we studied. Thus, the hemodynamic changes are due to increased flow through the capillary bed of Pagetoid bone, rather than through anatomical arteriovenous anastomoses greater than 15~ in diameter. Figure 14 shows the leg scan of a patient with Paget’s disease lo- calized to the left femur. It is interesting to speculate whether a form of treat- ment might be based on the finding that the blood flow to the involved region in patients with Paget’s disease is going through capillary-sized vessels rather than through anatomical arteriovenous shunts. If larger quantities of microspheres were injected into an artery leading to the involved region, perhaps regional blood flow could be reduced and pain and cardiovascular effects be diminished.
Arteriovenous shunt quantification has revealed that shunting through the

RADIOACTIVE TRACERS 21
Fig. 14. Leg scan in patient with Paget’s disease of left
femur. Aortic injection. R
L
extremities is not usually associated with occlusive vascular disease. The micro- sphere method is sensitive enough to detect anatomic A-V shunting in excess of 3%.34 This method appears to be potentially most useful in following patients with AV fistulae and hypertrophic pulmonary osteoarthropathy.35*36 We detected an 11% shunt in a patient with a high cardiac output otherwise unexplained.
DETECTION OF THROMBOEM BOLI
The detection of thromboemboli with radioactive tracers which specifically localize thromboemboli is feasible. Several substances are being evaluated for this purpose. Iodinated fibrinogen is useful in detecting forming clots.37-3Q How- ever, fully formed thrombi incorporate fibrinogen less readily, thus limiting its usefulness.3s*40 Clots also pick up radioactive particles when the radiopharma- ceutical is injected so that the material flows by the clot.4’ This can be used as an adjunct to lung scanning, in which case the radiopharmaceutical is divided into

22 WAGNER AND RHODES
two doses and injected into veins of the right and left feet. Both the lungs and the legs are scanned. Areas of uptake of radioactivity in the legs are noted at the sites of thrombosis. However, phlebitic lesions and varicosities may also result in focal points of radionuclide uptake.42
Radioiodinated antifibrin localizes in thromboemboli.43~44 Although patients have not reacted to injections of this radiopharmaceutical, it is potentially antigenic. Scans showing the clot sites are obtained I~-4 days after the injection. The blood levels of circulating tracer is high for several days; this nontarget back- ground limits the use of this agent45 as it does 13’1-labeled plasmin.
Radioiodinated streptokinase has been shown by autoradiographic techniques to be incorporated into blood clots. *‘Sag Recently, we have demonstrated that this radiopharmaceutical can be used to localize preformed pulmonary emboli in dogs.*’ Clots 1-48 hr old are readily visualized by scanning within 30 min after the injection of the tracer. Radiolabeled urokinaseSo also shows promise as a blood clot scanning agent. Labeled platelets and white blood cells are being evaluated for this purpose.
REFERENCES
I. Blumgart, H. L., and Weiss, S.: Studies on
the velocity of blood flow. III. The velocity of blood Row and its relation to other aspects of the circulation in patients with rheumatic and
syphilitic heart disease. J. Clin. Invest. 4: 149,
1927. 2. ~. and ~: Studies on the velocity of
blood flow. VII. The pulmonary circulation time
in normal resting individuals. J. Clin. Invest. 41399. 1921.
3. Wagner, H. N.. Jr.. Rhodes, B. A., Sasaki,
Y., and Ryan. J. P.: Studies of the circula- tion with radioactive microspheres. Radiology
4:374, 1969. 4. Rejali. A. M., Maclntyre, W. J., and
Friedell, H.L.: A radioisotopic method of visu- alization of blood pools. Amer. J. Roentgen.
79:129, 1958. 5. Wagner, H. N.. Jr., Sabiston, D. C.. Jr.,
Iio, M.. McAfee. J. G., Meyer, J. K., and Lan- gan. J. K.: Regional pulmonary blood flow in
man by radioisotope scanning. JAMA 187:601,
1964. 6. ~-, , McAfee, J. G., Tow, D. E.. and
Stern, H. S.: Diagnosis of massive pulmonary
embolism in man by radioisotope scanning. New Eng. J. Med. 271:377, 1964.
7. Anger, H. 0.: Scintillation camera. Rev. Sci. Instrum. 29:27, 1958.
8. Strauss, H. W., Hurley, P. J., Zaret, B. L..
Pitt, B., and Wagner, H. N., Jr.: Measurement of systolic and diastolic cardiac chamber volumes without cardiac catheterization. J.
Nucl. Med. 11:364, 1970.
9. Zaret, B. L., Strauss, H. W., Hurley,
P. J.. Natarajan, T. K.. and Pitt. B.: Scinti- photographic method for detecting regional ventricular dysfunction in man without cardiac
catheterization. New Eng. J Med. 284:1 165, 1971.
IO. Rhodes, B. A.. Greyson. N. D.. White.
R. I., Giorgiana, F., Williams, M.. and Wagner, H. N., Jr.: Leg scanning - characteristic per-
fusion patterns and clinical usefulness. Unpub- lished.
Il. Ross, R. W., Ueda, K., Lichtlen. P. R.,
and Rees, J. R.: Measurement of myocardial blood flow in animals and man by selective in-
jection of radioactive inert gas into the coro- nary arteries. Circ. Res. 15:28. 1964.
12. Endo, M., et al.: The direct diagnosis of
human myocardial ischemia using 13’I-MAA via selective coronary catheter. Amer. Heart J.
80:498, 1970. 13. Schelbert, H. R., Ashburn, W. L.. Cove]].
J. W., Simon, A. L., Braunwald, E.. and Ross, J. Jr.: Feasibility and hazards of the intra- coronary injection of radioactive serum al-
bumin macroaggregates for external myocardial perfusion imaging. Invest. Radio]. 6:379, 197 I.
14. Poe, N. D.: The effects of coronary arterial injection of radioalbumin macroaggre-
gates on coronary hemodynamics and myo- cardial function. J. Nucl. Med. 12:724. 1971.
15. Ashburn, W. L.. Braunwald, E., Simon. A. L., Peterson, K. L.. and Gault, J. H.: Myo- cardial perfusion imaging with radioactive-
labeled particles injected directly into the coro-

RADIOACTIVE TRACERS 23
nary circulation of patients with coronary artery disease. Circulation 44:85 I, 197 I.
16. Maseri, A., Manceni. P., Contini, C., Pesola. A., and Donato, L.: Method for the
estimation of total coronary flow by 9QT~ tagged albumin microspheres. J. Nucl. Biol. Med. 15:-
5x. 1971.
17. Hurley, P. J.. Cooper, M., Reba. R. C.. Poggenburg, K. J., and Wagner, H. N., Jr.: ‘3KCl: A new radiopharmaceutical for imaging
the heart. J. Nucl. Med. 12:516. 1971.
18. Yano, Y., Van Dyke, D.. Budinger, T. F., Anger, H. 0.. and Chu, P.: Myocardial uptake
studies with ‘29Cs and the scintillation camera. J. Nucl. Med. I I:1 I, 663, 1970.
19. Strauss, H. W., Hurley, P. J., Rhodes, B. A., and Wagner, H. N.. Jr.: Quantification
of right-to-left transpulmonary shunts in man. J. Lab. Clin. Med. 74:4, 1969.
20. Tow, D. E., Wagner, H. N., Jr., and
North, W. A.: Detection of venous obstruction
in legs with 99mTc-albumin. J. Nucl. Med. 8:277. 1967.
21. Rutherford, R. B., Krishna Reddy, C. M.. Walker, A. G., and Wagner, H. N., Jr.: A
new quantitative method of assessing the func-
tional status of the leg veins. Amer. J. Surg. 122:594, 1971.
22. Greyson. N. D., Rhodes, B. A., Williams, G. M.. and Wagner, H. N., Jr.: Radiometric
detection of venous diseases. Unpublished.
23. Wesselhoft, H., Hurley. P. J., Wagner, H. N., Jr., and Rowe, R. D.: Nuclear angio-
cardiography in the diagnosis of congenital disease in infants. Circulation 45:77, 1972.
24. Mason. D. T., Ashburn. W. L., Harbert.
J. C., Cohen, L. S., and Braunwald, E.: Rapid sequential visualization of the heart and great vessels in man using the wide-field Anger scintil-
lation camera. Circulation 39: 19, 1969.
25. Kriss, J. P., and Matin P.: Diagnosis of congenital and acquired cardiovascular diseases
by radioisotope angiocardiography. Trans. Ass.
Amer. Physicians 82: 109, 1969. 26. DeL.and, F. H.. and Wagner, H. N., Jr,:
Atlas of Nuclear Medicine, Vol. II. Lung and
Heart. Philadelphia, W. B. Saunders. 1970.
27. Kety, S. S.: Measurement of regional circulation by the local clearance of radio-
active sodium. Amer. Heart J. 38:321. 1949. 28. Lassen. N. A., Lindberg, I. F.. and Dahn.
I.: Validity of the xenon-133 method for mea- surement of muscle blood flow evaluated by simultaneous venous occlusion plethysmography.
Circulation Res. 16:287, 1965. 29. Krieger, H., Storaasli, J. P., MacIntyre.
W. J., Holden, W. D. and Friedell, H.: The use of radioiodinated human serum albumin in
evaluating the peripheral circulation. Ann. Surg. 136:357, 1952.
30. Pavoni. P.. Moen, T., Rhodes, B. A., and Wagner, H. N., Jr.: Changes in *33Xe clear-
ances resulting from electrically induced muscle
contractions. I. Study in dog. J. Nucl. Biol. Med. 15:16, II. Study in man. J. Nucl. Biol. Med. 15:19. 1971.
31. Izquierdo, G. F., Cuaron. A., Guerrero.
M.. Cobos. D., Trevino, H., and, Ramirez de Cervantes, M. E.: Scanning of the peripheral
circulation of the limbs. J. Cardiovasc. Surg.
(Torino)9:47, 1968. 32. Greyson. N. D., Rhodes, B. A., Hamilton,
C. R., Jr.. White, R. I., and Wagner. H. N..
Jr.: The absence of arteriovenous shunts in Paget’s disease of bone. Unpublished.
33. Gardner, T. J., Rhodes, B. A., Greyson.
N. D.. and Williams, G. M.: The clinical use-
fulness of leg scanning in arterial insufficiency using radioactive microspheres. Unpublished.
34. Rhodes, B. A.. Rutherford, R. B., Lopez-
Majano, V., Greyson, N. D., and Wagner, H. N.. Jr.: Arteriovenous shunt measurements in ex-
tremities. J. Nucl. Med. In press. 35. ~~: Blood flow through arteriovenous
anastomoses. In Horst, W. (Ed.): Frontiers of
Nuclear Medicine. Berlin, Springer-Verlag. 1971. p. 262.
36. Rutherford, R. B., Rhodes. B. A.. and
Wagner, H. N.. Jr.: The distribution of extrem- ity blood How before and after vagectomy in a
patient with hypertrophic pulmonary osteo-
arthropathy. Dis. Chest 56:19. 1969.
37. Hobbs. J. T.. and Davies, J. W. L: De-
tection of venous thrombosis with I-131 labeled
fibrinogen in the rabbit. Lancet 2: 134, 1960.
38. Atkins, P.. and Hawkins, L. A.: Detec- tion of venous thrombosis in the legs. Lancrt 2:1217, 1965.
39. Flanc, C.. Kakkar, V. V., and Clarke.
M. B.: The detection of venous thrombosis of the legs using lZsI labeled fibrinogen. Brit. J. Surg. 551742. 1968.
40. Seeker-Walker, R., and Potchen. E. J.:
Radiology of venous thrombosis-current status. Radiology lOl:449, 197 I.
41. Webber. M. M., Bennett, L. R.. Cragin.
M.. and Webb, R., Jr.: Thrombophlebitis
demonstration by scintiscanning. Radiology 97:620. 1969.
12. Rosenthall, L., and Greyson, N. D.: Ob- servations on the use of 99mTc-albumin macro-

24 WAGNER AND RHODES
aggregates for detection of thrombophlebitis. Radiology 94:413. 1970.
43. Spar, I. L.. Goodland. R. L., and Schwartz. S. I.: Detection of performed venous
thrombi in dogs by means of ‘311-labeled antibodies to dog fibrinogen. Circulation Res.
171322. 1965. 44. Reich, T.. Reynolds. B. M.. Healy. M..
Wang, M. C. H.. and Jacobson, J.: Detection of
venous thrombosis in the human by means of radioiodinated antifibrin-fibrinogen antibody. Surgery 60:121 I, 1966.
45. Spar, I. L.. Perry. J. M., Benz, L. L.. DeWeese, J. A., Mahoney, E. B., Izzo, M. J.,
Schwartz, S. I., and Yu, P. N.: Detection of left atria1 thrombi. Amer. Heart I. 78:731. 1969,
46. Ouchi, H., and Warren, R.: Detection of
intravascular thrombi by means of I-131 labeled plasmin. Surgery 5 I :42. 1962.
17. Gross, R.: Findings with labeled strep- tokmase in vitro and in viva. In. Proceedings of
9th Congress of European Society of Haematol-
ogy. Lisbon, 1963. Basel. S. Karger. p. 1342.
48. Pfeifer. G. W.: Distribution and placental
transfer of r3’1-streptokinase. Aust. Ann. Med.
Suppl. 19:18, 1970.
49. Siegel, M. E., Malmud, L. S.. Rhodes,
B. A., Bell, W. R., and Wagner. H. N., Jr.: Scanning of thrombo-emboli with 13’1-strepto- kinase. Radiology, in press.
50. Rhodes, B. A., Turahi. K. S , Bell, W. R..
and Wagner, H. N . Jr.: Radioactive urokinase
for blood clot scanning. J. Nucl. Med. In press.