Embed Size (px)
Citation preview

1328
Points of View
RADIOBIOLOGICAL SUPPORT FORRADIOTHERAPY
WHAT KIND OF RESEARCH?
TIKVAH ALPER
Medical Research Council Experimental RadiopathologyUnit, Hammersmith Hospital, London W12 0HS
Summary The radiation response of mammaliancells varies not only with their origin
but also with conditions of growth; so laboratoryobservations on human or other mammalian cellsand tissues are inadequate as a guide to the modeof their response in situ. Thus there is no basis at
present, other than clinical experience, for prescribingthe most effective radiotherapeutic regimen for treat-ment of a given tumour. The problem is exemplifiedby results with a pair of rat-tumour lines of commonorigin and similar histology. Neutrons would be moresuccessful than conventional radiotherapy for one
member of the pair but less so for the other; whereasthe positions would be reversed if hyperbaric-oxygentherapy were under test. Thus radiobiological researchshould be directed towards uncovering biologicalcharacteristics associated with variations in radiation
response. To this end, the most suitable methods arenot necessarily those claimed to be "related to theclinical situation ", although these may be regarded asmore worthy of funding. On the other hand, muchmore quantitative information is needed from clini-cians on the relationship of dose to effect on bothhuman tumours and normal tissues.
RADIOTHERAPY by the neutron beam from theM.R.C. cyclotron at Hammersmith Hospital is judgedto have given sufficiently promising results to justifymassive investment in an additional medical cyclotronin Edinburgh.1 This demonstrates an optimistic viewof the future of radiotherapy, despite the assertionsometimes made that this method of treating canceris bound soon to be superseded. Indeed, the rateof success achieved by radiotherapy in treating someforms of the disease has increased impressively overrecent years. It is timely to examine the nature ofancillary research on the results of which further
progress might be made.To sterilise a tumour the clonogenic cells must be
" killed ", in the sense that they should no longer beable to proliferate; but the normal tissues must bespared as far as possible. The more that is learnedabout radiation damage to normal tissues, the morecertainly are these effects also being ascribed to thekilling of cells that would normally proliferate; butthere are wide variations in radiation response betweencells of different origin, with no characteristic that
puts normal and neoplastic cells into separate classesin that respect. The difficult task of achieving therequired discrimination in effects on normal andmalignant tissues has been eased by the developmentof high voltage machines, or massive sources of
energetic y rays, which enable the radiation dose tobe delivered more specifically than previously to thetumour volume: and great improvements in tech-
nique have flowed from the collaboration of radio-
therapists with physicists, who first evolved suitablemethods for measuring doses, and who nowadaysnormally contribute also to treatment planning andother aspects of radiotherapeutic practice. But inthe main the successes achieved by radiotherapists aredue to the accumulation of clinical experience. How-
ever, there are still many failures, and the hope offurther improvement now lies in the solution of
biological problems.A reasonable aim is than the radiobiologist
[should] be of the same practical value to clinicalradiotherapy as the physicist has proved to be ... " 2
and, perhaps because the Zeitgeist demands that bio-medical research be more " consumer-oriented ", thoseresponsible for the funding and organisation of radio-biological research may be induced to regard as mostworthy of support certain lines of work that are
claimed to be " applicable to the clinical situation ";whereas " basic " research, aimed at elucidating themechanisms by which radiation kills cells, engendersless enthusiasm. But I believe it can be shown thatmuch more research at that level will have to be donebefore the radiobiologist will be able to render supportanalogous to that given by the physicist.Presumably even those radiobiologists, and the
funding authorities, who most favour the " direct " or"
applied " approach would acknowledge that thefoundations of some large-scale clinical trials now inprogress were laid by observations on the sort of testsystems that are now out of favour. The attentionof radiotherapists was drawn to the possibility that
hypoxic cells in tumours might be sensitised, withouta concomitant sensitisation of normal tissues, by a
review 3 of evidence from work with yeast, bacteria,and plants, well before the evolution of methods fordelineating " survival curves " for mammalian cells.But there are characteristics of dose-effect relation-ships, besides the oxygen effect, that are common tohigher and lower cells. For example, it has long beenknown that the radiation response of bacteria dependsnot only on the cell line-so that a single gene muta-tion may make a great difference-but also, sometimesvery strongly, on methods of growth before and afterirradiation. As experimental evidence has accumu-lated, the same variability has been found in the
responses of eukaryotic cells. For some time afterPuck and his co-workers evolved techniques for
growing cultured mammalian cells into clones, andinvestigated the mode of their killing by ionisingradiation,4‘5 it was believed that this was more or lessuniform for all lines, and that what happened in apetri dish would happen also in vivo. If that were
true, good laboratory experiments could be devisedthat would indeed be directly relevant to the clinicalsituation. The uncomfortable truth is that the vari-
ability is greatest in respect of those that matter mostto the radiotherapist. Every one of these varies withcell line; and many of them vary within the samecell line, depending on biological as well as chemicalenvironment.A very important aspect of cell killing by radiation

1329
is the response to the first two to three hundred rads,the normal size of the dose fraction in a radiotherapyschedule. The reason is that much of that initial dosemay be expended in inflicting injury which is not initself lethal, but which predetermines the response to
larger doses, if these are given immediately. However,the sublethal injury is usually shed or " repaired " be-tween one dose fraction and the next, if there is sufficienttime. With daily fractionation, the " repair " is usuallycomplete, so that the cells in the irradiated tissues are
affected as if each dose fraction were inflicting the damagecharacteristic of the initial region of the dose-responsecurve. Clearly if the dose used in inflicting sublethalinjury (" quasi-threshold dose ", or " DQ ") is large, inrelation to the average dose required to kill a cell (" Do "),a total dose divided into daily fractions would kill farfewer cells than if it were given all at once. Thus theratio DQ/Do is very important for the outcome of a
course of radiotherapy. The patient would benefit ifthe ratio were large for clonogenic cells in normal tissuesbut small for malignant cells. But that position mightonly too easily be reversed. The ratio DQ/Do variesgreatly not only between cells of different origin butalso with a variety of conditions. Examples are cell-cycle stage, conditions of growth, and-very importantfor neutron therapy-quality of radiation. With eukaryo-tic cells, DQ/Do tends to become less, as the density ofionisation increases; but no characteristics have yet beenidentified that would enable the extent of the diminutionto be predicted for any particular cell line.An earlier aim of radiobiological research was to culture
human tumour-biopsy specimens-in petri dishes, or evenin laboratory animals-so that details of the radiationresponse could be studied. But this method of study doesnot permit conclusions about the response of those cellsin the tumours left in situ.6,7 These reservations applyalso to results of experiments in vitro on cells culturedfrom normal tissue. For example, cells cultured by Pucket al.s from human skin and other tissues evinced littleor no sublethal (and therefore reparable) injury; whereasdose-response curves delineated by counting clones formedin the irradiated skin of mice have shown that the valueof DQ is quite larger and this seems to be true also ofhuman skin. If the stem cells in skin survived accordingto the petri dish results, dose fractionation would be ofsmall benefit and the total dose normally given in a
course of treatment could be expected to leave the patientwith skin quite incapable of healing; whereas the radio-therapist has known for a long time that dividing thetotal dose into fractions has a significant effect, leavingenough stem cells to repopulate the irradiated area.
, The position today, then, is that tissue-culture techniques! have served the purpose mainly of establishing importantli generalities about the radiation responses of mammalian: cells, many of them confirming observations previously
’ made on lower cells. Predictions may now be made on thebasis of these generalities, but the details of the radiationresponse of a particular cell line can only be establishedby experiment; furthermore, the details of the responsein vivo cannot be determined from those in vitro. Yetit is the minutiae of all aspects of the cells’ radiation
! response in situ that will determine the relative successi of different methods of radiotherapy.j These complexities of mammalian cellular radiobiologyj have important implications for clinical trials that are
commonly supposed to be firmly based on radiobiological’
principles. Since there is no method for predicting theI responses of the clonogenic cells in specific tumours, wei can confidently predict that hyperbaric oxygen, or neutron1 therapy, is bound to be used, in randomised trials, onI many patients whose tumours would respond at least as
B well to " conventional " radiotherapy, if not better. An
,
illustration of the experimental basis for that statementcomes from work in this unit 10 undertaken with the objectof identifying tumour lines that differed in respect of theeffectiveness of neutrons relative to X rays, and then tryingto discover the biological characteristics that determinethe difference. Because of the difficulties associated with
determining dose-response in vitro, use was made of thetechnique developed by Thomlinson, relating dose to
the delay in growth from the size at irradiation to somearbitrary standard. Among the tumour lines investigatedwere a pair of spindle-cell fibrosarcomas, identified as
SSB1(a) and (b). They originated from a single spon-taneous tumour, parts of which were passaged and thenmaintained as separate lines. Histologically, there is
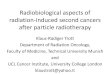
very little difference to be seen; certainly nothing thatcould be associated from any present knowledge withdifferences in radiobiological response. Indeed, there islittle difference in the response to X rays at low doses;but, with higher doses, it is evident that the response iscontrolled by hypoxic (and therefore relatively insensitive)cells in one member of the pair, but not in the other(fig. 1). This is shown by the flattening of the dose-response curve at higher doses.l1 But the effect of neutronsis strikingly different for the two tumours, and, interest-ingly enough, higher values of relative biological effective-ness (R.B.E.) are observed with the line that gives noevidence of hypoxic cells (fig. 2).Our analysis of the results suggests the reason for this
striking difference. It may be inferred that, in responseto neutron irradiation, the survival curve for tumour lineSSB1(b) changes shape dramatically, as compared withthe X-ray curve, that is, the ratio DQ/Do becomes muchsmaller; whereas this change in ratio is much less in thecase of SSB1(a). Whether or not the inference is correct,the results demonstrate that there is a radiobiological basisfor some improved results with neutron therapy other thanthat usually quoted. Hypoxic cells are much less effectivelyprotected against the densely ionising particles engenderedby neutron irradiation than against X or y rays, so it iscommonly supposed that the advantage of neutron therapydepends on the presence of hypoxic cells in tumours-i.e.,that the rationale is the same as for hyperbaric oxygenradiotherapy. In fact, hypoxia in tumours may prove
Fig. 1-Relation between delay in growth and radiation dose fora pair of tumour lines with a common origin.The response to X rays is the same to about 1600 rad; with
larger doses SSBl(a) becomes relatively less sensitive becausethe response is governed by that of the hypoxic cells. However,the response to neutrons is much greater with SSB1(b) thanSSB1(a).lo .

1330
to be only a minor reason for any usefulness neutron
therapy proves to have.Let us consider tumours SSBl(a) and (b) as models for
human tumours, in patients participating in a hyperbaric-oxygen trial or a neutron-therapy trial. They would beimpeccably matched, of the same size, with the same
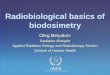
histology, and growing at the same site. With SSB1(a)it could be predicted that the breathing of oxygen at highpressure during irradiation would give a better resultthan air breathing (provided dose fractions were largeenough) : whereas there would be no advantage to thepatient with SSBl(b). Exactly the converse would betrue in the neutron-therapy trial. Neutrons will be moresuccessful than X rays only if their relative effectivenessis greater for the tumour than the normal tissues. Fig. 2shows that, with doses in the therapeutic range, the R.B.E.for SSBl(a) is as low as for some normal tissues, or lower,so the patient might well be better off treated by X rays.With SSBl(b), on the other hand, neutron therapy wouldbe triumphantly justified.
Surely it is the task of the most mission-oriented
radiobiologist to discover the biological subtleties thatdetermine phenomena of this kind. When ways aredevised of recognising microscopic or submicroscopicfeatures associated with large or small capacities forsublethal damage and its repair, with large or smallvalues of oxygen enhancement ratio, with great orsmall changes in survival curve shape, depending oncell cycle stage or radiation quality-then indeed thereis hope that the radiobiologist will be able to givethe radiotherapist the specific advice he needs on thebest form of treatment for a specific tumour..
If the right questions are asked, the answers canbe found, but by what means cannot be foretold. Theresearcher must not only be willing, but also free,to employ the most appropriate systems for testinghis hypotheses; and these are as likely to be bacteriaor biochemical systems in vitro as mammalian cells-
perhaps more likely. Some radiobiologists closely
Fig. 2-Effectiveness of neutrons compared with X rays, for rattumours SSB1(a) and (b), and damage to two normal tissues.The composite curves for normal tissue damage include
observations with fractionated doses. That relating to intestinaldamage is from observations on mice and rats; to skin damage,on mice, rats, pigs, and humans.I5 Neutron therapy cannot bemore successful than X or y rays unless the R.B.E. for the tumouris greater than for normal tissues at risk.
associated with radiotherapy seem rather unconcernedabout basic mechanisms of radiation action; perhapsbecause nothing of these has yet been learned fromwork with mammalian cells: but, more likely, becausethere is overemphasis on the notion that useful" applied " work can be done by radiobiologistsworking in radiotherapy departments. Since official
approval may readily be given only to experimentalprogrammes that are ostensibly " close to the clinicalsituation ", new ideas culled from observations on
other systems will fail to be tested in mammalian
cells, and therefore fail to be put to work to accountfor variability in their behaviour. The end result is
only too likely to confirm the view of some radio-therapists that radiobiology as a science is of no useto them and never will be.
However, those radiotherapists who are receptiveto the idea that radiobiological research may be ofvalue should not leave it all to the laboratory scieritist.The gap between experimental and human radio-
biology should be bridged from both sides. If theclinician recognises that human tumours are too
variable for any one change in procedure to be ofuniversal value, there is a way in which clinical trialscould be mounted that would demand fewer patientsand less effort than present schemes, for a significantimprovement to be shown. It has been suggested 12that trials should be based not on the site of a
tumour nor even on histological type, but ratheron tumours that are accessible for serial biopsy. The
highly accurate methods of prognosis developed byGlilcksmann and his colleagues 13°4 could then be usedto select patients for whose tumours the prognosiswith conventional radiotherapy was poor. Thesecould then be randomised and allocated to one or otherside of a trial. Besides the statistical and ethical
superiority of this approach, the biopsy specimenstaken during a course of radiotherapy would bevaluable material for study., As a long-term contribution, radiotherapists could,provide valuable information by making as accurateassessments as possible of measurable characteristicsof human tissues and tumours during and after irradia-tion. The staple information on which the radio-biologist depends is the quantitative relationship ofeffect to dose: much more of this sort of informationcould come out of the radiotherapy department thanis now available.
REFERENCES
1. University of Edinburgh Bulletin, January, 1974.2. Windeyer, B. Br. med. Bull. 1973, 29, 1.3. Gray, L. H., Conger, A. D., Ebert, M., Hornsey, S., Scott, O. C. A.
Br. J. Radiol. 1953, 26, 638.4. Puck, T. T., Marcus, P. I. Proc. natn. Acad. Sci. U.S.A. 1955, 41,
432.5. Puck, T. T., Morkovin, D., Marcus, P. I., Cieciura, A. J. J. exp.
Med. 1957, 106, 483.6. McNally, N. J. Br. J. Radiol. 1973, 46, 450.7. Fu, K. K., Phillips, T. L., Wharam, M. D. Personal communication.8. Emery, E. W., Denekamp, J., Ball, M. M., Field, S. B. Radiat. Res.
1970, 41, 450.9. Denekamp, J., Emery, E. W., Field, S. B. Radiology, 1971, 45, 80.
10. Howlett, J., Thomlinson, R. H., Alper, T. Br. J. Radiol. (in thepress).
11. Thomlinson, R. H., Craddock, A. Br. J. Cancer, 1967, 21, 108.12. Walter, L., Alper, T. Br. J. Radiol. (in the press).13. Glücksmann, A. ibid. 1941, 14, 187.14. Walter, L., Harrison, C. V., Glücksmann, A., Cherry, C. P. Br. med.
J. 1964, i, 1673.15. Hornsey, S., Field, S. B. Eur. J. Cancer (in the press).