Embed Size (px)
Citation preview

Radiographic assessment

Radiographic assessment
– Valuable Dx tool
– To help assist in etiology and Dx; curve magnitude; skeletal age; wedging; Rotation.
– P - A view is better…for reduction of radiation to visceral organs and breast tissue. Use rare earth screens to help minimize radiation in adolescent patient’s

A left view of the wrist is obtained to determine skeletal age.(Left wrist view comparison with standard atlas of Greulich and Pyle)
Most Accurate
Skeletal age is more importantthan Chronological age:
May vary months or years…veryimportant for prognosis
Risser Sign
– Use the A - P or P - A view to evaluate the Risser sign.
– A secondary ring apophysis (growth plate) develops over the top of each iliac crest.
– The apophysis will appear at the most lateral aspect of the crest near the A.S.I.S. and migrate medially toward the sacral ala. As the apophysis migrates, it is graded from 1 to 4 for females, and 1 to 5 for males.

Risser Sign
– It can be used as a prognostic indicator. A child with a low grade Risser sign (I.e., 1) and a scoliotic deformity of significant magnitude has a poorer prognosis than one who has a high grade Risser sign (I.e., 4) and equal curve magnitude.
– Low grade Risser…More growth potential and associated curve progression.
– High grade Risser…Less growth potential and less likely to demonstrate curve progression

Risser sign…4 for females, 5 for males.
Cobb’s Angle
–Locate the maximally tilted vertebral bodies in the curvature in the AP-PA projection
–Draw a line through the top end plate of the most superior and bottom end plate of most inferior vertebrae involved towards the concavity.
–Construct perpendicular lines through these and measure the acute angle

Draw a line through the top end plate of the most superior vertebrae, and through the bottom end plate of most inferior vertebrae...toward the concavity.

Draw a line through the top end plate of the most superior vertebrae, and through the bottom end plate of most inferior vertebrae...toward the concavity.

Draw a line through the top end plate of the most superior vertebrae, and through the bottom end plate of most inferior vertebrae...toward the concavity.

Construct perpendicular lines through these vertebrae and measure the acute angle


Treatment protocol
This illustration represents treatment protocol in 1674.
Note: Axial traction, pelvic traction, transverse loading, three-point bending, viscoelastic creep, and relaxation are all well demonstrated.

Treatment Protocol
–Correction belt(s) at apex of thoracic curvature.
–Holding belts on both sides of the correction belt.
–Lateral flexion of table towards apex of lumbar curve if present.

Treatment Protocol
–20 minutes daily
–5x/week…re-evaluate after two weeks.
–14-20 weeks…stability desired.
–Apply stretches & Myofascial protocol
–Adjust accordingly

Scoliosis
• Correcting straps are placed medial on the bracket
• Holding straps are placed lateral on the bracket
Medial side
Lateral side

Scoliosis
– Correcting straps bracket is placed opposite the convexity of the patient’s curvature
– Holding straps bracket is placed on the same side as the convexity

Scoliosis
– Straps are laid out before you position the patient on the table
– Abdominal piece is not lowered
Scoliosis
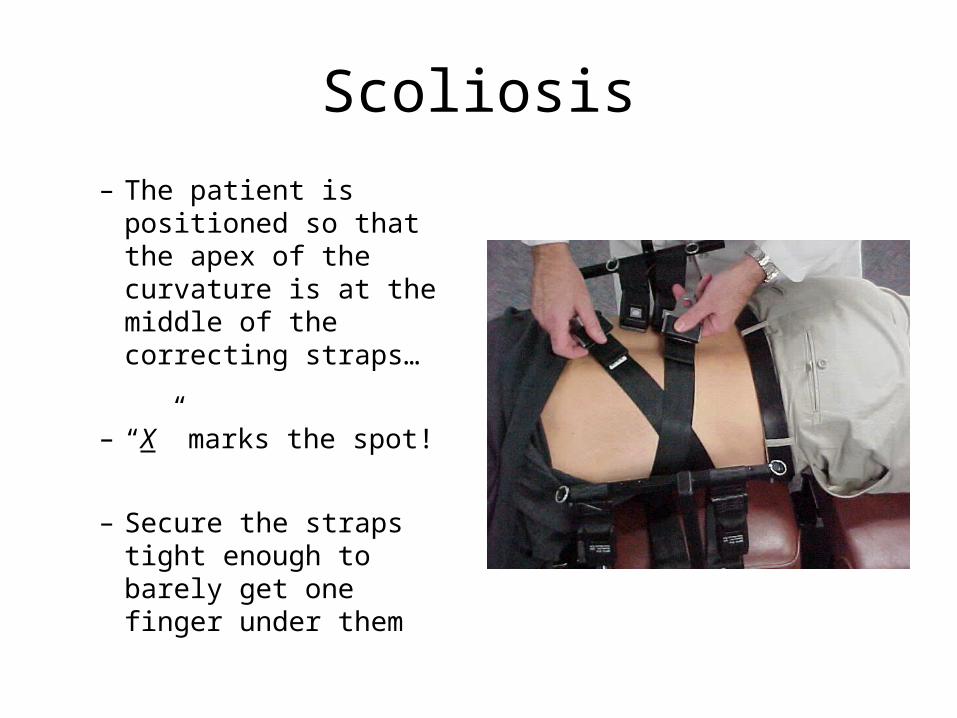
– The patient is positioned so that the apex of the curvature is at the middle of the correcting straps…
– “X” marks the spot!
– Secure the straps tight enough to barely get one finger under them
Scoliosis
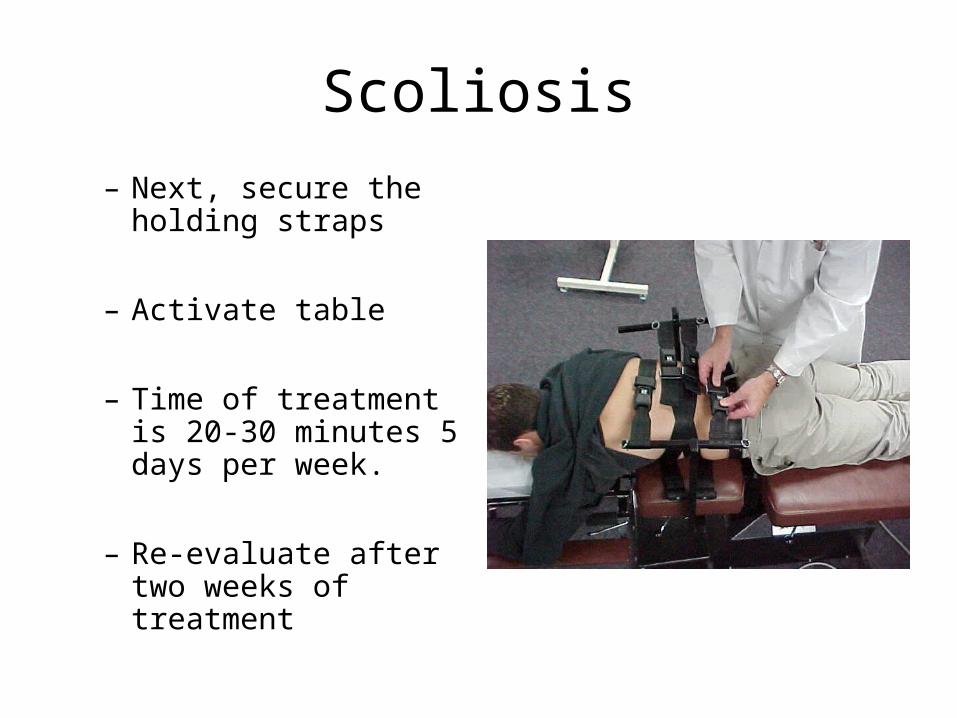
– Next, secure the holding straps
– Activate table
– Time of treatment is 20-30 minutes 5 days per week.
– Re-evaluate after two weeks of treatment

Scoliosis
• In the case of a double curvature, lateral flex the table toward the convexity of the lumbar curve.

A: Thoracic - 41° Lumbar - 25°
X-ray BTwelveminutes after X-ray A
B: Thoracic - 13° Lumbar - 9°

Thoracic: Pre - 41°
Post -32°
14 days of treatment
Lumbar: Pre- 25 °
Post 20 °

Treatment protocols
• Adjust Accordingly• TMAP• LMAP• Pelvic & CMAP
• Apply stretches & Myofascial protocol
• Psoas & Q.L.• X,Y,Z• Basic; Advanced;
Appendicular
Goals of the manipulation of the
scoliotic patient include the following:
• Alleviation of facet subluxations of the spine.
• Increased spinal flexibility.

Normal Facets Treatment Protocol
– Morris states that 70 % of the superimposed body weight is carried on the vertebral bodies and 30 % on the articular facets.
Morris JM, Lucas DB, Bresler B: Role of trunk in stability of the spine. J Bone Joint Surgery 43A: 327, 1961
Treatment ProtocolFacet - Abnormal
– It is obvious that weight distribution on the facets change with degenerative disc disease, in which narrowing of the disc places disproportionately more weight on the articular facets…as high as 47% to 70%

Treatment protocol
Goals of the manipulation of the scoliotic patient include
the following:
• Alleviation of facet subluxations of the spine.
• Increased spinal flexibility.

Treatment Protocol
• Panjabi presents the following algorithm of the stages of injury to the F.S.U.
• 1. Asymmetric disc injury at one F.S.U. level• 2. Disturbed kinematics of F.S.U.’s above and below• 3. Asymmetric movements at facet joints• 4. Unequal sharing of facet loads• 5. High load on one facet joint resulting in intra articular
cartilage degeneration, joint space narrowing, and facet atrophy.

Treatment protocol
• Alleviation of facet subluxations of the spine. White theorizes that malalignment of spinal facets may be the initial precipitating condition in the development of an adolescent deformity.
• “Facet fixations may set off a chain of events leading to asymmetrical loading on the epiphyseal plates and to muscle and ligamentous imbalance, ultimately resulting in curve progression”.
• This evolution of events, compounded with an adolescent growth spurt, may demonstrate how a benign flexible functional curve is transformed into a malignant progressive spinal deformity. Manipulation may be used to help restore normal facet orientation and intersegmental motion.
– Panjabi & White: Clinical Biomechanics of the spine.

Treatment Protocol
• Increased spinal flexibility is regarded as a positive prognostic sign. A rigid curve lacking flexibility is more likely to progress, and it is more difficult to control its progressive nature.
• A major contribution of chiropractic care for structural idiopathic adolescent curves will be to help increase spinal flexibility. Manipulation is used to derotate the spine and stretch shortened concave structures such as discs, muscle, and ligaments.

Other Treatment protocols for Scoliosis
– Utilize the flexion distraction table to help reduce the spinal curvatures…However, when necessary, refer out for other treatment plans and conservative care.
– Braces...Usually recommended for patients with curves 30-45°. 20-30° if there has been 5° or more curve advancement in the last year

Braces
– Milwaukee brace…introduced in 1946. The brace used counter pressure on the side of the patient, as well as distraction, to control the deformity. Generally used for thoracic curves with apices from about T7 upward.
– Boston brace (a.k.a. as the Wilmington brace). Treatment of choice for lower apical curves.
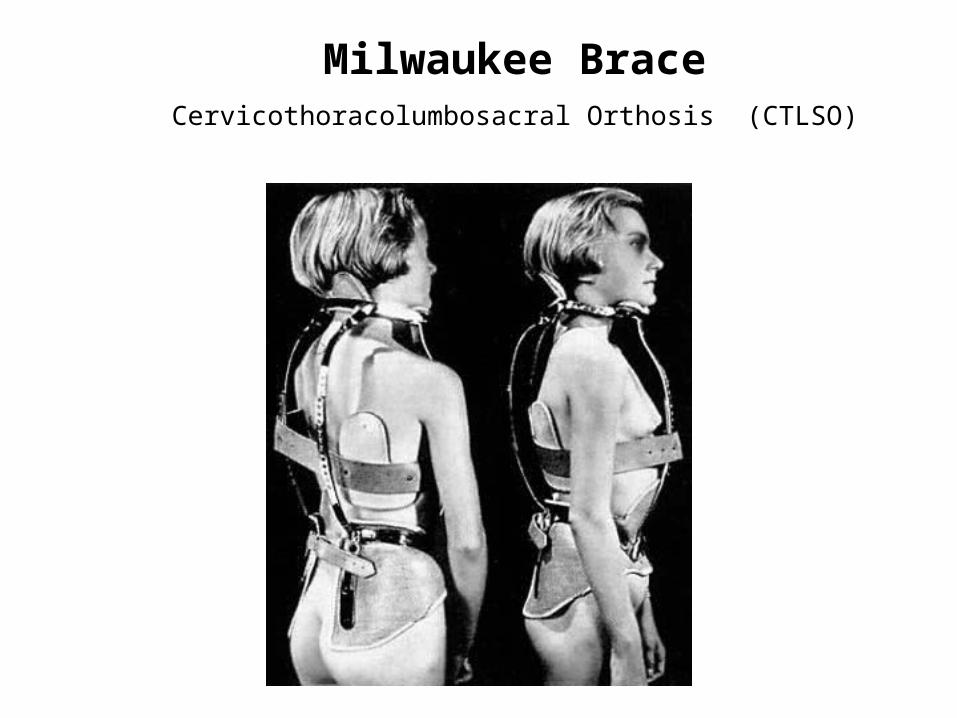
Milwaukee BraceCervicothoracolumbosacral Orthosis (CTLSO)


Boston BraceThoracolumbosacral Orthosis
(TLSO)