-
RadiographicOccultbonetrauma:CasePresentationandLiteratureReview
AnaCristinaManzanoDaz1
CarlosAlejandroGarcaGonzlez2
Summary
Thisarticlepresents13casesofpatientswithbonetraumaatthetimeoftheconsultation,
occult intheconventional radiographsandlater evidentinmagnetic
resonanceimaging
(MRI),.Medicalrecordsofthesepatients,incaseswhereXraysorCThadbeenreported
asnormal,werereviewedPersistent pain, with functional
impairment, unresponsive to
medical treatment was the most common feature leading to
clinical indication of MRI.
KeyWords(MeSH)
OccultFracture
Xrays
Magneticresonanceimaging
Woundsandinjuries
Introduction
1MDRadiologist.DepartamentodeRadiologa,HospitalUniversitariodeSanIgnacioPontificiaUniversidadJaveriana,Bogot,Colombia.2RadiologistResidentIV,DepartamentodeRadiologa,HospitalUniversitariodeSanIgnacioPontificiaUniversidadJaveriana,Bogot,Colombia.
1
-
Somebonelesionscausedbyacutetraumaorunusualmechanicalloadarenotdetectedon
conventionalradiographs,eitherbecausetheyareunapparentorduetodiagnosticerror.
Magneticresonanceimaging(MRI)hasbeenprovedtobeausefultooltodiagnosethese
occultXrayslesions,duetoitshighspatialresolutionandabilitytodiscriminatedifferent
typesof tissue(1).Thisdiagnostic methodis
indicatedforstressfractures, avulsionor
hiddenfractures(2).Patients
inwhichMRIhasbeenperformedforsuspectedmeniscal
injury, avascular necrosis or rotator cuff lesions, mayshow
radiographic hiddenbone
lesionssuchasintraosseoustrabeculardisruption,edema,hemorrhageorstresslesionsof
thetibialplateau,femoralcondyles,acetabulum,proximalhumerus,amongothers(3).We
present 13 cases of patients with trauma whose bone lesions were
unapparent on
conventionalradiographs,butevidentinmagneticresonanceimaging(MRI).
CASEPRESENTATION
Case1
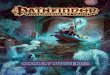
Occult fracture of the scapular glenoid. 69 y.o patient with
blunt trauma to his right
shoulder.Hecomesbackfivemonthslaterduetopersistenceofpain(Fig.1).
Case2
Occultfractureofthehumeralhead.45y.o.patientwithdirecttraumatohisrightshoulder.
Threemonthslaterhecomplainsofpersistentpainandrotatorcuffsyndrome(Fig.2).
2
-
Case3
Avascularnecrosisofthelunate.60y.opatientpresentswithhyperextensiontraumatothe
wrist.Onemonthlatershecomesinduetopersistentpain(Fig3).
Case4
Occultfractureofthescaphoid.A45yearoldpatientwithhyperextensiontraumatothe
wrist.Severalmonthslatercomplainsofpersistenceofpain.(Fig.4)
Case5
Occult fracture of the inferior pubic ramus 73 y.o.woman hit by
a car, whose initial
emergencyconsultationwasdiagnosedwithsofttissueinjuriesofthepelvis.8dayslater
duetopersistentpaininrighthipshecomesbacktotheemergencyroomwhereaCTscan
isordered..(Fig.5).
Case6
Occultfractureoftheacetabulum.79y.o.patientwithlefthipinjury.Hecamebackten
dayslaterasheremainssymptomatic,andanMRIwasperformed(Fig.6).
Case7
Occult fractureofthepatella.. 27y.opatient
withblunttraumatohisrightknee.The
patientcontinuedwithpain,soMRIwereperformed,(Fig.7).
3
-
Case8
Occultfractureofthetibialspine29y.o.axialtraumatohisknee.Duetothepersistentpain
andfunctionallimitation,MRIwasperformed(Fig.8).
Case9
Occultfractureofthetibialplateau.30y.o.patientwithrightkneeinjuryoccurredin
a
trafficaccident.15dayslater,hereferspersistentpain,soanMRIwasperformed.(Fig.
9).
Case10
Occultfractureofthefibula.42y.o.patientpresentswithblunttraumatohiskneeafterin
amotorvehicleaccident.Theinitialradiographshowednofractures.Thepatientconsulted
againonemonthlaterduetopersistentpainandlimp(Fig.10).
Case11
Occultfractureofthetalus48y.o.patientpresents
withtraumatohisheel afterfalling
froma1meterdistance.Painandfunctionalimpairmentpersist(Fig.11).
Case12
Bonecontusionofthecalcaneus.Apatientwith53yearsoldwhohasablunttrauma(axial
load)ofthefoot.Hehadaconsultationamonthlaterduetopersistentpain(Fig.12).
4
-
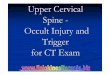
Case13
Stressfractureofthetalus.Apatientwith56yearsoldwithpersistentpainintheankleand
nohistoryofobvioustrauma.T1sagittalMRIoftheankleshowedastressfractureofthe
talus(Fig.13).
Discussion
TraumaticboneinjuriesthatareocculttoconventionalXraysare:bonecontusion,stress
fracturesandfractures.
Bonecontusion
Bonecontusionorbruisingofthebone"isatrabecularboneinjurythatcanresultinpain
andfunctionalimpairment(1).Itisinvisibleonconventionalradiographs,asitrepresents
bonemarrowedemaandmicrofractures,withoutinterruptionofthecortexInMRIbone
contusions are readily evident as bone marrow edema and
hemorrhage and appear
hyperintenseonT2weightedfatsuppressedimages,(1)(Case5).Itcanbeseenasearlyas
1to30hoursaftertheinjury(4),Theaveragetimeofclearanceofabonecontusionis42
weeks(5).
88%ofbonecontusionsinthekneedisappearin16months,butcanbepresentuptotwo
yearslater(6).Diffusionimages
aremoresensitivethanspinechotechniquestoquantify
edema.Therearemanycausesofbonemorrowedema,includingbonecontusion,whichis
5
-
oneofitsfewreversiblecauses.(7).Differentialdiagnosisincludeinfiltrative,neoplastic,
rheumatologicdiseases,,transientosteopenia,etc.
Ahistoryoftraumaisthemaindiagnostickey.Closefollowupofpatientsisadvisableto
ruleoutcomplications,sincebonecontusionscanprecedefracturesorarticularcollapse.
Nobonecontusionshouldbeconsideredinnocuous(8).Bonecontusionsareproducedby
directblow,axialcompressionofadjacentbonesortensileforcesinanavulsioninjury.
Locationofthebonecontusioncanpredictthemechanismoftraumaandassociatedlesions.
Traumainsportsinvolving kneeflexionandvalgusforces
presentbonecontusionsof
lateralfemoralcondyleandlateraltibialplateauassociatedwithanteriorcruciateligament
tears(9).
Inwristtrauma,bonecontusions arecommon,occurring
inupto63%ofpatientswith
normalradiographsandpersistentpain.Themostfrequentlyfracturedbonesarescaphoid,
thelunateandthetriquetrum,respectively(10).
StressFractures
Stressfracturesareinjuriesresultingfromrepetitivemechanicalforcesonnormalbone.
Earlyfindingsincludebonemarrowhyperemia,hemorrhageandedema.Ifabiopsyshould
beperformedinstressfracture inearly stages, it
couldsuggestaneoplasm,duetothe
presenceofimmaturecellsintherepairingprocess(1).MRIalsocandetectbonemarrow
edemaandthefracturelineillbeidentifiedwhileabonescanshowsnonspecificuptake(1).
Xraysarenormal,inparticularatthisstage,whileT2weightedimagesarehighlysensitive
toidentifyboneedemaandT1andT2weightedimagesidentifythefracturelineextending
6
-
through bone marrow and cortex.(Fig. 13). As time passes by, up
to six weeks for
diaphyseal lesions and four weeks for metaphyseal fractures, The
fracture can be
identifiedonlyinvolvingonecortex
andmayormaynotbeassociatedwithperiosteal
reactionandsomeendostealboneformation(2).
Fractures
Aradiographically occult fracture is one that was initially
unapparent on the Xray or
unnoticedbytheobserver (2). Thesemaybeincomplete
ornondisplacedfractures (1)
usuallyinvolve
epiphysisandmetaphysis,unlikestressfractureswhichoccurmostlyat
themetaphysis.On
MRIitpresentsasalowsignallinearlesion(bestvisualizedinspin
echoT1andT2weightedimages),surroundedbyalargearea,
ofpoorlydefined,bone
marrowedema(2)(cases18).Thefractureiscontinuouswiththecortexandextendsinto
thebonewithaperpendicularorientationtothecortexandthetrabeculaethatunderwent
theabnormal
weightorforceofthetrauma.IlldefinedlowsignalareasonT1weighted
images or cortical irregularity may represent an osteochondral
injury (2). All occult
fractures have a good clinical outcome and, on average, patients
reintegrate to daily
physicalactivityinthreemonthstime(6).
Inthehandandwrist,themostcommonfractureoccursinyoungadultscaphoid,witha
highcomplicationrateofnonunion,delayedunionoravascularnecrosisofthisbone(11).
Iftheinitialradiographisnormalandclinicalsuspicionishigh,aCTscanorMRImustbe
performed(2).Inmanyclinicalsettingsthediagnosismaytakeuptotwoweeksormore
7
-
beforethefracturebecomesapparentinthexray,duetoboneresorption(2).Treatment
consistsofsixmonthsofimmobilization(1114)(cases3and4).
Intheshoulder,occultfracturesofthegreatertuberosityarethemostfrequentandsimulate
rotatorcufflesionswhich,additionally,mayevencoexist.
Theyareusuallyunapparentwhenthereisnodisplacementoffragments(15)(cases1and
2).Thekneeisthejointmostofteninjured(2).
Radiographicoccultbonelesionsofthe
kneehavean incidence of16%inMRI(8). Theyareusually located on
thefemoral
condylesandthetibialplateau.Theymayextendverticallyandrarelycrossgrowthplates
(15). Avulsionfractures of the lowerpoleof thepatella occur
mainly in the immature
skeleton of patients that practice vigorous knee extension. (2).
MRI identifies a non
displacedfracture.Lesionsoftheposteriorlateralcomplex,thebicepstendonandlateral
collateralligament,areassociatedwithavulsionfractureofthefibularhead(2)(cases7
10).
Inthehip,theincidenceofoccultfracturesis2%10%inpatientswithpersistentpost
traumaticpain(11).InelderlypatientsitiseasilydetectedonMRI,whereasaCTscanmay
benormalinthefirstdaysaftertrauma(1).SomecentersperformasingleT1weighted
coronalimage,whenanoccultfractureissuspectedinthehip.Costislowercomparedto
othermorecomplexprotocolsandmaybediagnosticonitsown.(13)(Cases5and6).In
conventionalradiographs,theobturatorfatplanesigncanindicateanoccultfractureofthe
acetabulum(14).Italsoshouldbesuspectedinelderlypatientswithmildtraumatothehip
andposttraumaticpain(15).AMRIofthehipismuchmoresensitivethanconventional
radiographandCTscanstodiagnoseoccultfracturesofthehip(16).
8
-
Italsoavoidsunnecessaryhospitalizationsanddelaysindefinitivetreatment(17).There
areevidencebasedalgorithmsfordiagnosesofoccultfracturesthattakeintoaccountthe
riskfactorsandtypeoftrauma.Identifiedriskfactorsinclude:femalegender,womenwith
osteoporosis, alcoholism, malnutrition, endocrine diseases,
advanced age, steroid use,
inactivityandpoorcalciumintake(18).
Inthefootandankle,talarfractureoftenoccursatitsneckordome,indorsiflexionor
inversion trauma. Scaphoid fractures occur in athletes and are
usually due to stress.
Diagnosiscantakeup4months(7)(cases11and12).
Inarecentcostanalysissegmentstudy204pediatricpatientswithtraumaandnormalinitial
radiograph were followed up. 13% had fractures and, of these,
29% had not been
adequatelytreated.Halfofthepatientsdidnthavefracturesandweretreatedasiftheyhad.
Thecostofperformingmagneticresonanceinalimitedtraumaprotocol(onlyoneT1and
T2weightedimages
carriedoutinfiveminutes)iscomparablewiththedirectcostsof
inadequateinthesepatientsandcanbemuchlessthanthecostofadefinitivetreatment.If
alimitedtraumaprotocolMRIisperformed,tothesepatientstherewouldbeappropriate
immediatetreatment,especiallyimportantinchildrenwithhiddenSalterHarrisfractures,
withoutwastingresources(19).
Conclusion
The persistence of musculoskeletal pain that does not improve
with the conservative
treatment,itisthemostcommonsituationthatleadstopatientconsultingagaintoexplore
itscauses.DisablingorpersistentpaininpatientsshouldbestudiedwithMRItoruleout
9
-
occultbonelesions.Ourseriesofcasespointstotakespecialcareindetectinghiddenhip
fracturesinelderlypatients,andkneefracturesinyoungpatients.Wesuggestevaluating
thecosteffectivenessofMRI,performaunabbreviatedtraumaprotocol,forevaluationof
occultfracturesinaspecialgroupof
highriskpatientsinsteadofwaitingforpersistent
chronicpain.
References
1. Anderson M. Magnetic resonance imaging of radiographically
occult bony trauma.
WestJMed.1996JulAug;165(12):58.
2. Ahn JM, ElKhoury GY. Role of magnetic resonance imaging in
musculoskeletal
trauma.TopMagnResonImaging.2007Jun;18(3):15568.
3. Berger PE, Ofstein RA, Jackson DW, Morrison DS, Silvino N,
Amador R. MRI
demonstration of radiographically occult fractures: what have we
been missing?
Radiographics.1989May;9(3):40736.
4.
BlankenbakerDG,DeSmetAA,VanderbyR,McCabeRP,KoplinSA.MRIofacute
bonebruises:timingoftheappearanceoffindingsinaswinemodel.AmJRoentgenol.
2008;190(1):W1W7.
5.
BoksSS,VroegindeweijD,KoesBW,BernsenRMD,HuninkMG,BiermaZeinstra
SMA.MRIfollowupofposttraumaticbonebruisesofthekneeingeneralpractice.Am
JRoentgenol.2007;189(3):55662.
10
http://www.ncbi.nlm.nih.gov/pubmed/8855692?ordinalpos=189&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSumhttp://www.ncbi.nlm.nih.gov/pubmed/2727354?ordinalpos=252&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSumhttp://www.ncbi.nlm.nih.gov/pubmed/2727354?ordinalpos=252&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSumhttp://www.ncbi.nlm.nih.gov/pubmed/17762380?ordinalpos=22&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSumhttp://www.ncbi.nlm.nih.gov/pubmed/17762380?ordinalpos=22&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSum
-
6.
BoksSS,VroegindeweijD,KoesBW,HuninkMG,BiermaZeinstraSM.Followupof
occult bone lesions detected at MR imaging: systematic review.
Radiology.
2006;238(3):85362.
7.
BlumA,RochD,LoeuilleD,LouisM,BatchT,LecocqSetal.[Bonemarrowedema:
definition,diagnosticvalueandprognosticvalue].JRadiol.2009Dec;90(12):1789811.
8. Vannet N, Kempshall P, Davies J. Secondary collapse of
lateral femoral condyle
followingbonebruise:acasereport.ActaOrthopBelg.2009Oct;75(5):6958.
9. SandersTG , MedynskiMA, FellerJF, LawhornKW.
Bonecontusionpatternsofthe
kneeatMRimaging:footprintofthemechanismofinjury.Radiographics.2000Oct;20
SpecNo:S13551.
10. PierreJeromeC, Moncayo V, Albastaki U, Terk MR. Multiple
occult wrist bone
injuries and joint effusions: prevalence and distribution on
MRI. Emerg Radiol.
2009;17(3):17984.
11.
AhnJM,ElKhouryGY.Occultfracturesofextremities.RadiolClinNorthAm.2007
May;45(3):56179.
12. Lynch TC, Crues JV, Morgan FW, Sheehan WE, Harter LP, Ryu R.
Bone
abnormalities of the knee: prevalence and significance at MR
imaging. Radiology.
1989;171:761.
13. Quinn SF, McCarthy JL. Prospective evaluation of patients
with suspected hip
fractureandindeterminate radiographs: useofT1weightedMRimages.
Radiology.
1993;187(2):46971.
11
http://www.ncbi.nlm.nih.gov/pubmed/17601509?ordinalpos=24&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSumjavascript:AL_get(this,%20'jour',%20'Radiographics.');http://www.ncbi.nlm.nih.gov/pubmed?term=%22Lawhorn%20KW%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_RVAbstracthttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Feller%20JF%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_RVAbstracthttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Medynski%20MA%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_RVAbstracthttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Sanders%20TG%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_RVAbstract
-
14.
MouzopoulosG,LasanianosN,MouzopoulosD,TzurbakisM,GeorgilasI.Occult
acetabulumfracture:acasereport.EmergRadiol.2008Nov;15(6):4379.
15.
KakarR,SharmaH,AllcockP,SharmaP.Occultacetabularfracturesinelderly
patients:areportofthreecases.JOrthopSurg(HongKong).2007Aug;15(2):2424.
16. LubovskyM, Liebergall Y, Mattan Y, Weil Y, Mosheiff R. Early
diagnosis of
occulthipfractures.MRIversusCTscan.Injury.2005;36(6):78892.
17. VerbeetenKM,HermannKL,Hasselqvist
M,LaustenGS,JoergensenP,Jensen
CMetal.TheadvantagesofMRIinthedetectionofocculthipfractures.EurRadiol.
2005Jan;15(1):1659.
18. CannonJ,SilvestriS,MunroM.Imagingchoicesinocculthipfracture.
JEmerg
Med.2009Aug;37(2):14452.
19.
KanJH,EstradaC,HasanU,BracikowskiA,ShyrY,ShakhtourBetal.Management
ofoccultfracturesintheskeletallyimmaturepatient:costanalysisofimplementinga
limited trauma magnetic resonance imaging protocol. Pediatr
Emerg Care. 2009
Apr;25(4):22630.
Figures
Fig. 1. Occult fracture of the scapular glenoid. (A) The initial
radiograph shows no
fracture. Coronal spinechoT1weightedMRI(b)showsthefractureof
thesuperior
aspectoftheglenoid(arrow).
12
http://www.ncbi.nlm.nih.gov/pubmed/19382319?ordinalpos=2&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSumhttp://www.ncbi.nlm.nih.gov/pubmed/19382319?ordinalpos=2&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSumhttp://www.ncbi.nlm.nih.gov/pubmed/19382319?ordinalpos=2&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSum
-
Fig.2Undisplacedfractureofthegreatertuberosityofhumerus(N1).(A)Theinitial
radiographisnormal.CoronalspinechoT2weightedalowsignal
fractureline(black
arrow)visiblealsointhePDimage.(c).
Fig.3.Avascularnecrosisofthelunate.(A)Theinitialradiographshowsnoabnormality.
CoronalspinechoT2MRI(B)shows
hyperintensity(whitearrow)ofthelunatemedial
aspectdueavascularnecrosiswithcysticdegeneration.Notetheirregularityoftheulnar
insertionofthetriangularfibrocartilage,suggestiveoftear.
Fig.4.Occultfractureofthescaphoid.(A)Theinitialradiographshowsnoabnormality.
InCoronalspinechoT1weightedimage(B)showsthefractureofthescaphoidasalow
signalline(arrow)andcoronalSTIRT2weightedimage(c)showsaedemaofthebodyof
thescaphoid(arrow).
Fig.5.Occultinferiorpubicramusfracture.(A)Pelvisradiographshowsnofracture.)A
smallfracturewentunnoticedontheCTscan(b)(arrow).CoronalT2weightedimage(c)
showsedemaatthefracturesite(arrow).
Figure6.Occultfractureoftheacetabulum.(A)Hipradiographshowsnofracture.CT
coronal image of the pelvis is normal (b)l.Coronal T2 weighted
MRI demonstrates(c)
edemaandthelowsignalsfractureline(arrow)intheanterioraspectoftheacetabulum,
Fig.7.Occultfractureofthepatella.(A)Conventionalradiographshowsintraarticular
fluid.MultisliceCTscanwas(b)readasnormal.CoronalspinechoT2image(c)shows
13
-
edema of the lower pole of the patella (white arrow In
retrospect the fractures was
apparentontheCTscan,(whitearrow)asanavulsionfracture.
Fig.8.Occultfractureofthetibialspine.(A)Conventionalradiographshowsnofracture.
)CoronalmultisliceCtreformation(B)wasreadasnormal,althoughtherewasasubtle
fractureof themedial tibial plateaucortex(blackarrow).
CoronalT2weighted image
showed(c)edemaandanondisplacedobliquefracture(whitearrow)
ofthetibialspine
whichextendstothecortexoftheproximalmetaphysisofthetibia.
Fig.9.Occultfractureofthetibialplateau.(A)Initialradiographdoesntshowfractures.
T2weighted coronal image(B) shows edemaanda lowsignal line
(arrow) in the
externaltibialplateau.
Fig.10.Fibularoccult fracture.(B)Theinitial
radiographshowsnofracture.MRT2
weightedSTIRcoronalimagehidentifiesanextensiveedemaoftheheadofthefibula(c)a
lowsignalfracture(arrows),onthecoronalspinechoT1weightedimage.
Fig.11.Occultfractureofthetalus.(A)Theinitialradiographshowsnofracture.Sagital
spinechoT1images(b)demonstratesthetalarneckfractureasalowsignalline(arrow)
andsagittalT2weightedSTIRimages(c)showsassociatededema(arrows).
Fig.12.Calcaneusbonecontusion(a).Theinitialradiographshowednofractures.There
is anareaof sclerosis in theposterior tubercle of thecalcaneus
which represents the14
-
fracture.Thecoronal(b)andsagital(c)STIRT2weightedimagesshowhighsignalofthe
posteriorlateralaspectofthecalcaneus,representingboneedema.
Fig.13.Stressfractureofthetalus.T1weightedcoronalMRIshowsalinearfractureof
thetalus.(arrows).
Contact
AnaCristinaManzanoDaz
HospitalUniversitariodeSanIgnacio
RadiologyDepartment
Carrera7No.4062,piso2
Bogot,Colombia
[email protected]
Receivedforevaluation:October4th,2009
Acceptedforpublication:November17th,2009
15