-
radiosensitive tumorssuch as B cell lyinphomas in
patients(9,10), they havethe additionaladvantagethat theycanyield
precise information concerning biodistribution andtumor dosimetry.
These data can be useful for the selectionof the most
appropriatetype of antibody for radioimmunoscintigraphy and
radioimmunotherapy (9—19).
Monoclonal antibodies used for tumortargetingare generally
ofmurine origin and can elicit human anti-mouse IgGantibodies
(HAMA) in many patients (20—22).High titersof HAMA are
frequentlyobserved afterrepeatedinjectionsof MAbs or when they are
coupled to other immunogenicproteins such as toxins or enzymes.
Chimerization of anti
bodies representsa first step toward reducingthe immunogenicity
of MAbs for applicationin patients (1Z20,23,24).Immunogenicity is,
however, still a problem for certain chimericantibodies(25).
Furtherhumanizationby graftingonlythe
complementaiydeterminantregions(CDR)of the mouseMAb DNA into human
IgO DNA as described for the reshaped MAbs (26,27) or production of
human antibodies(28-30) might be necessaiy to further reduce
immunogemcity.
Chimeric antibodies allow the comparison of the biological
behavior of selected human IgO subclasses and verification of their
potential for tumor targeting.They can alsobe used to study
theireffector functions and the possibilityof obtainingfragmentsfor
immunoscintigraphyand radioimmunotherapy (1Z23,31,32). We have used
such chimeric anti-CEA MAbs of different IgG subclasses in
experimental animal models and could show that both theintact Ig02
MAb and its F(ab')2 fragment demonstratedexcellent tumor targeting
and in vivo stability (31). Thetumor localization capacity of the
intact Ig04 chimericMAb has been shown to be identical to the
origmal mouseMAb in tumor bearing nude mice (23). However, the
invivo behavior of chimeric 1g04 F(ab')2 fragments was
unsatisfactory in mice (32) and this fragment was thereforenot used
in patients.
Here we compare the intact chimeric anti-CEA MAb
Biodistributionand tumoruptakeof a
chimerichuman-mousemonoclonalantibody(MAb)andthe
originalmouseMAbhavebeencomparativelystudied.Methods:
Eighteenpatientswithsuspectedcolorectalcancerscheduledfor
surgeryunderwentimmunoscintigraphywith
msWabaledthimedcanti-CEAMAb.Iodine-125and
1311trace-labeledchimericandonginalmouseMAb were
simultaneousiyinjectedfor
[email protected]:Similarserumkineticsanda
lowimmunogenlcftywereobservedfor
bothantibodies.Meanbindingcapadtyto
CEAmeasuredinPBSafterradiolabelingwasidenticalforbothMAbsandit
wasslightlydecreasedwhenmeasuredin serum1-4 hrafter
injection.Radiochromatogramsof patientssera
showedimmunecomplexformationrelatedtotheamountofcirculatingCEA.Postoperativeexvivoradioa@tMtycountingintissuesampiesrevealedsimilarantibodydistributionswithnotal@ysimilarantibodyuptakesintumors.Hightumoruptakes(between0.02to
0.06%injecteddoseperg)wereobservedin3 of 13patientsoperatedfor
pnmaryor metastaticcokxectalcancer.Concludon: In this
dual-labeltechnique,the radiolodinatedanti-CEA19G4chimencMAb and
the o@iginaImouse lgG1MAb wereshownto havevery similarbehavlOrin
colorectalcancerpatients.
Key Words:
chimencmonodonalantibody;carcinoembryonicantigen;tumoruptake;colorectalcarcinoma
J Nuci Med 1995; 36:420-429
he concept of using monoclonal antibodies (MAbs) ascarriers to
deliver cytotoxic drugs, radioisotopes or toxinsmore selectively
into tumors continues to stimulate experimental and clinical
research (1—3).While radiolabeled antibodies have been shown to
be useful for therapy of human carcinomas in nude mice (4—8),and
of more
RecolvedMay31,1994;revisionacce@*edSept20.1994.Forcorrespondenceandrepdntscont@FranzBuchegger,MD,D@scnof
NudearMedicine.CHIN,CH-1011Lausanne,Switzerland.
420 TheJournalofNudearMedicine•Vol.36•No.3 •March1995
Radiolabeled Chimeric Anti-CEA MonoclonalAntibody Compared with
the Original MouseMonoclonal Antibody for Surgically
TreatedColorectal CarcinomaFranz Buchegger, Jean-Pierre Mach,
AndréPèlegrin,Michel Gullet, Charles-AndréVogel, Thierry
Buclin,Jean-Etienne Ryser, Bernard Delaloye, and Angelika Bischof
Delaloye
DivL@ionofNuclear Medicine, Depamnentr ofSwgety and Clinical
Pharmacolo@, Centre Hospitalier Unive,@itaireVaudoLr and I,t@titute
ofBiochemist,y, Univei@y ofLausanne, Lausanne, Switzerland; and
L@epa,iment of NuclearMedicine, HOpital Cantonal Universitaire,
Genève, Switzerland
-
(humanI@G4)with its originalmurineIgG@MAb by differential
labeling, co-injection and cx vivo measurement oftumor and normal
tissue radioactivity distributionsin patients.
METhODS
PatientsPatients selected for the
comparativebiodistributionstudy of
chimericand mouse anti-CEAMAb (n = 18)were suspectedofcolorectal
cancer. Surgerywas planned 1 to 5 days after MAbinjection.
Immunoscintigraphy was performed with the aim ofstaging more
precise'y the disease. Definitive diagnosis in thesepatients was:
primary colorectal adenocarcinoma in nine patients,
one of whom had initialliver metastasis, one local
recurrenceandfive liver metastases. One patient had an ovarian
carcinoma, onepatient a benign polyp and one patient with a
suspicion of liver
metastasis had no tumorat the time of surgery. For threeof
thesepatients, surgely was either performed too late after
antibodyinjectionor was cancelled.For determinationof the serum
halflifeof chimericMAb,nineadditionalpatientswereincludedwhowere
only injectedwith chimericMAb andhada follow-uptimeof2 to 6 days.
Finally,one patientincludedherehadsurgeiyforalivermetastasis8 days
after injectionof 2 mgof the IgG4chimericMAb together with 30 @gof
a chimeric MAb with the samevariableregionsbut with
humanIgG2constantdomains(32).
Monoclonal
AntibOdiesThemouse-humanchimericmonoclonalantibodyusedhereis
of humanI@G4subclassandwas derivedfromthe
murineMAbCE25/B7(6,23)(CIBAGEIGY,Basel,Switzerland).ThisMAbisdirected
against the epitope Gold 4 of CEA (33). It has a highspecificity
for CEA (34) and does not crossreact with NCA-55 orNCA-95 (35) or
other granulocyte glycoproteins.
Theoretically,themurineandchimericantibodysubclassesbothhaveminimaleffector
functions: they should not react with Fc receptors onmonocytesand
macrophagesand shouldnot activatethe complement cascade (36). The
original mouse MAb has been used inpatients both for
immunoscintigraphy(14) and in a first trial
ofrsdioimmunotherapy(1). MouseMAbwas preparedfromascitesby ammonium
sulfate precipitation and ion exchange chromatography(6).
ChimericMAbwas producedin Sp2@cellstransfectedwitha
singlevectorcontainingboththechimericheavyandlightchaingenes
(23).
RadlolabelingTwo to 4 mg of chimeric MAb were labeled by the
iodogen
methodwith 15 to 30 mCiof ‘@Ifor
immunoscintigraphy(finalspecific activities were 2 to 4.5 mCi per
mg antibody and 4 to 18mCiwere injectedper patient). Batches of 0.2
mg chimeric MAband oforiginal mouse MAb were separatelylabeled
using 250 @.tCiof 1@Iandof
‘@‘i,respectively(finalspecificactivitieswere0.8to 1.1
@&Ciper@ antibodyfor the trace labelings).For
threepatients,thetracelabelingswerereversedandthechimericMAbwas
labeled with ‘@‘Iand the mouse MAb with 1@I. Using
thepairedlabelingmethod,it ispossibleto
analyzethebiodistributionand tumor localizationcapacity of the two
MAbs in the samepatientand thus compare results obtained
underidenticalbiologicalconditions.The 1@I-labeledand the
trace-labeledMAbswerepooled, diluted in 100ml of0.9% NaCl and
perfused intravenouslywithin15 mm. Total amountof
injectedantibody(mouseandchimericMAbtogetheror
chimericMAbalone)rangedfrom2 to4 mgin all
patients.The15-mmperfusiontime(usedfor safety
reasons) does not significantly influence the
pharmacokinetic
analysisbecauseboth antibodieshave been injectedin the
sameperfusion and showed a very similar behavior in the hours
followinginjection.
T@*
Sam@sPatientserumwascollectedimmediatelyfollowingand1,4—6,
24 and 48 hr after injection;additionallyblood
samplingwasperformed during surgery (at the moment of tumor
removal).Tumorsamplesof primarytumorsor
localrecurrenceswereanalyzed together with normal colon and fat.
Normal colon tissuewas dissected into the normal mucosa, known to
contain CEA(37), and the rest of normalbowel wall. Liver
metastaseswereanalyzedtogetherwithlivertissuesurroundingthe
tumorandasmall biopsy of distantnormalliver and fat. The tumorwas
macroscopicallyseparatedfromnormaltissueand fromnecrosis.Tissue
samples were weighed and counted in a triplechannelgammacounter
togetherwith a sample ofthe injected material that servedas
referencefor the totalinjecteddose. Samplesstillcontaining1231were
counted again after complete decay ofthis isotope. Final
radioactivitymeasurementswerecorrectedforcrossoverof 1311inthe
1@Ichannel.
In Vitro Testing of Radlolabeled
MAbsTheinvitroimmunoreactivefractionof radiolabeledchimeric
and original mouse MAb was determined in a binding assay onCEA
insolubilizedon CNBr-Sepharose(Pharmacia,Uppsala,Sweden).Tento 50
nCiof radiolabeledMAbwereincubatedfor16hrat 25°Cin
PBSbuffercontaining1%normalmouseserumand1%normalhumanserumwith5
@dpackedCEA-Sepharose(containingabout2
@&gpurifiedCEA).Afterwashing,boundradioactivity was determined
as percent of input radioactivity. Similarly, patients, serum
samples obtained 1 to 4 hr after injection(containingsimilar
amounts of radioactivity)were diluted 113inPBS
buffercontaining1%normalmouseserumandwere alsoincubatedwith 5
@1packedCEA-Sepharose.Nonspecificbindingwas measured by incubation
with irrelevant protein also coupledto CNBr-Sepharose.Itwas
alwaysbelow2%andwas subtractedfromCEAbindingvalues.
Trichloroaceticacid
precipitationofradioactivityafterlabelingshowedthat morethan95%of
theradioactivity was bound to protein for all preparations.
MalytiCaIsize chromatographyof the radiolabeledMAbs was done on
aSephadexG-200columnor on a Superdex200
FPLCcolumn(bothPharmacia).Immediatelyafterlabeling,a
sharppeakwasobtainedforbothMAbswithoutdetectableamountsof
aggregatesandwithonlytraceamountsof freeiodine.
CEA and HAMA AssayCirculating CPA was determined in a serum
sample of each
patient taken before injection of radiolabeledantibodies using
apreviouslydescribedsolidphase enzymeimmunoassay(38).
HAMA and anti-idiotype antibodies were measured in
threesandwichassays.Briefly,forthethreetestsA, B andC,
polystyreneballswerecoatedwithA), irrelevantmouseIgG,B), mouseMAb
CE 25 or C), chimenc MAb, respectively. These balls wereincubated
for 3 hr at 25°Cwith 10 p1 patients serum (taken 5—6wkafter
antibody injection)diluted in 300 @lPBS and
peroxidasecoupledmouseMAbCE25(testA andB)orradiolabeledchimericMAb
in test C. A rabbit anti-mouse F(ab')2 antiserum (10
@.dserumdiluted1:10'000in PBS) servedas a
positivecontrol.Normalhumanseraservedas negativecontrols.All
patientsseratestedbefore any MAbinjectionwere also negative.
421@himencversusMouseMAbin Patients•Bucheggerat Si.
-
Patientno.Age
SexDiagnosisDifferentIatiOnDukesSurgery(day)147
MPrimaryrectumIntermB2271FUver met.sigmoldIntermC1369FPrimary
cciascIntermB2478FPrim andmetcci
ascIntermD1570FOvarlanadenocaLow5657
MHyperplasticPolyp1765FLocal
rec.sigmoldIntermC2879MPrimarysigmoldInterm-wellBI944
MPrlmatysigmoidLowC21073FPrimarysigmoidIntermB—1
187 MPrimarysigmoidmt-wellD11266MPrimaiycoltrIntermB—1364
MUver metsigmokinaB—1463MLiver metrectumIntern,C21
574 MLiver metcolonnaC21672FLiver
metrectumIntermC51742FSuspected liver
mata@asin11858 FPrimary colondrIntermB2na
=not available.
TABLE IPatientsInjectedwithChirnedcandOnginalMouseAnti-CEA
MAbsandMajorClinicalParametersPharmacokineticswere analyzedby
modelinga time (hr)—
radioactivity (cpm/ml) curve for each patient. Time 0
immediatelyafter injection was taken as 100%.Using the SIPHAR
program(Simed,Creteil,France)individualpatientdatawereanalyzedinatwo-compartmentmodel.Aweightedleast-squaresmethodwithweights
being the reciprocal of the predicted radioactivity wasusedto
estimatetheparameters.A linearcorrelationanalysiswasusedto
calculatethecorrelationcoefficientbetweenthechimericand the
original mouse MAb in serum.
RESULTS
Eighteen patients were injected with ‘@I-labeledchimeric
anti-CEA MAb together with “SIand ‘@‘Itracelabeled chimeric
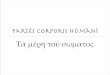
and original mouse MAb (Table 1). Although immunoscintigraphy is
not the objective of thisstudy, two representative illustrations of
a primaiy and ametastatic tumorimmunoscintigraphyare shown in
Figure1.SerumCEAof thesetwo patientswaslow (1.7and1.3ng/ml) and
immune complex formation was almost negative. Both
immunoscintigraphsclearly show antibody uptake in the tumor 6 and
24 hr after injection. At these times,blood radioactivity was still
high as it has been observedearlier after injection of
radioiodinatedintact MAbs.
B-:@‘@
A
FiGURE 1. (A)Uptakeof thimeiic anti-CEAMAbIna primarytumorof the
colonascendens(Patient3) and (B)in a
livermetastasisofacoloncarcinoma(Patient19).InPanelA,a6-gprimarytumorofthecolonascendensiscleedyvisibleontheplanarview6hrafter1@l-MAbinjection.PanelBshowsa
coronalsectionoftheabdomenofa
patientwithan8-9livermetastasisintheleftliverlobe24hrafter1@IMAbinjection.Uptakeinthe
metastasis(arrow)is ofsimilarintensitythan that of heartand
blgvessela,witha
hypoactivecentercorrespondingtonecrotictissue.Activityinnormalliverislow.
422 TheJournalofNuclearMedicine•Vol.36•No.3 •March1995
-
100
•0•apg60ga
@40@ :-‘•U0 20
hours aft.r Injic010n pircantB/
400080100dcr•aa•chimiric
MAb
A
(
300Ca@Wb
ic.i:C —..— chi..•.@I
@,1500
@ 1000U
500
020 30 40 50 60 70
CI IIIj@@*30
40 50 60 7030 40 50 6070tubs
numbar
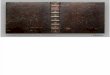
FIGURE2. (@4@Radk,actMtyconcentrationsof thechimericMAb(0) andof
the originSimouseMAb4). Arrowslnd@atepercentInsaraof Patients2 and4
andshowexceptionallyshortcirculationtimesfor
bothchimerleMAbandoriginalmouseMAb.(B)Serumdisappearanceof
mouseMAbIsplottedaginstthstofct@medcMAbofallserumsam—InPanelA(Patients2and4arenot—.
Theca@stedregressionsWSig@linehasthecharactedstlcsof
Y=-1.54+1.146x;correlationcoefficientr@= 0.95.
Overall,asimilarserumdisappearancekhietlcofbothantibodyformsisapparentwltha
marginallyshorterhat-lifeforthemouseMAb.
Sirum KineticsThe serum half-Me of the two MAb forms was
very
similar in all patients with a tendency of
marginallylongerretentionof the chimeric MAb laterafter
injection(after24to 48 hr, Fig. 2A).
Many of these patients were followed for only one totwo days
since serum collection was discontinued aftersurgery. Frequently,
this short observation time did not
permit us to obtain a clear result concerning serum alphaand
beta half-lives. It appears, however, from the individual data
shown in Figure 2A that there is only a minordifference in the
circulationkinetics between the two antibodies. Thus, a high
correlation (correlation coefficient r@= 0.95) was observed for the
two radiolabeled antibody
fonns in the serum samples as shown in a double plotanalysis
(Fig. 2B).
In two patients (Patients2 and 4), the serum half-lives ofboth
the chimeric MAb and of the original mouse MAbwere very short (5
and 7.1 hr) and only between 6 to 13%of radioactivity remained in
circulation after one day forboth antibody forms. In one of these
two patients (Patient4) the accelerated half-lifewas most likely
due to bindingofthe antibodies to CEA, since no HAMA and no
anti-idiotypes were detected in his serum. Indeed, he had a
highamount of serum CPA (342ng/ml) and 47% of the chimericMAlIand
43%of the mouse MAt, were in aggregatedformearly after injection,
as determined by size chromatography on Sephadex 0200 (Fig. 3C).
For the second patient(Patient 2), no obvious reason for the short
half-lifeof thetwo antibody forms was found. CEA in serum was
relatively low (24 ng/ml), and both antibody forms appeared
tocirculate at a high percent in monomeric form: the
serumcollected4 hr after injectioncontainedonlyabout4%ofaggregates
as determined by Sephadex G200 radiochromatography. No indication
of increased dehalogenation inserum was found since only low
amounts of free iodine(
-
PedantPercentbindingCEAinChimericMAbMouseMAbno.In
vitroin serumIn vitroIn serum(nglml)
TABLE 2Percent Bindingof the Two RadiolabeledMAbs Before and
AfterInjectionandSerumCEALevelsEaa
C
Ua0
VS
CaU
a0.
1 50 52 61 52 25.22 82* 80 50 60 23.83 76 73 80 75 1.74 53 27 76
35 3425 53 32 76 35 0.36 53 48 76 52 1.37 75 28 76 30 1378 79 43 56
31 2.89 80@ 35 70 36 16.7
10 81 61 72 56 3311 81 18 79 20 26.712 81 16 79 19 9.613 76 42
76 46 3314 84 75 82 84 1.915 83 81 81 80 9016 77* 63 67 63 2.017 68
74 71 69 0.918 63 51 60 59 nd.
amthreepatients,tracelabelingofchimericMAbandoriginalmouseMAbwaswith1311and1@l,respectively,Insteedof
the
normallyused‘25t-1al@eledchimericMAband‘@‘l-labeledodginalmouseMAb(reversicnof
Isotopes).
nd = notdone
of circulating CEA in whom about 2%, 10% and 45% ofMAb
aggregates were found. Note the appearance of significant amounts
of free iodine (5% to 6%) only in theserum of Patient 4 (Fig. 3C)
who had more than 40% ofimmune complexes.
HAMA were tested in 9 patients 5 to 6 weeks afterinjection of
chimeric and mouse MAb. One patient developed anti-idiotype
antibodies reacting with the chimericmolecule as well as HAMA to
irrelevant mouse immunglobulin. An additional patient (mentioned
above) hadHAMA reacting only with the mouse immunglobulinbutno
reactivity against the chimeric MAb was detected.
Antibody Blodistributlon In Tumor and Normal TissuesFifteen of
the 18 patients injected with both antibody
forms underwent surgery 1 to 5 days after injection (Table
1). In one patient, a suspected malignantrecurrenceturnedout to
be negative (Patient 17) and in another patient abenign polyp was
removed at surgery while a first polypshowing malignant
transformation had been completely removed duringendoscopy before
injection of the antibody(Patient 6). In a third patient with
suspected adenocarcinoma of the rectum, the final diagnosis was a
non-CEAproducing ovarian carcinoma infiltrating the rectum(Patient
5).
Primary adenocarcinoma of colorectal origin or a locoregional
recurrence were surgically removed from eight patients
includingboth patients with short serum T1,@of the
24 48 72 96 120hours aftar injection
FiGURE 4. Serumradioactivityof chimericMAbfor 12
patientsfollowedfor2to6days(dottedlines).Thethickcurverepresentsthemedianhalt-lifecalculatedfor
a two-compartmentmodelwith thecharecteristicsof
medIanTi,@a7.2hrandmedianTiap91.1 hr,
leadingto:
Y = (lOON) - (0.685 - e@1t+ 0.315 . e@),
whereV = 0.99,A1= 0.0076and A@= 0.097.In addition,the
t@thinstra@itlinesrepresentthecalculatedmedianalphaandbetahalt-lives(the
beta halt-lifestraightIkie Is fused with the medianhalt-lifeafter48
hr).
ies. There was no direct correlationbetween the decreaseof
antibodybindingto CEA andthe percentageof antibodyaggregates.
Interestingly, except for Patient 6, all otherpatients had a
similar decrease of CEA binding for thechimeric and mouse MAb.
Overall, binding capacity inserum was decreased as compared to
binding after labelingby about 22%for both the chimeric MAb and the
originalmouse MAb. The mean bindingof chimeric MAb in bufferand in
serum was 71.9 ±12.0 and 50 ±21.3, respectively.The corresponding
figures for mouse MAb are 71.6 ±9.2and 50.1 ±19.9.
Analytic size chromatography was performed on thefreshly labeled
MAbs and on the early serum samples,which allowed the % of in vivo
aggregatedantibody to becalculated. The formation of immune
complexes correlatedwith the amount of circulating CEA. Taking
arbitrarily30ngof circulatingCEA/m1asthelimit, 12of 17patientshad
lower serum CEA levels and the percentage of awegates was 3% to
14%.In contrast, all 5 remainingpatientswith CEA levels higher than
30 ng/ml had more than 15%of aggregates for both the chimeric MAb
and the mouseMAb. In one patient with 342 ng/ml of circulating
CEA(Patient 4), 47% and 43% of injected chimeric and mouseantibody,
respectively, were found as immune complexes.At the time of
antibody injection, none of these 5 patientshad significantHAMA
titers. In one of them (Patient 10) alow titer of anti-mouse IgU
antibodies (test A + B) wasfound five weeks after injection, but no
reactivity againstthe chimeric MAb appeared.Figure3 shows the
radiochromatograms of three representative patients with low
(2.8ng/ml), medium (26.7 ng/ml) and high (342 ng/inl) amounts
424 TheJournalof NudearMedicine@ Vol.36@ No.3@ March1995
-
PatientnumberTumorNormalbowel
waitChimericMAbMouse MAbChimeric MAbMouse MAb
I
IILI
!
SpM$int2SaI:
I:@
@ I I ‘.11
*MeasuredseparatelyasshownInFigures5-7.@Tumorand normal bowel
wait redloactMtyuptake is expressedIn
%ID/gtlssuex*Tumor@tD@nonnalbowelwallredloactMtyratiosaregh,enInparen
theses
I
I
I@I!E@;i@ !,gI@
;@@ ! @‘
!
TABLE 3Comparisonof Tumor Uptakeof
RadiolabeledChimericandOr@nSiMouseMAbto
NormalBowelWallSthppedfrom
NormSiMucosa*
[email protected] .5 (6.5)@I.5(7.0)37.97.93.4(2.3)3.1(2.5)42.03.11
.0(2.0)0.9(3.4)710.111.04.7 (2.1)3.1(3.5)814.29.42.1
(6.8)1.7(5.5)98.08.21.6(5.0)1.7(5.0)1116.917.82.3(7.3)1.7(10.4)1852.655.73.6
(14.6)2.2(25.3)FIGURE 6. Tumorand normaltissue blodlstñbutionof
chimericanti-CEAMAb IgG4(darkshading)and od@nSimouseMAb
(lightshading)intwopatientswhohadsurgeryforIniermetastasesofthecolonand
rectalcardnorna,respectivaly.Verticalbars indicatetherangefor two
or morepieces.Patient4 hed surgeryfor a primarytumor and a liver
metastasis.Uptakeof both MAbs In the
latterexceededthatoftheprimarytumor,whereasuptakeInnecroticpartsof
the livermetastasiswas not higherthan that of
adjacentnormalliver.
antibodies. In these eight patients the mean % ID/g tumorwas
identical for both MAb with 0015% and a large scatter, while the
percentages in the normal bowel wall,stripped of the CEA producing
mucosa, were 0.0025% and0.002% for the chimeric and the mouse MAb,
respectively(Table 3). Figure 5 shows one patientwith a rectum
carcinoma (Patient 1) with a typical median antibody
biodistribution and in comparison the result of the patient with
anovarian carcinoma (Patient 5). In this second patient,
theantibody concentrations in the ovarian malignancy (without
evidence for productionof CEA) was much less thaninblood and also
less than in the normal bowel wall. Figure 6shows an
additionalpatient with a colon carcinoma(Patient 4) having a very
low uptake in its primarytumor(probablyrelatedto highamountsof CEA
in the circulationand immuncomplex formation), while Figure 7 shows
apatient with a primary colon carcinoma and a very highantibody
uptake (Patient 18).
Seven liver metastases were surgically removed andcounted from
patients after injection of both the chimericMAb Ig04 and the
originalmouse MAb. One patient presented with a primarytumorand a
liver metastasis (DukesD, Patient 4), Patient 2 had a large liver
metastasis and amicrometastasis and Patient 16 had two liver
metastasesthat were surgically removed and analyzed.
In the seven metastases, for the chimeric and the mouseMAb, the
mean % ID/g tumor was 0.015 and 0.014%,respectively, with a large
scatter, while the percentages innormal distant liver were 0.0017%
and 0.0023%, respectively (Table 4). Figure 6 shows one patient
(Patient 16)who had two liver metastases from a colon
carcinomawith
FIGURE 7. Tumorand normaltissueblodistributlonof
chimericant@CEAMAb IgG4(darkshacting)and or@nSimouseMAb
(lightsheding)Intwopatientswhohal surgeryfor
primarycoloncardnomaandlivermetastaSis.VerticalbarsIndicatetherangefortwoormore
pieces.In Patient18,a high uptakeof bothantibodieswasobservedin the
primarytumor.The lymphnodewas foundtumorfree by
[email protected] Patient2, a
highconcentrationofbothantibodieswas foundIn a
60-mgmicrometastaals,whileantibodyuptakein a
76-9metastasiswasmuchless.Themicrometastasisshowedfive to six times
higherantibodyuptakethan thelargertumor.
FiGURE 5. Tumorand normaltissuebiOdiatIlbutiOnof
chimedcantl-CEAMAb 1gG4(darkshading)and originalmouseMAb
(lightsha@ng) in two patients (one with rectal and one with ovarian
carcinoma).Verticalbars indicatethe rangefor tissueswheretwo ormore
pieceswere available.Clear uptake is shown In the rectalcarcinomaof
PatientI, whereasno uptakeia demonstratedin theovariancarcinomaof
Patient5.
ChimericversusMouseMAbinPatients@ ButheggeratSi. 425
.. S !@
S@@
it t I Iit j ft
-
Patientno.Liver
metastasisNormalliverChimeric
MAbMouse MAbChimeric MAbMouse MAb
•Radk@actMtyuptake In the liver metastasIsand normal liver is
expressedin %lDIgtissuex
tp@@ comparinglivermetastasisradloactMtyto that In
normalliveraregivenInparentheses.
*AntIbodyuptakeina micrometastasis0140mgfoundduringdissectionof
normallivertissueadjacentto thelargemetastasis.
a typical mean antibody uptake in tumor. A second patientshown
in Figure 6 (Patient 4) presented with a colon carcinoma and with
an initial liver metastasis. While antibodyuptake in both tumor
sites was low, uptake in the livermetastasis was about two times
higherthan in the primarytumor. This patient had the highest amount
of circulatingCEA and aggregated antibodies in the serum (43%
and47%) and a very short half-life of both antibody forms thatmight
explain the low uptake of antibodies in the tumors.Patient 2 shown
in Figure 7 was operated for a liver metastasis 1 day after
antibody injection. While the largetumor (75 g) had a mean uptake
of about 0.010% ID/g, amicrometastasis of 40 mg, found at
dissection of the adjacent normal liver tissue, had an uptake of
0.062% and0.038%injected dose per g for the chimeric and the
mouseMAb, respectively, in other words, five to six times
higherthan in the large metastasis.
A finalpatient is presented in Figure8 who was operatedfor a
liver metastasis 8 days after injection of the Ig04chimeric MAb
labeled with 1@I, together with a smallamount (30 /Lg)of the Ig02
chimeric MAb, labeled with1311 In this patient, 3.5 to 4.5 times
higher tumor-to-blood
and tumor-to-liver ratios were obtained with the chimericMAb of
IgG2 subclass than with the IgG4 chimeric MAb.Both antibodies
injected in this patient (having the samevariable domains) showed
highbindingto CEA afterradiolabeling (79%for the Ig04 chimeric MAb
and 88%for theIg02 chimeric MAb) that was only marginally decreased
inserum. Ifconfirmed the surprisingly higher tumor uptake ofthe
IgG2chimeric MAb would suggest its use in patientsinstead of the
Ig04 chimeric MAb.
DISCUSSION
In this study eighteen patients were injected with achimeric MAb
of human IgG4 subclass together with theoriginal mouse 1g01 MAb.
Both are directed against thesame epitope ofCEA and have an
identical affinity(23,32).
TABLE 4Comparisonof RadiOlabSiedChimencand OnginSiMouseMAb
Uptake in Uver Metastasesand Normal Uver Thsue
— — patI.nt 19 •@@
@ 0 c@suss
i:11111@i@j1TTT
210.4*7.82.1
(5.O)t4.8(1.6)[email protected](29.8)4.8(7.9)44.37.31
.2 (2.7)2.1(3.5)148.517.61.3(6.5)1.3(13.5)154.63.81.8
(2.6)1.7(2.2)166.49.32.1(3.0)1.4(6.6)168.212.12.1
(3.9)1.4(8.6)
FiGURE 8. Comparisonof tumor uptakeof
chimencIgG4MAb(darkshading)withthatof IgG@subclass(openbars)that
has identicalspecificity(becauseIt wasdeducedfromthe
sameoriginalmouseMAb) In a patientwfth liver metastasisfrom
coloncancer.The livermetastasiswassurgicallyresected8
daysafterInjectionofthetwotrace-labeledantibodies.Verticalbarsindicatethe
rangefort@ or morepiaces.
The capacity of antibodies to localize in tumors dependson
multipleparameters,amongothers on the immunoreactive fraction after
radiolabelingand injection. Tumor size,the
interstitialfluidpressure (40), vascularization and
vascularpermeability(41) tightjunctions in
well-differentiatedtumors and the so called binding-site barrier
(42) (absorption of high-affinityantibodies to antigenon
tumorsurface)can further modulate antibody uptake. The comparison
oftwo antibodies using the double-labeling technique,whereby both
antibody forms encounter identical biological parameters in each
patient, allows a meaningful comparativeanalysis in a
limitednumberof patients. Since theoverall total amount of antibody
injected in this study(4 mg) was low, tumor antigen was in excess
and no majorcompetition for antigenic sites should have
occurred.
Overall, tumor uptakes and normal tissue
radioactivitydistributions showed a similar behavior for both
MAbforms. Some variationwas observed in individualpatientsthat can
be attributedto a certain degree of variability inthe different
batches of MAb preparations and in iodinequality and labeling. The
in vitro quality controls reflectpart of these variations while
others might be apparent onlyin vivo as suggested by other studies
(3Z39).
In serum, the chimeric MAb had a marginally longerhalf-Me than
the original mouse MAb. This was observedwhether patients had high
or low amounts of circulatingCEA. Since both antibodies have an
identical affinity forantigen (23,32), the percentage of immune
complexes forboth was very similar in individual patients related
to serum CEA. Apparently, the elimination of these immunecomplexes
by the RES was also similar. The measuredhalf-life of the IgG4
chilneric MAb was shorter than expected. It is possible thateven
small amountsof circulatingCEA induced formation of immune
complexes that influenced the beta half-life. Additionally, the
observation time
426 The JoumSiof Nudear Medicine@ Vol. 36@ No. 3@ March 1995
-
is relatively short in many patients and might have influenced
evaluation of this half-life in some patients.
In the present comparison of mouse and chimeric MAb,we measured
the immunoreactivefractionbefore and afterinjection. While the sera
of certain patients had little or noinfluence on the binding
capacity of the antibodies, in otherpatients the binding capacity
of both of them was drastically reduced afterinjection.
Reducedbindingwas found inpatients with large amounts of immune
complexes due tocirculatingCEA, as in Patients 4, 7 and 13. In some
cases,however, reduced antibody binding after injection wasfound in
patientswith low serum CEA, as in Patients5 and8. In these
patients, the diminished binding after injectionmight be due to a
non-specific influence of serum on antigen-antibodyassociation:
ionic strengthhas been shown toinfluence the affinity of antibodies
against a closely relatedepitope ofCEA by a factorofup to 100(43).
Ourassay thatmeasures bindingof radiolabeledantibody to a limited
cxcess of antigenmightbe particularlysensitive to such nonspecific
binding inhibition in serum.
Our results concerning HAMA and anti-idiotype antibody
formationin patients show that both the radiolabeledchimeric and
original mouse MAb have a low immunogenicity after a single
injection. Several other reports haveshown a higher immunogenicity
of mouse MAbs, especially after repeated injections, but also low
immunogenicity after single injections of MAb have been reported
(20—22). Our results are in line with our previous
observationswhere after a single injection of radioiodinated
mouseMAbs for immunoscintigraphy detectable HAMA titerswere only
rarely found. Such a first MAb injection might,however, stimulate
formation of memory cells in manypatients. This is suggested by the
fact that a second MAbinjectionwas followed frequentlyby a
rapidappearanceofimportant HAMA titers already after 2 wk
(unpublishedobservation).
For chimeric MAbs, a weak immunogenicity has beendescribed more
frequently (12,24). However, one studywith the chimeric human IgG4
MAb B72.3 showed that ithad a high immunogenicity (25): after a
single injection of3.4 to 6.9 mg, 7 of 12 patients developed
measurableHAMA titers against this antibody (25). This MAb had
alongerserumbeta half-life(224 ±66 hr)as comparedto ourchimeric
anti-CEA MAb (91hr median beta half-life) and isdirected against an
antigen that is less frequently elevatedin patient's serum. Since
the two MAbs have differenthuman Ig64 constant domains, it remains
unclear whetherthe higher immunogemcity of the B72.3 IgG4
chimericMAb is due to its different mouse variable domains or tothe
differentallotypic epitopes on the human constant domains.
Interestingly, the formation of immune complexesin our patients
does not appearto promote HAMA formation. Immune complexes are
preferentially bound by thelow affinity IgG Fc receptors on
macrophages (44) andhave been used in immunizationprotocols.
Of interest are a few data concerning high tumoruptakeof
radiolabeled MAbs: Figure 7 shows a very good local
ization for both the chimeric MAb and the original mouseMAb in a
primary tumor operated two days after antibodyinjection (Patient
18). Similarhigh antibody uptake in primary tumors has been
observed in a series of six patientswho were injected with higher
amounts of the same chimeric anti-CEA antibody (10 mg per patient)
trace labeledwith radioiodineand coinjected with the identical
antibodycoupled to fluorescein for the purpose of
immunophotodetection (45). Figure 7 shows another patient operated
for aliver metastasis where on dissection of the adjacent
normalliver tissue, a micrometastasis of 40 mg was found
(Patient2). Here, the micrometastasis showed, on a per gram basis,a
five to six times higher antibody uptake than the largemetastasis.
This patient had a very short circulation halflife for both
antibody forms that remains unexplained. Patient 19, who had
surgery eight days after antibody injection, had a relatively high
tumor uptake as compared tonormaltissues: 0.01%of the injected dose
per g tumorwasfound for the Ig04 chimeric MAb, and more than
0.02%ofthe coinjected Ig62 chimeric MAb labeled with 1311.Thetwo
chimeric MAbs of different human IgO subclasses arederived from the
same anti-CEA mouse MAb and have asimilar affinity for CPA (32).
Interestingly, the chimeric1g02 MAb injected in trace amounts (30
@g)gave 3.5 to 4.5times highertumor-to-liverand
tumor-to-bloodratios thanthe Ig04 Chllfl@riCMAb. While the limited
amount of antibody injected might explain the faster
disappearancefromblood for the chimeric IgG2 MAb@its higher tumor
uptakecertainly merits further investigation.
The three patients mentioned above with particularlyhigh
antibody uptake in tumor stimulate some reflectionsconcerning
dosimetry for a potential
radioimmunotherapy.Consideringradioimmunotherapyin a postoperative
adjuvant setting where occult micrometastases would be thetarget,
such micrometastases might accumulate higher antibody doses than
large tumormasses as it is suggested bythe results from Patient 2
and by other reports (7,17,46).Thus, a tumor uptake in the range of
0.06% ID/g could beobtained more frequently in small tumors as
compared tolarger ones. Assuming homogenous irradiation of
suchsmallnodules with a radionucide emittingbeta-radiationofmedium
energy (e.g., 1311or 67@), the MIRD formulawould predict an
irradiationof 2100 rad for an injection of100 mCi ‘@‘Iand a
60-hr effective half-life in the tumor. Fora repeated injection of
2 x 100 mCi, the total tumor dosewould reach 4200 rad. Such
radiationdoses in micronodules thatareoptimallyoxigenated
andradiosensitivewouldhave a good chance to be efficient. The
effective tumorradiationdose could, however, be modulated by
parameters such as the percent of absorbed energy in a
givenmicronodule and for a given radiation type (47), the
microheterogeneity of tumor irradiationdue to uneven distribution
of antibody (48) and the low dose rate of irradiationthat is
generallyobtainedin radioimmunotherapy(49). Theextrapolationof our
results and those fromother groups asshown above should, however,
encourage future experi
427chimencversusM@ i@i@in Patients@ Bucheggerat Si.
-
mentalandclinical radioimmunotherapystudies of minimalresidual
disease.
Altogether, the results obtained with the chimeric antiCEA
IgG4MAb showed a tumor localization capacity thatis comparableto
that of the originalmouse MAb which hadbeen selected for high
affinity and antigen binding. Thetumor uptake of these two MAbs was
similar or evenslightly superior to that observed with anti-B cell
MAbs(9,10) which have been successfully used for radioimmunotherapy
of lymphomas.
ACKNOWLEDGMENTS
The authorsthankMrs. K. Foamier for
efficienttechnicalassistance. We are grateful to Dr. F. Healy for
reviewingthemanuscript.The chimericMAb wasproducedby
CibaGeigy,BaselSwitzerland.Thisworkwassupportedby
theSwissFoundationfor
ScientificResearch(grantnumber31-31238-91),byRechercheSuisse contre
le Cancer(Akt 312) and the RobertWenner Swiss Cancer Research Award
1991.
REFERENCES1. MachJ-P,PulegrinA, BucheggerF.
Imagingandtherapywith monoclonal
antibodiesin
non-hematopoictictumors.CurrOpEnImmwsol1991;3:685—693.
2. Scheinberg DA. Current applications ofmonoclonal antibodies
for the therapy of hematopoleticcancers. Cwr OpinImmwsd
1991;3:679-684.
3. OoldenbergDM,Schiom3. Thecomingof
ageofcancerradloimmunoconjugates. Immunol Today 1993;14:5-7.
4. CheungNK, LandmeierB, Neely3, et
at.Completetumorablationwithiodine131-radiolabeleddiSialOgangliOsideGD2-specilicmonoclonalantibody
against human neuroblastoma xenografted in nude mice.JNatI
Canca@Inst 1986;77:739—745.
5. SenekowitschR, ReidelG,MOlleUStãdtS, KriegelH,
PabstHW.Curativeradioimmunotherapyof humanbreasttumorswith
131-I-labeledmonoclonat antibodies. JNuclMed 198930:531-537.
6. Buthegger F, Pfister C, Fournier K, et al. Ablation of human
colon cardnoma in nude miceby
131-I-labeledmonoclonalanticarcinoembiyonkantigenantilxxlyF(ab')2
fragments.I ClinInvest 1989;83:1449-1456.
7. Buchegger F, PèlegrinA, Delalcye B, BischofDelalcye A, Mach
J-P. 131-Ilabeled F(ab')2 fragments are more efficient and less
toxic than intact antiCEA antibodiesin radioimmunotherapyof large
human colon
carcinomagraftedinnudemice.JNucIMed1990;31:1035—1044.
8. Sharkey RM, Weadock KS, Natale A, Ct al. Successful
radioimmunotherapy for lung metastasis of human colonic cancer in
nude mice. I NailCancerlnst 1991;83:627—632.
9. Press OW, Eary iF, Appelbaum FR, Ctat. Radiolabeled-antibody
therapyofB-celllymphomawithautologousbonemarrowsupportNEnglJMed1993;329:1219—1224.
10.KaminakiMS, ZasadnyKR, FrancisIR, et aL
RadioimmunotherapyofB-celllymphomawith
(‘311)anti-B1(anti-CD2O)antibody.N E@ogII Med1993329:459-465.
11. Breitz HB, Weiden PL, Vanderheyden J-L, Ctal. Clinical
experience withRhenium-186-labeledmonoclonal antthodies for
radioimmunotherapy: resuIts of phase I trials. JNucl Med
1992;33:1099-1112.
12. LoBugJio AF, Wheeler RH, Trang J, Ctal. Mouse/human chimeric
monodonal antil,ody in man: Kinetics and immune
response.PmcNadAcadSciUSA 1989;86:4220—4224.
13. Delalcye B, BischofDelalcye A, Buchegger F, Ctal. Detection
of colorectalcarcinomaby emission-computerizedtomographyafter
injectionof 123-I-labeledFabor
F(ab')2fragmentsframmonoclonalanti-carcinoembiyonicantigen
antibodies. I Clin Invest 1986;77:301-311.
14. Bischof Delaloye A, Delalcyc B, Buchegger F, Ct al. Qinical
value ofimmunoscintigraphyin colorectalcarcinomapatients:a
prospectivestudy.JNucI Med 1989;30:1646-1656.
15. RyserJE,JonesR, Egei R, et al.
Coloncarcinomaimmunoscintigraphybymonodlonalanti-CEAantilxxlylabeledwith
gallium-67aminooxyacetyldeferroxamine. INuciMed 199233:1766-lm.
16. Begent RHJ, Ledermann JA, Green Al, et al.
AntilXXIydistribution and
dosimetiyinpatientsreceivingradiolabelledantilxxlytherapyforcolorectalcancer.BrI
Cancer 1989;60:406-412.
17. @haadJ-F, Saccavini J-C, Gestin i-F, Ctat. Biodistribution
of indium-illlabeled 0C125 monoclonal antibody intraperitoneally
injected into patientsoperatedon for ovariancarcinomas.CancerRes
1989;49:3087—3094.
18. MilenicDE, Yokota1, FilpulaDR,et al.
Construction,bindingproperties,metabolism,andtumortargetingof a
single-chainFv derivedfromthepancarcinomamonoclonalantibodyCC49.
CancerRes 1991;51:6363-6371.
19. Buchsbaum Di, Weasels BW. Radiolabeled antibody tumor
dosimetiy.MedicalPhys 1993;20:499—501.
20. Kuus-ReichelK, GrauerLS,KaravodinLM, KnottC,KrusemeierM,
KayNE. Minireview.Will
immunogenicitylimittheuse,efficacy,andfuturedevelopment
oftherapeutic monoclonal antilxxlies? Clin Diagn Lab Immunol
1994;l:365—372.
21. HyamsD, ReynoldsJC, CarrasquilloJA, et al. The effectof
circulatinganti-murineantthody on the pharmacokineticsand
biodistributionof injected radiolabeled monoclonal antthody
[Abstracti. I Nuci Med 1986;27:92@
22. Abdel-NabiHH, Doerr Ri, Chan H.W, et aL Safety and role of
repeatedadministrationof Indium-ill-labeled
anticarcinoembiyonicantigenmonoclonal antilxxly ZCE 025 in the
postoperative follow-up ofcolorectal cardnoma patients.JNucIMed
199233:14-22.
23. HardmanN, Gill LL, De Winter RF, et al. Generationof a
recombinantmouse-human chimaeric monoclonal antibody directed
against human carcinoemblyosicantigen.Intl Cancer
1989;44:424-433.
24. GoodmanGE, HellstrOmI, YeltonDE, et al PhaseI trialof
chimeric(human-mouse)monoclonalantibody L6 in patients with
non-small-celllung,colon, and breast cancer.
Cancerlmmwzollmmunother1993;36:267-273.
25. Khazaei MB, Saleh MN, Liu TP, et al. Pharmacokineticsand
immuneresponseof131I-Qtimencmouse/humanB72.3(humangamma4)monoclonal
antibody in humans. CancerRes l991@1:5461-5466.
26. RiechmannL, Qark M, WaldmannH, Winter 0. Reshapinghuman
antibodiesfortherapy.Nature1988;332:323—327.
27. SingerII, KawkaDW,DeMartinOiA, et al. Optimalhumanizationof
1B4,an anti-CD18murine monodonal antil,ody, is achieved by correct
choice ofhumanV-regionframeworksequences.Jlmmunol
1993;150:2844-2857.
28. GriffithsAD,WilliamsSC, Hartley0, et al. Isolationoflugh
affinityhumanantthodiesdirectlyfromlargesyntheticrepertoires.EMBO!
1994;13:3245—3260.
29. Lonberg N, Taylor LD, HardingFA, et al.
Antigen-specifichuman
antibodiesfrommicecomprisingfourdistinctgeneticmodifications.Natw@1994368:856—859.
30. MorrisonSL Successinspecification.Nature1994;368:812-813.31.
VogelCA, BischofDelaloyeA, MachJ-P,et al. Directcomparisonof a
radioiodinatedintact chimericanti-CEAMab with its F(ab')2
fragmentinnude mice bearing different colon cancer xenografts. BrJ
Cancer 1993;68:684—690.
32. ButheggerF, PIlegrinA, HardmanN, et al. Differentbehaviourof
mousehumanchimericantibodyF(ab')2fragmentsof IgGi,
1g02andIgG4subclass in vivo. Intl Cancer 199250:416-422.
33. HammarstromS, Shive@yJE, PaxtonRi, et aLAntigenicsites in
carcinoembryonicantigen.CancerRes1989;49:4852-4858.
34. Nap M, HammarstrOmML, BOrmer0, et al. Specificityand
affinityofmonoclonalantibodiesagainstcarcinoembtyonicantigen.CancerRes
1992;52:2329—2339.
35. BucheggerF, SchreyerM, CarrelS, Machi-P.
Monoclonalantthodiesidentify a CPA crossreacting antigen of 95 kD
(NCA.95) distinct in antigenicityand tissuedistributionfromthe
previOUslydescribedNCAof55 kD.Intl Cancer198433:M3-649.
36. Roth IM, Brostoff 3, Male DK. Mtil,ody structure and
function. In:&nnett D, ed.
Immunology.London,England:GowerMedicalPublishingLtd;
1985:5.1—5.10.
37. FritscheR, MachJP. Isolationandcharacterizationof
carcinoembiyonicantigen (CEA) extracted from normal human colon
mucosa. Immunochem1977;14:119—127.
38. Buchegger F, Mach i-P. Different SOlid-phaseenzyme
immunoassays usingfive monoclonal antthodies reactingwith distinct
epitopes of carcinoembryorik antigen. In: Avrameas S, et aL, ads.
Immuncenzymatic
Techniques.Amsterdam,TheNetherlands:ElsevierSciencepublishersB.V.;1983:385—394.
39. DeNardOGL, DeNardO Si, Miyao NP, Ctal. Non-dehalogenation
mochanismsforexcretionofradioiodineafteradministrationoflabeledantibodies.JntlBiolMai*ers
1988;3:i-9.
40.JamRK,BaxterLI.
Mechanismsofheterogeneousdistributionofmono
428 TheJournalofNudearMediane@ Vol.36@ No.3@ March1995
-
donal antibodies and other macromolecules in tumors:
significance of dcvated interstitialpressure. CancerRes
1988;48:7022—7032.
41. Folli S, PIlegrin A, Chalandon Y, et al. lumor necrosis
factor can enhanceradio-antibody uptake in human colon carcinoma
xenografts by selectiveincreaseofvascular permeability.Intl Cancer
199353:829-836.
42. FujimonK, CovellDO,FletcheriE,WeinsteinJN.A
modelinganalysisofmonoclonalantibodypercolationthroughtumors: a
binding-sitebarrier.INuci Med 1990;31:1i91—1198.
43. HaskellCM,BucheggerF, SchreyerM, CarrelS, Machi-P.
Monoclonalantibodies to carcinoembryonic antigen: ionic strength as
a factor in theselection of antibodies for iminUnOScintigraphy.
CancerRes 1983;43:3857-3864.
44. HunzikerW, FumeyC. A di-leucinemotifmediatesendocytosisand
baso.lateral sorting of macrophage IgG Fc receptors in MDCK cells.
EMBO I1994;13:2963—2969.
45. Folli S, WagniIres 0, PIlegrin A, Ct al. Localization and
detection offluoresceinatedchimeric antibodies against
carcinoembiyonicantigen
inprimarycolorectalcarcinomas:firstapproachto
clinicalimmunophotodiagnosiLProc NatlAcad Sd USA i992;89
973-7977.
46. HaganPL, HalpernSE, DillmanRO, et al. lumor size: effecton
monoclonal antibody uptake in tumor models. INuciMed
1986;27:422-427.
47. AkabaniG, PostonSrJW,BolchWE.Estimatesofbeta
absorbedfractionsin small tissuevolumes for selected
radionuclides.JNuclMed 199l;32:835-839.
48. HumznJL
Dosimetricaspectsofradloinbeledantibodiesfortumortherapy.INuciMed
1986;27:i490-1497.
49. Fowler JF. Radiobiological aspects oflow dose rates in
radioimmunotheral,),.InJRadia@ OncolBk,!Phys 1990;18:1261-1269.
429ChimencversusMouseMAbin Patients•Bucheggerat Si.