Embed Size (px)
Citation preview
This report is about detection of asymptomatic lung cancer by periodic radiologicand cytologic screening. The idea for thisstudy was conceived by the members ofthe American Cancer Society's Lung (‘ancer Advisory Committee in 1955 and 1956and was finally activated in June, 1958.
Planning is carried out b@a (‘oordinating Committee consisting of reprcsentatives from a Statistics (‘enter,a RadiologyCenter, four Cytology Center.@: and sixVeterans Administration domiciliary unitsas the Screening (‘enters.
This is a pilot study which was not designed to he definitive. We are really trying to find out on a relatively small scale(about 11,000 men) what the indicationsare for a larger study of the value of massscreening of a nonpatient populationgroup by cytologic and radiologic means.The study is not designed to examine thevalue of screening in ternis of five-yearsurvival rates. However, if, for example,90 per cent of unsuspected cases of lungcancer turned up are resectahle, semiannual screening would certainly deservefurther consideration. On the other hand,if only 5 to 10 per cent of the new cases
discovered are resectable, then the valueof the screening would not lie too great,at least until improved methods of therapyarc found.
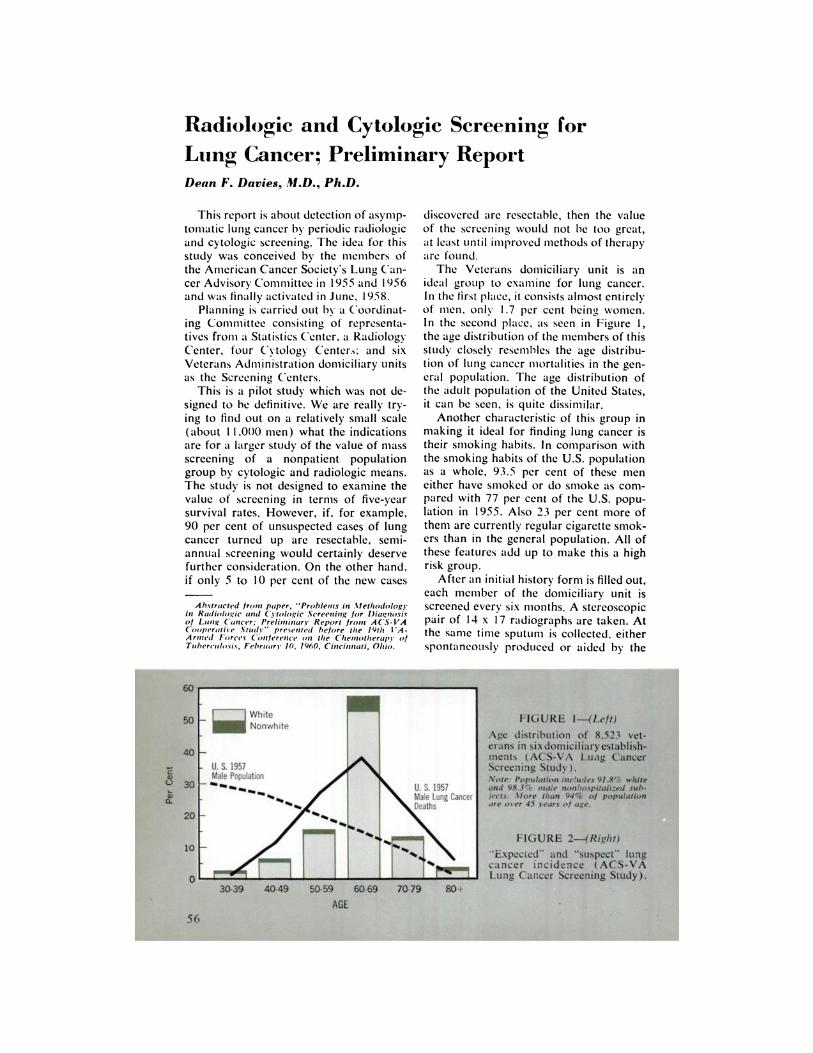
The Veterans domiciliary unit is anideal group to examine for lung cancer.In the first place, it consists almost entirelyof men, only 1.7 per cent being women.In the second place, as seen in Figure 1,the age distribution of the members of thisstudy closely resembles the age distribution of lung cancer mortalities in the general population. The age distribution ofthe adult population of the United States,it can be seen, is quite dissimilar.
Another characteristic of this group inniaking it ideal for finding lung cancer istheir smoking habits. In comparison withthe smoking habits of the U.S. populationas a whole, 93.5 per cent of these iiieneither have siiioked or do smoke as compared with 77 per cent of the U.S. population in 1955. Also 23 per cent more ofthem are currently regular cigarette smokers than in the general population. All ofthese features add up to make this a highrisk group.
After an initial history forni is filled out,each member of the domiciliary unit isscreened every six months. A stereoscopicpair of 14 x 17 radiographs are taken. Atthe sanie time sputuni is collected, eitherspontaneously produced or aided by the
A b.stracted froom paper, ‘¿�‘Proble,mmsi,m .‘mletimodologyi,m Radio/at_ic amid Cytologic .Screemmumgfor Diaç',mosisof Lu,mg ( aimeer; Prelinmi,mary Report fro,,m A CS- VA(ooperatime Study'' pre.seimted before time 1Ytim I A—A rimmed Forces (ommferm'mmcemm time Cimemotimerapy ofTuberculosis, February 10, 1960, Ci,mci,m,mati, ()imio.
FIGURE l—(Left)Age distribution of 8,523 veterans in sixdomrciliaryestablishments (ACS-VA Luag CancerScreening Study).Note: Population Includes 91.8% whIte.and 98.3% male nonhospitalized subjects. More than 94% of populailonare over 45 years o/ age.
FIGURE 2—(Right)‘¿�Expected―and “¿�suspect―lungcancer incidence, (ACS-VALung Cancer Screening Study).
AGE56
Radiologic and Cytologic Screening for
Lung Cancer; Preliminary ReportDean F. Davies, M.D., Ph.D.
use of a machine delivering large voluniesof an aerosol. This sputagenic machinewas invented and developed specificallyfor this study. The films are read (but notstereoscopically) by the local radiologists,and the sputum specimens are sniearedby technicians. The x rays are mailed tothe Study's Radiology Center and theslides are mailed to its four Cytology Centers in rotation. Suspects are followed upby physicians at the screening center untilsatisfactory explanation of x-ray or cytologic abnormality is found. Of course thehistory form and subsequent symptom supplements may in retrospect reveal how tofurther narrow down a high risk group.
As might be expected, the radiologistsare not always satisfied with the excellenceof the films, nor the cytologists with thesmears. The technical problems in x-rayscreening have been more rapidly overconic than those of cytologic screening. Itis clear, however, that the latter niethodis practicable.
The agreement between radiologists ondual reading of films is lowest (19 percent) for the “¿�suspectneoplasm― category
@ndhighest (66.7 per cent) for the negative film. When suspicions of any significant pulmonary abnormalities—neoplasticand other—are considered together, thepercentagreementbetweenradiologistsmore than doubles froni 19 to 42 per centof all films so classified by either reader.
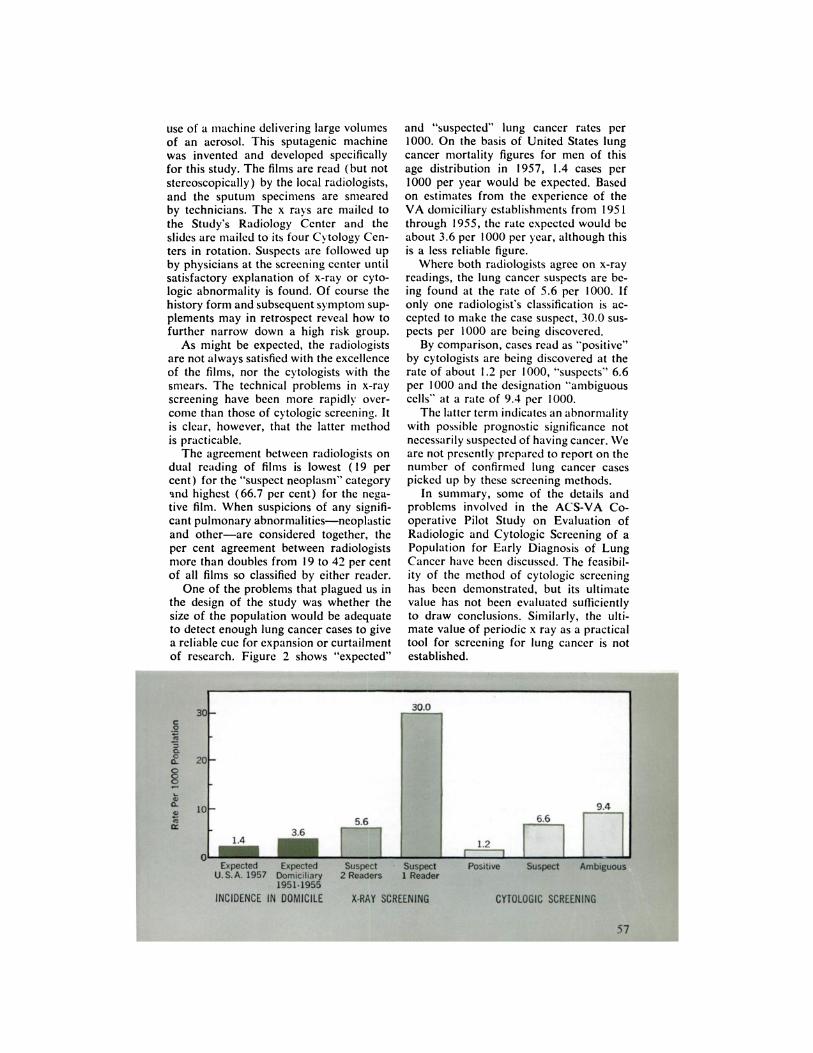
One of the problems that plagued us inthe design of the study was whether thesize of the population would be adequateto detect enough lung cancer cases to givea reliable cue for expansion or curtailmentof research.Figure2 shows “¿�expected―
ix@2O
§10
and “¿�suspected―lung cancer rates per1000. On the basis of United States lungcancer mortality figures for men of thisage distribution in 1957, 1.4 cases per1000 per year would be expected. Basedon estiniates froni the experience of theVA domiciliary establishments from 1951through 1955, the rate expected would beabout 3.6 per 1000 per year, although thisis a less reliable figure.
Where both radiologists agree on x-rayreadings, the lung cancer suspects are being found at the rate of 5.6 per 1000. Ifonly one radiologist's classification is accepted to make the case suspect, 30.0 suspects per 1000 are being discovered.
By coniparison, cases read as “¿�positive―by cytologists are being discovered at therate of about 1.2 per 1000, “¿�suspects―6.6per 1000 and the designation “¿�ambiguouscells―at a rate of 9.4 per 1000.The latterterniindicatesanabnormality
with possible prognostic significance notnecessarily suspected of having cancer. Wearenotpresentlypreparedtoreporton thenumber of confirmed lung cancer casespicked up by these screening methods.
In suniniary, sonic of the details andproblems involved in the ACS-VA Cooperative Pilot Study on Evaluation ofRadiologic and Cytologic Screening of aPopulation for Early Diagnosis of LungCancer have been discussed. The feasibility of the method of cytologic screeninghas been demonstrated, but its ultimatevalue has not been evaluated sufficientlyto draw conclusions. Similarly, the ultimate value of periodic x ray as a practicaltool for screening for lung cancer is notestablished.
INCIDENCEIN DOMICILE





























