Embed Size (px)
Citation preview

Cancer Immunology Miniatures
Radiologic Heterogeneity in Responses toAnti–PD-1/PD-L1 Therapy in MetastaticRenal Cell CarcinomaGuillermo de Velasco1,3, Katherine M. Krajewski4, Laurence Albiges5, Mark M. Awad1,2,3,Joaquim Bellmunt1,2,3, F. Stephen Hodi1,2,3, and Toni K. Choueiri1,2,3
Abstract
Radiologic assessment of tumor response remains a chal-lenge in patients treated with immune checkpoint inhibitors. Inmetastatic melanoma, for example, a spectrum of imagingpatterns in response to immunotherapies have been recognizedand associated with clinical benefit. In metastatic renal cellcarcinoma (mRCC), less than half of patients treated withimmune checkpoint inhibitors achieve objective responses, butsome of the responses have been durable. In this series, fivedifferent imaging patterns of response and progression are
described in mRCC patients treated with anti–PD-1/PD-L1agents: (i) early and complete response, (ii) pseudoprogres-sion, (iii) disease stability before ultimate response, (iv) mixedresponse with new lesions, and (v) early progression/primaryrefractory disease. The implications of the different imagingpatterns of patient responses on disease prognosis are dis-cussed and highlight the need for individualized patientassessment when using these novel immune-targeted agents.Cancer Immunol Res; 4(1); 12–17. �2015 AACR.
IntroductionThe programmed death 1 (PD-1) pathway is a negative feed-
back system that represses immune responses, but if it is unreg-ulated, it can damage the host, and it can contribute to autoim-mune disease and cancer when dysregulated (1). The upregula-tion of the PD-1 pathway and associated complex interactionswith thehost havebeen seen inmultiple cancers, and theblockadeof this pathway has led to remarkable clinical responses inpatients with advanced melanoma, non–small cell lung cancer(NSCLC), renal cell carcinoma (RCC), and several other types ofcancer (2–4).
PD-L1 and PD-L2 are the major ligands for PD-1, which is areceptor expressed on T cells (1). PD-L1 binding to PD-1 nega-tively regulates the immune response and activity of antitumorT cells. Both PD-1 and its ligand PD-L1 are targets of new immunetherapies. Studies have shown that the expression of PD-1 ligandson the surface of tumor cells or immune cells might be animportant predictive biomarker of response to PD-1 blockade (5).
Nivolumab is a new anti–PD-1 mAb that has been recentlyassociated with durable responses in approximately 20% ofpatients with metastatic renal cell carcinoma (mRCC; ref. 2).Nivolumab has already been approved by the FDA for metastatic
melanoma (6) and NSCLC (7). Data from early studies in mRCCsupport current ongoing phase III clinical trials assessing nivolu-mab infirst- and second-line therapy, both as a single agent and incombination with different anti–VEGF-targeted therapies (8).Another PD-1 inhibitor, pembrolizumab, is also being tested incombination with other agents such as ipilimumab in RCC (9).
Antibodies that also target the PD-L1 ligand are also underdevelopment for treatment of mRCC (5). Atezolizumab(MPDL3280A), a mAb against PD-L1, has been tested in a phaseI trial with 69 mRCC patients, with a median progression-freesurvival (PFS) of 24 weeks (10). Durvalumab (MEDI4376),another anti–PD-L1 antibody, is being studied in combinationwith tremelimumab in patients with advanced solid tumors,including RCC (11).
As seen with ipilimumab, a CTLA-4 inhibitor approved foradvanced melanoma, the kinetics of response to anti–PD-1 andanti–PD-L1 agents are rather heterogeneous and might be differ-ent from those for cytotoxic and targeted therapies (12).Objectiveresponses can be observed in variable time frames, from a fewweeks to several months after therapy initiation. Response orstable disease inmRCCmaybepreceded by apparent early diseaseprogression, as has been seen in melanoma patients treated withipilimumab (12). At this point, it is not clear whether aminimumamount of time is required to assess treatment responsewith anti–PD-1/PD-L1 therapy (13) or whether this new form of immuno-therapy should be given continuously until progression or inter-mittently. Understanding the kinetics of response to immune-checkpoint inhibitors will help to improve the outcome ofpatients treatedwith anti–PD-1/PD-L1 therapies.Here, wediscussseveral cases illustrating the heterogeneous kinetics of radiologicresponse to PD-1/PD-L1–blocking agents in mRCC.
Case 1 (Early and Complete Response)A 60-year-old man with excellent functional capacity and
minimal symptoms was diagnosed with intermediate-risk
1Department ofMedical Oncology, Dana-Farber Cancer Institute, Bos-ton, Massachusetts. 2Department of Medical Oncology, Brigham andWomen's Hospital, Boston, Massachusetts. 3Harvard Medical School,Boston,Massachusetts. 4Departmentof Imaging,Dana-FarberCancerInstitute and Department of Radiology, Brigham and Women's Hos-pital, Boston,Massachusetts. 5Department ofMedical Oncology, Insti-tut Gustave-Roussy, Villejuif, France.
Corresponding Author: Toni K. Choueiri, Dana-Farber Cancer Institute, 450Brookline Avenue, Dana 1230, Boston, MA02215. Phone: 617-632-5456; Fax: 617-632-2165; E-mail: [email protected]
doi: 10.1158/2326-6066.CIR-15-0197
�2015 American Association for Cancer Research.
CancerImmunologyResearch
Cancer Immunol Res; 4(1) January 201612
on February 2, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/2326-6066.CIR-15-0197

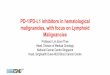
metastatic clear cell renal cell carcinoma (ccRCC) based on theInternational Metastatic Renal Cell Carcinoma Database Consor-tium (IMDC). Restaging scans after cytoreductive nephrectomyshowed increase in the size of several biopsy-proven pulmonaryand lymph node metastases in the thorax and abdomen (Fig. 1Aand B). The patient was started in a trial of anti–PD-1 treatment asafirst-line therapy. After only two doses of study drug, a follow-upCT showed a complete response (CR). The patient tolerated thistherapy well and continued treatment for 14 months withoutinterruption. Ultimately, the patient stopped the drug due to thelate development of immune-related adverse effects (grade 2uveitis). Despite 2 years without any treatment, the responsecontinues to be durable and the patient remains with no evidenceof disease.
Case 2 (Pseudoprogression)A 54-year-old man presented with intermediate-IMDC risk
metastatic ccRCC (lung nodules and retroperitoneal lymphade-nopathy). This patient's first-line treatment was a sunitinib-basedcombination [multitargeted tyrosine kinase inhibitor (TKI),including VEGFRs and platelet-derived growth factor (PDGFR)]as part of a phase II clinical trial, but he did not respond. Forsecond-line therapy, the patient was then entered into a clinicaltrial assessing the combination of temsirolimus (inhibitor ofmTOR) and bevacizumab (anti-VEGF mAb), and he achieved apartial response (PR) lasting 10 months. Progression with newbone metastases as well as growth in lymph node and soft tissuemetastases made the patient eligible for a clinical trial with ananti–PD-1 mAb. The scan at week 6 (Fig. 2B) showed a 19.6%increase in tumor burden (stable disease according to RECISTcriteria). The patient continued in the study, especially in view ofhis symptomatic improvement (resolution of asthenia andanorexia). Subsequent scans at week 12 showed a PR, with target
lesions having decreased in size (Fig. 2C). This case illustrates thatdespite images that show apparent early growth, continued treat-ment may result in a clinical benefit to a particular patient.
Case 3 (Disease Stability before UltimateResponse)
A 72-year-old woman, who presented initially with a largeright-sided kidney cancer, underwent nephrectomy for ccRCC.Initial staging indicated good-IMDC risk metastatic disease. Thepatient was treated first with pazopanib (a TKI that targets, amongother receptors, VEGFRs, PDGFRs, and c-kit) for 18 months untilprogression, and then everolimus (mTOR inhibitor), which wasstopped after 1 month due to intolerance. Subsequently, thepatient received an anti–PD-1 mAb as part of a clinical trial.Scans initially showed stable disease with no tumor growth orshrinkage (Fig. 3B). After 8months of treatment, therewasmild tomoderate shrinkage of the target lesions (Fig. 3C). One year afterthe start of treatment, retrocaval adenopathy had resolved and thepatient achieved a delayed PR (Fig. 3D). At cycle 31 (month 21),the patient's treatment was complicated by pneumonitis, neces-sitating treatment discontinuation. The PR was maintained for 6months after she stopped the anti–PD-1 inhibitor, and then thepatient's disease progressed.
Case 4 (Mixed Response with New Lesion)A 57-year-old woman was diagnosed with intermediate-IMDC
riskmetastatic ccRCCwith sarcomatoid features and underwent aleft radical nephrectomy showing ccRCC. Shortly thereafter, shewas started on single-agent anti–PD-L1 mAb as part of a clinicaltrial. Her CT scan 8 weeks after the start of therapy showed thatseveral lung nodules had decreased in size (Fig. 4C) and lymphnodes (not pictured); however, there was a new small (<1 cm)
Figure 1.Complete response to PD-1 inhibitor. At baseline (A and B), contrast-enhanced CT shows mediastinal, hilar, and retroperitoneal lymphadenopathy, as wellas lung nodules. On the first follow-up CT scan 6 weeks later (C and D), complete resolution of the lymphadenopathy and lung metastases was shown.CR persists 2 years after stopping treatment (E and F).
Radiologic Response with Anti–PD-1/PD-L1 Therapy in mRCC
www.aacrjournals.org Cancer Immunol Res; 4(1) January 2016 13
on February 2, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/2326-6066.CIR-15-0197

indeterminate subcutaneous nodule in the left lower paraverteb-ral area (Fig. 4D). Additional imaging 8 weeks later showedcontinued shrinkage of the lung nodule and lymph nodes (Fig.4E), but with an increased size of the lesion in the lower back (Fig.4F). Excisional biopsy of the growing lesion was consistent withRCC with sarcomatoid features.
Case 5 (Early Progressive Disease/PrimaryRefractory Disease)
A49-year-oldmanwas diagnosedwith intermediate-IMDC riskmetastatic ccRCC and underwent surgical debulking of a T11lesion followed by radiation. Imaging showed pulmonary, adre-nal, and liver metastases. The patient progressed on sunitinib andbevacizumab-based clinical trial combinations. He was subse-quently started on an anti–PD-1 mAb as part of another clinicaltrial. The first CT scan after therapy initiation showed an increasein the size of liver lesions, with further increase on the secondfollow-up CT scan, as well as clinical deterioration, representingtrue progression (Fig. 5A–C).
DiscussionPD-1/PD-L1 pathway inhibitors have shownpromising activity
in the treatment of several advanced solid tumors (4, 5). Although
RCC has been treated with cytokines—immunomodulatingagents—for nearly 40 years (14), the imaging patterns and fea-tures of response to the new anti–PD-1/PD-L1 therapy needfurther characterization. In metastatic RCC, many clinical trialsare currently ongoing in the first- and second-line setting asmonotherapy, or in combination with targeted therapy or otherimmune-checkpoint blockers, such as CTLA-4 inhibitors. Indeed,a phase III clinical trial comparing nivolumab with everolimus(NCT01668784) has been stoppedprematurely because the studyhasmet the primary endpoint by demonstrating increased overallsurvival (OS) compared with the control arm in patients withpreviously treated mRCC (15).
In patients treated with these agents, interpretation of imag-ing results is challenging, considering the complexity of theimmune response and underlying tumor heterogeneity (16).This case series illustrates some of the imaging patterns ofresponse to PD-1/PD-L1–blocking agents being assessed foruse in metastatic RCC.
Up to 29% of objective responses, as per RECIST criteria, wereobserved in a refractory cohort of mRCC included in a phase Iclinical trial with nivolumab (2). In the same trial, 60%of patientswith mRCC had some degree of tumor shrinkage and 9%had atypical immune-related response as described in Case 2.Variable expression of PD-L1, differences in T-cell content or T-cell
Figure 2.Pseudoprogression to PD-1 inhibitor. Baseline CT shows a left retroperitoneal metastasis with enhancing solid component (A). This increased in size (longestdiameter by 19.6%) on a 6-week follow-up (B), before decreasing in size on 12-week follow-up (C).
Figure 3.Disease stability before ultimateresponse. Baseline contrast–enhancedCT (A) shows nodal metastases(arrows). Staging follow-up CT up to 4months after the start of treatmentshows radiologic stability (B). After4 months, the patient started toexperience gradual minor shrinkage inher target lesions, with mild tomoderate shrinkage at 8 months(C, arrows). One year after the start oftreatment (D), the retrocavaladenopathy resolved (the inferiorvena cava is now visualized at the sitewhere the adenopathy resolved), andthe patient experienced a delayedPR by RECIST.
de Velasco et al.
Cancer Immunol Res; 4(1) January 2016 Cancer Immunology Research14
on February 2, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/2326-6066.CIR-15-0197

response, and intertumoral heterogeneity in treated patients aresome of the possible explanations for these different patterns ofresponse (5, 17): Patients experiencing benefit may have differenttiming of response as seen in Cases 1 to 4, and physiciansmust befamiliar with the various patterns.
A CR, as shown in Case 1, is rarely seen in other targetedtherapies (less than 1% in first-line sunitinib or pazopanib;ref. 18). It is impossible to predict which patients will achievesuch a good response as there are no validated predictivebiomarkers despite intense research in this field (17). Further-more, the durable response in Case 1, with continued benefitextending more than 2 years after treatment was stopped, isextraordinary. This long-lasting response, without treatment, isin contrast with clinical experience with TKIs, the currentstandard of care in RCC, a setting in which treatment discon-tinuation is usually associated with growth or even growthacceleration in some reports (19).
In terms of the timing and kinetics of tumor shrinkage andresponse, it remains unknown whether patients with the bestoutcomes will be those who respond immediately to the first few
doses of therapy or those who require a longer period of time ontreatment, as seen in Case 3. If a longer time to produce responsewith the PD-1 pathway blockade is needed in some patients, wecould argue for a rational combinatorial approach with additionof another immune checkpoint blocker (e.g., CTLA-4 inhibitors)or a VEGF-targeted agent that may lead to a faster, and perhapsmore durable, response.
Genomic heterogeneity of tumors, a phenomenon well des-cribed in mRCC (20) and common in patients treated withtargeted therapy, may explain the mixed response seen in Case4. Although some of the lesions were responding, a dominantresistant population of cells may have been present at baseline(soft tissue nodule, Fig. 4F) andwas only appreciated after startingtherapy. This scenario suggests that genomic heterogeneity mayresult in a mixed response, as assessed by CT scans. It is notunreasonable that anti–PD-1 therapy be continued beyond "pro-gression," while addressing the "resistant clone" with a localtherapy such as surgery (20).
A challenging pattern of response is demonstrated in Case 2.The size ofmetastases may increase significantly before regression
Figure 4.Response with new lesion. At baseline (A and B), contrast-enhanced CT shows a right-lower-lobe lung metastasis. There is no focal abnormality in thesubcutaneous tissues of the lower back. On the first follow-up CT scan 8 weeks later (C and D), the lung metastasis has decreased in size and a lower backsubcutaneous nodule has developed. On the second follow-up CT scan 14 weeks after the start of treatment (E and F), the right-lower-lobe nodule has furtherdecreased in size, while the subcutaneous lesion has increased. Biopsy of the subcutaneous lesion revealed metastatic RCC.
Figure 5.Early progressive disease. Coronal contrast–enhanced CT before the start of treatment shows liver and left-adrenal metastases (A). Both kidneys are intact, as noprimary RCC was found in this patient. Coronal contrast–enhanced CT 6 weeks after the start of treatment shows mild to moderate increase in the size ofthe liver metastases and mild increase in the left adrenal metastasis (B). Coronal contrast–enhanced CT 12 weeks after the start of treatment confirms continuedgrowth of the lesions, representing true progression (C).
Radiologic Response with Anti–PD-1/PD-L1 Therapy in mRCC
www.aacrjournals.org Cancer Immunol Res; 4(1) January 2016 15
on February 2, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/2326-6066.CIR-15-0197

or response is detected, as previously described with ipilimumabtreatment inmelanoma (12). "Pseudoprogression" might lead topremature withdrawal of the treatment, which may not be in thepatient's best interest, particularly if the treatment is well toler-ated. A subsequent scan showed the delayed response. This is therationale for the recommendation of follow-up confirmatoryimaging, as described in the Immune-Related Response Criteria(irRC; ref. 21). The use of traditional imaging methods to assessresponse during the first few weeks may therefore be challenging.The immune response generated by these agents may produce"tumor inflammation," possibly due to a massive T-cell infiltra-tion in the target lesions, resulting in apparent tumor growth (12).Careful evaluation of each patient's clinical situation is importantto avoid either premature discontinuation or a continuation oftherapy when the patient is not actually benefiting. Comprehen-sive evaluation of new or enlarging lesions early in the course oftherapy should also include assessment of location of the lesionand the amount of growth, to decide upon the need for acomplementary intervention or a change in systemic treatment.The symptomatic improvement in our patient led us to continuesystemic therapy. The irRC, still under development, may play amajor role in guiding response assessment in mRCC patientstreated with PD-1/PD-L1 inhibitors (22).
Another unanswered question in the use of checkpoint immunetherapies in mRCC involves the optimum length of treatment.Everolimuscanprovideclinicalbenefit/disease stabilization regard-less of whether treated patients experience a significant decrease intumor burden (23). This has been well captured with PFS as theendpoint, a strategy used for the approval ofmost targeted agents inmRCC. However, use of PFS as an endpoint in mRCC patientstreatedwith immune checkpoint blockersmay not be ideal.Motzerand colleagues (24) used median PFS from nivolumab as theendpoint in their study of mRCC; PFS ranged between 2.7 and4.2 months, despite a very promising OS ranging between 18and 25 months in a highly refractory mRCC population. ThePFS in these reports suggests a moderate benefit, at best, so itdoes not necessarily reflect the efficacy of PD-1/PD-L1 inhibi-tors for some patients with mRCC. Median OS would moreaccurately describe antitumor activity. In this series, PFS in Case2 might have been reported in as short a time as 6 weeks.
As highlighted in Case 1, patients may achieve an immediateCR as a durable event after stopping treatment. Even in this earlystage of development, durable responses with PD-1 inhibitorshave already been reported in mRCC (2). Conversely, Case 3illustrates a prolonged time to achieve PR, though the clinicalbenefits and CT scans continued for more than 2 years. It ispossible that intermittent treatment, whether by reinstating ther-apy upon progression or instituting a treatment break after anoptimal response is achieved, has a place in certain subsets ofpatients who achieve an exceptional initial response, with theadvantage of less potential toxicity and cost savings. Genome
sequencing analysis of tumor biopsy samples could help todefine the escape resistance mechanisms, which may be due tocomplex immune mechanisms or merely "de novo" mutations,as seen with some forms of targeted therapy (25).
ConclusionsThe response to anti–PD-1/PD-L1 agents may be very hetero-
geneous, with a spectrum of patterns seen on imaging. Carefulassessment of the responses of patients treatedwith these immunecheckpoint inhibitors is needed, andmultidisciplinary awarenessof the commonly observed patterns and potential pitfalls ininterpretation (i.e., "pseudoprogression") is necessary. Observeddurable responses to treatment represent a great source of opti-mism and hope in the management of advanced RCC.
Disclosure of Potential Conflicts of InterestL. Albiges serves in a consulting or advisory role for Bristol-Myers Squibb,
Pfizer, Novartis, and Bayer. J. Bellmunt serves in a consulting or advisory rolefor Pfizer, GlaxoSmithKline, Novartis, Bristol-Myers Squibb, and Genentech.F.S. Hodi is a consultant at Merck and Genentech, reports receiving acommercial research grant from Bristol-Myers Squibb and has ownershipinterest (including patents) in MICA Related Disorders IP as per institutionalpolicy. T.K. Choueiri serves in an advisory role for Bristol-Myers Squibb,Merck, and Roche.
Authors' ContributionsConception and design: G. de Velasco, L. Albiges, T.K. ChoueiriDevelopment of methodology: G. de Velasco, L. Albiges, F.S. Hodi,T.K. ChoueiriAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): G. de Velasco, K.M. Krajewski, L. Albiges, J. Bellmunt,F.S. Hodi, T.K. ChoueiriAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis):G. de Velasco, K.M. Krajewski, L. Albiges,M.M. Awad,F.S. Hodi, T.K. ChoueiriWriting, review, and/or revision of the manuscript: G. de Velasco,K.M. Krajewski, L. Albiges, M.M. Awad, J. Bellmunt, F.S. Hodi, T.K. ChoueiriAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): G. de Velasco, T.K. ChoueiriStudy supervision: G. de Velasco, T.K. Choueiri
Grant SupportThis study was supported by The Trust family, Loker Pinard, and Michael
Brigham Funds for Kidney Cancer Research (to T.K. Choueiri) at Dana-FarberCancer Institute, the Dana-Farber/Harvard Cancer Center Kidney Cancer Pro-gram, and the Dana-Farber/Harvard Cancer Center Kidney Cancer SPORE P50CA101942-01. It was also supported by the Spanish Society of Medical Oncol-ogy (SEOM/CRIS; to G. de Velasco).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
ReceivedAugust 10, 2015; revised September 4, 2015; accepted September 21,2015; published OnlineFirst November 20, 2015.
References1. Freeman GJ, Long AJ, Iwai Y, Bourque K, Chernova T, Nishimura H, et al.
Engagement of the PD-1 immunoinhibitory receptor by a novel B7 familymember leads to negative regulation of lymphocyte activation. J Exp Med2000;192:1027–34.
2. McDermott DF, Drake CG, Sznol M, Choueiri TK, Powderly JD, SmithDC, et al. Survival, durable response, and long-term safety in patientswith previously treated advanced renal cell carcinoma receiving nivo-lumab. J Clin Oncol 2015;33:2013–20.
3. Powles T, Eder JP, Fine GD, Braiteh FS, Loriot Y, Cruz C, et al. MPDL3280A(anti-PD-L1) treatment leads to clinical activity in metastatic bladdercancer. Nature 2014;515:558–62.
4. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, Lao CD, et al.Combined nivolumab and ipilimumab or monotherapy in untreatedmelanoma. N Engl J Med 2015;373:23–34
5. Harshman LC, Drake CG, Choueiri TK. PD-1 blockade in renal cell carci-noma: to equilibrium and beyond. Cancer Immunol Res 2014;2:1132–41.
de Velasco et al.
Cancer Immunol Res; 4(1) January 2016 Cancer Immunology Research16
on February 2, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/2326-6066.CIR-15-0197

6. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm436534.htm [Internet]. Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm436534.htm.
7. U.S. Department of Health and Human Services. FDA expands approveduse of Opdivo to treat lung cancer [Internet]. 2015 [cited 2015 Jul 7].Available from: http://www.fda.gov/newsevents/newsroom/pressan-nouncements/ucm436534.htm.
8. http://www.cancer.gov/about-cancer/treatment/clinical-trials/search/results?protocolsearchid¼6371785 [Internet]. Available from: http://www.cancer.gov/about-cancer/treatment/clinical-trials/search/results?protocolsearchid¼6371785.
9. Atkins MB, Choueiri TK, Hodi FS. Pembrolizumab (MK-3475) plus low-dose ipilimumab (IPI) in patients (pts)with advancedmelanoma (MEL) orrenal cell carcinoma (RCC): data from the KEYNOTE-029 phase 1 study. InJ Clin Oncol 2015;33 (suppl; abstr 3009). Available from: http://meet-inglibrary.asco.org/content/149087-156.
10. McDermott DF, Sznol M, Sosman JA. Immune correlates and long termfollow up of a phase Ia study of MPDL3280A, an engineered PD-L1antibody, in patients with metastatic renal cell carcinoma (mRCC).Ann Oncol (2014) 25 (suppl_4): iv280-iv304. 10.1093/annonc/mdu337.
11. CallahanMK, Ott PA, Odunsi K. A phase 1 study to evaluate the safety andtolerability of MEDI4736, an anti–PD-L1 antibody, in combinationwith tremelimumab in patients with advanced solid tumors. J Clin Oncol2014;32:5s. (suppl; abstr TPS3120^). Available from: http://meetingli-brary.asco.org/content/130062-144.
12. Saenger YM, Wolchok JD. The heterogeneity of the kinetics of responseto ipilimumab in metastatic melanoma: patient cases. Cancer Immun2008;8:1.
13. Rihan FA, Abdelrahman DH, Al-Maskari F, Ibrahim F, Abdeen MA. Delaydifferentialmodel for tumour-immune responsewith chemoimmunother-apy and optimal control. ComputMathMethodsMed 2014;2014:982978.
14. Ferreira AM, Mendes JR. Regression of bone metastases from renal cellcarcinoma achieved by combined therapy. Eur Urol 1976;2:100–1.
15. CheckMate -025, a Pivotal Phase III Opdivo (nivolumab) Renal CellCancer Trial, Stopped Early [Internet]. 2015. [cited July 20 2015]. Availablefrom: http://news.bms.com/press-release/checkmate-025-pivotal-phase-iii-opdivo-nivolumab-renal-cell-cancer-trial-stopped-early.
16. Junttila MR, de Sauvage FJ. Influence of tumour micro-environmentheterogeneity on therapeutic response. Nature 2013;501:346–54.
17. Choueiri TK, Fishman MN, Escudier BJ. Immunomodulatory activity ofnivolumab in previously treated and untreated metastatic renal cell car-cinoma (mRCC): biomarker-based results froma randomized clinical trial.In J Clin Oncol 32:5s, 2014.
18. Motzer RJ, Hutson TE, McCann L, Deen K, Choueiri TK. Overall survival inrenal-cell carcinoma with pazopanib versus sunitinib. N Engl J Med2014;370:1769–70.
19. Iacovelli R,Massari F, Albiges L, Loriot Y,MassardC, Fizazi K, et al. Evidenceand clinical relevance of tumor flare in patients who discontinue tyrosinekinase inhibitors for treatment of metastatic renal cell carcinoma. Eur Urol2015;68:154–60.
20. Gerlinger M, Horswell S, Larkin J, Rowan AJ, Salm MP, Varela I,et al. Genomic architecture and evolution of clear cell renal cellcarcinomas defined by multiregion sequencing. Nat Genet 2014;46:225–33.
21. Wolchok JD, Hoos A, O'Day S, Weber JS, Hamid O, Lebb�e C, et al.Guidelines for the evaluation of immune therapy activity in solidtumors: immune-related response criteria. Clin Cancer Res 2009;15:7412–20.
22. NishinoM,Giobbie-Hurder A,GarganoM, SudaM, RamaiyaNH,Hodi FS.Developing a common language for tumor response to immunotherapy:immune-related response criteria using unidimensional measurements.Clin Cancer Res 2013;19:3936–43.
23. Stein A, Bellmunt J, Escudier B, Kim D, Stergiopoulos SG, Mietlowski W,et al. Survival prediction in everolimus-treated patients with metastaticrenal cell carcinoma incorporating tumor burden response in theRECORD-1 trial. Eur Urol 2013;64:994–1002.
24. Motzer RJ, Rini BI, McDermott DF, Redman BG, Kuzel TM, HarrisonMR, et al. Nivolumab for metastatic renal cell carcinoma: results of arandomized phase II trial. J Clin Oncol [Internet]. 2014 Dec 1 [cited2015 Apr 6]. Available from: http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2014.59.0703.
25. Wagle N, Berger MF, Davis MJ, Blumenstiel B, Defelice M, Pochanard P,et al. High-throughput detection of actionable genomic alterations inclinical tumor samples by targeted, massively parallel sequencing.Cancer Discov 2012;2:82–93.
www.aacrjournals.org Cancer Immunol Res; 4(1) January 2016 17
Radiologic Response with Anti–PD-1/PD-L1 Therapy in mRCC
on February 2, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/2326-6066.CIR-15-0197

2016;4:12-17. Published OnlineFirst November 20, 2015.Cancer Immunol Res Guillermo de Velasco, Katherine M. Krajewski, Laurence Albiges, et al. Therapy in Metastatic Renal Cell Carcinoma
PD-1/PD-L1−Radiologic Heterogeneity in Responses to Anti
Updated version
10.1158/2326-6066.CIR-15-0197doi:
Access the most recent version of this article at:
Cited articles
http://cancerimmunolres.aacrjournals.org/content/4/1/12.full#ref-list-1
This article cites 17 articles, 7 of which you can access for free at:
Citing articles
http://cancerimmunolres.aacrjournals.org/content/4/1/12.full#related-urls
This article has been cited by 3 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerimmunolres.aacrjournals.org/content/4/1/12To request permission to re-use all or part of this article, use this link
on February 2, 2020. © 2016 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst November 20, 2015; DOI: 10.1158/2326-6066.CIR-15-0197