Embed Size (px)
Citation preview
Radiologic Terrorism• Radiation Exposure• Dirty Bombs• Atomic Bombs
Five decades after the first atomic bomb
Terrorist atomic bomb
• Nuclear Power Plants
Three Mile Island accident 1978 in PA
Chernobyl accident, April 26, 1986, in the Ukrainian SSR
• Management of pregnant women and children
Radiologic Terrorism• Radiation Exposure• Dirty Bombs• Atomic Bombs
Five decades after the first atomic bomb
Terrorist atomic bomb
• Nuclear Power Plants
Three Mile Island accident 1978 in PA
Chernobyl accident, April 26, 1986, in the Ukrainian SSR
• Management of pregnant women and children
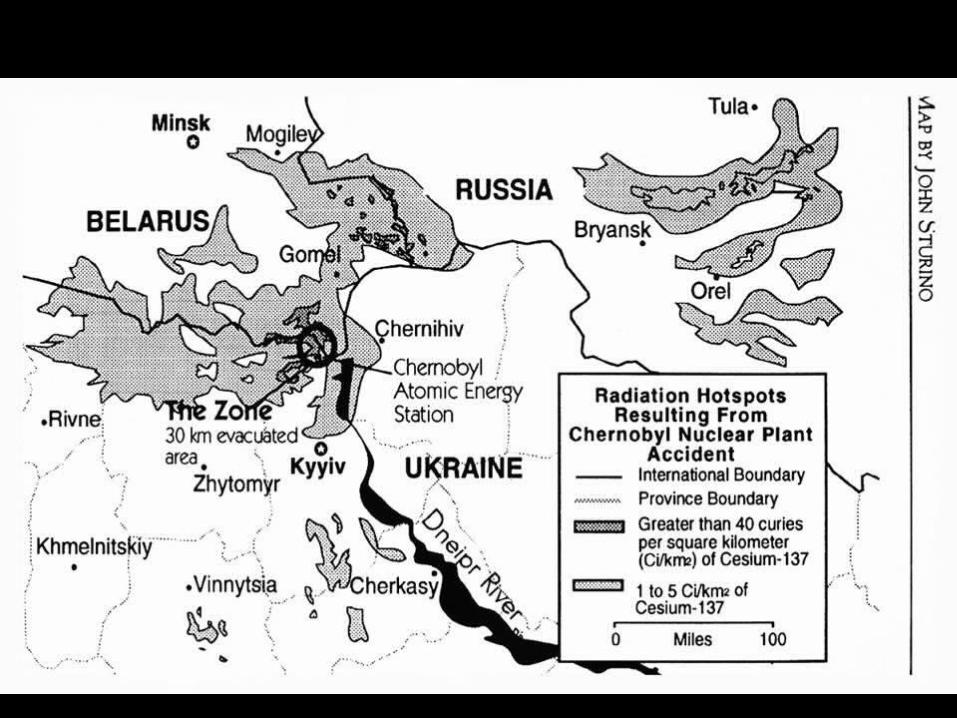
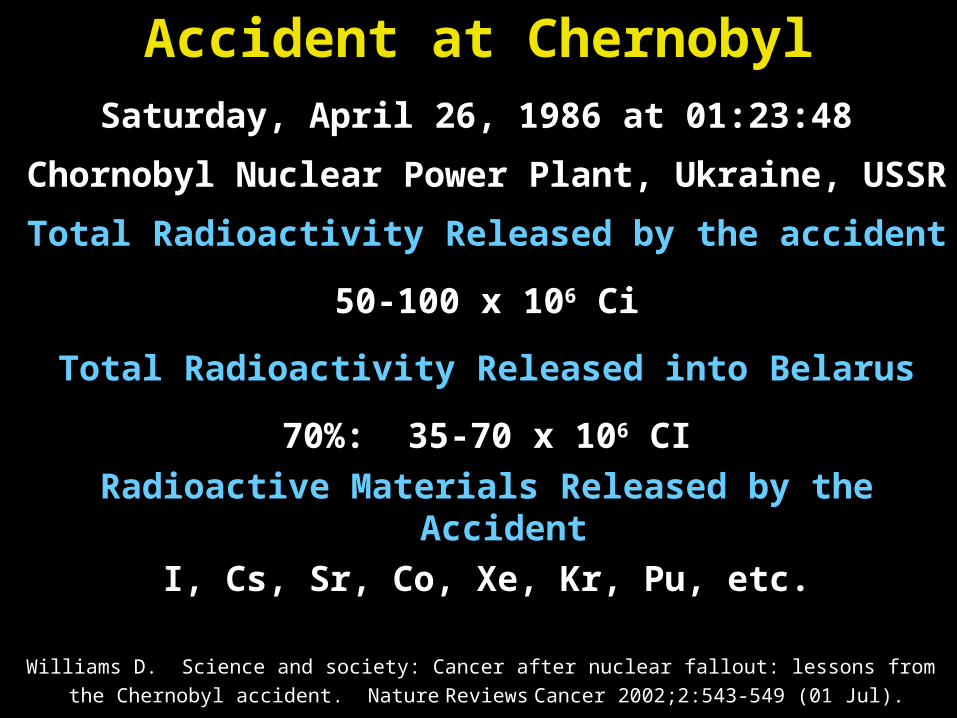
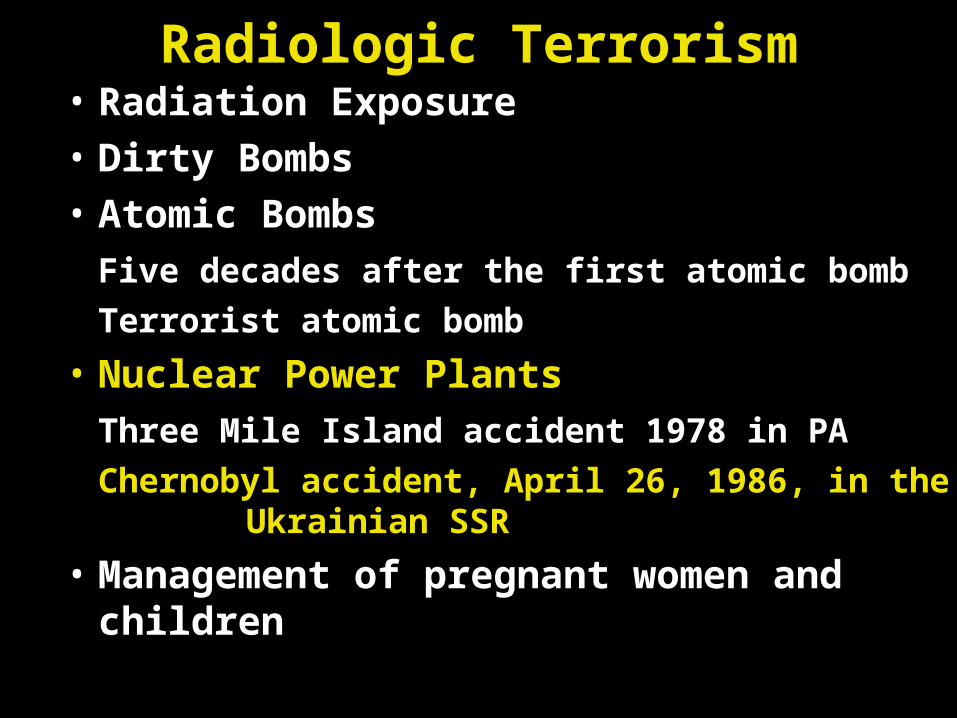
Accident at ChernobylSaturday, April 26, 1986 at 01:23:48
Chornobyl Nuclear Power Plant, Ukraine, USSR
Total Radioactivity Released by the accident
50-100 x 106 Ci
Total Radioactivity Released into Belarus
70%: 35-70 x 106 CI
Radioactive Materials Released by the Accident
I, Cs, Sr, Co, Xe, Kr, Pu, etc.
Williams D. Science and society: Cancer after nuclear fallout: lessons from
the Chernobyl accident. Nature Reviews Cancer 2002;2:543-549 (01 Jul).
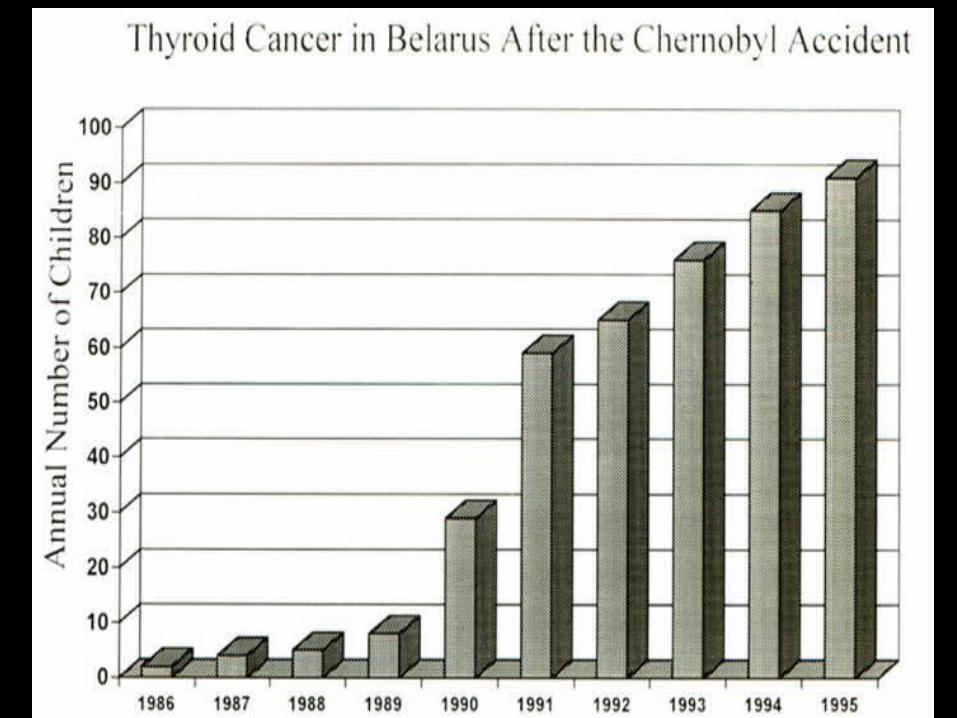
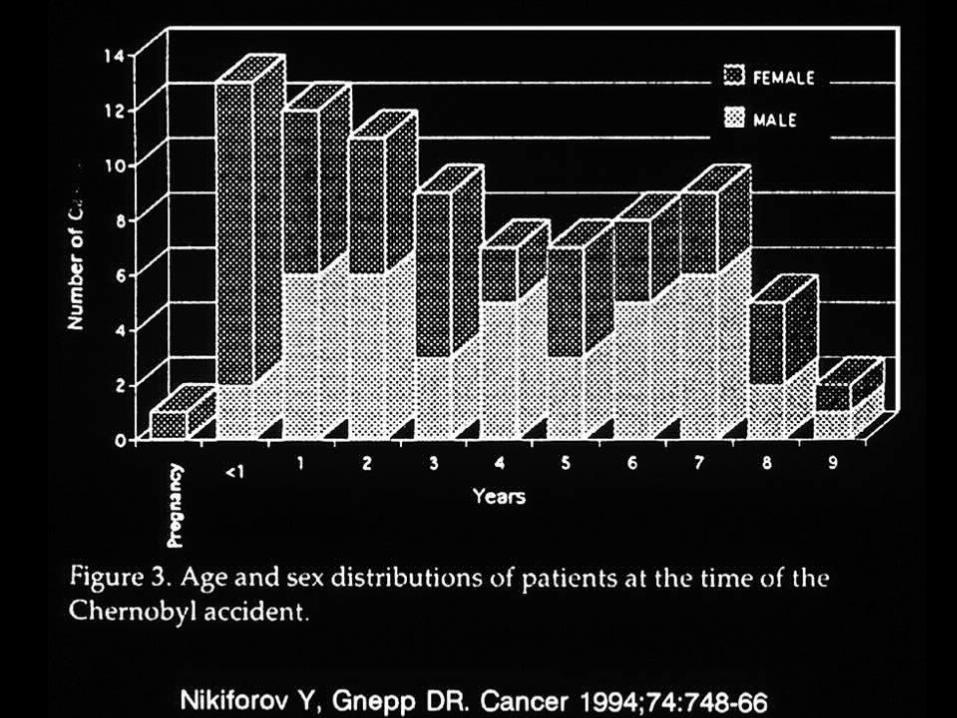

Populations at High Risk for Thyroid Neoplasia from Exposure to Radiation
• Fetus after 12 weeks of gestation in April 1986.• Number of cases dramatically decreased after 2000.
• Children ages < 6 years in April, 1986.• Children ages 0 to 1 year have the highest risk.
• Children living in areas with iodine deficiency.• Greater radioiodine uptake increases the dose of
radiation exposure to the thyroid gland.
• Children exposed to > 1 cGy of radiation.• Rapid thyroid growth in young children occurs with
chromosomal rearrangements (PTC1 and PTC3).

The Carcinogenic Effects of Radiation
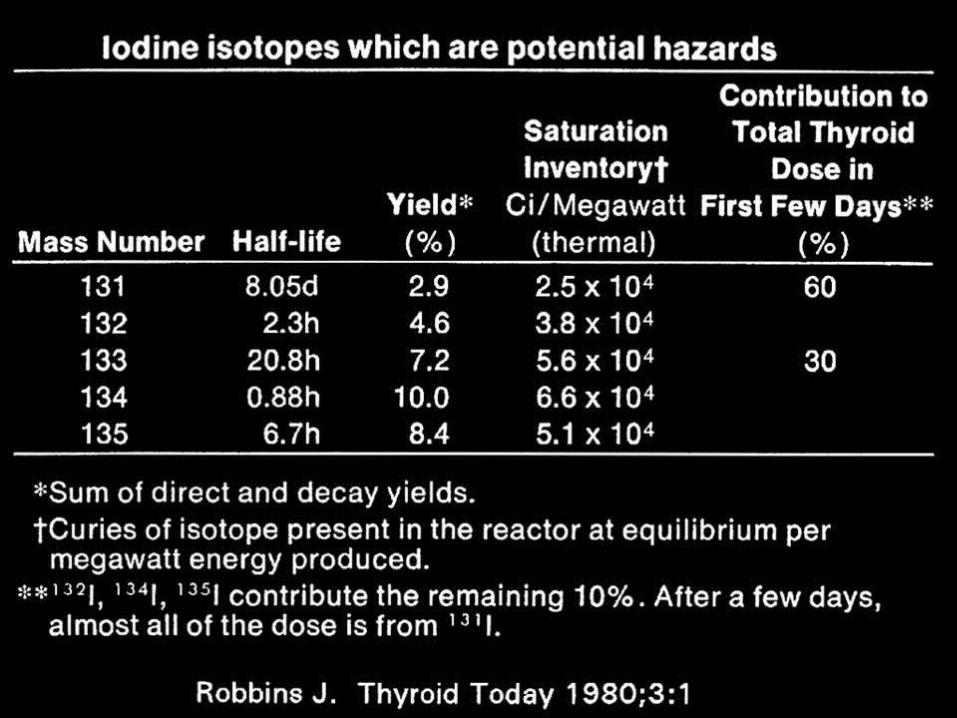
• The isotopes of iodine-131, -132, -133
• Chronic exposure to Cesium-137
• Higher tissue exposure to radiation occurs in those tissues that concentrate iodine:
– Thyroid → ↑ incidence of adenoma, carcinoma
– Breast → ↑ incidence of carcinoma
– Salivary gland
– Gastric mucosa
Iodine Prophylaxis in Poland
• Radiation detected 36 hours after initial release.• KI distribution began in the PM on day 3.
– 10.5 million doses of KI given to children– 7 milion doses of KI given to adults
• Exposure to radioiodines in infants age < 1 year– > 50 mSv (5 Rem) if unprotected from radioiodine– < 50 mSv when protected by KI + substituted
milk• KI caused ~ 40% reduction in Rem dose to thyroid.
With early prophylaxis, ~ 60-70% reduction in Rem dose primarily because inhaled 131I is blocked.
• Incidence of 0.2% for medically significant, but not serious side effects.
Radiologic Terrorism• Radiation Exposure• Dirty Bombs• Atomic Bombs
Five decades after the first atomic bomb
Terrorist atomic bomb
• Nuclear Power Plants
Three Mile Island accident 1978 in PA
Chernobyl accident, April 26, 1986, in the Ukrainian SSR
• Management of pregnant women and children
Management of Pregnant Women and Children Exposed to Radiation
• Evacuation– Priority evacuation protocols for pregnant
women, infants and pre-pubertal children– Evacuation to an identified location at least 50
miles from the source of radiation
• Potassium Iodide– KI tablets or liquid administered on
notification by authorities of the possibility of radiation exposure.
– Dose schedules and negligible toxicity
Evacuation of Pregnant Women and Children Exposed to Radiation
• Priority Evacuation– Priority identification signs should be provided
to pregnant women and families of infants and pre-pubertal children to display on the windshield for priority rapid “HOV-lane” emergency evacuation.
– Evacuation routes should be defined in advance.
• Distance from Radiation Source– The radiation plume travels in the direction and
at the speed of the prevailing winds.– Biologically significant radiation exposure may
occur 100-200 miles from the source depending upon the atmospheric conditions.
Management of Pregnant Women and Children Exposed to Radiation
• Evacuation– Priority evacuation protocols for pregnant
women, infants and pre-pubertal children– Evacuation to an identified location at least 50
miles from the source of radiation
• Potassium Iodide– KI tablets or liquid administered on
notification by authorities of the possibility of radiation exposure.
– Dose schedules and negligible toxicity
KI Therapy for Pregnant Women and Children Exposed to Radiation
• Potassium Iodide for Radioiodine Exposure– Pre-packaged, pre-distributed KI tablets or liquid
should be readily available in homes, schools, day care centers and nurseries near reactors.
– On notification by authorities of the possibility of radiation exposure, parents should give or have given authorization to dispense KI if authorities declare a radiation-exposure emergency.
• KI toxicity– Negligible, minor side effects, and rare in children.
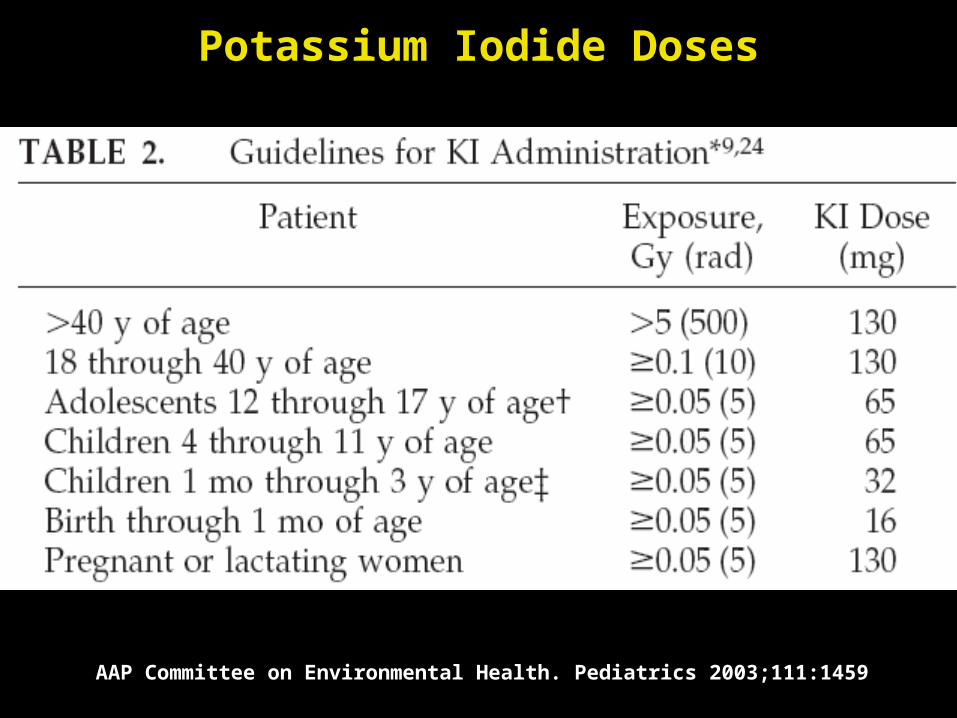
Potassium Iodide Doses
AAP Committee on Environmental Health. Pediatrics 2003;111:1459
KI Therapy for Pregnant Women and Children Exposed to Radiation
• Potassium Iodide for Radioiodine Exposure– Pre-packaged, pre-distributed KI tablets or liquid
should be readily available in homes, schools, day care centers and nurseries near reactors.
– On notification by authorities of the possibility of radiation exposure, parents should give or have given authorization to dispense KI if authorities declare a radiation-exposure emergency.
• KI toxicity– Negligible except in very rare cases of iodinism.
Potassium Iodide Safety• KI toxicity
– Acute poisoning is uncommon– Hypersensitivity reactions are rare, but dangerous:
• Angioedema and laryngeal edema• Serum-sickness-like reactions
[fever, lymphadenitis, arthralgia, arthritis]• Chronic exposure
– Iodism (parotid pain and swelling); skin rashes– Goiter and primary hypothyroidism on occasion at any age
• Contraindicated during pregnancy and infancy• High dose KI as treatment of Sporotrichosis
– Children: 50 mg/dose tid; ↑ by 50 mg/dose daily– Children: 150-500 mg/dose up to 500-750 mg tid– Older Child: 250 mg tid; Maximum: 1-2 grams/dose tid
Management of Children Exposed to Ionizing Radiation
• Preparation: Supplies of KI, infant formula, powered milkEvacuation routes and locations
• Emergency battery operated communications– Radios– Cellular telephones
• Priority EvacuationDefined routes [HOV Routes]Priority evacuation Identification on vehicles
• Potassium iodidePriority 1: pregnant women and infantsPriority 2: young children
• Monitor TSH in infants and pregnant women
Radiologic Terrorism: Bibliography• Williams, Dillwyn. Science and society: Cancer after
nuclear fallout: lessons from the Chernobyl accident. Nature Reviews Cancer 2002;2:543-549 (01 Jul). [Review]
• CDC: www.bt.cdc.gov/radiation• AAP Policy Statement. Radiation disasters and children.
Pediat 2003;111(6):1455-1466.• Mettler FA, Voelz GL. Major radiation exposure – what to
expect and how to respond. NEJM 2002;346:1554-1561.• www.atomicarchives.com/Example/ExampleStart.shtml• Nauman J, Wolff J. Iodide prophylaxis in Poland after the
Chernobyl reactor accident: Benefits and risks. Am J Med 1993;94(5):524-532. [Review]
• Nagataki S, Yamashita S, Eds. Nagasaki Symposium Radiation & Human Health, Elsevier, 1996, p xii.