Embed Size (px)
Citation preview

Radiology Grand Rounds University of Maryland
Baltimore, MDFebruary 1, 2006
Radiology Grand Rounds University of Maryland
Baltimore, MDFebruary 1, 2006
Impact of Advanced TechnologiesFuture of Medicine
Impact of Advanced TechnologiesFuture of Medicine
Richard M. Satava, MD FACSProfessor of Surgery
University of Washington
Program Manager, Advanced Biomedical TechnologiesDefense Advanced Research Projects Agency (DARPA)
and
Special Assistant, Advance Medical TechnologiesUS Army Medical Research and Materiel Command
Richard M. Satava, MD FACSProfessor of Surgery
University of Washington
Program Manager, Advanced Biomedical TechnologiesDefense Advanced Research Projects Agency (DARPA)
and
Special Assistant, Advance Medical TechnologiesUS Army Medical Research and Materiel Command
on the

Conflict of
Interest
Truth in
Advertising
I have nothing to disclose
and no conflict of interest with any corporation
or institution

Air Force 1 - refit Unofficial Administration request
UNCLASSIFIED


“The Future is not what it used to be”
….Yogi Berra
“The Future is not what it used to be”
….Yogi Berra
Disruptive Visions
“The Future is here …
. . . it’s the Information Age”
“The Future is here …
. . . it’s the Information Age”
Current Visions

New technologies that are emerging from Information Age discoveries are changing our basic approach in all areas of medicine
. . . EXAMPLES
New technologies that are emerging from Information Age discoveries are changing our basic approach in all areas of medicine
. . . EXAMPLES
Fundamental Concept
Information basis for surgery
Borrow from Industry - CAD/CAM
Information basis for surgery
Borrow from Industry - CAD/CAM
The Fundamental Changes

Why Robots?
The Touch Lab, MITMovie: Alien

Holomer Total body-scan for total diagnosis
Satava March, 2004
From visible human to Virtual Soldier Multi-modal total body scan on every trauma patient in 15 seconds

Why robotics, imaging and modeling & simulation
• Healthcare is the only industry without a computer representation of its “product”
•A robot is not a machine . . .it is an information system with arms . . .
• A CT scanner is not an imaging system it is an information system with eyes . . .
thus
• An operating room is an information system with . . .

Total Integration of Surgical Care
Joel Jensen, SRI International, Menlo Park, CA
Minimally Invasive Surgery
Pre-operative planning
Intra-operative navigation
Remote Surgery
Simulation & Training
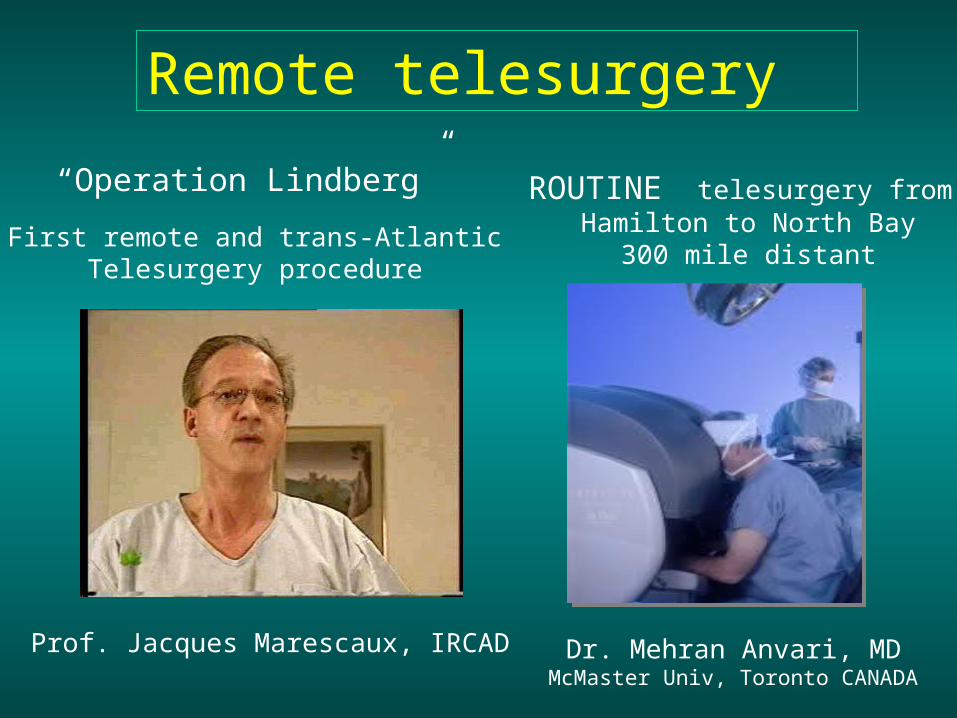
Prof. Jacques Marescaux, IRCAD
Remote telesurgery
Dr. Mehran Anvari, MDMcMaster Univ, Toronto CANADA
“Operation Lindberg”
First remote and trans-AtlanticTelesurgery procedure
ROUTINE telesurgery from Hamilton to North Bay
300 mile distant
Mechanical to directed-energy
Therapy to combined with Diagnosis
Minimally invasive to non-invasive
Macro to micro to intra-cellular
Mechanical to directed-energy
Therapy to combined with Diagnosis
Minimally invasive to non-invasive
Macro to micro to intra-cellular
Different instrumentation

“TriCorder” Point-of-care noninvasive therapy
High Intensity Focused Ultrasound for Non-invasiveAcoustic hemostasis
HIFU
Courtesy Larry Crum, Univ Washinton Applied Physics Lab
Mechanics to energy
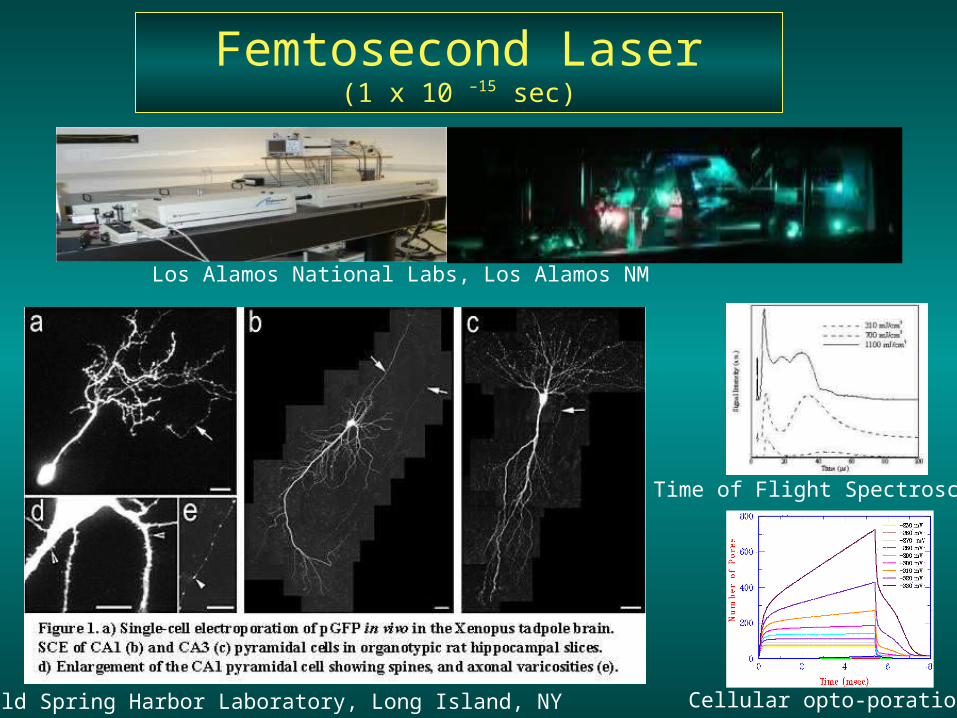
Cold Spring Harbor Laboratory, Long Island, NY
Femtosecond Laser(1 x 10 –15 sec)
Time of Flight Spectroscopy
Cellular opto-poration
Los Alamos National Labs, Los Alamos NM
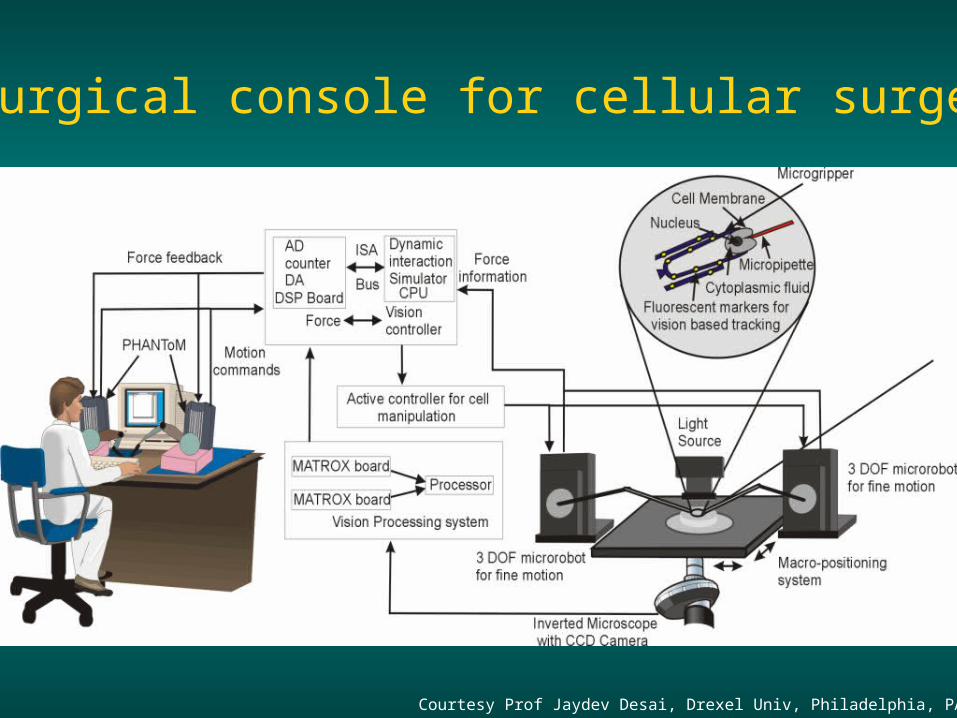
Surgical console for cellular surgery
Courtesy Prof Jaydev Desai, Drexel Univ, Philadelphia, PA 2005

Surgical console for cellular surgery
Courtesy Prof Jaydev Desai, Drexel Univ, Philadelphia, PA 2005
Motion Commands

Fig. 2. Top: Fluorescent micrograph of the actin cytoskeleton of an engineered striated muscle cell. Bottom: AFM-acquired topographical map. Wrinkles and lines along the diagonals of the 30 micron square are actin stress fibers under the lipid membrane surface.
Fig. 3. Schematic illustrating the technique for functionalizing AFM tips to identify specific molecules on the cell surface during raster scanning.
Fig. 4. Nanoincision by electroporation. (A) The AFM cantilever is positioned above a region of interest in the cell. (B) Electrical current is injected through the cantilever tip, causing the formation of a nanometer scale pore in the membrane, thru which the AFM tip can be dropped, or other instrumentation attached to the tip, prior to the membrane resealing.
New Surgical Tools
Courtesy Prof Kit Parker, MD, Harvard Univ, Boston, MA 2005
Atomic Force Microscope ManipulatorFemtosecond Lasers

Mechanical to directed-energy
Therapy to combined with Diagnosis
Minimally invasive to non-invasive
Macro to micro to intra-cellular
Mechanical to directed-energy
Therapy to combined with Diagnosis
Minimally invasive to non-invasive
Macro to micro to intra-cellular
Trans-gastric and Natural Orifice
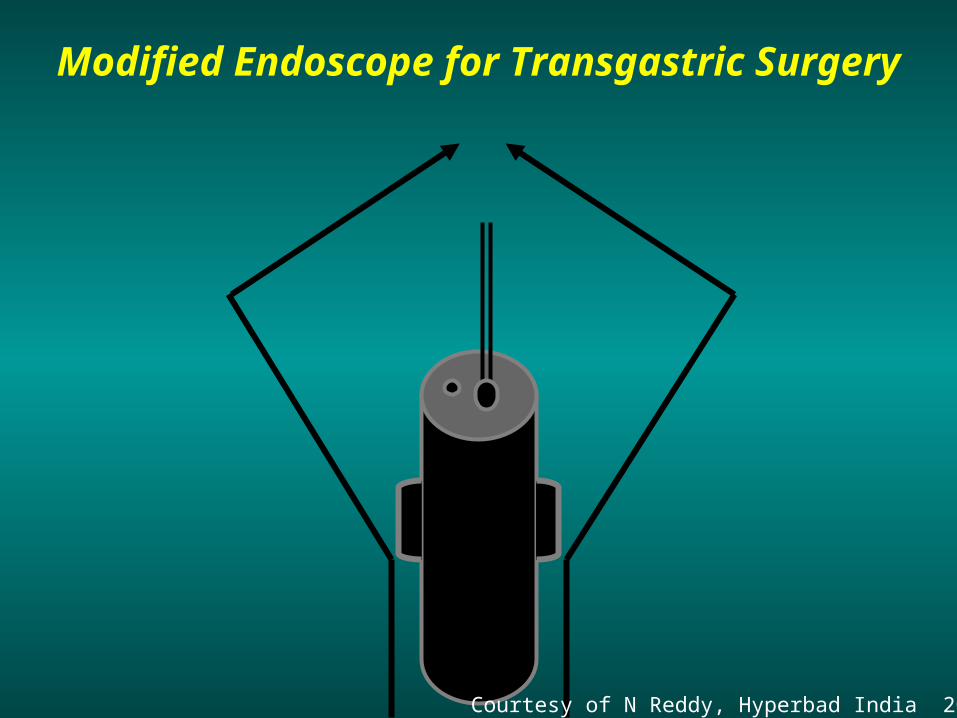
Modified Endoscope for Transgastric Surgery
Courtesy of N Reddy, Hyperbad India 20005

Trans Oral Intra-peritoneal Surgery - Future
Courtesy of N Reddy, Hyperbad India 20005

Peroral Transgastric Endoscopic Surgery
Need for development of modified accessories and endoscopes
Courtesy of N Reddy, Hyperbad India 20005

Early Luminal Malignancies - Robotic EMR
Courtesy of N Reddy, Hyperbad India 20005
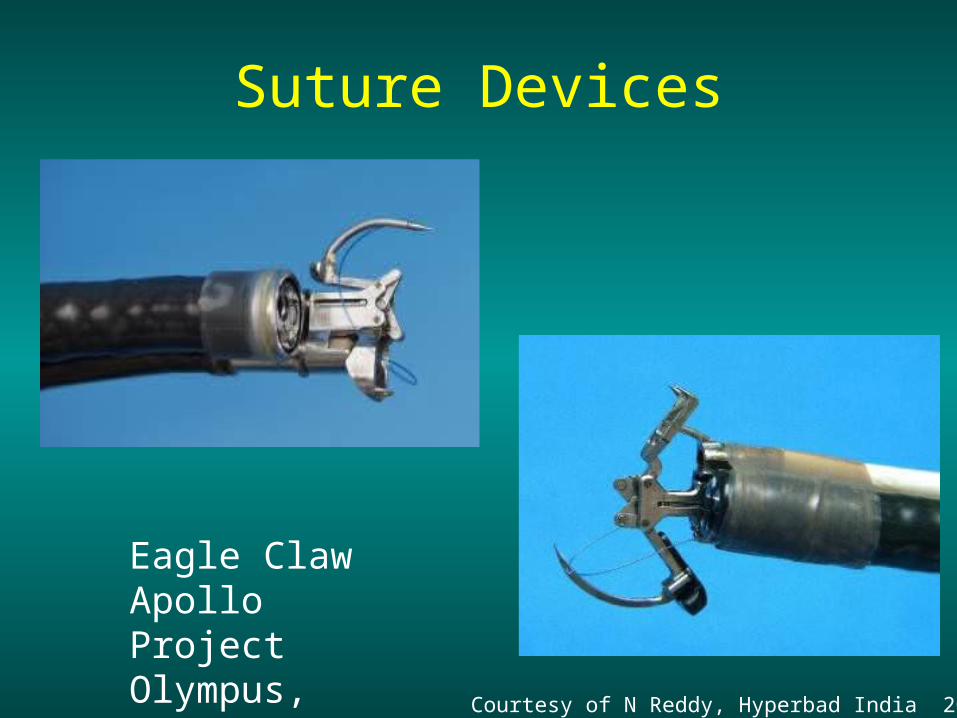
Suture Devices
Eagle ClawApollo ProjectOlympus, Tokyo.
Courtesy of N Reddy, Hyperbad India 20005

Trans-gastric appendectomy
Courtesy of N Reddy, Hyperbad India 20005

So What ?

Figure 3. Micro-robotic endoscopy. Physician controling micro-robot (which has been inserted into the rectum) from endoscope workstation
Figure 2. Translational endoscopy workstation. Physician advancing insertion tube of colonoscope by hand while controlling the tip and valves from endoscopic workstation.
Figure 1. Conventional colonoscopy
Satava RM Future of endoscopy. GI Clin NA, Oct, 1983

Operating Room without lights
Operating Room without people
Operating Room without anesthesia
Operating Room without lights
Operating Room without people
Operating Room without anesthesia
The “operating room” of the future

Eric LaPorta, Barcelona, Spain 2005
New Concepts for OR of the Future
Lighting

“Ubiquitous lights” and “Sea of Cameras”Courtesy Eric LaPorte, MD Barcelona, Spain 2005Courtesy Takeo Kanade, PhD Pittsburg, PA 1999
l
Continuous training, assessment and maintenance of certification
“Black Box”

“Penelope” – robotic scrub nurse
Michael Treat MD, Columbia Univ, NYC. 2003

Integrating Surgical Systems for AutonomyThe Operating Room (personnel) of the Future
Satava March, 2000
Surgeon Assistant Scrub Nurse Circulating nurse
100,000



The Operating Room of the Future


SATAVA 7 July, 1999DARPA
Fighter Pilots – until 2002 Fighter Pilots – Beyond 2003Predator 2003


Wizard of Id by Brant Parker

Robotic Medical Assistant
SATAVA 7 July, 1999DARPA
Nursing shortage crisis
Applicable at all levelsHospitalsClinicsNursing HomeAssisted living
Courtesy Yulun Wang, InTouch Technologies, Inc, Goleta, CA

Biomimetic Micro-robot
Courtesy Sandia National Labs
Capsule camera for gastrointestinal endoscopy
Courtesy Paul Swain, London, England


University of Wisconson, 1999

Greg Kovacs. Stanford University, 1990
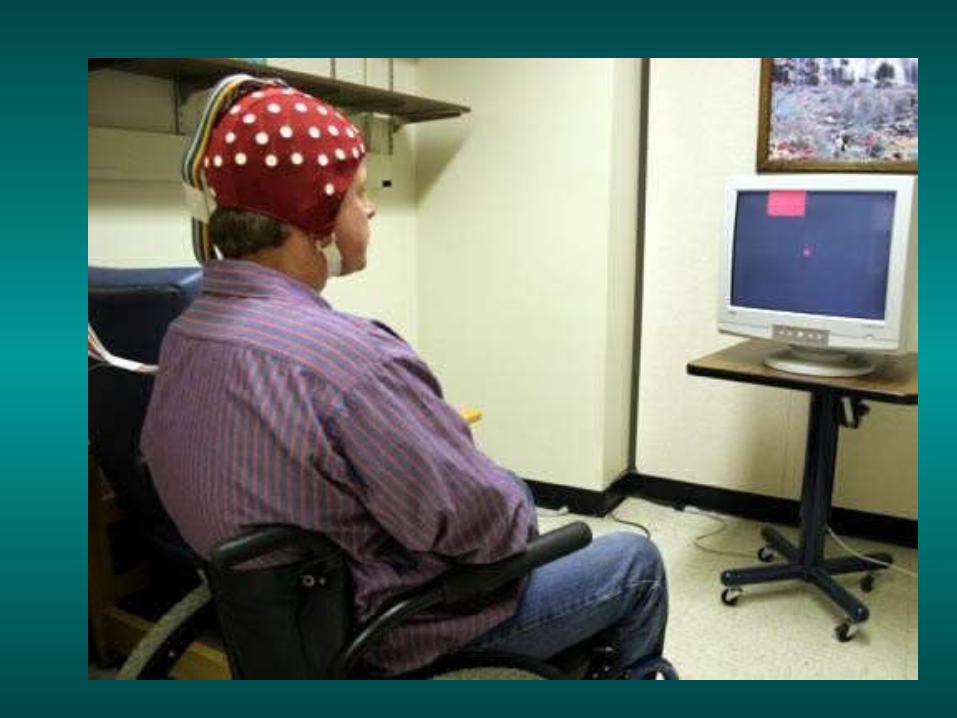
“BrainGate” John Donohue, Brown University, 2001
Richard Andersen, CalTech, 2003

Recorded activity for intended movement to a briefly flashed target.
TARGET MOVEMENT
Time
PLAN
Courtesy Richard Andersen, Cal Tech, Pasadena, CA
Brain Machine Interface – Controlling motion with thoughts

Thoughts into Action
Miguel Nicholai, Duke University, 2002Satava March, 2000
Direct brain implant control of robot arm


Relative size of subjects
Alaska Black Bear
Artic Ground Squirrel
Research in hibernation suspended animation hypometabolic states
resuscitation reperfusion
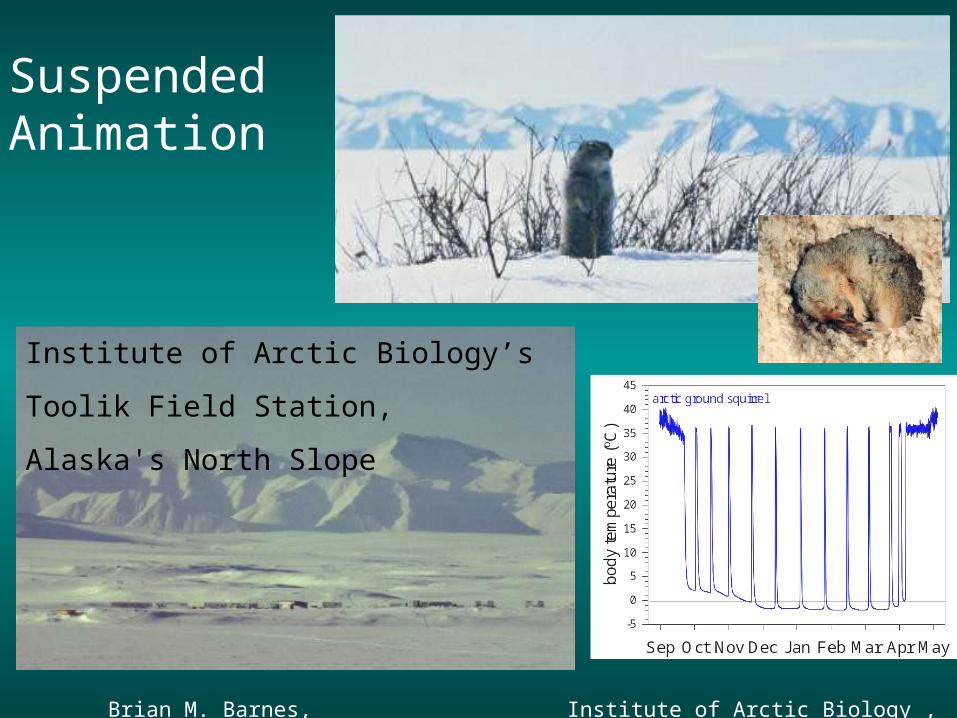
Brian M. Barnes, Institute of Arctic Biology , University of Alaska Fairbanks 11/02
SuspendedAnimation
Institute of Arctic Biology’s
Toolik Field Station,
Alaska's North Slope
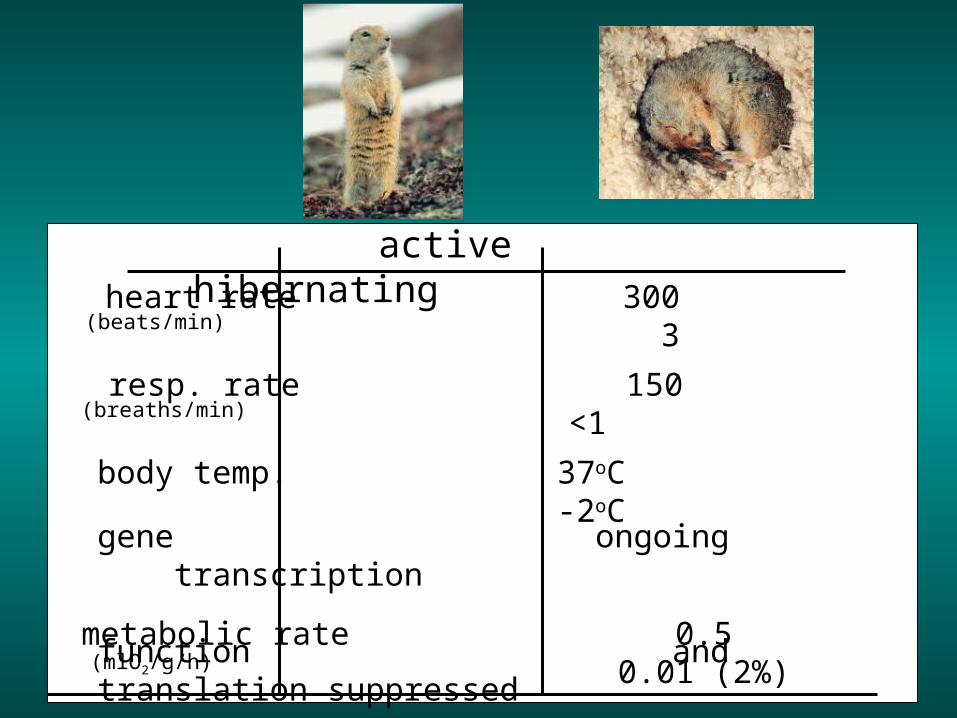
metabolic rate 0.5 0.01 (2%)
active hibernating
body temp. 37oC -2oC
gene ongoing transcription function and translation suppressed
heart rate 300 3
resp. rate 150 <1 (breaths/min)
(beats/min)
(mlO2/g/h)

Confidential

Classic Education and Examination
How is technology changing the educational process?

Laparoscopic Simulator with tactile feedback Courtesy Murielle Launay, Xitact, Lausanne Switzerland
Laparoscopic hysterectomy Courtesy Michael vanLent, ICT, Los Angeles, CA
LapSim simulator tasks - abstract & texture mapped Courtesy Andres Hytland, Sugical Science, Gothenburg, Sweden, 2000
SurgicalSimulators
Simulation and Objective Assessment

“Blue Dragon” passive recording device
Courtesy Blake Hannaford, University of Washington, Seattle
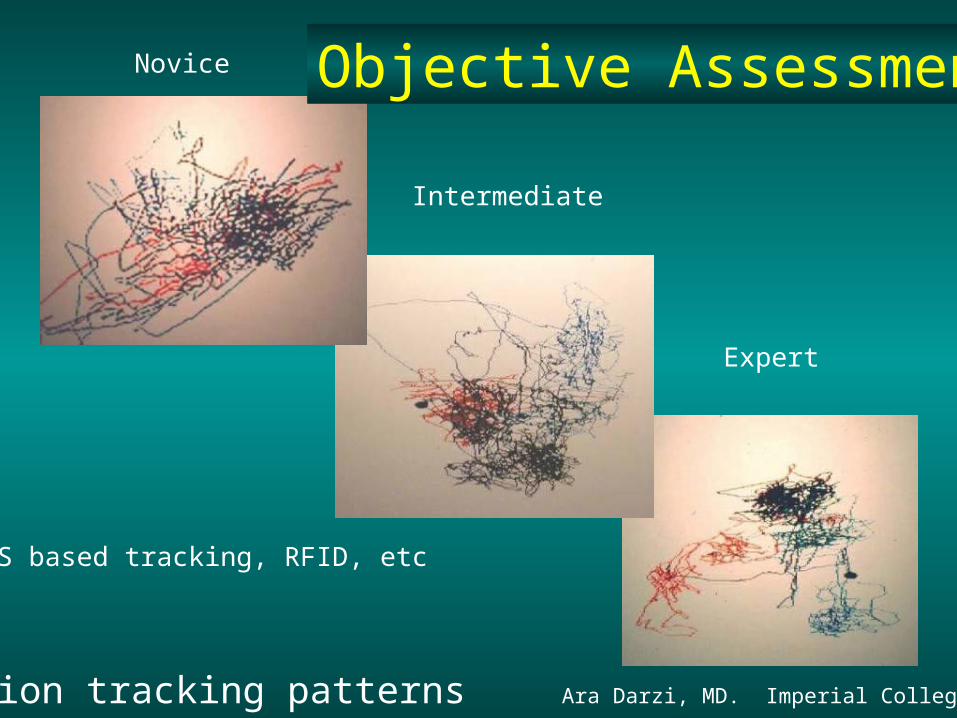
Hand motion tracking patterns Ara Darzi, MD. Imperial College, London, 2000
Novice
Intermediate
Expert
Objective Assessment
MEMS based tracking, RFID, etc

Paradigm Change All Surgical Education & Training
• Adhere to the 6 competencies (ACGME & ABMS)
• Curriculum, not the simulation
• Validation of the curriculum (and simulator)
• Criterion-based (proficiency level) training
for

Speculation on Future
Simulation will become part of surgical procedures (eg surgical rehearsal/assessment)
Training will be continuously assessed (Black box – Ara Darzi)
Training will be embedded in robotic surgery
Team-training of set-up done on mannequins

The next steps
• Intelligent tutors
• Complex procedures
• Digital libraries
• Surgical Rehearsal

• “Information” is critical to surgical integration• Robotics is one of the key technologies• “Instruments” will change dramatically• Open, minimal, non-invasive will find their niche• The OR will take on a whole new meaning• Anesthesia will be revolutionized• Training with simulators and surgical rehearsal• Objective assessment/certification is continuous
• “Information” is critical to surgical integration• Robotics is one of the key technologies• “Instruments” will change dramatically• Open, minimal, non-invasive will find their niche• The OR will take on a whole new meaning• Anesthesia will be revolutionized• Training with simulators and surgical rehearsal• Objective assessment/certification is continuous
SUMMARY
The Future is not what it used to be . . . Yogi Berra
Wake
up !!
Reason there are no penguins at the North Pole