Embed Size (px)
Citation preview

543
RADIOLOGY IN CARDIAC DISEASEBy G. SIMON, M.D., F.F.R.
Department of Radiology, The Brompton Hospital
Radiology has been used on an increasing scalein the diagnosis and prognosis of cardiac diseasefor the past 30 years, and has become an invaluablesupport to the clinician. Big advances in the lastfew years have been the result not only of newtechniques, such as cardiac catheterization andangiocardiography, but of a new and more in-terested attitude to cardiac radiology in general.
It was, for instance, common in the past for acardiologist to base his opinions solely on thesubjective and sometimes misleading evidenceafforded by fluoroscopy; whereas a generalphysician would often confine himself to a singleanterior-view skiagram, which in many cases wouldbe quite inadequate. A modern routine radio-logical examination would not be complete withoutthe use of both methods.
The Routine Cardiac Radiological Investiga-tionFluoroscopy, which is used first, is particularly
valuable in showing the movements of the heartand great vessels. The shape of the heart can bestudied while the patient is rotated during thescreen examination. The contour and position ofthe barium-filled oesophagus should be recordedat the same time. From the results of thefluoroscopy, it will be possible to decide whetherskiagrams in one or other of the oblique views willbe required in addition to the routine anteriorview.The anterior-view skiagram is taken at a tube-
film distance of 6 ft., the patient standing withbreath held in fairly deep inspiration. From thiscan be obtained the measurement of the transversediameter of the heart, which is one of the mostuseful contributions of radiology to the study ofcardiac disease. Taking into consideration a con-stant distortion of some o.8 mm., the routineanterior-view skiagram is as accurate a method forthis purpose as orthodiagraphy and often quickerand more convenient.
The Size and Shape of the HeartOf the various heart measurements available,
that of the transverse diameter (T.D.) is the mostuseful, probably' because 'it is also the mostaccurate. The points on the X-ray image, be-tween which the line of measurement has to be
drawn, are usually more easily defined in the caseof the transverse diameter than in the various otherdiameters.Whatever method is used to acquire the T.D.,
simple or elaborate, the important task of in-terpretation remains. Even assuming the accuracyof the measurement, it is difficult to decide whatthe limits of the normal are, and whether patho-logical enlargement of the heart is present or notin any particular patient under examination for thefirst time. The vastness of the literature on thissubject (over I50 references are given by Roesler,1943) is but a reflection of the difficulties involved.Two methods of assessing the limits of the
normal are now used:-(i) The cardio-thoracicratio; and (2) Tables of averages for people ofgiven height, weight and age.With increasing experience, it has become
apparent that in certain cases the cardio-thoracicratio can exceed 50 per cent. without there beingany pathological enlargement of the heart. Thismay be so in the case of infants, when it may beimpossible to obtain a skiagram during full in-spiration; in obese patients of hypersthenic build,especially when the diaphragm does not descendfar during inspiration, and in some people over6o years of age. If the radiological factors areimperfect, such as a tube-film distance of lessthan 5 to 6 ft., or a posterior view necessitated bythe illness of the patient, the ratio is of courseartificially raised. If these possible sources of errorare taken into consideration, the cardio-thoracicratio is a useful yardstick by which to assess thesignificance of any given transverse diameter ofthe heart.
Tables correlating height, weight and age withthe transverse diameter of the heart, such as thoseof Hodges and Eyster (I926), are possibly a rathermore certain method for detecting pathologicalenlargement; but as these only deal in averages,allowances have to be made for individual patients.
All such methods of assessing the limits of thenormal are, of course, made unnecessary if aprevious skiagram of the patient in a healthier ornormal condition is available for comparison.This is by far the most reliable test, and patho-logical enlargement of the heart can be detected inthis way before the cardio-thoracic ratio exceeds50 per cent., or before there is an appreciable in-
Protected by copyright.
on Septem
ber 5, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.289.543 on 1 Novem
ber 1949. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
crease over the predicted measurement derivedfrom the height-weight-age tables. It is thereforerecommended that an initial skiagram be takenwhen the patient is first seen, be it with rheumaticcarditis, hypertension or any other condition likelyto cause heart enlargement.When an increase of i to 2 cm. is observed in
the later skiagram, the question of the accuracy orconsistency of the normal T.D. measurementnaturally arises. A general test of this factor wasmade by the author recently, using the routineyearly chest skiagrams of a group of nurses andmedical students. These skiagrams were all madeunder identical conditions. The T.D. measure-ments were taken for three consecutive years andvariations in each individual noted.The smallest variation recorded was i mm.,
the largest 2 cm. The average for ioo subjectswas 0.56 cm. The subject with a variation of 2 cm.was obese; in the middle skiagram which showedthe largest measurement, the diaphragm washigher than in the other two pictures, suggestingthat she did not inspire as fully. Being herself aradiographer, she must be considered average asfar as co-operation is concerned. A number ofsubjects were rejected from the test because forone reason or another the heart borders were notsharp on the skiagrams and errors of measurementup to z cm. or more might be expected.Whether this average variation of 0.56 cm. is due
to differences between systole and diastole, rota-tion of the subject, differences in the depth ofrespiration, or true alterations in the heart size, isnot revealed, but it is an indication of what toexpect under average working conditions. Thenumber of X-ray machines available in which thetime of exposure is set in relation to the R wave ofthe electrocardiograph, is so small as to be of nohelp to most cardiologists, so that variations re-sulting from the systole-diastole difference in sizeare unavoidable. What is perhaps surprising is therelative constancy of the T.D. over some years,regardless of the life the subject leads, whetherstrenuous or quiet.The shape of the heart is also a significant factor
in diagnosis. The T.D. may be normal and yetalterations in contour may indicate a serious lesion.It is, however, important not to consider alterationsof the heart shape in isolation, but to correlatethem with the other radiological and clinicalfeatures. It is not safe for instance to use termssuch as ' mitral heart' or ' hypertensive heart,'etc., in connection with the X-ray appearancesseen on a single anterior-view skiagram. To takethe first as an example: An identical prominenceof the left border below the aortic knuckle may beseen in cases of mitral stenosis, patent ductusarteriosus or the so-called ' cor pulmonale' re-
sulting from some long sustained pulmonary con-dition. In mitral stenosis, however, there will beposterior deviation of the oesophagus visible inthe right oblique view, whilst clinical distinctionbetween these three conditions should be easy.An alteration in the position of the heart will
often result in an alteration in its shape and of theT.D. For instance, slight displacement to theleft from scoliosis, a depressed sternum or somepulmonary condition will often cause an undueprominence of the left border just below the aorticknuckle which might be mistaken for a heartlesion. When gross displacement is present,radiology may be of little value in estimating theheart size.
In short, it is essential to use the radiologicalmethod with care and discrimination. It is oftenunsafe to reach hasty conclusions as to whetherthe heart is enlarged or not from the sole evidenceof an anterior-view skiagram, or whether anabnormality of shape seen in this view is indicativeof some particular lesion. In the majority of casesthe full routine radiological examination is essentialand in particular circumstances additional andmore elaborate radiological investigations are also-justified. These include special-posture radio-graphy, tomography, kymography by the multiple-slit method, kymoscopy, cardiac catheterizationand angiocardiography.
Special-posture RadiographySpecial-posture radiography is sometimes valu-
able when mediastinal or pleuro-pericardial ad-hesions are suspected. Three views are used;two anterior views with the X-ray beam parallelto the floor, the patient lying on the table on hisleft side for the first film, on his right for thesecond; and a lateral view with the patient supine.These may show restricted postural movement ofthe heart or puckering out of the cardiac outlineat the point where an adhesion is situated. Suchcases are not common, but the technique is simpleand should be kept in mind.
TomographyIt is often possible to demonstrate valvular
calcifications by tomography (Davies, 1949), butsince these are more certainly identified by thecharacteristic movement of the shadow onfluoroscopy, it is probably not worth the ex-penditure of timae and films.Tomography is, however, valuable in certain
cases where a massive shadow is seen on the routineskiagrams in the region of the heart or greatvessels, and the nature of the shadow is uncertain.Tomograms may show the relation of the abnormalshadow to the trachea and main bronchi, or to thepulmonary vessels. Delineation of the early
November I949544P
rotected by copyright. on S
eptember 5, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.543 on 1 N
ovember 1949. D
ownloaded from

SIMON : Radiology in Cardiac Disease
division of the right and left pulmonary arteriesand final junctions of the pulmonary veins mayalso give useful information in some cardiac con-ditions. For instance, tomography is often betterthan the plain skiagram to show whether the mainvessels are dilated or not in a case of patent ductusarteriosus. Dilatation may be an additional pointin favour of tying the ductus in some cases.
KymographyKymography by the multiple-slit method
(Stumpf kymogram) is 'simple and inexpensive, andthe fact that it is not -more generally used isprobably due to the difficulties of interpreting theresulting skiagrams. The heart movements, beingcomplicated, are never parallel to the kymographgrid intervals throughout the exposure, so thatthe resulting curves are grossly distorted. Never-theless a constant and fairly characteristic pictureis seen in normal.people, so that any alterations tothis picture may give useful information in somepathological conditions (Simon, 1939).By observing the timing and shape of the
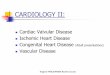
notches, the various parts of the heart can bedifferentiated in a way impossible by-plain radio-graphy. For instance, the aorta and pulmonaryartery show a rapid out-thrust movement and slowrecoil starting just after the inward movement ofthe left ventricle. On the other hand, auricularmovements are later in time and show a morepointed curve. If, therefore, there is a prominenceof the left heart border below the aortic knuckle, itis often possible to see from a kymogram whetherthis represents an enlarged pulmonary artery or aleft auricular appendage. Fig. i, a kymogram ofa case of idiopathic dilatation of the pulmonaryartery, shows that the' prominence on the leftborder moves in phase with the aorta and istherefore an enlarged pulmonary artery.The following perhaps over-simplified tabula-
tion gives an indication of the present position ofX-ray kymography:
It is of no value:For examining babies, young children or
older people who cannot suspend their breathingfor at least three seconds.
It is much inferior to electrocardiography inconfirming the presence and position of areas ofcardiac infarction.It is of some value:
In certain pericardial conditions. When asmall pericardial effusion is present, the absenceof pulsation may be a useful diagnostic feature.When constrictive pericarditis is suspected.
The combination of a small heart and absenceof movement may be a useful confirmatory sign.
Pleuro-pericardial adhesions may be demon-strated.
When a massive shadow has been seen, butdifferentiation between an aneurysm and 'a'mediastinal tumour is difficult on both clinicaland routine radiological examination. Thepresence or absence of pulsation of the shadowitself is not a helpful point, since a vasculartumour may pulsate, while an aneurysm with aclot in it may not; but the presence or absenceof a normally pulsating aortic shadow in-dependent of the main shadow will be ofdecisive importance and may make angiographyunnecessary.
In some congenital cardiac conditions inolder children and young adults.The site of narrowing in co-arctation of the
aorta may be indicated by the absence ofpulsation below it; but it must be admittedthat angiography will give more detailed informa-ation about the size and length of the defect.
In patent ductus arteriosus, abnormalities areseen (Smith et al., 1949) but they are notsufficiently marked or characteristic to be de-cisive in cases where there is clinical doubtabout the diagnosis.The presence of ' hilar dance' can be con-
firmed and recorded, but this is usually obviouson fluoroscopy.On the whole, in spite of various disappoint-
ments, kymography is frequently- worth doingsince it is occasionally helpful, whilst the techniqueis easy and does not upset the patient.
KymoscopyBy kymoscopy the movements of one particular
part of the heart border are studied. A single-slitgrid is used, only some 2 cm. in length. This isorientated under fluoroscopic control so that theslit lies as nearly as possible parallel to the move-ments of the particular part being studied. Theresulting curves are a more accurate representationof the movements of this part than can be obtained'from a multiple-slit kymograph of the whole heart,in which the slits are inevitably out of line withmany of the heart movements.
It would not be practicable to have a movingfilm behind the single-slit grid, but a selenium'cell answers the purpose just as well. The X-raybeam is centred over the heart border, some of ittraverses the lung lateral to the heart, passesthrough the grid slit and enters the selenium cell.As the heart moves to and fro it will allow more orless of the X-ray beam to reach the cell; thus theappropriate current changes are produced, andare in their turn recorded on a moving film. Twosuch cells may be used on different parts of theheart border simultaneously with the electro-cardiograph (or phonograph). The curves result-ing from all three of these examinations can be
November I1949- 454SP
rotected by copyright. on S
eptember 5, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.543 on 1 N
ovember 1949. D
ownloaded from

POSTGkADUATE MEDICAL JOURNAL
recorded on the same film. The X-ray exposureis continued for two to three seconds as in the caseof a kymograph.
Interpretation of the curves resulting fromkymoscopy is not much easier than in the case ofkymography, in spite of the greater accuracy.
Cardiac Catheterization: X-ray SafetyMeasuresThe radiologist's contribution to cardiac
catheterization would appear to be simple enough,but in practice there are one or two factors whichrequire careful consideration by anyone using thismethod. One of these is the protection of thepatient from excessive exposure to X-rays. Atest to measure the output of X-rays should firstbe made under routine working conditions with asubject representing the patient. The X-ray beamshould cover a large area of his back-about iz in.by io in. Assuming the tube filtration is I mm. ofaluminium (or its equivalent), a dose rate on thepatient's back of some 20 r units per minute willbe recorded. This dose rate will allow with safetya total exposure time of seven to ten minutes. Ifthe dose rate is found to be higher than this atthe test, then either the working conditions mustbe alterect, or the time during which actual screen-ing takes place must be reduced.
For young children, the figures must also bereduced. A reduction in milliamperes from 4 to Iiwill often give adequate illumination and at thesame time allow some five minutes screening time.These ' safe' .imes sound-extremely low for a
procedure which may occupy an hour or two, butthe danger is real enough and risks of greaterdosage should not be taken.The following precautions will also increase the
margin of safety: Catheterization should, ifpossible, be arranged well in advance, and atleast a fortnight should elapse between a pre-liminary diagnostic routine fluoroscopy and thisinvestigation. Under no circumstances should asecond catheterization be done within a fortnightof a previous one. At least one member of theteam should be fully dark adapted by the use ofsuitable dark glasses, so that he is able to see assoon as the room is fully darkened. He (pre-ferably the radiologist) should control the size ofthe X-ray beam so that it is no larger thannecessary. The actual time during which thescreening current is on should be recorded and theoperator informed if there is any danger of ex-ceeding the safe time limit.Assuming only one or two such investigations a
week, there is no danger to the physician intro-ducing the catheter; but if more are done, heshould have some protection from scatteredradiation. The standard lead-rubber apron will
usually suffice for this purpose. There is nodanger to the occasional helper or observer.
Should a general anaesthetic be used, the usualprecautions should be taken to preclude an ex-plosion initiated by a static electric spark; thismay occur even with modem shock-proofapparatus.
Technique of Cardiac CatheterizationA suitable vein is selected in the elbow region,
usually the left; the skin over it is anaesthetized,the vein dissected out and a small incision made init through which the catheter is gently introduced.Rough handling at this stage may induce veno-spasm and necessitate abandonment of the in-vestigation. Once the catheter has been intro-duced into the vein and pushed upwards, its pro-gress is carefully controlled under fluoroscopicvision. First the lower neck and retroclavicular areaon the side of introduction are screened to ensurethat the catheter travels towards the superior venacava, and not up into the neck, across to the otherside or down the lateral thoracic vein as some-times happens. If the X-ray beam is cut down to asmall area the screening time spent on this part ofthe procedure can be ignored since the rest of theexposure will be on a different skin area. Carefulinspection of the ppsition and direction of theslightly curved tip will be a guide to the physicianin his manipulations, and will enable him tojudge the appropriate moment at which to intro-duce it further.As a rule the catheter is quite easily recognized
on the screen, but in a large adult it may bedifficult to see it through the spine unless the eyesof the observer are fully dark adapted. Occasion-ally a catheter is not as radio-opaque as it shouldbe but of recent months manufacture has improvedand this is rarely a difficulty. If for any reasonthere should be difficulty in seeing the catheter, askiagram should be taken and rapidly developed.This will nearly always show the catheter, andthereafter the observer, knowing where to look,will be able to pick it up on fluoroscopy.
In many cases the catheter will enter the rightauricle with ease; then, with a little furthermanipulation, the right ventricle, the main pul-monary artery and finally the right or left branch(Fig. 2). An endeavour should be made to reachthis point at an early stage, and then to take thepressure readings and blood samples from thepulmonary artery and heart chambers while thecatheter is being withdrawn under fluoroscopiccontrol.
Sometimes the vigorous movements of the tipof the catheter will indicate its successful entry intothe right ventricle; but if there is any doubt, thiscan be checked by a pressure reading. Once the
546 November I949P
rotected by copyright. on S
eptember 5, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.543 on 1 N
ovember 1949. D
ownloaded from

November I949 SIMON: Radiology in Cardiac Disease 547
.
.......
.........................
......
...... ...... ....
......
Md
FIG. i.-Kymogram in a case of dilatation of the pulmonary artery. The aortic pulsations are seenin frame 3. The pulsations of the prominence (frame 8) are of similar type and phase, proving theprominence to be an enlarged pulmonary artery.
Protected by copyright.
on Septem
ber 5, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.289.543 on 1 Novem
ber 1949. Dow
nloaded from

548 POSTGRADUATE MEDICAL JOURNAL November I949
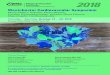
FIG. 2.-Skiagram showing a cardiac catheterwith its tip in the right pulmonary artery ina case of pulmonary stenosis.
FIG. 3.-Skiagram showing the cardiac cathetercoiled up in the greatly enlarged right auricle,in a case of primary pulmonary hypertension.
Protected by copyright.
on Septem
ber 5, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.289.543 on 1 Novem
ber 1949. Dow
nloaded from

November 1949 SIMON: Radiology in Cardiac Disease 549
:.".'. ... ...
...
..?.
..:
...:.: :::::::...:...
... ....
'''. ftj....
...... ........
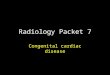
-~~ ..... ::.::::...~~..: FIG. 4.-Skiagram showing a cardiac catheter
with its tip folded up in an aneurysm of theleft pulmonary artery.
A
CI 2B
FIG. 5.-Cassette changer for angio-cardiography. The cassettes arestacked in the lead-covered boxA. i and 3 are in the lead-covered tunnel but at 2 there is aradio-translucent window overwhich the patient lies. Thecassettes are moved across bv theplunger C, D. J is a check stopwhich comes up just before thecassette reaches it. B is thereception box.
After M. McGregor (1949
FIG. 6.-Cassette changer for angio-cardiography. The lead-lined,ray-proof lid on which the patientlies is raised to show the positionof the cassettes marked C. Theone on the left is entering the re-ception box. X is the radio-translucent window under thepatient's thorax. Y is the spacein which the casettes are loaded.One revolution of the handlemoves a iz in. by io in. casetteiz in. and then stops it abruptly,at which point the exposure ismade. The next revolutionpushes it on into the spring-loaded reception box, and at thesame time moves the next cassetteunder the window X.
,By courtesy of A. E. Dean & Co.
Protected by copyright.
on Septem
ber 5, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.289.543 on 1 Novem
ber 1949. Dow
nloaded from

550 POSTGRADUATE MEDICAL JOURNAL November I949
...: :.*#. .# . . .: . : ::?. :..: :::. :::
;....,.', .'......|??N<: ?? .o;' ''°x ': '^ 'f;
..:..! :..:.: .3:::: .' , :.' N:.N ee?>.... .r S t.
tESi?SSX12|lls l ! !, ''
rss.lo.i..iw..!.:> £?5
:1a iii>R{?b8Hfis?c;?U{si,;io?
.50:.W'??S;?wW
'3 ?iwEa |
{= uN=...<:..
''..':S''.' Bu3:.e :'.'"' :#'e
..<oa ;Sw'.'|Bli
X|i?3H':': 'i'X';,'..er'.. S'.:e3'." ^" :'.E-S'88su.e ^ , ': ' ' ?' 4? '' ?' s s ?.S':. .: . : : :.:.a ?.:s?'''; 1 ! ! | | ?., ........ ... :. s . ?.'^,?, XS2 .... ... ...... . , o,.: ....
.. :.s :
.. :. :::* : :. :}::::: .:::. ::: ... .:.:... ....,;..
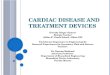
FIG. 7.-Skiagram showing coarctation ofthe aorta. The narrow area is seenopposite the arrow. The tip of theNo. 8 catheter introduced into theradial artery is seen near the top of theaortic arch. 40 cc. pyelosil injected inIS seconds.
catheter is in the right ventricle, it is advisable tokeep an eye on the heart movements for fear ofpossible adverse effects of the catheter on the heartaction.- Any irritability and irregular contractionsof the heart can be easily seen on the screen andare a warning not to keep the catheter in thischamber too long; they do not occur when thecatheter is in the -auricle.
It may be possible in some cases to introducethe tip of the catheter into the coronary sinus(Bing, I949). Its presence there may be inferredradiologically if the tip is seen not to proceed anyfurther. Definite confirmation can usually beobtained only by the appearance of the bloodsample which will be dark.
Skiagrams may be useful to mark the exact siteat which pressure readings were taken or bloodsamples withdrawn. They are often not essentialand, with a view to limiting the amount of X-rayson the patient's skin, may in most cases be limitedto one or two. When the tip of the catheter is inone of the pulmonary arteries or in the superiorvena cava, the position is so obvious on the screenthat a skiagram is unnecessary.When congenital abnormalities are present the
simple routine described above may not be
possible. The catheter may pass out of the rightauricle through an anomalous vein or into the leftauricle through an interatrial septal defect. If thishappens a pressure reading or blood sample maybe taken there and then before reaching thepulmonary artery. Sometimes the catheter curlsup in a greatly enlarged right auricle (Fig. 3). Insuch a case the number of attempts to get it intothe right ventricle must inevitably be limited by theX-ray safety factors already mentioned.
Should venospasm occur it may be impossibleto introduce the catheter any further; it may evenbe difficult to withdraw it. The spasm can bediminished sufficiently to permit withdrawal by theinjection of I.7 cc. of coramine down the catheter.
Indications for Cardiac CatheterizationThe chief clinical indications for cardiac
catheterization are as follows:-(i) Cyanotic heart disease. In the tetralogy of
Fallot it is often necessary to confirm the diagnosis.In a typical case, a high pressure reading will befound in the right ventricle and a low one in thepulmonary artery distal to the point of the stenosis.Incidentally the point at which the pressure in thepulmonary artery falls markedly below that in the
Protected by copyright.
on Septem
ber 5, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.289.543 on 1 Novem
ber 1949. Dow
nloaded from

SIMON : Radiology in Cardiac Disease
right ventricle, will often mark the site of thestenosis. A skiagram showing the position of thetip-of the catheter when this occurs may help thesurgeon in his selection of the type of operation(Brock, i949). On the other hand high pressurein the pulmonary artery (over 50 cm. of water) willbe a contraindication to a Blalock type ofanastomosis.
(2) In some cases of interatrial septal defect, toconfirm the diagnosis and differentiate it from anEisenmenger complex. In a typical interatrialseptal defect with a left to right shunt, the oxygencontent in the right auricle will be appreciablyhigher than in the superior vena cava.
(3) In a doubtful case of patent ductus arteriosuscatheterization may help if a left to right shunt canbe demonstrated in the pulmonary artery. If,however, there is much regurgitation of bloodfrom the pulmonary artery into the right ventriclethe findings will simulate a high ventricular septaldefect and thus be misleading.
(4) If there is doubt whether a shadow seen onradiological investigation is a neoplasm or ananeurysm of the pulmonary artery (Fig. 4).
AngiocardiographyThe two essentials for successful angio-
cardiography are an adequate concentration of thecontrast medium in the heart and great vessels,and the correct timing of the skiagrams. Theformer depends gn the rapidity of the intravenousinjection, which should be given through a wide-bore needle at the rate of 40 cc. in two seconds. Inorder to observe the bolus of contrast medium onits way through the various chambets of the heartand into the main vessels, it is necessary to take aseries of six to eight skiagrams at very short andprecise intervals. To achieve this some device isneeded to speed up the process of film changing sothat a rate of at least one exposure per second isattained. Three different ways of doing this areat present in use:
(i) Cine camera photography of the screenimage. Speeds up to one frame per second havebeen reached by this method and no doubt fasterspeeds will be developed in the future, possibly bythe use of an electron acceleration screen to in-crease the brightness of the screen image. Suchincreases in speed may yet make this the methodof choice but, at present, losses of detail andcontrast, due to the fact that the photographs areindirect, make it inferior to other methodsavailable.
(2) A device to ensure rapid changing of ordinaryX-ray films and cassettes. There are four types ofdevice available giving speeds easily up to oneexposure per second for six or eight seconds. Inthe first type, the cassettes are stacked in an X-ray
protected box to one side of the patient and arepushed one by one through a tunnel underneathhim (Fig. 5). Each cassette stops abruptly whenit is beneath the patient, remains stationary duringthe exposure and is then pushed on into an X-rayprotected reception box by the next incomingcassette. The reception box end of this deviceshould be on the side of the patient chosen forinjection since it is flush with the table top andwill therefore no. be in the way of the outstretchedarm. This is a simple device and if the cassettesare light in weight there is little risk of theirjamming.The three other devices are variations of this
one. In the first, the lead-backed cassettes arestacked directly beneath the patient and are pushedup against the table top one by one for each ex-posure. Once exposed, they move off towards thehead or foot of the table and fall into the receptionbox. In the second variant the cassettes aremounted on a large wheel which is rotated be-neathi the patient, the exposure being made as eachcassette comes into position beneath the patient.Stopping and restarting the wheel at the correctmoment presents some difficulty, which in turnlimits the speed to one exposure per second. It is,however, a suitable device for use with a sittingpatient. In the third variant the cassettes aremoved in line along a flexible band, passing in atunnel under the patient (Fig. 6). Here, again, thedifficulty is to start, move and stop the cassettessufficiently quickly.
(3) Roll film radiography. A somewhat higherspeed of working is made possible by the use of aI2 in. wide roll film. The intensifying screenshave to be separated after each exposure to allowthe roll of film to move, and then pressed againstthe film again when it is stationary for the nextexposure. Elaborate mechanical coupling isneeded for this, as for the other methods described,and there is no indication yet which will be thesimplest and most effective routine method for thefuture.Having solved the problem of correct timing by
one of the foregoing methods, the rest of thetechnique of angiocardiography is fairly straight-forward. The view (posterior, lateral or oblique)must be chosen according to which lesion issuspected clinically. For Fallot's tetralogy, aposterior view is most useful; for coarctation of theaorta, an oblique view is best. If the first series ofskiagrams is not satisfactory, it is safe to give asecond injection 20 minutes later and take asecond series in another view. It is possible, byusing two X-ray tubes and generators, and twocassette changers, to take two series simul-taneously, one in a posterior and the other in alateral view; but the apparatus for this is com-
November i 949 551P
rotected by copyright. on S
eptember 5, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.543 on 1 N
ovember 1949. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
plicated and on occasion an oblique view may bepreferable to the lateral one, so that the simplermethod is more satisfactory as a routine.The examination is usually done with the patient
lying down, since an anaesthetic is often required,but an adult may sometimes sit up for it if theapparatus is adaptable to that position. Thecassettes are numbered with lead figures, so thatthe films can be re-assembled in the order in whichthey were exposed.The tube-film distance is reduced to 3 to 4 ft.
to ensure rapidity of exposure. A well-exposedfilm is necessary to show up the contrast mediumclearly; for a child of 2, for instance, an exposureof 200 milliamperes, .05 second and 65 K.V.P.would be necessary for the posterior view; in anadult, .I second and 75 K.V.P.The first film is taken towards the end of the
injection in most cases, but if the abnormality isthought to be in the aortic region, the first film canbe taken one to two seconds later.
Th-e total dosage of X-rays received by thepatient's skin during the eight exposures is soslight that it can be ignored, even if the examina-tion follows directly, after cardiac catheterization.It would correspond to less than 20 secondsscreening and is in any case not directly on thesame skin area.The X-ray beam should be coned down so that
the personnel are safe from everything butscattered radiation. If anyone is giving severalinjections during a week, a light lead-rubberscreen can be placed to protect the hands and theroutine lead-rubber apron can be worn to protectthe body. By now most cassette changing de-vices are mechanical, so that other personnel neednot be in the danger zone. The anaesthetist willbe protected by the lead top of the reception boxin some methods, but he can wear a lead-rubberapron if necessary.
Intra-arterial Angiography of the AortaIn the case of patients suffering from coarctation
of the aorta, it is often difficult to get sufficientcontrast medium into the required area by intra-venous angiocardiography, and more definite in-formation may be given by retrograde arterio-graphy. A catheter is introduced into the radialartery and passed onwards into the aorta. Thecontrast medium is then injected and the serialradiographs taken. Since it is only possible tointroduce a small-sized catheter, a much slowerrate of injection is inevitable, but nevertheless asatisfactory picture is usually obtainable (Fig. 7).
The Lung Changes in Cardiac ConditionsIn one's enthusiasm for these elaborate X-ray
investigations of the heart, simple inspection of the
lung fields, particularly on the skiagram, should notbe neglected. If this is done in an orderly manner(as when inspecting a skiagram for a lung lesion),features may often be discovered which are ofhelp in the diagnosis or prognosis of cardiac lesions.
First, the position of the diaphragm should benoted. A high position may cause the heart tolie more horizontally than usual and thus to appearlarger than it, in fact, is. Excess of air below theleft dome, or air translucencies in an unusualposition should be noted. Deviation of the tracheawill suggest the possibility of slight heart dis-placement, which must be taken into considera-tion when assessing the significance of its size andshape.
Particular attention should then be paid to thepulmonary vascular pattern. It may be diminishedin certain types of congenital cyanotic heartdisease, or increased in other types or in any con-dition resulting in stasis of the pulmonary circula-tion. It is only fair to say that there are widevariations in the normal appearance of the pul-monary vessels, and early c-hanges may thereforenot be detected unless a previous skiagram isavailable for comparison taken before the onset ofcardiac failure, etc.
Apart from changes in the density and size ofthe main vascular arborizations, two other general-ized pulmonary abnormalities are sometimes seenin cardiac diseases. Firstly, there may be analteration in the peripheral pulnronary pattern, sothat arborizing vascular (or lymphatic) channelsbecome visible in the lower axillary regions where,normally, there are no distinctive markings. Thisis sometimes seen, for instance, in chronic mitralstenosis. Secondly, fine discrete mottled shadows0.5 to i mm. in size, caused by haemosiderosis,may occasionally be seen in well-compensated andlong-standing mitral stenosis, when the cardiacfindings may be relatively inconspicuous. Theseshadows must not be confused with those ofmiliary tuberculosis.The shadow of a pleural effusion may be visible
on the skiagram before there are physical signs toindicate its presence, and this will be a factor to beconsidered when planning treatment. At theonset of pulmonary oedema, physical signs usuallyprecede radiological evidence of the condition, butsometimes a large area of clouding is seen in thelower half of the lungs when there is as yet noclinical evidence of oedema. Should the cardiaccondition improve, these shadows will disappearrapidly. When uraemia supervenes in hyper-tension, large areas of opacity are sometimes seenspreading out from the hilum and are of graveprognostic significance.
Infarction during the course of a chronic cardiaccondition may occur and be obvious clinically, and
November I1949552P
rotected by copyright. on S
eptember 5, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.543 on 1 N
ovember 1949. D
ownloaded from

November I949 GARDNER: Angiocardiography 553
yet there may be no radiological evidence of thesite and size of the affected area. Even if a shadowis seen, it is usually ill-defined, and in the singleposterior view, which is usually all that is available,there is no evidence of a pyramidal shape. If it isas small as i cm. it may be more or less circular,but when larger its ill-defined margins are oftenpartly masked by a superadded pleural effusion.When studying a skiagram of the lungs in a
patient with cardiac disease, it must not be for-gotten that other pathological conditions may co-
exist. For instance, a bronchial neoplasm mayarise in a patient with long-standing, but well.compensated, mitral stenosis; while ordinaryinflanmmatory conditions may occur in the lungsindependently of the cardiac lesion. A coalminer with pneumonokoniosis may develop mitralstenosis, in which case it may be difficult todifferentiate the shadows of the pneumonokoniosisfrom those of a possible haemosiderosis. It istherefore essential to consider the X-ray appear-ances from a broad angle of general medicine.
BIBLIOGRAPHYBING, R. J. (I949), Amer. Heart. J., 38, I.BROCK, R. C. (I949), Brit. Med. 7., 2, 399.DAVIES, C. E., and STEINER, R. E. (I949), Brit. Heart J., Ix,
126.HODGES, P. C., and EYSTER, J. A. E. (1926), Arch. Int. Med.,
706.HODGES, P. C., EYSTER, J. A. E., and BOURNE, G. (I949),'An Introduction to Cardiology,' London.McGREGOR, M. (I949), Brit. .7. Radiol., 22, 459.ROESLER, H. (I943), ' Clinical Roentgenology of the Cardio-
Vascular System.' Illinois.SIMON, G. (I939), Proc. Roy. Soc. Med., 23, 1157.SMITH, K. SHIRLEY, and WOOD, F. G. (I949), Brit. Heart
Y., 1I, 257.
ANGIOCARDIOGRAPHYBy FRANCES GARDNER, M.D., M.R.C.P.
From the Cardiac Department of the Royal Free Hospital
Angiocardiography is now an establisheddiagnostic procedure in the fields of thoracic andcardiac surgery. By intravenous injection of anopaque substance combined with rapid serialradiography it is possible to study the heartchambers and great vessels during life. Themethod was conceived more than 20 years ago,though its application in clinical medicine isrecent. Improvements in radiological techniquehave encouraged wider use of the procedure butthe interest in the diagnosis of congenital heartdisease and the advances in its treatment, aremainly responsible for modern development ofthis method of investigation.
HistoryIn 1929 Forssman first injected an opaque
substance into the living human heart. Like laterworkers in this field, notably Ameuille (1936),Forssman used sodium iodide for the intravenousinjection. In the quantity and concentrationemployed this substance gave good angiograms ofthe pulmonary arteriat tree, but it was not suf-ficiently opaque to outline the heart chambers orthe aorta. For this reason little progress was madein this method of investigation until Castellanos
(I938) and his co-workers in Cuba introduced theorganic iodides as the contrast medium. With35 per cent. neoiopax these workers were able toshow the right heart chambers and the aorta andits larger branches in children with cyanotic con-genital heart disease. But, because of dilution inthe pulmonary circulation, satisfactory angio-cardiograms ofthe left heart in acyanotic conditionscould not be obtained.
In 1938 Robb and Steinberg prepared and useda 70 per cent. aqueous solution of the diethanol-amine salt of 3, 5-diiodo-4-pyridone-N-acetic acidfor the intravenous injection. With this substancethey were able to outline, first, the right heartchambers and pulmonary arteries and later theleft heart and aorta. The introduction of multiplecassette-changing devices has enhanced the valueof angiocardiography, but in other respects theprocedure described by Robb and Steinberg ismore satisfactory than any other and is in generaluse today.
Contrast MediaDiodone or diodrast, the material originally
prepared by Robb and Steinberg, is still the mostwidely employed contrast medium in angio-
Protected by copyright.
on Septem
ber 5, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.289.543 on 1 Novem
ber 1949. Dow
nloaded from







![[PGI] Radiology Airways Disease](https://img.pdfslide.net/doc/110x75/577c84731a28abe054b9009f/pgi-radiology-airways-disease.jpg)