Embed Size (px)
Citation preview

1X
A Robust Response2
56% ORRc (97.5% CI: 45-67; n=110)
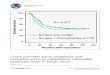
Unprecedented Survival2
16.7-month median PFS#,d (95% CI: 11.6-21.4; n=110)
34.1-month median OS#,c (95% CI: 27.7-NR; n=110)
Durable CNS Efficacy3
18.4-month median intracranial PFS d,e (95% CI: 12.6-NR; n=73)
16.6-month median intracranial DOR d,f
(95% CI: 3.7-16.6; n=12)
67% intracranial ORR d,f
(95% CI: 41-87; n=18)
RAISING EXPECTATION IN ALK+ NSCLC
TREATMENTFor patients with ALK+ metastatic NSCLC
who have progressed on or are intolerant to crizotinib
23/F & 24/F, East Exchange Tower, 38 Leighton Road, Causeway Bay, Hong Kong Tel: 2133 9800 Fax: 2856 2728
Takeda Pharmaceuticals (HK) Ltd
INDICATION4
ALUNBRIG is indicated for the treatment of patients with ALK+ metastatic NSCLC who have progressed on or are intolerant to crizotinib. This indication is approved based on tumor response rate and duration of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial.
ALK+=anaplastic lymphoma kinase positive; CNS=central nervous system; CI=confidence interval; DOR=duration of response; IRC=independent review committee; NR=not reached; NSCLC= non-small cell lung cancer; ORR=objective response rate; OS=overall survival; PFS=progress free survivea=for 90 mg once daily regimen; b=for 180 mg once daily regimen with a 7-day lead in at 90 mg once daily; c=investigator assessed; d=IRC assessed; e=in patients with any brain metastases at baseline; f=among patients with measurable brain metastases (≥10mm in longest diameter) at baseline; #=Kaplan-Meier estimate
For further information, please consult full prescribing informationReference: 1.Kim DW et al., J Clin Oncol. 2017;35:2490-8 2.Huber RM et al., J Clin Oncol. DOI :10.1200/JCO.2018.36.15_suppl.9061 3.Ahn M et al., WCLC ALTA slides. Oral presentation IASLC WCLC 2017 (Abstract 8027) 4.Alunbrig HK prescribing information (PLFT0156A1)
Abbreviated product information: Alunbrig (brigatinib) tablets I: Patients w/ anaplastic lymphoma kinase (ALK)-positive metastatic non-small cell lung cancer (NSCLC) who have progressed on or are intolerant to crizotinib. D: Initially 90 mg once daily for the 1st 7 days, increased to 180 mg once daily if initial dose is tolerated. SP: Risk of interstitial lung disease (ILD)/pneumonitis, hypertension (HTN), bradycardia, visual disturbances (eg, blurred vision, diplopia, & reduced visual acuity), creatine phosphokinase (CPK) & pancreatic enzyme elevation, hyperglycemia. Withhold treatment in patients w/ Grade 3 or 4 CPK elevation; Grade 3 or 4 pancreatic enzyme elevation; inadequate hyperglycemic control. Permanently discontinue in case of Grade 3 or 4 ILD/pneumonitis or recurrence of Grade 1 or 2 ILD/pneumonitis; Grade 4 HTN or recurrence of Grade 3 HTN; life-threatening bradycardia; Grade 4 visual disturbances. Use w/ caution in combination w/ antihypertensive agents causing bradycardia. Females of reproductive potential should use effective non-hormonal contraception during treatment & for at least 4 mth follow-ing the final dose. Males w/ female partners of reproductive potential should use effective contraception during treatment & for at least 3 mth after last dose. AR: Pneumonia, ILD/pneumonitis, increased CPK, nausea, diarrhea, vomiting, constipation, abdominal pain, fatigue, pyrexia, cough, dyspnea, hypoxia, headache, peripheral neuropathy, rash, hypertension, muscle spasms, back pain, myalgia, arthralgia, pain in extremity, decreased appetite, visual disturbance, insomnia, increased aspartate aminotransferase, hyperglycemia, increased CPK, increased lipase, increased alanine aminotransferase, increased amylase, increased alkaline phosphatase, decreased phosphorus, prolonged activated partial thromboplastin time, anemia, lymphopenia. INT: Increased plasma conc & adverse reactions w/ strong CYP3A inhibitors [eg, certain antivirals (boceprevir, cobicistat, indinavir, lopinavir, nelfinavir, ritonavir, saquinavir), macrolide antibiotics (clarithromycin), antifungals (itraconazole, ketoconazole, posaconazole, voriconazole), conivaptan]; grapefruit or grapefruit juice. Decreased plasma conc & efficacy w/ strong CYP3A inducers (eg, rifampin, carbamazepine, phenytoin, St. John’s Wort). Decreased conc & loss of efficacy of CYP3A substrates (eg, hormonal contraceptives).
Convenient dosing: One tablet once daily taken with or without food4
HK/
BRI/2
0190
5-00
013
At the recommended doseb, ALUNBRIG® delivered...

STRATIFIED BY:Brain metastases at baseline (absent or present)
Best responses to prior crizotinib
n=110ALUNBRIG 180 mg once daily(180 mg once daily with a 7-day lead-in at 90 mg once daily)
n=112ALUNBRIG 90 mg once-daily regimen
ALUNBRIG® ALTA STUDY1
The safety and efficacy of ALUNBRIG® were evaluated in an open-label, randomized, multicenter, international phase II study in patients with
crizotinib-refractory advanced ALK+ NSCLC
a=for 90 mg once daily regimen; b=for 180 mg once daily regimen with a 7-day lead in at 90 mg once daily; †=patient in the arm (90mg once-daily regimen) were permitted to escalate to 180mg QD
after RECIST progression; ††=as assessed by investigator; IRC=Independent Review Committee
RA
ND
OM
ISE
D 1
:1 222
ADULT PATIENTS
LOCALLY ADVANCED OR METASTATIC ALK+ NSCLCPROGRESSED ON CRIZOTINIB
Disease progression requiring an alternative systemic therapy†
Intolerable toxicity
Consent withdrawal
Primary endpoint Confirmed ORR per RECIST v1.1 (per investigator)
Key secondary endpointsConfirmed ORR (per central IRC), CNS response (IRC assessed intracranial ORR & PFS in patients with active brain metastases), DOR, PFS, OS, safety and tolerability
Baseline Characteristics in ALTA (N=222)
90 mg Once Daily 180 mg Once Daily Total n=112 (with lead-inb) N=222 n=110
Median age, years (range) 50.5 (18-82) 56.5 (20-81) 54 (18-82)
Gender, % Female 55 58 57
Race, % White, Asian, Other 64, 35, 1 69, 27, 4 67, 31, 2
ECOG performance status, % 0, 1, 2 30, 63, 6 41, 51, 8 36, 57, 7
Smoking history, % Yes, No, Unknown 36, 63, 1 43, 57, 0 39, 60, <1
Brain matastases at baseline††, % Present 71 67 69
Prior chemotherapy, % Yes 74 74 74
Histology, % Adenocarcinoma 96 98 97









![SELECTED ABSTRACTS - American Neurotology Society · private insurance (OR: 2.4 [95% CI: 1.10-5.04]) and Medicare (OR: 7.6 [95% CI: 1.9-30.3]) was associated with higher levels of](https://img.pdfslide.net/doc/110x75/5fb6d2d27d512c27083590da/selected-abstracts-american-neurotology-society-private-insurance-or-24-95.jpg)

![Research Paper Adjuvant Chemotherapy Improves Survival in ...median OS and DFS were 30.7 months (95% confidence interval [CI]: 27.5– 33.9) and 26.4 months (95% CI: 21.2–31.6),](https://img.pdfslide.net/doc/110x75/60806bce239a02239475df4d/research-paper-adjuvant-chemotherapy-improves-survival-in-median-os-and-dfs.jpg)




![Incidence and progression of diabetic retinopathy in ... · diabetic retinopathy compared with the control arm: 0.82 [95% CI 0.65–1.02] and 0.76 [95% CI 0.45-1.22], respectively)](https://img.pdfslide.net/doc/110x75/5f8dfc9fb00857357003c053/incidence-and-progression-of-diabetic-retinopathy-in-diabetic-retinopathy-compared.jpg)

![PREVALÊNCIA DE MORMO E ANEMIA INFECCIOSA EQUINA EM ...€¦ · interval (CI) 95% = [1.01% - 4.2%] for owners testing positive and 1.81% confidence interval (CI) 95% = [0.55% - 3.07%]](https://img.pdfslide.net/doc/110x75/5f6b6d9603f9d777492a7177/prevalncia-de-mormo-e-anemia-infecciosa-equina-em-interval-ci-95-101.jpg)




![ASPEN-01: A Phase 1 Study of ALX148, a CD47 Blocker, in ......(EVAL) ORR (%) [95% CI] DOR (m) [95% CI] PFS (m) [95% CI] PFS Rate at 6 m OS (m) [95% CI] OS Rate at 12 m Follow Up (m)](https://img.pdfslide.net/doc/110x75/6144ab7ab5d1170afb440666/aspen-01-a-phase-1-study-of-alx148-a-cd47-blocker-in-eval-orr-95.jpg)