Embed Size (px)
Citation preview

Randomized control trials in ALS: lessons learned
Hiroshi Mitsumoto, Paul Gordon, Petra Kaufmann, Clifton Gooch, Serge Przedborski and Lewis P RowlandThe Eleanor and Lou Gehrig MDA/ALS Research Center, Columbia University Medical Center
Introduction
As we stated in the Preface, a major impetus for organizing
the ALS Clinical Trial Meeting held in Tarrytown, New York,
was the overall great frustration we have had in treating ALS;
that is, since 1996 when riluzole received FDA approval, we
have not identified any new medications for ALS. Although
we have been prescribing riluzole, its efficacy is modest at
best. We desperately need more effective drugs. Although a
cure may come only after the cause of ALS is elucidated, we
do not have the luxury of waiting when we are confronted by
the progressive paralysis of our patients. Vigorous basic
research in ALS has offered new hypotheses and opportunities
to test novel drugs. In the past two decades, we have had
more than 25 randomized clinical trials (RCTs) in ALS
(Table 1). Although we surely have made great progress in
these trials, the collective experience is still less than that in
many other diseases. An important lesson is always to learn
from others and from the past. We have therefore decided to
provide here not a review but rather an overview of the
collective experience in past ALS RCTs, which hopefully will
serve as a useful Introduction to this supplement. The issues
that we raise are examined in detail by the other contributors
to the supplement.
Bench to clinic
Drug effects in animal models have not been reliablepredictors of human effects
A critical limitation of RCTs is that our experience in ALS
trials is not large enough. Because only riluzole has given
positive RCT results, we cannot determine what type of results
in preclinical studies in animal models will predict the results
in human trials. At present, positive results in animals are
rather misleading at best, and it is uncertain how much we
actually have relied on the preclinical results. For example,
the decision to test riluzole in humans was not based on
studies in any animal models, only on its known anti-
glutamate effects in in vitro studies. Riluzole was tested in
SOD transgenic mice (termed SOD1 mice in this article) only
after riluzole had already been approved (and also because
transgenic mice carrying the human familial ALS mutation
became generally available after the approval of riluzole). The
effect size was small in both the mice and humans.18,28
The SOD1 mouse is now considered to be the best animal
model for preclinical testing in ALS. Earlier, neurotrophic
factors were tested in other mouse models, such as the
wobbler, pmn, and mnd mice, with some positive results that
led to human trials of neurotrophic factors, including ciliary
neurotrophic factors (CNTF), brain-derived neurotrophic
factors (BDNF), and insulin-like growth factor-I (IGF-I).29
When a number of neurotrophic factors were tested in SOD1
mice, negative findings were not published and trials were
performed in spite of such findings. When most neurotrophic
factors available for testing showed no clinical benefit in
patients, trialists in retrospect felt that preclinical results in
these less acceptable animal models had led to the negative
results in human studies, and subsequently to the loss of
interest in neurotrophic factor therapy.29 Some major RCTs
have been done without any preliminary studies in animal
models, or were performed despite the fact that studies in
animal models were negative, as seen in the examples of
riluzole and xaliproden. Thus, it seems fair to state that
animal studies have not been a critical factor in the decision-
making for RCTs.
Another issue is the timing of drug treatment in SOD1
mice. Presymptomatic treatment may not be ideal because it
can be done only in those at risk for familial ALS, not in
those with sporadic ALS. Because survival in SOD1 mice is
usually less than 2 weeks after the onset of clinically
detectable disease, particularly in the most commonly used
mice (G93A SOD), almost all drug treatments have been
initiated long before symptoms appear. At least two studies,
which showed dramatic responses to therapeutic agents,
commenced treatment after disease onset in SOD1 mice.
Those studies include IGF-I gene transfer using adeno-
associated virus36 and a preliminary report with Mn-
porphyrin treatment (J. Crow et al; reported at the 14th
International ALS/MND Symposium, Milan 2003). Other
complicating issues in SOD1 mice include the question of
whether mutant SOD1 transgenic mouse results (which
correspond to familial ALS) can be generalized in the
majority of patients with sporadic ALS , the variations in
progression and life span depending on the particular
transgenic mouse model used, and the time and costs
involved in careful animal testing.
High hopes for clinical trials
Demanding too much effect size? Modest orunequivocal benefit?
In the past, some trialists thought that not many patients
were needed to test drug efficacy in ALS. If a drug showed
unequivocal benefit (something like wheelchair-bound
patients starting walking again), we would know this
immediately. In reality, it is possible that some effective
drugs will have only a modest benefit that can be
DOI: 10.1080/17434470410019942
ALS and other motor neuron disorders 2004 5(Suppl 1), 8–13# 2004 ALS and other motor neuron disorders. All rights reserved. ISSN 1466-0822 8
Introduction
Am
yotr
oph
Lat
eral
Scl
er D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
Dav
is o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.
demonstrated only through statistical analysis of a large RCT.
Also, if research funds are limited, one tends to look for a
large effect size (large difference in the primary outcome
between placebo and drug) when testing a new medication.
Many RCTs in ALS have aimed for at least a 30% difference
from placebo. Such a large effect helps to reduce study costs,
partly by decreasing the number of patients required.
Furthermore, this approach effectively eliminates drugs that
have no major impact on the disease; on the other hand, it
would miss drugs that have modest benefits – less than 30%.
With the growing belief that the benefits of any new
treatment might be modest, we may have to lower the
effect size in future trials. As oncologists have done in RCTs,
we need to change our bias for large effects, and instead look
for effects of perhaps only 10% to 20%. A smaller effect size
requires a larger number of enrolled patients; however, there
is a recent trend towards enrolling more patients in ALS RCTs,
so this may not be a problem.
While a large effect size was an unrealistic approach to
identifying drugs with modest benefits, it may be useful when
the trial objective is different. A Phase II trial with a large
effect size would allow rapid screening of potential drugs
using a relatively small number of patients. Drugs found to
have large effects would then have top priority for testing in
subsequent Phase III trials. Alternatively, trialists could change
their statistical approach, setting the null hypothesis to be that
the new drug is effective, which would control for the Type I
error of eliminating a potentially beneficial medication. This will
allow us to decrease the sample size while setting the desired
effect size at a reasonable level. In essence, effect size must be
determined based on the goal of the trial.
Small clinical trials
There have been a number of small negative trials, which are
reviewed elsewhere.31,32 For this overview, we have defined
small negative studies as those with negative results that were
potentially underpowered. Those small studies guided us in the
direction ALS trials took because of their negative results, but in
retrospect many of these trials may have had potential problems
with sample size. By the same token, some RCTs listed in Table 1
may also have had the same problem. The relatively small
sample sizes in these studies may have left them underpowered
to test for efficacy, suggesting potential Type II errors rather than
truly negative results for the tested medications.
Searching for reliable primaryendpoints
Survival is the gold standard, but defining death iscomplex
FDA approval of riluzole influenced subsequent ALS RCTs.
The riluzole trial used survival as the primary endpoint; and
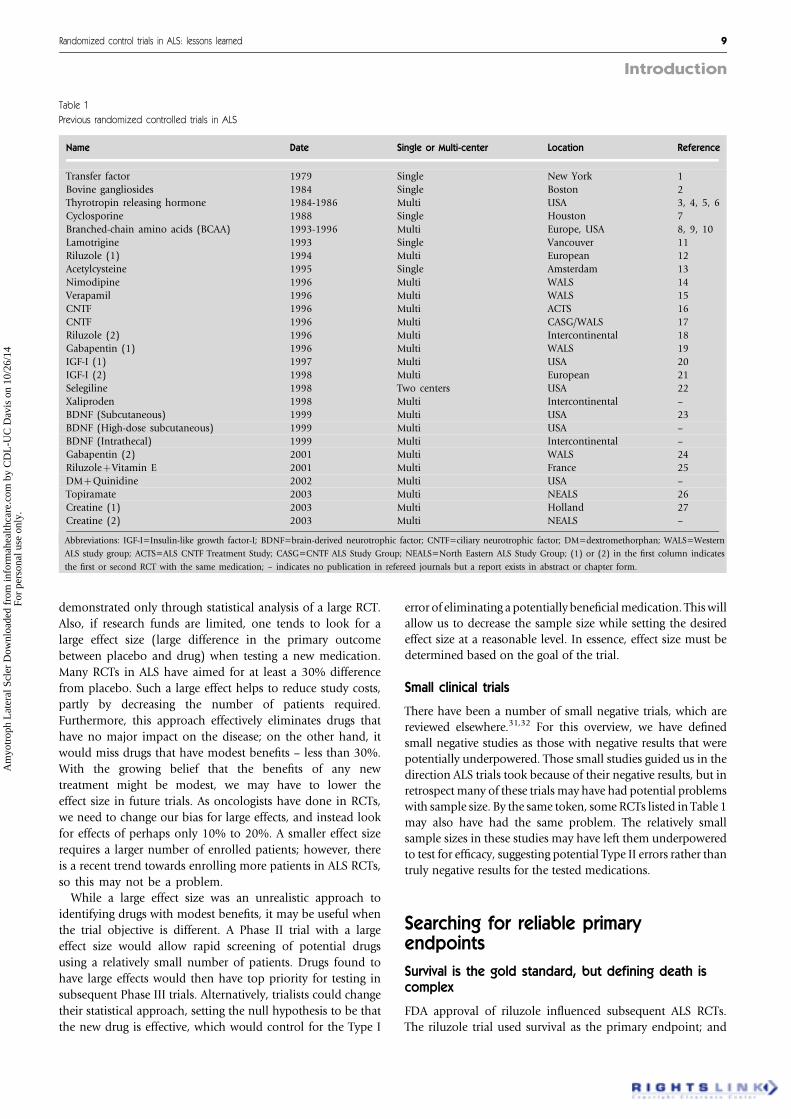
Table 1
Previous randomized controlled trials in ALS
Name Date Single or Multi-center Location Reference
Transfer factor 1979 Single New York 1
Bovine gangliosides 1984 Single Boston 2Thyrotropin releasing hormone 1984-1986 Multi USA 3, 4, 5, 6
Cyclosporine 1988 Single Houston 7
Branched-chain amino acids (BCAA) 1993-1996 Multi Europe, USA 8, 9, 10
Lamotrigine 1993 Single Vancouver 11Riluzole (1) 1994 Multi European 12
Acetylcysteine 1995 Single Amsterdam 13
Nimodipine 1996 Multi WALS 14
Verapamil 1996 Multi WALS 15CNTF 1996 Multi ACTS 16
CNTF 1996 Multi CASG/WALS 17
Riluzole (2) 1996 Multi Intercontinental 18Gabapentin (1) 1996 Multi WALS 19
IGF-I (1) 1997 Multi USA 20
IGF-I (2) 1998 Multi European 21
Selegiline 1998 Two centers USA 22Xaliproden 1998 Multi Intercontinental –
BDNF (Subcutaneous) 1999 Multi USA 23
BDNF (High-dose subcutaneous) 1999 Multi USA –
BDNF (Intrathecal) 1999 Multi Intercontinental –Gabapentin (2) 2001 Multi WALS 24
RiluzolezVitamin E 2001 Multi France 25
DMzQuinidine 2002 Multi USA –Topiramate 2003 Multi NEALS 26
Creatine (1) 2003 Multi Holland 27
Creatine (2) 2003 Multi NEALS –
Abbreviations: IGF-I=Insulin-like growth factor-I; BDNF=brain-derived neurotrophic factor; CNTF=ciliary neurotrophic factor; DM=dextromethorphan; WALS=Western
ALS study group; ACTS=ALS CNTF Treatment Study; CASG=CNTF ALS Study Group; NEALS=North Eastern ALS Study Group; (1) or (2) in the first column indicates
the first or second RCT with the same medication; – indicates no publication in refereed journals but a report exists in abstract or chapter form.
Randomized control trials in ALS: lessons learned 9
Introduction
Am
yotr
oph
Lat
eral
Scl
er D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
Dav
is o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.
survival was defined as time to death or tracheostomy.
Because riluzole trials were positive and riluzole was
approved, survival became the primary endpoint in trials
that followed. However, trials of BDNF and xaliproden gave
negative results, and the difficulties engendered by using
survival as the primary endpoint began to become apparent.
The main issue in using survival as the primary endpoint
concerns how death is defined for the purpose of RCTs in
ALS. How to define survival has become more difficult
because defining death has become less clear with the advent
of life-extending measures such as non-invasive positive-
pressure ventilation (NIPPV). For example, should any use of
NIPPV be considered equivalent to death in an ALS trial or
should more extended use, perhaps 24 h a day for 7 days, be
considered the defining marker? Clearly, defining death is
crucial if survival is to be used as the primary endpoint in
RCTs. The same problem applies to other life-extending
measures. For example, the majority of tracheostomized
patients require a permanent ventilator at the time of
tracheostomy. However, occasionally patients undergo tra-
cheostomy without ventilator support for management of
excessive secretions, and on rare occasions, proactive
tracheostomy is performed. How is death defined in these
situations? Making the matter more complicated, a few
reports have suggested that percutaneous endoscopic gastro-
stomy (PEG) prolongs survival in patients with ALS. Finally,
although riluzole marginally increases survival, retrospective
studies suggest that the survival effects may extend life by
about two months more than originally indicated.33 These
findings raise concern about confounding effects of pro-
longed survival in patients taking riluzole plus the test
therapy during an RCT. Therefore, we must conclude that
survival is strongly influenced by many factors, including
standard of care and management.
Outcome measures other than survival
One US study of insulin-like growth factor-I (IGF-I) demon-
strated a significant delay in functional deterioration as
measured by the Appel ALS scale.20 IGF-I, however, was not
approved by the FDA because a companion European RCT
showed no benefit.21 The beneficial changes in vital capacity
also were found significant in patients treated with xaliproden
(V. Meininger reported at the International ALS/MDA
Symposium, Arhus, 2001). Forced vital capacity (FVC) also
modestly but significantly differed between a subset of
patients receiving BDNF and those receiving placebo in a
Phase II RCT of BDNF. A Phase II study of gabapentin also
revealed a marginal difference (P=0.057) in the slope of
maximum voluntary muscle contraction (MVIC), favoring the
study drug;19 however, this difference proved to be due to the
more rapid decline in the placebo group.24 RCTs of CNTF
(ACTS group) or topiramate demonstrated significant wor-
sening of MVIC and FVC in those who received the study
drugs.16,26 Although these data are the painful reality, they
strongly support the idea that various outcome measures
other than survival or death can be useful for detecting
changes over time. A leading expert on clinical measures in
neuromuscular diseases once expressed the somewhat cynical
view that when facing repeated negative results in clinical
trials, investigators tend to shift from using one measure to
another. Without any doubt we are facing clear difficulty in
selecting primary outcomes. Simplicity, practicality, and
economy may be some of the important determining factors
when choosing the primary measure. Reflecting these goals,
the ALS functional rating scale (ALSFRS) and revised ALSFRS
seem to be having increasingly broad acceptance for use as
primary outcome measures in clinical trials.34 These topics
will be discussed in the supplement. We predict that the
second gold standard will be determined by the next primary
outcome measure that shows positive results in future RCTs.
Difficulties in using quantitative measures
The issue of intra- and inter-rater variability has been a
concern ever since quantitative measures were first applied in
multicenter ALS studies.17 Certification for the evaluators and
continued training during an RCT are imperative. Also
troublesome is that data are more likely to be missing
when changes are measured quantitatively in ALS trials.
Patients become progressively more disabled during the trial
and find it increasingly difficult to visit the study center for
quantitative studies. Furthermore, when the measures require
the patient’s cooperation to move, position, and give
maximum effort, as seen with MVIC, the test itself becomes
laborious and tiring, increasing the likelihood that data will
not be collected. Incomplete data obviously decrease the
power of the study. In particular, when the change in a
measure over time is used as the outcome, missing data
severely affect the determination of the rate of progression of
disease, i.e., determination of slope. Moreover, how to impute
missing data is a critical issue that has yet to be resolved.
Improving study design
Determining drug dose levels
ALS trialists tend to use higher doses or maximally tolerated
doses of the test medication to identify clinical benefits. This
practice is intended to ensure that the drug maximally
penetrates the central nervous system and to prevent trial
failure because the dose is deemed ‘‘insufficient’’. For
example, in a gabapentin trial, the dose was increased from
Phase II to Phase III,19,24 and in a topiramate trial, a
maximally tolerated dose was used.26 Other dose levels were
not included in either RCT. Multiple dose levels would be
prohibitively expensive, and investigator-initiated RCTs tend
to use a single dose level that would give the highest chance
of benefit. On the other hand, high doses may increase the
chance of intolerable side- effects or worsening of ALS, as
seen in trials of CNTF, topiramate, and gabapentin.16,24,26
Therefore, higher doses are not necessarily better than lower
doses, and multiple dose levels should be considered in RCTs.
Concomitant use of riluzole in RCTs
Although there is no evidence at this point, without doubt
almost all ALS experts and patient advocates suspect that ALS
10 H. Mitsumoto et al
Introduction
Am
yotr
oph
Lat
eral
Scl
er D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
Dav
is o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

must be treated with a combination of multiple effective
drugs in the future, as seen in any other difficult diseases
which are usually treated with multiple medications. The next
logical assumption, although it might sound naıve, is that
adding riluzole is intuitively a ‘‘good thing’’. In fact, several
years ago, after a US IGF-I trial showed benefit, investigators
designed a combination trial of riluzole and IGF-I. This plan
was aborted when the FDA did not approve IGF-I, but the
combination was appropriate at that time. An ideal
combination trial with riluzole was conducted for the RCT
of xaliproden (Table 1). There were two protocols: one in
which patients received a high or low dose of xaliproden plus
riluzole, and one in which patients received xaliproden alone.
However, the trial results showed that administering riluzole
with another study drug might put patients at risk. A drop of
vital capacity to less than 50% was seen more often in those
who took both the higher xaliproden dose and riluzole than
in those who took xaliproden alone (data reported by V.
Meininger et al. at the International ALS/MND Symposium,
Arhus, 2001). In a wobbler mouse study, disease progressed
more rapidly in mice receiving both BDNF and riluzole than
in those receiving either drug alone (T. Ishiyama, unpub-
lished observation 2003). Preclinical studies of combined
treatment with riluzole and the study drug would seem
essential. Inclusion of riluzole without careful preclinical and
clinical consideration may be risky because drug interactions
in ALS are presently unknown.
Trial center and country effects may jeopardize studyresults
The use of NIPPV, PEG, and riluzole varies from center to
center.35-37 When the number of patients enrolled in a study
is not balanced among study centers in a multicenter RCT,
this imbalance may affect study results. In the Phase III
riluzole study, there was a large imbalance in patient
enrollment in different centers. Although the hypothesis is
totally speculative, such imbalance might explain an unusual
result of that trial:18 the Kaplan-Meier survival curve for
European patients receiving riluzole was identical to that of
the North American patients receiving placebo. What we
describe here may have nothing to do with center or country
effects, but it is suggestive of such a problem. In conducting
an ideal RCT, unbalanced enrollment between centers or
regions must be avoided lest it confound the results.
The ‘natural history’ of the placebo group isuncertain
Munsat 38,39 advocated using placebo patient groups from
earlier RCTs, and such historical controls would be sufficient
if an ALS treatment showed unequivocal benefit. Trials using
historical controls might be useful for rapid screening of
multiple new drugs, or to decrease study costs. However, this
design has not been accepted, because the ‘natural history’ in
the placebo arm may not be truly natural because it is
modified by placebo effects 2-4 and selection bias according to
inclusion and exclusion criteria. Furthermore, the natural
histories of control groups in past RCTs differ from one
another.19,22,24 As a result, there is now little support for trials
without placebo controls. As clinical trial experience
increases, however, the use of historical placebo controls
may again seem reasonable.
Another impediment to designing trials with historical
controls is the continuing paucity of historical control data.
Placebo data are not available for every ALS RCT. For
instance, in industry-sponsored trials some data were
considered proprietary and not released to the public. In
our experience, the leaders of the RCTs left the project or firm,
which then lost contact with them, and access to data is now
impossible. In the future, regardless of whether studies are
industry- or investigator-initiated, all placebo data must be
the property of the ALS community. The WALS study group is
providing its control data to other ALS trialists upon request,
and the NEALS group (Dr. Merit Cudkowicz, personal
communication, 2003) has initiated a program to store all
placebo data in an NINDS control databank. In other
neurological disorders, such as multiple sclerosis, virtual control
groups are created by entering all RTC data into a large,
multinational database [http://www.nationalmssociety.org].
In ALS, developing an organized system for storing and
accessing all placebo data is essential to improving ALS
research and RCT design.
Lessons about data and safetymonitoring
Patient safety and data management
An effective Data and Safety Management Program (DSMP) is
key to protecting the study patients from avoidable serious
adverse effects. To ensure rapid and effective triage and
decision-making systems, effective and accurate data manage-
ment and administrative systems are required. Investigator-
initiated studies in ALS are usually constrained by costs. Data
management may suffer most because sophisticated data
management is costly and is therefore a greater obstacle in
investigator-initiated studies than in industry-supported trials.
In the past decade, the NIH has established increasingly
stringent DSMP guidelines so that the DSMPs for NIH-funded
RCTs are now similar to those of industry-designed RCTs.
Well-planned DSMP and data management are imperative for
reliable RCTs.
Lessons for the investigators
Providing open-label medication after a RCT
Patients are often willing to participate in a RCT because they
are desperate and want to take the active drug. If a study does
not guarantee access to the test drug for all participants in an
‘open-label’ component after the formal trial, patients may be
discouraged from enrolling, and the dropout rate may
increase if patients suspect they have been given the placebo.
Access to the test drug is obviously one of the important
benefits and motivations for those who courageously
participate in prolonged and arduous trials. In fact, providing
Randomized control trials in ALS: lessons learned 11
Introduction
Am
yotr
oph
Lat
eral
Scl
er D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
Dav
is o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

the active drug to all the patients in an RCT is one of the WFN
guidelines for RCTs.40
However, conducting the open-label phase after a RCT may
not be simple. The investigators must be certain that the agent
is safe. The open-label phase often is considered as merely an
extension of the blind phase, particularly when the agent is
an off-label drug that has been used in other disorders long
enough to guarantee safety. Consequently, safety might be
taken for granted because it already has been proven, and
participating investigators may have experience with the drug
in other diseases. Patients with ALS, however, may have a
different response to off-label drugs, because of 1. impending
alveolar hypoventilation caused by respiratory muscle weak-
ness, 2. dehydration due to dysphagia, and 3. weakened
immune responses because of malnutrition. Thus, off-label
drugs might act more adversely in patients with ALS than in
other diseases. For example, adverse events resulted in
discontinuation of the open-label phase of the topiramate
trial for ALS.26,41 ALS investigators will be studying more off-
label drugs and will need to pay strict attention to adverse
effects, particularly in patients with rapidly deteriorating
motor neuron function.
Publishing the results
The publication of RCT results, positive or negative, is the
investigators’ responsibility. The pharmaceutical industry has
been criticized for not publishing negative results, and, for
investigators, the experience can be frustrating if the sponsor
loses interest or declines to publish. Negative ALS study
results that have not yet been published include the second
BNDF high-dose subcutaneous study and the BNDF intra-
thecal study. We have been told that manuscripts for the
xaliproden studies are in preparation.
Some industry sponsors have published the results of
negative studies; for example, the IGF-I USA and European
studies, two CNTF studied by the CNTF Study Group and the
ALS CNTF Treatment Study group, and BDNF Study Group
were industry-initiated and had negative results. The inves-
tigators themselves may have been the driving force for
publication of these trials. Negative investigator-driven studies
may also go unreported or be reported in unrefereed journals,
such as a subcutaneous thyrotropin-releasing hormone
multicenter study and the Pan European BCAA study.
However, these studies were done years ago, and perhaps
the importance of publishing negative study results in ALS
was not realized. Journal editors are also likely to resist using
precious pages for the publication of negative results.
In planning a new RCT, the publication plan should be
clearly defined. Without an explicit plan to publish the
results, positive or negative, the RCT should not be
implemented. The development of RCTs for ALS is still in
the early stages, and we must learn as much as possible from
each RCT. Publication is imperative if we are to develop
effective and efficient RCTs for discovering useful ALS
treatments.
Conclusions
In this introduction we have described what we believe we
have learned from past RCTs for ALS. We hope that our
comments will generate discussion and even argument. Every
past RCT in ALS has provided opportunities to learn about
the issues involved in conducting trials. The experience and
the knowledge so generated provide the basis for developing
more effective, more efficient, and more innovative study
designs. We hope this introductory overview will serve as
background for the in-depth discussions, new ideas, opinions,
and critical suggestions that follow in this supplement. We
believe that ALS clinical trials have reached a decisive point
because of the use of diverse outcome measures, study
designs, available drugs, the number of ALS study groups, and
funding opportunities. Moreover, the ALS community is
beginning to work more cohesively. We have come a long
way – RCTs in ALS have matured to a level likely to assure the
proper evaluation of new drugs that can be approved by the
FDA for the treatment of ALS. Much, however, remains to be
accomplished, and it is up to us, particularly the young
investigators, to ensure that future trials are ideally designed,
implemented, analyzed, and published.
Acknowledgements
This publication is in part supported by the MDA Wings Over
Wall Street Fund. Cassandra Talerico-Kaplin provided editor-
ial assistance.
References
1. Olarte MR, Gersten JC, Zabriskie J, Rowland LP. Transfer factor
is ineffective in amyotrophic lateral sclerosis. Ann Neurol 1979;
5(4): 385–388.
2. Bradley WG, Hedlund W, Cooper C et al. A double-
blind controlled trial of bovine brain gangliosides in
amyotrophic lateral sclerosis. Neurology 1984; 34: 1079–1082.
3. Brooke MH, Florence JM, Heller SL et al. Controlled
trial of thyrotropin releasing hormone in amyotrophic lateral
sclerosis. Neurology 1986; 36: 146–151.
4. Mitsumoto H, Salgado ED, Negroski D et al. Amyotrophic
lateral sclerosis: effects of acute intravenous and chronic
subcutaneous administration of thyrotropin-releasing
hormone in controlled trials. Neurology 1986; 36: 152–159.
5. Brooks BR, Sufit RL, Montgomery GK, Beaulieu DA, Erickson LM.
Intravenous thyrotropin releasing hormone in patients with
amyotrophic lateral sclerosis: dose response and
randomized concurrent placebo controlled pilot studies.
Neurol Clin 1987; 5: 143–158.
12 H. Mitsumoto et al
Introduction
Am
yotr
oph
Lat
eral
Scl
er D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
Dav
is o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.
6. The National TRH Study Group. Multicenter controlled trial:
no effect of alternate-day 5mg/kg subcutaneous thyrotropin-
releasing hormone (TRH) on isometric strength decrease in
amyotrophic lateral sclerosis [abstract]. Neurology 1989; 39
(suppl): 322.
7. Appel SH, Stewart SS, Appel V et al. A double-blind study of the
effectiveness of cyclosporine in amyotrophic lateral sclerosis.
Arch Neurol 1988; 45(4): 381–386.
8. Steiner TJ. Motor Neurone Disease: Experience with Large
Multicenter Trials. In: Guiloff RJ, ed. Clinical Trials in Neurology.
London: Springer-Verlag, 2001: 451–463.
9. The Italian ALS Study Group. Branched-chain amino acids and
amyotrophic lateral sclerosis: a treatment failure? Neurology
1993; 43: 2466–2470.
10. Tandan R, Bromberg MB, Forshew D et al. A controlled trial of
amino acid therapy in amyotrophic lateral sclerosis: I. Clinical,
functional, and maximum isometric torque data. Neurology
1996; 47: 1220–1226.
11. Eisen A, Stewart H, Schulzer M, Cameron D. Anti-glutamate
therapy in amyotrophic lateral sclerosis: a trial using lamotrigine.
Can J Neurol Sci 1993; 20: 297–301.
12. Bensimon G, Lacomblez L, Meininger V. A controlled trial of
riluzole in amyotrophic lateral sclerosis. ALS/Riluzole Study
Group. N Engl J Med 1994; 330: 585–591.
13. Louwerse ES, Weverling GJ, Bossuyt P et al. Randomized,
double-blind, controlled trial of acetylcysteine in amyotrophic
lateral sclerosis. Arch Neurol 1995; 52: 559–564.
14. Miller RG, Shepherd R, Dao H et al. Controlled trial of
nimodipine in amyotrophic lateral sclerosis. Neuromuscul
Disord 1996 6; 20: 101–104.
15. Miller RG, Smith SA, Murphy JR et al. A clinical trial of verapamil
in amyotrophic lateral sclerosis.MuscleNerve 1996; 19: 511–551.
16. The ALS CNTF Treatment Study (ACTS) Phase III Study Group.
A double-blind placebo controlled trial of subcutaneous recom-
binant human ciliary neurotrophic factor (rHCNTF) in amyo-
trophic lateral sclerosis. Neurology 1996; 46: 1244–1249.
17. Miller RG, Petajan JH, Bryan WW et al. A placebo controlled trial
of recombinant human ciliary neurotrophic (rhCNTF) factor in
amyotrophic lateral sclerosis. Ann Neurol 1996; 39: 256–260.
18. Lacomblez L, Bensimon G, Leigh PN et al. Dose-ranging study of
riluzole in amyotrophic lateral sclerosis. Amyotrophic Lateral
Sclerosis/Riluzole Study Group II. Lancet 1996; 347: 1425–1431.
19. Miller RG, Moore D, Young LA et al. Placebo controlled trial of
gabapentin in patients with amyotrophic lateral sclerosis.
Neurology 1996; 47: 1383–1388.
20. Lai EC, Felice KJ, Festoff BW et al. Effect of recombinant human
insulin-like growth factor-I on progression of ALS: a placebo
controlled study. The North America ALS/IGF-I Study Group.
Neurology 1997; 49: 1621–1630.
21. Borasio GD, Robberecht W, Leigh PN et al. A placebo controlled
trial of insulin-like growth factor-I in amyotrophic lateral
sclerosis. European ALS/IGF-I Study Group. Neurology 1998;
51: 583–586.
22. Lange DJ, Murphy PL, Diamond B et al. Selegiline is ineffective
in a collaborative double-blind controlled trial for treatment of
amyotrophic lateral sclerosis. Arch Neurol 1998; 55: 93–96.
23. BDNF Study Group. A controlled trial of recombinant methionyl
human BDNF in ALS. The BDNF Study Group (Phase III).
Neurology 1999; 52: 1427–1433.
24. Miller RG, Moore DH Jr, Gelinas DF et al. Phase III randomized
trial of gabapentin in patients with amyotrophic lateral sclerosis.
Neurology 2001; 56: 843–848.
25. Desnuelle C, Dib M, Garrel C, Favier A. A double-blind, placebo
controlled randomized clinical trial of alpha-tocopherol (vitamin
E) in the treatment of amyotrophic lateral sclerosis. ALS riluzole-
tocopherol Study Group. Amyotroph Lateral Scler Other Motor
Neuron Disord 2001; 2: 9–18.
26. Cudkowicz ME, Shefner JM, Schoenfeld DA et al. A randomized,
placebo controlled trial of topiramate in amyotrophic lateral
sclerosis. Neurology 2003; 61: 456–464.
27. Groeneveld GJ, Veldink JH, van der Tweel I et al. A randomized
sequential trial of creatine in amyotrophic lateral sclerosis. Ann
Neurol 2003; 53: 437–445.
28. Gurney ME, Fleck TJ, Himes CS, Hall ED. Riluzole preserves
motor function in a transgenic model of familial amyotrophic
lateral sclerosis. Neurology 1998; 50: 62–66.
29. Mitsumoto H, Tsuzaka K. Neurotrophic factors and neuro-
muscular diseases. Part I and Part II. Muscle Nerve 1999; 22:
983–999 (I) and 1000–1021 (II).
30. Kaspar BK, Llado J, Sherkat N, Rothstein JD, Gage FH. Retrograde
viral delivery of IGF-1 prolongs survival in a mouse ALS model.
Science 2003; 301: 839–342.
31. Murray B, Mitsumoto H. Drug therapy in amyotrophic lateral
sclerosis. In: Pourmand R, Harati Y, eds. Neuromuscular
Disorders. New York: Lippincott, Williams and Wilkins.
Advances in Neurology 2002; 88 63–82.
32. Rowland LP, Schneider NA. Medical progress: amyotrophic
lateral sclerosis. N Engl J Med 2001; 344: 1688–1700.
33. Traynor BJ, Alexander M, Corr B et al. Riluzole and prognosis in
ALS: findings of the Irish ALS registry from 1995–2000. ALS and
other Motor Neuron Diseases 2001; 2 (Suppl 2): 43–44.
34. The ALS CNTF Treatment Study (ACTS) Phase I-II Study Group.
The Amyotrophic Lateral Sclerosis Functional Rating Scale.
Assessment of activities of daily living in patients with
amyotrophic lateral sclerosis. Arch Neurol 1996; 53: 141–147.
35. Bryan WW, McIntire D, Camperlengo L et al. Factors influencing
the use of riluzole by ALS patients. 8th International Symposium
on ALS/MND. November1997(abstract).Published in J Neurol Sc.
36. Cedarbaum JM, Stambler N. Disease status and use of ventilatory
support by ALS patients. BDNF Study Group. Amyotroph Lateral
Scler Other Motor Neuron Disord 2001; 2: 19–22.
37. Mitsumoto H, Davidson M, Moore DH et al. Percutaneous
endoscopic gastrostomy (PEG) in patients with ALS and bulbar
dysfunction. Amyotrophic Lateral Scler Other Motor Neuron
Disord 2003; 4: 177–185.
38. Munsat TL, Andres PL, Finison L, Conlon T, Thibodeaur L. The
natural history of motor neuron loss in amyotrophic lateral
sclerosis. Neurology 1988; 38: 409–413.
39. Munsat TL, Andres P, Skerry L. Therapeutic trials in amyotrophic
lateral sclerosis: measurement of clinical deficit. In: Rose FC, ed.
Amyotrophic Lateral Sclerosis. New York: Demos, 1990: 65–76.
40. The World Federation of Neurology Research Group on
Neuromuscular Diseases, Subcommittee on Motor Neuron
Disease: Airlie House Guidelines. Therapeutic trials in amyo-
trophic lateral sclerosis. J Neurol Sci 1995; 129 (suppl): 1–10.
41. Kaufmann P, Lomen-Hoerth C. ALS treatment strikes out
while trying for a homer:the topiramate trial. Neurology 2003;
61: 434–435.
Randomized control trials in ALS: lessons learned 13
Introduction
Am
yotr
oph
Lat
eral
Scl
er D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
Dav
is o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.





























