Embed Size (px)
Citation preview
CONCLUSIONS
Randomized Controlled Comparison of IV Catheter with Coiled Tip Guidewire and Conventional Peripheral IV Catheter
Bette K. Idemoto, PhD, RN, ACNS-BC, CCRN CNS & James R. Rowbottom, MD, Anesthesia Dept Chair
University Hospitals Case Medical Center, Cleveland, OH
BACKGROUND RESULTS
Acknowledgements: Dr. Amir Belson, Inventor; Sponsor, Vascular Pathways, Inc.; UHCMC SICU/LT3 Study RNs & Medical-Surgical Dept of Nursing
PURPOSE
METHODS
RESULTS
Seventy percent of hospitalized patients experience frequent intravenous
therapy as a treatment modality.
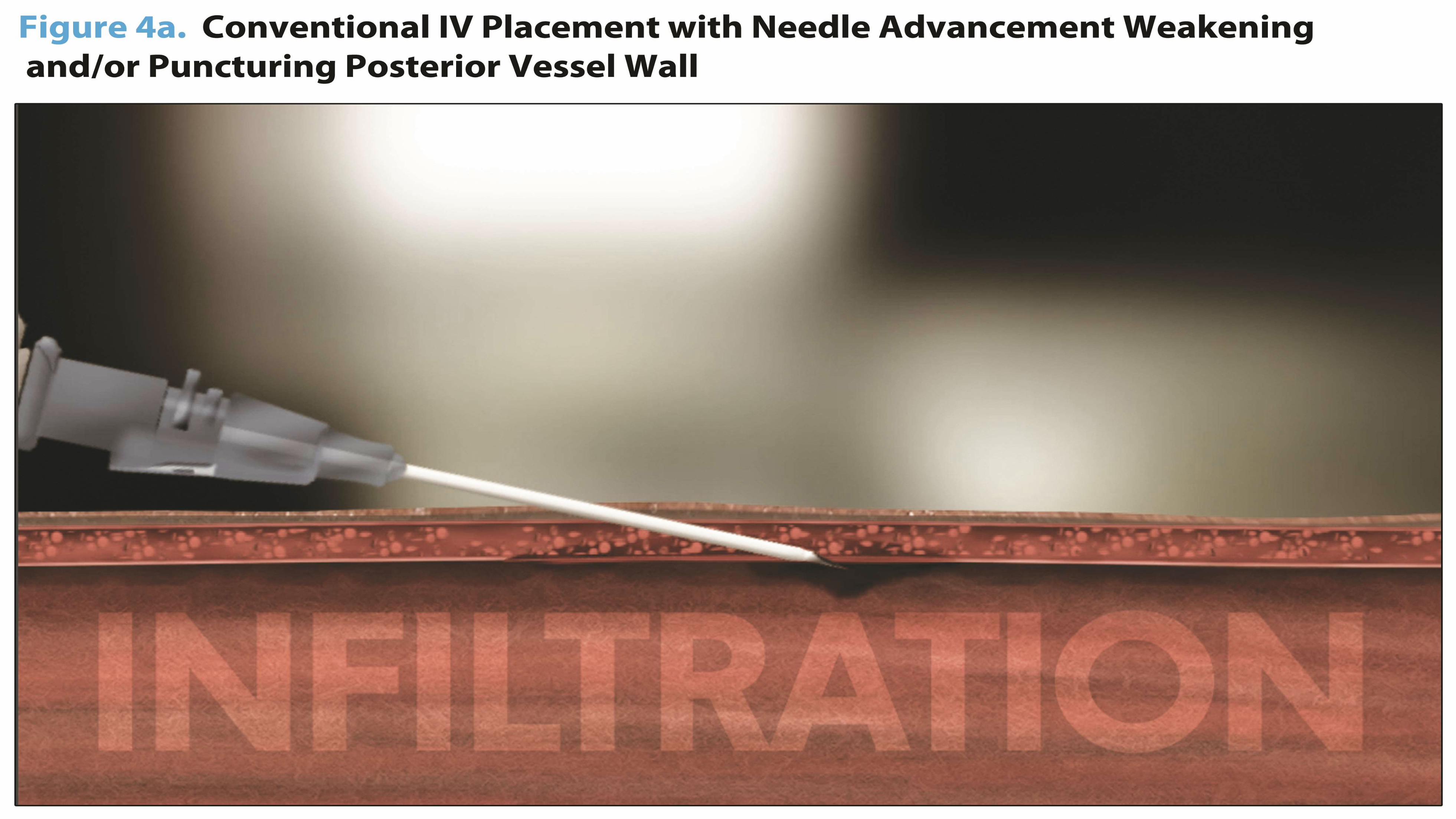
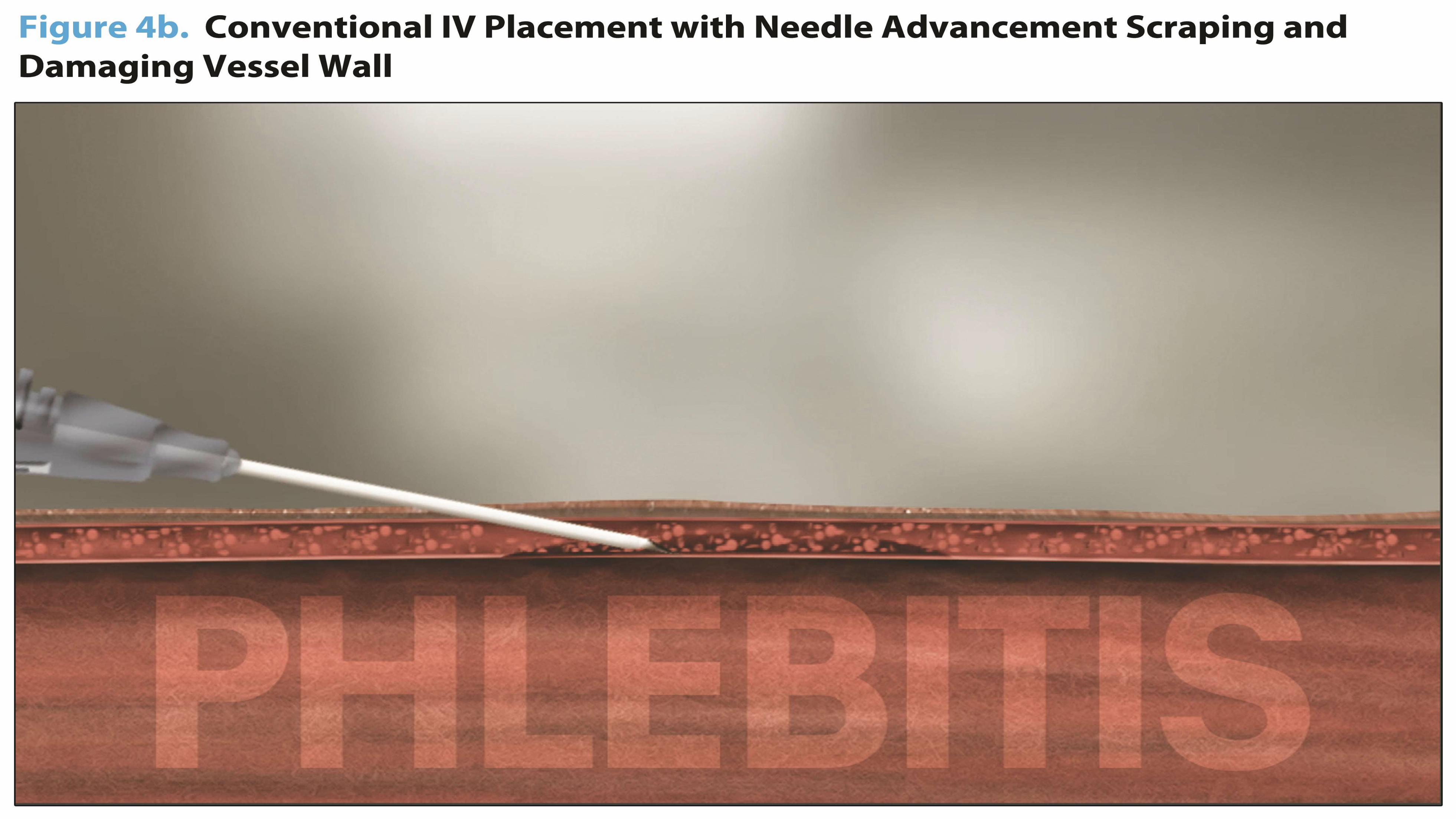
However, peripheral IVs are often associated with pain/discomfort and
risk of phlebitis, infiltration or infections. Therefore, first attempt
success and dwell time for IV catheters are important outcomes.
Currently first attempt success averages 40% in adults, complications
occur 47% and average IV dwell time is 44 hrs. 50% of PIV lines require
replacement before completion of therapy.
Multiple attempts at insertion and multiple IVs during each admission
result in poor patient and clinician satisfaction as well as unnecessary
costs.
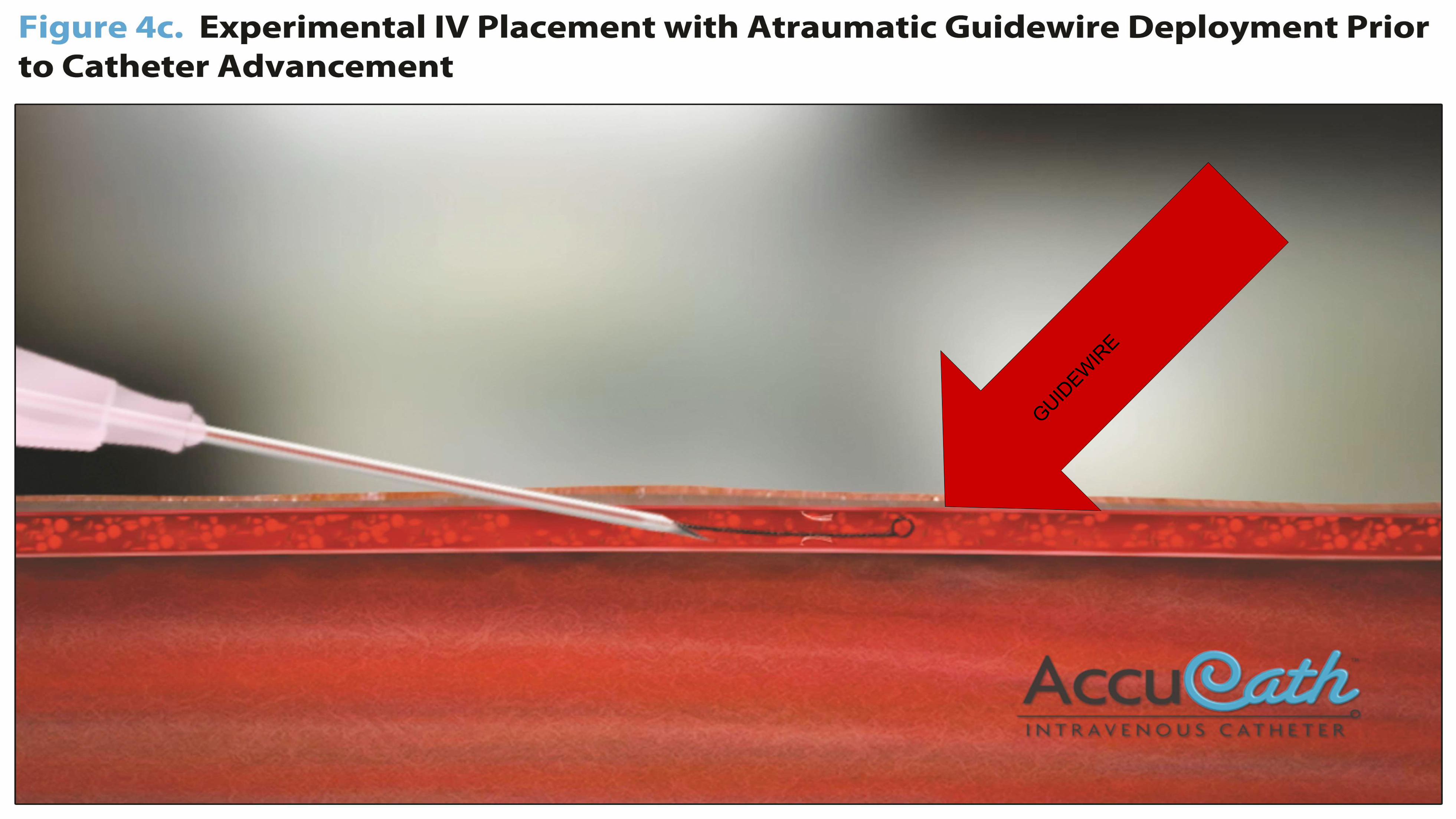
A new peripheral IV catheter technology that uses a proprietary coiled
tip guidewire design previously seen only in central lines is now
available.
This prospective study compared Experimental and Conventional IV
catheters in adult patients.
Outcomes evaluated included: rate of successful placement on first
attempt, complication rates, dwell times, rate of completion of therapy,
patient and clinician satisfaction and overall costs of therapy.
Patient satisfaction with IV insertion for Experimental using a 5 point
Likert Scale:
This study demonstrated that the use of the Experimental IV was feasible for
hospitalized adults, associated with better outcomes without increasing overall
cost of care and significantly improved patient and clinician satisfaction.
Use of the Experimental IV was associated with positive outcomes including
first attempt success, fewer complications, increased dwell time, higher
completion of therapy, and decreased cost of therapy.
Larger studies are needed to validate this technology in other populations and
multiple care settings.
Industry and hospital IRB approval were obtained prior to
beginning
the study.
Adult medical-surgical patients who required a non-emergent IV
catheter were consented and enrolled.
Randomized enrollment was ensured with sealed envelopes, which
were opened once patient consent was obtained.
Data was collected by the Study RNs using a standardized
instrument.
The study was conducted over 4 months: total of 248 patients
(Experimental IV 123 patients, Conventional IV 125 patients).
Outcomes were assessed using parametric and non-parametric
tests.
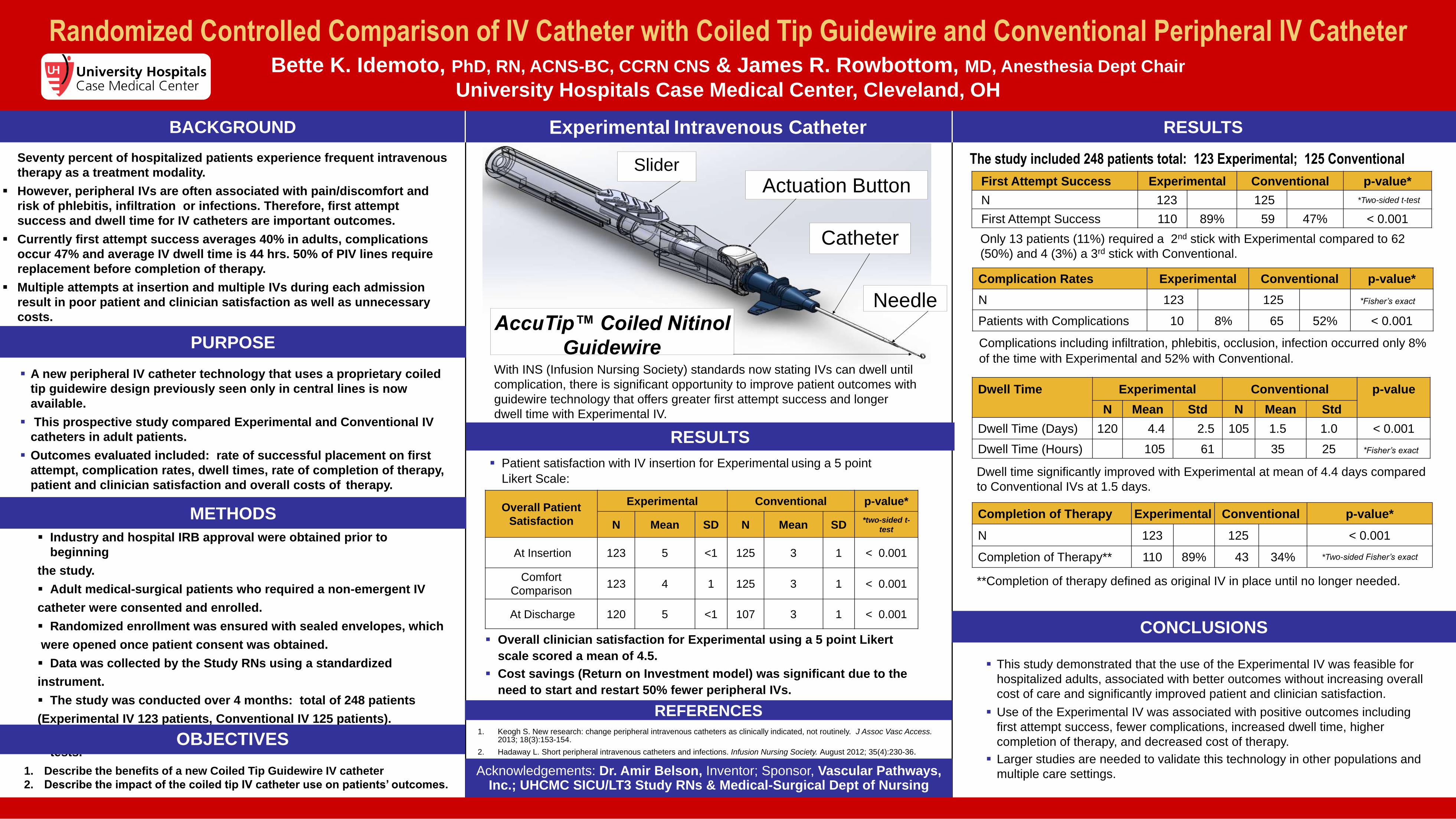
First Attempt Success Experimental Conventional p-value*
N 123 125 *Two-sided t-test
First Attempt Success 110 89% 59 47% < 0.001
Complication Rates Experimental Conventional p-value*
N 123 125 *Fisher’s exact
Patients with Complications 10 8% 65 52% < 0.001
Dwell Time Experimental Conventional p-value
N Mean Std N Mean Std
Dwell Time (Days) 120 4.4 2.5 105 1.5 1.0 < 0.001
Dwell Time (Hours) 105 61 35 25 *Fisher’s exact
With INS (Infusion Nursing Society) standards now stating IVs can dwell until
complication, there is significant opportunity to improve patient outcomes with
guidewire technology that offers greater first attempt success and longer
dwell time with Experimental IV.
Completion of Therapy Experimental Conventional p-value*
N 123 125 < 0.001
Completion of Therapy** 110 89% 43 34% *Two-sided Fisher’s exact
Complications including infiltration, phlebitis, occlusion, infection occurred only 8%
of the time with Experimental and 52% with Conventional.
Dwell time significantly improved with Experimental at mean of 4.4 days compared
to Conventional IVs at 1.5 days.
**Completion of therapy defined as original IV in place until no longer needed.
Overall clinician satisfaction for Experimental using a 5 point Likert
scale scored a mean of 4.5.
Cost savings (Return on Investment model) was significant due to the
need to start and restart 50% fewer peripheral IVs.
The study included 248 patients total: 123 Experimental; 125 Conventional
Experimental Intravenous Catheter
Only 13 patients (11%) required a 2nd stick with Experimental compared to 62
(50%) and 4 (3%) a 3rd stick with Conventional.
Actuation Button
Catheter
Needle AccuTip™ Coiled Nitinol
Guidewire
Slider
Overall Patient
Satisfaction
Experimental Conventional p-value*
N Mean SD N Mean SD *two-sided t-
test
At Insertion 123 5 <1 125 3 1 < 0.001
Comfort
Comparison 123 4 1 125 3 1 < 0.001
At Discharge 120 5 <1 107 3 1 < 0.001
OBJECTIVES
1. Describe the benefits of a new Coiled Tip Guidewire IV catheter
2. Describe the impact of the coiled tip IV catheter use on patients’ outcomes.
1. Keogh S. New research: change peripheral intravenous catheters as clinically indicated, not routinely. J Assoc Vasc Access. 2013; 18(3):153-154.
2. Hadaway L. Short peripheral intravenous catheters and infections. Infusion Nursing Society. August 2012; 35(4):230-36.
REFERENCES