Embed Size (px)
Citation preview

02 (2006) 432–439www.elsevier.com/locate/ygyno
Gynecologic Oncology 1
Randomized phase III trial of three versus six cycles of adjuvantcarboplatin and paclitaxel in early stage epithelial ovarian carcinoma:
A Gynecologic Oncology Group study
Jeffrey Bell a,⁎,1, Mark F. Brady b, Robert C. Young c, Janice Lage d, Joan L. Walker e,Katherine Y. Look f, G. Scott Rose g, Nick M. Spirtos h
a Ohio State University and Division of Gynecologic Oncology, Riverside Methodist Hospital (Columbus Cancer Council),Columbus, OH, USA
b Gynecologic Oncology Group Statistical and Data Center, Roswell Park Cancer Institute, Buffalo, NY 14263, USAc Fox Chase Cancer Center, Philadelphia, PA 19111, USA
d Department of Pathology and Laboratory Medicine, Medical University of South Carolina, Charleston, SC 29425, USAe Section of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of Oklahoma Health Sciences, Oklahoma City, OK 73190, USA
f Department of Obstetrics and Gynecology, Indiana University School of Medicine, Indianapolis, IN 46202, USAg Division of Gynecologic Oncology, Walter Reed Army Medical Center, Washington, DC 20307, USA
h Division of Gynecologic Oncology, University of Nevada School of Medicine and Women’s Cancer Center of Nevada, Las Vegas, NV 89102, USA
Received 4 January 2006Available online 24 July 2006
Abstract
Objective. Compared to 3 cycles, to determine if 6 cycles of adjuvant carboplatin (C) and paclitaxel (P) significantly lower the rate ofrecurrence in surgically staged patients with stage IA grade 3, IB grade 3, clear cell, IC, and completely resected stage II epithelial ovarian cancer(EOC); and to compare toxicities.
Methods. Postoperatively, randomization was to either 3 or 6 cycles of chemotherapy consisting of P (175 mg/m2 over 3 h) and C (7.5 AUCover 30 min) every 21 days. Recurrence was any clinical or radiological evidence of new tumor.
Results. Of 457 patients, 427 (93%) were histologically and medically eligible. While thorough surgical staging was required, it wasincomplete or inadequately documented in 29% of otherwise eligible patients. Median age was 55.5 years; 69% of patients had stage I disease.Median follow-up is 6.8 years for 344 women alive at last contact. Grade 3 or 4 neurotoxicity occurred in 4/211 (2%) and 24/212 (11%) treatedpatients on the 3- and 6-cycle regimens, respectively (p<0.01); 6 cycles also caused significantly more severe anemia and granulocytopenia. Therecurrence rate for 6 cycles was 24% lower (hazard ratio [HR]: 0.761; 95% confidence interval [CI]: 0.51–1.13, p=0.18), and the estimatedprobability of recurrence within 5 years was 20.1% (6 cycles) versus 25.4% (3 cycles). The overall death rate was similar for these regimens (HR:1.02; 95% CI: 0.662–1.57).
Conclusions. Compared to 3 cycles, 6 cycles of C and P do not significantly alter the recurrence rate in high risk early stage EOC but areassociated with more toxicity.© 2006 Elsevier Inc. All rights reserved.
Keywords: Adjuvant chemotherapy; Early stage EOC; Recurrence rate; Carboplatin; Paclitaxel
⁎ Corresponding author. Riverside Methodist Hospital, 500 Thomas Lane,Suite 3B Columbus, OH 43214, USA. Fax: +1 614 538 0443.
E-mail address: [email protected] (J. Bell).1 Current address: Suite 511 North Medical Building, 3545 Olentangy River
Road, Columbus, OH 43214, USA.
0090-8258/$ - see front matter © 2006 Elsevier Inc. All rights reserved.doi:10.1016/j.ygyno.2006.06.013
Introduction
Approximately 30% of ovarian carcinomas are localized andamenable to complete surgical resection at the time of their initialpresentation. The need for adjuvant therapy for patients with earlystage epithelial ovarian cancer (EOC) has been the basis fornumerous clinical trials conducted over the past two decades. For

433J. Bell et al. / Gynecologic Oncology 102 (2006) 432–439
patients with stage IA or IB disease and favorable histology,survival after thorough surgical staging alone is excellent (>90%disease-free survival at 6 years). In these cases, adjuvant therapy isconsidered unnecessary when thorough surgical staging andhistological confirmation have been performed [1].
In contrast, other patients with early stage EOC (stage IA orIB and unfavorable histology including grade 3 or clear cell,stage IC, or stage II) are candidates for adjuvant treatment basedupon significant 5-year recurrence rates of approximately 25–45%. The optimal adjuvant treatment for this group of high riskearly stage EOC patients is unknown. Early experience in theGynecologic Oncology Group (GOG) showed that such patientstreated with either intraperitoneal phosphorus-32 or oralmelphalan had similar survival rates of approximately 80% at6 years [1]. A subsequent study of patients with the same diseasestages compared intraperitoneal phosphorus-32 to 3 cycles ofcisplatin plus cyclophosphamide. Although not statisticallysignificant, the recurrence rate on the cisplatin regimen was 31%lower than the phosphorus-32 regimen [2]. A multicenter Italiantrial also comparing cisplatin to intraperitoneal phosphorus-32 instage IC EOC found that cisplatin significantly reduced therelapse rate by 61% [3]. This series of studies led the GOG toselect platinum-based chemotherapy as the standard treatmentfor high risk early stage ovarian cancer.
Carboplatin plus paclitaxel has become the standard adjuvantchemotherapy for advanced ovarian cancer based upon datademonstrating that the combination of cisplatin plus paclitaxelis superior to that of cisplatin plus cyclophosphamide [4] andthat carboplatin's activity is equivalent to that of cisplatin [5].Based on these data, the GOG chose the combination ofcarboplatin plus paclitaxel for this trial in early stage ovariancancer.
The optimal duration of adjuvant chemotherapy in ovariancarcinoma is unclear. Three randomized trials in primarilyadvanced ovarian cancer comparing 5–6 cycles versus 8–12cycles of cisplatin-based chemotherapy failed to show abenefit from chemotherapy beyond 6 cycles [6]. In early stagedisease, the GOG has historically used 3 cycles of chemother-apy as the standard treatment. The objective of this study wasto compare recurrence rates following randomization to eithera standard regimen of 3 cycles of C plus P or 6 cycles of thesame agents.
Methods
All eligible patients had a histological diagnosis of epithelial ovarian cancerincluding serous, mucinous, endometrioid, mixed, undifferentiated, Brenner,clear cell, and transitional types. Borderline or low malignant potential tumorswere ineligible. Participating institutions' institutional review boards approvedthe study prior to enrolling any patient; and all patients provided writteninformed consent consistent with federal, state and local regulations beforerandomization. After a staging operation, patients were to have completelyresected stage IA grade 3 (or clear cell), stage IB grade 3 (or clear cell), stage IC,or stage II disease. Other eligibility criteria included: no prior treatment exceptsurgery, adequate bone marrow, renal, and hepatic function, and a GOGperformance status less than 4. All patients were to be entered onto the trialwithin 6 weeks following staging laparotomy.
Surgical staging was to be performed according to GOG standards. Requiredprocedures included total hysterectomy, bilateral salpingo-oophorectomy,
resection of all gross disease, aspiration of free peritoneal fluid, peritonealwashings for cytology, infracolic omentectomy, selective bilateral pelvic andaortic node dissections, peritoneal biopsies from four pelvic locations andbilateral paracolic areas, and right diaphragm cytology or biopsy. Surgicalreports, pathology reports and representative pathology materials were reviewedcentrally in order to confirm eligibility.
All patients were registered and randomly allocated at the GOG Statisticaland Data Center. The randomized treatment was revealed after patientregistration. This report includes an accounting of all patients registered ontothe study. Patients were to receive either 3 or 6 cycles of chemotherapyconsisting of paclitaxel 175 mg/m2 by 3 h infusion and carboplatin dosed atAUC 7.5 by infusion over 30 min. Treatment cycles were scheduled every21 days. Standard preparative regimen for paclitaxel included dexamethasone,diphenhydramine, and cimetidine.
Toxicities were evaluated according to standard GOG toxicity criteria [7].Those patients who did not receive any carboplatin or paclitaxel are not includedin the summary of toxicities.
Treatment modifications were designed to maximize dose intensity.Minimum blood counts required for treatment were absolute neutrophil count(ANC) of 1500 cells/mm3 and platelets of 100,000 cells/mm3. Treatmentmodifications were instituted in a sequential manner, employing course delay,dose reduction, and filgrastim. Chemotherapy dose was not reduced unlesstreatment was delayed more than 2 weeks. No dose modification was made foruncomplicated nadirs. Patients received G-CSF only if they experiencedrecurrent delays or neutropenic complications after a dose reduction. Patientswere to have weekly blood counts during therapy and physical examinationsprior to each treatment, then quarterly for 2 years, semi-annually for 3 years,then annually.
In this study, the primary measure for assessing the therapeutic benefit of 3additional cycles of C plus P is the recurrence rate within each randomizedtreatment group. In order to promote internal as well as external validity, womenwho did not complete the protocol-required staging procedure or whose stagingprocedure was not adequately documented were included in the current analysisunless otherwise specifically noted. Recurrence was defined as any clinical orradiographic evidence of new tumor. Time at risk of recurrence was assessedfrom the date the patient was registered onto the study to the date of recurrenceor to the date of last contact if no recurrence was observed. The recurrence ratesfor the study regimens were compared using a proportional hazards modeladjusted for FIGO (International Federation of Gynecology and Obstetrics)stage and histological grade.
Patients were included in the analyses of recurrence and survival accordingto their randomized treatment assignment regardless of the amount of studytreatment received. The targeted accrual size was 330 eligible patientsundergoing complete staging surgery. The study design specified an interimanalysis be conducted when at least 35 recurrences were noted among theeligible patients to rule out an extreme difference in the recurrence rate betweenthe treatment groups. The data were to be considered sufficiently mature for thefirst general release of results when at least 21% of the eligible patients hadexperienced recurrence. In anticipation of a loss in statistical power due to thepossibility that some patients randomized to 6 cycles would not receive allprescribed therapy, the statistical design allowed for an increase in the minimumrequired number of events necessary for study maturity by either increasing thetargeted accrual or the post-accrual follow-up period [8]. The study designprovided an 85% chance of identifying a treatment regimen as active if itreduced the recurrence rate 50% when the type I error was set to 0.05 for a one-tail test. This treatment effect is comparable to increasing the expectedpercentage of patients who are recurrence-free at 4 years from 80.6% to 89.8%.All p-values in this report are for two-tail tests unless otherwise indicated. Thecumulative incidence of cancer recurrence is estimated using a procedure thattreats non-cancer-related death as a competing risk [9].
Results
Between March of 1995 and May of 1998, 457 patients wereenrolled in this study, of whom 427 (93%) were consideredeligible following centralized pathologic and medical review(Table 1). In a subsequent centralized review of all the surgical

Table 1
434 J. Bell et al. / Gynecologic Oncology 102 (2006) 432–439

Table 2Patient characteristics (n=427)
Characteristic Randomized treatment
CP×3 cycles CP×6 cycles
No. % No. %
Age<40 19 8.9 23 10.740–49 50 23.5 49 22.950–59 68 31.9 57 26.660–69 46 21.6 49 22.9≥70 30 14.1 36 16.8
RaceHispanic 9 4.2 7 3.3Non-Hispanic Black 10 4.7 7 3.3Non-Hispanic White 187 87.8 194 90.7Asian 7 3.3 5 2.3Native American 0 0.0 1 0.5
StageI 141 66.2 152 71.0II 72 33.8 62 29.0
Cell typeSerous adenocarcinoma 53 24.9 44 20.6Endometrioid adenocarcinoma 46 21.6 59 27.6Mucinous adenocarcinoma 12 5.6 19 8.9Clear cell adenocarcinoma 70 32.9 60 28.0Mixed epithelial
adenocarcinoma24 11.3 17 7.9
Other 8 3.7 15 7.0
Grade of primary tumor1 27 12.7 34 15.92 50 23.5 49 22.93 66 31.0 71 33.2Clear cell (no grade) 70 32.9 60 28.0
CP=carboplatin plus paclitaxel.
Table 4Grade 2–4 toxicity for patients who received any of their assigned study therapy
Toxicity CP×3 cycles (n=211) CP×6 cycles (n=212)
Grade Grade
435J. Bell et al. / Gynecologic Oncology 102 (2006) 432–439
reports, 126 of the 427 (29%) had surgical procedures that wereconsidered inadequately documented or less thorough thanspecified by the protocol. Of the 427 patients deemedpathologically and medically eligible, 293 (69%) were surgicalstage I and 134 (31%) were stage II. Table 2 describes the othercharacteristics of these patients. Of the eligible patients, 213were randomly assigned to the 3-cycle regimen and 214 to the6-cycle regimen. The proportion of patients completing the 3-cycle regimen was 96% compared to 83% for the 6-cycle
Table 3Reasons for stopping study treatment
Reason stopped Randomized treatment (n=427)
CP×3 cycles CP×6 cycles
No. % No. %
Completed study regimen 204 95.8 177 82.7Progression 1 0.5 4 1.9Death 1 0.5 1 0.5Toxicity 6 2.8 27 12.6Patient refused 1 0.5 3 1.4Other 0 0.0 2 0.9Total 213 214
CP=carboplatin plus paclitaxel.
regimen. The percent of patients who received fewer than 3cycles was 4% in the 3-cycle regimen and 5% in the 6-cycleregimen. Table 3 summarizes the reasons patients did notcomplete their prescribed therapy.
Table 4 summarizes toxicities of treatment. Grade 3 and 4neurotoxicity occurred in 2% of patients in the 3-cycle arm andin 11% in the 6-cycle regimen (p<0.01). Grade 4 granulocy-topenia was reported in 52% and 66% of the 3-cycle and 6-cyclearms, respectively (p<0.01). Grade 2 or higher anemia occurredin 32% and 48% of the 3-cycle and 6-cycle arms, respectively(p<0.01). Treatment may have contributed to the death of twopatients. One patient experienced a fatal cardiac arrest duringher second cycle of treatment; another died from acuterespiratory distress after her second cycle of chemotherapy.One patient on the 3-cycle regimen developed a myelodysplas-tic syndrome (MDS) 3 years, 5 months after entering the study.After completing protocol therapy, she was treated with anadditional six cycles of carboplatin–paclitaxel for diseaserecurrence and, failing this treatment, had recently initiatedchemotherapy with etoposide when the MDS occurred.
The median duration of follow-up for the 344 patients whowere alive at last contact is 6.8 years (1st and 3rd quartile are 5and 8 years, respectively). There have been 101 reportedrecurrences. In two women (one in each treatment arm), anti-cancer salvage therapy was initiated even though a risingCA125 level was the only indication for recurrent disease. Thedate of this event (48 months and 53 months, respectively) wasused to indicate recurrence for these two patients in this report.
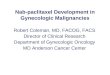
Among the patients in the standard (3-cycle) arm, theestimated cumulative incidence of cancer recurring within5 years was 25.4% compared to 20.1% in the 6-cycle arm.Adjusting for initial FIGO stage and tumor grade, the recurrencerate was 24% lower for patients treated with 6 cycles ofchemotherapy (relative hazard=0.761, 95% CI=0.512–1.13,p=0.18). Fig. 1 displays the cumulative incidence of recurrencefor the two treatment groups.
2 3 4 2 3 4
Granulocytopenia a 20 57 108 17 41 141Thrombocytopenia b 21 23 23 35 20 25Anemia 58 9 1 89 14 0GI 32 10 0 44 10 9Renal 1 0 0 1 0 0Neurologic 28 4 0 38 22 2Alopecia 124 0 0 135 0 0Ototoxicity 1 0 0 6 0 0Infection 10 1 1 12 2 0Fever 11 0 0 17 1 0Allergy 2 1 2 6 3 4Myalgia 16 1 0 17 2 0
CP=carboplatin plus paclitaxel.a Repeat assessment not available in 2 patients.b Repeat assessment not available in 1 patient.

Fig. 1. Cumulative incidence of recurrence by randomized treatment.
436 J. Bell et al. / Gynecologic Oncology 102 (2006) 432–439
Fig. 2 shows the estimated treatment hazard ratios bydisease stage. After adjusting for histologic grade, theestimated treatment hazard ratio is 0.769 among patientswith stage I disease and 0.751 among those with stage IIdisease. The cumulative incidence of recurrence within5 years was 18% and 33% for those women diagnosed withFIGO stage I and stage II disease, respectively. Likewise,the estimated probability of surviving 5 years was 84% and73%, respectively.
Overall survival by treatment group is displayed in Fig. 3.The estimated probability of surviving 5 years is 81% on the 3-cycle regimen and 83% on the 6-cycle regimen. The overalldeath rate is very similar for the two treatment groups (hazardratio 1.02; 95% CI=0.662–1.57, p=0.94).
An unexpected large number of patients (58 in the 3-cycle arm and 68 in the 6-cycle arm; not statisticallysignificant) had an incomplete or inadequately documentedsurgical staging procedure. Fig. 4 compares the cumulativeincidence of recurrence for patients who either had or didnot have a documented complete staging procedure. The
Fig. 2. Treatment hazard ratios fo
cumulative incidence of recurring within 5 years was 22%for those who did have a documented complete stagingprocedure and 26% for those who did not. This difference isnot statistically significant. The treatment hazard ratiosadjusted for FIGO stage and histologic grade are 0.796 forthe former group and 0.660 for the latter (Fig. 5). That is,the estimated benefit of 6 cycles was slightly less amongthose having complete staging surgery, although there is nosignificant evidence of heterogeneity in the treatment effect.In the subset of patients for whom complete surgical stagingwas documented, the cumulative incidence of recurrencewithin 5 years was 23% and 20%, respectively, for the 3-cycle and 6-cycle regimens.
Among the 301 patients considered to have had completestaging surgery, 205 (68%) had stage I disease and 96(32%) had stage II disease. The cumulative incidence ofrecurrence within 5 years for those two groups was 18%and 31%, respectively. Likewise, among the 126 patientswithout a complete staging procedure, 88 (70%) had stage Idisease and 38 (30%) had stage II disease. The cumulative
r recurrence by disease stage.

Fig. 3. Overall survival by randomized treatment.
437J. Bell et al. / Gynecologic Oncology 102 (2006) 432–439
incidence of recurrence within 5 years was 20% and 40%,respectively.
Discussion
This multi-institutional study demonstrates that adding 3cycles of carboplatin plus paclitaxel to the standard 3 cyclesdoes not significantly reduce the cancer recurrence rates forpatients with high risk, early stage EOC. On the other hand, theadditional cycles of chemotherapy did significantly increasetoxicity. Not surprisingly, fewer patients completed the 6-cycleregimen. Whereas 95% of patients (pooling both treatmentgroups) completed 3 cycles, only 83% completed 6 cycles of
Fig. 4. Cumulative incidence of recurrence
therapy, primarily due to increased toxicity (4%) or patientrefusal (14%). Of note is one patient who developed an MDSnearly 3½ years after study entry. There have been previousreports of a dose–response relationship between platinum-based chemotherapy and risk of secondary leukemia in ovariancancer patients [10]; thus, clinicians should consider limitingtherapy to the fewest effective number of cycles.
Members of the GOG GYN Management Committee andone of the authors (JB) carefully reviewed all of the operativereports to determine if the extent of surgical staging wasconsistent with the GOG recommended staging procedures.This review identified an unexpectedly high number of patients(29%) in whom the staging procedure was inadequate or
by completeness of surgical staging.

Fig. 5. Treatment hazard ratios for recurrence by completeness of surgical staging.
438 J. Bell et al. / Gynecologic Oncology 102 (2006) 432–439
incompletely documented. In order to promote validity, thesepatients are included in these analyses; however, among womenwho were completely staged, the probability of remainingdisease-free for at least 5 years is 77% and the estimated benefitof 3 additional cycles of therapy is to reduce the cumulativeincidence of recurrence by 3%.
This group of patients with early stage EOC appears to havea fairly similar risk of recurrence regardless of the type ofadjuvant therapy received. In the GOG experience, the expectedprobability of remaining disease-free for at least 5 years in thispatient population is about 78–80% after either 12 cycles ofmelphalan or intraperitoneal phosphorus-32 [1], 79% after 3cycles of cisplatin/cyclophosphamide [2], and 75–80% follow-ing carboplatin/paclitaxel in this trial. The Norwegian RadiumHospital experience with stage I patients demonstrated a 5-yearrecurrence-free survival rate of 79% with 6 cycles of cisplatinand 82% with phosphorus-32 [11]. An Italian cooperative grouptrial with stage IC patients reported very similar progression-free survival of 85% after 6 cycles of cisplatin [3]. Furthermore,among oncologists treating this disease, there is no universallypreferred platinum-based therapy. This is evident in a report oftwo randomized trials comparing any combination of platinum-based chemotherapy versus observation for high risk, earlystage EOC patients. The result was a 76% 5-year disease-freesurvival for stage IA–IIA patients who received adjuvantchemotherapy [12].
Seemingly, some percent of patients with early EOC,perhaps 15–30%, has cancer resistant to various forms ofadjuvant cytotoxic therapy. If the population of high risk earlyEOC patients includes a fairly constant subset of chemotherapy-resistant subjects, then an important question arises: doeswithholding postoperative chemotherapy until recurrence ofdisease result in acceptable overall survival while sparingtoxicity for the majority of these patients who may not need anychemotherapy? The European Organization for Research andTreatment of Cancer (EORTC) investigated this concept in theAdjuvant ChemoTherapy in Ovarian Neoplasm (ACTION) trialin which patients were randomized to either platinum-basedadjuvant chemotherapy (at least four cycles) or observation.Eligibility for that trial, including surgical staging criteria, wassimilar to our study. The results showed a significantimprovement in 5-year recurrence-free survival among patientsreceiving adjuvant treatment after surgery (76% versus 68%,p=0.02), but a non-significant difference in overall survival(85% versus 78%, p=0.10). Interestingly, the extent of surgical
staging may have influenced the survival outcome. Patientswith suboptimal surgical staging randomized to observationexperienced significantly worse recurrence-free survival (78%versus 65%, p=0.009) and overall survival (84% versus 75%,p=0.03) compared to patients receiving adjuvant chemother-apy. On the other hand, among patients with optimal surgicalstaging, there was no difference in recurrence-free survival(83% versus 80%) or overall survival (87% versus 89%)regardless of treatment arm. However, since only 34% ofpatients underwent optimal staging surgery, the number may betoo small to draw a definitive conclusion [13].
The fact that many patients who enrolled in the current trialunderwent incomplete surgical staging raises some concerns.Although the rate of cancer recurrence for incompletely stagedpatients was similar to the rate for those with complete staging,the design of this trial does not allow any definitive conclusionsregarding the efficacy of 3 versus 6 cycles of chemotherapywithin the subgroups of completely or incompletely stagedpatients. Thorough surgical staging has been a dictum forgynecologic oncologists since the inception of the subspecialty.Surgical staging is important for interpreting study results andfor deciding whether adjuvant therapy is needed. For example,randomized trials have shown no benefit of adjuvant therapy forlow risk stage I patients who have been surgically staged [1].Conversely, retrospective data indicate that withholding adju-vant treatment for patients with low risk gross stage I cancersnot surgically staged results in a significantly higher rate ofcancer recurrence compared to patients who have surgicallydocumented stage I disease [14]. With respect to high risk stageI patients, the ACTION trial suggests that the group of patientswho have had complete surgical staging may have an option ofdelaying chemotherapy until cancer recurrence without sig-nificantly compromising their survival [13]. Furthermore, non-randomized trials seem to indicate that the extent of surgicalstaging itself might have prognostic significance [15]. If theoncologist elects to offer stage I–II patients adjuvant platinum–paclitaxel treatment, the current trial suggests that 3 cycles ofchemotherapy for surgically staged patients is reasonabletreatment based on consideration of both toxicity and relativerecurrence rates. Gynecologic oncologists should continue toemploy thorough surgical staging as the standard of care since itcan identify a subset of patients who do not require furthertherapy.
In conclusion, following complete surgical staging, 3 cyclesof carboplatin and paclitaxel is a reasonable treatment for

439J. Bell et al. / Gynecologic Oncology 102 (2006) 432–439
women with high risk early stage epithelial ovarian cancer.Three additional cycles of carboplatin–paclitaxel chemotherapyare, at best, likely to provide only a modest reduction in theabsolute risk of recurrence yet are associated with increasedtoxicity. The risk of recurrent cancer in this patient populationseems to have remained relatively unchanged over the years,such that the door remains open for innovative research usingcombination chemotherapy, biological modifiers, and moleculartargeting. The GOG is currently investigating three cycles ofadjuvant carboplatin and paclitaxel followed by either weeklypaclitaxel for 6 months or observation in a trial designed tomeasure the impact of low dose paclitaxel as a potentialbiological modifier (GOG 175).
Acknowledgments
This study was supported by National Cancer Institutegrants to the Gynecologic Oncology Group AdministrativeOffice (CA 27469) and the Gynecologic Oncology GroupStatistical and Data Center (CA 37517). The following GOGmember institutions participated in this study: University ofAlabama at Birmingham, Duke University Medical Center,Abington Memorial Hospital, Walter Reed Army MedicalCenter, Wayne State University, University of MinnesotaMedical School, University of Mississippi Medical Center,Colorado Gynecologic Oncology Group, P.C., University ofCalifornia at Los Angeles, University of Washington, Uni-versity of Pennsylvania Cancer Center, Milton S. HersheyMedical Center, University of Cincinnati, University of NorthCarolina School of Medicine, University of Iowa Hospitals andClinics, University of Texas Southwestern Medical Center atDallas, Indiana University Medical Center, Wake ForestUniversity School of Medicine, Albany Medical College,University of California Medical Center at Irvine, Tufts-NewEngland Medical Center, Rush-Presbyterian-St. Luke's Med-ical Center, SUNY Downstate Medical Center, University ofKentucky, The Cleveland Clinic Foundation, State Universityof New York at Stony Brook, Washington University School ofMedicine, Cooper Hospital/University Medical Center, Colum-bus Cancer Council, University of Massachusetts MedicalCenter, Fox Chase Cancer Center, Medical University of SouthCarolina, Women's Cancer Center, University of Oklahoma,University of Virginia, University of Chicago, Tacoma GeneralHospital, Thomas Jefferson University Hospital, Mayo Clinic,Case Western Reserve University, Tampa Bay Cancer Con-sortium, North Shore University Hospital, and BrookviewResearch Inc.
The authors gratefully acknowledge Caron Modeas forassistance in the preparation and editing of the manuscript.
References
[1] Young RC, Walton LA, Ellenberg SS, et al. Adjuvant therapy in stage I andstage II epithelial ovarian cancer. N Engl J Med 1990;322:1021–7.
[2] Young RC, Brady MF, Nieberg RM, et al. Adjuvant treatment for earlyovarian cancer: a randomized phase III trial of intraperitoneal 32P orintravenous cyclophosphamide and cisplatin—A Gynecologic OncologyGroup study. J Clin Oncol 2003;21(23):4350–5.
[3] Bolis G, Colombo N, Pecorelli S, et al. Adjuvant treatment for earlyepithelial ovarian cancer: results of two randomized clinical trialscomparing cisplatin to no further treatment or chromic phosphate (32P).GICOG: Gruppo Interregionale Collaborativo in Ginecologia Oncologica.Ann Oncol 1995;6(9):887–93.
[4] McGuire WP, Hoskins WJ, Brady MF, et al. Cyclophosphamide andcisplatin compared with paclitaxel and cisplatin in patients with stage IIIand stage IV ovarian cancer. N Engl J Med 1996;334(1):1–6.
[5] Alberts DS, Green S, Hannigan EV, et al. Improved therapeutic index ofcarboplatin plus cyclophosphamide versus cisplatin plus cyclophospha-mide: final report by the Southwest Oncology Group of a phase IIIrandomized trial in stages III and IVovarian cancer. J Clin Oncol 1992;10(5):683–5.
[6] Bertelsen K, Grenman S, Rustin GJ. How long should first-linechemotherapy continue? Ann Oncol 1999;10(Suppl 1):17–20.
[7] Blessing JA. Design, analysis and interpretation of chemotherapy trials ingynecology cancer. In: Deppe G, editor. Chemotherapy of GynecologyCancer. 2nd Ed. New York, NY: Alan R Liss Inc.; 1990. p. 63–97.
[8] Lachlin JM, Foulkes MA. Evaluation of sample size and power foranalyses of survival with allowance for non-uniform patient entry, losses tofollow-up, noncompliance and stratification. Biometrics 1986;42:507–19.
[9] Pepe MS, Mori M. Kaplan–Meier, marginal or conditional probabilitycurves in summarizing cometing risks failure time data? Stats Med 1993;12:737–51.
[10] Travis LB, Holowaty EJ, Bergfeldt K, et al. Risk of leukemia afterplatinum-based chemotherapy for ovarian cancer. N Engl J Med 1999;340(5):351–7.
[11] Vergote IB, Vergote-De Vos LN, Abeler VM, et al. Randomized trialcomparing cisplatin with radioactive phosphorus or whole-abdomenirradiation as adjuvant treatment of ovarian cancer. Cancer 1992;69(3):741–9.
[12] Trimbos JB, Parmar M, Vergote I, et al. International collaborativeovarian neoplasm trial 1 and adjuvant chemotherapy in ovarianneoplasm trial: two parallel randomized phase III trials of adjuvantchemotherapy in early-stage ovarian carcinoma. J Natl Cancer Inst2003;95(2):105–12.
[13] Trimbos JB, Vergote I, Bolis G, et al. Impact of adjuvant chemotherapy andsurgical staging in early-stage ovarian carcinoma: European Organisationfor Research and Treatment of Cancer—adjuvant chemotherapy in ovarianneoplasm trial. J Natl Cancer Inst 2003;95:113–25.
[14] Le T, Adolph A, Krepart GV, Lotocki R, Heywood MS. The benefits ofcomprehensive surgical staging in the management of early-stage epithelialovarian carcinoma. Gynecol Oncol 2002;85:351–5.
[15] Trimbos JB. Staging of early ovarian cancer and the impact of lymph nodesampling. Int J Gynecol Cancer 2000;10(S1):8–11.