Embed Size (px)
Citation preview

VALIDITY OF DIETARY QUESTIONNAIRES IN SRI LANKAN ADULTS AND THE ASSOCIATION OF
DIETARY INTAKE WITH OBESITY
Ranil Jayawardena Mallika Arachchige
MBBS (Colombo), HND (UK), MSc (Glasgow)
Submitted in fulfilment of the requirements for the degree of
Doctor of Philosophy
Institute of Health and Biomedical Innovation
School of Exercise and Nutrition Sciences,
Faculty of Health,
Queensland University of Technology
April 2013


Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity i
Keywords
Body Weight Perception, Diabetes, Diet, Dietary Diversity, Food Frequency
Questionnaire, Non-Communicable Diseases, Nutrition, Obesity, Sri Lanka.
ii Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
Abstract
Traditionally, infectious diseases and under-nutrition have been considered major
health problems in Sri Lanka with little attention paid to obesity and associated non-
communicable diseases (NCDs). However, the recent Sri Lanka Diabetes and
Cardiovascular Study (SLDCS) reported the epidemic level of obesity, diabetes and
metabolic syndrome. Moreover, obesity-associated NCDs is the leading cause of
death in Sri Lanka and there is an exponential increase in hospitalization due to
NCDs adversely affecting the development of the country. Despite Sri Lanka having
a very high prevalence of NCDs and associated mortality, little is known about the
causative factors for this burden. It is widely believed that the global NCD epidemic
is associated with recent lifestyle changes, especially dietary factors. In the absence
of sufficient data on dietary habits in Sri Lanka, successful interventions to manage
these serious health issues would not be possible. In view of the current situation the
dietary survey was undertaken to assess the intakes of energy, macro-nutrients and
selected other nutrients with respect to socio demographic characteristics and the
nutritional status of Sri Lankan adults especially focusing on obesity. Another aim of
this study was to develop and validate a culturally specific food frequency
questionnaire (FFQ) to assess dietary risk factors of NCDs in Sri Lankan adults.
Data were collected from a subset of the national SLDCS using a multi-stage,
stratified, random sampling procedure (n=500). However, data collection in the
SLDCS was affected by the prevailing civil war which resulted in no data being
collected from Northern and Eastern provinces. To obtain a nationally representative
sample, additional subjects (n=100) were later recruited from the two provinces
using similar selection criteria. Ethical Approval for this study was obtained from the
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity iii
Ethical Review Committee, Faculty of Medicine, University of Colombo, Sri Lanka
and informed consent was obtained from the subjects before data were collected.
Dietary data were obtained using the 24-h Dietary Recall (24HDR) method. Subjects
were asked to recall all foods and beverages, consumed over the previous 24-hour
period. Respondents were probed for the types of foods and food preparation
methods. For the FFQ validation study, a 7-day weight diet record (7-d WDR) was
used as the reference method. All foods recorded in the 24 HDR were converted into
grams and then intake of energy and nutrients were analysed using NutriSurvey 2007
(EBISpro, Germany) which was modified for Sri Lankan food recipes. Socio-
demographic details and body weight perception were collected from interviewer-
administrated questionnaire. BMI was calculated and overweight (BMI ≥23 kg.m-2),
obesity (BMI ≥25 kg.m-2) and abdominal obesity (Men: WC ≥ 90 cm; Women: WC
≥ 80 cm) were categorized according to Asia-pacific anthropometric cut-offs. The
SPSS v. 16 for Windows and Minitab v10 were used for statistical analysis purposes.
From a total of 600 eligible subjects, 491 (81.8%) participated of whom 34.5%
(n=169) were males. Subjects were well distributed among different socio-economic
parameters. A total of 312 different food items were recorded and nutritionists
grouped similar food items which resulted in a total of 178 items. After performing
step-wise multiple regression, 93 foods explained 90% of the variance for total
energy intake, carbohydrates, protein, total fat and dietary fibre. Finally, 90 food
items and 12 photographs were selected. Seventy-seven subjects completed
(response rate = 65%) the FFQ and 7-day WDR. Estimated mean energy intake (SD)
from FFQ (1794±398 kcal) and 7DWR (1698±333 kcal, P<0.001) was significantly
different due to a significant overestimation of carbohydrate (~10 g/d, P<0.001) and
to some extent fat (~5 g/d, NS). Significant positive correlations were found between

iv Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
the FFQ and 7DWR for energy (r = 0.39), carbohydrate (r = 0.47), protein (r = 0.26),
fat (r =0.17) and dietary fiber (r = 0.32). Bland-Altman graphs indicated fairly good
agreement between methods with no relationship between bias and average intake of
each nutrient examined.
The findings from the nutrition survey showed on average, Sri Lankan adults
consumed over 14 portions of starch/d; moreover, males consumed 5 more portions
of cereal than females. Sri Lankan adults consumed on average 3.56 portions of
added sugars/d. Moreover, mean daily intake of fruit (0.43) and vegetable (1.73)
portions was well below minimum dietary recommendations (fruits 2 portions/d;
vegetables 3 portions/d). The total fruit and vegetable intake was 2.16 portions/d.
Daily consumption of meat or alternatives was 1.75 portions and the sum of meat
and pulses was 2.78 portions/d. Starchy foods were consumed by all participants and
over 88% met the minimum daily recommendations. Importantly, nearly 70% of
adults exceeded the maximum daily recommendation for starch (11portions/d) and a
considerable proportion consumed larger numbers of starch servings daily,
particularly men. More than 12% of men consumed over 25 starch servings/d. In
contrast to their starch consumption, participants reported very low intakes of other
food groups. Only 11.6%, 2.1% and 3.5% of adults consumed the minimum daily
recommended servings of vegetables, fruits, and fruits and vegetables combined,
respectively. Six out of ten adult Sri Lankans sampled did not consume any fruits.
Milk and dairy consumption was extremely low; over a third of the population did
not consume any dairy products and less than 1% of adults consumed 2 portions of
dairy/d. A quarter of Sri Lankans did not report consumption of meat and pulses.
Regarding protein consumption, 36.2% attained the minimum Sri Lankan
recommendation for protein; and significantly more men than women achieved the
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity v
recommendation of ≥3 servings of meat or alternatives daily (men 42.6%, women
32.8%; P<0.05).
Over 70% of energy was derived from carbohydrates (Male:72.8±6.4%,
Female:73.9±6.7%), followed by fat (Male:19.9±6.1%, Female:18.5±5.7%) and
proteins (Male:10.6±2.1%, Female:10.9±5.6%). The average intake of dietary fiber
was 21.3 g/day and 16.3 g/day for males and females, respectively. There was a
significant difference in nutritional intake related to ethnicities, areas of residence,
education levels and BMI categories. Similarly, dietary diversity was significantly
associated with several socio-economic parameters among Sri Lankan adults. Adults
with BMI ≥25 kg.m-2 and abdominally obese Sri Lankan adults had the highest diet
diversity values.
Age-adjusted prevalence (95% confidence interval) of overweight, obesity, and
abdominal obesity among Sri Lankan adults were 17.1% (13.8-20.7), 28.8% (24.8-
33.1), and 30.8% (26.8-35.2), respectively. Men, compared with women, were less
overweight, 14.2% (9.4-20.5) versus 18.5% (14.4-23.3), P = 0.03, less obese, 21.0%
(14.9-27.7) versus 32.7% (27.6-38.2), P < .05; and less abdominally obese, 11.9%
(7.4-17.8) versus 40.6% (35.1-46.2), P < .05. Although, prevalence of obesity has
reached to epidemic level body weight misperception was common among Sri
Lankan adults. Two-thirds of overweight males and 44.7% of females considered
themselves as in “about right weight”. Over one third of both male and female obese
subjects perceived themselves as “about right weight” or “underweight”. Nearly 32%
of centrally obese men and women perceived that their waist circumference is about
right. People who perceived overweight or very overweight (n = 154) only 63.6%
tried to lose their body weight (n = 98), and quarter of adults seek advices from
professionals (n = 39).

vi Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
A number of important conclusions can be drawn from this research project. Firstly,
the newly developed FFQ is an acceptable tool for assessing the nutrient intake of Sri
Lankans and will assist proper categorization of individuals by dietary exposure.
Secondly, a substantial proportion of the Sri Lankan population does not consume a
varied and balanced diet, which is suggestive of a close association between the
nutrition-related NCDs in the country and unhealthy eating habits. Moreover, dietary
diversity is positively associated with several socio-demographic characteristics and
obesity among Sri Lankan adults. Lastly, although obesity is a major health issue
among Sri Lankan adults, body weight misperception was common among
underweight, healthy weight, overweight, and obese adults in Sri Lanka. Over 2/3 of
overweight and 1/3 of obese Sri Lankan adults believe that they are in “right weight”
or “under-weight” categories.
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity vii
THE FOLLOWING PAPERS HAVE BEEN PUBLISHED DURING MY CANDIDATURE
Publications included in the thesis
1. R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills (2012). Food
consumption of Sri Lankan adults: an appraisal of serving characteristics
Public Health Nutrition: 16 (4): 653-658.
2. R Jayawardena, P Ranasinghe, NM Byrne, MJ Soares, P Katulanda, AP
Hills (2012). Prevalence and trends of the diabetes epidemic in South Asia: a
systematic review and meta-analysis. BMC Public Health 12: 380.
3. R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills (2012).
Development of a food frequently questionnaire for Sri Lankan adults.
Nutrition Journal 11: 63.
4. R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills (2012). The
obesity epidemic in Sri Lanka Revisited. Asia Pac J Public Health. doi:
10.1177/1010539512464650. 2012 Nov 27. [Epub ahead of print].
5. R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills (2013). High
dietary diversity is associated with obesity in Sri Lankan adults. BMC Public
Health 13: 314.
6. R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. Body weight
perception and weight losing practices in Sri Lankan adults. Obesity Research
and Clinical Practice (DOI: 10.1016/j.orcp.2013.05.003).
7. R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. Prevalence,
Trends and Associated Socio-Economic Factors of Obesity in South Asia.
Obesity Facts (in press).
viii Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
8. R Jayawardena, SN Thennakoon, NM Byrne, MJ Soares, P Katulanda, AP
Hills. Energy and Nutrient Intakes among Sri Lankan Adults. BMC Research
Notes (in press).
9. R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. Validation
of Food Frequency Questionnaire for Sri Lankan adults. Nutrition Journal
(Under review).
Relevant publications (with QUT affiliation) not included in the thesis
2012
1. R Jayawardena, P Ranasinghe, P Galappatty, RLDK Malkanthi, GR
Constantine and Prasad Katulanda (2012) Effects of Zinc supplementation on
Diabetes Mellitus: a systematic review and meta-analysis. Diabetology &
Metabolic Syndrome 4:13 (doi:10.1186/1758-5996-4-13)
2. P Ranasinghe, R Jayawardana, N de Vas Gunawardana, P Katulanda.
(2012) Efficacy and safety of ‘True’ cinnamon (Cinnamomum zeylanicum)
as a pharmaceutical agent in diabetes: a systematic review and meta-analysis.
Diabetes Medicine 2012 DOI: 10.1111/j.1464-5491.2012.03718.x
3. P Katulanda, P Ranasinghe, R Jayawardena, MHR Sheriff, DR Matthews.
(2012) The prevalence, patterns and correlates of diabetic peripheral
neuropathy in Sri Lanka. Diabetology & Metabolic Syndrome 4:21
4. P Katulanda, P. Ranasinghe, R Jayawardena, MHR Sheriff, DR Matthews.
(2012) Metabolic Syndrome among adults from a developing country:
Prevalence, patterns and correlates. Diabetology & Metabolic Syndrome
2012, 4:24
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity ix
5. P Ranasinghe, R Jayawardena, P Katulanda. (2012) Diabetes Mellitus in
South Asia: a scientific evaluation of the research output. Journal of Diabetes
DOI: 10.1111/jdb.12003
6. P Katulanda, R Jayawardena, P Ranasinghe, MHR Sheriff, DR Matthews.
(2012) Physical activity patterns and correlates among Sri Lankan adults: the
Sri Lanka Diabetes and Cardiovascular Study. Public Health Nutrition, 2012,
Firstview 1-9
7. P Ranasinghe, R Jayawardena, P Katulanda. (2012) Sri Lanka in the global
map of medical research: a scientific analysis of the Sri Lankan research
output during 2000-2009. BMC Research Notes 5:121
2013
8. R Jayawardana, P Ranasinghe, MHR Sheriff, DR Matthews, P Katulanda.
(2013) Waist to height ratio: a better anthropometric predictor of diabetes and
cardio-metabolic risk factors in Sri Lankan adults. Diabetes Research and
Clinical Practice 99 292–299.
9. P Ranasinghe, R Jayawardana, N de Vas Gunawardana, P Katulanda.
(2013) Re Response to Akilen et al. Efficacy and safety of ‘true’ cinnamon
(Cinnamomum zeylanicum) as a pharmaceutical agent in diabetes: a
systematic review and meta-analysis Diabet Med. 2013 Jan 28. doi:
10.1111/dme.12141. [Epub ahead of print]
10. P Ranasinghe, R Jayawardena, ASAD Pigera, P Katulanda, GR
Constantine, P Galappaththy. Zinc supplementation in pre-diabetes: study
protocol for a randomized, double-blind, placebo-controlled clinical trial.
Trials 2013, 14:52

x Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
11. P Ranasinghe, R Jayawardena, P Katulanda. The growing epidemic of
Diabetes Mellitus in Sri Lanka: facts, figures and reality. BMC Research
Notes (Under review)
12. AK Pathirana, NC Lokunarangoda, I Ranathunga, R Ekananyaka, WS
Santharaja, R Jayawardena. Prevalence of malnutrition among cardiac
patients in a developing country. Journal of Human Nutrition and Dietetics
(Under review)
13. Anidu K Pathirana, Ranil Jayawardena, Ishara Ranathunga, Sandamali P
Premaratne, W S Santharaj and Niroshan C Lokunarangoda. Is malnutrition
worsening during hospitalization? BMC Research Notes (Under review)
14. R Jayawardena, NC Lokunarangoda, I Ranathunga, WS Santharaj, AO
Walawwatta and AK Pathirana. Predicting clinical outcome of cardiac
patients by six malnutrition screening tools. Nutrition Journal (Under review)
15. R Jayasuria, J Pinidiyapathirage, R Wickremasinghe, R Jayawardena, P de
Zoysa, A Kasturiratne. Translational Research for Diabetes self management
in Sri Lanka. The Diabetic Educator (Under review)
16. C Ranasinghe, P Ranasinghe, R Jayawardena, A Misra. Physical activity
patterns among South-Asian adults: a Systematic Review. IJBNPA (Under
review)
17. P Katulanda, P Ranasinghe, R Jayawardena, MHR Sheriff, DR Matthews
The prevalence, patterns and predictors of hypertension in Sri Lanka: a cross-
sectional population based national survey. Hypertension (Under review)
18. C Ranasinghe, P Ranasinghe, R Jayawardena, MHR Sheriff, DR Matthews
P Katulanda. Evaluation of physical activity among adults with diabetes

Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xi
mellitus from Sri Lanka. The Journal of Diabetes and Metabolic Disorders.
(Under review)
19. KM Rathnayake, A Satchithananthan, S Mahamithawa, R Jayawardena.
Early life predictors of preschool overweight and obesity: a case-control
study in Sri Lanka. BMC Public Health (Under review)
Conference publications during my candidature
2010
• Jayawardana MAR, Hills AP, Soares MJ, Katulanda P. Development and
validation of a food frequency questionnaire (FFQ) for Sri Lankan adults.
IHBI inspires 2010, Gold Coast, 25-26 Nov, 2010, pg 91
• Jayawardana MAR, Hills AP, Soares MJ, Katulanda P. Obesity in South
Asia: A review. IHBI Inspires 2010, Gold Coast, 25-26 Nov, 2010, pg 92
2011
• R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. Prevalence
and associated socio-economic factors of obesity and overweight in South
Asian countries; The 7th Asia Pacific Conference on Clinical Nutrition (7th
APCCN 2011) 5-8 June 2011 in Bangkok, Thailand (406)
• RLDK Malkanthi, MSF Shakira, KDRR Silva, R Jayawardena and KPB
Herath. Association of Serum Zinc level and percentage of body fat in
healthy adults: a case control study; The 7th Asia Pacific Conference on
Clinical Nutrition (7th APCCN 2011) 5-9 June 2011 in Bangkok, Thailand
(434)

xii Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
• R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. Prevalence,
trends and associated socio-economic factors of obesity in South Asia. 18th
European Congress of Obesity, 25- 28 May 2011, Istanbul, Turkey
• R Jayawardena, P Ranasighe, NM Byrne, MJ Soares, P Katulanda, AP
Hills. The association between weight perception and obesity among Sri
Lankan adults. 6th Asia-Oceania Conference on Obesity. Aug. 31 - Sept. 2,
2011 Sofitel Philippine Plaza Manila, Philippines
• R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. Prevalence
of obesity, overweight and abdominal obesity in Sri Lankan adults. 6th Asia-
Oceania Conference on Obesity. Aug. 31 - Sept. 2, 2011 Sofitel Philippine
Plaza, Manila, Philippines
• R Jayawardena, P Ranasighe, NM Byrne, MJ Soares, P Katulanda, AP
Hills. Body weight perception and weight loss practices in adults with
diabetes. World Diabetes Congress, Dec 4-8, 2011 Dubai
• P Ranasinghe, R Jayawardena, MHR Sheriff, DR Matthews, P Katulanda.
The patterns and correlates of diabetic peripheral neuropathy in Sri Lanka.
World Diabetes Congress, Dec 4-8, 2011 Dubai
• R Jayasuriya, MJ Pinidiyapathirage, A Kasturiratne, P Godamunne, P de
Zoysa, R Jayawardana, J Perera, S Siyambalapitiya, AR Wickremasinghe.
Efficacy of a patient centred diabetes self management model in a developing
country: a randomized controlled trial World Diabetes Congress Dubai; Dec
4-8: 2011
2012
• R Jayawardena, P Ranasinghe, NM Byrne, MJ Soares, P Katulanda and AP
Hills. Prevalence and trends of the diabetes epidemic in South Asia: a
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xiii
systematic review. Annual sessions 2012; Nutrition Society of Sri Lanka; 23-
24 Jan 2012
• R Jayawardena, MSF. Shakira, NM Byrne, MJ Soares, P Katulanda and AP
Hills. The association between body weight perception and obesity among Sri
Lankan adults. Annual sessions 2012; Nutrition Society of Sri Lanka; 23-24
Jan 2012
• R Jayawardena, MSF Shakira, NM Byrne, MJ Soares, P Katulanda and AP
Hills. Fruit and vegetable intake among adults in Sri Lanka. Annual sessions
2012; Nutrition Society of Sri Lanka; 23-24 Jan 2012
• R Jayawardena, P Katulanda, NM Byrne, MJ Soares, AP Hills. Body weight
perception and weight loss practices among Sri Lankan adults. SLMA, 2012,
P.(20)
• R Jayawardena, P Katulanda, NM Byrne, MJ Soares, AP Hills. Energy and
nutrient intake - findings from a Sri Lankan adult nutrition survey. SLMA,
2012, P.(22)
• R Jayawardena, P Ranasinghe, P Katulanda, R Sheriff, DR Matthews.
Patterns and correlates of physical activity among Sri Lankan adults. SLMA,
2012, P.(23)
• P Ranasinghe, R Jayawardena, GR Constantine, R Sheriff, P Katulanda. The
prevalence, patterns and correlates of diabetic peripheral neuropathy in Sri
Lanka. SLMA, 2012, P.(25)
• R Jayawardena, P Ranasinghe, P Galappatthy, GR Constantine, P
Katulanda. Effects of zinc supplementation on diabetes mellitus: a systematic
review and meta-analysis. SLMA, 2012, P.(26)
xiv Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
• P Ranasinghe, R Jayawardena, P Katulanda, R Sheriff, DR Matthews.
Metabolic syndrome among Sri Lankan adults - prevalence, patterns and
correlates. SLMA, 2012, P.(49)
• P Ranasinghe, R Jayawardena, WRUAS Wijesundara,WMUA Wijetunga,
TAD Tilakaratne, S Subasinghe, P Katulanda. Waist-to-height ratio has the
best anthropometric association with cardio-metabolic disease among Sri
Lankan adults. SLMA, 2012, P.(49)
• P Ranasinghe, R Jayawardena, P Katulanda. Diabetes mellitus in South Asia
- a scientific evaluation of the research output. SLMA, 2012, P.(93)
• R Jayawardena, P Katulanda, MJ Soares, NM Byrne, AP Hills.
Development of a Food Frequency Questionnaire for Sri Lankan adults
SLMA, 2012, P.(125)
• P Ranasinghe, R Jayawardena, P Katulanda. Sri Lanka in global medical
research: a scientific analysis of the Sri Lankan research output. SLMA,
2012, P.(137)
• P Ranasinghe, R Jayawardena, P Galappaththy, GR Constantine, P
Katulanda. Efficacy and safety of ‘true’ cinnamon (Cinnamomum
zeylanicum) as a pharmaceutical agent in diabetes. SLMA, 2012, P.(148)
• Ranasinghe P, Jayawardana R, Constantine GR, Sheriff R, Matthews DR,
Katulanda P Prevalence and correlates of complicated Diabetes Mellitus and
associated co-morbidities among Sri Lankan adults: the Sri Lanka Diabetes
and Cardiovascular Study” at the 48th Annual meeting of the European
Association for Study of Diabetes, held in Berlin, Germany, 2012
• R Jayawardena, P Ranasinghe, P Katulanda, R Sheriff, DR Matthews.
Waist-to-height ratio has the best anthropometric association with cardio-

Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xv
metabolic disease among Sri Lankan adults. IDF-WPR and AASD
conference, Kyoto, Japan 2012
2013
• R Jayawardena, A Pathirana, N Lokunarangoda, I Ranathunga, W
Santharaj, A Walawwatta. Prevalence of Malnutrition among cardiac patients
in Sri Lanka. Annual Scientific Sessions 2013, Nutrition Society of Sri
Lanka. Feb 2-3, 2013.
• R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. Validation
of Food Frequency Questionnaire for Sri Lankan adults. Nutrition Journal
(selected to IUNS -20th International congress of nutrition, Granada, Spain)
• Jayawardana R, Ranasinghe P, Constantine GR, Sheriff R, Matthews DR,
Katulanda P. Prevalence, patterns and correlates of Diabetes Retinopathy
among Sri Lankan adults (selected to World Diabetes Congress 2013 in
Melbourne)
Awards and grants during my candidature
• Research Awards
EM Wijerama Prize- 125th anniversary international medical congress,
Sri Lanka Medical Association, 2012
Sir Nicholas Attygalle Prize - 125th anniversary international medical
congress, Sri Lanka Medical Association, 2012
• Travel Grant Awards
European Association for Study of Diabetes (EASD) travel grant 2013
– EASD Annual Conference, Barcelona, Spain (Euro 2000)
European Association for Study of Diabetes (EASD) travel grant 2012
– EASD Annual Conference, Berlin, Germany (Euro 2000)
Asian Association for Study of Diabetes (AASD) travel support 2012
– AASD Annual Conference, Kyoto, Japan (Yen 50000)
xvi Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
• Scholarships
QUT Tuition Fee Waiver Scholarship, Queensland University of
Technology, Australia
QUT Postgraduate Award (QUTPRA), Faculty of Health, Queensland
University of Technology, Australia
IHBI Top Up Scholarship 2011, Queensland University of
Technology, Australia
• International competitive fellowships
EASD scholarship to follow Scientist Training Course in University
of Heidelberg, Germany, 2011
SEAMEO scholarship to follow Public Health And Community
Nutrition System And Analysis: University of Indonesia, Jakarta
Chronic Disease Control (CCDC) and the Public Health Foundation
of India (PHFI) scholarship to follow “Cardiovascular Disease
Epidemiology and Physical Activity Research Methods Course”
InfoSys campus, Mysore, India
Full scholarship to follow short course in Prevention Strategies for
Non-Communicable Diseases (15-20 July 2012) in University of
Oxford, UK
SJRI fellowship to follow Heath Research Methodology course, St’
John’s Medical College & Research Institute, Bangalore, India. 2012
IUNS-KNS - Capacity and Leadership Development in Nutritional
Sciences. Seoul National University, Republic of Korea. 14-16th Nov
2012. (country representation)
International Course in Nutrition Research Methods Sponsored by the
Bangalore Boston Nutrition Collaborative, St John’s Research
Institute, Bangalore. 21st Jan -1st Feb 2013.
Scholarly activities undertaken:
Training and workshop
2010
• The required unit AIRS [IFN001] has been completed.

Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xvii
• Followed UQ Sport's ISAK Level 1 Anthropometry Course 1st Oct- 3rd Oct-
2010 and Obtained full ISAK (level 1) accreditation as an anthropometrist
2011
• Cardiovascular Disease Epidemiology and Physical Activity Research
Methods Course, Mysore, India, 18-24 May 2011
• Public Health And Community Nutrition System And Analysis: SEAMEO
RECFON University of Indonesia, Jakarta: October 31 – November 14, 2011
• EASD Scientist Training Course 2011, University Hospital Heidelberg,
Germany: October 9-15, 2011
2012
• Prevention Strategies for Non-Communicable Diseases. University of
Oxford, UK, 15 - 20 July 2012
• Health Research Methodology, St’ John’s Medical College and Research
Institution, Bangalore, India. 3-15th Sep 2012
• IUNS-KNS - Capacity and Leadership Development in Nutritional Sciences.
Seoul National University, Republic of Korea. 14-16th Nov 2012.
• International Course in Nutrition Research Methods Sponsored by the
Bangalore Boston Nutrition Collaborative, St’ John’s Medical College and
Research Institution, Bangalore, India. 21st Feb – 1st March, 2013
2013
• 1st Singapore Clinical Nutrition Meeting, Grand Copthorne Waterfront,
Singapore. 6-7th April, 2013.
Conferences
• IHBI inspires 2010, Gold Coast, Australia; 25th-26th November 2010
xviii Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
• 7th Asia Pacific Conference on Clinical Nutrition, 5th-8th June, 2011
Bangkok, Thailand
• Annual Scientific Sessions 2012, Nutrition Society of SL, Jan 23-24th, 2012
• 125th Anniversary International Medical Congress, Colombo, Sri Lanka, 2-6th
July 2012
• 48th Annual Meeting of the European Association for the Study of Diabetes,
Berlin, Germany. 1-5th October 2012
• The 44th APACPH conference 2012, Colombo, Sri Lanka, 14-17th October
• 9th IDF-WPR Congress and 4th AASD Scientific Meeting, Kyoto, Japan,
Nov 24-27, 2012
• Annual Scientific Sessions 2013, Nutrition Society of Sri Lanka, Feb 2-3rd,
February 2013
• IUNS -20th International congress of nutrition, Granada, Spain, Sep. 15-20
(registered)
• 49th Annual Meeting of the European Association for the Study of Diabetes,
Barcelona. Spain. Sep 23-27th (registered)
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xix
Table of Contents
Keywords .................................................................................................................................................i
Abstract .................................................................................................................................................. ii
The following papers have been published during my candidature ..................................................... vii Publications included in the thesis ............................................................................................ vii Relevant publications (with QUT affiliation) not included in the thesis .................................. viii Awards and grants during my candidature ................................................................................. xv Scholarly activities undertaken: ................................................................................................ xvi Conferences ............................................................................................................................ xvii
Table of Contents ................................................................................................................................. xix
List of Figures .................................................................................................................................... xxii
List of Tables .................................................................................................................................... xxiii
List of Abbreviations ........................................................................................................................... xxv Statement of Original Authorship ...................................................................................................... xxvi
Acknowledgements .......................................................................................................................... xxvii
Dedication .......................................................................................................................................... xxix
CHAPTER 1: INTRODUCTION ....................................................................................................... 1 Background ............................................................................................................................................. 1
Aims and objectives ................................................................................................................................ 6 Thesis orientation .................................................................................................................................... 7
Significance of the thesis......................................................................................................................... 9
Reference list ......................................................................................................................................... 12
CHAPTER 2: MANUSCRIPT 1 ....................................................................................................... 14 Title page............................................................................................................................................... 15 Abstract ................................................................................................................................................. 16
Background ........................................................................................................................................... 17
Methods ................................................................................................................................................. 19
Results ................................................................................................................................................... 21
Discussion ............................................................................................................................................. 26
Conclusions ........................................................................................................................................... 30 References ............................................................................................................................................. 31
CHAPTER 3: MANUSCRIPT 2 ....................................................................................................... 47 Title page............................................................................................................................................... 48
Summary ............................................................................................................................................... 49
Introduction ........................................................................................................................................... 50
Methods ................................................................................................................................................. 51 Results ................................................................................................................................................... 52
Discussion ............................................................................................................................................. 55
Limitations ............................................................................................................................................ 59

xx Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
Conclusion ............................................................................................................................................ 60
References ............................................................................................................................................. 61
CHAPTER 4: MANUSCRIPT 3 ....................................................................................................... 69 Title page .............................................................................................................................................. 70
Abstract ................................................................................................................................................. 71
Introduction ........................................................................................................................................... 72
Methodology ......................................................................................................................................... 72
Results ................................................................................................................................................... 77 Discussion ............................................................................................................................................. 78
Conclusion ............................................................................................................................................ 81
Reference list ........................................................................................................................................ 83
Supplementary Materials, Part 1 ........................................................................................................... 89
Supplementary Materials, Part 2 ........................................................................................................... 96
CHAPTER 5: MANUSCRIPT 4 ....................................................................................................... 97 Title page .............................................................................................................................................. 98
Abstract ................................................................................................................................................. 99
Introduction ......................................................................................................................................... 100
Methods .............................................................................................................................................. 101
Results and Discussion ........................................................................................................................ 104
Conclusion .......................................................................................................................................... 108 Reference list ...................................................................................................................................... 109
CHAPTER 6: MANUSCRIPT 5 ..................................................................................................... 116 Title page ............................................................................................................................................ 117
Abstract ............................................................................................................................................... 118
Introduction ......................................................................................................................................... 119 Methodology ....................................................................................................................................... 120
Results ................................................................................................................................................. 123
Discussion ........................................................................................................................................... 126
Reference list ...................................................................................................................................... 131
CHAPTER 7: MANUSCRIPT 6 AND 7 ......................................................................................... 142 Chapter 7a: Manuscript 6 .................................................................................................................... 143 Chapter 7b: Manuscript 7 .................................................................................................................... 147
Title page ............................................................................................................................................ 148
Abstract ............................................................................................................................................... 149
Introduction ......................................................................................................................................... 150
Methodology ....................................................................................................................................... 151
Results ................................................................................................................................................. 154 Discussion ........................................................................................................................................... 155
Reference list ...................................................................................................................................... 160
CHAPTER 8: MANUSCRIPT 8 ..................................................................................................... 167
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xxi
Title page............................................................................................................................................. 168
Abstract ............................................................................................................................................... 169 Introduction ......................................................................................................................................... 170
Material and Methods ......................................................................................................................... 172
Results ................................................................................................................................................. 174
Discussion ........................................................................................................................................... 175
Conclusion .......................................................................................................................................... 180
References ........................................................................................................................................... 182
CHAPTER 9: MANUSCRIPT 9 ..................................................................................................... 188 Title page............................................................................................................................................. 189
Abstract ............................................................................................................................................... 190
Introduction ......................................................................................................................................... 191
Methods ............................................................................................................................................... 192
Results ................................................................................................................................................. 194 Discussion ........................................................................................................................................... 195
Conclusion .......................................................................................................................................... 197
Reference list ....................................................................................................................................... 199
CHAPTER 10: GENERAL DISCUSSION ................................................................................. 206 Comparison of different dietary assessment tools ............................................................................... 207
Nutritional issues in South Asia in relation to current diabetes epidemic ........................................... 212 Strengths of the study .......................................................................................................................... 216
Limitations of the study ...................................................................................................................... 216
Recommendations ............................................................................................................................... 218
Conclusions ......................................................................................................................................... 221
Reference list ....................................................................................................................................... 222 Appendices .......................................................................................................................................... 227
Appendix A FFQ...................................................................................................................... 227
xxii Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
List of Figures
Figure 2-1: Summarized search protocol .............................................................................................. 42
Figure 2-2: Trends in prevalence in South Asia of a) diabetes mellitus and b) pre-diabetes (Data for individual countries were extracted from the following references; Bangladesh [18]; India [35-39]; Sri Lanka [27, 40, 41]) ...................................................... 43
Figure 2-3: Diabetes epidemicity index of South Asian countries (Ban – Bangladesh; Ind – India; Mal – Maldives; Nep – Nepal; Pak – Pakistan; SL – Sri Lanka; u – urban; r – rural; u+r – urban and rural; Diabetes [ ]; Diabetes Epidemicity Index [ ]) ...................... 44
Figure 2-4: Forest plot showing pooled odds ratios for a) Family history, b) Age, c) Male gender, d) Systolic Blood Pressure, e) Diastolic Blood Pressure, f) Body Mass Index and g) Waist-Hip ratio associated with diabetes (IV-Inverse variance; SE-Standard Error) .................................................................................................................................... 46
Figure 3-1: Trends in the prevalence of obesity (BMI ≥25 kg.m-2) in Sri Lanka, Bangladesh, Nepal, India and Pakistan in adult males ............................................................................. 68
Figure 3-2: Trends in the prevalence of obesity (BMI ≥25 kg.m-2) in Sri Lanka, Bangladesh, Nepal, India and Pakistan in adult females .......................................................................... 68
Figure 4-1: Study design of the Sri Lanka Diabetes and Cardiovascular Study. .................................. 73
Figure 4-2: Map of Sri Lanka with data collection (▀) sites ................................................................. 75
Figure 4-3. Example of a disaggregated recipe showing multiple levels (Chicken Koththu) ............... 88 Figure 4-4 : A typical Sri Lankan lunch ................................................................................................ 96
Figure 5-1: Example of a food photograph (200 g of rice) ................................................................. 115
Figure 12 Percentage energy contribution from macronutrients according to gender, ethnicity and area of residance,BMI,educational level and age groups. ........................................... 141
Figure 9-1: Bland and Altman plots for energy with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of agreements in red line. ................................................................... 204
Figure 9-2: Bland and Altman plots for protein with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of agreements in red line. ................................................................... 204
Figure 9-3: Bland and Altman plots for fat with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of agreements in red line. ......................................................................................... 205
Figure 9-4: Bland and Altman plots for carbohydrates with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of agreements in red line. ................................................................... 205

Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xxiii
List of Tables
Table 1-1. Thesis orientation .................................................................................................................. 9
Table 2-1 Prevalence of diabetes and pre-diabetes in South Asian countries ....................................... 37
Table 2-2: Prevalence of diabetes according to area of residence ........................................................ 39
Table 2-3: Prevalence of diabetes in different regions .......................................................................... 41
Table 3-1: National prevalence of obesity (as percentage) in individual South Asian countries (BMI=Body mass index, WC=waist circumference) ........................................................... 65
Table 3-2: Socio-economic factors associated with the prevalence of obesity in the South Asian region. .................................................................................................................................. 67
Table 4-1: Demographic characteristics and BMI characteristics of the sample ................................... 85
Table 4-2: Average dietary intake of servings from different food group by Sri Lankan adults ........... 86
Table 4-3: Comparison of food intake of Sri Lankan adults with national and international recommendations. ................................................................................................................ 86
Table 4-4: Percentage distribution of the study sample according to their consumed foods portions from different food groups ..................................................................................... 87
Table 5-1: Demographic characteristics of the sample of the study population .................................. 112
Table 5-2: Nutrient intake of the study population.............................................................................. 113
Table 5-3: Elements of the food frequency questionnaire ................................................................... 114
Table 6-1: Socio-demographic characteristics of the survey population ............................................. 133 Table 6-2: Energy intake (kcal) of Sri Lankan adults by socio-demographic characteristics ............. 134
Table 6-3 Carbohydrate intake (g) of Sri Lankan adults by socio-demographic characteristics ......... 135
Table 6-4 Protein intake (g) of Sri Lankan adults by socio-demographic characteristics ................... 136
Table 6-5 Fat intake (g) of Sri Lankan adults by socio-demographic characteristics ......................... 137
Table 6-6 Dietary fiber intake (g) of Sri Lankan adults by socio demographic characteristics........... 138 Table 6-7 Sodium intake (mg) of Sri Lankan adults by socio-demographic characteristics ............... 139
Table 6-8: Mean Daily Micronutrient Intake by Sri Lankan Adults. .................................................. 140
Table 7-1. Mean and SD of dietary diversity score (DDS), dietary diversity score of portions (DDSP) and food variety score (FVS) ................................................................................ 163
Table 7-2 Percent consumption of different food groups by DDS for Sri Lankan adults (n=481) ..... 164
Table 7-3 Percent consumption of different food groups by DDSP for Sri Lankan adults (n=481) ............................................................................................................................... 165
Table 7-4 Mean BMI, Waist circumference and energy intake of the subjects according to DDS, DDSP and FVS. ........................................................................................................ 166
Table 8-1: Socio-demographic characteristics, BMI and abdominal obesity categories. .................... 185
Table 8-2: Awareness of body weight and height ............................................................................... 185
Table 8-3: Percentage of adults in each category of weight perception, by BMI category calculated from measured height and weight. .................................................................... 186
Table 8-4: Percentage of adults in each category of waist circumference perception, according to WC cut-offs. ................................................................................................................... 186
Table 8-5: Logistic regression model of under perception, correct perception and over perception of body weight. ................................................................................................. 187
xxiv Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
Table 9-1: Comparison of consumption of nutrients estimated by 7DWR vs. FFQ. .......................... 201
Table 9-2: Percentage of subjects correctly classified by FFQ relative to the 7DWFR ...................... 202 Table 9-3 (Supplementary): Means, Standard Deviations Pearson’s Correlation Coefficients of
Nutrient intakes Based on FFQ 2 and FFQ 1 ..................................................................... 203
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xxv
List of Abbreviations
BMI Body Mass Index CVD Cardiovascular Disease
d Day
DDS Diet Diversity Score
DDSP Dietary Diversity Score with Portions
FFQ Food Frequency Questionnaire
FVS Food Variety Score
HDL High Density Lipoproteins
IV Inverse Variance
kg kilograms
LDL Low Density Lipoproteins
m meters
NCD Non-Communicable Diseases
NHS National Health Survey
OW Overweight
OR Odd Ratio
SD Standard Deviation
SE Standard Error
SLDCS Sri Lanka Diabetes and Cardiovascular study
TAG Triglycerides
TC Total Cholesterol
WC Waist Circumference
WHO World Health Organization
xxvi Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
Statement of Original Authorship
The work contained in this thesis has not been previously submitted to meet
requirements for an award at this or any other higher education institution. To the
best of my knowledge and belief, the thesis contains no material previously
published or written by another person except where due reference is made.
Signature:
Date: 7th November 2013
Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xxvii
Acknowledgements
I greatly acknowledge the assistance I received from numerous individuals and
institutions for completing this research.
First and foremost, I would like to thank to my supervisory team, Prof. Andrew Hills,
Prof. Nuala Byrne, A/Prof. Mario Soares and Dr. Prasad Katulanda for their support,
advice, experience, and guidance throughout my candidature. I appreciate the
significant amount of time and assistance my supervisors have invested in the
development of my research and professional skills. Prof. Hills was a great mentor
and always provided me warm support and assistance over and above my
expectations. A/Prof. Soares expertise and critical perspectives were invaluable to
the development of this thesis. Dr. Katulanda provided a stimulating environment
with productive discussion through the research that helped make me a better
researcher. I am grateful to all of them for their invaluable support, wisdom and the
kind-hearted assistance extended to me during last three years.
I would like to express my gratitude to staff members of the university. I would like
to thank Queensland University of Technology for offering me a scholarship to
complete my PhD. The university has offered me many opportunities to attend and
present at seminars, trainings and conferences to further enhance my research skills
and disseminate my research findings. I must thank the Faculty of Health for
granting me the tuition fee waiver and living allowance scholarship, without which
my PhD study would not have been possible.
I would like to greatly acknowledge staff members from Diabetes Research Unit
(DRU), Faculty of Medicine, University of Colombo for support for field visits, data
collection, data analysis and data entering. I would like to thank my colleagues and
xxviii Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
friends, Katy Horner, Priyanga Ranasinghe, Fathima Shakira, Shalika Tennakoon
and Upekha Ganegoda. I would also like to thank Connie Wishart for laboratory
analyses at IHBI and Martin Reese who helped me correct the English in this
dissertation.
I would like to thank all my family for their support, especially my mother Nalini,
brother Chathura and my mother-in-law Kusum who encouraged me to travel
overseas to further my studies. I am sure they are thrilled to see the end in sight. I am
deeply grateful to my wife, Kavindya, who accepted my decisions to undertake this
PhD journey, always believes in and stands by me, and continues to bring a smile to
my face. I could not have completed this research without your help.
Additionally, I would like to thank the participants in this study for their
contribution and cooperation. Their valuable input was a major factor in
accomplishing this study.

Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity xxix
Dedication
To my loving father, who passed away one month before I started my PhD.

1
Chapter 1: Introduction
BACKGROUND
Traditionally, infectious diseases and under-nutrition have been considered major health
problems in the developing world [1] with little attention paid to obesity and associated Non-
Communicable Diseases (NCDs). In the past, obesity was regarded as a sign of wealth in
developing settings and therefore has long been viewed as desirable. However, the prevalence of
obesity and NCDs are increasing at an alarming rate worldwide [2] and an increasing body of
evidence shows that people originating from the Indian sub-continent have a high risk for NCDs
including diabetes mellitus type 2 (DM), coronary heart disease (CHD) and stroke compared to
Europeans [3]. South Asia has the highest number of diabetics worldwide and 50% of the adult
disease burden in South Asia is attributable to NCDs [4]. Developing countries, particularly Sri
Lanka, have not been spared [5]. It has been identified that recent lifestyle changes, mainly
nutritional factors, may be associated with the increasing prevalence of NCDs globally.
Therefore, it is vital to be able to quantify existing dietary habits and associated health
conditions. Because eating habits vary significantly among ethnic groups, it is not possible to
predict dietary patterns without reliable country-specific information. In the absence of sufficient
and relevant data on diet and obesity levels in South Asian countries, successful interventions to
manage diet associated NCDs would not be possible.
The increasing prevalence of obesity, diabetes and associated NCDs is a major public health
problem in South Asia. The problem is exacerbated by the ethnic susceptibility of South Asians
to NCDs, a rapidly ageing population, socioeconomic changes and the lack of resources to

2 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
intervene. Sri Lanka recorded 524 deaths per 100,000 from cardiovascular and cerebrovascular
disease, considerably higher than in many affluent countries such as the UK (427), USA (397),
Australia (308) and France (205) [6]. Ischemic heart disease (10.6%) and cerebrovascular
diseases (9.0%) are reported as the leading causes of death in Sri Lanka [7]. According to
mortality data, from 1981 to 2000, there was an exponential increase in hospitalization due to
NCDs in Sri Lanka and it was previously estimated that by 2010 there would be a 40%, 36% and
29% increase in hypertension, diabetes mellitus and ischemic heart disease, respectively [8].
Despite Sri Lanka having a very high prevalence of NCDs and associated mortality, little is
known about the causative factors for this health burden. It is widely believed that the global
NCD epidemic is associated with recent lifestyle changes, especially increased intake of calorie-
dense foods, saturated fatty acids, sugary drinks, refined carbohydrates and lower intake of fruit
and vegetables [9].
In the UK, the National Diet and Nutrition Survey (NDNS) showed a very strong association
between diet and NCDs in adults [10]. The Sri Lankan Nutrition Survey was conducted in 1975,
however the main concern at that time was under-nutrition and protein-energy malnutrition in
children [11]. STEP survey findings noted a number of risk factors associated with NCDs in an
urban province in Sri Lanka, namely smoking, physical inactivity and low fruit and vegetable
intake [12]. The authors were unable to identify specific causes for NCD risk, possibly due to a
lack of comprehensive information on dietary habits. It is believed that the high prevalence and
incidence of NCDs is associated with the Sri Lankan population’s dietary practices. This is the
first diet and nutrition survey in Sri Lanka.
In Sri Lanka, diet-related chronic diseases currently account for 18.3% of all deaths and 16.7%
of hospital expenditure [13]. Despite consensus that diet plays a major role in the epidemic of
NCDs in Sri Lanka, nutritional interventions are far beyond the scope of the current capacity in
the country. Firstly, there are very few nutrition or dietetic experts in Sri Lanka and no dietetic

3
or clinical nutrition training available in the educational system therefore advice to the
population is minimal. Secondly, Sri Lanka has never conducted a food consumption survey due
to the absence of a validated dietary assessment tool and the necessary resources, and no cross-
sectional nutritional information is currently available on dietary habits and associated NCDs in
the country [14]. In addition, the cultural and ethnic diversity of the population may also affect
lifestyle considerably.
On the other hand, dietary diversity also affects disease status. All people need a variety of foods
to meet requirements for essential nutrients, and the value of a diverse diet has long been
recognized [15]. Traditionally, dietary diversity was linked to under-nutrition. There is very
limited evidence on the association between diet diversity and NCDs [16].
Different nutritional assessment tools are commonly used for dietary surveys in many countries,
including the 7-day weighed food approach widely used in the UK [10]. However, the approach
is costly and associated with significant participant burden. On the other hand, various Food
Frequency Questionnaires (FFQs) have been widely used and are recognized as reliable and
suitable for dietary assessment at the population level [17]. The FFQ is the most common dietary
assessment tool used in large epidemiologic studies of diet and health [18]. FFQs assess energy
and/or nutrient intake by determining how frequently a person consumes a limited number (100-
150) of foods which are the main sources of nutrients or of a particular dietary component in
question [19]. Respondents indicate how many times a day, week, month, or year they usually
consume the food items [20]. In some FFQs, standard portion sizes are used but not in all. For
example, an Australian FFQ included photographs of important portion sizes [21]. The strengths
of FFQs are: 1) a modest demand on time and energy of respondents; 2) relatively easy to
administer; 3) some are self-administered and machine readable and thus are relatively
economical to use in large-scale studies [18]. The main limitations of FFQs are that they limit
food lists to 100-150 items even though free-living individuals could be consuming more than
4 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
this number [22]. Similarly, limiting portion sizes may confuse some respondents. Another
limitation is reliance on the ability of respondents to explain their diet [23]. Despite these
limitations, the FFQ has been used in the US to collect nutritional intake and is considered the
method of choice for research on diet-disease relationships [24]. However, as foods vary by
culture and region, culture- or region-specific FFQs have been developed. The culture- or
region-specific FFQ consists of a list of foods eaten commonly in a particular country or by a
particular population, each food’s commonly eaten portion size and the reported intake
frequency. The FFQ food list typically explains 80–90% of the variability in the nutrients of
interest [18].
Developing a region-specific FFQ would be particularly helpful to identify high diet-related
disease status in Sri Lankan adults and would greatly assist in planning for the conduct of a
national level cross-sectional survey in 2014-2015. Developing the food item list from a
representative population is vital. A restricted food list may not be able to capture the full
variability of the Sri Lankan diet, which includes a variety of foods, ingredients, cooking
practices and brands. In this study, as energy, macro-nutrients and selected micro-nutrients will
be measured it is crucial to establish a comprehensive food list. To ensure that data are
representative of the population for whom the FFQ will be developed, large, representative,
randomly-selected samples are needed.
Public health promotion efforts aimed at overweight and obesity prevention often proceed from
the assumption that most individuals prefer to be thin, and that the first step in motivating
individuals to lose weight and associated health risk is to raise awareness of weight status among
those who are overweight [25]. This approach may be fitting for Western populations that value
thinness in women and lean, muscular physiques in men, and educated societies where
abdominal obesity may considered as a risk factor for metabolic problems such as diabetes.
However, this assumption may not be appropriate for South Asians where body size preference
5
may differ. In most non-Western cultures it is recognized that large bodies in both males and
females are associated with wealth and health [26]. That culture influences weight perception
preference has been the rationale for many studies researching the association between weight
perception and obesity among different ethnic groups. However, many of the studies have either
focused on minority immigrant populations in affluent countries [27] or primarily adolescent age
groups [26]. Results from these two groups may not represent the association between weight
perception and obesity in adults in South Asian countries where obesity has now reached an
epidemic level.
In summary, it is evident Sri Lanka is facing a significant health burden due to diet-related
NCDs. However, large nutritional interventions are far beyond the current capacity of the
country. Sri Lanka has never conducted a food consumption survey mainly due to the absence of
a validated dietary assessment tool and resources. Therefore, there are no available cross-
sectional nutritional data on dietary habits and associated NCDs in Sri Lanka. There is a
considerable cultural and ethnic diversity which may be associated with the dietary intake of the
population. Secondly, the associations between obesity, diet and behaviour, including weight
perception, is an unexplored area of interest.
6 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
AIMS AND OBJECTIVES
To address the research questions, this research project was separated into two parts. Part 1
comprised a cross-sectional study to obtain details of dietary habits of Sri Lankan adults. In
addition to nutritional data, anthropometric and behavioural data were collected. Validating a
dietary tool necessitated a separate study sample. Part 2 therefore, investigated the validity of the
dietary questionnaire against a reference method in a representative sample.
The aims and objectives for each phase are listed below. These aims and objectives are based on
gaps in existing knowledge identified from the literature which will be discussed in the
respective chapters.
Part 1
1. To identify food consumption according to servings in Sri Lankan adults.
2. To develop a FFQ for Sri Lankan adults to measure habitual dietary intake.
3. To assess the intakes of energy, macro-nutrients and selected other nutrients with respect
to socio-demographic characteristics and the nutritional status of Sri Lankan adults
focusing on diet-related metabolic chronic disease.
4. To explore the association of diet diversity with obesity in Sri Lankan adults.
5. To assess self-perception of body weight among Sri Lankan adults.
Part 2
1. To assess the validity of a newly developed FFQ to estimate nutrient intake compared
with a reference method.
7
THESIS ORIENTATION
This program of research is presented as a Thesis by Publication (Table 1 below). Nine
manuscripts (six published, two in press, one under review) are included as components of the
chapters in this thesis. All manuscripts have been accepted in, or submitted to, international
peer-reviewed journals. Each manuscript is written in the conventional style for the journal,
including reference style and spelling. As each manuscript is designed to stand alone, there is an
inevitable degree of overlap in their Introduction, Methods and Discussion sections.
The first two chapters incorporate the literature review for this thesis. South Asia is home to
almost one quarter of the world’s population. With the rapid emergence of obesity in the region,
an increasing body of evidence suggests that people originating from the Indian sub-continent,
including Sri Lanka, have a higher risk of type 2 diabetes, coronary heart disease and stroke
compared to Europeans. In addition, the socio-economic characteristics of the South-Asian
population are distinct from those seen in developed countries. South Asia has the highest
number of diabetes cases in the world. Therefore, the following section will further review the
current literature on obesity and diabetes in the region. Chapter 2 systematically evaluates the
scientific literature on the prevalence, trends and risk factors for diabetes in the South Asian
region. Manuscript 1 has been published (and tagged as “highly accessed”) in BMC Public
Health (2012). Similarly, Chapter 3 discusses the prevalence of overweight and obesity among
the adult population from individual countries in South Asia using the most recent representative
evidence and identifies and discusses the socio-economic factors associated with obesity in the
region. Chapter 3 is based on Manuscript 2, which has been accepted for publication (in press)
in Obesity Facts.
8 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
This research work is divided into two parts. Measurement of current food habits and obesity
among Sri Lankan adults comprises part 1, and the development and validation of a food
frequency questionnaire represents part 2. Chapter 4 includes a description of study design,
details methodology and presents the results. This chapter also includes Manuscript 3, based on
part 1, which has been published in the journal, Public Health Nutrition (2012). Importantly,
Chapter 4 provides additional methodological details due to the limited ability to describe
methodology in the published manuscripts. Manuscript 4 reports on the methods used in part 2,
the FFQ. Chapter 5 subsequently presents the methodological details of the development of
Food frequency Questionnaire. Manuscript 4 has been published in the Nutrition Journal
(2012).
Chapter 6 presents the results of part 1. National diet and nutrition surveys provide valuable
information on a possible partial explanation for the health status and disease risk of the
population studied. Manuscript 5 reports on a dietary survey undertaken to assess the intakes of
energy, macronutrients and selected other nutrients with respect to socio-demographic
characteristics and nutritional status of Sri Lankan adults focusing on diet-related metabolic
chronic disease. Manuscript 5 has been accepted in BMC Research Notes and is currently in
press.
Chapter 7 provides details of current obesity level in Sri Lanka and the association with dietary
factors. This chapter includes Manuscripts 6 and 7. Prevalence of obesity among Sri Lankan
adults is reported briefly in manuscript 6. This manuscript has been published in the Asia Pacific
Journal of Public Health (2012). Manuscript 7 provides further detailed information regarding
the association of obesity and dietary diversity. This manuscript has been published (tagged as
“highly accessed”) in the BMC Public Health (2013).
Chapter 8 presents the body weight perception and weight loss practices among Sri Lankan
adults. This chapter discusses the self-perception of body weight and weight loss approaches

9
among Sri Lankan adults. Manuscript 8 has been published in Obesity Research and Clinical
Practice.
Development of the Food Frequency Questionnaire is reported in Chapter 9. Study 2 is
described in detail in this chapter including a description of the methods and presentation of
results. This chapter also includes Manuscript 9, based on the results of part 2, and has been
submitted to the Nutrition Journal.
Finally, Chapter 10 provides a synthesis of the study findings across the three manuscripts, and
discusses the study limitations, directions for future research and the public health and clinical
significance of the research findings.
Table 1-1. Thesis orientation
Section Chapters Manuscripts
Introduction 1 N/A
Literature review 2, 3 1, 2
Methods 4, 5 3, 4
Results 6, 7, 8, 9 5,6,7,8,9
Discussion 10 N/A
N/A: not applicable
SIGNIFICANCE OF THE THESIS
The research and outcomes of this thesis are located within the priority field of nutrition and
obesity. Although the research was conducted among native Sri Lankan adults, many of the
findings can be generalized to native South Asians and South Asians living in other countries
such as Australia. Their significance is summarized in the following points.
10 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
1. This study was the first to develop and validate a FFQ for Sri Lankan adults using a
nationally representative sample. Dietary assessment of this population is invaluable to
understand the role of nutrition in chronic disease so that preventive strategies can be
implemented. The main weakness of the previous national level NCD survey in Sri
Lanka was the absence of nutritional data on the population and their relationship with
the high NCD risk in the country. One of the main objectives of the current work was to
develop a FFQ to administer in the next national level NCD survey. Moreover, this FFQ
could also be used to assess dietary habits of Sri Lankans living in other countries, as
they practice similar eating patterns to native Sri Lankans.
2. Most Sri Lankan meals are mixed dishes. We described a method to translate a mixed
meal to food group categories. Food which is a mixture of several food types was
systematically disaggregated before ingredients were categorized into appropriate food
groups. Decisions were then made about the point at which to stop the disaggregation
process so that foods or their ingredients could be tabulated in the appropriate food
groups. This study provided the first national estimate of energy and nutrient intake of
the Sri Lanka adult population. It is evident that consumption of high levels of
carbohydrate, fat mainly from saturated sources, low protein, low dietary fiber and high
levels of sodium may have detrimental effects on health and be related to the current
epidemic of NCDs.
3. This thesis is the first to report on dietary habits and nutrient intake of Sri Lankans.
Excess consumption of starchy foods but inadequate intake of dairy products, fruit and
vegetables may be associated with higher prevalence of diet associated NCDs. Dietary
diversity and variety have long been recognized as key elements of high quality diets.
Moreover, this thesis reports on a positive association between high dietary diversity and

11
obesity among Sri Lankan adults. Increased dietary diversity in health promotion may
not be appropriate for combating obesity epidemic in Sri Lanka.
4. The prevalence of obesity has reached epidemic levels in many parts of the world and Sri
Lanka is no exception. During the last two decades the level of obesity has increased
substantially in Sri Lanka. We found nearly a quarter of Sri Lankan adults are obese.
Although obesity levels have reached epidemic proportions, body weight misperception
was common among Sri Lankan adults. Two-thirds of overweight males and 45% of
females considered themselves as ‘about right weight’. Over one-third of both male and
female obese subjects perceived themselves as ‘about right weight’ or ‘underweight’.
12 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
REFERENCE LIST
1. Muller, O. and M. Krawinkel, Malnutrition and health in developing countries. Canadian
Medical Association Journal, 2005. 173(3): p. 279. 2. James, P.T., et al., The worldwide obesity epidemic. Obes Res, 2001. 9 Suppl 4: p. 228S-
233S. 3. Misra, A. and L. Khurana, Obesity-related non-communicable diseases: South Asians vs
White Caucasians. International Journal of Obesity, 2010. 4. Ghaffar, A., K. Reddy, and M. Singhi, Burden of non-communicable diseases in South
Asia. British Medical Journal, 2004. 328(7443): p. 807. 5. Misra, A. and L. Khurana, Obesity and the metabolic syndrome in developing countries.
Journal of Clinical Endocrinology & Metabolism, 2008. 93(11_Supplement_1): p. s9. 6. Abeywardena, M., Dietary fats, carbohydrates and vascular disease: Sri Lankan
perspectives. Atherosclerosis, 2003. 171(2): p. 157. 7. Jayasekara, R. and T. Schultz, Health status, trends, and issues in Sri Lanka. Nursing &
Health Sciences, 2007. 9(3): p. 228-233. 8. Premaratne, R., A. Amarasinghe, and A. Wickremasinghe, Hospitalisation trends due to
selected non-communicable diseases in Sri Lanka, 2005–2010. Ceylon Medical Journal, 2005. 50(2): p. 51.
9. WHO. Diet. Global Strategy on Diet, Physical Activity & Health 2010 2010 [cited 2010 9/10]; Available from: http://www.who.int/dietphysicalactivity/diet/en/index.html.
10. Henderson, L., J. Gregory, and G. Swan, The national diet & nutrition survey: Adults aged 19 to 64 years2003: Stationery Office.
11. Brink, E.W., et al., Sri Lanka Nutrition Status Survey, 1975. International Journal of Epidemiology, 1978. 7(1): p. 41-47.
12. Somatunga, L.C., NCD Risk Factor Survey in Sri Lanka (STEP Survey), 2004, WHO. 13. Popkin B.M., H.S., Kim S.,, The Nutritional Transition and Diet-Related Chronic
Diseases in Asia: Implications for Prevention. Washington, DC: International Food Policy Research Institute FCND Discussion Paper, 2001. 105.
14. FAO, FAO-Nutrition Country Profiles, 1999, Food and Agriculture organization of the United Nations Rome.
15. Ruel, M., Operationalizing dietary diversity: a review of micronutrient issues and research priorities. J Nutr, 2003. 133: p. 3911 - 3926.
16. Kennedy, G., M. Pedro, and C. Seghieri, Dietary diversity score is a useful indicator of micronutrient intake in Non-Breast-Feeding Filipino children. J Nut, 2007. 137: p. 472 - 477.
17. Cade, J., et al., Food-frequency questionnaires: a review of their design, validation and utilisation. Nutrition research reviews, 2004. 17(01): p. 5-22.
18. Willett, W., Nutrition Epidemiology. 2 ed1998, NEW YORK: Oxford University Press. 19. Subar, A.F., et al., Improving Food Frequency Questionnaires: A Qualitative Approach
Using Cognitive Interviewing. Journal of the American Dietetic Association, 1995. 95(7): p. 781-788.
20. Block, G., Human dietary assessment: methods and issues. Preventive Medicine, 1989. 18(5): p. 653-660.
21. Victoria, C.C. Dietary questionnaires. 2010; Available from: http://www.cancervic.org.au/about-our-research/epidemiology/nutritional_assessment_services.

13
22. Iqbal, R., et al., Refinement and validation of an FFQ developed to estimate macro-and micronutrient intakes in a south Indian population. Public Health Nutrition, 2009. 12(01): p. 12-18.
23. Mullen, B., et al., Validity of a food frequency questionnaire for the determination of individual food intake. American Journal of Clinical Nutrition, 1984. 39(1): p. 136.
24. Centers for Disease Control and Prevention. NHANES III. 2010; Available from: http://www.cdc.gov/nchs/nhanes/nh3data.htm.
25. Wammes, B., et al., The impact of a national mass media campaign in The Netherlands on the prevention of weight gain. Public Health Nutrition, 2005. 8(08): p. 1250-1257.
26. Becker, A.E., S.E. Gilman, and R.A. Burwell, Changes in Prevalence of Overweight and in Body Image among Fijian Women between 1989 and 1998**. Obesity Research, 2005. 13(1): p. 110-117.
27. Brener, N.D., et al., The Association between Weight Perception and BMI among High School Students. Obesity, 2004. 12(11): p. 1866-1874.
14 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
Chapter 2: Manuscript 1
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or publisher of
journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the Australasian
Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Prevalence and trends of the diabetes epidemic in South Asia: a systematic review and meta-analysis Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Priyanga Ranasinghe Study design and data collection. Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying
authorship.
Nuala Byrne 18/04/2013
Name signature Date
15
TITLE PAGE
Prevalence and trends of the diabetes epidemic in South Asia: a systematic
review and meta-analysis
Ranil Jayawardena1,2*, Priyanga Ranasinghe2,3, Nuala M. Byrne1, Mario J. Soares4, Prasad
Katulanda2, Andrew P. Hills5
1- Institute of Health and Biomedical Innovation, Queensland University of Technology,
Brisbane, Queensland, Australia
2- Diabetes Research Unit, Department of Clinical Medicine, Faculty of Medicine, University of
Colombo, Colombo, Sri Lanka
3- Department of Pharmacology, Faculty of Medicine, University of Colombo, Colombo, Sri
Lanka
4- Curtin Health Innovation Research Institute, School of Public Health, Curtin University,
Perth, Australia
5- Mater Mothers’ Hospital, Mater Medical Research Institute and Griffith Health Institute,
Griffith University, Brisbane, Queensland, Australia.
Citation
R Jayawardena, P Ranasinghe, NM Byrne, MJ Soares, P Katulanda, AP Hills (2012) Prevalence
and trends of the diabetes epidemic in South Asia: a systematic review and meta-analysis. BMC
Public Health 12:380

16 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
ABSTRACT
Background: Diabetes mellitus has reached epidemic proportions worldwide. South Asians are
known to have an increased predisposition for diabetes which has become an important health
concern in region. We discuss the prevalence of pre-diabetes and diabetes in South Asia and
explore the differential risk factors reported.
Methods: Prevalence data was obtained by searching the Medline® database with; ‘prediabetes’
and ‘diabetes mellitus’ (MeSH major topic) and ‘Epidemology/EP’ (MeSH subheading). Search
limits were articles in English, between 01/01/1980-31/12/2010, on human adults (≥19 years).
The conjunction of the above results was narrowed down with country names.
Results: The most recent reported prevalence of pre-diabetes:diabetes in regional countries
were; Bangladesh–4.7%:8.5% (2004-2005;Rural), India–4.6%:12.5% (2007;Rural); Maldives–
3.0%:3.7% (2004;National), Nepal–19.5%:9.5% (2007;Urban), Pakistan–3.0%:7.2%
(2002;Rural), Sri Lanka–11.5%:10.3% (2005-2006;National). Urban populations demonstrated a
higher prevalence of diabetes. An increasing trend in prevalence of diabetes was observed in
urban/rural India and rural Sri Lanka. The diabetes epidemicity index decreased with increasing
prevalence of diabetes in respective countries. A high epidemicity index was seen in Sri Lanka
(2005/2006–52.8%), while for other countries, the epidemicity index was comparatively low
(rural India 2007-26.9%; urban India 2002/2005–31.3%, and urban Bangladesh–33.1%). Family
history, urban residency, age, higher BMI, sedentary lifestyle, hypertension and waist-hip ratio
were associated with an increased risks of diabetes.
Conclusion: A significant epidemic of diabetes is present in the South Asian region with a rapid
increase in prevalence over the last two decades. Hence there is a need for urgent preventive and
curative strategies .
Keywords: Diabetes Mellitus; South Asia; epidemiology; prevalence; trends; risk factors
17
BACKGROUND
Diabetes mellitus has reached epidemic proportions worldwide, placing a substantial burden on
healthcare services. Historically, diabetes was considered a disease confined to developed
countries and affluent people. However, recent estimates suggest that the prevelence of diabetes
is rising globally, particularly in developing countries [1]. South Asia, commonly known as the
Indian sub-continent, is home to almost one-quarter of the world’s population and is comprised
of many diverse ethnic, linguistic and religious groups. India, Pakistan, Bangladesh, Nepal, Sri
Lanka, Bhutan and Maldives are the countries of the region. South Asians are known to have an
increased predisposition for Type 2 diabetes [2]. In addition to the large population living in
South Asia, a significant number of immigrants from the region are living in affluent Western
nations. For example, the 2001 UK census reported that around 4.0% (2.3 million) of the
country’s total population were of South Asian origin [3]. As a consequence, a disease such as
Type 2 diabetes affecting the ethnic South Asian sub-population will have potential implications
for global health.
Diabetes mellitus has become an important health concern in the South Asian region with an
estimated increase in the prevalence of diabetes of over 151% between 2000 and 2030 [1].
Studies have consistently demonstrated that South Asians are at an increased risk of developing
diabetes in comparison to other ethnic groups [2]. In the UK, the risk of diabetes is five times
higher for immigrants from Pakistan and Bangladesh and three times higher for Indian
immigrants, with an associated increased risk of complications, morbidity and mortality
compared with the native white Caucasian population [4]. Furthermore, South Asian patients
with diabetes were younger and less obese compared to the native white Caucasians [4].
Progression of diabetes is also known to be more rapid among South Asians and Mukhopadhyay
et al. [5] reported that the decline in glycaemic control over time was much more rapid among
18 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
South Asians when compared to Europeans. Hence, it is apparent that diabetes among South
Asians represents a significant health concern with differential risk factors and a more
aggressive progression than in other ethnic groups.
Although there have been comprehensive reviews on diabetes in the Asian region [6], among
South Asians immigrants living in developed countries [7] and from individual South Asian
countries such as India [8], to date no studies have explored the prevalence and trends of the
diabetes epidemic for the region. The present study aims to discuss the prevalence of pre-
diabetes and diabetes among adults from individual countries in the South Asian region and
explore the differential factors reported to be associated with the development of diabetes in
these countries.
19
METHODS
The study was conducted in adherence to the PRISMA (Preferred Reporting Items for
Systematic Reviews and Meta-Analyse) guidelines and the PRISMA checklist is provided as a
Supplementary file (Additional File 1). Diabetes prevalence data among South Asian adults in
regional countries was obtained in a three-stage process. In the first stage a search of the online
Medline® database (Medical Literature Analysis and Retrieval System) was performed with a
combination of MeSH® (Medical Subject Headings) terms; ‘prediabetes’ and ‘diabetes mellitus’
where the MeSH major topic and ‘Epidemology/EP’ was the MeSH subheading. The search
limits were; language (‘English’), dates (between ‘1st January 1980’ and ‘31st December 2011’),
Species (‘Humans’) and age (‘all adults: 19+ years’). The conjunction of the above results were
narrowed down by adding the name of each regional country (India, Pakistan, Bangladesh, Sri
Lanka, Nepal, Bhutan and Maldives), South Asian and Indian Asians as key words. In the
second stage the total hits obtained from searching Medline® using the above search criteria were
screened by reading the ‘title’ and ‘abstract’. Studies not satisfying the inclusion criteria were
excluded at this stage. The studies selected for inclusion in stage two were further screened for
suitability during stage three by reading the selected manuscripts. At this stage studies were
excluded based on the following exclusion criteria: being confined to only a specific age group,
being hospital/clinic-based, studies reporting the results of larger studies as duplications and
studies conducted among South Asians residing elsewhere. To obtain additional data a manual
search was performed using the reference lists of selected articles. This process was conducted
by two independent reviewers and the final group of articles to be included in the review was
determined after an iterative consensus process among the reviewers.
20 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
For the purpose of describing prevalence data for the individual countries, the studies that were
most recent, nationally representative or with the largest sample size were included. For
meaningful comparisons of prevalence data among the countries, age-standardized data are
presented here, unless otherwise stated. Additional data not available in the published
manuscript such as gender and area-specific prevalence were obtained from corresponding
authors or calculated using available raw data. Area of residence and social status are key factors
determining the prevalence of diabetes; therefore, when exploring the secular trend in diabetes
prevalence it is meaningless to plot the prevalence data from studies based on different
populations. Hence, when evaluating secular trends we only considered studies that evaluated
the temporal change in prevalence between similar populations or prospective studies based on
the same population.
Presence of ‘diabetes mellitus’ in the individual studies was defined according to the World
Health Organization (WHO) or American Diabetes Association (ADA) criteria adopted at the
time of the respective studies. ‘Prediabetes’ was defined as the presence of Impaired Fasting
Glucose (IFG) or Impaired Glucose Tolerance (IGT) according to the above criteria. The
diabetes epidemicity index (a prognostic index of the diabetes epidemic in a population) was
defined as the ratio between the prevalence of IGT/IFG (pre-diabetes) and Total Glucose
Intolerance (TGI) (diabetes and pre-diabetes) i.e., the ‘diabetes epidemicity index’ is the
percentage of the TGI made up by IGT/IFG [9].
A meta-analysis of studies examining the risk factors associated with diabetes mellitus in South
Asian populations was conducted for parameters that were defined identically across studies.
Hence the meta-analysis was performed on the following clinical and biochemical parameters;
family history of diabetes, age, male gender, Body Mass Index (BMI), Waist-Hip Ratio (WHR),
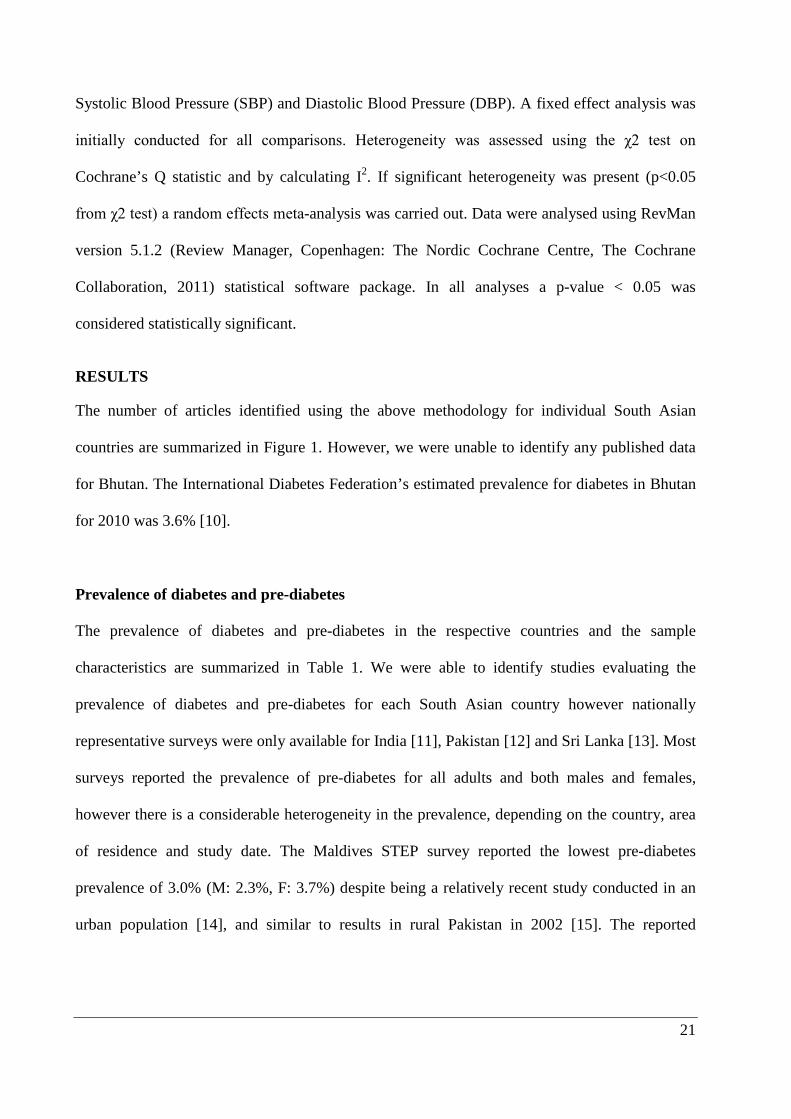
21
Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP). A fixed effect analysis was
initially conducted for all comparisons. Heterogeneity was assessed using the χ2 test on
Cochrane’s Q statistic and by calculating I2. If significant heterogeneity was present (p<0.05
from χ2 test) a random effects meta-analysis was carried out. Data were analysed using RevMan
version 5.1.2 (Review Manager, Copenhagen: The Nordic Cochrane Centre, The Cochrane
Collaboration, 2011) statistical software package. In all analyses a p-value < 0.05 was
considered statistically significant.
RESULTS
The number of articles identified using the above methodology for individual South Asian
countries are summarized in Figure 1. However, we were unable to identify any published data
for Bhutan. The International Diabetes Federation’s estimated prevalence for diabetes in Bhutan
for 2010 was 3.6% [10].
Prevalence of diabetes and pre-diabetes
The prevalence of diabetes and pre-diabetes in the respective countries and the sample
characteristics are summarized in Table 1. We were able to identify studies evaluating the
prevalence of diabetes and pre-diabetes for each South Asian country however nationally
representative surveys were only available for India [11], Pakistan [12] and Sri Lanka [13]. Most
surveys reported the prevalence of pre-diabetes for all adults and both males and females,
however there is a considerable heterogeneity in the prevalence, depending on the country, area
of residence and study date. The Maldives STEP survey reported the lowest pre-diabetes
prevalence of 3.0% (M: 2.3%, F: 3.7%) despite being a relatively recent study conducted in an
urban population [14], and similar to results in rural Pakistan in 2002 [15]. The reported

22 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
prevalence of pre-diabetes elsewhere in South Asia also showed a wide variation from 4.1% in
urban India [16] to 19.5% in urban Nepal [17].
The prevalence of diabetes also demonstrated a wide variation among countries. In Bangladesh
no studies were based on a nationally representative sample, however, regional surveys in urban
and semi-urban populations showed a moderately high prevalence of diabetes (6.8%-10.5%) [18,
19]. In rural Bangladeshi populations the prevalence of diabetes which was 3.8% in 1999-2000
[20], had increased to 8.5% by 2004-2005 [21]. In India, many studies have explored the
prevalence of diabetes with estimates varying considerably between different geographical areas
and between urban and rural populations. The Prevalence Of Diabetes in India Study (PODIS)
reported an age-standardized prevalence of 4.3%, 4.4% and 4.5% for all adults, and males and
females, respectively [11]. However, more recent studies based on urban populations or rapidly
developing regions have reported a higher prevalence of diabetes (10.1%) [16, 22] while other
studies from rural Indian populations have demonstrated an even higher prevalence (12.5%-
13.2%) [23, 24].
Results from the STEPS survey conducted in urban Male, Maldives showed a 4.5%, 4.3% and
4.7% prevalence of diabetes in all adults, males and females, respectively [14]. A survey
conducted in urban Nepal between 2001 and 2002 showed that 10.8% and 13.2% of males
suffered from diabetes and pre-diabetes respectively, with the values for females being 6.9% and
10.2%, respectively [25]. According to the Pakistan National Diabetes Survey (PNDS), 9.3%
males and 11.1% females suffered from diabetes in 1995 [12] and a rural survey showed a
higher proportion of males were affected by diabetes (10.1%) but not females (4.3%) [15]. No
recent data are available to regarding the present situation and therefore explore current trends in
Pakistan. A nationally representative diabetes and pre-diabetes study in Sri Lanka showed that
the age-standardized prevalence of diabetes among Sri Lankan adults was 10.3% [males 9.8%,
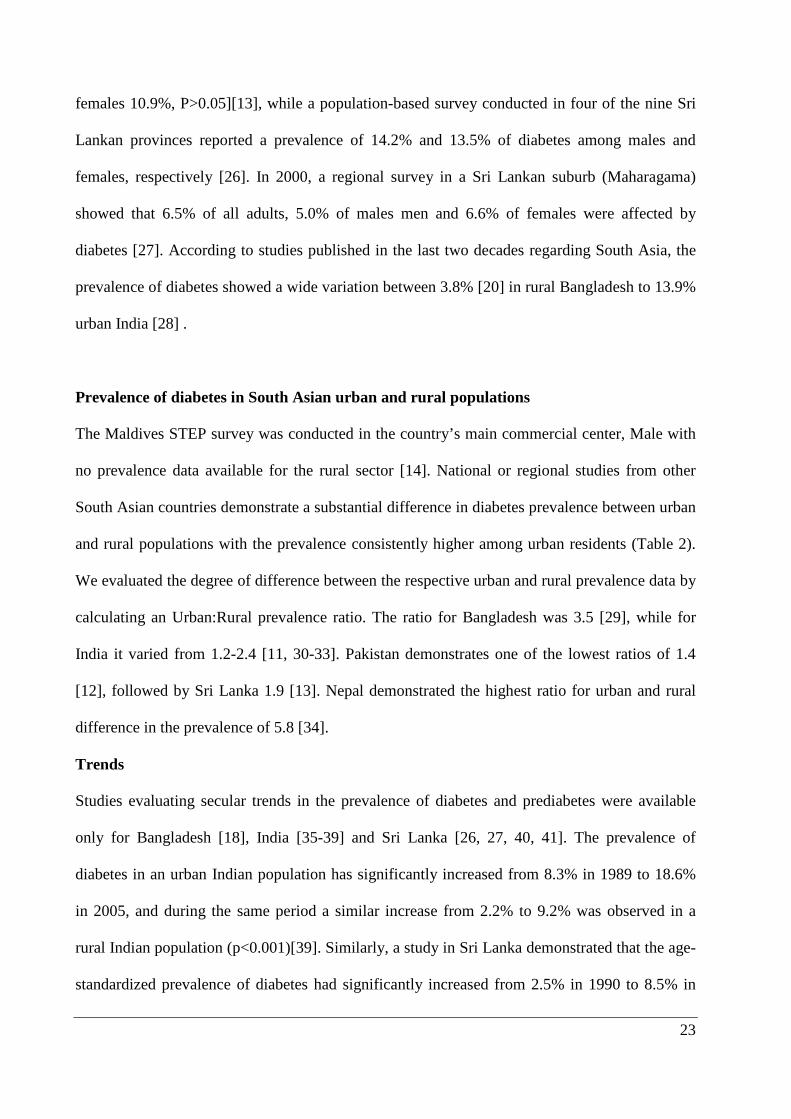
23
females 10.9%, P>0.05][13], while a population-based survey conducted in four of the nine Sri
Lankan provinces reported a prevalence of 14.2% and 13.5% of diabetes among males and
females, respectively [26]. In 2000, a regional survey in a Sri Lankan suburb (Maharagama)
showed that 6.5% of all adults, 5.0% of males men and 6.6% of females were affected by
diabetes [27]. According to studies published in the last two decades regarding South Asia, the
prevalence of diabetes showed a wide variation between 3.8% [20] in rural Bangladesh to 13.9%
urban India [28] .
Prevalence of diabetes in South Asian urban and rural populations
The Maldives STEP survey was conducted in the country’s main commercial center, Male with
no prevalence data available for the rural sector [14]. National or regional studies from other
South Asian countries demonstrate a substantial difference in diabetes prevalence between urban
and rural populations with the prevalence consistently higher among urban residents (Table 2).
We evaluated the degree of difference between the respective urban and rural prevalence data by
calculating an Urban:Rural prevalence ratio. The ratio for Bangladesh was 3.5 [29], while for
India it varied from 1.2-2.4 [11, 30-33]. Pakistan demonstrates one of the lowest ratios of 1.4
[12], followed by Sri Lanka 1.9 [13]. Nepal demonstrated the highest ratio for urban and rural
difference in the prevalence of 5.8 [34].
Trends
Studies evaluating secular trends in the prevalence of diabetes and prediabetes were available
only for Bangladesh [18], India [35-39] and Sri Lanka [26, 27, 40, 41]. The prevalence of
diabetes in an urban Indian population has significantly increased from 8.3% in 1989 to 18.6%
in 2005, and during the same period a similar increase from 2.2% to 9.2% was observed in a
rural Indian population (p<0.001)[39]. Similarly, a study in Sri Lanka demonstrated that the age-
standardized prevalence of diabetes had significantly increased from 2.5% in 1990 to 8.5% in

24 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
2000 (p<0.01) in a rural community [40], with only a slight increase in urban Sri Lanka from
5.3% to 6.5% during the same period [27, 41]. These findings are summarized in Figure 2a. The
trends for the prevalence of pre-diabetes are not as definitive For example, the increased
prevalence observed in urban India in the period 1989 (8.3%) to 2000 (16.7%) had declined to
7.4% by 2006. Prevalence data in rural populations of India and Sri Lanka also showed a decline
in prevalence during a similar period (Figure 2b). An increase in the prevalence of pre-diabetes
has been observed among urban Bangladeshi populations during the last decade.
The diabetes epidemicity index
The temporal change in the diabetes epidemicity index and prevalence of diabetes in the regional
countries are shown in Figure 3. The epidemicity index decreases as the prevalence of diabetes
increases in the respective countries (an epidemicity index calculated as the percentage of total
glucose intolerance made up by impaired glucose tolerance) [9]. The most recent available data
suggests a high epidemicity index in Sri Lanka (2005/2006 – 52.8%) and urban India (54.3%),
while for other countries in the region for which recent data are available, the epidemicity index
is comparatively low (rural India 2007 – 37.7% and urban Bangladesh – 33.1%).
Risk factors
A forest plot of the studies evaluating risk factors associated with diabetes among South Asians
is shown in Figure 4. The pooled odds ratio from random effects analysis for family history is
2.75 (95% CI: 2.11, 3.58; p<0.001). The significant overall effect indicates that family history is
a significantly associated risk factor for diabetes (Figure 4a). The forest plot for age also shows a
similar distinct increase in risk of diabetes with increasing age (Figure 4b). Male gender does not
demonstrate a similar distinct pattern, the increased risk shown by several studies have been
contradicted by others (Figure 4c). The forest plot of SBP demonstrates a significant increase in
risk of diabetes with increasing SBP (Figure 4d). In contrast DBP does not show a similar

25
distinct pattern (Figure 4e). Increasing BMI (Figure 4f) and WHR (Figure 4g) were both
associated with a significantly increased risk of diabetes.

26 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
DISCUSSION
This is the first comprehensive report to systematically evaluate the scientific literature on the
prevalence, trends and risk factors for diabetes in the South Asian region. Prevalence, based on
the most recent national surveys in the countries of the region were; 4.5% in Maldives (2004)
[14], 4.3% in India (1999-2002) [11], 8.7% (1995) in Pakistan (1995) [12] and 10.3% in Sri
Lanka (2005-2006) [13]. However, it is noteworthy that more recently published data from India
indicates a much higher prevalence of 9.2% (rural) and 18.6% (urban) in 2006 [39]. In addition,
recent reports also highlight a secular increase in prevalence in the region. Hence, it is apparent
that despite the differences in methodology, diagnostic criteria and age of subjects studied, the
region is facing an epidemic of diabetes. This is more evident when the observed prevalence is
compared with available data from other regions (Table 3), with observed prevalence
comparable to recent global and regional estimates by the International Diabetes Federation
(2011) [10].
The increased prevalence of diabetes in the South Asian region could be attributed to regional
changes in disease patterns from communicable to non-communicable diseases [42]. The reasons
attributed to this shift in disease pattern include: increased life expectancy, rapid population
growth, unplanned urbanization, low literacy and increased external debt with resultant cutbacks
on national healthcare expenditure [42]. Collectively, these and related issues have contributed
to the emergence of non-communicable diseases such as diabetes as a substantial regional health
problem. This so-called ‘epidemiological transition’ could also be linked to the rapid
industrialization occurring in the region as evidenced by the high prevalence of diabetes among
urban residents [43]. It is important to note that this epidemiologic transition and the rate of
increase in non-communicable diseases such as diabetes in developing countries is far greater
than that previously observed in high income countries, and hence there is a need to find
27
solutions a much shorter time frame and with far fewer resources [44]. Recent national level data
from Maldives indicates a very low prevalence of both diabetes and pre-diabetes despite
approximately two-thirds of the population being overweight, the highest in the region [14]. The
Maldives is an island nation in the Indian Ocean and relatively isolated from the rest of the
region, and with an economy based on tourism and the fishing industry. Hence it is debatable
whether diabetes in the Maldives presents as a different disease entity compared to the rest of the
South Asian region or differential exposure to risk factors/healthy lifestyles have resulted in a
low prevalence. This difference merits further investigation.
The high prevalence of pre-diabetes observed in many South Asian countries highlights a
potential indicator of further progression of the epidemic in the region. The combined prevalence
of diabetes and prediabetes (IGT/IFG), i.e. total glucose intolerance (TGI), may serve as a useful
measure of the public health impact of the epidemic. It has also been postulated that the
‘diabetes epidemicity index’ (% of the TGI made up by IGT/IFG) has a predictive value in
determining the stage of an epidemic of glucose intolerance in a given population [9]. Our
results also bear evidence to this fact as demonstrated by the decrease in the ‘epidemicity index’
in the different countries with progressive secular increase in the frequency of diabetes increases
(Figure 3). Hence with the prevalent diabetes epidemic in the region at present the recent
‘epidemicity indices’ for most regional countries are relatively low. However, it is noteworthy
that the present prevalent epidemic in the region had been preceded by a high ‘epidemicity
index’. Hence strategies aimed at primary prevention could be helpful to ameliorate a further
increase in the diabetes epidemic in populations such as Sri Lanka where recent data shows a
high prevailing ‘epidemicity index’.

28 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
Family history, age, male gender, BMI, WHR, systolic and diastolic blood pressure were
significant risk factors for diabetes among South Asians. In addition, few studies have also
demonstrated an association between diabetes and wealth/income [19, 24, 36, 45],
hypercholesterolemia [24], physical inactivity [19, 32, 37, 45], the presence of acanthosis
nigricans [16], graduate education [39] and office-based occupation [45]. A meta-analysis could
not be performed for these risk factors due to the limited number of studies or due to variations
in definitions/classifications of risk factors between studies. The recent epidemic of diabetes in
the region could be primarily due to environmental factors such as diet and physical activity
levels coupled with a genetic predisposition [7, 46]. The strong evidence for the association
between diabetes and family history highlights a genetic contribution the prevalent epidemic
[47]. In addition, in this ethnically diverse population, increasing age and body weight have also
been demonstrated as important contributory factors. This is evident by the association between
diabetes and increasing BMI, waist-hip ratio and abdominal obesity [16, 21, 24, 45]. This may
be the cause of the high susceptibility for diabetes and other metabolic abnormalities among
South Asians [7].
People in South Asia have faced under-nutrition for many generations; they are born smaller
however coupled with subsequent obesity increases risk for insulin resistance syndrome in later
life [48]. A recent review has reported several dietary factors associated with insulin resistance
among South Asians, such as higher intakes of carbohydrate, saturated fatty acids, trans-fatty
acids and n-6 PUFA, and lower intakes of n-3 PUFA and fiber, hence the Asian diet may be an
important contributory factor for the high disease prevalence [46]. During recent years
urbanization has risen unprecedentedly in the South Asian region [42]. There are unhealthy
lifestyle changes that are known to be associated with urbanization such as the lack of physical
activity, changes in dietary habits and stress, all of which increases the risk of diabetes, as
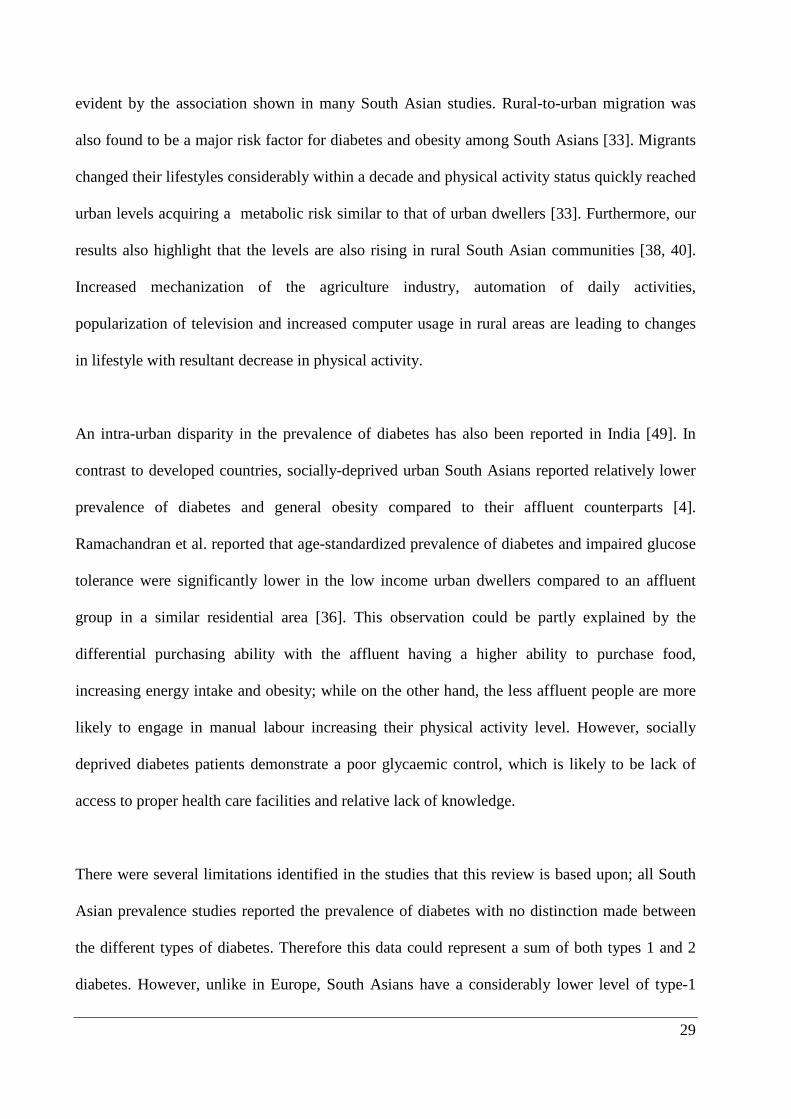
29
evident by the association shown in many South Asian studies. Rural-to-urban migration was
also found to be a major risk factor for diabetes and obesity among South Asians [33]. Migrants
changed their lifestyles considerably within a decade and physical activity status quickly reached
urban levels acquiring a metabolic risk similar to that of urban dwellers [33]. Furthermore, our
results also highlight that the levels are also rising in rural South Asian communities [38, 40].
Increased mechanization of the agriculture industry, automation of daily activities,
popularization of television and increased computer usage in rural areas are leading to changes
in lifestyle with resultant decrease in physical activity.
An intra-urban disparity in the prevalence of diabetes has also been reported in India [49]. In
contrast to developed countries, socially-deprived urban South Asians reported relatively lower
prevalence of diabetes and general obesity compared to their affluent counterparts [4].
Ramachandran et al. reported that age-standardized prevalence of diabetes and impaired glucose
tolerance were significantly lower in the low income urban dwellers compared to an affluent
group in a similar residential area [36]. This observation could be partly explained by the
differential purchasing ability with the affluent having a higher ability to purchase food,
increasing energy intake and obesity; while on the other hand, the less affluent people are more
likely to engage in manual labour increasing their physical activity level. However, socially
deprived diabetes patients demonstrate a poor glycaemic control, which is likely to be lack of
access to proper health care facilities and relative lack of knowledge.
There were several limitations identified in the studies that this review is based upon; all South
Asian prevalence studies reported the prevalence of diabetes with no distinction made between
the different types of diabetes. Therefore this data could represent a sum of both types 1 and 2
diabetes. However, unlike in Europe, South Asians have a considerably lower level of type-1
30 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
diabetes (1-2%) and thus these prevalence data closely resemble the total prevalence of type 2
diabetes [1]. In addition, all studies included in our review were community-based surveys.
Hence, this data may be an underestimate of the true regional burden, since a significant
proportion of patients with diabetes may well be admitted in hospitals and care centers.
Moreover, some studies have reported the prevalence of only known diabetes. The definitions
and diagnostic criteria have also changed over the last two decades influencing prevalence rates.
However, for the purpose of describing prevalence data for the individual countries the studies
that were most recent were included. Hence the variations in diagnostic criteria are likely to be
minimal as older studies were excluded. In addition when evaluating secular trends (Figure 2)
we have used studies that were on the same population and used the same diagnostic criteria.
The definition of pre-diabetes also varies between studies, with some studies using only IFG [16,
50], some IGT [31, 36] and some using both [13]. There is also a heterogeneity in analytical
methods as some studies applied capillary blood and glucometers whereas others used venous
blood and sophisticate biochemical analysis.
CONCLUSIONS
In conclusion, our review highlights a significant epidemic of diabetes in the South Asian region
with a rapid increase in prevalence over the last two decades. It is evident that several modifiable
and non-modifiable risk factors play an important role in the pathogenesis of diabetes among
South Asians. Hence there is a need for urgent preventive and curative strategies to be
implemented.
31
REFERENCES
1. Wild S, Roglic G, Green A, Sicree R, King H: Global Prevalence of Diabetes. Diabetes
Care 2004, 27:1047-1053.
2. Mather HM, Keen H: The Southall Diabetes Survey: prevalence of known diabetes in
Asians and Europeans. Br Med J (Clin Res Ed) 1985, 291:1081-1084.
3. UK population: by ethnic group: Census update
[http://www.statistics.gov.uk/statbase/ssdataset.asp?vlnk=6588&More=Y]
4. Health Survey for England: The health of minority ethnic groups ’99. In Book The
health of minority ethnic groups ’99 (Editor ed.^eds.). City; 2001.
5. Mukhopadhyay B, Forouhi NG, Fisher BM, Kesson CM, Sattar N: A comparison of
glycaemic and metabolic control over time among South Asian and European
patients with Type 2 diabetes: results from follow-up in a routine diabetes clinic.
Diabetic Medicine 2006, 23:94-98.
6. Ramachandran A, Wan Ma RC, Snehalatha C: Diabetes in Asia. The Lancet 2010,
375:408-418.
7. Barnett A, Dixon A, Bellary S, Hanif M, O’hare J, Raymond N, Kumar S: Type 2
diabetes and cardiovascular risk in the UK south Asian community. Diabetologia
2006, 49:2234-2246.
8. Mohan V, Sandeep S, Deepa R, Shah B, Varghese C: Epidemiology of type 2 diabetes:
Indian scenario. Indian J Med Res 2007, 125:217-230.
9. Dowse GK, Zimmet PZ, King H: Relationship between prevalence of impaired
glucose tolerance and NIDDM in a population. Diabetes Care 1991, 14:968-974.
10. International Diabetes Federation: The Diabetes Atlas. Fifth edn. Brussels: International
Diabetes Federation; 2011.
11. Sadikot SM, Nigam A, Das S, Bajaj S, Zargar AH, Prasannakumar KM, Sosale A,
Munichoodappa C, Seshiah V, Singh SK, et al: The burden of diabetes and impaired
glucose tolerance in India using the WHO 1999 criteria: prevalence of diabetes in
India study (PODIS). Diabetes Res Clin Pract 2004, 66:301-307.
12. Shera AS, Jawad F, Maqsood A: Prevalence of diabetes in Pakistan. Diabetes Res Clin
Pract 2007, 76:219-222.
13. Katulanda P, Constantine GR, Mahesh JG, Sheriff R, Seneviratne RD, Wijeratne S,
Wijesuriya M, McCarthy MI, Adler AI, Matthews DR: Prevalence and projections of

32 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
diabetes and pre-diabetes in adults in Sri Lanka--Sri Lanka Diabetes,
Cardiovascular Study (SLDCS). Diabet Med 2008, 25:1062-1069.
14. Aboobakur M, Latheef A, Mohamed AJ, Moosa S, Pandey RM, Krishnan A,
Prabhakaran D: Surveillance for non-communicable disease risk factors in Maldives:
results from the first STEPS survey in Male. Int J Public Health 2010, 55:489-496.
15. Basit A, Hydrie MZ, Ahmed K, Hakeem R: Prevalence of diabetes, impaired fasting
glucose and associated risk factors in a rural area of Baluchistan province
according to new ADA criteria. J Pak Med Assoc 2002, 52:357-360.
16. Menon VU, Kumar KV, Gilchrist A, Sugathan TN, Sundaram KR, Nair V, Kumar H:
Prevalence of known and undetected diabetes and associated risk factors in central
Kerala--ADEPS. Diabetes Res Clin Pract 2006, 74:289-294.
17. Ono K, Limbu YR, Rai SK, Kurokawa M, Yanagida J, Rai G, Gurung N, Sharma M, Rai
CK: The prevalence of type 2 diabetes mellitus and impaired fasting glucose in semi-
urban population of Nepal. Nepal Med Coll J 2007, 9:154-156.
18. Rahim MA, Hussain A, Azad Khan AK, Sayeed MA, Keramat Ali SM, Vaaler S: Rising
prevalence of type 2 diabetes in rural Bangladesh: a population based study.
Diabetes Res Clin Pract 2007, 77:300-305.
19. Sayeed MA, Mahtab H, Khanam PA, Latif ZA, Banu A, Khan AK: Prevalence of
diabetes and impaired fasting glucose in urban population of Bangladesh.
Bangladesh Med Res Counc Bull 2007, 33:1-12.
20. Sayeed MA, Mahtab H, Akter Khanam P, Abdul Latif Z, Keramat Ali SM, Banu A,
Ahren B, Azad Khan AK: Diabetes and impaired fasting glycemia in a rural
population of Bangladesh. Diabetes Care 2003, 26:1034-1039.
21. Rahman MM, Rahim MA, Nahar Q: Prevalence and risk factors of type 2 diabetes in
an urbanizing rural community of Bangladesh. Bangladesh Med Res Counc Bull
2007, 33:48-54.
22. Ajay VS, Prabhakaran D, Jeemon P, Thankappan KR, Mohan V, Ramakrishnan L, Joshi
P, Ahmed FU, Mohan BV, Chaturvedi V, et al: Prevalence and determinants of
diabetes mellitus in the Indian industrial population. Diabet Med 2008, 25:1187-
1194.
23. Chow CK, Raju PK, Raju R, Reddy KS, Cardona M, Celermajer DS, Neal BC: The
prevalence and management of diabetes in rural India. Diabetes Care 2006, 29:1717-
1718.
33
24. Vijayakumar G, Arun R, Kutty VR: High prevalence of type 2 diabetes mellitus and
other metabolic disorders in rural Central Kerala. J Assoc Physicians India 2009,
57:563-567.
25. Shrestha UK, Singh DL, Bhattarai MD: The prevalence of hypertension and diabetes
defined by fasting and 2-h plasma glucose criteria in urban Nepal. Diabet Med 2006,
23:1130-1135.
26. Wijewardene K, Mohideen MR, Mendis S, Fernando DS, Kulathilaka T, Weerasekara D,
Uluwitta P: Prevalence of hypertension, diabetes and obesity: baseline findings of a
population based survey in four provinces in Sri Lanka. The Ceylon medical journal
2005, 50:62-70.
27. Malavige G, de Alwis N, Weerasooriya N, Fernando D, Siribaddana S: Increasing
diabetes and vascular risk factors in a sub-urban Sri Lankan population. Diabetes
research and clinical practice 2002, 57:143-145.
28. Ramachandran A, Snehalatha C, Satyavani K, Vijay V: Impaired fasting glucose and
impaired glucose tolerance in urban population in India. Diabet Med 2003, 20:220-
224.
29. Hussain A, Rahim MA, Azad Khan AK, Ali SMK, Vaaler S: Type 2 diabetes in rural
and urban population: diverse prevalence and associated risk factors in
Bangladesh. Diabetic Medicine 2005, 22:931-936.
30. Singh RB, Bajaj S, Niaz MA, Rastogi SS, Moshiri M: Prevalence of type 2 diabetes
mellitus and risk of hypertension and coronary artery disease in rural and urban
population with low rates of obesity. Int J Cardiol 1998, 66:65-72.
31. Zargar AH, Khan AK, Masoodi SR, Laway BA, Wani AI, Bashir MI, Dar FA:
Prevalence of type 2 diabetes mellitus and impaired glucose tolerance in the
Kashmir Valley of the Indian subcontinent. Diabetes Res Clin Pract 2000, 47:135-
146.
32. Mohan V, Mathur P, Deepa R, Deepa M, Shukla DK, Menon GR, Anand K, Desai NG,
Joshi PP, Mahanta J, et al: Urban rural differences in prevalence of self-reported
diabetes in India--the WHO-ICMR Indian NCD risk factor surveillance. Diabetes
Res Clin Pract 2008, 80:159-168.
33. Ebrahim S, Kinra S, Bowen L, Andersen E, Ben-Shlomo Y, Lyngdoh T, Ramakrishnan
L, Ahuja RC, Joshi P, Das SM, et al: The effect of rural-to-urban migration on
obesity and diabetes in India: a cross-sectional study. PLoS Med 2010, 7:e1000268.
34 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
34. Singh DL, Bhattarai MD: High prevalence of diabetes and impaired fasting
glycaemia in urban Nepal. Diabet Med 2003, 20:170-171.
35. Mohan V, Deepa M, Deepa R, Shanthirani CS, Farooq S, Ganesan A, Datta M: Secular
trends in the prevalence of diabetes and impaired glucose tolerance in urban South
India--the Chennai Urban Rural Epidemiology Study (CURES-17). Diabetologia
2006, 49:1175-1178.
36. Ramachandran A, Snehalatha C, Vijay V: Temporal changes in prevalence of type 2
diabetes and impaired glucose tolerance in urban southern India. Diabetes Res Clin
Pract 2002, 58:55-60.
37. Ramachandran A, Snehalatha C, Latha E, Vijay V, Viswanathan M: Rising prevalence
of NIDDM in an urban population in India. Diabetologia 1997, 40:232-237.
38. Ramachandran A, Snehalatha C, Baskar AD, Mary S, Kumar CK, Selvam S, Catherine S,
Vijay V: Temporal changes in prevalence of diabetes and impaired glucose
tolerance associated with lifestyle transition occurring in the rural population in
India. Diabetologia 2004, 47:860-865.
39. Ramachandran A, Mary S, Yamuna A, Murugesan N, Snehalatha C: High prevalence of
diabetes and cardiovascular risk factors associated with urbanization in India.
Diabetes Care 2008, 31:893-898.
40. Illangasekera U, Rambodagalla S, Tennakoon S: Temporal trends in the prevalence of
diabetes mellitus in a rural community in Sri Lanka. J R Soc Promot Health 2004,
124:92-94.
41. Fernando DJ, Siribaddana S, de Silva D: Impaired glucose tolerance and diabetes
mellitus in a suburban Sri Lankan community. Postgrad Med J 1994, 70:347-349.
42. Islam A, Tahir MZ: Health sector reform in South Asia: new challenges and
constraints. Health Policy 2002, 60:151-169.
43. Mohan V: Why are Indians more prone to diabetes? J Assoc Physicians India 2004,
52:468-474.
44. Misra A, Khurana L: Obesity and the metabolic syndrome in developing countries. J
Clin Endocrinol Metab 2008, 93:S9-30.
45. Ramachandran A, Snehalatha C, Kapur A, Vijay V, Mohan V, Das AK, Rao PV, Yajnik
CS, Prasanna Kumar KM, Nair JD: High prevalence of diabetes and impaired glucose
tolerance in India: National Urban Diabetes Survey. Diabetologia 2001, 44:1094-
1101.

35
46. Misra A, Khurana L, Isharwal S, Bhardwaj S: South Asian diets and insulin resistance.
Br J Nutr 2009, 101:465-473.
47. Mohan V, Shanthirani CS, Deepa R: Glucose intolerance (diabetes and IGT) in a
selected South Indian population with special reference to family history, obesity
and lifestyle factors--the Chennai Urban Population Study (CUPS 14). J Assoc
Physicians India 2003, 51:771-777.
48. Yajnik CS: Early life origins of insulin resistance and type 2 diabetes in India and
other Asian countries. J Nutr 2004, 134:205-210.
49. Mohan V, Shanthirani S, Deepa R, Premalatha G, Sastry NG, Saroja R: Intra-urban
differences in the prevalence of the metabolic syndrome in southern India -- the
Chennai Urban Population Study (CUPS No. 4). Diabetic Medicine: A Journal Of The
British Diabetic Association 2001, 18:280-287.
50. Gupta A, Gupta R, Sarna M, Rastogi S, Gupta VP, Kothari K: Prevalence of diabetes,
impaired fasting glucose and insulin resistance syndrome in an urban Indian
population. Diabetes Res Clin Pract 2003, 61:69-76.
51. Abu Sayeed M, Mahtab H, Akter Khanam P, Abul Ahsan K, Banu A, Rashid AN, Azad
Khan AK: Diabetes and impaired fasting glycemia in the tribes of Khagrachari hill
tracts of Bangladesh. Diabetes Care 2004, 27:1054-1059.
52. Ravikumar P, Bhansali A, Ravikiran M, Bhansali S, Walia R, Shanmugasundar G,
Thakur JS, Kumar Bhadada S, Dutta P: Prevalence and risk factors of diabetes in a
community-based study in North India: the Chandigarh Urban Diabetes Study
(CUDS). Diabetes Metab 2011, 37:216-221.
53. Zaman FA, Pal R, Zaman GS, Swati IA, Kayyum A: Glucose indices, frank and
undetected diabetes in relation to hypertension and anthropometry in a South
Indian rural population. Indian J Public Health 2011, 55:34-37.
54. Vaz NC, Ferreira AM, Kulkarni MS, Vaz FS: Prevalence of diabetes mellitus in a
rural population of Goa, India. Natl Med J India 2011, 24:16-18.
55. Mehta KD, Karki P, Lamsal M, Paudel IS, Majhi S, Das BK, Sharma S, Jha N, Baral N:
Hyperglycemia, glucose intolerance, hypertension and socioeconomic position in
eastern Nepal. Southeast Asian J Trop Med Public Health 2011, 42:197-207.

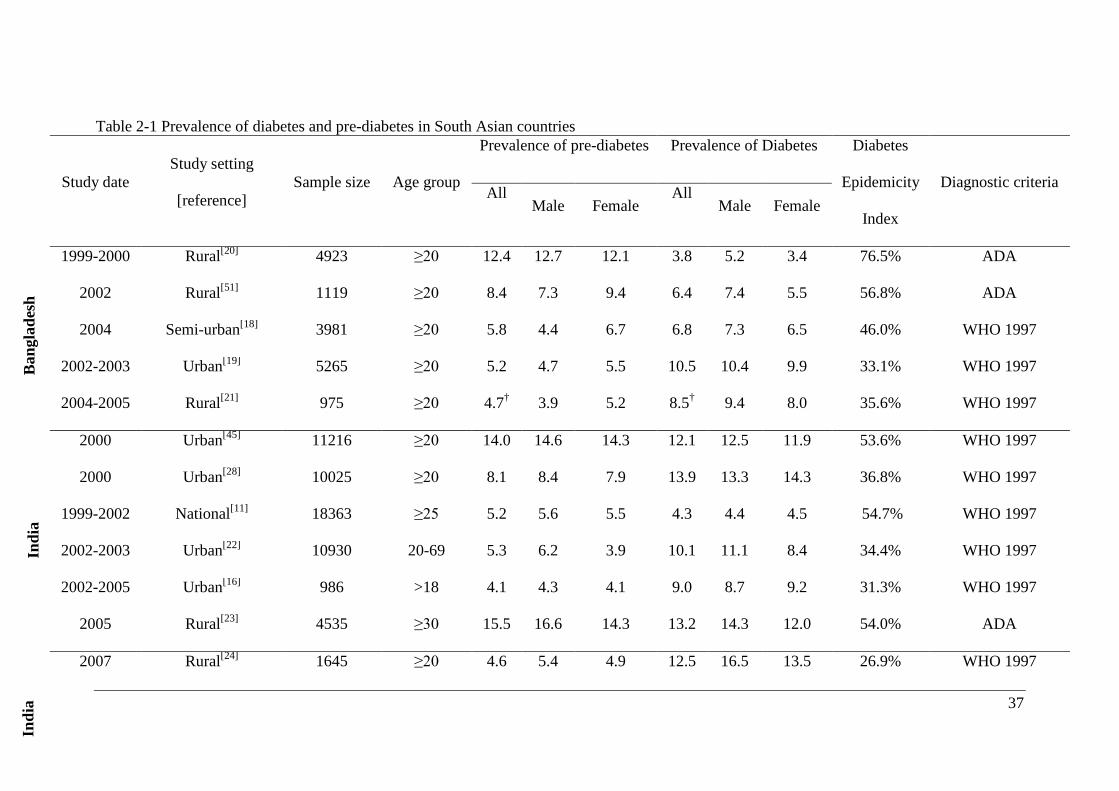
37
Table 2-1 Prevalence of diabetes and pre-diabetes in South Asian countries
Study date Study setting
[reference] Sample size Age group
Prevalence of pre-diabetes Prevalence of Diabetes Diabetes
Epidemicity
Index
Diagnostic criteria All
Male Female All
Male Female
1999-2000 Rural[20] 4923 ≥20 12.4 12.7 12.1 3.8 5.2 3.4 76.5% ADA
2002 Rural[51] 1119 ≥20 8.4 7.3 9.4 6.4 7.4 5.5 56.8% ADA
2004 Semi-urban[18] 3981 ≥20 5.8 4.4 6.7 6.8 7.3 6.5 46.0% WHO 1997
2002-2003 Urban[19] 5265 ≥20 5.2 4.7 5.5 10.5 10.4 9.9 33.1% WHO 1997
2004-2005 Rural[21] 975 ≥20 4.7† 3.9 5.2 8.5† 9.4 8.0 35.6% WHO 1997
2000 Urban[45] 11216 ≥20 14.0 14.6 14.3 12.1 12.5 11.9 53.6% WHO 1997
2000 Urban[28] 10025 ≥20 8.1 8.4 7.9 13.9 13.3 14.3 36.8% WHO 1997
1999-2002 National[11] 18363 ≥25 5.2 5.6 5.5 4.3 4.4 4.5 54.7% WHO 1997
2002-2003 Urban[22] 10930 20-69 5.3 6.2 3.9 10.1 11.1 8.4 34.4% WHO 1997
2002-2005 Urban[16] 986 >18 4.1 4.3 4.1 9.0 8.7 9.2 31.3% WHO 1997
2005 Rural[23] 4535 ≥30 15.5 16.6 14.3 13.2 14.3 12.0 54.0% ADA
2007 Rural[24] 1645 ≥20 4.6 5.4 4.9 12.5 16.5 13.5 26.9% WHO 1997
Ban
glad
esh
Indi
a In
dia
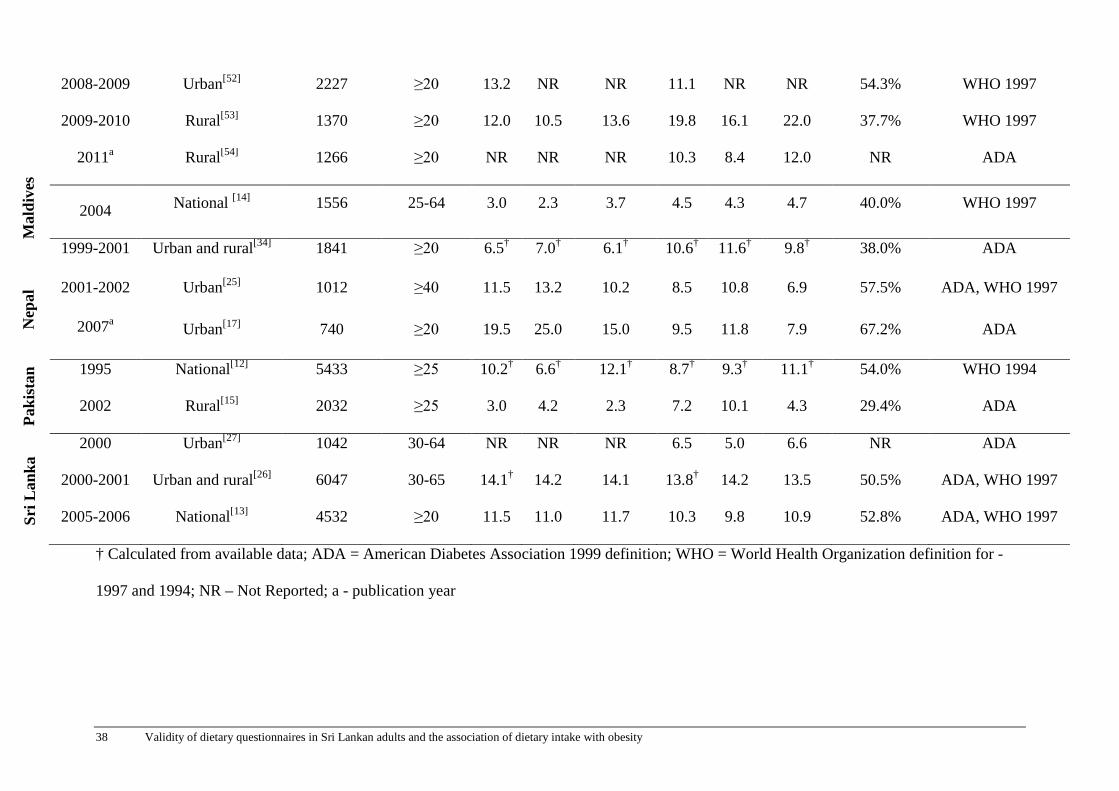
38 Validity of dietary questionnaires in Sri Lankan adults and the association of dietary intake with obesity
2008-2009 Urban[52] 2227 ≥20 13.2 NR NR 11.1 NR NR 54.3% WHO 1997
2009-2010 Rural[53] 1370 ≥20 12.0 10.5 13.6 19.8 16.1 22.0 37.7% WHO 1997
2011a Rural[54] 1266 ≥20 NR NR NR 10.3 8.4 12.0 NR ADA
2004 National [14] 1556 25-64 3.0 2.3 3.7 4.5 4.3 4.7 40.0% WHO 1997
1999-2001 Urban and rural[34] 1841 ≥20 6.5† 7.0† 6.1† 10.6† 11.6† 9.8† 38.0% ADA
2001-2002 Urban[25] 1012 ≥40 11.5 13.2 10.2 8.5 10.8 6.9 57.5% ADA, WHO 1997
2007a Urban[17] 740 ≥20 19.5 25.0 15.0 9.5 11.8 7.9 67.2% ADA
1995 National[12] 5433 ≥25 10.2† 6.6† 12.1† 8.7† 9.3† 11.1† 54.0% WHO 1994
2002 Rural[15] 2032 ≥25 3.0 4.2 2.3 7.2 10.1 4.3 29.4% ADA
2000 Urban[27] 1042 30-64 NR NR NR 6.5 5.0 6.6 NR ADA
2000-2001 Urban and rural[26] 6047 30-65 14.1† 14.2 14.1 13.8† 14.2 13.5 50.5% ADA, WHO 1997
2005-2006 National[13] 4532 ≥20 11.5 11.0 11.7 10.3 9.8 10.9 52.8% ADA, WHO 1997
† Calculated from available data; ADA = American Diabetes Association 1999 definition; WHO = World Health Organization definition for -
1997 and 1994; NR – Not Reported; a - publication year
Sri L
anka
Pa
kist
an
Nep
al
Mal
dive
s

Chapter 2: Manuscript 1 39
Table 2-2: Prevalence of diabetes according to area of residence Country
[reference] Year
Urban sector Rural sector Urban:Rural
ratio All Males Females All Males Females
Bangladesh[29] 2005a 8.1 7.7 8.5 2.3 1.9 2.5 3.5
India[30] 1998a 5.9 7.0 5.0 2.9 3.0 2.7 2.0
India[31] 1996-1998 2.2 2.6 1.7 1.8 1.8 1.8 1.2
India[11] 1999-2002 5.6 5.6 5.8 2.7 2.5 2.5 2.1
India[32] 2003-2005 7.3 NR NR 3.1 NR NR 2.4
India[33] 2005-2007 13.5 14.0 10.2 6.2 5.6 5.9 2.2
Nepal[34] 1999-2001 14.6 14.9 14.3 2.5 4.1 1.2 5.8
Nepal[55] 2005-2006 22.8 NR NR 20.0 NR NR 1.1
Pakistan[12]† 1995 10.5 11.6 10.3 7.6 8.3 7.4 1.4
Sri Lanka[13] 2005-2006 16.4 NR NR 8.7 NR NR 1.9
† calculated from available data; NR – Not reported; a - publication year

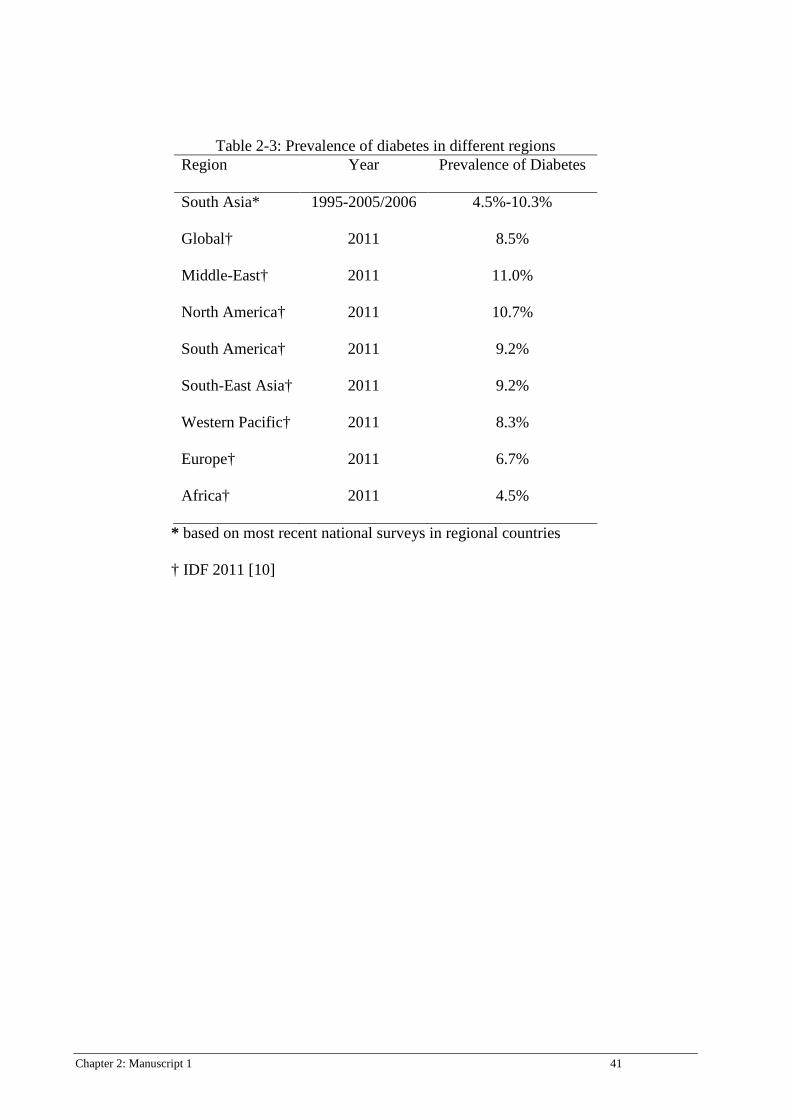
Chapter 2: Manuscript 1 41
Table 2-3: Prevalence of diabetes in different regions Region Year Prevalence of Diabetes
South Asia* 1995-2005/2006 4.5%-10.3%
Global† 2011 8.5%
Middle-East† 2011 11.0%
North America† 2011 10.7%
South America† 2011 9.2%
South-East Asia† 2011 9.2%
Western Pacific† 2011 8.3%
Europe† 2011 6.7%
Africa† 2011 4.5%
* based on most recent national surveys in regional countries
† IDF 2011 [10]

42 Chapter 2: Manuscript 1
Figure 2-1: Summarized search protocol
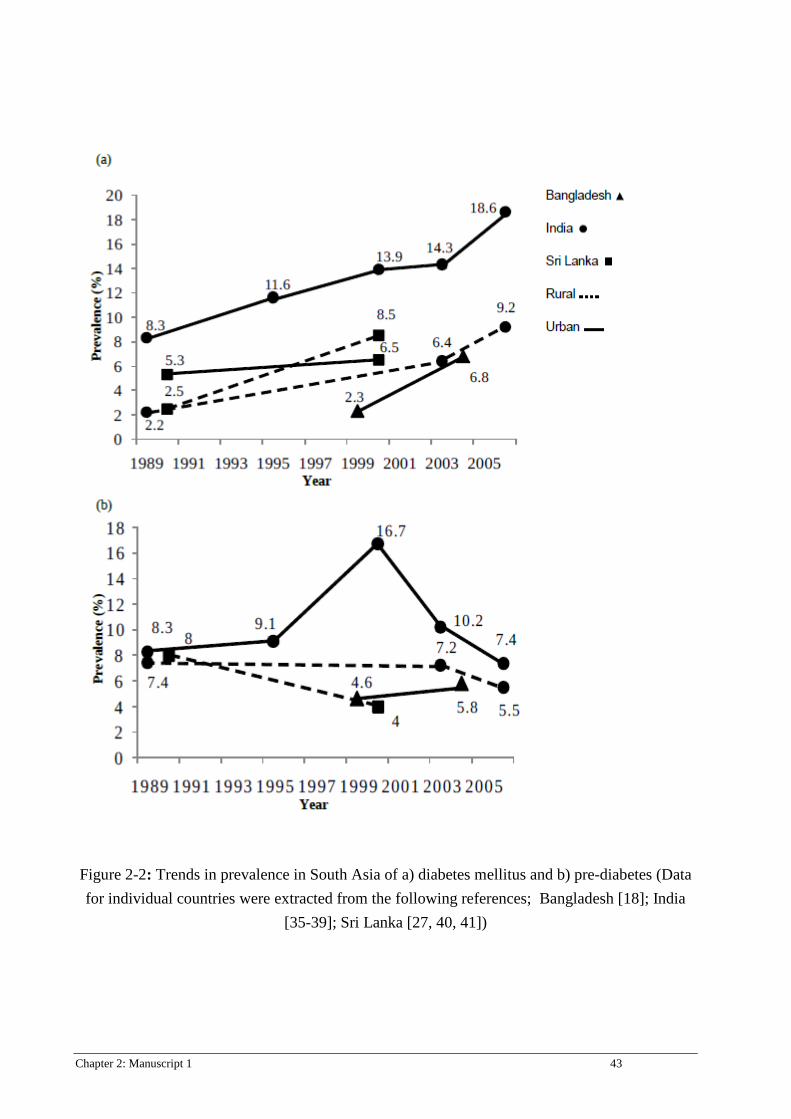
Chapter 2: Manuscript 1 43
Figure 2-2: Trends in prevalence in South Asia of a) diabetes mellitus and b) pre-diabetes (Data for individual countries were extracted from the following references; Bangladesh [18]; India
[35-39]; Sri Lanka [27, 40, 41])
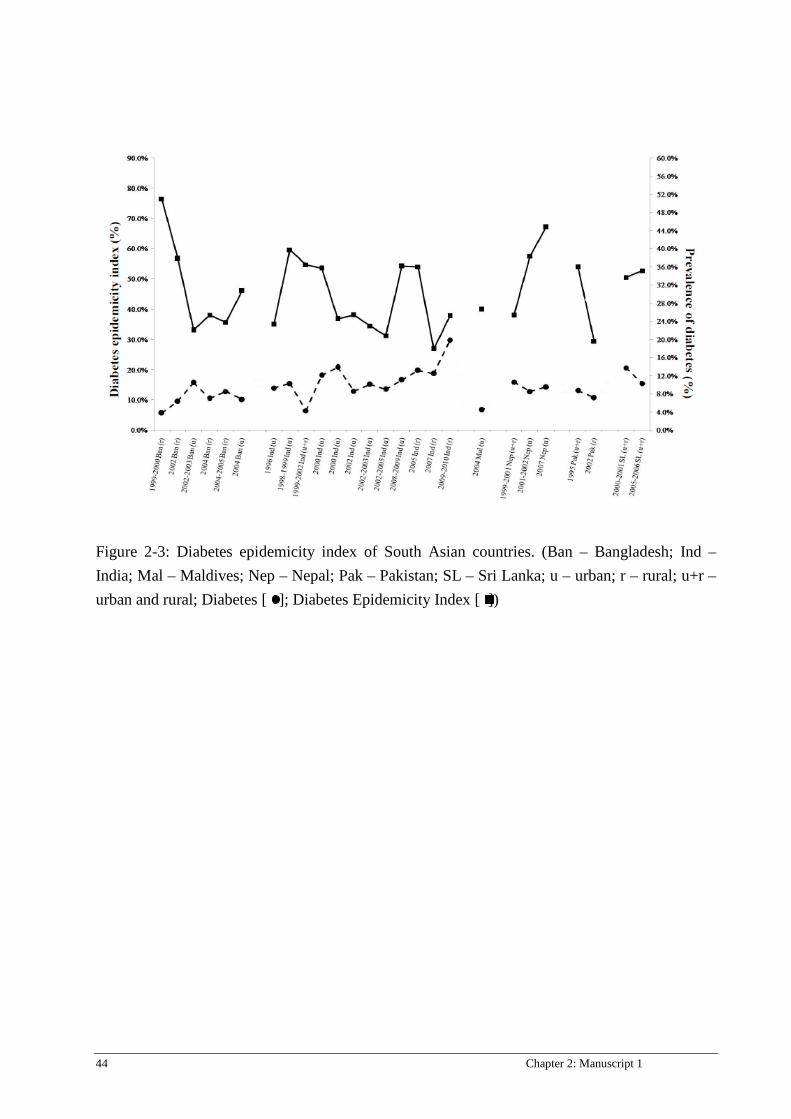
44 Chapter 2: Manuscript 1
Figure 2-3: Diabetes epidemicity index of South Asian countries. (Ban – Bangladesh; Ind – India; Mal – Maldives; Nep – Nepal; Pak – Pakistan; SL – Sri Lanka; u – urban; r – rural; u+r – urban and rural; Diabetes [ ]; Diabetes Epidemicity Index [ ])

Chapter 2: Manuscript 1 45
Continue to page 46.
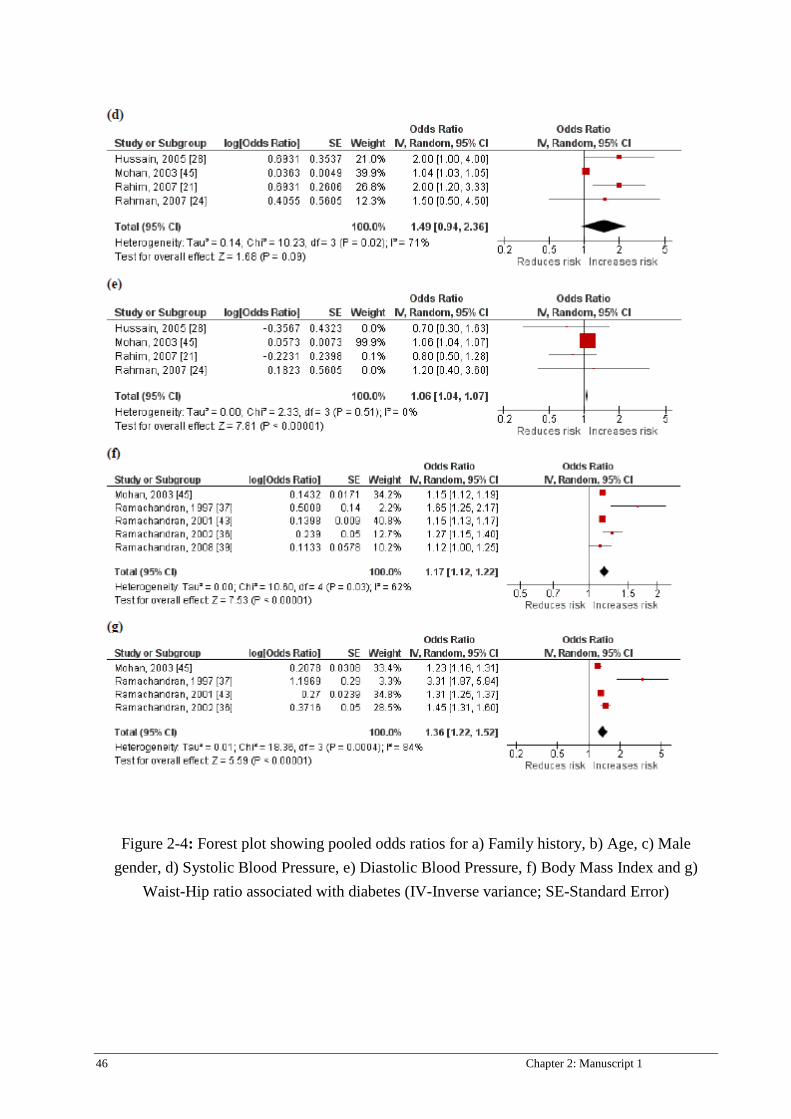
46 Chapter 2: Manuscript 1
Figure 2-4: Forest plot showing pooled odds ratios for a) Family history, b) Age, c) Male gender, d) Systolic Blood Pressure, e) Diastolic Blood Pressure, f) Body Mass Index and g)
Waist-Hip ratio associated with diabetes (IV-Inverse variance; SE-Standard Error)
Chapter 3: Manuscript 2 47
Chapter 3: Manuscript 2
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Prevalence, trends and associated socio-economic factors of obesity in South Asia Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date

48 Chapter 3: Manuscript 2
TITLE PAGE
Prevalence, trends and associated socio-economic factors of obesity in South Asia Ranil Jayawardena1,2, Nuala M. Byrne1, Mario J. Soares3, Prasad Katulanda2, Andrew P. Hills4 1Institute of Health and Biomedical Innovation, Queensland University of Technology, Brisbane, Queensland, Australia 2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka 3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health Sciences, Curtin University, Perth, WA, Australia 4Mater Mother’s Hospital, Mater Medical Research Institute and Griffith Health Institute, Griffith University, Brisbane, Queensland, Australia
Citation
R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills (2013). Prevalence, Trends and
Associated Socio-Economic Factors of Obesity in South Asia. Obesity Facts (in press) Ms No.:
201202017

Chapter 3: Manuscript 2 49
SUMMARY
Worldwide obesity levels have increased unprecedentedly over the past couple of decades.
Although the prevalence, trends and associated socio-economic factors of the condition have
been extensively reported in Western populations, less is known regarding South Asian
populations. A review of articles using MEDLINE with combinations of the MeSH terms:
Obesity, Overweight, and “Abdominal Obesity” limiting to epidemiology and south Asian
counties. Although the methodological heterogeneity and variation according to country, area of
residence, gender exist, the most recent nationally representative and large regional data show a
clear epidemic of obesity, overweight and abdominal obesity. Prevalence estimates of
overweight and obesity [based on Asian cut-offs; Overweight ≥23 kg/m2, Obesity ≥25 kg/m2]
ranged from 3.5% in rural Bangladesh to over 65% in the Maldives. Abdominal obesity was
more prevalent than general obesity in both sexes in this ethnic group. Countries with the lowest
prevalence had the highest upward trend of obesity. Socio-economic factors associated with
greater obesity in the region included female gender, middle age, urban residence, higher
educational and economic status. In conclusion, South Asia is significantly affected by the
obesity epidemic. Collaborative public health interventions to reverse these trends need to be
mindful of many socioeconomic constraints in order to provide long term solutions.
50 Chapter 3: Manuscript 2
INTRODUCTION
Worldwide obesity levels have increased unprecedentedly over the past couple of decades.
Indeed, according to the World Health Organization’s (WHO) recent global estimates, over one
billion and nearly 300 million adults are overweight and obese, respectively [1]. In many
affluent countries, obesity has reached epidemic levels and is associated with non-communicable
diseases (NCDs) including diabetes, hypertension, dyslipidemia and coronary heart disease, all
major public health issues [2]. In affluent countries, socio-economic status and education level
are negatively associated with the prevalence of obesity, a situation which contrasts to that in
South Asia [3]. Traditionally, infectious diseases [4] and under-nutrition [5] were considered
major health problems in South Asia and little attention was paid to obesity by healthcare
workers, policy makers or researchers. However, with the rapid emergence of the obesity
epidemic in South Asian countries, and an increasing body of evidence that people originating
from the Indian sub-continent have a high risk for NCDs including diabetes mellitus type 2
(DM), coronary heart disease (CHD) and stroke compared to Europeans [6], greater attention is
being paid. Alarmingly, South Asia has the highest number of patients with diabetes worldwide
and 50% of the adult disease burden in South Asia is attributable to NCDs [7].
It is estimated that the total population living in South Asia now exceeds 1.56 billion with India
(2nd), Pakistan (6th) and Bangladesh (7th) among the ten most populated countries in the world
[8]. Moreover, people who originated from the Indian sub-continent are also widespread in most
countries of the world, predominantly in affluent nations. The disease burden in South Asians is
invariably a high priority as a global health issue. Although there have been a few in-depth
reviews on obesity and associated disease in Asia [6,9], none has discussed obesity prevalence
and trends for individual countries in the region. Therefore, the main aim of this study was to

Chapter 3: Manuscript 2 51
discuss the prevalence of overweight and obesity among the adult population from individual
countries in South Asia using the most recent representative evidence. Associated aims were to
plot obesity trends over time across the last few decades, and identify and discuss the socio-
economic factors associated with obesity in the region.
METHODS
In this review, South Asians are defined as people living in the Indian subcontinent which
consists of the following countries: India, Pakistan, Sri Lanka, Bangladesh, Nepal, Bhutan and
the Maldives. Countries from the Far East (Japan, China etc.) and South East Asia (Malaysia,
Thailand, Singapore etc.) were excluded [10]. There is an active collaboration and mutual
assistance (South Asian Association for Regional Cooperation - SAARC) among these countries
in economic, social, cultural, technical and scientific fields [11]. Despite the existence of
considerable heterogeneity among the inhabitants of South Asia, there are several similarities in
the biological and socio-cultural aspects of the people from this region that allows this group to
be considered as a single unit for the purpose of examination of health issues [12].
Overweight and obesity prevalence data among adults in the South Asian countries studied were
obtained by searching Medline with combinations of the MeSH terms: Obesity and Overweight
as separate main key words for papers published in English between 1 January 1980 and 31
December 2011. Secondly, each key word was divided into subheadings and Epidemiology/EP
included for searching with main key words. Thirdly, the conjunction of the above results was
narrowed down by adding the name of each country (India, Pakistan, Bangladesh, Sri Lanka,
Nepal, Bhutan and Maldives) as key words. A manual search was performed for future evidence
using the reference lists of selected articles and corresponding authors were contacted to obtain
additional data. Furthermore, relevant governmental health and WHO websites were browsed.

52 Chapter 3: Manuscript 2
The primary search was focused on research investigating the prevalence of overweight, obesity
or abdominal obesity in each country. Priority was given to larger (n>2000), nationally
representative samples.
Studies done in the clinical settings and patients with especial medical conditions and limited to
especial groups (e.g. doctors) or age category (e.g. age >65 y) were excluded. Studies of South
Asians living in the non-South Asian countries were excluded.
Initial screening of articles was carried out using abstracts. Unless it was clear from the abstract
that this strategy met the inclusion criteria for the review, the article was rejected. For prevalence
data, the most recent, well-designed and nationally representative or large studies were included.
Trends were plotted by available prevalence data from each country according to gender.
RESULTS
National prevalence of obesity in individual countries (Table 1)
No data were found from Bhutan. Limited nationwide surveys were found in the region and most
recent studies were completed between 2004 and 2006. The STEPS survey in the Maldives [13]
and SLDC study [14] in Sri Lanka reported on prevalence of overweight, obesity and abdominal
obesity using similar anthropometric cut-offs and in a similar period of time. The study in the
Maldives reported the highest prevalence of overweight, obesity and abdominal obesity in the
region with 60.8% of males and 65.5% of females overweight and obese. The overall prevalence
of obesity and abdominal obesity were 43.5% and 40.0% with half the women being obese
(48.1%) and abdominally obese (54.1%) [13]. Sharma et al. recently reported a very high
prevalence of overweight among both Nepalese men (59.1%) and women (61.8%), however they
have reported lower BMI cut-offs to define overweight (≥22 kg/m2) [15]. As per the WHO
definition for overweight in Asian adults (BMI ≥23 kg/m2) a quarter of Sri Lankan adults (M:
22.6%, F: 28.0%) were overweight [14]. In Bangladesh, a large survey undertaken on
reproductive age woman reported levels of overweight of 9.6% and 18.9% among rural and poor

Chapter 3: Manuscript 2 53
urban areas [16]. No nationally representative data are available on men, however data from four
sites in Bangladesh showed around 10% of men have BMI scores above 25 kg/m2 [17]. Results
from the National Health Survey of Pakistan showed a high prevalence of overweight (M: 22.0%
F: 27.9%) and obesity (M: 12.5% F: 18.6) in the early 1990s [18] moreover, authors noted a 2.5
times greater prevalence of obesity among urban than among rural residents [18]. In 2007, a
study on a rural population showed 19.5% and 24.7% obesity levels (BMI ≥25 kg/m2) in men
and women, respectively [19].
Prevalence data in India is more complex. For example, the Indian National Family Health
Survey-3 reported prevalence data on obesity in a large sample (n=111781) across 26 states [20]
with moderate levels of obesity; 9.3% for men and 12.6% for women. However in contrast,
Deepa et al. [21] reported 46.1% and 50.2% overweight and obesity in a study in South India. In
addition, using the Asian waist circumference cut–offs, the same study reported that 35.1% of
men and 56.2% of women had abdominal obesity, a higher level than any other national values
for countries in the region [21]. A study undertaken in six different geographical locations in
India (East, South, North, West/Central) showed different levels of obesity according to rural or
urban residence. In urban areas, obesity levels were as high as 30.7% in men and 38.8% in
women; whilst in rural areas values were 9.4% in men and 14.1% in women. In contrast, obesity
levels in slums were intermediate, 16.7% and 26.1%, for men and women respectively [22].
Similar patterns were reported for abdominal obesity.
Time trends in the prevalence of obesity
No well-designed nationally representative studies were found for the Maldives or Bhutan.
Limited time series information is available for other countries. Prevalence data were plotted in
the time trends according to the methodological similarities of the studies. BMI ≥25 kg/m2 was
used as it was the commonly used cut-off for most of the recent and earlier studies, which allows
54 Chapter 3: Manuscript 2
conclusions to be drawn on weight trends. An obvious upward trend was seen in all countries in
the region (figure 1a and 1b). In Sri Lanka, the age-adjusted prevalence of obesity in both men
and women increased from 7.0% (male) and 13.4% (female) in 1990 to 9.9% (male) and 19.2%
(female) in 2000. A further increase in obesity can be seen in 2005 (M: 16.4%; F: 20.7%)
[23,24] [14]. As obesity data in 1990 and 2000 were taken from an urban area (Colombo,
Maharagama) [23,24], the comparison in 2005 was taken from obesity prevalence in the urban
area [14]. Obesity prevalence in males may have be under-reported in 2000 and 1995 as the
authors used a BMI level of >27 kg/m2 as the obesity cut-off for males but >25 kg/m2 for female
counterparts [23,24].
Although the absolute prevalence of overweight and obesity in Nepal and Bangladesh are
currently the lowest in the region, the relative increases over the last two decades are the highest
in the region. A series of national or regional obesity datasets on ever-married, non-pregnant
women in Bangladesh show a clear positive trend in both urban and rural populations [25]. In
1996, only 2.7% of women had a BMI >25 kg/m2 and within three years the proportion had
reached 4.4%. By 2004, a value three times higher than in 1996 (8.9%) [25] was seen. In Nepal,
the prevalence of obesity among women was 1.6% which increased to 6.4% in 2001, then to
10.1% in 2006. This level of change over such a short period is the highest in the region. Despite
the absence of trend data on the prevalence of overweight and obesity in Pakistan, Shah et al.
[19] conducted two independent cross-sectional population surveys in rural Pakistan in 1995 and
2007. The age-adjusted prevalence of overweight and obesity (BMI >25 kg/m2) increased from
13.9% in 1995 to 19.4% in 2007. In men, the increase was from 15.4% to 19.5%; and in women
from 12.5% to 24.7%.
There are a few nationwide and several regional studies in India over the last few decades,
however, there is no series of national level study to cover all parts of the country. This may be
due to the size of the population and lack of resources. The National Nutrition Monitoring
Chapter 3: Manuscript 2 55
Bureau of India conducted a couple of large studies in nine rural states in India in 2000 [26] and
2005 [27]. The obesity prevalence was 5.7% and 8.2% in men and women respectively in 2000,
which increased to 7.8% and 10.9% in 2005. Although values are low in both circumstances,
obesity levels had increased by 37% and 32% in both men and women respectively over the
five-year period. Some regional studies reported very high levels of obesity, in particular in
urban areas [21,22,28]. However, in India, there is a considerable disparity in the prevalence and
in the time trends in the prevalence of obesity by different geographical regions and residents in
different areas of the same geographical location. A recent review noted the complexity of over
and under-nutrition problems in India [29].
Socio-economic factors associated with prevalence of obesity in the South Asian region
Several similar socio-economic factors are associated with the increase in obesity in the region.
Female sex, middle age, urban residence, higher educational and economic status, physical
inactivity and some dietary habits (Table 2) were positively associated with a high prevalence of
obesity. Yajnik [30] suspects the obesity epidemic may be associated with low birth weight in
Indian babies. In contrast to the above factors, smoking and Tuberculosis were negatively
associated [31]. Many studies have shown that smokers have lower body weights than their non-
smoking counterparts, however in contrast a study by Gosh et al (2006), showed that both ex
smoking and never smoking decreased WHR significantly, whereas smoking increased WHR
[32]. There was considerable variation in the prevalence of obesity according to sub-ethnicity,
region of the country, religion, caste and marital status for women.
DISCUSSION
Historically, under-nutrition and deficiencies have been considered the major health issues in
South Asian countries. Even in the most recent literature, the region is considered to have one of
56 Chapter 3: Manuscript 2
the lowest levels of excess body weight [33]. However, this information alone is misleading
because it does not examine the prevalence, trends and associated factors of obesity in the
region. To our knowledge, this is the first systematic review to discuss prevalence trends and
associated socio-economic factors of obesity in South Asian countries. Despite the very limited
recent nationally representative obesity prevalence data from countries in the Indian
subcontinent, our results show that the prevalence of obesity has reached epidemic levels in
almost every country and is more serious in urban areas. Considering the size of the population
of the region, the number of people who are affected by overweight and obesity represents
numbers well above those in most developed countries. These studies have mainly used Asian
BMI and waist circumference cut-offs (OW ≥23 kg/m2; Ob ≥25 kg/m2) to define overweight,
obesity and abdominal obesity (waist circumference: M ≥90 cm; F ≥80 cm) [34,35]. However, a
growing body of evidence suggests that BMI ≥23 kg/m2 is not sensitive enough to identify the
obesity-associated disease risk in South Asian populations.
BMI and waist circumference for obesity in South Asians
Studies from India [36], Pakistan [18], and Sri Lanka [37] have shown that a BMI of 21 kg/m2
would be the appropriate anthropometric cut-off level to identify overweight. Similarly, an
Indian consensus statement also suggested a BMI of ≥21 kg/m2 as the diagnostic cut-off value
for overweight for Asian Indians [38]. Moreover, multi-ethnic studies on body composition [39]
and metabolic risk factor analysis [40] showed that a BMI of 21 kg/m2 is the most appropriate
anthropometric cut-off for South Asian ethnic groups. Considering all factors, if obesity was
defined using a lower BMI level, the prevalence of obesity in the respective countries would be
substantially increased. Similarly, lower abdominal obesity cut-offs have been recommended for
the South Asians [38]. However, a considerable portion of Nepalese and Bhutanese are from

Chapter 3: Manuscript 2 57
Chinese origin, therefore lower anthropometric cut-offs are not equally suitable for all ethnic
groups.
There has been considerable delays between data collection and the publication of findings in
some countries, for instance a 16-year gap between data collection and publication date in a
Pakistan national survey [18]. The rate of increase in the obesity epidemic is very fast globally,
but particularly in the South Asian region, so published reports to date may significantly
underestimate the current prevalence.
Socio-economic factors
If environmental factors have a major role in triggering increased body weight subsequent to
increased prevalence of overweight and obesity, one would expect a lower prevalence of obesity
in rural areas, where people follow a traditional lifestyle. Such an urban–rural difference has
been reported in almost all countries in the region. For example in Sri Lanka, the prevalence of
obesity in urban areas is three times that of rural areas [14] and similar patterns have been
reported in India [22] and Pakistan [18]. However, Shah et al. reported that in rural Pakistan, the
age-adjusted prevalence of overweight and obesity also increased from 13.9% in 1995 to 19.4%
in 2007 [19]. These results suggest that the rate of obesity might also increase in rural
communities as they become more urbanised. Between 1990 and 2000, the mean BMI increased
by nearly 2.5 kg/m2 in rural Sri Lanka [41]. Recent economic development has improved the
availability and accessibility to foods, which has occurred simultaneously with an increased
quality of life in many countries. Advances in both technical and agricultural sectors has helped
to reduce under-nutrition, however, the increased availability of energy-dense foods may lead to
weight gain and subsequently, obesity. This transition has occurred rapidly, particularly in urban
regions of South Asian countries, which compares with a more gradual advancement in many
affluent countries. Interestingly, most South Asian meals consist of excess carbohydrate [42].
58 Chapter 3: Manuscript 2
In 2007-2008, the prevalence of obesity was estimated to be 35.5% in US women [43]. Despite
obesity prevalence among US women being high, over a 10-year period there has not been a
significant upward trend. In comparison, the obesity level increased six-fold in Nepalese women
between 1996 and 2006 [25]. Thus, despite the prevalence of obesity in South Asian countries
being lower that in the USA, the rate at which overweight and obesity has increased during
recent decades (Figures 1 and 2), and the likelihood of further increases, provides substantial
grounds for concern. Obesity trend data from the Asia-Pacific region also shows low absolute
values of obesity in Asian countries such as China and Japan compared to Australia but with
rapid increases in the relative values during the last decades [44].
Worldwide, more females are overweight and obese compared to males [33]. In the UK, an
estimated 25% of women and 23% of men were obese in 2002 [45], while in the US, 32.2% of
men and 35.5% of women suffered from obesity in 2007/2008 [43]. In contrast, the gender
difference in prevalence of obesity in South Asia is significantly higher, for instance, in rural
Bangladesh the prevalence of obesity in women is 2.5 times higher than in males [46]. Socio-
economic characteristics of the epidemic of obesity in South Asia also differ from those reported
in other parts of the world. In South Asia, the highest prevalence is reached in the middle-aged
(30-50 years) group whereas in the UK, obesity prevalence tends to increase progressively with
age (up to 64 years) [45]. In South Asia, obesity is more common in people with high
educational levels, high income or wealth and in skilled workers [14,18,47]. In contrast, the
opposite is seen in the UK [45]. Unlike more affluent countries, a considerable proportion of
South Asian populations suffer from under-nutrition [25], with people with higher education and
income having relatively higher accessibility to energy and nutrient-rich foods. Interestingly,
religion, caste, sub-ethnicity, region of location within the country and marital status are
Chapter 3: Manuscript 2 59
significant socio-economic factors leading to obesity in the region [18,29,31,47]. This is partly
due to the abovementioned factors being strongly associated with their cultural dietary patterns
and freedom of movement or physical activity levels [47]. It is very important to identify key
socio-economic factors prior to initiating weight loss programmes as complex associations
between obesity and socio-economic factors may make the implementation of weight loss
strategies in South Asians more challenging. Prevalence of diabetes is has reached to epidemic
portion in the south Asia [48].
LIMITATIONS
Interpretation of obesity prevalence and trends in the region is difficult due to use of various
anthropometric cut-offs. For example, older studies defined overweight and obesity using global
BMI cut-offs of ≥25 kg/m2 for overweight and ≥30 kg/m2 for obesity whereas in recent studies
ethnic-specific anthropometric cut-offs have been used. Secondly, overweight has been
classified differently in the literature, with some researchers defining overweight/obesity using
one value. For example, in the Maldives study, overweight is considered as a BMI of 23 kg/m2
and above [13], whereas in a Bangladeshi study [49] overweight was classified using the
traditional range (25.0-29.9 kg/m2). Another limitation is that different studies have used various
age groups although this review focused only on adult populations, whereas some countries have
included older adolescents [18,20,49] and the elderly for prevalence studies [14,18,21]. The
inclusion of younger individuals and also older adults may lead to underestimates of the
prevalence of obesity in adults. Similarly, in some countries, prevalence data were restricted to
one gender [25], a specific area of residence [50] and a single time point [13], each of which
limits interpretation of the general obesity prevalence and trends in the region. Prospective
studies are needed to indentify the incidence of the obesity in the region.
60 Chapter 3: Manuscript 2
CONCLUSION
It is evident that overweight and obesity has already reached epidemic proportions in South
Asian countries and based on current trends, the longer-term prognosis is even more threatening.
The widespread use of more appropriate lower anthropometric cut-offs may further increase
current estimates. Furthermore, obesity in South Asia has a unique cluster of associated socio-
economical factors. Immediate action is required in both prevention and management with the
engagement of healthcare workers, policy makers and educators before overweight and obesity
levels achieve more alarming proportions.
Acknowledgements
We are grateful to Mr Peter Sondergeld, who helped us in literature searching. Conflict of interest
The authors declare no conflict of interest.
Chapter 3: Manuscript 2 61
REFERENCES
1 WHO: Obesity and overweight; in WHO (ed): Global Strategy on Diet, Physical Activity
and Health, 2010, 2010,
2 Caballero B: The global epidemic of obesity: An overview. Epidemiologic reviews
2007;29:1.
3 McLaren L: Socioeconomic status and obesity. Epidemiologic reviews 2007
4 Snyder JD, Merson MH: The magnitude of the global problem of acute diarrhoeal
disease: A review of active surveillance data. Bull World Health Organ 1982;60:605-613.
5 Muller O, Krawinkel M: Malnutrition and health in developing countries. Canadian
Medical Association Journal 2005;173:279.
6 Misra A, Khurana L: Obesity-related non-communicable diseases: South asians vs white
caucasians. International Journal of Obesity 2010
7 Ghaffar A, Reddy K, Singhi M: Burden of non-communicable diseases in south asia.
British Medical Journal 2004;328:807.
8 The Central Intelligence Agency: The world factbook: South Asia, 2010,
9 Yoon K, Lee J, Kim J, Cho J, Choi Y, Ko S, Zimmet P, Son H: Epidemic obesity and
type 2 diabetes in asia. The Lancet 2006;368:1681-1688.
10 Sharma M: Designing effective health education interventions for preventing obesity in
South Asian Americans. Californian Journal of Health Promotion 2006;4:119-128.
11 SAARC: South asian association for regional cooperation, 2009, 2010,
12 Ahmed S, Lemkau J: Cultural issues in the primary care of south asians. Journal of
Immigrant Health 2000;2:89-96.
13 Aboobakur M, Latheef A, Mohamed A, Moosa S, Pandey R, Krishnan A, Prabhakaran
D: Surveillance for non-communicable disease risk factors in maldives: Results from the first
steps survey in male. International Journal of Public Health:1-8.
14 Katulanda P, Jayawardena MA, Sheriff MH, Constantine GR, Matthews DR: Prevalence
of overweight and obesity in sri lankan adults. Obes Rev 2010
15 Sharma SK, Ghimire A, Radhakrishnan J, Thapa L, Shrestha NR, Paudel N, Gurung K, R
M, Budathoki A, Baral N, Brodie D: Prevalence of hypertension, obesity, diabetes, and
metabolic syndrome in nepal. International Journal of Hypertension 2011;821971. Epub 2011
Apr 19.
62 Chapter 3: Manuscript 2
16 Shafique S, Akhter N, Stallkamp G, de Pee S, Panagides D, Bloem MW: Trends of
under- and overweight among rural and urban poor women indicate the double burden of
malnutrition in bangladesh. International Journal of Epidemiology 2007;36:449-457.
17 Razzaque A, Nahar L, Van Minh H, Ng N, Juvekar S, Ashraf A, Ahmed SM,
Soonthornthada K, Kanungsukkasem U, Huu Bich T: Social factors and overweight: Evidence
from nine asian indepth network sites. Glob Health Action 2009;2
18 Jafar TH, Chaturvedi N, Pappas G: Prevalence of overweight and obesity and their
association with hypertension and diabetes mellitus in an indo-asian population. CMAJ:
Canadian Medical Association Journal = Journal De L'association Medicale Canadienne
2006;175:1071-1077.
19 Shah S, Hussain A, Jafar T, Reeder B: Obesity in a south asian population: Trends
between 1995 and 2007. Obesity Reviews 2010;11:59.
20 IIPS and Macro International: National family health survey (nfhs-3), 2005–06: India; in
Sciences IIfP (ed). Mumbai, 2007,
21 Deepa M, Farooq S, Deepa R, Manjula D, Mohan V: Prevalence and significance of
generalized and central body obesity in an urban asian indian population in chennai, india (cures:
47). European journal of clinical nutrition 2009;63:259-267.
22 Mohan V, Mathur P, Deepa R, Deepa M, Shukla DK, Menon GR, Anand K, Desai NG,
Joshi PP, Mahanta J, Thankappan KR, Shah B: Urban rural differences in prevalence of self-
reported diabetes in india--the who-icmr indian ncd risk factor surveillance. Diabetes research
and clinical practice 2008;80:159-168.
23 Fernando D, Siribaddana S, De Silva D: Impaired glucose tolerance and diabetes mellitus
in a suburban sri lankan community. British Medical Journal 1994;70:347.
24 Malavige G, de Alwis N, Weerasooriya N, Fernando D, Siribaddana S: Increasing
diabetes and vascular risk factors in a sub-urban sri lankan population. Diabetes research and
clinical practice 2002;57:143-145.
25 Balarajan Y, Villamor E: Nationally representative surveys show recent increases in the
prevalence of overweight and obesity among women of reproductive age in bangladesh, nepal,
and india. The Journal Of Nutrition 2009;139:2139-2144.
26 NNMB: Diet and nutritional status of rural population; in BUREAU NNM (ed): NNMB
Technical Report 2002,
27 NNMB: Diet and nutritional status of population and prevalence of hypertension
amongst adults in rural areas.; in Bureau NNM (ed): National Nutrition Monitoring Bureau
Technical Report, 2007,
Chapter 3: Manuscript 2 63
28 Singh RB, Pella D, Mechirova V, Kartikey K, Demeester F, Tomar RS, Beegom R,
Mehta AS, Gupta SB, De Amit K, Neki NS, Haque M, Nayse J, Singh S, Thakur AS, Rastogi
SS, Singh K, Krishna A: Prevalence of obesity, physical inactivity and undernutrition, a triple
burden of diseases during transition in a developing economy. The five city study group. Acta
Cardiologica 2007;62:119-127.
29 Wang Y, Chen HJ, Shaikh S, Mathur P: Is obesity becoming a public health problem in
india? Examine the shift from under- to overnutrition problems over time. Obesity Reviews: An
Official Journal Of The International Association For The Study Of Obesity 2009;10:456-474.
30 Yajnik CS: Obesity epidemic in india: Intrauterine origins? The Proceedings Of The
Nutrition Society 2004;63:387-396.
31 Subramanian SV, Kawachi I, Smith GD: Income inequality and the double burden of
under- and overnutrition in india. Journal Of Epidemiology And Community Health
2007;61:802-809.
32 Ghosh A: Effects of socio-economic and behavioural characteristics in explaining central
obesity--a study on adult asian indians in calcutta, india. Collegium Antropologicum
2006;30:265-271.
33 Balkau B, Deanfield J, Després J, Bassand J, Fox K, Smith Jr S, Barter P, Tan C, Van
Gaal L, Wittchen H: International day for the evaluation of abdominal obesity (idea): A study of
waist circumference, cardiovascular disease, and diabetes mellitus in 168 000 primary care
patients in 63 countries. Circulation 2007;116:1942.
34 WHO expert consultation: Appropriate body-mass index for asian populations and its
implications for policy and intervention strategies. The Lancet 2004;363:157-163.
35 WHO: Obesity: Preventing and managing the global epidemic. Report of a who
consultation.: World Health Organ Tech Rep Ser, 2000, 894, pp i–xii, 1–253.
36 Misra A, Vikram N, Gupta R, Pandey R, Wasir J, Gupta V: Waist circumference cutoff
points and action levels for asian indians for identification of abdominal obesity. International
Journal of Obesity 2005;30:106-111.
37 Katulanda P, Jayawardena MA, Sheriff MH, Matthews DR: Derivation of
anthropometric cut-off levels to define cvd risk in sri lankan adults. Br J Nutr 2011;105:1084-
1090.
38 Misra A, Chowbey P, Makkar BM, Vikram NK, Wasir JS, Chadha D, Joshi SR, Sadikot
S, Gupta R, Gulati S, Munjal YP: Consensus statement for diagnosis of obesity, abdominal
obesity and the metabolic syndrome for asian indians and recommendations for physical activity,
medical and surgical management. J Assoc Physicians India 2009;57:163-170.
64 Chapter 3: Manuscript 2
39 Deurenberg-Yap M, Schmidt G, Van Staveren W, Deurenberg P: The paradox of low
body mass index and high body fat percentage among chinese, malays and indians in singapore.
International Journal of Obesity 2000;24:1011-1017.
40 Razak F, Anand S, Shannon H, Vuksan V, Davis B, Jacobs R, Teo K, McQueen M,
Yusuf S: Defining obesity cut points in a multiethnic population. Circulation 2007;115:2111.
41 Illangasekera U, Rambodagalla S, Tennakoon S: Temporal trends in the prevalence of
diabetes mellitus in a rural community in sri lanka. The Journal of the Royal Society for the
Promotion of Health 2004;124:92.
42 Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Hills AP: Consumption of sri
lankan adults: An appraisal of serving characteristics Public Health Nutrition 2012;FirstView
Article : pp 1-6
43 Flegal K, Carroll M, Ogden C, Curtin L: Prevalence and trends in obesity among us
adults, 1999-2008. Jama 2010;303:235.
44 The burden of overweight and obesity in the asia-pacific region. Obesity Reviews: An
Official Journal Of The International Association For The Study Of Obesity 2007;8:191-196.
45 Rennie KL, Jebb SA: Prevalence of obesity in great britain. Obesity Reviews 2005;6:11-
12.
46 Zaman MM, Yoshiike N: Prevalence of overweight defined by body mass index in a
rural adult population of bangladesh. Journal Of Health, Population, And Nutrition 2003;21:162-
163.
47 Garg C, Khan SA, Ansari SH, Garg M: Prevalence of obesity in indian women. Obesity
Reviews: An Official Journal Of The International Association For The Study Of Obesity
2010;11:105-108.
48 Jayawardena R, Ranasinghe P, Byrne N, Soares M, Katulanda P, Hills A: Prevalence and
trends of the diabetes epidemic in south asia: A systematic review and meta-analysis. BMC
Public Health 2012;12:380.
49 Khan MMH, Kraemer A: Factors associated with being underweight, overweight and
obese among ever-married non-pregnant urban women in bangladesh. Singapore Medical
Journal 2009;50:804-813.
50 Vaidya AK, Pokharel PK, Nagesh S, Karki P, Kumar S, Majhi S: Association of obesity
and physical activity in adult males of dharan, nepal. Kathmandu University Medical Journal
(KUMJ) 2006;4:192-197.
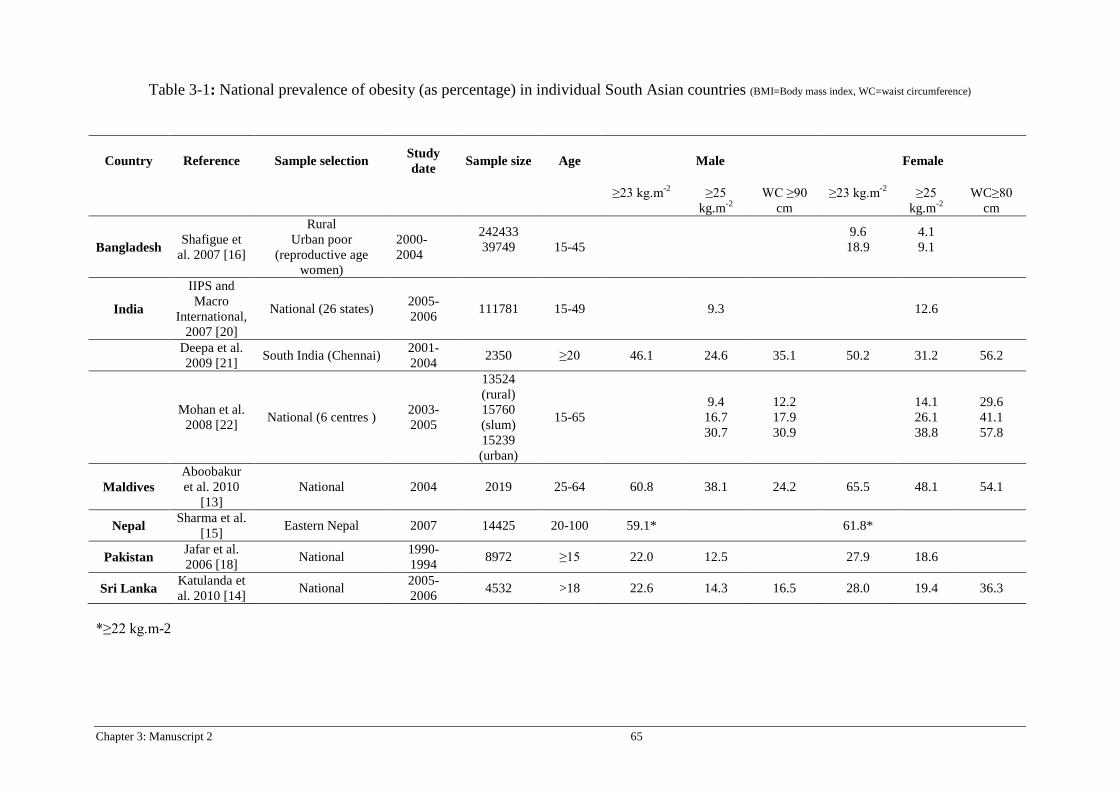
Chapter 3: Manuscript 2 65
Table 3-1: National prevalence of obesity (as percentage) in individual South Asian countries (BMI=Body mass index, WC=waist circumference)
*≥22 kg.m-2
Country Reference Sample selection Study date Sample size Age Male Female
≥23 kg.m-2
≥25
kg.m-2 WC ≥90
cm ≥23 kg.m-2
≥25
kg.m-2 WC≥80
cm
Bangladesh Shafigue et al. 2007 [16]
Rural Urban poor
(reproductive age women)
2000-2004
242433 39749
15-45
9.6 18.9
4.1 9.1
India
IIPS and Macro
International, 2007 [20]
National (26 states) 2005-2006 111781 15-49 9.3 12.6
Deepa et al. 2009 [21] South India (Chennai) 2001-
2004 2350 ≥20 46.1 24.6 35.1 50.2 31.2 56.2
Mohan et al. 2008 [22] National (6 centres ) 2003-
2005
13524 (rural) 15760 (slum) 15239 (urban)
15-65 9.4
16.7 30.7
12.2 17.9 30.9
14.1 26.1 38.8
29.6 41.1 57.8
Maldives Aboobakur et al. 2010
[13] National 2004 2019 25-64 60.8 38.1 24.2 65.5 48.1 54.1
Nepal Sharma et al. [15] Eastern Nepal 2007 14425 20-100 59.1* 61.8*
Pakistan Jafar et al. 2006 [18] National 1990-
1994 8972 ≥15 22.0 12.5 27.9 18.6
Sri Lanka Katulanda et al. 2010 [14] National 2005-
2006 4532 >18 22.6 14.3 16.5 28.0 19.4 36.3
66 Chapter 3: Manuscript 2
• Overweight and obesity have reached epidemic proportions in many part of South Asia.
• Obesity associated metabolic burden is substantial among South Asians, therefore, lower BMI and waist circumference cut-offs are more appropriate.
• Culturally-appropriate preventive strategies are necessary to handle this epidemic.
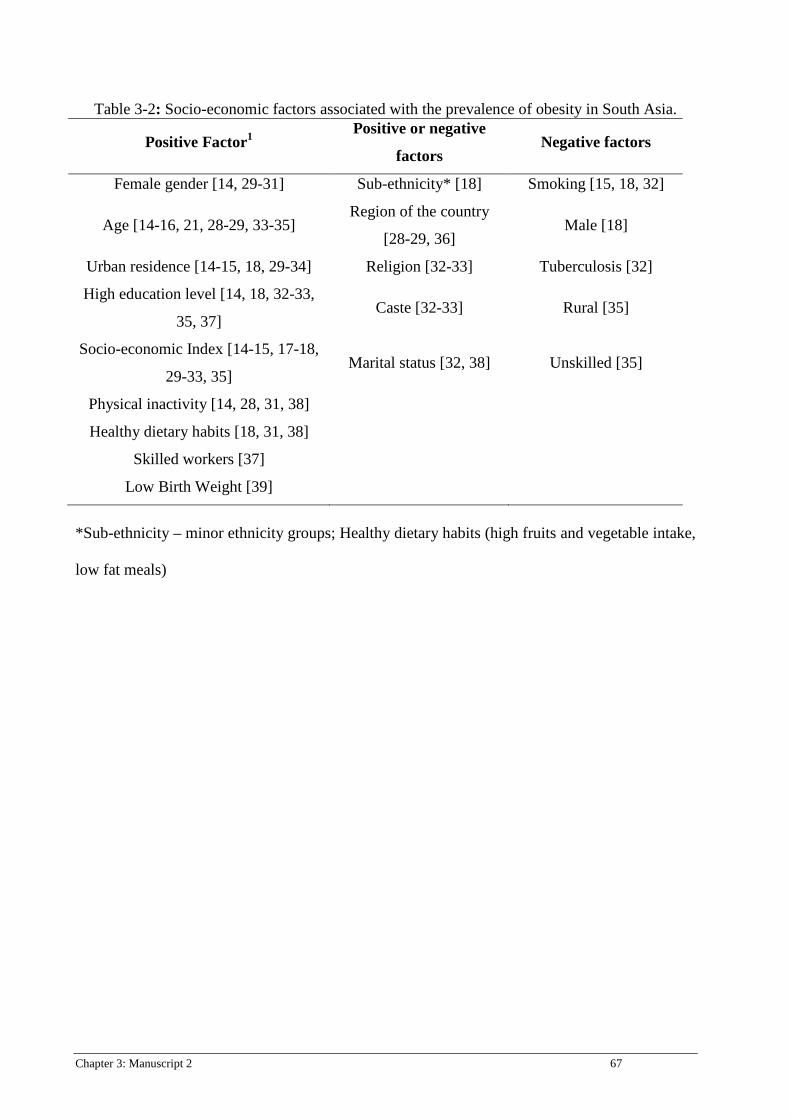
Chapter 3: Manuscript 2 67
Table 3-2: Socio-economic factors associated with the prevalence of obesity in South Asia.
Positive Factor1 Positive or negative
factors Negative factors
Female gender [14, 29-31] Sub-ethnicity* [18] Smoking [15, 18, 32]
Age [14-16, 21, 28-29, 33-35] Region of the country
[28-29, 36] Male [18]
Urban residence [14-15, 18, 29-34] Religion [32-33] Tuberculosis [32]
High education level [14, 18, 32-33,
35, 37] Caste [32-33] Rural [35]
Socio-economic Index [14-15, 17-18,
29-33, 35] Marital status [32, 38] Unskilled [35]
Physical inactivity [14, 28, 31, 38]
Healthy dietary habits [18, 31, 38]
Skilled workers [37]
Low Birth Weight [39]
*Sub-ethnicity – minor ethnicity groups; Healthy dietary habits (high fruits and vegetable intake,
low fat meals)
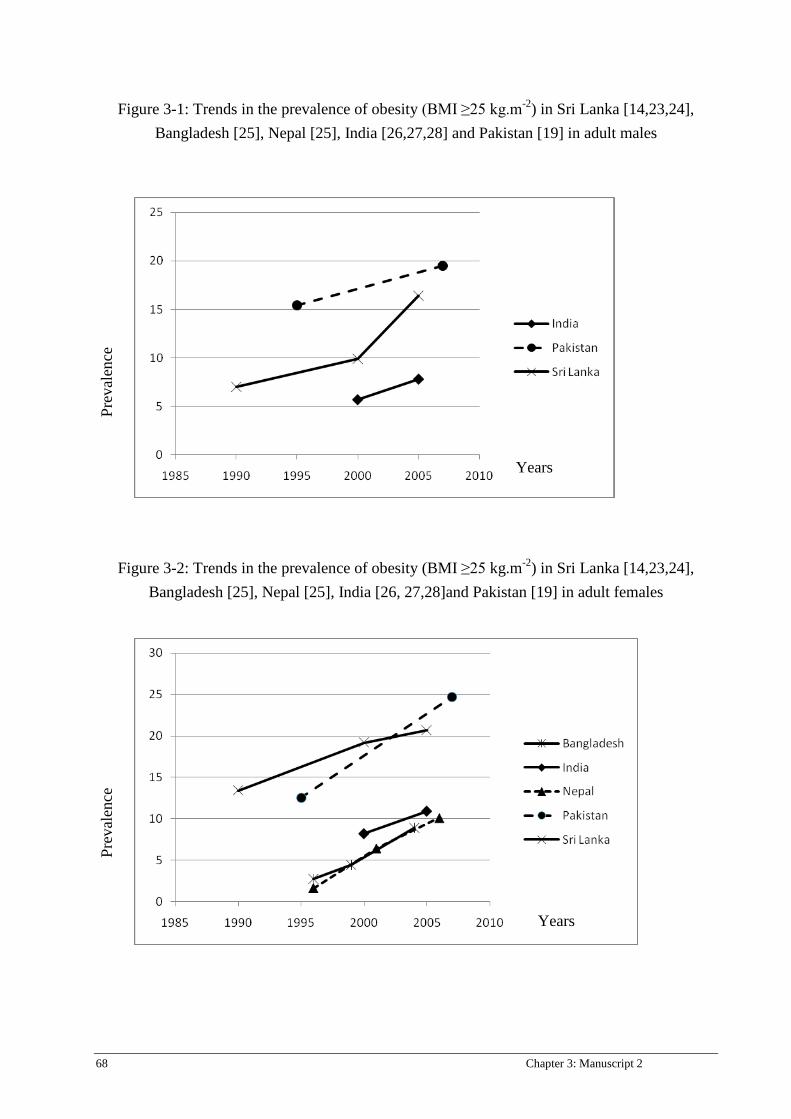
68 Chapter 3: Manuscript 2
Figure 3-1: Trends in the prevalence of obesity (BMI ≥25 kg.m-2) in Sri Lanka [14,23,24], Bangladesh [25], Nepal [25], India [26,27,28] and Pakistan [19] in adult males
Figure 3-2: Trends in the prevalence of obesity (BMI ≥25 kg.m-2) in Sri Lanka [14,23,24], Bangladesh [25], Nepal [25], India [26, 27,28]and Pakistan [19] in adult females
Prev
alen
ce
Prev
alen
ce
Years
Years

Chapter 4: Manuscript 3 69
Chapter 4: Manuscript 3
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Food consumption of Sri Lankan adults: an appraisal of serving characteristics Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
70 Chapter 4: Manuscript 3
TITLE PAGE
Food consumption of Sri Lankan adults: an appraisal of serving characteristics Ranil Jayawardena1,2, Nuala M. Byrne1, Mario J. Soares3, Prasad Katulanda2, Andrew P. Hills4 1Institute of Health and Biomedical Innovation, Queensland University of Technology, Brisbane, Queensland, Australia 2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka 3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health Sciences, Curtin University, Perth, WA, Australia 4Mater Mothers’ Hospital, Mater Medical Research Institute and Griffith Health Institute, Griffith University, Brisbane, Queensland, Australia
Citation
R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. (2012) Food consumption of Sri
Lankan adults: an appraisal of serving characteristics Public Health Nutrition: 16 (4); 653-658
Chapter 4: Manuscript 3 71
ABSTRACT
Objective
The main aim of this study was to identify food consumption in Sri Lankan adults based on
serving characteristics.
Design
This is a cross-sectional study. Fruits, vegetables, starch, meat, pulses, dairy products and sugar
were assessed in the diet with portion sizes estimated using standard methods.
Setting
Randomly selected twelve clusters from Sri Lanka Diabetes Cardiovascular Study.
Subjects
Six hundred non-institutional adults.
Results
The daily intake of fruits (0.4), vegetables (1.7) and dairy (0.4) portions were well below
national recommendations. Only 3.5% of adults consumed the recommended five fruits and
vegetables per day and over one third of the population consumed no dairy products, and less
than 1% of adults consumed 2 portions per day. In contrast, Sri Lankan adults consumed over 14
portions of starch, and 3.5 portions of added sugars daily. Almost 70% of those studied exceeded
the upper limit of the recommendations for starch intake. The total number of meat and pulse
portions was 2.78 per day.
Conclusion
Dietary guidelines emphasize the importance of a balanced and varied diet however a substantial
proportion of the Sri Lankan population studied failed to achieve such a recommendation. Health
promotion should be focused on improving healthier dietary habits among this population.
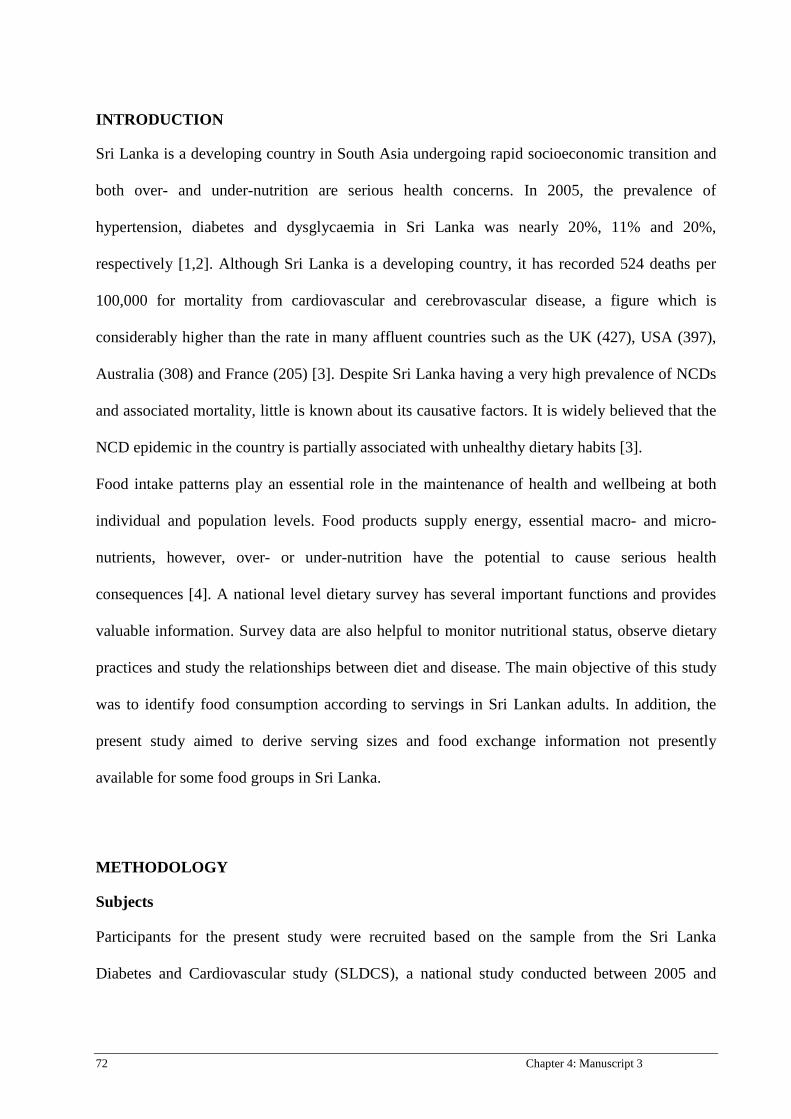
72 Chapter 4: Manuscript 3
INTRODUCTION
Sri Lanka is a developing country in South Asia undergoing rapid socioeconomic transition and
both over- and under-nutrition are serious health concerns. In 2005, the prevalence of
hypertension, diabetes and dysglycaemia in Sri Lanka was nearly 20%, 11% and 20%,
respectively [1,2]. Although Sri Lanka is a developing country, it has recorded 524 deaths per
100,000 for mortality from cardiovascular and cerebrovascular disease, a figure which is
considerably higher than the rate in many affluent countries such as the UK (427), USA (397),
Australia (308) and France (205) [3]. Despite Sri Lanka having a very high prevalence of NCDs
and associated mortality, little is known about its causative factors. It is widely believed that the
NCD epidemic in the country is partially associated with unhealthy dietary habits [3].
Food intake patterns play an essential role in the maintenance of health and wellbeing at both
individual and population levels. Food products supply energy, essential macro- and micro-
nutrients, however, over- or under-nutrition have the potential to cause serious health
consequences [4]. A national level dietary survey has several important functions and provides
valuable information. Survey data are also helpful to monitor nutritional status, observe dietary
practices and study the relationships between diet and disease. The main objective of this study
was to identify food consumption according to servings in Sri Lankan adults. In addition, the
present study aimed to derive serving sizes and food exchange information not presently
available for some food groups in Sri Lanka.
METHODOLOGY
Subjects
Participants for the present study were recruited based on the sample from the Sri Lanka
Diabetes and Cardiovascular study (SLDCS), a national study conducted between 2005 and
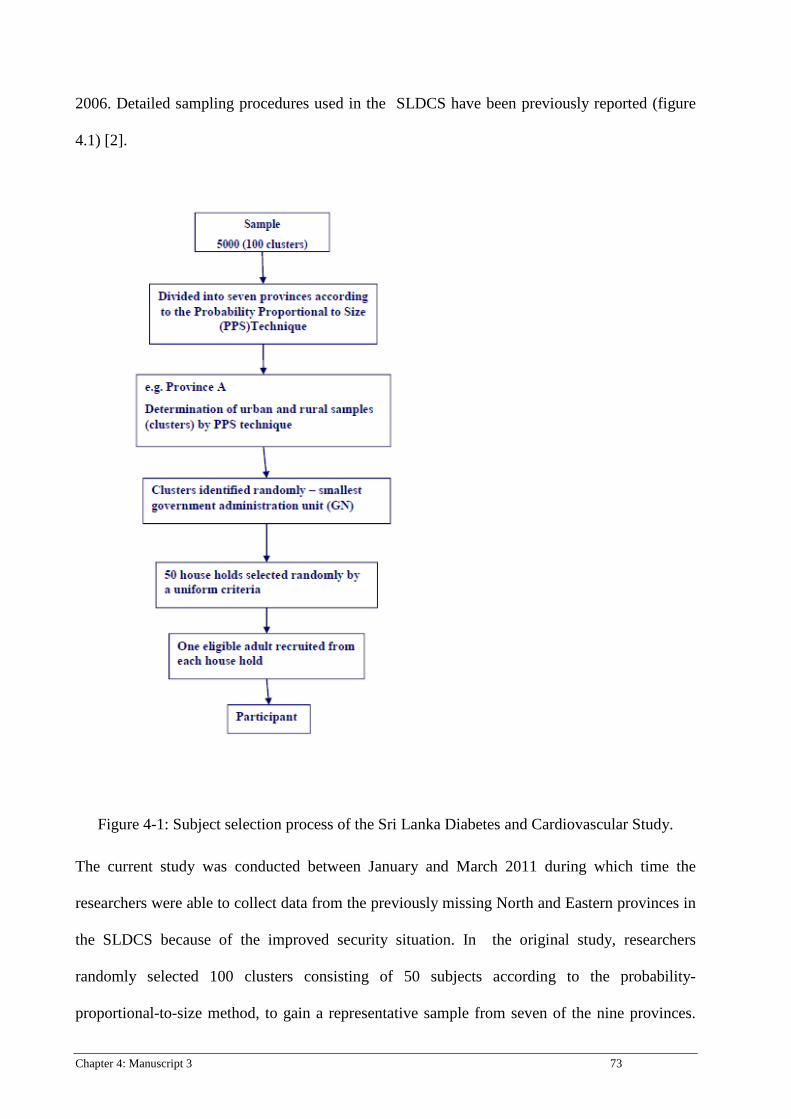
Chapter 4: Manuscript 3 73
2006. Detailed sampling procedures used in the SLDCS have been previously reported (figure
4.1) [2].
Figure 4-1: Subject selection process of the Sri Lanka Diabetes and Cardiovascular Study.
The current study was conducted between January and March 2011 during which time the
researchers were able to collect data from the previously missing North and Eastern provinces in
the SLDCS because of the improved security situation. In the original study, researchers
randomly selected 100 clusters consisting of 50 subjects according to the probability-
proportional-to-size method, to gain a representative sample from seven of the nine provinces.

74 Chapter 4: Manuscript 3
From the 100 clusters, ten were randomly selected stratifying to the area of residence and
ethnicity. To address the gap in national data from the remaining two provinces, we selected one
cluster of 50 participants from the North and East by using ‘Village Office Units’ voter lists to
randomly select one household. The remaining 49 households were selected applying the
uniform method used in the SLDCS. In summary, the total sample in the present study
comprised 600 subjects (500 from previous SLDCS areas and 100 additional from the Northern
and Eastern provinces). Figure 2 shows the data collecting sites. Those who were pregnant,
lactating, acutely ill or on a therapeutic diet were excluded. The present study was approved by
the Ethics Review Committee, Faculty of Medicine, University of Colombo, Sri Lanka.
Measurements
The selected households were initially contacted via telephone by the study team who provided
information regarding the study and verbal consent was taken. Where telephone facilities or
contact phone numbers were unavailable, households were visited by the study team with prior
postal notice. Subsequently, households were visited on a random day to minimize bias for food
selection. Dietary and demographic details were obtained after final written informed consent
was obtained. An interviewer-administered questionnaire was used for data collection.
Information regarding socio-demographic factors, timing of daily routines and meals were
obtained.
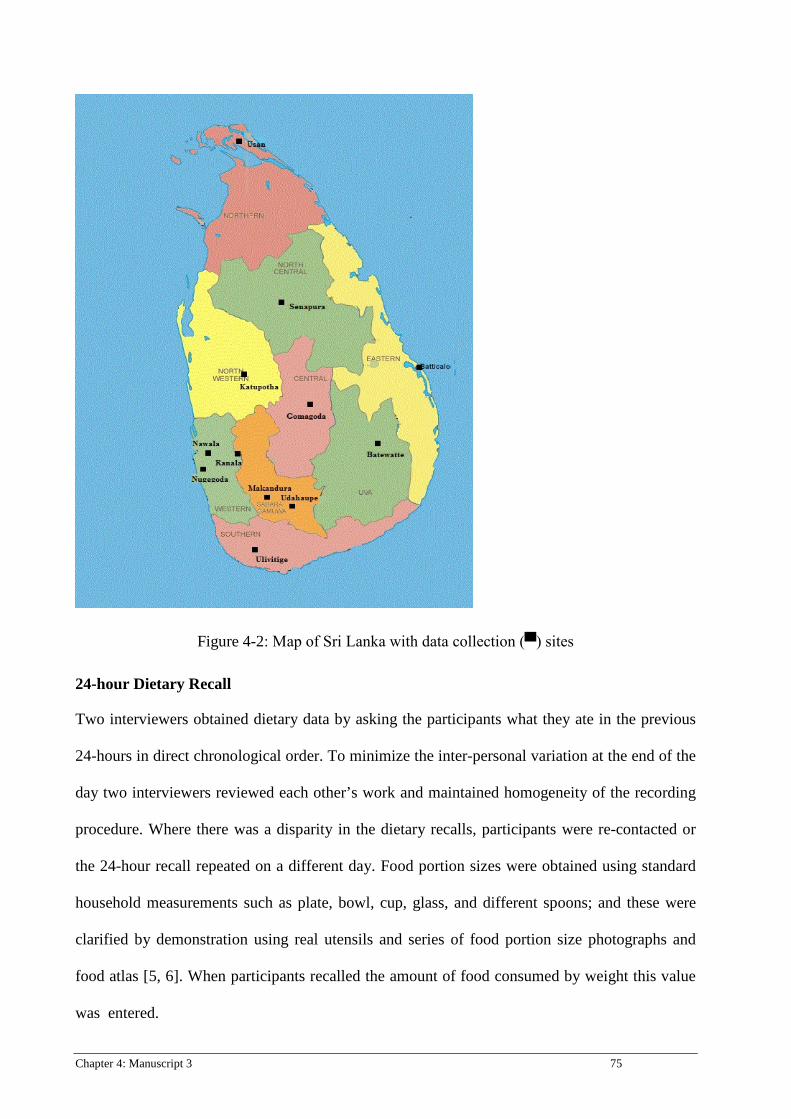
Chapter 4: Manuscript 3 75
Figure 4-2: Map of Sri Lanka with data collection (▀) sites
24-hour Dietary Recall
Two interviewers obtained dietary data by asking the participants what they ate in the previous
24-hours in direct chronological order. To minimize the inter-personal variation at the end of the
day two interviewers reviewed each other’s work and maintained homogeneity of the recording
procedure. Where there was a disparity in the dietary recalls, participants were re-contacted or
the 24-hour recall repeated on a different day. Food portion sizes were obtained using standard
household measurements such as plate, bowl, cup, glass, and different spoons; and these were
clarified by demonstration using real utensils and series of food portion size photographs and
food atlas [5, 6]. When participants recalled the amount of food consumed by weight this value
was entered.
76 Chapter 4: Manuscript 3
Data entry and analysis
The daily food intake was divided into seven food groups, namely 1) Cereal or equivalents
(starchy food); 2) Vegetables; 3) Fruits; 4) Meat or alternatives; 5) Pulses; 6) Dairy, and 7)
Added sugar. Detailed methodology regarding the translation of food eaten into the respective
food groups is provided in Appendix 1 (after this manuscript).
Method for translating food consumed into food group servings
All food recorded in 24-hour recall by each participant was assigned to one of the seven major
food groups defined above. Food was recorded either in household measures (cups, spoons etc.)
or by weight in the 24 hour recall and was translated into serving size for of each food
consumed. Thus, weight of food in grams or amount of household measure of food was divided
by weight of one serving or amount of household measure for one serving and summed to derive
servings of each food group. Food which was a mixture of several food types was disaggregated
before ingredients were categorized into appropriate food groups. An example of disaggregation
is illustrated in figure 4-3. A similar method was used for the US population for food grouping
when food mixtures required disaggregation [7]. The servings of food consumed in mixed foods
were calculated by modifying existing recipe files to develop a cascaded recipe file with multiple
levels of breakdown. Common recipes were accepted after checking for face validity by
consulting nutritionists and when in doubt, respective households were contacted [8]. For
uncommon food items, detailed recipes were collected at the time of the 24-hour dietary recall
from participants or other responsible person from each household.
Statistics
Average daily portion sizes were calculated as the total portion size divided by the number of
participants. The sum of vegetable and fruit portions were divided to obtain average daily fruit

Chapter 4: Manuscript 3 77
and vegetable consumption, and the same method was used to calculate average daily meat and
pulse intake. We analyzed the mean daily consumption of each food group according to gender.
Two sample t-tests were used to determine whether the mean values differed between the
genders. Data were analyzed using SPSS version 14 (SPSS Inc., Chicago,IL, USA) statistical
package. In all analyses a p value <0.05 was considered statistically significant.
RESULTS
Sample size was 490 (with a response rate of 82%), of which 34.5% (n=169) were males. The
socio-demographic profile of the study population is shown in Table 4.1.
The estimated mean daily servings from the five major pyramid food groups from the random
24-hour dietary recall, according to gender is shown in Table 2. In addition, sub-categories of
protein types, namely pulses and meat and alternatives, and added sugar are also reported. Mean
intake of fruits (0.43 portions/day) and vegetables (1.73 portions/day) were well below minimum
recommendations (fruits >2 portions; vegetables >3 portions). The total of fruit and vegetable
intake was 2.16 portions per day. Daily consumption of meat or alternatives was 1.75 portions
and the sum of meat alternatives and pulses was 2.78 portions per day. On average, Sri Lankan
adults consumed over 14 portions of starch daily, moreover males consumed five more cereal
portions compared to females. Sri Lankan adults consumed on average, 3.5 portions of added
sugars per day. Table 3 compares food consumption of Sri Lankan adults with national [9] and
international (US) recommendations [10].
We identified considerable variations in consumption frequency for each food type and their
portion size in the study population. Table 4 illustrates that participants reported an intake of
different portion sizes for main food groups and their combinations. Starchy foods were
consumed by everybody; and over 88% met the minimum daily recommendations. Importantly,
nearly 70% of adults exceeded the maximum daily recommendation for starch portions per day

78 Chapter 4: Manuscript 3
(11/day). More than 12% of men consumed ≥25 starch servings per day. In contrast to their
starch consumption, participants reported a very low intake of other food groups (Table 4). Only
11.6%, 2.1% and 3.5% of adults consume the minimum daily recommended servings of
vegetables, fruits and, combined fruit and vegetable servings, respectively. Six out of ten adult
Sri Lankans sampled did not consume any fruit. Milk and dairy consumption was extremely low,
over one third of the population did not have any dairy products and less than 1% of adults
consumed 2 portions per day. A quarter of Sri Lankans did not report consumption of meat and
pulses. Regarding protein consumption, 36.2% attained the minimum Sri Lankan
recommendation of protein; and significantly more men achieved the recommendation of ≥3
meat or alternative servings per day (M:42.6%; F:32.8%, p<0.05).
DISCUSSION
Recently, the WHO STEP survey reported on some dietary aspects from one health area in the
Western Province [11] but apart from this the present study represents the first national level
dietary survey undertaken in Sri Lanka to obtain habitual dietary intake data of the general
population. As the UK National Nutrition and Dietary Survey (NDNS) collected dietary details
from 1724 participants from a population of 60 million; we believe that the sample size of 600
used in the current study is within adequate limits.
During the last 5 years, Sri Lanka has faced significant urbanization and this has resulted in
some previous study clusters changing from rural to urban status. Whilst the present study
population is reasonably representative of all major ethnic groups in the country, there was a
higher proportion of urban living, mean age and participants with a higher mean BMI compared
to previous surveys [12]. Our results showed a low mean daily intake of fruit and vegetables
amongst Sri Lankan adults (2.16 portions) compared to the US (3.0) and France (3.6) [13]. The

Chapter 4: Manuscript 3 79
low intake of fruits and vegetables may be a contributing factor to the high prevalence of diet-
associated NCDs such as diabetes, non-alcoholic fatty liver and cardiovascular diseases in Sri
Lanka compared to other countries [3]. The specific reason for the low intake of fruit and
vegetables is unclear; studies from developed countries suggest a lack of perceived social
pressure to increase fruits and vegetable intake and suggest that increased public health efforts
require stronger health messages that incorporate consumer awareness of the low consumption
levels [14]. Moreover, peoples’ low purchasing ability and seasonal variation of fruits and
vegetables prices may adversely affect consumption. Despite five servings of fruits and
vegetables per day being considered the minimum daily intake by national dietary guidelines [9]
nearly half of the population eats less than 2 portions of fruits and vegetables, with less than 4%
reaching the minimum recommendation. Somathunga reported that 96.9% of Sri Lankan adults
did not consume five fruits and vegetables daily in the WHO Step Survey (2004) undertaken in
the Western province of Sri Lanka, comparable with our findings [11].
Pulses were the main source of protein, mainly dhal, the most common curry in the local
context, and boiled pulses eaten for breakfast. Although pulses are grouped in the protein
category, the main nutrient is carbohydrate, and thus invariably, consumption of pulses masks
significant amounts of carbohydrate. There is no conclusive evidence regarding protein intake
and disease risk in Sri Lanka. The MASALA study reported that higher levels of protein
consumption are associated with increased odds of diabetes in South Asians independent of age,
sex, waist circumference and hypertension [15]. A significant proportion of Sri Lankan males
(data not shown) consume over 5 servings of meat per day.
Sri Lankans consumed large numbers of starch servings; nearly 65% consumed well above the
upper cut-offs of the food pyramid guidelines and a considerable proportion of males consumed
very high levels of starch. This is mainly due to the average person’s meal being comprised of
three of quarters rice with a small amount of vegetable curry (averaging 15 g), a small piece of

80 Chapter 4: Manuscript 3
meat or fish (15 g) and some starchy curry such as potato or dhal (supplementary file 1).
Relatively low levels of starch portions were consumed by females mainly due to low absolute
food intake. A high carbohydrate meal leads to negative metabolic consequences such as
hyperinsulinaemia, high serum TAG and low HDL-cholesterol levels [16]. Most Sri Lankans
consume the largest starch portion for lunch or dinner and limit themselves to three meals per
day (data not shown); which may cause postprandial hyperglycaemia and
hypertriacylglycerolaemia [16]. More than one fifth of Sri Lankan adults are dysglycaemic and
the prevalence of diabetes is alarmingly high [2]; the high consumption of carbohydrate may be
associated with the diabetes epidemic in the country.
Dairy products provide valuable nutrients such as calcium, which is important for building and
maintaining strong bones. In addition, milk products provide several essential nutrients such as
proteins, vitamins and minerals. Lekamwasam and colleagues reported a 45% prevalence of
osteoporosis among postmenopausal women in Sri Lanka [8]. The CARDIA study revealed that
dairy consumption was inversely associated with the incidence of all individual components of
insulin resistance syndrome among individuals with a BMI ≥25 kg/m2 and increased dairy
consumption may reduce risk of type 2 diabetes and cardiovascular disease. Dairy intake is
substantially lower than Sri Lankan recommendations; over 1/3 of the population did not have
any dairy products and only 5% reached minimum levels. The main reason behind the low dairy
consumption could be the price of dairy products is unaffordable mainly due to the lack of local
production of dairy products and the consumption of dairy products largely depends on imported
milk powder [17];
This first national level dietary survey provides a sound basis for future food policy as it affects
Sri Lankan adults, and for the development of relevant nutrition education programs.
Furthermore, the rational assessment of food portion exchange tables will offer health

Chapter 4: Manuscript 3 81
professionals such as nutritionists, general practitioners, and nurses, valuable insights into Sri
Lankan meals and the development and prescription of meal plans in clinical and community
settings. A major strength of our study was the recruitment of a representative group from all
ethnic, education, areas of residence and age groups. Despite the relatively low participation of
male participants, women’s diet composition is similar to that of their male counterparts as most
Sri Lankan men eat at home. Second, the use of a random 24-hour dietary recall method helped
to obtain accurate results regarding dietary habits. Thirdly, disaggregation of food in Sri Lankan
dishes to guideline-based food groups leads to the more accurate counting of small portions of
foods in respective groups (as shown in figure 4-4). The main limitation of our data collection
and analysis was lack of data on oil consumption. Unlike meals in Western countries, coconut
oil, coconut milk or scraped coconuts are included in most mixed dishes which lead to
significant methodological challenges in obtaining accurate measurements of fat intake [18].
Secondly, portion sizes were estimated by recalling commonly used utensils and demonstrating
standard spoons, cups and plates, in addition to series of food photographs.
CONCLUSION
Dietary guidelines have emphasized the importance of a balanced and varied diet. Meals that
include no servings or very few servings of different food groups such as fruits and vegetables,
dairy products, fish and meat and pulses, lack both balance and variety. It is evident that a
substantial proportion of the Sri Lankan population does not consume a varied and balanced diet
which is suggestive of a close association between the nutrition-related NCDs in the country and
these unhealthy eating habits. We recommend that the government, health institutions and
organizations conduct larger national level dietary and nutrition surveys periodically to identify
associated disease conditions. This would allow practical public health initiatives to improve the
quality of the Sri Lankan diet.

82 Chapter 4: Manuscript 3
Chapter 4: Manuscript 3 83
REFERENCE LIST
1. Wijewardene, K., et al., Prevalence of hypertension, diabetes and obesity: baseline
findings of a population based survey in four provinces in Sri Lanka. The Ceylon
medical journal, 2005. 50(2): p. 62-70.
2. Katulanda, P., et al., Prevalence and projections of diabetes and pre-diabetes in adults in
Sri Lanka—Sri Lanka Diabetes, Cardiovascular Study (SLDCS). Diabetic Medicine,
2008. 25(9): p. 1062-1069.
3. Abeywardena, M., Dietary fats, carbohydrates and vascular disease: Sri Lankan
perspectives. Atherosclerosis, 2003. 171(2): p. 157.
4. Krebs-Smith, S., et al., Characterizing food intake patterns of American adults. The
American Journal Of Clinical Nutrition, 1997. 65(4): p. 1264S-1268S.
5. Michael Nelson et al, A Photographic Atlas of Food Portion Sizes. 1997, UK: MAFF
publications.
6. Suzana Shahar et al. Atlas of Food Exchanges & Portion Sizes. 2009, MDC Publishers:
Kuala Lampur.
7. Cleveland, L., et al., Method for assessing food intakes in terms of servings based on
food guidance. The American Journal Of Clinical Nutrition, 1997. 65(4): p. 1254S-
1263S.
8. Dissanayake, C., Ceylon Cookery. 9 ed. 2010, Sri Lanka: Stamford Lake (pvt) Ltd.
9. U.M.M. Samaranayake et al., Food Base Dietary Guidelines for Sri Lanka. 2011,
Colombo: Nutrition Devision, Ministry of Healthcare and Nutrition, Sri Lanka.
10. United States Department of Agriculture, The Food Guide Pyramid in Home and Garden
Bulletin Number 252 Center for Nutrition policy and Promotion, Editor. 1992. p. 17.
11. Somatunga, L.C., NCD Risk Factor Survey in Sri Lanka (STEP Survey). 2004, WHO.

84 Chapter 4: Manuscript 3
12. Katulanda, P., et al., Prevalence of overweight and obesity in Sri Lankan adults. Obes
Rev, 2010.
13. Tamers, S.L., et al., US and France adult fruit and vegetable consumption patterns: an
international comparison. Eur J Clin Nutr, 2009. 63(1): p. 11-7.
14. Levin, A., Nutrition and Policy. 5: Who Should Teach Patients about Nutrition? Annals
of Internal Medicine, 1999. 131(4): p. 317-318.
15. Wang, E.T., L. de Koning, and A.M. Kanaya, Higher Protein Intake Is Associated with
Diabetes Risk in South Asian Indians: The Metabolic Syndrome and Atherosclerosis in
South Asians Living in America (MASALA) Study. Journal of the American College of
Nutrition, 2010. 29(2): p. 130-135.
16. Misra, A., et al., South Asian diets and insulin resistance. Br J Nutr, 2009. 101(4): p.
465-73.
17. FAO, Sri Lanka –dairy products, in FAO Briefs on Import Surges. 2007, Trade and
Markets Division (EST), Food and Agriculture Organization of the United Nations
(FAO): Rome.
18. Amarasiri, W.A. and A.S. Dissanayake, Coconut fats. Ceylon Med J, 2006. 51(2): p. 47-
51.
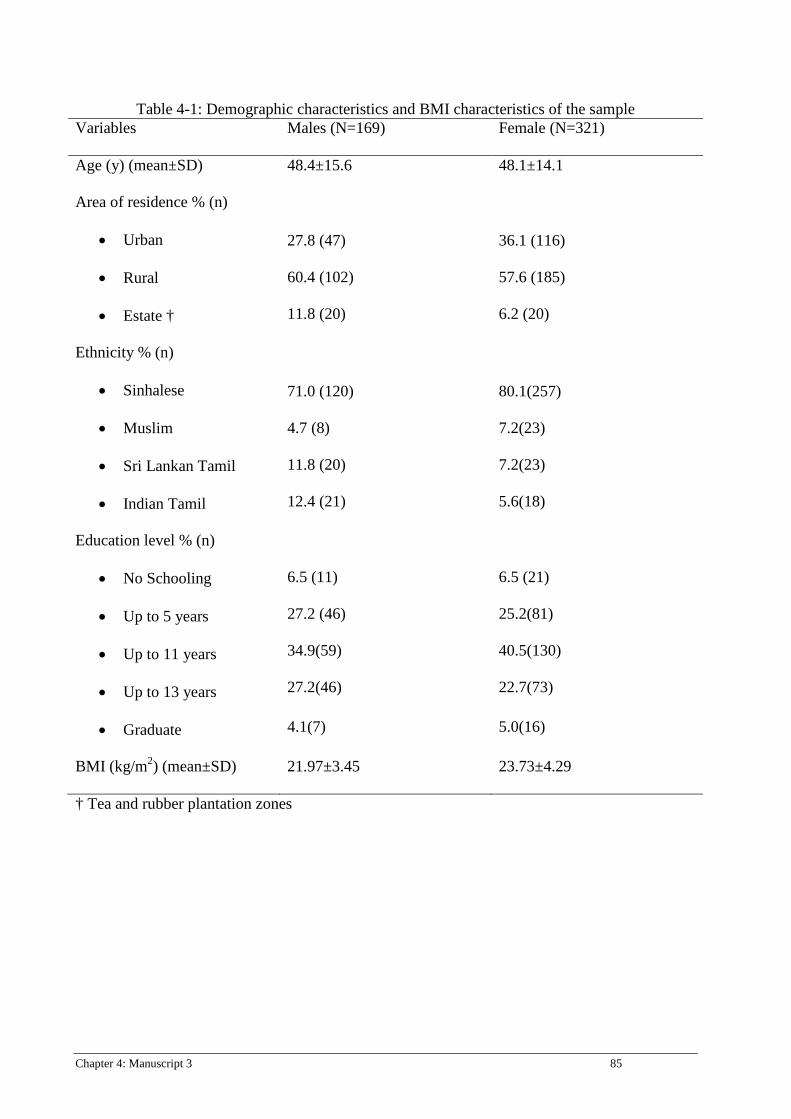
Chapter 4: Manuscript 3 85
Table 4-1: Demographic characteristics and BMI characteristics of the sample Variables Males (N=169) Female (N=321)
Age (y) (mean±SD) 48.4±15.6 48.1±14.1
Area of residence % (n)
• Urban
• Rural
• Estate †
27.8 (47)
60.4 (102)
11.8 (20)
36.1 (116)
57.6 (185)
6.2 (20)
Ethnicity % (n)
• Sinhalese
• Muslim
• Sri Lankan Tamil
• Indian Tamil
71.0 (120)
4.7 (8)
11.8 (20)
12.4 (21)
80.1(257)
7.2(23)
7.2(23)
5.6(18)
Education level % (n)
• No Schooling
• Up to 5 years
• Up to 11 years
• Up to 13 years
• Graduate
6.5 (11) 6.5 (21)
27.2 (46) 25.2(81)
34.9(59) 40.5(130)
27.2(46) 22.7(73)
4.1(7) 5.0(16)
BMI (kg/m2) (mean±SD) 21.97±3.45 23.73±4.29
† Tea and rubber plantation zones
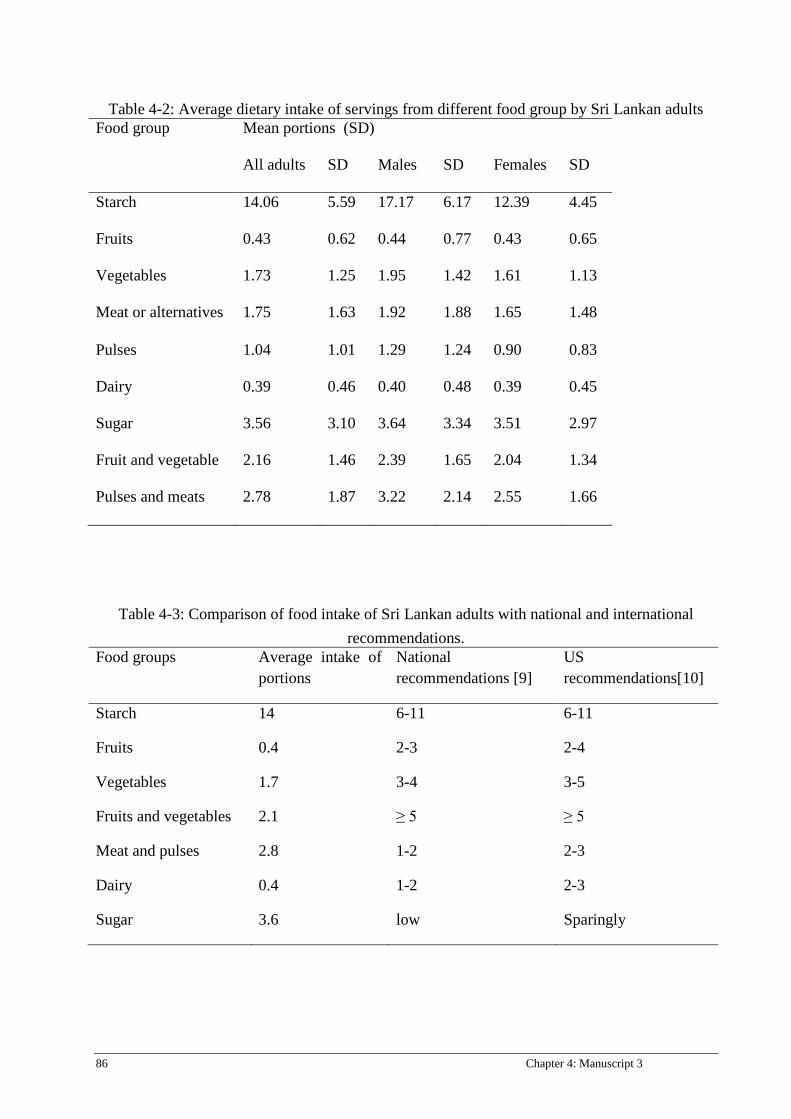
86 Chapter 4: Manuscript 3
Table 4-2: Average dietary intake of servings from different food group by Sri Lankan adults Food group Mean portions (SD)
All adults SD Males SD Females SD
Starch 14.06 5.59 17.17 6.17 12.39 4.45
Fruits 0.43 0.62 0.44 0.77 0.43 0.65
Vegetables 1.73 1.25 1.95 1.42 1.61 1.13
Meat or alternatives 1.75 1.63 1.92 1.88 1.65 1.48
Pulses 1.04 1.01 1.29 1.24 0.90 0.83
Dairy 0.39 0.46 0.40 0.48 0.39 0.45
Sugar 3.56 3.10 3.64 3.34 3.51 2.97
Fruit and vegetable 2.16 1.46 2.39 1.65 2.04 1.34
Pulses and meats 2.78 1.87 3.22 2.14 2.55 1.66
Table 4-3: Comparison of food intake of Sri Lankan adults with national and international recommendations.
Food groups Average intake of portions
National recommendations [9]
US recommendations[10]
Starch 14 6-11 6-11
Fruits 0.4 2-3 2-4
Vegetables 1.7 3-4 3-5
Fruits and vegetables 2.1 ≥ 5 ≥ 5
Meat and pulses 2.8 1-2 2-3
Dairy 0.4 1-2 2-3
Sugar 3.6 low Sparingly
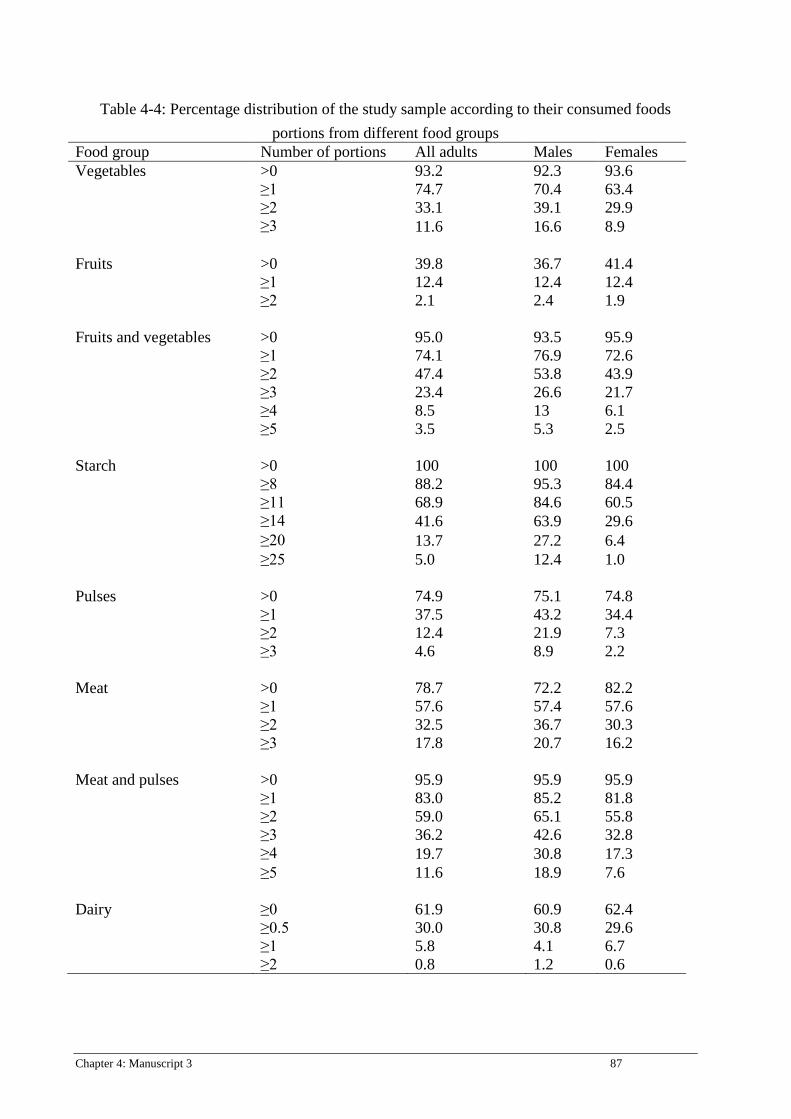
Chapter 4: Manuscript 3 87
Table 4-4: Percentage distribution of the study sample according to their consumed foods portions from different food groups
Food group Number of portions All adults Males Females Vegetables >0 93.2 92.3 93.6 ≥1 74.7 70.4 63.4 ≥2 33.1 39.1 29.9 ≥3 11.6 16.6 8.9 Fruits >0 39.8 36.7 41.4 ≥1 12.4 12.4 12.4 ≥2 2.1 2.4 1.9 Fruits and vegetables >0 95.0 93.5 95.9 ≥1 74.1 76.9 72.6 ≥2 47.4 53.8 43.9 ≥3 23.4 26.6 21.7 ≥4 8.5 13 6.1 ≥5 3.5 5.3 2.5 Starch >0 100 100 100 ≥8 88.2 95.3 84.4 ≥11 68.9 84.6 60.5 ≥14 41.6 63.9 29.6 ≥20 13.7 27.2 6.4 ≥25 5.0 12.4 1.0 Pulses >0 74.9 75.1 74.8 ≥1 37.5 43.2 34.4 ≥2 12.4 21.9 7.3 ≥3 4.6 8.9 2.2 Meat >0 78.7 72.2 82.2 ≥1 57.6 57.4 57.6 ≥2 32.5 36.7 30.3 ≥3 17.8 20.7 16.2 Meat and pulses >0 95.9 95.9 95.9 ≥1 83.0 85.2 81.8 ≥2 59.0 65.1 55.8 ≥3 36.2 42.6 32.8 ≥4 19.7 30.8 17.3 ≥5 11.6 18.9 7.6 Dairy ≥0 61.9 60.9 62.4 ≥0.5 30.0 30.8 29.6 ≥1 5.8 4.1 6.7 ≥2 0.8 1.2 0.6
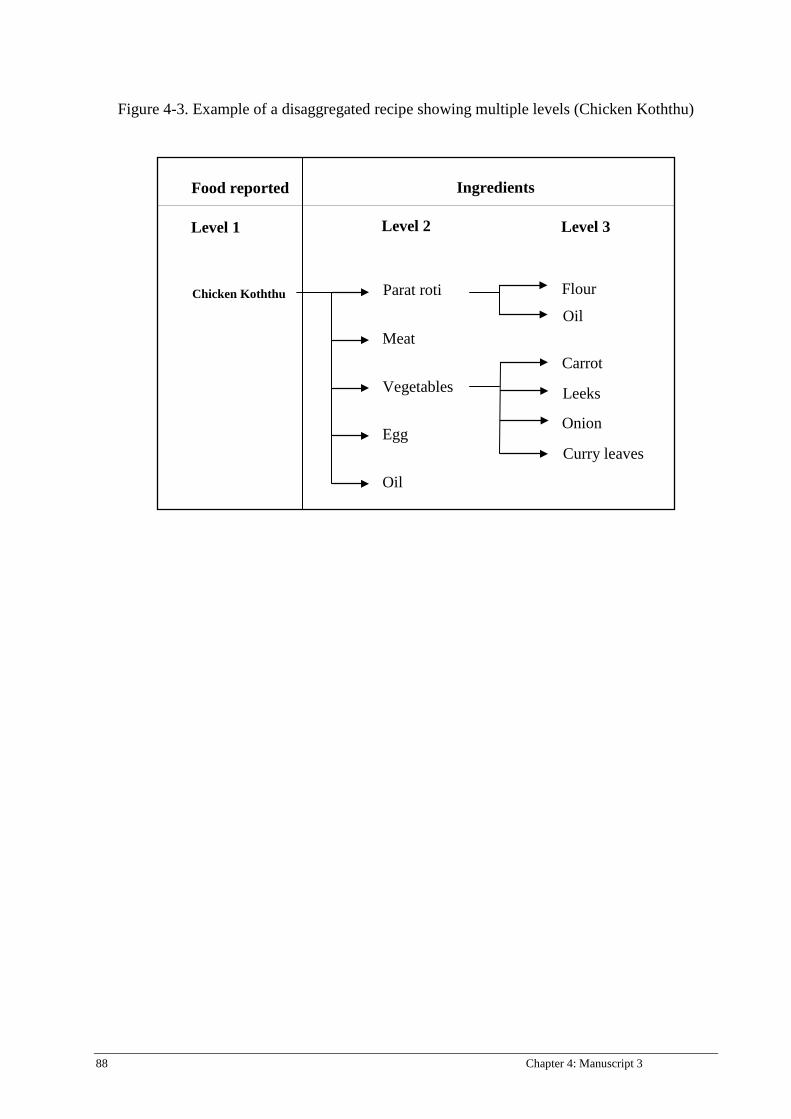
88 Chapter 4: Manuscript 3
Figure 4-3. Example of a disaggregated recipe showing multiple levels (Chicken Koththu)
Food reported
Level 1
Ingredients
Level 2 Level 3
Oil
Flour
Onion
Carrot
Curry leaves
Leeks
Chicken Koththu
Oil
Egg
Meat
Vegetables
Parat roti

Chapter 4: Manuscript 3 89
SUPPLEMENTARY MATERIALS, PART 1
Portion size estimations
Estimation of vegetable portions
Fruits, vegetables and leaves of all kinds whether fresh, canned, frozen, cooked, or raw, and
juices all count in the diet. However, starchy food such as potatoes, yam, roots, jack fruits (not
ripen), bread fruits, jack fruit seeds and ash plantain (without peel) were not included in the fruit
and vegetable group although they were consumed as curries in the Sri Lankan context, they
were counted as for cereal or equivalents. Well-ripened jack fruits (Waraka and Wala) contribute
to the fruits group. However, ash plantain (with peel) is considered a vegetable due to the high
level of dietary fiber and plant nutrients but only counts as a maximum one portion per day with
the remainder included in the starch group. Pumpkin which is a starchy vegetable, was
categorized under the vegetable group. In Sri Lanka, most green leaves are half-cooked or mixed
with coconut scrapes or oil however were included in the vegetable group. Coconut sambol (pol
sambol) is a very common Sri Lankan cuisine and widely consumed in rural communities. As
the main ingredient of coconut sambol is finely grated coconut, chilli, onion, curry leaves and
lime juice, without disaggregation it was considered a vegetable although it contains a
significant amount of fat. Moreover, Lunu-miris (chilli and onion paste), seeni-sambol (cooked
onion with sugar) was also considered in the vegetable group, However, katta-sambol (mixed
with dry fish and onion) was disaggregated to its main ingredients. Other mixed curries were
disaggregated for respective food groups according to recipes. For example, potato and pea curry
was divided to food groups according to respective pre-cooked proportions of potato and peas.
‘Polos’ which is the young jack fruit, is considered a vegetable as it contains less starch. Kiri
hodi (milk curry) is basically prepared mainly with coconut milk and some spices. In contrast to

90 Chapter 4: Manuscript 3
coconut sambol it consists of low plant products and therefore kirihodi is not included in the
vegetable group. However, kirihodi is not categorized under any food group.
Vegetables are prepared as salad, individual curries and mixed curries by using several types of
food preparation methods. While cooking the texture and the moisture content of vegetables are
changed or reduced, thus volume is reduced. Therefore, three heaped table spoons or ½ cup or
80 grams of cooked vegetable is defined as one vegetable serving [1-4]. If there is a vegetable
curry with half amount gravy six table spoons are defined as one vegetable portion. In Sri Lanka,
vegetables are served from table spoons and coconut spoons and thus as a default, one medium
size coconut spoon is considered as three table spoons or one serving. However, investigators
cross-checked and clarified the size of coconut spoons with model coconut spoons and food
images.
Despite ash plantain (with peel) and sweet potato being considered as vegetables they were
calculated for maximum of one portion in a day. One serving of commonly consumed curries is
weighed to define the weight of one portion of individual vegetable curry. When faced with
difficulties to find the weight of one tablespoon of a vegetable curry, the weight of one table
spoon was considered as 15 grams.
Estimation of fruit portions
Fresh, juiced or dried fruits all count in the diet. Fruit juice was included in 'pieces of fruit' if it
was at least a glass of fresh juice in a day. Even if more than one glass per day was reported, it
would only count as one portion of fruit per day [2]. A smoothie or fresh fruit juice containing
all of the edible pulped fruit and/or vegetable may count as more than one portion but this
depends on how it's made. Smoothies count as up to a maximum of two portions per day [3].

Chapter 4: Manuscript 3 91
However, unlike western countries the frequency of fruit/vegetable intake as juice was very
limited. Cordial and artificially flavoured fruit drinks were not categorized and they were
classified in the sugary group.
The portion sizes of fruits were defined as follow.
One portion of fruit:
• Small sized fruits– Ten fruits considered as one portion, example: grapes, veralu, nelli,
lovi, rose apple (jamboo);
• Small–medium size fruits – number may vary (2-6): ambarella, banana (small), naminan,
rambutan, passion fruit, mangosteen, jack fruit ripened (waraka);
• Medium-sized - one medium fruit, such as one apple, banana, pear, orange, guava,
woodapple, belli, mandarin;
• Large-sized - one slice of papaya, one slice of melon (two-inch slice), one large slice of
pineapple, two slices of mango (two-inch slices), pomegranate (1/2 medium), durian (2
pieces);
• Dried fruit: One tablespoon of raisins, currants, sultanas, one tablespoon of mixed fruit,
two figs, three prunes, one handful of banana chips;
• Juice: One medium glass (150 ml) of fruit juice;
• A-half cup of chopped fruits.
Some of the portions were adjusted to Sri Lankan conditions by considering the size of the fruit.
Though pineapple is defined as one longitudinal slice, in Sri Lanka pineapple is commonly cut
into round shapes. Therefore, a pineapple portion was defined as one large slice or two round
shapes slices. The portion size of banana is the equivalent of one medium-sized banana in
several dietary guidelines. Since several types of Sri Lankan bananas are smaller than in Western

92 Chapter 4: Manuscript 3
countries, two bananas were defined as one portion. One portion of fruit is defined as 80 grams
of edible portion of fruit or 100 grams of whole fruit and the average number of fruit items was
counted. Curries prepared from fruits are defined under the vegetable category, for example:
mango curry, papaw salad.
Estimation of pulse portions
Pulses are another sub-food group categorized under meat exchange as it provides protein [5].
Pulses are rich in nutrients including protein, dietary fiber, vitamins (folate) and minerals (zinc,
iron, and magnesium) and are low in total and saturated fat and contain no cholesterol. While
pulses contain fiber, they do not provide the same mixture of vitamins, minerals and other
nutrients as fruit and vegetables [3]. Thus, beans and pulses are not included in the vegetable
group in our classification.
Cooked pulses, ½ tea cup or three full table spoons or 1 coconut spoon is defined as one pulse
portion. The weight of one serving of cooked pulse varieties are defined by considering that one
serving should have 7 grams of protein. ‘Soya meat’ is superior in nutritional quality than other
pulses (http://www.soyfoods.org/soy-products/soy-fact-sheets/soy-meat-alternative-fact-sheet).
It contains more protein and is also a good source of iron and calcium. Soya products (e.g.
texturized vegetable protein) contain high quality protein and approximately 7 g of protein will
be contained in two table spoons.
Estimation of dairy products
All fluid milk products and many foods made from milk are considered part of this food group
[6]. Milk contains numerous beneficial nutrients such as calcium, phosphorous, magnesium,
vitamin B12, vitamin A, zinc and riboflavin. These nutrients are favorable for healthy bones and
teeth, for muscle function, and for immune function.

Chapter 4: Manuscript 3 93
One glass (250 ml) of fresh milk is defined as one portion [4]. As milk powder is used
commonly in Sri Lanka as a primary dairy food source three table spoonfuls is defined as one
serving equivalent to fresh milk. Two small cups of yoghurt (80 g each) and one tea cup or eight
table spoons of curd is considered as one serving [4]. Two slices or two wedges of cheese or 1/8
from 250 g of cheddar cheese are defined as one portion [1, 7]. Malted milk powders and Milo
are drunk as replacements for milk. However, those are defined under the starch group as they
contain a considerable amount of carbohydrate [7].
Estimation of cereal or equivalent portions
Cereals contain significant amount of vitamins, minerals, carbohydrates, fats, oils, and protein in
their natural form (as in whole grain). When a cereal is milled or processed the bran and wheat
germ is removed. Through these processes many of the vitamins, minerals and phytochemicals
are lost and remainder is mostly carbohydrate. Similarly, tubers and starchy vegetables have
high carbohydrate content.
One portion of cereal or equivalent is defined as the amount of starchy food in which 15 g of
carbohydrate is contained. 1/3 tea cup of rice, milk rice and noodles, one slice of bread, ¼ of 10
cm diameter and 0.5 cm thickness coconut roti, 2 string hoppers and ½ hopper is considered as
one serving of each food. 1/3 tea cup of boiled bread fruit, jak and sweet potato, ½ tea cup of
ash plantain and yam is defined as one portion.
Servings of cooked starch vegetables are decided by comparing the amount of curry which
contains 15 g of carbohydrate. Then portion size is calculated as how many household measures
with the above weight of curry. This is used for both cooked and raw foods. As an example, one
portion of manioc curry is 90 g and it comprises three table spoons. Ash plantain curry 90 g is
defined as one serving and six table spoons of it is taken as one portion.
94 Chapter 4: Manuscript 3
Biscuits, cake, short eats (roll, cutlet), vegetable roti and papadam are also included in starch
portions [8]. One piece of 4 cm slice cake and one short eat (small bakery items) is calculated for
one portion cereal or equivalent. As size and weight of biscuits vary, servings of biscuits were
taken from pre-defined portion size from nutrition information leaflets and direct contact with
manufacturers.
Estimation of meat portions
The meat group is large and includes meat and meat alternatives fish, seafood, eggs and pulses
[5]. These foods contain protein and are also a good source of iron and zinc and several B
vitamins.
One egg, 30 g of meat, fish, and 30 g of prawns and meat balls is defined as one meat portion.
The serving size was defined considering 7 grams of protein in that food portion. Since dry fish
contains more protein, 15 g is defined as one portion. But when it is defined for dry fish curry
one portion is considered as 30 g since it contains gravy. Commonly, sprats are served using
table spoons. As one table spoon holds 7-8 sprats weight of one table spoon is considered as 7.5-
8 g. Thus 2 table spoons of sprats are defined as one portion. In Sri Lanka, 1 kg of chicken is cut
into 13-15 pieces and one piece of chicken is considered as two portions. Since non-vegetarian
fried rice contains more than 2.6 g protein than normal cooked rice, it is considered as 1/3 of a
meat portion.
Estimation of sugar portion sizes
All types of glycaemic carbohydrates will be digested, absorbed and ultimately converted to
glucose or metabolized in the body. Although all sugar and starches are indistinguishable in
metabolic effect, there are different health implications (e.g. hyperglycemia) between
carbohydrates in terms of their dietary origin [8]. Extracted sugar from food has virtually no
Chapter 4: Manuscript 3 95
nutrients only energy. A high intake of sugar is associated with negative health consequences;
hence sugar was defined as a separate food group. Five grams of sugar is defined as a portion.
One portion of honey, treacle and jaggery was calculated estimating the weight or volume which
contains 5 g of sugar. The amount of sugar in sweets, desserts and sugary beverages were
estimated by recipes.
Reference list
1. Michael Nelson, M.A., James Meyer, A Photographic Atlas of Food Portion Sizes. 1997,
UK: MAFF publications.
2. The British Dietetic Association (2006) Fruit and Vegetables - Enjoy 5 a day!! Food
Fact.
3. nhs-uk. 5 A DAY: what counts? Popular topics 2009 18/12/2009 [cited 2011 10/06];
Available from: http://www.nhs.uk/Livewell/5ADAY/Pages/Whatcounts.aspx.
4. Non-Communicable Disease Unit, Food Base Dietary Guidelines for Sri Lanka. 2003,
Colombo: Ministry of Healthcare and Nutrition, Sri Lanka.
5. USDA. Protein foods. Food groups 2011 [cited 10/6/2011.
6. USDA, Dairy Group. Food groups. 2011: usda.org.
7. Suzana Shahar, N.A.M.Y., Nik Shamita Safii, Rafidah Ghazau, Roslina Ahmad., Atlas of
Food Exchanges & Portion Sizes. 2009, MDC Publishers: Kuala Lampur.
8. Jayatissa, R., Optimum Nutrition for Beating Diabetes. 1 ed. 2011, Colombo: Lalith
Printers.

96 Chapter 4: Manuscript 3
SUPPLEMENTARY MATERIALS, PART 2:
Figure 4-4 : A typical Sri Lankan lunch
Chapter 5: Manuscript 4 97
Chapter 5: Manuscript 4
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Development of a food frequency questionnaire for Sri Lankan adults. Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Sumathi Swaminathan Study design and statistics analysis Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
98 Chapter 5: Manuscript 4
TITLE PAGE
Development of a food frequency questionnaire for Sri Lankan
adults.
Ranil Jayawardena1,2*, Sumathi Swaminathan3, Nuala M. Byrne1, Mario J. Soares 3,4,
Prasad Katulanda2, Andrew P. Hills5
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Department of Clinical Medicine, Faculty of Medicine, University of
Colombo, Colombo, Sri Lanka.
3St John's Research Institute, St John’s National Academy of Health Sciences, Bangalore, India.
4Curtin Health Innovation Research Institute, School of Public Health, Curtin University, Perth,
Western Australia.
5Mater Mothers’ Hospital, Mater Medical Research Institute and Griffith Health Institute,
Griffith University, Brisbane, Queensland, Australia.
Citation
R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. (2012) Development of a food
frequently Questionnaire for Sri Lankan adults. Nutrition Journal 11:63.
Chapter 5: Manuscript 4 99
ABSTRACT
Background: Food Frequency Questionnaires (FFQs) are commonly used in
epidemiologic studies to assess long-term nutritional exposure. Because of wide variations in
dietary habits in different countries, a FFQ must be developed to suit the specific population. Sri
Lanka is undergoing nutritional transition and diet-related chronic diseases are emerging as an
important health problem. Currently, no FFQ has been developed for Sri Lankan adults. In this
study, we developed a FFQ to assess the regular dietary intake of Sri Lankan adults.
Methods: A nationally representative sample of 600 adults was selected by a multi-stage
random cluster sampling technique and dietary intake was assessed by random 24-h dietary
recall. Nutrient analysis of the FFQ required the selection of foods, development of recipes and
application of these to cooked foods to develop a nutrient database. We constructed a
comprehensive food list with the units of measurement. A stepwise regression method was used
to identify foods contributing to a cumulative 90% of variance to total energy and
macronutrients. In addition, a series of photographs were included.
Results: We obtained dietary data from 482 participants and 312 different food items were
recorded. Nutritionists grouped similar food items which resulted in a total of 178 items. After
performing step-wise multiple regression, 93 foods explained 90% of the variance for total
energy intake, carbohydrates, protein, total fat and dietary fibre. Finally, 90 food items and 12
photographs were selected.
Conclusion: We developed a FFQ and the related nutrient composition database for Sri
Lankan adults. Culturally specific dietary tools are central to capturing the role of diet in risk for
chronic disease in Sri Lanka. The next step will involve the verification of FFQ reproducibility
and validity.
100 Chapter 5: Manuscript 4
INTRODUCTION
It is widely recognized that an unhealthy diet is a major risk factor for many of the chronic non-
communicable diseases and improving dietary habits is not simply an individual but a societal
problem [1]. However, it is difficult to assess the dietary habits of free-living individuals because
of variability in food preference and availability, socio-economic factors, cultural concerns and
educational level [2]. National dietary surveys have several important functions and provide
valuable information on dietary habits and nutritional status. Moreover, nutritional monitoring is
important for implementation of programs related to food, nutrition, and health promotion for
any country serious about promoting the health and wellbeing of its population [3]. Food
Frequency Questionnaires (FFQs) are the most common dietary assessment tool used in large
epidemiologic studies of diet and health [4]. To cater for differences in food based on cultural
and regional factors, numerous FFQs have been developed comprising the list of foods
commonly eaten in a particular country or by a particular population.
Sri Lanka is a ‘low-middle’ income country in South Asia with a population of nearly 21
million. Sinhalese is the main ethnic group but there are significant proportions of Tamils and
Moors living in different parts of the country. With recent economic development, urbanization
and changes in lifestyle patterns, Sri Lanka is experiencing a nutritional transition with the
coexistence of under-nutrition and overweight and obesity [5,6]. A high prevalence of iron
deficiency anemia among pregnant women, and subclinical vitamin A deficiency, stunting and
wasting among pre-school children, are still major public health problems [7]. Recent studies in
Sri Lanka indicate a high prevalence of diabetes mellitus with one in every five adults aged
above 20 years having either diabetes or pre-diabetes [8], and the prevalence of hypertension,
obesity, dyslipidaemia in urban areas are reaching epidemic proportions [9,10]. A quarter of
adults is suffering from metabolic syndrome [11]. In the Sri Lankan context, diet-related chronic

Chapter 5: Manuscript 4 101
diseases currently account for an estimated 18.3% of total mortality and 16.7% of hospital
expenditure [6].
Despite strong indications of a rise in lifestyle-related non-communicable diseases (NCDs) in Sri
Lanka, published guidelines are not justified with sound research evidence on dietary habits
[12]. There is a paucity of data on the dietary habits of Sri Lankans and in order to assess dietary
intake, a culturally specific dietary assessment tool is necessary. This paper describes the
development of a FFQ for Sri Lankan adults designed to assess and monitor dietary intake and
be used to assist in national level programs to combat non-communicable diseases.
METHODS
Study sample
Data were collected from a subset of the national ‘Sri Lanka Diabetes and Cardiovascular Study’
(SLDCS) using a multi-stage, stratified, random sampling procedure (n=500) [8]. However, data
collection in the SLDCS was affected by the prevailing civil war which resulted in no data being
collected from Northern and Eastern provinces. To obtain a nationally representative sample,
additional subjects (n=100) were later recruited from the two provinces using similar selection
criteria. Details of subject selection are published elsewhere [13].
Data collection
Selected households were contacted via telephone and the purpose of the study explained and
verbal consent taken. Where telephone facilities or contact phone numbers were unavailable,
households were visited by the study team with prior postal notice. Subsequently, households
were visited on a random day and dietary and demographic details obtained after informed
written consent was provided. An interviewer-administered questionnaire was used for data
collection and information regarding socio-demographic factors and 24-h dietary recall (24DR)
102 Chapter 5: Manuscript 4
was obtained. Two trained nutritionists retrieved dietary data using a standardized manual of
procedure. Food portion sizes were obtained from participants using standard household
measures such as a plate, bowl, cup, glass, and spoons of different size; as well as using
photographs (Supplementary file 1) of food portion size and a food atlas [14, 15].
Development of a nutrient composition database
It is essential to have food composition values to convert information from an FFQ into
macronutrient and micronutrient values. Currently the database on Sri Lankan dishes is meagre.
We therefore compiled information from the food composition tables of Sri Lanka [16], United
States Department of Agriculture nutrient database (USDA) [17], the Indian Food Composition
Tables [18], and McCance and Widdowson’s food composition tables [19] to develop a
comprehensive and new nutrient composition database as follows:
a) Nutrition values for single food items were taken mainly from the USDA nutrient
database.
b) Nutrition information leaflets or details from direct contact with producers were used for
locally available food products (e.g. biscuits).
c) For mixed dishes and cooked foods, local recipes were taken from popular cookery
books [20] and by interviewing participants. All recipes were accepted after checking
for face validity by consulting local housewives and nutritionists. According to the
recipes, ingredients were weighed to the nearest 1 g for edible portions of the foods, and
the food items were cooked and weighed. Nutritional composition of the final recipe
was calculated by entering nutritional values and weights of individual ingredients into
a spreadsheet. The sum of each nutrient was computed and standardised to 100 g of the
final product. Data on weight loss associated with cooking (e.g. due to water
evaporation) was recorded to ensure accurate nutrient density of the portion size
Chapter 5: Manuscript 4 103
consumed. However, nutrient losses (e.g. vitamins) during food preparation were not
considered.
Newly developed food composition data for each recipe was entered into NutriSurvey 2007
(EBISpro, Germany) nutrient analysis software.
Development of the FFQ
In addition to 24-h recalls, a number of additional methods were used to obtain a more
comprehensive food list.
• Open ended questions were asked to capture details of seasonal fruits and festival foods.
• Alcohol intake and use of dietary supplements were collected separately.
• Local nutrition experts were contacted to obtain unreported foods for the different ethnic
groups.
Food items were divided into eight groups by two independent nutritionists and included: 1)
cereals or equivalents; 2) vegetables; 3) pulses; 4) meat or equivalents; 5) fruits; 6) drinks; 7)
miscellaneous; and 8) alcohol.
• Using stepwise multiple regression analysis, food items that contributed to a cumulative
90% of the variance in energy, carbohydrates, fat, protein and dietary fibre were included
in the FFQ.
• Food items with similar consumption patterns and nutrients were aggregated into groups
on the basis of their energy, carbohydrate, fat, protein and dietary fibre.
To improve the quantification of food intake we included food photographs to estimate habitual
portion sizes for those foods that could not be easily assessed in natural units or household
measures. The FFQ contains colour photographs of 3 different sized portions of four commonly
consumed foods namely rice, vegetable, chicken, and dhal (lentil). For each food, photograph A
represents the 25th percentile, B the median and C the 75th percentile of the distribution of

104 Chapter 5: Manuscript 4
serving sizes reported in this study. Seven different serving sizes can be attributed to each food
class, by selecting serving sizes that are equal to A, B or C, less than A, greater than C and
between A-B or between B-C [21]. However, we found low clarity in determining portion sizes
from pre-test subjects when vegetables, meat and dhal were pictured alone on the plate. In Sri
Lanka, curries are served on rice, not as a side dish; therefore, to improve precision and accuracy
regarding portion sizes, we displayed individual food items on the medium rice plate (B) as the
background.
The majority of FFQs from developed countries have used several frequency categories [22,23].
However, this is not the case in Southern India [24]. To some extent, open-ended response scales
(number of units taken at a time: ‘per day’, ‘week’, ‘month’ or ‘year’) reflect the precision with
which participants can realistically describe their usual intake. We also used an open-ended
response scale. FFQs were designed to incorporate interviewer-administered methods. A
protocol was developed to obtain data uniformly. The questionnaire was pilot tested for clarity,
interpretation and improvement of format in 25 individuals who had similar demographic
characteristics to the study group but who were not participants in the study. All statistical
analyses were undertaken using SPSS version 16 (SPSS Inc., Chicago, IL, USA) and
independent sample T-test was used to compare demographic characteristics and nutrient intake
between men and women. The significance level was set at 0.05 in all analyses.
RESULTS AND DISCUSSION
From the total sample of 600, 482 completed (Male=166; Female=316) all demographic,
anthropometric and dietary profiles. The demographic profile of the study population is shown in
Table 5.1. Overall, there was a preponderance of Sinhalese followed by Tamils and Moors.
Males had lower BMI values compared to their female counterparts (M: 22.0±3.5 vs. 23.7±4.3
kg/m2; p<0.05). Average daily energy intake was 1656.7±535.0 kcal, with significantly higher
Chapter 5: Manuscript 4 105
caloric consumption by men compared to women (p<0.05). The main source of energy was from
carbohydrates for both men and women. Total protein and fat intake for men was 52.8±43.0
g/day and 40.5±18.1 g/day respectively and for women, 40.0 ±13.9 g/day and 31.9 ±14.1 g/day
(Table 5.2).
In this study 312 different food items were recorded. Nutritionists grouped similar food items
which resulted in a total of 178 food items. After performing step-wise multiple regression, 93
foods explained 90% of the variance for total energy intake, carbohydrates, protein, total fat and
dietary fibre. Subsequently, conceptually similar food items were grouped together yielding a
final list of 81 food items (Table 3). An additional nine food items were included to cover
festival and seasonal dietary habits and the final 90 food items were categorized as cereal or
equivalents (n=19), vegetables (n=20), pulses (n=6), meat or alternatives (n=10), fruits (n=9),
beverages (n=7), miscellaneous (n=14), and alcohol (n=5).
The paper describes the process of development of a FFQ for Sri Lankan adults using a
nationally representative sample. Dietary assessment of this population is invaluable to
understand the role of nutrition in chronic disease so that preventive strategies can be
implemented. The aim of dietary assessment of populations is to rank people by a measure of
usual rather than current diet. The strengths of this study include a nationally representative
sample of Sri Lankan adults and the creation of a comprehensive new database for nutrient
analysis. However, males are under-represented in this study which stems from data collection
being on a random day when most males were engaged in active occupations away from home.
However, in Sri Lanka family members consume similar foods; therefore, obtaining dietary data
from females did not significantly affect the food list in our study. The number of food items in a
FFQ is a crucial factor in determining the accuracy of the data and the practicability of the
questionnaire. Many FFQs have between 100–150 items [25] and the risk of over-reporting
through increased subject burden increases with the large number of items [22, 25]. In our FFQ,
106 Chapter 5: Manuscript 4
we have 90 items and 12 photos of food items to enable an accurate estimation of dietary
exposure.
Sri Lanka as a tropical island has no clear four seasons but two monsoons influence cultivation.
Hence, additional seasonal fruits and vegetables are also included in our FFQ. Over 55% of adult
males are current alcohol drinkers [26]; however in our data collection alcohol consumption was
under-reported (0.5% of participants) with no women reporting the consumption of alcohol. In
Sri Lanka, drinking alcohol has negative social and religious stigma. Thus, common alcoholic
beverages were added to the FFQ. Dietary recalls indicated differences between the ethnic
groups in the type of nutrients derived from different food sources. The main carbohydrate
source varied among ethnic groups; Indian Tamils reported consuming wheat flower (as Roti)
whereas Sinhalese eat rice as the main staple food and Sri Lankan Tamils consume Dose, Itale
and Wade frequently. Ethnicity was an important factor in the selection of foods containing
protein, not surprisingly; pork and beef consumption was not reported by Moors (Muslims) and
Tamils, respectively.
A variety of methods are available to collect food consumption data but a common challenge for
individual-based dietary assessment methods is portion size estimation. Although weighing
served portions is often considered the gold standard; for practical reasons, portion estimation
using photographs are used among both adults and children [27]. A study conducted in Burkina
Faso showed that food photographs are valuable for the quantification of food portion size
among rural and less educated middle-aged women [28]. Men usually consume larger portions
than women [29] and the use of photographs helps to categorize gender variation in portion sizes
more precisely. This is crucial to obtaining reliable estimates of macronutrient and micronutrient
intakes. Several countries use FFQs with photo series and scoring systems [30, 31].
Chapter 5: Manuscript 4 107
The main weakness of the previous national level NCD survey (SLDCS) was the absence of
nutritional data on the population and their relationship with the high NCD risk in the country.
One of the main objectives of the current work was to develop a FFQ to administer in the next
national level NCD survey. Moreover, this FFQ could also be used to assess dietary habits of Sri
Lankans living in other countries, as they practice similar eating patterns to native Sri Lankans.
There is no updated nutrient database in the country. Sri Lankan food composition tables were
published in 1979, and since then many chemical analysis techniques have changed. Newer
processed food items have been introduced into the market. We used the USDA food
composition tables as the backbone of our nutrient database. This is arguably the most
comprehensive, standardized, largest and continuously updated database that has used to develop
population-specific food composition tables in other countries [25]. Mixed dishes were not listed
in the USDA database, and for such items we followed calculated values from traditional
recipes. The recipes vary according to ethnic groups in Sri Lanka and were therefore modified to
allow generalization to the whole country.
Limitations
Coconut oil is the main cooking oil in Sri Lanka [32], however, other types of cooking oils are
used in different communities. Our FFQ does not enable us to differentiate the types of cooking
oil consumed which may have important health implications for NCDs. However, we used
additional questions to obtain details of oil consumption. Another limitation is the lack of data
on micronutrients on Sri Lankan mixed dishes, prolonged cooking time and addition of various
spicies and herbs which could alter the nutritional values of the raw ingredients [33].
108 Chapter 5: Manuscript 4
CONCLUSION
This study highlights the development of a FFQ and the related nutrient composition database
for Sri Lankan adults. Culturally specific dietary tools are central to capturing the role of diet in
risk for chronic disease in Sri Lanka. While the reproducibility and validity of this FFQ needs to
be determined, an important ongoing program would be the regular updating of the new nutrient
database we have also developed.
Acknowledgements
The authors would like to acknowledge Miss Fathima Shakira and other members in the
Diabetes Research Unit, Colombo, for their contribution in arranging logistics for the study.
Chapter 5: Manuscript 4 109
REFERENCE LIST
1. Somatunga, L.C., NCD Risk Factor Survey in Sri Lanka (STEP Survey). 2004, WHO.
2. Stamler, J., Assessing diets to improve world health: nutritional research on disease causation in populations. American Journal of Clinical Nutrition, 1994. 59(1): p. 146S.
3. Lee R.D., N.D.C., National Dietary and Nutrition Surveys, in Nutritional Assessments, D.C.N. Robert D. Lee, Editor. 2002, McGraw-Hill Science Engineering. p. 111-143.
4. Willett, W., Nutrition Epidermiology. 2 ed. 1998, NEW YORK: Oxford University Press.
5. FAO, FAO-Nutrition Country Profiles. 1999, Food and Agriculture organization of the United Nations Rome.
6. Popkin B.M., H.S., Kim S.,, The Nutritional Transition and Diet-Related Chronic Diseases in Asia: Implications for Prevention. Washington, DC: International Food Policy Research Institute FCND Discussion Paper, 2001. 105.
7. Meera Shekar, A.S., Lidan Du, , Malnutrition in Sri Lanka: Scale, Scope, Causes, and Potential Response, W. Bank, Editor. 2007, Human Development Unit, South Asia Region.
8. Katulanda, P., et al., Prevalence and projections of diabetes and pre-diabetes in adults in Sri Lanka—Sri Lanka Diabetes, Cardiovascular Study (SLDCS). Diabetic Medicine, 2008. 25(9): p. 1062-1069.
9. Wijewardene, K., et al., Prevalence of hypertension, diabetes and obesity: baseline findings of a population based survey in four provinces in Sri Lanka. The Ceylon medical journal, 2005. 50(2): p. 62-70.
10. Katulanda, P., et al., Prevalence of overweight and obesity in Sri Lankan adults. Obes Rev, 2010.
11. Katulanda, P., et al., Metabolic syndrome among Sri Lankan adults: prevalence, patterns and correlates. Diabetology & Metabolic Syndrome, 2012. 4(1): p. 24.
12. Samaranayake U.M.M. et al., Food Base Dietary Guidelines for Sri Lanka. 2011, Colombo: Nutrition Devision, Ministry of Healthcare and Nutrition, Sri Lanka.
13. Jayawardena R., B.N.M., Soares M.J., Katulanda P., Hills A.P.,, Consumption of Sri Lankan adults: an appraisal of serving characteristics Public Health Nutrition, 2012. FirstView:1-6.
14. Nelson M., A.M., Meyer J.,, A Photographic Atlas of Food Portion Sizes. 1997, UK: MAFF publications.
110 Chapter 5: Manuscript 4
15. Shahar S., Y.N.A.M., Safii N.S., Ghazau R., Ahmad R., , Atlas of Food Exchanges & Portion Sizes. 2009, MDC Publishers: Kuala Lampur.
16. Perera W.D.A., J.P.M., Thaha S.Z., , Tables of food composition for use in Sri Lanka. 1979.
17. USDA. Foods List. National Nutrient Database for Standard Reference 2012 3/30/2012; 24:[Available from: http://ndb.nal.usda.gov/ndb/foods/list.
18. Gopalan C., R.B.V., Balasubramanian S.C.,, Nutritive value of Indian foods, ed. N.I.o. Nutrition. 1989, Hyderabad.
19. Welch A.A., U.I.D., Buss D.H., Paul A.A., Southgate D.A.T., , McCance and Widdowson’s The Composition of Foods. 5th ed. 1995, Cambridge: Royal Society of Chemistry.
20. Dissanayake, C., Ceylon Cookery. 9 ed. 2010, Sri Lanka: Stamford Lake (pvt) Ltd.
21. Hodge A., P.A.J., Brown W.J., Ireland P., Giles G., , The Anti Cancer Council of Victoria FFQ: relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Australian and New Zealand Journal of Public Health 2000. 24(6): p. 576-586.
22. Kobayashi, T., et al., Development of a food frequency questionnaire to estimate habitual dietary intake in Japanese children. Nutrition Journal, 2010. 9(1): p. 17.
23. Ireland P., J.D., Giles G., O'Dea K., Powles J., Rutishauser I., Wahlqvist M.L., Williams J.,, Development of the Melbourne FFQ: a food frequency questionnaire for use in an Australian prospective study involving an ethnically diverse cohort. Asia Pacific J Clin Nutr, 1994. 3: p. 19-31.
24. Bharathi, A., et al., Development of food frequency questionnaires and a nutrient database for the Prospective Urban and Rural Epidemiological (PURE) pilot study in South India: Methodological issues. Asia Pacific Journal of Clinical Nutrition, 2008. 17(1): p. 178-185.
25. Dehghan, M., et al., Development of a semi-quantitative food frequency questionnaire for use in United Arab Emirates and Kuwait based on local foods. Nutrition Journal, 2005. 4(1): p. 18.
26. Rahav, G., et al., The influence of societal level factors on men's and women's alcohol consumption and alcohol problems. Alcohol and alcoholism (Oxford, Oxfordshire). Supplement, 2006. 41(1): p. i47-55.
27. Frobisher C., M.S.M., The estimation of food portion sizes: a comparison between using descriptions of portion sizes and a photographic food atlas by children and adults. Journal of Human Nutrition and Dietetics, 2003. 16(3): p. 181-188.
28. Huybregts, L., et al., Validity of photographs for food portion estimation in a rural West African setting. Public Health Nutrition, 2008. 11(06): p. 581-587.

Chapter 5: Manuscript 4 111
29. Caster, W.O., Systematic estimation of food intakes from food frequency data. Nutrition Research, 1986. 6(4): p. 469-472.
30. Victoria, C.C. Dietary questionnaires. 2010; Available from: http://www.cancervic.org.au/about-our-research/epidemiology/nutritional_assessment_services.
31. Ocké, M.C., et al., The Dutch EPIC food frequency questionnaire. I. Description of the questionnaire, and relative validity and reproducibility for food groups. International Journal of Epidemiology, 1997. 26(suppl 1): p. S37.
32. Amarasiri, W., Coconut fats. Ceylon Med J, 2009. 51(2).
33. Khokhar S., R.M., Swan G.,, Carotenoid and retinol composition of South Asian foods commonly consumed in the UK. Journal of Food Composition and Analysis, 2012. 25(2): p. 166-172.

112 Chapter 5: Manuscript 4
Table 5-1: Demographic characteristics of the sample of the study population Variables Males % (169) Female % (321)
Age (y) 48.4±15.6 48.1±14.1
BMI (kg/m2)* 22.0±3.5 23.7±4.3
Area of Residence
• Urban
• Rural
• Estate
27.8 (47)
60.4 (102)
11.8 (20)
36.1 (116)
57.6 (185)
6.2 (20)
Ethnicity (%)
• Sinhalese
• Moors
• Sri Lankan Tamil
• Indian Tamil
71.0 (120)
4.7 (8)
11.8 (20)
12.4 (21)
80.1(257)
7.2(23)
7.2(23)
5.6(18)
Education level (%)
• No Schooling
• Up to 5 years
• Up to 11 years
• Up to 13 years
• Graduate
6.5 (11) 6.5 (21)
27.2 (46) 25.2(81)
34.9(59) 40.5(130)
27.2(46) 22.7(73)
4.1(7) 5.0(16)
Data are mean ± SD. Values in parenthesis are total number. *p<0.05
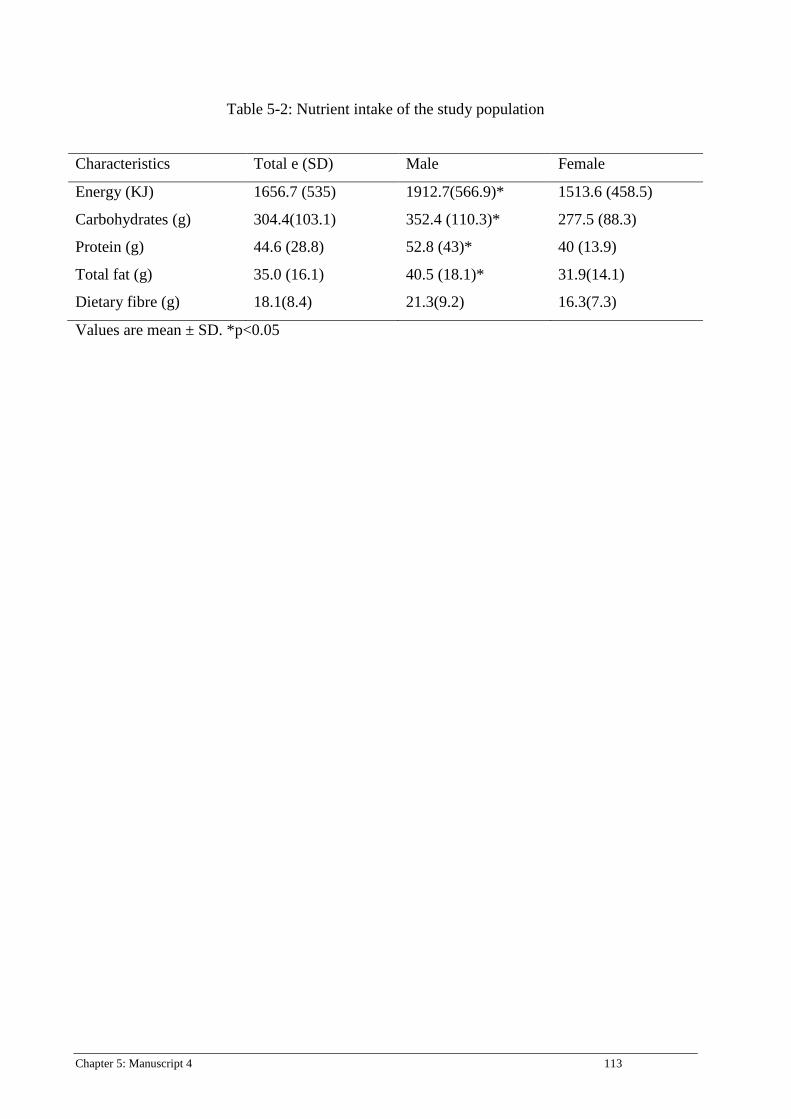
Chapter 5: Manuscript 4 113
Table 5-2: Nutrient intake of the study population
Values are mean ± SD. *p<0.05
Characteristics Total e (SD) Male Female
Energy (KJ) 1656.7 (535) 1912.7(566.9)* 1513.6 (458.5)
Carbohydrates (g) 304.4(103.1) 352.4 (110.3)* 277.5 (88.3)
Protein (g) 44.6 (28.8) 52.8 (43)* 40 (13.9)
Total fat (g) 35.0 (16.1) 40.5 (18.1)* 31.9(14.1)
Dietary fibre (g) 18.1(8.4) 21.3(9.2) 16.3(7.3)
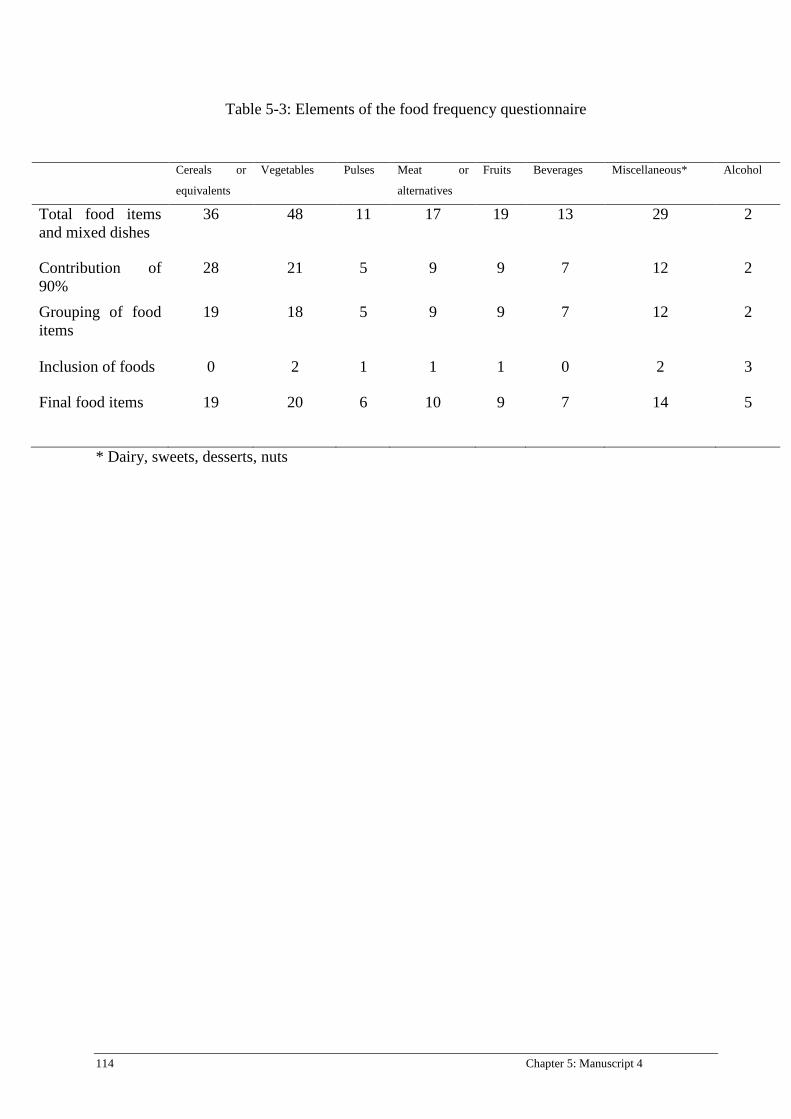
114 Chapter 5: Manuscript 4
Table 5-3: Elements of the food frequency questionnaire
* Dairy, sweets, desserts, nuts
Cereals or
equivalents
Vegetables Pulses Meat or
alternatives
Fruits Beverages Miscellaneous* Alcohol
Total food items and mixed dishes
36 48 11 17 19 13 29 2
Contribution of 90%
28 21 5 9 9 7 12 2
Grouping of food items
19 18 5 9 9 7 12 2
Inclusion of foods 0 2 1 1 1 0 2 3
Final food items 19 20 6 10 9 7 14 5
Chapter 5: Manuscript 4 115
Supplementary file 1
Figure 5-1: Example of a food photograph (200 g of rice)

116 Chapter 6: Manuscript 5
Chapter 6: Manuscript 5
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Energy and Nutrient Intakes among Sri Lankan Adults
Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Shalika Tennakoon data collection and data analysis Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
Chapter 6: Manuscript 5 117
TITLE PAGE
Energy and Nutrient Intakes among Sri Lankan Adults
R. Jayawardena1,2*, S.N. Thennakoon2, N.M. Byrne1, M.J. Soares3, P. Katulanda2, A.P.
Hills4
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka.
3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health
Sciences, Curtin University, Perth, WA, Australia.
4Mater Mothers’ Hospital, Mater Medical Research Institute and Griffith Health Institute,
Griffith University, Brisbane, Queensland, Australia.
Citation
R Jayawardena, SN Thennakoon, NM Byrne, MJ Soares, P Katulanda, AP Hills. Energy and
Nutrient Intakes among Sri Lankan Adults. BMC Research Notes (in press) MS:
1400644043847201
118 Chapter 6: Manuscript 5
ABSTRACT
Introduction
Dietary practices are a key factor related to health status at both individual and population levels.
Over- and under-nutrition both have the potential to contribute to serious health consequences.
Sri Lanka is undergoing a rapid socioeconomic transition which is related to a significant health
burden related to under-nutrition and an epidemic of non-communicable diseases. However, to
date, detailed data on food consumption in the Sri Lankan population is limited. The aim of this
study was to identify energy and major nutrient intake among Sri Lankan adults.
Methods
A nationally-representative sample of adults was selected using a multi-stage random cluster
sampling technique. An interviewer-administered 24-h dietary recall was used to obtain data
concerning the nutritional intake of the population. NutriSurvey® software was used to analyze
the nutritional composition of typical meals.
Results
Data from 463 participants (166 Males, 297 Females) were analyzed. Total energy intake was
significantly higher in males (1913±567 kcal/d) than females (1514±458 kcal/d). However, there
was no significant gender differences in the percentage of energy from carbohydrate
(Male:72.8±6.4%, Female:73.9±6.7%), fat (Male:19.9±6.1%, Female:18.5±5.7%) and protein
(Male:10.6±2.1%, Female:10.9±5.6%). The average intake of dietary fiber was 21.3 g/day and
16.3g/day for males and females, respectively. There was a significant difference in nutritional
intake related to ethnicities, areas of residence, education levels and BMI categories.
Discussion
The present study provides the first national estimates of energy and nutrient intake of the Sri
Lankan adult population. Regular nutrition surveys are needed at the national level to obtain
valuable information on diet and associated diseases.
Chapter 6: Manuscript 5 119
INTRODUCTION
The epidemic of nutrition related non-communicable diseases (NCDs) such as type 2 diabetes
mellitus, obesity, cardiovascular diseases (CVDs) and certain cancers are continuing to
challenge the health sectors in Asia [1]. Sri Lanka is a low-middle income South Asian country
with a population of approximately 20 million. Despite most Sri Lankans having relatively good
health status, during the last two decades NCDs have become a more prominent health issue in
the country [2]. A quarter of Sri Lankan adults suffer from metabolic syndrome [3]. According
to results from the Sri Lanka Diabetes and Cardiovascular Study (SLDCS), the prevalence of
diabetes among Sri Lankan adults was nearly 11% and one-fifth of adults have diabetes or pre-
diabetes while one third of those with diabetes are un-diagnosed [4]. Premarathna et al. have
also reported that there was an increase in the incidence of hospitalization of Sri Lankan adults
by 36%, 40% and 29% due to diabetes mellitus, hypertensive disease and ischemic heart disease,
respectively, in 2010 compared to 2005 [5]. Diet-related chronic diseases currently account for
18.3% of all deaths and 16.7% of hospital expenditure in the country [1]. There is a significant
health burden due to NCDs and this will be a challenge to the health sector in a developing
country like Sri Lanka.
Some methods to assess the quantity and quality of dietary intake include prospective food
records (with weighed or estimated food portions), retrospective 24-h recalls (24 HDR), and
food frequency questionnaires (FFQs) [6]. The 24HDR which is less time-consuming and has a
low respondent burden, is the method used to gather the quantitative estimate of all foods and
beverages an individual has consumed in the previous 24 hours at a population level. Several
national dietary surveys have used 24 HDR and it is known to be acceptable for gathering
dietary information on a given day at the population level [7,8].

120 Chapter 6: Manuscript 5
National diet and nutrition surveys provide valuable information on a possible partial
explanation for the people’s health status and disease risk [9]. Assessment of the dietary and
nutritional status of the population is also essential to monitor the ongoing nutrition transition in
a country [6]. As a developing country, no studies have been carried out to investigate the
information on the diet of Sri Lankans and their nutritional status at a national level. Since Sri
Lanka is a multi-cultural country, peoples’ foods and dietary habits at a national level should be
assessed with a representative sample of Sri Lankan adults, which will be more useful to
implement health policies and to initiate many interventions. By keeping this view in mind, the
current dietary survey was carried out to assess the intakes of energy, macro-nutrients and
selected other nutrients with respect to socio-demographic characteristics and the nutritional
status of Sri Lankan adults focusing on diet-related metabolic chronic disease.
METHODOLOGY
Study sampling and the subjects
The eligible respondents of this study were healthy Sri Lankan adults aged >18 years recruited
from a sub-sample of the Sri Lanka Diabetes and Cardiovascular Study [4]. In this study, a total
of 600 subjects were randomly selected representing all nine provinces. This sample population
was then stratified for area of residence and ethnicity. Description of sample selection is
published elsewhere [10]. Ethical approval for this study was obtained from the Ethical Review
Committee, Faculty of Medicine, University of Colombo, Sri Lanka.
Measurements
Socio-demographic variables
The selected subjects were initially contacted via telephone or a postal notice by the study team
and the information regarding the study was provided in order to obtain their willingness to
participate in the study. On the study day, the purpose of the study was briefly explained to the
subjects and information sheets related to the study were also given out. Written consent was

Chapter 6: Manuscript 5 121
obtained from each volunteer prior to data collection. Socio-demographic details and diabetes
status were obtained by using an interviewer-administered questionnaire and body weight and
height were measured using a standard method. Areas of residence, ethnicities, and education
levels were categorized according to Sri Lankan governmental standards [11]. Body mass index
(BMI) was calculated by weight (in kilograms) divided by height squared (in meters) and several
cut-offs were presented as recommended by WHO experts for Asian populations [12].
Dietary assessment
Dietary data were obtained from a 24 HDR method. Subjects were asked to recall all foods and
beverages consumed over the previous 24-hour period. Respondents were probed for the types of
foods and food preparation methods. For uncommon mixed meals, the details of recipes and
preparation methods were collected at the time of taking the 24 HDR. Dietary recalls were
collected by two trained nutritionists who had received uniform training and adhered to the
standard operating procedure (SOP). As dietary assessment aids, the standard household
measurements such as plate, bowl, cup, glass, and different spoons etc. and food photograph
atlases were used to facilitate the quantification of portion sizes. One medium-sized coconut
spoon of rice was taken as 100 g, a full plate as 400 g, one cup of liquid as 150 ml, one glass of
liquid as 200 ml, a table spoon as 15 g and a tea spoon was taken as 5 g. For different curries,
weights of average respective amounts were taken. Household measurements were clarified by
demonstration of the real utensils and the food portion size photographs. When subjects recalled
some food amount in grams, that information was directly entered. Further details of dietary
assessment were published previously [10].
Data analysis
All foods recorded in 24 HDR were converted into grams and then, the intake of total energy,
macro nutrients (Carbohydrate, Protein and Fat), sodium and dietary fiber were analyzed using
122 Chapter 6: Manuscript 5
NutriSurvey 2007 (EBISpro, Germany) which was modified for Sri Lankan food recipes. As no
updated nutritional database has been gathered for some Sri Lankan food, we used the US
Department of Agriculture (USDA) nutrient database [13] as our standard to estimate nutrient
content in addition to local and regional food composition databases [14, 15]. Due to the absence
of energy and nutrient information on local mixed cooked dishes, we used a cookery book [16].
All the recipes were accepted after checking for face validity by consulting local housewives and
nutritionists. According to recipes, ingredients were weighed to the nearest 1 g for edible
portions of the foods. Then food items were cooked accordingly and the end product was
weighed. Nutritional composition of the final meal was calculated by entering nutritional values
and the weight of individual ingredients to the spreadsheet. The sum of each nutrient was
computed and standardized to 100 g of final product. We also excluded participants whose
reported daily energy intake was not between 800 and 4200 kcal to identify under- and over-
reporters of food intake [17].
Statistical Analysis
All data were doubly entered and rechecked in Microsoft Excel 2007. Data sorting and cleaning
were carried out before data analysis. Data on energy, macro-nutrients and some selected
nutrient intakes were transferred from the NutriSurvey 2007 to the Minitab version 15.0 for
statistical analysis. Nutrient intake distributions are presented as mean ±SE, median, 25th and
75th percentiles to characterize population intake levels for socio-demographic characteristics
(gender, ethnicity, age groups, and educational levels) and BMI categories. One-way ANOVA
and t-test were used to examine the differences in mean intakes energy and nutrients intakes. P
value < 0.05 was considered statistically significant.
Chapter 6: Manuscript 5 123
RESULTS
Socio-demographic profile
From 600 subjects, 491 (81.8%) participated and 28 under-reported their energy intake.
Accordingly, a total of 463 (77.2%) were included for the analysis. Socio-demographic profiles
and BMI categories of subjects are presented in Table 6.1. The majority of subjects were from
rural areas (59.7%) with 33% of the population from urban areas and the balance from the estate
sector (tea plantation area) 7.3%. The majority were women (n=297). By ethnic group, the
following were represented: Sinhalese (78%), Sri Lankan Tamil (9%), Indian Tamil (7%), and
Muslim (6%). Adults between the age of 41 and 50 years formed the biggest group (25.27%)
while the smallest group was the youngest adults aged between 18-30 yrs (13.17%). It was
significant that a majority of the study population (39%) had received formal education up to
Ordinary Level. The next largest group was adults (25%) who had studied up to Advanced
Level.
Energy intake
Table 6.2 represents the distribution of energy intake of Sri Lankan adults. The mean energy
intake of men was significantly higher (1912.7 kcal/d) than that of women (1513.6 kcal/d)
(p<0.05). People living in the estate sector had a significantly lower energy intake compared to
both the urban and rural subjects (p<0.05). Muslims had the highest intake of daily energy
(1748.8 kcal) while Indian Tamils had the lowest (1437.7 kcal/d) a statistically significant
difference for both men and women (p<0.05). Calorie consumption of both gender groups
declined gradually with age. Energy intake increased gradually with educational level.
According to BMI categories, lower energy levels were reported in both extremes and no distinct
pattern was seen.

124 Chapter 6: Manuscript 5
Carbohydrate intake
The mean daily carbohydrate intake is shown in Table 6.3. The total mean carbohydrate intake
of Sri Lankan adults was approximately 304.4 g (71.2% of total energy from carbohydrates as
shown in Figure 1). By strata, rural adults had a higher intake of carbohydrate (307.7 g) than
their estate counterparts (270.3 g). Mean carbohydrate intake was highest in Sinhalese (308.7 g)
and lowest in Indian Tamils (269.9 g). Male adults’ carbohydrate intake (352.4 g/day) was
significantly higher than that of women (277.5 g/day) and carbohydrate intake declined with age.
Protein intake
Sri Lankan adults recorded a mean daily protein intake of 44.6 g with men’s intake (52.8 g)
significantly higher than that of women (40.0 g). As shown in Table 6.4, rural (42.9 g/day) and
estate (43.7g/day) adults had similar daily intakes of protein. However, by ethnicity, mean
protein intake was significantly higher in Muslims (52.2 g) compared others. The youngest age
group also consumed significantly more protein than others, but only in men.
Fat intake
Estimated daily mean fat intake of Sri Lankan adults was 35 g. A more or less similar fat
consumption was noted for rural and urban residents (Table 6.5) whereas estate people had
significantly lower intake of fat (24.76 g; p>0.05). The youngest age group recorded the highest
fat intake (37.7 g) while the lowest intake was observed in the oldest age group (30.8 g). By
ethnic group, Muslims had the highest fat intake (44.7 g) whilst the Indian Tamils had the lowest
(24 g), being significantly lower than Muslims (p<0.05). With education level, fat consumption
increased, particularly among men. Adults with a normal BMI and BMI >25 - < 27.5 kgm-2 had
a higher fat intake than other BMI categories.
Chapter 6: Manuscript 5 125
Energy contribution from macro nutrients
As a whole, 71.2% of total calories came from carbohydrates, 10.8% from protein and 18.9%
from fat. Comparisons of the percentage of total calories derived from macronutrients according
to socio-demographic profile and BMI categories are shown in Figure 6.1. By ethnic group,
Muslims consumed more energy from fat (22.3%) while Indian Tamils had the lowest amount of
fat (15.5%) and highest intake of carbohydrates (75%). The percentage of calories from protein
was relatively higher among the graduates. In contrast, adults who did not receive a formal
education had a higher percentage of calories from carbohydrates compared to other groups.
There was no difference in energy distribution between diabetic and non-diabetic subjects.
Dietary fiber
The daily mean dietary fiber intake of Sri Lankan adults was 18.1 g (men: 21.3 g; women: 16.3
g; p<0.05). By area of residence, estate adults had a higher dietary fiber intake (20.6 g) than their
urban and rural counterparts (Table 6.6). Mean dietary fiber intake was highest in Indian Tamils
(20.6 g) and lowest in Sinhalese (17.6 g) (p<0.05). Dietary fiber intake increased with
educational level and a similar trend was observed for women as men. Daily dietary fiber intake
was always higher among men than women from different socio-demographic backgrounds.
Adults aged >60 years had the lowest intake of fiber.
Sodium
Daily mean sodium intake was 3.26 g and 2.51 g for men and women, respectively (p<0.05).
Dietary sodium intake of Sri Lankan adults according to demographic and BMI categories is
shown in Table 6.7. Mean sodium intake of rural adults was 2.89 g, followed by urban adults
(2.73 g). The Estate sector had the lowest intake (2.48 g). Muslims and Sri Lankan Tamils had a
higher intake of sodium than Sinhalese and Indian Tamils. With aging, sodium intake declined
and the youngest age group recorded the highest intake (3.04 g).
126 Chapter 6: Manuscript 5
DISCUSSION
Although national dietary and nutrition surveys have a number of important functions and can
provide much valuable information, Sri Lanka had never conducted a national food consumption
survey, probably due to lack of human and financial resources. This is the first attempt to report
energy and macronutrient intakes in a fairly representative sample over the island using updated
food composition data. Subject distribution of ethnic groups, area of residence and educational
levels closely mirror the national statistics [11].
Differences in calorie consumption were seen according to demographic and BMI categories.
Men typically consume larger portions of foods and are expected to derive a higher amount of
energy than their female counterparts [18]. The daily intake of energy by Sri Lankan men was
found to be higher than that of women by about 350 kcal. Similar differences were reported
among Malaysian adults [19] and in Britain where the difference was nearly 700 kcal [20].
When compared to people living in urban and rural areas, estate workers consume fewer
calories. Lower mean energy intake was also reported among Malaysian estate workers [21].
The decline in calorie consumption with age was probably due to a reduction in physical activity
levels and poor appetite, particularly in older adults. Different energy intakes in ethnic groups
may represent their cultural eating habits. For instance, Muslim people tend to have a higher
energy intake and eat more fat rich food items compared to Indian Tamils. Up to A/L (12 years
education) by education level, energy consumption gradually increased, which is probably
associated with increased purchasing power with higher education status; however, graduate
groups may be also aware of health issues associated with excess caloric intake. In developed
countries, calorie consumption is inversely associated with education levels [22]. Except for the
very obese category, consumption of total energy intake rose steadily with BMI category.
Under-reporting of food intake by obese subjects is well documented [23].

Chapter 6: Manuscript 5 127
The total daily intake of protein in Sri Lankan adults is almost half that of US adults and, among
Americans, two-thirds of all protein is derived from animal sources [24]. In contrast, plant
sources (rice and pulses) are the main contributors of protein among Sri Lankan adults [10,25].
American men consume over 100 g of fat daily and for women, 65 g [26]. Corresponding values
for Sri Lankans are 40.5 g and 31.9 g, respectively. In addition to the amount of fat, the type of
fat is crucial for the development of diet-related chronic diseases such as cardiovascular disease.
Although sub-types of fat are not reported in this analysis, the main lipid source in the Sri
Lankan diet is coconut milk/oil which is high in saturated fatty acids [27]. Therefore, it is
important to conduct further studies to explore the coconut consumption and associated
cardiovascular disease risk in this population.
According to the ranges of population nutrient intake goals recommended by WHO, the
percentage of energy from total carbohydrates, fats and proteins should be 15-30%, 55-75% and
10-15%, respectively [28]. British adults consume less than fifty percent of calories (men:
47.7%; women: 48.5%) from carbohydrates, whilst fat intake contributes 35.8% and 34.9% of
total calories for men and women, respectively. The contribution of protein as an energy source
is 16.5% for both sexes [20]. In contrast to Western countries, Malaysians derive nearly 60% of
their energy from carbohydrates, 14% of energy from protein and the rest from fats [19]. In
contrast to Western countries and some Asian countries, Sri Lankan adults consume
proportionally more carbohydrates (>71% of calories) and less fat (<19% of calories) and
proteins (<11%). The prevalence of diabetes in Sri Lanka is 11% and one-fifth of adults are
suffering from diabetes despite low levels of obesity (BMI >30 kg/m2 = 3.7%) [4]. Since the
study is cross-sectional in nature, we cannot conclude that the association between the relatively
larger contribution of energy from carbohydrate and higher prevalence of diabetes/dysglycemia
among Sri Lankan adults, in spite of carbohydrates contributing over 70% of energy for both
128 Chapter 6: Manuscript 5
diabetics and non-diabetics. Longitudinal studies assessing the prospective risk of developing
diabetes and the proportion of energy derived from macronutrients are needed to fully elucidate
an association. A high intake of carbohydrate may lead to hyperinsulinaemia, high serum TAG
and low HDL-cholesterol levels and chronic consumption of large carbohydrate meals may
cause postprandial hyperglycaemia and hypertriacylglycerolaemia and eventually develop
insulin resistance and diabetes [29].
A generous intake of dietary fiber reduces risk of developing many diseases including coronary
heart disease, stroke, hypertension, diabetes, obesity, and certain gastrointestinal disorders as
well as improving metabolic parameters and immune functions [30]. The definition, method of
measuring fiber and recommendations varies in different countries. The backbone of our food
composition data is based on Food Composition Databases USDA. According to US guidelines,
the current recommendation is to consume 14 g fiber per every 1000 kcal, therefore using the
energy guideline of 2000 kcal/day for women and 2600 kcal/day for men, the recommended
daily dietary fiber intake is 28 g/day for adult women and 36 g/day for adult men [31]. Although
Sri Lankan adults consume fewer calories compared to US adults, their dietary fiber intake is
insufficient according to their calorie intake.
Epidemiological, clinical and animal experimental evidence showed a direct relationship
between dietary electrolyte consumption and blood pressure [32]. Furthermore, clinical trials
show that a reduction in salt (NaCl) intake reduces BP levels in normotensive and hypertensive
populations and prevents the development of hypertension [32]. Recommended Na intake is a
maximum of 2.3 g/day [32]. Our findings showed that most Sri Lankan adults exceed current
recommendations. The high consumption of sodium may be associated with the epidemic of
hypertension (Men: 18.8%; Women: 19.3%) among Sri Lankan adults [33].
Chapter 6: Manuscript 5 129
This study has several limitations. Sri Lanka has over 20 million inhabitants. Therefore, diet
records of a sample of 463 subjects may not represent the eating patterns of the whole
population. However, a well-conducted UK NDNS [20] measured the dietary records of 1724
respondents and achieved a lower response rate of 47%. Considering available resources, the
high response rate and satisfactory representation of demographic parameters, we believe this is
a practical sample size. Secondly, 24 HDR may not be the best tool to determine habitual diet,
however, random 24 HDR in a large sample has been used in other national surveys [7]. Thirdly,
our findings were limited to energy and selected major macronutrients due to sub-quality
nutritional information on sub-categories of macronutrients and micronutrients of Sri Lankan
mixed dishes (Table 6.8). Another limitation is that despite reports of high alcohol consumption
among Sri Lankan men [34], alcohol intake was under-reported in our study (<0.5%). In this
survey, low energy reporters (<800 kcal/day) were excluded, therefore exclusion will have
biased the data towards higher intakes. Lastly, we did not attempt to correlate energy intake and
its adequacy to this population as calorie recommendations may vary with several factors such as
gender, age, body weight, body composition and physical activity level.
Acknowledging the limitations of the survey, the present study provides the first national
estimates of energy and nutrient intake of the Sri Lankan adult population. It is evident that
consumption of high levels of carbohydrate, fat mainly from saturated sources, low protein, low
dietary fiber and high levels of sodium may have detrimental effects on health and be related to
the current epidemic of NCDs. Unfortunately, current food-based dietary guidelines are based on
limited research [25]. Therefore, well-designed and nationally representative studies are needed
to explore the association between diet and chronic disease among Sri Lankan adults. Moreover,
regular diet and nutrition surveys should be carried out to obtain information on dietary patterns

130 Chapter 6: Manuscript 5
and nutrient intakes and, ideally, periodical monitoring is needed to identify the changing trends
in food intake and to assess public responses to dietary recommendations.
Chapter 6: Manuscript 5 131
REFERENCE LIST
1. Popkin B.M. HS, Kim S.,: The Nutritional Transition and Diet-Related Chronic Diseases in Asia: Implications for Prevention. Washington, DC: International Food Policy Research Institute FCND Discussion Paper 2001, 105.
2. Jayasekara R, Schultz T: Health status, trends, and issues in Sri Lanka. Nursing & Health Sciences 2007, 9:228-233.
3. Katulanda P, Ranasinghe P, Jayawardena R, Sheriff R, Matthews D: Metabolic syndrome among Sri Lankan adults: prevalence, patterns and correlates. Diabetology & Metabolic Syndrome 2012, 4:24.
4. Katulanda P, Constantine GR, Mahesh JG, Sheriff R, Seneviratne RD, Wijeratne S, Wijesuriya M, McCarthy MI, Adler AI, Matthews DR: Prevalence and projections of diabetes and pre-diabetes in adults in Sri Lanka--Sri Lanka Diabetes, Cardiovascular Study (SLDCS). Diabet Med 2008, 25:1062-1069.
5. Premaratne R, Amarasinghe A, Wickremasinghe AR: Hospitalisation trends due to selected non-communicable diseases in Sri Lanka, 2005-2010. Ceylon Med J 2005, 50:51-54.
6. Walter Willett EL: Nutritional epidemiology. In Monographs in Epidemiology and Biostatistics. Edited by Willett W: Oxford University Press; 1998: 101-147
7. University of Otago and Ministry of Health: A Focus on Nutrition: Key findings of the 2008/09 New Zealand Adult Nutrition Survey. In Book A Focus on Nutrition: Key findings of the 2008/09 New Zealand Adult Nutrition Survey. (Editor ed.^eds.). City: Ministry of Health; 2011.
8. Giskes K, Turrell G, Patterson C, Newman B: Socio-economic differences in fruit and vegetable consumption among Australian adolescents and adults. Public Health Nutr 2002, 5:663-669.
9. Sasaki S: The value of the National Health and Nutrition Survey in Japan. Lancet 2011, 378:1205-1206.
10. Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Hills AP: Consumption of Sri Lankan adults: an appraisal of serving characteristics Public Health Nutrition 2012, FirstView Article : pp 1-6.
11. Statistical Abstract [http://www.statistics.gov.lk/abstract2010/Pages/index.htm] 12. WHO expert consultation: Appropriate body-mass index for Asian populations and
its implications for policy and intervention strategies. The Lancet 2004, 363:157-163. 13. USDA: Foods List. In Book Foods List (Editor ed.^eds.), 24 edition. City; 2012. 14. Perera W.D.A. JPM, Thaha S.Z., : Tables of food composition for use in Sri Lanka. 1979. 15. Gopalan C. RBV, Balasubramanian S.C.,: Nutritive value of Indian foods. Hyderabad;
1989. 16. Dissanayake C: Ceylon Cookery. 9 edn. Sri Lanka: Stamford Lake (pvt) Ltd; 2010. 17. Azadbakht L, Mirmiran P, Esmaillzadeh A, Azizi F: Dietary diversity score and
cardiovascular risk factors in Tehranian adults. Public Health Nutrition 2006, 9:728-736.
18. Caster WO: Systematic estimation of food intakes from food frequency data. Nutrition Research 1986, 6:469-472.
19. Mirnalini K ZM, Safiah MY, Tahir A, Siti Haslinda MD, Siti Rohana D, Khairul Zarina MY, Mohd Hasyami S & Normah H,: Energy and Nutrient Intakes: Findings from the Malaysian Adult Nutrition Survey (MANS). Mal J Nutr 2008, 14:1-24.

132 Chapter 6: Manuscript 5
20. Swan G: Findings from the latest National Diet and Nutrition Survey. Proc Nutr Soc 2004, 63:505-512.
21. Chee SS ZH, Ismail MN, and Ng KK,: Anthropometry, dietary patterns and nutrient intakes of Malaysian estate workers. Mal J Nutr 1996, 2:112-126.
22. Rennie KL, Jebb SA: Prevalence of obesity in Great Britain. Obes Rev 2005, 6:11-12. 23. Heitmann BL, Lissner L: Dietary underreporting by obese individuals--is it specific
or non-specific? BMJ 1995, 311:986-989. 24. Smit E, Nieto FJ, Crespo CJ, Mitchell P: Estimates of animal and plant protein intake
in US adults: results from the Third National Health and Nutrition Examination Survey, 1988-1991. J Am Diet Assoc 1999, 99:813-820.
25. Samaranayake U.M.M. et al.: Food Base Dietary Guidelines for Sri Lanka. Colombo: Nutrition Devision, Ministry of Healthcare and Nutrition, Sri Lanka; 2011.
26. Kennedy ET, Bowman SA, Powell R: Dietary-fat intake in the US population. J Am Coll Nutr 1999, 18:207-212.
27. Amarasiri W: Coconut fats. Ceylon Med J 2009, 51. 28. Report of a Joint WHO/FAO Expert Consultation: Diet, Nutrition and the prevention
of Chronic Diseases. In Book Diet, Nutrition and the prevention of Chronic Diseases (Editor ed.^eds.). City; 2003.
29. Misra A, Khurana L, Isharwal S, Bhardwaj S: South Asian diets and insulin resistance. Br J Nutr 2009, 101:465-473.
30. Anderson JW, Baird P, Davis RH, Jr., Ferreri S, Knudtson M, Koraym A, Waters V, Williams CL: Health benefits of dietary fiber. Nutr Rev 2009, 67:188-205.
31. USDA: The Food Supply and Dietary Fiber: Its Availability and Effect on Health. In Book The Food Supply and Dietary Fiber: Its Availability and Effect on Health (Editor ed.^eds.), vol. 36. City: U.S. Department of Agriculture; 2007.
32. Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D, Obarzanek E, Conlin PR, Miller ER, 3rd, Simons-Morton DG, et al: Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med 2001, 344:3-10.
33. Wijewardene K, Mohideen MR, Mendis S, Fernando DS, Kulathilaka T, Weerasekara D, Uluwitta P: Prevalence of hypertension, diabetes and obesity: baseline findings of a population based survey in four provinces in Sri Lanka. The Ceylon medical journal 2005, 50:62-70.
34. Rahav G, Wilsnack R, Bloomfield K, Gmel G, Kuntsche S: The influence of societal level factors on men's and women's alcohol consumption and alcohol problems. Alcohol and alcoholism (Oxford, Oxfordshire) Supplement 2006, 41:i47-55.
.

Chapter 6: Manuscript 5 133
Table 6-1: Socio-demographic characteristics of the survey population
Characteristics Total (n = 463) Men (n = 166) Women (n = 297) n % n % n %
Area of Residence Urban Rural Estate
153 276 34
33.04 59.61 7.34
45 102 19
26.51 61.45 11.45
108 174 15
36.36 58.58 5.05
Age group (yrs) 18-29 30-39 40-49 50-59 >60
61 84 117 106 95
13.17 18.14 25.27 22.89 20.52
27 23 38 40 38
16.26 13.85 22.89 20.10 22.89
34 61 79 66 57
12.73 22.85 29.59 24.72 21.35
Ethnicity Sinhala Muslim Sri Lankan Tamil Indian Tamil
360 27 42 34
77.75 5.83 9.07 7.34
118 8 20 20
71.08 4.82 12.05 12.05
242 19 22 14
8.15 6.40 7.41 4.71
Educational Level No Schooling Up to 5 years Up to O/L Up to A/L Graduate
27 113 182 116 25
58.31 24.41 39.31 25.05 5.39
11 43 59 46 07
6.62 25.90 35.54 27.71 4.22
16 70 123 70 18
5.39 23.57 41.41 23.57 6.06
BMI Category < 18.5 kg.m-2
> 18.5 - < 22.9 kg.m-2 > 23 - < 24.99 kg.m-2
> 25 - < 27.5 kg.m-2 > 27.5 kg.m-2
64 163 76 95 65
13.82 35.21 16.41 20.52 14.04
29 75 21 32 09
17.47 45.18 12.65 19.28 5.42
35 88 55 63 56
11.78 29.63 18.52 21.12 18.86

134 Chapter 6: Manuscript 5
Table 6-2: Energy intake (kcal) of Sri Lankan adults by socio-demographic characteristics
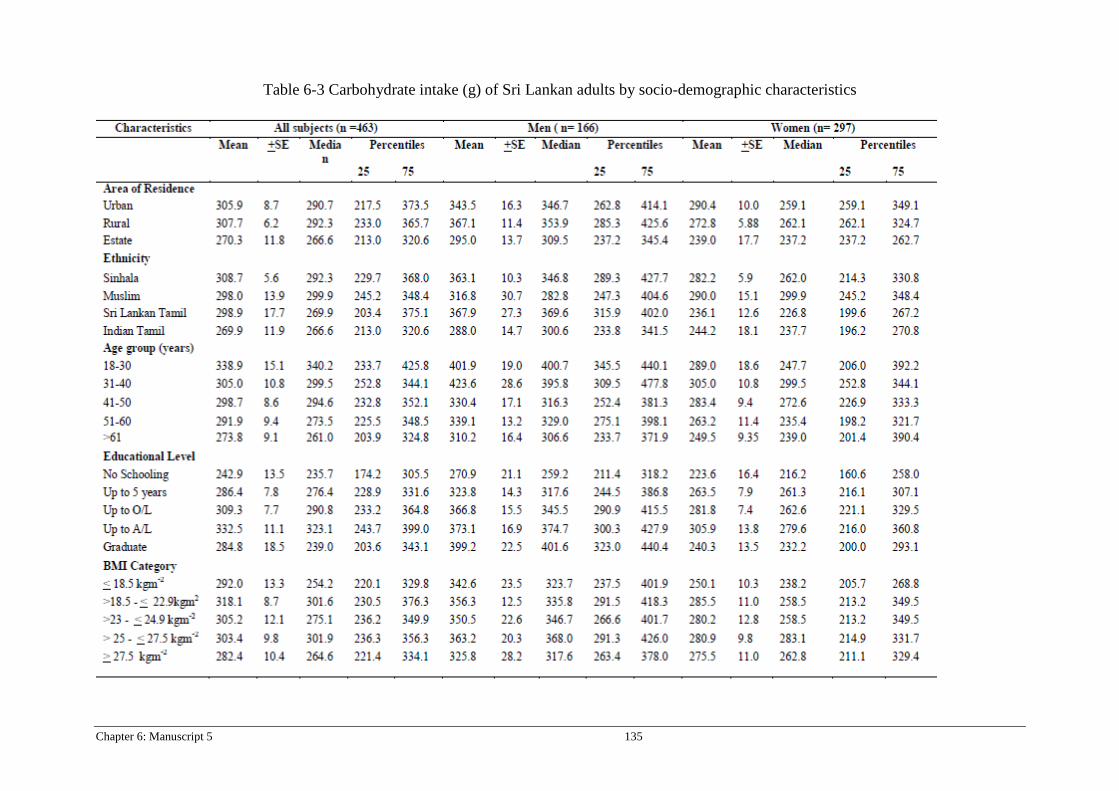
Chapter 6: Manuscript 5 135
Table 6-3 Carbohydrate intake (g) of Sri Lankan adults by socio-demographic characteristics

136 Chapter 6: Manuscript 5
Table 6-4 Protein intake (g) of Sri Lankan adults by socio-demographic characteristics

Chapter 6: Manuscript 5 137
Table 6-5 Fat intake (g) of Sri Lankan adults by socio-demographic characteristics
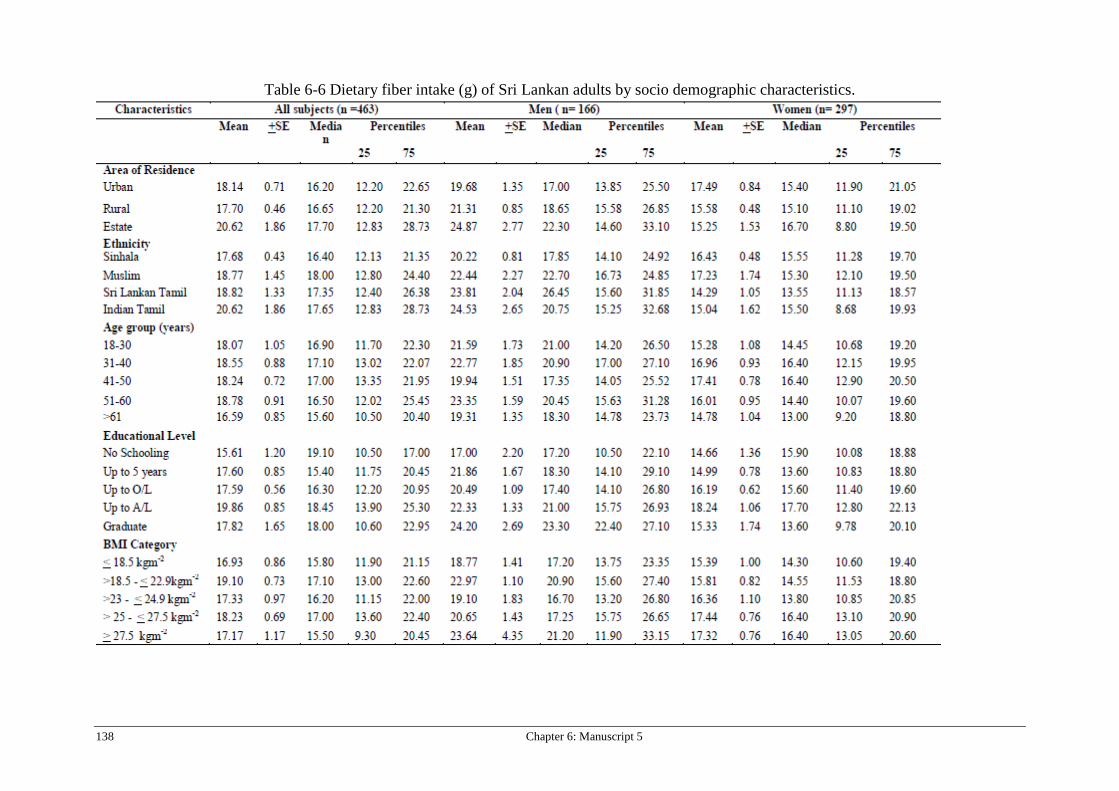
138 Chapter 6: Manuscript 5
Table 6-6 Dietary fiber intake (g) of Sri Lankan adults by socio demographic characteristics.
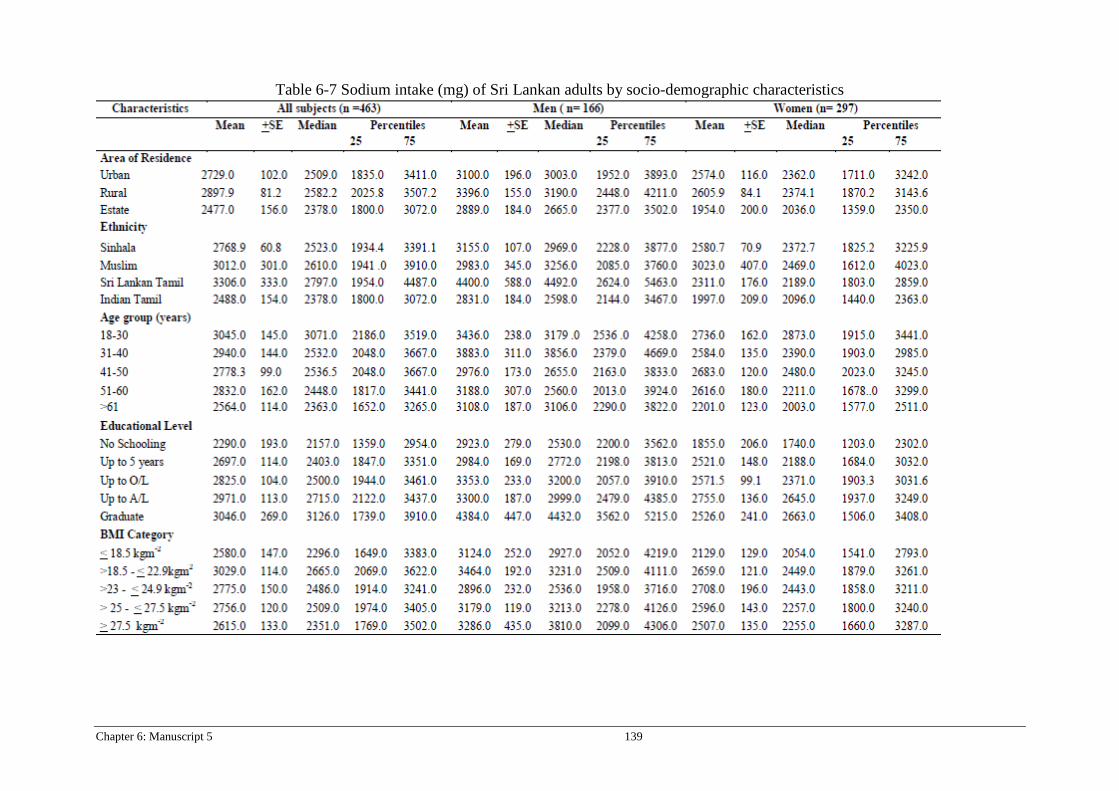
Chapter 6: Manuscript 5 139
Table 6-7 Sodium intake (mg) of Sri Lankan adults by socio-demographic characteristics

140 Chapter 6: Manuscript 5
Table 6-8: Mean Daily Micronutrient Intake by Sri Lankan Adults.
Micronutrients
All subjects Men Women Mean
SD SE Median
Percentiles Mini mum
Maxi mum
Mean
SD SE Median
Percentiles Mini mum
Maxi mum
Mean
SD SE Median
Percentiles Mini mum
Maxi mum 25th 75th 25th 75th 25th 75th
Vitamin A_µg (n= 393)
215 169 8.57 163 106 254 50.4 954 208.0 172 14.5 150 99.0 239 51.3 954 225 171 11.1 179 108 278 50.4 917
Vitamin C_mg (n=413)
26.5 20.5 1.31 16.8 9.93 32.2 4.80 158 25.1 24.7 2.04 16.5 10.0 26.1 5.40 158 28.0 27.9 1.77 17.2 10.0 33.6 4.80 147
Vitamin D_ µg (n=334)
5.55 9.45 0.52 2.00 1.00 3.93 0.08 47.4 5.70 9.23 0.89 2.00 1.00 4.26 0.08 47.4 5.67 9.79 0.67 2.00 1.00 3.90 0.08 45.1
Vitamin B1_ mg (n=472)
1.36 0.62 0.03 1.27 0.94 1.69 0.15 5.01 1.64 0.68 0.05 1.58 1.19 1.88 0.50 5.01 1.26 0.53 0.03 1.16 0.87 1.54 0.15 3.88
Vitamin B2_ mg(n=472)
0.99 0.76 0.04 0.79 0.48 1.26 0.10 5.23 1.08 0.77 0.06 0.88 0.53 1.35 0.10 5.23 0.98 0.76 0.05 0.76 0.48 1.23 0.12 5.04
Vitamin B6_ mg (n=472)
1.65 5.34 0.25 0.62 0.32 1.11 0.04 63.3 1.93 6.01 0.47 0.78 0.38 1.26 0.04 53.2 1.54 5.06 0.30 0.58 0.32 1.10 0.04 63.3
Vitamin B12 µg (n=454)
1.46 2.28 0.11 0.77 0.33 1.47 0.01 21.2 1.72 3.27 0.26 0.64 0.26 1.51 0.10 21.2 1.43 2.16 0.13 0.78 0.35 1.46 0.01 15.5
Folic acid_ µg (n=414)
31.4 19.1 0.94 30.0 15.9 42.5 0.30 95.0 33.9 22.7 1.78 35.0 18.6 45.0 0.30 118 25.4 19.4 1.15 24.0 10.0 37.5 0.34 95.0
Pottasium_mg (n=472)
1405 578 26.6 1325 1012 1723 294 5119 1649 653 51.2 1532 1216 2071 477 5119 1314 481 28.4 1258 995 1613 294 3180
Calcium_mg (n=470)
408 218 10.0 364 264 494 106 1486 463 250 19.6 404 309 520 133 1486 401 225 13.0 360 262 483 106 1827
Magnesium_mg (n=471)
219 125 5.77 186 133 266 45.0 1217 253 141 11.1 211 156 303 72.8 8446 211 126 7.48 180 128 241 45.0 1217
Phosphorus_mg (n=472)
810 364 16.8 750 540 1007
204 2771 970 421 33.0 915 674 1187
225 2771 751 293 17.3 717 530 927 204 1930
Iron_mg (n=472)
11.1 6.18 0.29 9.81 7.14 13.8 2.54 59.5 10.5 5.10 0.30 9.49 7.08 13.1 2.54 35.0 12.9 7.59 0.60 11.4 8.29 15.9 2.92 59.5
Zinc_mg (n=472)
8.84 6.50 0.29 7.10 5.33 9.90 1.34 45.2 10.8 7.82 0.61 8.26 6.44 11.4 2.03 42.7 7.90 5.39 0.32 6.76 5.27 8.74 1.34 45.2
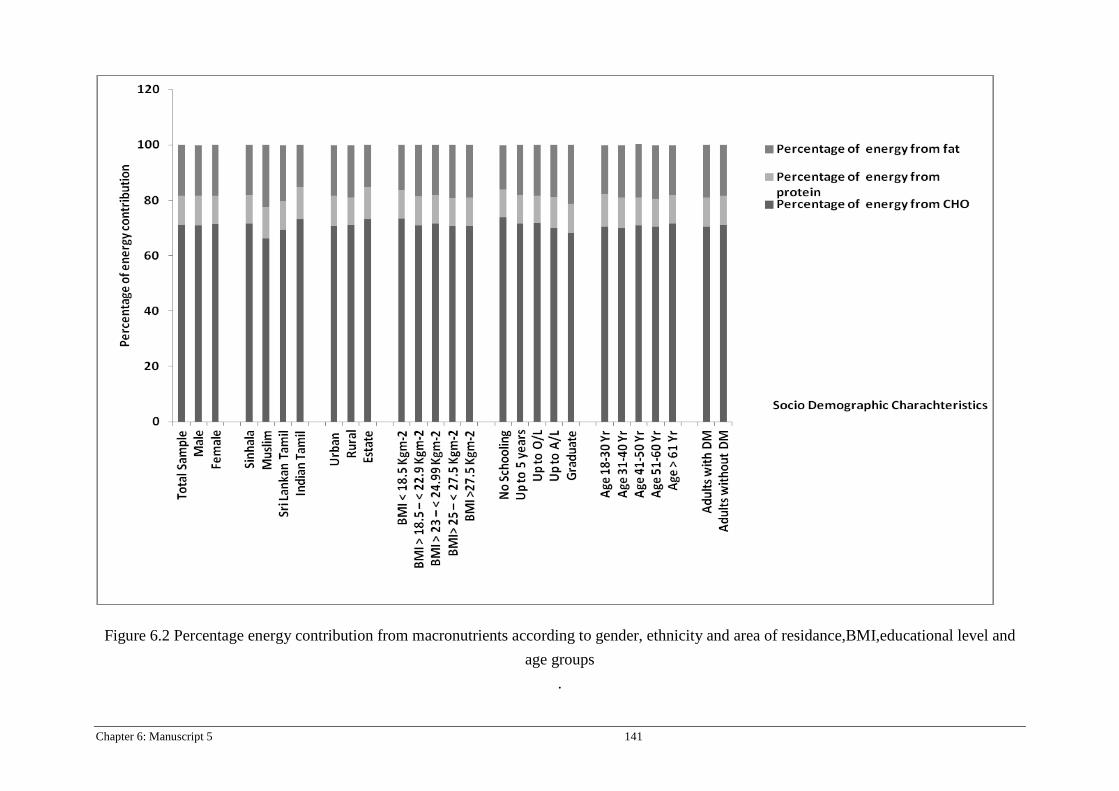
Chapter 6: Manuscript 5 141
Figure 6.2 Percentage energy contribution from macronutrients according to gender, ethnicity and area of residance,BMI,educational level and age groups
.
Chapter 7: Manuscript 6 and 7 142
Chapter 7: Manuscript 6 and 7
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: The obesity epidemic in Sri Lanka revisited Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
Chapter 7: Manuscript 6 and 7 143
CHAPTER 7A: MANUSCRIPT 6
Letter to the editor
The obesity epidemic in Sri Lanka revisited.
Ranil Jayawardena MBBS, MSc1,2, Nuala M. Byrne MSc PhD1, Mario J. Soares MBBS
MSc PhD3, Prasad Katulanda MD DPhil2, Andrew P. Hills MSc PhD4
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka.
3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health
Sciences, Curtin University, Perth, WA, Australia.
4Mater Mothers’ Hospital, Mater Medical Research Institute and Griffith Health Institute,
Griffith University, Brisbane, Queensland, Australia.
Citation
R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. (2012) The obesity epidemic in
Sri Lanka Revisited. Asia Pac J Public Health. doi: 10.1177/1010539512464650. 2012 Nov 27.
[Epub ahead of print]

144 Chapter 7: Manuscript 6 and 7
Obesity has reached epidemic levels in most affluent countries. In contrast, South Asia is
presently considered a minimally affected region as malnutrition and infectious diseases are still
their main health concerns (1). South Asians have poor attitudes toward obesity and being obese
considered as sign of prosperity (2).
Sri Lanka is a low-middle income South Asian country with a population of over 20 million.
Obesity and associated metabolic problems are emerging as major health problems in the
country with an estimated 20% of all adults suffering from dysglycemia and 11% from Type 2
diabetes (3). The Sri Lanka Diabetes and Cardiovascular Disease Study (SLDCS) was conducted
between 2005-2006 and reported an obesity prevalence (≥25 kg.m-2) of 14.3% and 19.4% in
males and females, respectively (4). In early 2011, we revisited random sub-samples from the
SLDCS and in addition we collected data from the previously missing North and Eastern
provinces in the SLDCS. In total, six hundred adults were approached from 12 clusters of 50
participants each. Details of the study design and sample selection have been described in detail
elsewhere (5). While we believe this is the first report from Sri Lanka to include the North and
Eastern provinces, we did encounter poorer participation of males with only single clusters being
measured in some of these regions. Age adjusted prevalence of overweight (BMI ≥23 kg.m-2),
obesity (BMI ≥25 kg.m-2) and abdominal obesity (Men: WC ≥ 90 cm; Women: WC ≥ 80 cm)
were categorized according to Asia-pacific anthropometric cut-offs (6).
Four hundred and ninety adults participated in the study giving us a response rate of 82%. Mean
age was 48.1 ±14.8 years. The majority of the study population were ‘Sinhalese’ in ethnicity
(n=377, 76.9%), educated up to grade 11 (n=189, 38.6%), were female (n= 321, 65.5 %) and
resided in rural areas (n=287, 58.7%). Age-adjusted prevalence (95%CI) of overweight, obesity
and abdominal obesity among Sri Lankan adults were 17.1(13.8-20.7)%, 28.8(24.8-33.1)% and
30.8(26.8-35.2)%, respectively. Men compared to women, were less overweight but not

Chapter 7: Manuscript 6 and 7 145
statistically [14.2 (9.4-20.5)% vs. 18.5 (14.4-23.3)%, p<ns], obese [21.0 (14.9-27.7)% vs. 32.7
(27.6-38.2)%, p<0.05] and abdominally obese [11.9 (7.4-17.8)% vs. 40.6 (35.1-46.2)%, p<0.05].
The prevalence of obesity in 1990 was 7.0% and 13.4% for men and women in Colombo
suburbs (7), but by 2000 the overall obesity prevalence had doubled to 19.2% in the same study
area (8). Our study which covers a greater area of Sri Lanka shows an obesity prevalence of 21%
for men and 32.5% for women. Compared to the original SLDCS data, we found a higher overall
prevalence of overweight and abdominal obesity. Levels of overweight and abdominal obesity
are clearly higher among women compared to men. In such comparisons of data, there could be
heterogeneity between studies due to sampling, selected study areas, age group representation
and clinical cut-offs of obesity. The large upward shift in the prevalence of overweight between
SLDCS and our data would in part reflect these facets and needs further investigation. However
they would also reflect changes in environmental factors such as increased availability of
calorie-dense foods post-war (4), and improvements in socio-economic status of the country.
Hwang et al. reported that each kg.m-² of BMI gained was associated with an 18% increase in
the risk of developing hypertension and a 26% increase in risk for the metabolic syndrome (9).
Already a quarter of Sri Lankan adults are suffering from metabolic syndrome (10). It is time
that legislators, clinicians and public health authorities give this issue their considered attention
to begin the process of reversing this alarming trend. Recent consensus reports provide a good
framework for action that could be tailored to suit the needs of Sri Lanka.
146 Chapter 7: Manuscript 6 and 7
Reference list
1. Balkau B, Deanfield JE, Després J-P, Bassand J-P, Fox KAA, Smith SC, et al.
International Day for the Evaluation of Abdominal Obesity (IDEA). Circulation. 2007 October
23, 2007;116(17):1942-51.
2. Simkhada P, Poobalan A, Simkhada PP, Amalraj R, Aucott L. Knowledge, Attitude, and
Prevalence of Overweight and Obesity Among Civil Servants in Nepal. Asia-Pacific Journal of
Public Health. 2011 July 1, 2011;23(4):507-17.
3. Katulanda P, Constantine GR, Mahesh JG, Sheriff R, Seneviratne RDA, Wijeratne S, et
al. Prevalence and projections of diabetes and pre-diabetes in adults in Sri Lanka—Sri Lanka
Diabetes, Cardiovascular Study (SLDCS). Diabetic Medicine. 2008;25(9):1062-9.
4. Katulanda P, Jayawardena MAR, Sheriff MHR, Constantine GR, Matthews DR.
Prevalence of overweight and obesity in Sri Lankan adults. Obesity Reviews. 2010;11(11):751-
6.
5. Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Hills AP. Food consumption of Sri
Lankan adults: an appraisal of serving characteristics. Public Health Nutrition.FirstView:1-6.
6. WHO/IASO/IOTF. The Asia-Pacific Perspective: Redefining Obesity and its
Treatment.2000.
7. Fernando D.J.S. SSH, De Silva D.R., Perera S.D.,. The prevalence of obesity and other
coronary risk factors in a suburban Sri Lankan community. Asia Pacific J Clin Nutr. 1994;3:155-
9.
8. Malavige GN, de Alwis NMW, Siribaddana SH, Weerasooriya N, Fernando DJS.
Increasing diabetes and vascular risk factors in a sub-urban Sri Lankan population. Diabetes
research and clinical practice. 2002;57(2):143-5.
9. Hwang LC, Bai CH, Sun CA, Chen CJ. Prevalence of metabolically healthy obesity and
its impacts on incidences of hypertension, diabetes and the metabolic syndrome in Taiwan. Asia
Pac J Clin Nutr. 2012;21(2):227-33.
10. Katulanda P, Ranasinghe P, Jayawardena R, Sheriff R, Matthews D. Metabolic syndrome
among Sri Lankan adults: prevalence, patterns and correlates. Diabetology & Metabolic
Syndrome. 2012;4(1):24.

Chapter 7: Manuscript 6 and 7 147
CHAPTER 7B: MANUSCRIPT 7
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: The obesity epidemic in Sri Lanka revisited and High dietary diversity is associated with obesity in Sri Lankan adults: an evaluation of three dietary scores Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Bijesh Yadav statistical analysis Andrew Hills Study design, data interpretation and revision
of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date

148 Chapter 7: Manuscript 6 and 7
TITLE PAGE
High dietary diversity is associated with obesity in Sri Lankan adults: an
evaluation of three dietary scores
Ranil Jayawardena1,2*, Nuala M. Byrne1, Mario J. Soares3, Prasad Katulanda2, Bijesh Yadav4,
Andrew P. Hills5
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka.
3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health
Sciences, Curtin University, Perth, WA, Australia.
4Department of Biostatistics, Christian Medical College, Vellore, India
5Mater Mothers’ Hospital, Mater Medical Research Institute and Griffith Health Institute,
Griffith University, Brisbane, Queensland, Australia.
Citation
R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills (2013). High dietary diversity is
associated with obesity in Sri Lankan adults. BMC Public Health 13:314.
Chapter 7: Manuscript 6 and 7 149
ABSTRACT
Background: Dietary diversity is recognized as a key element of a high quality diet. However,
diets that offer a greater variety of energy-dense foods could increase food intake and body
weight. The aim of this study was to explore association of diet diversity with obesity in Sri
Lankan adults.
Methods: Six hundred adults aged >18 years were randomly selected by using multi-stage
stratified sample. Dietary intake assessment was undertaken by 24-hour dietary recall. Three
dietary scores, Dietary Diversity Score (DDS), Dietary Diversity Score with Portions (DDSP)
and Food Variety Score (FVS) were calculated. Body mass index (BMI) ≥ 25 kg.m-2 is defined
as obesity and Asian waist circumference cut-offs were used to diagnose abdominal obesity.
Results: Mean of DDS for men and women were 6.23 and 6.50 (p=0.06), while DDSP was 3.26
and 3.17, respectively (p=0.24). FVS values were significantly different between men and
women 9.55 and 10.24 (p=0.002). Dietary diversity among Sri Lankan adults was significantly
associated with gender, residency, ethnicity, education level but not with diabetes status. As
dietary scores increased, the percentage consumption was increased in most of food groups
except starches. Obese and abdominal obese adults had the highest DDS compared to non obese
groups (p<0.05). With increased dietary diversity the level of BMI, waist circumference and
energy consumption was significantly increased in this population.
Conclusion: Our data suggests that dietary diversity is positively associated with several socio-
demographic characteristics and obesity among Sri Lankan adults. Although high dietary
diversity is widely recommended, public health messages should emphasize to improve dietary
diversity in selective food items.
150 Chapter 7: Manuscript 6 and 7
INTRODUCTION
Dietary diversity and variety have long been recognized as key elements of high quality diets. A
diverse diet increases the probability of nutrient adequacy among adults [1] and leads to positive
health outcomes such as reduced complications of diabetes [2], incidence of several cancers [3,
4] and all-cause mortality [5]. As dietary factors are associated with increased risk of chronic
diseases, local and international dietary recommendations promote increased dietary diversity
but limiting saturate fats, refined sugar and salt. However, lack of dietary diversity is a major
nutritional concern over among deprived people from the low-income countries [6]. Changing
from a monotonous diet to one with varied food types has been shown to improve energy and
nutrient intakes in the people from developing countries. The demographic and economic
transition that many developing countries are undergoing is producing important changes in diet
and lifestyle that greatly impact on disease risks [7]. Despite under-nutrition and nutrient
deficiencies being a major concern in developing countries, the recent nutrition transition and
changes in physical activity patterns, diet-related metabolic problems have emerged as an
alarming public health problem in many developing countries, particularly among urban
dwellers [8].
Sri Lanka is a low-middle income country undergoing rapid epidemiological and nutritional
transition. Despite nutritional deficiencies such as iron deficiency anemia, vitamin A deficiency
and protein energy malnutrition being reported in some segments of the Sri Lankan population
[9], non-communicable diseases (NCDs) are also emerging as the major diet-associated health
problem in Sri Lanka. The prevalence of overweight, obesity and central obesity among Sri
Lankan adults was 25.2%, 9.2% and 26.2%, respectively in 2005-2006, as defined by Asian
Body Mass Index (BMI) cut-offs [10], a clear upward trend [11]. The age-adjusted prevalence of
Metabolic Syndrome among Sri Lankan adults was 24.3% (95% CI: 23.0–25.6) [12]. The
Chapter 7: Manuscript 6 and 7 151
prevalence of obesity-related metabolic problems such as diabetes and hypertention among Sri
Lankan adults was 13-14% and 18-19%, respectively [13]. Moreover, in Sri Lanka, diet-related
chronic diseases currently account for 18.3% of all deaths and 16.7% of hospital expenditure
[14].
Although prevalence rates are higher in affluent countries, obesity and abdominal obesity are
becoming major public health concerns in South Asia [15]. Causes of obesity are multi-factorial,
among them various dietary factors play an important role. Association between individual
nutrients and obesity/abdominal obesity has been widely researched, but little attention has been
given to overall dietary diversity and obesity/abdominal obesity. Dietary diversity is an indicator
of overall diet. Higher diet variety is associated with increased intake of fiber and vitamins [16]
and on the other hand, increased variety contributes to high calorie consumption [17]. Sri Lanka
has an interesting socio-economic relationship with obesity. For instance, higher wealth and
education is positively associated with obesity among Sri Lankan adults [10]. Therefore,
evaluating the association between diet diversity and obesity is interesting to explore in this
population. Exploring the underlying associations between obesity and dietary diversity are very
important as lifestyle interventions can change dietary diversity in different populations.
Accordingly, the aim of this study was to explore association of diet diversity with obesity in Sri
Lankan adults.
METHODOLOGY
Study design and sample selection
Subjects were recruited from a subset of the Sri Lanka Diabetes and Cardiovascular Study [18].
Six hundred adults aged >18 years were randomly selected using a multi-stage stratified sample.
Details of sample selection have been published elsewhere [10, 19]. Ethical approval for this
study was obtained from the Ethical Review Committee, Faculty of Medicine, University of
152 Chapter 7: Manuscript 6 and 7
Colombo, Sri Lanka and informed consent was obtained from the subjects before the data was
collected.
Dietary Assessment
Dietary intake assessment was undertaken by a 24-hour dietary recall by trained nutritionists in a
random day to obtain ‘usual’ intake. Although multiple 24–hour passes may be more
representative of ‘usual’ intake, a single 24-hour recall is considered the best reference period to
assess dietary diversity as longer reference periods result in less accurate information due to
imperfect recall [20]. However, if the previous 24-hour period is atypical due to a special
occasion or illness, a different day was selected for the interview. We collected a detailed
description of the foods eaten and the amount was estimated using food photographs and
common household utensils. For mixed dishes, food types were disaggregated before ingredients
were categorized into appropriate food groups as detailed earlier [19].
Socio-demographic and anthropometric
Socio-demographic details and clinical status (self-reported diabetes) were collected from
interviewer-administrated questionnaire. Height was measured using a portable Holtain
Stadiometer (Chasmors Ltd, London, UK) to the nearest 0.1 cm. Body weight was measured
using a SECA electronic scale (Hamburg, Germany) to the nearest 0.1 kg. Most participants
were weighed wearing light clothes and after fasting. Waist circumference was measured using a
tape to the nearest 0.1 cm at the midpoint between the lower costal border and the top of the iliac
crest, at the end of normal expiration. BMI was calculated by dividing body weight (in
kilograms) by height (in meters squared). Definition of overweight (BMI ≥23 kg.m-2), obesity
(BMI ≥25 kg.m-2) and abdominal obesity (Men: WC ≥90 cm; Women: WC ≥80 cm) were
categorized according to Asia-pacific anthropometric cut-offs [10].

Chapter 7: Manuscript 6 and 7 153
Dietary Diversity Score (DDS)
A DDS was defined as the total count of different food groups irrespective of the amount
consumed by individuals over the 24-hour period. All the food items consumed by subjects were
categorized into 12 food groups which were starch (cereals, tubers, roots and starchy vegetables
such as jackfruits), vegetables, green leafy vegetables (green salads and ‘Mallum’), fruits, fish
(including dried fish and seafood) meat (including poultry, egg), legumes (including nuts and
seeds except coconut), milk (including all dairy products), beverages (tea, coffee and fizzy
drinks), oils and fats (coconut products were included), sweets and miscellaneous (e.g. alcohol).
The choice of the 12 food groups was based on the local and international food grouping
techniques adapting cultural context [20, 21]. So the maximum score was 12, one point given for
each group consumed during the registration period.
Dietary Diversity Score with Portions (DDSP)
We defined DDSP considering major food groups in the Sri Lankan food pyramid as starch,
vegetables, green leafy vegetables, meat [meat/poultry/egg], fish [fish/dry fish/sea foods], milk
[milk/dairy products], pulses and fruits [21]. DDSP was calculated applying a minimum
consumption of one portion for respective food groups. Details of the portion sizes were
published previously [19]. The maximum score for DDSP was 8.
Food Variety Score (FVS)
FVS was defined as the number of different food items eaten during last 24–hour period [16].
The total number of foods included irrespective of quantity consumed. There is no maximum
value here.
Data Analysis
Statistical Package for Social Sciences software version 16 (SPSS Inc., Chicago, IL, USA) was
used to conduct all the statistical analyses. Descriptive data are presented as means and SDs.
Percentage of consumption of different food groups according to DDS and DDSP were sorted.

154 Chapter 7: Manuscript 6 and 7
DDS and FVS were further categorized to groups according to DDS and FVS values. Then BMI,
WC and energy intake were calculated for the groupings of dietary diversity values. Total energy
was analyzed using NutriSurvey 2007 (EBISpro, Germany) software. Independent samples test
and ANOVA were used to compare the means. For all statistical tests, a P value <0.05 was
accepted as significant.
RESULTS
The response rate was 80% (n=481) and details of the subjects’ characteristics are reported in
table 7.1. Mean of DDS for men and women were 6.23 and 6.50 (p=0.06), while DDSP was 3.26
and 3.17, respectively (p=0.24). FVS values were significantly different between men and
women 9.55 and 10.24 (p=0.002). Several socio-demographic parameters were significantly
associated with all three dietary diversity parameters. People living in the estate areas had the
lowest DDS, DDSP and FVS compared to both urban and rural. Similarly, Indian Tamils had
lowest values for all three diet diversity parameters. Higher education level was associated with
increased dietary scores but not for age categories. Adults with BMI ≥25.0 kg.m-2 had the
highest DDS, DDSP and FVS values. Centrally obese participants had significantly higher DDS,
DDSP and FVS values but no significant difference was seen between diabetic and non-diabetic.
Table 7.2 shows the distribution pattern of consumption of foods from different food groups
among Sri Lankan adults according to DDS. Minimum DDS was 2 and maximum was 11 out of
12. As DDS increased, the percentage consumption was increased in most of food groups except
starch as everybody consumes starch from DDS value of 2. Cereals were the most commonly
consumed food groups among Sri Lankans with the lowest DDS and DDSP scores. Milk and
dairy product intake increased slowly, but gradually with both DDS and DDSP, whereas meat
products are consumed by a significant proportion of the population only at higher dietary scores
(DDS ≥8; DDSP ≥5). Pulses reach more than 50% from DDS value of 3, followed by
Chapter 7: Manuscript 6 and 7 155
vegetables, beverages from DDS of 4. However, meat/poultry/egg reached ≥50% at the DDS of
10. Similar to DDS patterns, DDSP also showed maximum value for starch group but lower
values for green leafy vegetables, meat, milk and fruits (Table 7.3).
Mean BMI, WC and energy intakes were gradually increased with DDS, DDSP and FVS
categories (table 7.4). Participants with 2-5 DDS value had a BMI of 22.16 kg.m-2 and WC of
77.0 cm which gradually rose up to a BMI of 23.82 kg.m-2 and WC of 80.04 cm with DDS 8-11
category. Energy consumption also followed the same pattern.
DISCUSSION
Sri Lankan adults had relatively low dietary diversity values, in particular, relatively higher FVS
and DDS and lower DDSP value indicates that although people consume several types of food
items, the amount of consumption is low for many food groups. The WHO STEP Survey
reported that 3% of Sri Lankan consume more than five fruits and vegetable per day [22].
Rathnayake et al. reported much lower mean DDS (4.4) and FVS (8.4) among group of rural
elderly people [23]. DDS, DDSP and FVS values for Indian Tamils were remarkably less than
Sinhalese and Muslim ethnic groups. It is reported that malnutrition and nutritional deficiencies
are highest in the estate sector where most of Indian Tamils are living [9]. Although we have
lack of data on nutrient adequacy in this study sample, one can postulate that low dietary
diversity may cause deficiencies among Sri Lankan adults. People with better education may
have high profile occupations and greater purchasing power which could lead to higher
consumption of different food varieties. Although no previous data are available on dietary
diversity among Sri Lankan adults, children who lived in the estate sector had a lower dietary
diversity [24]. Moreover, lower maternal education was negatively associated with receiving a
diverse diet for those children [24]. Obese and abdominal obese participants had higher DDS,
DDSP and FVS values compared to non-obese and non-abdominally obese groups.

156 Chapter 7: Manuscript 6 and 7
Sri Lankans consume an excess of starchy foods but lower amount of fruits, vegetables and dairy
products [19]. Table 7.2 and 7.3 showed that 100% values for the starch group in every DDS and
DDSP indicated that starchy staple food was the most common food group in Sri Lankan meals.
Nearly five percent participants had almost complete starch meals without a significant amount
of other food groups across the whole day, due to some people consuming cereal (e.g. rice) with
a starchy vegetable (e.g. potato curry). Predominantly carbohydrate diets result in an elevation in
plasma glucose, insulin, triglycerides and non-esterified fatty acids leading to insulin resistance
[25]. Total carbohydrate intake is associated with risk of diabetes among South Indian adults
[26]. High prevalence of diabetes and its complications among Sri Lankan adults may be
associated with starch-based but poor variety meals [18, 27]. Amongst the food groups of the
dietary pyramid, meat, green leafy vegetables, milk and fruits were least frequently consumed.
Increased intake of fruits and vegetables could play a protective role against obesity-associated
metabolic risk factors in South Indians who are prone to premature coronary artery disease [28].
Reasons for the monotonous diet among many Sri Lankan adults needs to be further explored
despite it being associated with a low obesity level. Public health initiatives to improve
appropriate diversity of the diet are important.
Torheim et al. reported a positive correlation between energy intake and DDS, as well as variety
of different food groups in Mali [29]. When a diet is composed of foods that differ on sensory
characteristics such as colour, flavour and shape may cause hyperphagia [30]. One hypothesis
for the increase intake of food consumption with higher food variety is due to hedonic ratings of
a food eaten to sensation decrease with different food items [30]. Animal and human studies
showed that food intake increases when there is more variety in a meal or diet and that greater
dietary variety is associated with increased body weight and subsequently obesity [30]. Dietary
variety within food groups was positively associated with body fatness among healthy adults
[31]. Several studies showed a positive correlation between calorie intake and dietary diversity

Chapter 7: Manuscript 6 and 7 157
[17, 29]. On the contrary, an inverse association between DDS and obesity/abdominal adiposity
was reported among the female students of Isfahan University [32]. In US women, low BMI was
associated with higher DDS; in US men, there was no clear relation of BMI to dietary diversity
[5]. Our results show a positive association between all three dietary diversity indices with
calorie intake suggesting that consumption of a large number of food items may lead to
excessive intake of energy and weight gain. Although many dietary guidelines promote
consumption of varied diet, it should be selective (e.g. vegetables) rather than absolute in
number. Moreover, food guide pyramids are not designed to maintain energy balance, but show
nutritional adequacy and balance [17]. Increased dietary diversity in health promotion may not
be appropriate for combating the obesity epidemic in Sri Lanka. A reduction in dietary variety of
highly palatable and energy-rich foods may be a more appropriate strategy to prevent and treat
obesity in the country. At the same time, to prevent deficiencies foods with high nutrient but low
energy (e.g. green vegetables, low fat milk) should be encouraged.
Limitations
We used a single 24-hour recall to obtain usual intake, however multiple dietary recalls during
weekdays and weekends may provide a better picture of the habitual diet. In the nutritional
literature, DDS and FVS are widely used and show appropriate correlation with nutritional status
and association with chronic disease. Simple counting of food groups or consumed food items
are used to define diet diversity scores. These methods have limitations. First, although it is not
easy to distinguish healthy and unhealthy food items, these counting systems are assigned equal
values for every food item respective of the health outcome (e.g. fruits and sweets). Second, the
distributions of individual food quantities are not considered by count measures. In this exercise
we defined DDSP with consumption of minimum of one portion of respective food groups;
however we did not define an upper limit. Drescher et al. recommend considering health values

158 Chapter 7: Manuscript 6 and 7
of consumed food items in measuring healthy food diversity [33]. Another limitation is that we
did not measure the diversity within food groups and most Sri Lankan dishes are mixed in
nature, which causes considerable practical limitations for food item groupings. Furthermore,
there are no updated food composition tables for Sri Lankan mixed dishes, in particular for
micronutrients. Therefore, we were not able to calculate nutrient adequacy ratio and mean
adequacy ratio. Moreover, lack of physical activity data among this population limits our ability
to calculate daily energy requirements. Absence of economical statues may limit the performing
multivariate analysis. However, the main aim of this study was to explore the associations
between dietary diversity/variety and obesity.
A follow-up study showed an inverse dietary diversity-mortality association was adjusted for
potential dietary and socio-demographic confounders [5]. DDS is population-specific and there
is no standard scoring method, therefore it is invariably difficult to compare DDS values among
different countries. Because of the cross-sectional nature of this study, we cannot express long-
term health outcomes with regarding dietary diversity among Sri Lankan adults. Moreover,
obesity is associated with multiple socio-economic factors which could be possible confounding
factors for diet diversity. Prospective studies are needed to explore association between dietary
diversity and weight gain/obesity.
Acknowledging the limitations of this study, these results showed the dietary diversity, portion
consumption and number of food item intakes according to different socio-demographic
characteristics. Globally, normative data on ‘ideal’ or ‘target’ levels of diversity are usually not
available. Therefore, our results can be used to assess the current picture of the dietary diversity
among Sri Lankan adults. Repeating a similar study in a given time may help to assess
improvements in food security and expected changes in the population. Illangasekara et al.
(2004) reported temporal trends in the prevalence of diabetes mellitus in a rural community in
Sri Lanka which is closely accompanied by an increase in the monthly income [34]. However,
Chapter 7: Manuscript 6 and 7 159
there is a lack of data on changes in dietary habits in this population with related to epidemic of
diabetes and other diet-associated metabolic disorders. As our aim was to assess individual diet
diversity our sample included predominantly housewives as in Sri Lanka the majority of people
consume homemade foods. These results can therefore be used as household dietary diversity
values and may indicate the socio-economic level of the household [20].
In conclusion, our data suggests that dietary diversity and variety are associated with obesity
among Sri Lankan adults. High dietary diversity is widely recommended as it can be used as a
proxy indicator of nutrient adequacy. Therefore, public health messages should emphasize how
to improve dietary diversity in selected food items. Further studies are needed to confirm this
finding on other diet-associated chronic diseases.
160 Chapter 7: Manuscript 6 and 7
REFERENCE LIST
1. Foote JA, Murphy SP, Wilkens LR, Basiotis PP, Carlson A: Dietary Variety Increases
the Probability of Nutrient Adequacy among Adults. The Journal Of Nutrition 2004,
134:1779-1785.
2. Wahlqvist ML, Lo CS, Myers KA: Food variety is associated with less macrovascular
disease in those with type II diabetes and their healthy controls. J Am Coll Nutr
1989, 8:515-523.
3. Fernandez E, D'Avanzo B, Negri E, Franceschi S, La Vecchia C: Diet diversity and the
risk of colorectal cancer in northern Italy. Cancer Epidemiol Biomarkers Prev 1996,
5:433-436.
4. Lucenteforte E, Garavello W, Bosetti C, Talamini R, Zambon P, Franceschi S, Negri E,
La Vecchia C: Diet diversity and the risk of squamous cell esophageal cancer. Int J
Cancer 2008, 123:2397-2400.
5. Kant AK, Schatzkin A, Harris TB, Ziegler RG, Block G: Dietary diversity and
subsequent mortality in the First National Health and Nutrition Examination
Survey Epidemiologic Follow-up Study. The American Journal Of Clinical Nutrition
1993, 57:434-440.
6. Ruel MT: Operationalizing Dietary Diversity: A Review of Measurement Issues and
Research Priorities. The Journal Of Nutrition 2003, 133:3911S-3926S.
7. Popkin B: Nutrition in transition: the changing global nutrition challenge. Asia
Pacific Journal of Clinical Nutrition 2001, 10:13-18.
8. Caballero B, Rubinstein S: Environmental factors affecting nutritional status in
urban areas of developing countries. Arch Latinoam Nutr 1997, 47:3-8.
9. Meera Shekar AS, Lidan Du, : Malnutrition in Sri Lanka: Scale, Scope, Causes, and
Potential Response. In Book Malnutrition in Sri Lanka: Scale, Scope, Causes, and
Potential Response (Editor ed.^eds.). City: Human Development Unit, South Asia
Region; 2007.
10. Katulanda P, Jayawardena MA, Sheriff MH, Constantine GR, Matthews DR: Prevalence
of overweight and obesity in Sri Lankan adults. Obes Rev 2010.
11. Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Hills AP: The Obesity Epidemic
in Sri Lanka Revisited. Asia Pac J Public Health 2012.
Chapter 7: Manuscript 6 and 7 161
12. Katulanda P, Ranasinghe P, Jayawardena R, Sheriff R, Matthews D: Metabolic
syndrome among Sri Lankan adults: prevalence, patterns and correlates.
Diabetology & Metabolic Syndrome 2012, 4:24.
13. Wijewardene K, Mohideen M, Mendis S, Fernando D, Kulathilaka T, Weerasekara D,
Uluwitta P: Prevalence of hypertension, diabetes and obesity: baseline findings of a
population based survey in four provinces in Sri Lanka. Ceylon Medical Journal
2005, 50:62.
14. Popkin B.M. HS, Kim S.,: The Nutritional Transition and Diet-Related Chronic
Diseases in Asia: Implications for Prevention. Washington, DC: International Food
Policy Research Institute FCND Discussion Paper 2001, 105.
15. Ramachandran A, Snehalatha C: Rising burden of obesity in Asia. J Obes 2010, 2010.
16. Hatloy A, Torheim LE, Oshaug A: Food variety--a good indicator of nutritional
adequacy of the diet? A case study from an urban area in Mali, West Africa. Eur J
Clin Nutr 1998, 52:891-898.
17. Mirmiran P, Azadbakht L, Azizi F: Dietary diversity within food groups: an indicator
of specific nutrient adequacy in Tehranian women. J Am Coll Nutr 2006, 25:354-361.
18. Katulanda P, Constantine GR, Mahesh JG, Sheriff R, Seneviratne RDA, Wijeratne S,
Wijesuriya M, McCarthy MI, Adler AI, Matthews DR: Prevalence and projections of
diabetes and pre-diabetes in adults in Sri Lanka—Sri Lanka Diabetes,
Cardiovascular Study (SLDCS). Diabetic Medicine 2008, 25:1062-1069.
19. Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Hills AP: Consumption of Sri
Lankan adults: an appraisal of serving characteristics Public Health Nutrition 2012,
FirstView Article : pp 1-6.
20. Anne Swindale PB: Household Dietary Diversity Score (HDDS) for Measurement of
Household Food Access: Indicator Guide (v.2). In Book Household Dietary Diversity
Score (HDDS) for Measurement of Household Food Access: Indicator Guide (v.2)
(Editor ed.^eds.). City: Academy for Educational Development; 2006.
21. Samaranayake U.M.M. et al.: Food Base Dietary Guidelines for Sri Lanka. Colombo:
Nutrition Devision, Ministry of Healthcare and Nutrition, Sri Lanka; 2011.
22. Somatunga LC: NCD Risk Factor Survey in Sri Lanka (STEP Survey). In Book NCD
Risk Factor Survey in Sri Lanka (STEP Survey) (Editor ed.^eds.). City: WHO; 2004.
23. Rathnayake K, Madushani P, Silva K: Use of dietary diversity score as a proxy
indicator of nutrient adequacy of rural elderly people in Sri Lanka. BMC Research
Notes 2012, 5:469.
162 Chapter 7: Manuscript 6 and 7
24. Senarath U, Godakandage SSP, Jayawickrama H, Siriwardena I, Dibley MJ:
Determinants of inappropriate complementary feeding practices in young children
in Sri Lanka: secondary data analysis of Demographic and Health Survey 2006–
2007. Maternal & Child Nutrition 2012, 8:60-77.
25. Wolever TM, Mehling C: Long-term effect of varying the source or amount of
dietary carbohydrate on postprandial plasma glucose, insulin, triacylglycerol, and
free fatty acid concentrations in subjects with impaired glucose tolerance. The
American Journal Of Clinical Nutrition 2003, 77:612-621.
26. Mohan V, Radhika G, Sathya RM, Tamil SR, Ganesan A, Sudha V: Dietary
carbohydrates, glycaemic load, food groups and newly detected type 2 diabetes
among urban Asian Indian population in Chennai, India (Chennai Urban Rural
Epidemiology Study 59). Br J Nutr 2009, 102:1498-1506.
27. Katulanda P, Ranasinghe P, Jayawardena R, Constantine G, Sheriff MHR, Matthews D:
The prevalence, patterns and predictors of diabetic peripheral neuropathy in a
developing country. Diabetology & Metabolic Syndrome 2012, 4:21.
28. Radhika G, Sudha V, Mohan Sathya R, Ganesan A, Mohan V: Association of fruit and
vegetable intake with cardiovascular risk factors in urban south Indians. Br J Nutr
2008, 99:398-405.
29. Torheim LE, Ouattara F, Diarra MM, Thiam FD, Barikmo I, Hatloy A, Oshaug A:
Nutrient adequacy and dietary diversity in rural Mali: association and
determinants. Eur J Clin Nutr 2004, 58:594-604.
30. Raynor HA, Epstein LH: Dietary variety, energy regulation, and obesity. Psychol Bull
2001, 127:325-341.
31. McCrory MA, Fuss PJ, McCallum JE, Yao M, Vinken AG, Hays NP, Roberts SB:
Dietary variety within food groups: association with energy intake and body fatness
in men and women. The American Journal Of Clinical Nutrition 1999, 69:440-447.
32. Azadbakht L, Esmaillzadeh A: Dietary diversity score is related to obesity and
abdominal adiposity among Iranian female youth. PHNutr 2011, 14:62-69.
33. Drescher LS, Thiele S, Mensink GB: A new index to measure healthy food diversity
better reflects a healthy diet than traditional measures. J Nutr 2007, 137:647-651.
34. Illangasekera U, Rambodagalla S, Tennakoon S. Temporal trends in the prevalence of
diabetes mellitus in a rural community in Sri Lanka. J R Soc Health 2004; 124: 92–
94.
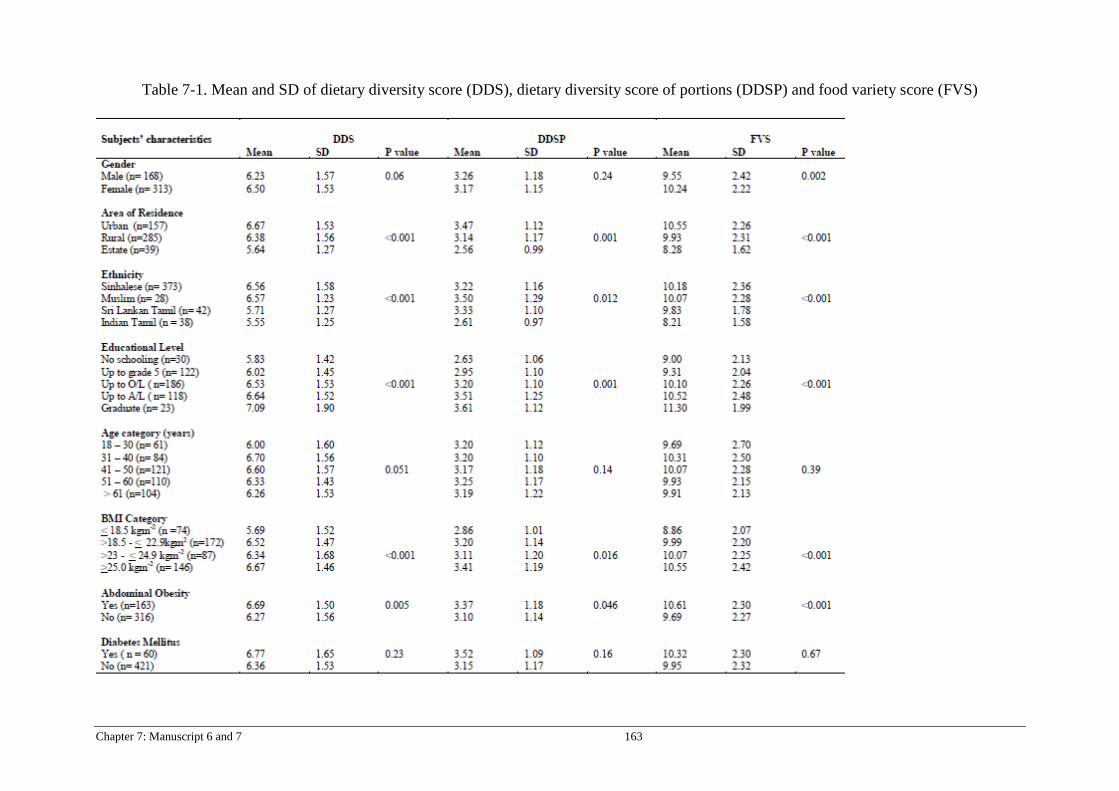
Chapter 7: Manuscript 6 and 7 163
Table 7-1. Mean and SD of dietary diversity score (DDS), dietary diversity score of portions (DDSP) and food variety score (FVS)
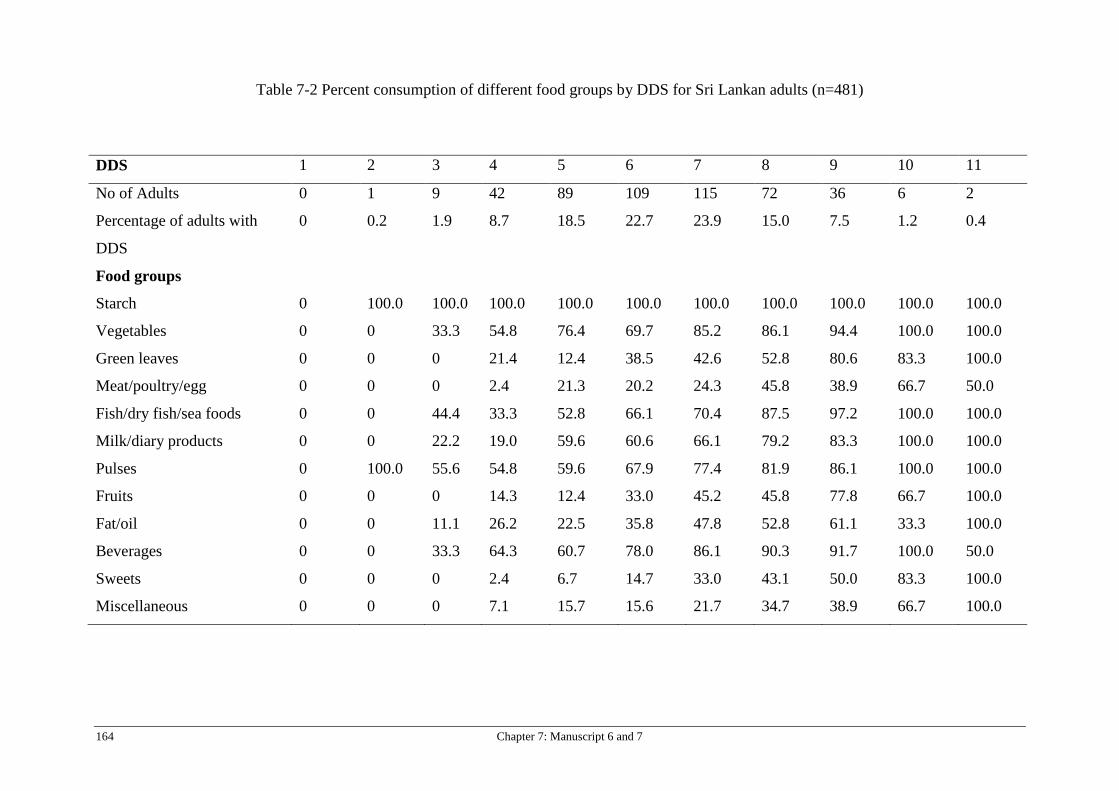
164 Chapter 7: Manuscript 6 and 7
Table 7-2 Percent consumption of different food groups by DDS for Sri Lankan adults (n=481)
DDS 1 2 3 4 5 6 7 8 9 10 11
No of Adults 0 1 9 42 89 109 115 72 36 6 2
Percentage of adults with
DDS
0 0.2 1.9 8.7 18.5 22.7 23.9 15.0 7.5 1.2 0.4
Food groups
Starch 0 100.0 100.0 100.0 100.0 100.0 100.0 100.0 100.0 100.0 100.0
Vegetables 0 0 33.3 54.8 76.4 69.7 85.2 86.1 94.4 100.0 100.0
Green leaves 0 0 0 21.4 12.4 38.5 42.6 52.8 80.6 83.3 100.0
Meat/poultry/egg 0 0 0 2.4 21.3 20.2 24.3 45.8 38.9 66.7 50.0
Fish/dry fish/sea foods 0 0 44.4 33.3 52.8 66.1 70.4 87.5 97.2 100.0 100.0
Milk/diary products 0 0 22.2 19.0 59.6 60.6 66.1 79.2 83.3 100.0 100.0
Pulses 0 100.0 55.6 54.8 59.6 67.9 77.4 81.9 86.1 100.0 100.0
Fruits 0 0 0 14.3 12.4 33.0 45.2 45.8 77.8 66.7 100.0
Fat/oil 0 0 11.1 26.2 22.5 35.8 47.8 52.8 61.1 33.3 100.0
Beverages 0 0 33.3 64.3 60.7 78.0 86.1 90.3 91.7 100.0 50.0
Sweets 0 0 0 2.4 6.7 14.7 33.0 43.1 50.0 83.3 100.0
Miscellaneous 0 0 0 7.1 15.7 15.6 21.7 34.7 38.9 66.7 100.0
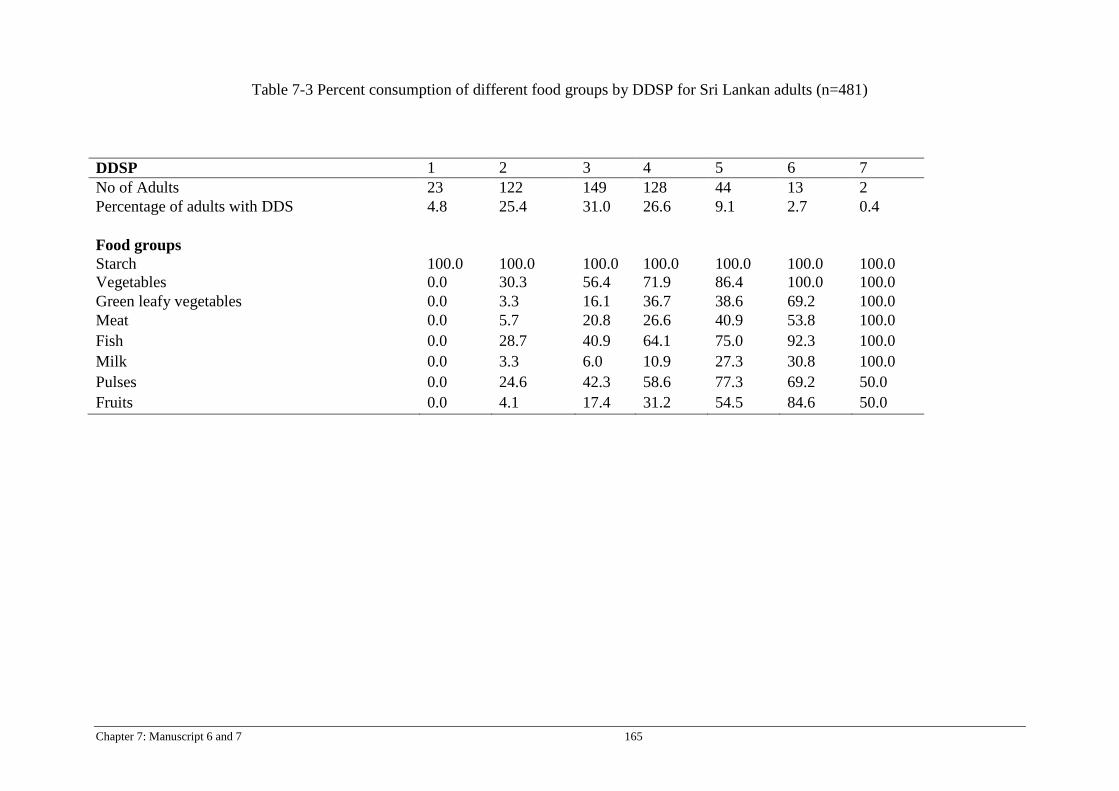
Chapter 7: Manuscript 6 and 7 165
Table 7-3 Percent consumption of different food groups by DDSP for Sri Lankan adults (n=481)
DDSP 1 2 3 4 5 6 7 No of Adults 23 122 149 128 44 13 2 Percentage of adults with DDS 4.8 25.4 31.0 26.6 9.1 2.7 0.4
Food groups Starch 100.0 100.0 100.0 100.0 100.0 100.0 100.0 Vegetables 0.0 30.3 56.4 71.9 86.4 100.0 100.0 Green leafy vegetables 0.0 3.3 16.1 36.7 38.6 69.2 100.0 Meat 0.0 5.7 20.8 26.6 40.9 53.8 100.0 Fish 0.0 28.7 40.9 64.1 75.0 92.3 100.0 Milk 0.0 3.3 6.0 10.9 27.3 30.8 100.0 Pulses 0.0 24.6 42.3 58.6 77.3 69.2 50.0 Fruits 0.0 4.1 17.4 31.2 54.5 84.6 50.0

166 Chapter 7: Manuscript 6 and 7
Table 7-4 Mean BMI, Waist circumference and energy intake of the subjects according to DDS, DDSP and FVS.
BMI (kgm-2) Waist circumference (cm) Energy intake Mean SD P values Mean SD P values Mean SD P values
DDS 2-5 (n=141) 22.16 4.11 0.002
77.00 10.48 0.034
1705 615 <0.001 6-7 (n=223) 23.38 4.24 79.39 10.50 1792 597
8-11 (n=116) 23.82 3.40 80.04 9.37 2004 580 DDSP 1-2 (n=144) 22.76 3.94
0.027
77.74 9.93 0.009
1652 609 <0.001
3 (n=149) 22.84 4.29 77.70 10.22 1739 540 4 (n=127) 23.24 4.12 79.80 10.88 1985 617 5-7(n=59) 24.54 3.34 82.14 9.19 2079 583 FVS 3–8 (n =121) 21.76 3.97
<0.001
76.16 10.08 0.002
1651 596 <0.001
9-10 (n= 271) 23.33 4.46 79.19 11.08 1804 633 11 (n=68) 23.28 3.35 78.69 9.03 1826 558 12–18 (n= 118) 24.14 3.55 81.16 9.46 2003 570

Chapter 8: Manuscript 8 167
Chapter 8: Manuscript 8
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Body weight perception and weight loss practices among Sri Lankan adults Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
168 Chapter 8: Manuscript 8
TITLE PAGE
Body weight perception and weight loss practices among Sri Lankan adults
Ranil Jayawardena 1,2*, Nuala M. Byrne 1, Mario J. Soares 3, Prasad Katulanda 2, Andrew P.
Hills 4
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka.
3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health
Sciences, Curtin University, Perth, WA, Australia.
4Mater Mothers’ Hospital, Mater Medical Research Institute and Griffith Health Institute,
Griffith University, Brisbane, Queensland, Australia.
Citation
R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. (2013) Body weight perception
and weight losing practices in Sri Lankan adults. Obesity Research and Clinical Practice
http://dx.doi.org/10.1016/j.orcp.2013.05.003

Chapter 8: Manuscript 8 169
ABSTRACT
Objectives: The purpose of the present study was to evaluate the association between self-
perception of body weight, waist circumference (WC) with body mass index (BMI) and WC cut-
offs and weight loss approaches among Sri Lankan adults.
Methods: A nationally representative sample of 600 adults aged ≥18 years was selected using a
multi-stage random cluster sampling technique. An interviewer-administrated questionnaire was
used to assess demographic characteristics, body weight perception, abdominal obesity
perception and details of weight losing practices. Weight, height and WC were measured and
BMI calculated. According to Asian anthropometric cut-offs levels, underweight (BMI >18.50
kg.m-2), normal-weight (BMI=18.50-22.99 kg.m-2), overweight (BMI=23-24.99 kg.m-2), obesity
(BMI ≥25 kg.m-2) and abdominal obesity (WC ≥90 cm in men and ≥80 cm in women) were
defined.
Results: Body weight misperception was common among Sri Lankan adults. Two-thirds of
overweight males and 44.7% overweight females considered themselves as ‘about right weight’,
moreover, 4.1% and 7.6% overweight men and women reported themselves as being
‘underweight’. Over one-third of both male and female obese subjects perceived themselves as
‘about right weight’ or ‘underweight’. Nearly 32% of centrally obese men and women perceived
that their WC is about right. Of the people who perceived themselves as overweight or very
overweight (n=154) only 63.6% tried to lose weight (n=98), and one quarter of adults sought
advice from professionals (n=39).

170 Chapter 8: Manuscript 8
Conclusion: Body weight misperception was common among underweight, healthy weight,
overweight, and obese adults in Sri Lanka. Over 2/3 of overweight and 1/3 of obese Sri Lankan
adults believe they are in right weight category or are under weight.
INTRODUCTION
The prevalence of obesity has reached epidemic levels in many parts of the world. World Health
Organization (WHO) estimations in 2008 indicated that 1.5 billion adults worldwide were
overweight, while nearly 500 million adults were suffering from obesity [1]. Obesity has also
become an emerging public health problem in Sri Lanka. Despite the limited availability of data,
previous studies have demonstrated a clear upward trend in age-adjusted prevalence of obesity in
Sri Lankan males and females; increasing from 7.0% (males) and 13.4% (females) in 1990 to
9.9% and 19.2%, respectively in 2000 [2]. In 2005, national level obesity prevalence data
showed that 25.2% of adults were overweight (BMI ≥23 kg.m-2) and 16.8% were obese (BMI
≥25 kg.m-2) [3]. One quarter of the Sri Lankan adult population are suffering from central
obesity, in particular, one in every two urban dwelling females are affected by abdominal obesity
[3]. Katulanda et al. have reported that female gender, urban living, higher level of education,
higher income and middle age are risk factors for obesity among Sri Lankans. These socio-
economic factors associated with obesity amongst Sri Lankan adults are in contrast to risk
factors from developed countries, where less educated, economically deprived and people living
in rural area are more obese [3]. Hence, there could be unique socio-economic factors driving
the obesity epidemic in Sri Lanka.
It is well documented that being overweight and obese are associated with many negative
medical, psychological, social and economic consequences. Health promotion efforts aimed at
overweight and obesity prevention often proceed with the assumption that most individuals
prefer to be thin, and that the initial step in motivating individuals who are overweight to lose
Chapter 8: Manuscript 8 171
weight is to raise awareness of their present weight status and associated health risks [4]. This
approach may be fitting for Western populations that value thinness in women and lean muscular
physiques in men, and highly health literate societies that recognize that abdominal obesity is a
risk factor for many deleterious metabolic consequences such as diabetes. However, this
assumption may not be suitable in Sri Lanka where traditionally abdominal obesity has been
considered a sign of wealth and status. This feature is commonplace in many non-western
cultures which traditionally recognize that a large body size, especially abdominal obesity in
either males or females is a sign of prosperity, wealth and health [5]. That culture influences
weight perception preference has been the rationale for many studies researching the association
between weight perception and obesity among different ethnic groups. Many of these studies
have either focused on minority immigrant populations in affluent countries [6] or primarily
adolescent age groups [7]. Sri Lanka is a country in nutritional transition with epidemic levels of
obesity mainly in urban areas and considerable under-nutrition and nutritional deficiencies also
commonplace [8]. Although there is an increased interest in the prevention of obesity and
associated non-communicable diseases by health authorities, professional associations and the
mass media, there are no national level data on body weight perception and weight loss practices
among Sri Lankan adults.
The success of a public health intervention is dependent upon the people’s awareness of the
health issue and their motivation to change. Self-perception of body weight is a strong
determinant of nutritional habits and weight management [6]. A skewed perception of body
weight may be a barrier to successful weight loss [9] and healthy weight management goals
should be set taking into consideration an individual’s weight perception [10]. The purpose of
the present study was to assess the association between self-perception of body weight and WC
172 Chapter 8: Manuscript 8
with BMI and WC cut-offs among Sri Lankan adults. In addition, we report the knowledge of
their body weight, concept about the BMI and weight loss approaches among Sri Lankan adults.
MATERIAL AND METHODS
Study population and sampling
Data were collected from a subset (n=600) of a previously conducted nationally representative
study, the Sri Lankan Diabetes Cardiovascular Study (SLDCS) using a multi-stage, stratified,
random sampling procedure during January to March 2011. The details of sampling of the
SLDCS are described elsewhere [11]. Data relevant to the present study were obtained in
community settings and included demographic, socio-economic, self-reported diabetes mellitus,
anthropometric measurements, body weight and waist circumference perception, and weight loss
practices. This study was approved by the Ethics Review Committee, Faculty of Medicine,
University of Colombo, Sri Lanka.
Anthropometric measurements
Height was measured using a portable Holtain Stadiometer (Chasmors Ltd, London, UK) to the
nearest 0.1 cm. Body weight was measured using a SECA electronic scale (Hamburg, Germany)
to the nearest 0.1 kg. Most of the participants were weighed wearing light clothes and after
fasting. BMI was calculated as body weight (kg) divided by the square of height (m). WC was
measured using a tape to the nearest 0.1 cm at the midpoint between the lower costal border and
the top of the iliac crest, at the end of normal expiration.
Body weight and waist circumference perception
An interviewer-administrated questionnaire was used which included items such as self-reported
height and weight, body weight perception, abdominal obesity perception and details of weight
Chapter 8: Manuscript 8 173
loss practices. Specifically, these questions asked subjects to report their height in feet and
inches or meters (“How tall are you without your shoes on?”) and weight in kilograms or pounds
(“How much do you weigh without your shoes on?”). Self-reported height and weight were
converted to metric units for calculation of ‘Self-reported’ BMI. The weight perception question
asked was “How do you describe your weight?” Choices included: very underweight,
underweight, about the right weight, overweight, and very overweight [6, 10]. However, for
analysis, very underweight and underweight were merged to form one group. Similarly, with
regard to abdominal obesity, the question asked was, “How do you describe your waist
circumference?” answers were; low, about right, and high. In addition, self-reported weight and
height, presence/absence of diabetes mellitus, details of weight loss practices and knowledge of
BMI were also collected.
Statistical analysis
Analysis was undertaken using SPSS version 16 (SPSS Inc., Chicago, IL, USA). Subjects were
classified into four groups according to their ‘Measured’ BMI values as follows: underweight:
<18.5 kg.m-2; normal weight: 18.5-22.9 kg.m-2, overweight: 23.0-25.0 kg.m-2; obese ≥ 25.0
kg.m-2 [12]. Abdominal obesity was defined as a waist circumference >90 cm for males and >80
cm for females [12]. For categorical variables, Pearson's chi-square test was used. Percentages of
responses were reported according to BMI and WC level and respective weight and WC
perception. A multiple logistic regression analysis was carried out with perceived overweight as
the dependent variable and age, ‘Measured’ BMI, ethnicity, gender, and education as
independent variables. All independent variables were simultaneously included in the regression
model regardless of their statistical significance. A similar regression was carried out for
knowledge of BMI. In all analyses a P value < 0.05 was considered statistically significant.

174 Chapter 8: Manuscript 8
RESULTS
Four hundred and ninety adults participated in the study (a response rate of 82%). Table 8.1
shows the socio-demographic characteristics and obesity prevalence of the study population. The
majority of participants were female (n=321, 65.5%) and the mean age was 48.4±15.6 y for
males and 48.1±14.1 y for females. Overall, there was a preponderance of Sinhalese (M: 71.1%;
F: 80.1%), with most residing in rural areas (M: 60.4%; F: 57.6%). In the study population,
10.6% males and 12.8% females had self-reported diabetes mellitus. The prevalence of
overweight and obesity in males was 14.2% and 20.2%, and in females, 20.2% and 35.9%,
respectively. Nearly 45% of females had abdominal obesity; however, in contrast, only 13% of
males had abdominal obesity.
In this sample over half of total population (54.7%) were aware of their own body weight.
However, less than a quarter (24.7%) correctly predicts their weight close to the measured
weight (±2 kg). Similar to body weight, 50.1% population were aware of their height and 32.4%
of subjects reported height close to the measured values (±5 cm) (Table 8.2). Moreover only 57
adults (M=27, F=30) predicted both height (±5 cm) and weight (±2 kg) correctly. Only 94 adults
(19.2%) had knowledge of what is meant by BMI - there was no significant difference between
knowledge levels of males (21.3%) and females (18.1%). Younger age (p<0.001), living in an
urban area (p<0.03) and higher education (p<0.001) was significantly associated with knowledge
of BMI. Weight misperception varied among BMI groups (table 3). According to ‘Measured’
BMI categories, majority of underweight adults perceived themselves correctly as being
‘underweight’. However, subjects who had normal ‘Measured’ BMI values misperceived their
body weight; about one third of these adults perceived themselves as being ‘underweight’ and in
those with normal ‘Measured’ BMI 9.9% males and 11.2% females reported that they are
overweight or very overweight. One third of overweight males and 44.7% females considered

Chapter 8: Manuscript 8 175
themselves as ‘about right weight’, moreover, 4.1% and 7.6% overweight men and women
reported themselves as being ‘underweight’. Over one third of both male and female obese
subjects perceived themselves as ‘about right weight’ or ‘underweight’. Only 3% of obese males
reported themselves as being ‘very overweight’, however in contrast, 17.5% of females who
were obese considered themselves as ‘very overweight’. Table 4 shows the percentage of
abdominally obese adults who reported that they were having ‘low’, ‘about right’ and ‘high’
waist circumference. Nearly 32% of centrally obese men and women perceived that their WC is
about right. Despite having high WC, small percentage of (M: 4.5%; F: 2.1%) adults believed
that they were having a ‘low’ WC. People who perceived overweight or very overweight
(n=154) only 63.6% tried to lose their body weight (n=98), and quarter of adults seek advices
from professionals (n=39). In this population, almost all obtained weight reduction advices from
medical doctors (Doctor: Nutritionist = 38:1).
Table 5 shows the multiple logistic regression models for under perception, correct perception
and over perception of body weight. The Hosmer-Lemeshow goodness-of-fit test was not
significant for all three models. Older age was a significant predictor of under perception of
body weight (OR = 1.02; 95% CI = 1.01 - 1.03). However in contrast correct perception was
significantly associated with younger age (OR = 0.98; 95% CI = 0.97 - 0.99). None of other
variables were significantly associated with both under perception and correct perception.
However for over perception of body weight, there was a significant association with male
gender (OR = 1.85; 95% CI = 1.00 - 3.40). People from ethnic groups other than Sinhalese also
tends to over perceive their body weight (OR = 2.36; 95% CI = 1.25 - 4.45).
DISCUSSION
To the best of our knowledge, this is the first study to measure body weight and WC perception
and weight loss practices in a nationally representative sample of Sri Lankan adults. Most South
Asian countries, particularly in urban populations, have shown evidence of an epidemic of
176 Chapter 8: Manuscript 8
obesity [3, 13, 14]. In addition, unlike their Western counterparts, South Asians suffer from
obesity-associated metabolic complications at very low BMI levels [15]. Accurate body weight
and waist circumference perception, knowledge of BMI and weight loss initiatives are important
indicators of population’s concern and attitudes toward obesity and weight control. This study
provides valuable details regarding body weight and waist circumference perceptions, and
attitudes toward weight loss practices among Sri Lankan adults. The results have practical
implications for future weight management approaches.
In Sri Lanka only less than one quarter of adults could predict their body weight correctly
although most were screened for body weight and weight circumference in SLDCS several years
back. Lack of concern regarding body weight may put such individuals at risk for further weight
gain and associated health consequences [16]. The ability to identify unhealthy weight changes,
knowledge of one’s own weight, measuring body weight frequently and keeping records of body
weight is recognized as essential in the prevention of unhealthy weight gain [17]. BMI is widely
considered an easy tool to identify obesity but less than 20% of Sri Lankan adults surveyed had
knowledge of concept of BMI. Presently, details of BMI have been included in the school
curriculum and pregnancy records, therefore such initiatives may help to improve the knowledge
and understanding of younger generations in this important area. In addition, increased
awareness of obesity in the mass media may have an impact on the urban and educated
population over time.
Findings highlight that weight misperception is highly prevalent among Sri Lankan adults with
over 70% of overweight and 41% of obese males and over 50% overweight females and one
third of obese females not perceiving themselves as overweight. Among US adults, 40% of
overweight and 8% of obese adults considered themselves to be ‘about the right weight’ [18].

Chapter 8: Manuscript 8 177
Similarly, in 2007 53% of the British population had a BMI in the overweight or obese range, of
whom only 75% reported as being overweight, very overweight, or obese [19]. A related study
on a group of adolescent girls in Sri Lanka reported that in those who were overweight, 5.6%
perceived themselves as being underweight, and 11.1% as normal-weight. These values are
lower than our findings, however, in contrast to the present study these investigators used
WHO cut-offs to categorize overweight [20]. It is reported that Sri Lankan adults have an
increased risk for CVD starting from a BMI of 21 kg.m-2 [15]. Thus, it is appropriate to use
lower BMI cut-offs for primary prevention of obesity. Although they are subject to metabolic
complications [15] and have a high body fat percentage [21] at a low BMI, overweight and
obese Sri Lankan adults may not perceive their excess body weight due to several reasons. Sri
Lankans are typically a lean population (3.9% ≥30 kg.m-2) and low obesity perception in the
population is reasonable. Historically, overweight people were wealthy and powerful and in
contrast, lean people were poor manual workers. Many societies still consider overweight as a
sign of wealth and power. Similarly, among a group of South African black women, being
moderately overweight was considered to be acceptable, and was associated with dignity,
respect, health, wealth and strength [23]. In some societies, fat women are considered to be a
sign of well-caring by their husbands [16]. Prevalence of diabetes is extremely common in
urban, middle aged adults, one in every three adults having diabetes in the over 50 years of age
category and a significant portion is undiagnosed [11]. Therefore, low body weight or weight
loss may have a negative social stigma in this society due to weight loss being associated with
undiagnosed diabetes. Similarly, in South Africa, weight loss has a socially negative stigma due
to HIV infection [24].
Two-thirds of centrally obese Sri Lankan adults perceived themselves as having higher WC.
Abdominal obesity misperception being lower than body weight misperception indicates that Sri

178 Chapter 8: Manuscript 8
Lanka adults are more aware of their waist circumference compared to body weight. Changes in
waist circumference can be easily identified by clothing; however, body weight may not be as
evident due the need to measure. Sri Lankan males have a higher prevalence of weight
misperception than females, most notably with a higher proportion of overweight and obese
males incorrectly under assessing their weight category. In general, females are more weight
conscious and attempt to identify weight control strategies [25]. Although there is reasonable
agreement between BMI estimated from reported weight and height and BMI calculated from
measured variables in this population, there is limited practical value of self-reported weight and
height for clinical practices. Rowland reported that obese people underestimate their weight and
overestimate height [26]. BMI calculated from self-reported height and weight had greater
association with weight perceptions than did BMI calculated from measured height and weight.
Among adolescents, self-reporting of height and weight is probably influenced to some degree
by body weight perception [6]. This is due to underestimating their weight and overestimating
their height compared with measured values. Still when weight perceptions were compared with
BMI calculated from self-reported values, a significant number of adults misperceived their
weight status.
It is reported that obese individuals with body size misperception have a lower awareness of
obesity associated health risk [9]. However, a large proportion of adults who are overweight or
obese fail to perceive them as such and, consequently, are unlikely to look for weight reduction
practices such as dieting and exercise to lose weight. Surprisingly, among those who tried to lose
body weight, less than half seek professional advice. It is evident that weight management
requires professional support, preferably from a multi-disciplinary team [27]. Limited facilities
for nutrition counselling and weight management in Sri Lanka are a hindrance to successfully
combat the obesity epidemic. Data on the socio-economic association and body weight
Chapter 8: Manuscript 8 179
perception is limited. Young people are more likely to perceive correct body weight in contrast
to older people. This indicates that younger generations are much more aware of their body
weight and shape than older generations in Sri Lanka.
Future perspectives
There is an urgent public health necessity to initiate health awareness programs to identify
healthy body weight, negative health consequences of excess body weight, and practical lifestyle
strategies for the general public. As the causes of weight misperception could be complex, public
health interventions should be a multifaceted [9]. There should be encouragement for people to
measure their own body weight, WC and maintain BMI records in every hospital or general
practitioner visit. Furthermore, identified cases should be referred to necessary health care
centres for early treatment. It is widely reported that patients cite physicians as the most credible
source of nutrition information and ahead of nutritionists [28]. In Sri Lanka, most obese adults
seek weight reduction advice from doctors therefore, medical professional associations and
medical schools must initiate training programs to improve the competence of nutritional and
lifestyle knowledge and skills of doctors. The General Medical Council (UK) recognized that all
medical graduates should obtain satisfactory knowledge on the role of lifestyle and human
nutrition promoting health and prevent disease and human nutrition should be treated as a
discrete medical discipline for clinicians to specialize [29]. Sri Lanka needs a professional
organization to handle this obesity epidemic and more studies should be conducted to obtain a
better understanding of erroneous perception of body weight and poor weight loss practices in
this population. It is widely reported that distorted weight perception and body image among
adolescents is negatively associated with unhealthy eating habits and disordered eating
behaviour [6,30]. Inability of adults to self-perceive body weight may also be a contributing
factor for misjudgement of their children’s body weight. Therefore, future studies are needed to
obtain data on weight perception of children and adolescents.
180 Chapter 8: Manuscript 8
Limitations
Data collection was at community settings during the day therefore a large proportion of eligible
male participants were not present due to occupational commitments. On the other hand, females
enthusiastically participated in this study. Weight cut-offs of ±2 kg and height cut-offs of 5 cm
are used arbitrarily. We could not obtain accurate details of the economic status or household
income of participants which could have an association with weight perception. Similarly,
metabolic parameters were not measured, abnormal body weight and WC could have been
associated with adverse metabolic risk. Moreover, details of perception of body shape/image and
details of weight loss strategies were not obtained in this study. As this was a cross-sectional
study, causality could not be inferred between perceived weight, actual (estimated) BMI, and
weight loss practices. Future studies are needed to identify whether correct perception of own
body weight has a positive impact on weight reduction behaviour and healthy weight
maintenance in this population.
CONCLUSION
Body weight misperception was common among underweight, healthy weight, overweight, and
obese adults in Sri Lanka. Over 2/3 of overweight and 1/3 of obese Sri Lankan adults believe
they are in the right weight or underweight category. Minorities were more likely to over-
estimate their body weight, as well as males and people with lower educational levels. As
perception of overweight or obesity is an important determinant of lifestyle habits and weight
reduction, many overweight and obese Sri Lankans are unlikely to engage in weight control
practices. A minor percentage of Sri Lankans have an accurate awareness of their own body
weight and height, and knowledge of the BMI concept was also poor. Surprisingly, despite some
who recognized themselves as being overweight did not seek advice from health care providers.
Increasing awareness of the medical definition of overweight, obesity and abdominal obesity and

Chapter 8: Manuscript 8 181
understanding of the importance of body composition amongst medical practitioners may make a
significant contribution to healthier lifestyles of Sri Lankans.
182 Chapter 8: Manuscript 8
REFERENCES
1. WHO. Statistics. Country Health Profile 2008 [cited 2010 2 Nov]; Available from:
http://www.who.int/countries/en/.
2. Illangasekera, U., S. Rambodagalla, and S. Tennakoon, Temporal trends in the
prevalence of diabetes mellitus in a rural community in Sri Lanka. The Journal of the
Royal Society for the Promotion of Health, 2004. 124(2): p. 92.
3. Katulanda, P., et al., Prevalence of overweight and obesity in Sri Lankan adults. Obes
Rev, 2010.
4. Wammes, B., et al., The impact of a national mass media campaign in The Netherlands
on the prevention of weight gain. Public Health Nutrition, 2005. 8(8): p. 1250-1257.
5. Becker, A.E., S.E. Gilman, and R.A. Burwell, Changes in Prevalence of Overweight and
in Body Image among Fijian Women between 1989 and 1998* &ast. Obesity, 2005.
13(1): p. 110-117.
6. Nicolaou, M., et al., Body size preference and body weight perception among two
migrant groups of non-Western origin. Public Health Nutrition, 2008. 11(12): p. 1332-
1341.
7. Brener, N.D., et al., The association between weight perception and BMI among high
school students. Obesity, 2004. 12(11): p. 1866-1874.
8. Meera Shekar, A.S., Lidan Du, Malnutrition in Sri Lanka: Scale, Scope, Causes, and
Potential Response, W. Bank, Editor. 2007, Human Development Unit, South Asia
Region.
9. Powell, T.M., et al., Body Size Misperception: A Novel Determinant in the Obesity
Epidemic. Arch Intern Med, 2010. 170(18): p. 1695-1697.
10. Rahman, M. and A.B. Berenson, Self-Perception of Weight and Its Association With
Weight-Related Behaviors in Young, Reproductive-Aged Women. Obstetrics &
Gynecology, 2010. 116(6): p. 1274-1280 10.1097/AOG.0b013e3181fdfc47.
11. Katulanda, P., et al., Prevalence and projections of diabetes and pre-diabetes in adults in
Sri Lanka—Sri Lanka Diabetes, Cardiovascular Study (SLDCS). Diabetic Medicine,
2008. 25(9): p. 1062-1069.
12. WHO, I.a.I., The Asia-Pacific Perspectives: Redefining Obesity and its treatment. 2000.
13. Wang, Y., et al., Is obesity becoming a public health problem in India? Examine the shift
from under- to overnutrition problems over time. Obesity Reviews: An Official Journal
Of The International Association For The Study Of Obesity, 2009. 10(4): p. 456-474.

Chapter 8: Manuscript 8 183
14. Jafar, T.H., N. Chaturvedi, and G. Pappas, Prevalence of overweight and obesity and
their association with hypertension and diabetes mellitus in an Indo-Asian population.
CMAJ: Canadian Medical Association Journal = Journal De L'association Medicale
Canadienne, 2006. 175(9): p. 1071-1077.
15. Katulanda, P., et al., Derivation of anthropometric cut-off levels to define CVD risk in Sri
Lankan adults. Br J Nutr, 2011. 105(7): p. 1084-90.
16. Faber, M. and H.S. Kruger, Dietary intake, perceptions regarding body weight, and
attitudes toward weight control of normal weight, overweight, and obese Black females
in a rural village in South Africa. Ethnicity & disease, 2005. 15(2): p. 238-45.
17. Linde, J., et al., Self-weighing in weight gain prevention and weight loss trials. Annals of
Behavioral Medicine, 2005. 30(3): p. 210-216.
18. Dorsey, R.R., M.S. Eberhardt, and C.L. Ogden, Racial/Ethnic Differences in Weight
Perception. Obesity, 2009. 17(4): p. 790-795.
19. Johnson, F., et al., Changing perceptions of weight in Great Britain: comparison of two
population surveys. BMJ, 2008. 337.
20. de Lanerolle-Dias M, d.S.A., Lanerolle P, Atukorala S., BMI & body weight perception:
the need to create awareness. Annals of Nutrition and Metabolism., 2009. 55: p. 220.
21. Deurenberg-Yap, M., et al., The paradox of low body mass index and high body fat
percentage among Chinese, Malays and Indians in Singapore. International journal of
obesity and related metabolic disorders : journal of the International Association for the
Study of Obesity, 2000. 24(8): p. 1011-7.
22. Wijewardene, K., et al., Prevalence of hypertension, diabetes and obesity: baseline
findings of a population based survey in four provinces in Sri Lanka. The Ceylon
medical journal, 2005. 50(2): p. 62-70.
23. Puoane T, F.J., Shapiro M, Rosling L, Tshaka NC, Oelofse A, ‘Big is beautiful’ – an
exploration of urban black women in South Africa. South African Journal of Clinical
Nutrition, 2005. 18(1): p. 6-15.
24. Hurley E, C.A., Giddy J, Knight SE, Loots E, Esterhuizen TM, Weight evolution and
perceptions of adults living with HIV following initiation of antiretroviral therapy in a
South African urban setting. S Afr Med J 2011. 101: p. 645-650.
25. Tiggemann, M. and E.D. Rothblum, Gender differences in social consequences of
perceived overweight in the United States and Australia. Sex Roles, 1988. 18(1): p. 75-
86.

184 Chapter 8: Manuscript 8
26. Rowland, M., Self-reported weight and height. The American Journal Of Clinical
Nutrition, 1990. 52(6): p. 1125-1133.
27. Arthur, F., A Multidisciplinary Approach to Obesity Management: The Physician's Role
and Team Care Alternatives. Journal of the American Dietetic Association, 1998. 98(10,
Supplement): p. S44-S48.
28. Levin, A., Nutrition and Policy. 5: Who Should Teach Patients about Nutrition? Annals
of Internal Medicine, 1999. 131(4): p. 317-318.
29. Lean, M. and M. Wiseman, Malnutrition in hospitals. BMJ, 2008. 336(7639): p. 290-
290.
30. Al-Sendi, A.M., P. Shetty, and A.O. Musaiger, Body weight perception among Bahraini
adolescents. Child: Care, Health and Development, 2004. 30(4): p. 369-376.

Chapter 8: Manuscript 8 185
Table 8-1: Socio-demographic characteristics, BMI and abdominal obesity categories. Variables Males (169) Female (321) Age (y) (mean±s.d.) 48.4±15.6 48.1±14.1 Area of Residence
• Urban • Rural • Estate
27.8 (47) 60.4 (102) 11.8 (20)
36.2 (116) 57.6 (185) 6.2 (20)
Ethnicity • Sinhalese • Sri Lankan Tamil • Indian Tamil • Muslim
71.1 (120) 11.8 (20) 12.4 (21) 4.7 (8)
80.1(257) 7.2(23) 5.5(18) 7.2(23)
Education level • No Schooling • Up to 5 years • Up to 11 years • Up to 13 years • Graduate
6.5 (11) 6.5 (21) 27.2 (46) 25.2(81) 34.9(59) 40.6(130) 27.2(46) 22.7(73)
4.2(7) 5.0(16)
Prevalence of Diabetes Mellitus 10.6 (18) 12.8 (41) Underweight (BMI<18.5 kg.m-2) 18.3 (31) 13.4 (43) Normal weight (18.5≥ BMI <22.9 kg.m-2) 47.4 (80) 30.6 (98) Overweight (23.0≥ BMI <24.9 kg.m-2) 14.2 (24) 20.2 (65) Obesity (BMI >25.0 kg.m-2) 20.1 (34) 35.9 (115) Abdominal obesity* 13.0 (22) 44.9 (144) *Abdominal obesity (M: 90 cm>WC ; F: 80 cm>WC)
Table 8-2: Awareness of body weight and height Number of Participants (%)
All Male Female
Body Weight
Awareness
Prediction of weight ± 2 kg
268 (54.7%)
121 (24.7%)
104 (61.5%)
47 (27.8%)
164 (51.1%)
74 (23.1%)
Height
Awareness
Prediction of height ± 5 cm
245 (49.9%)
159 (32.4%)
116 (68.6%)
80 (47.3%)
129 (40.2%)
79 (24.6%)
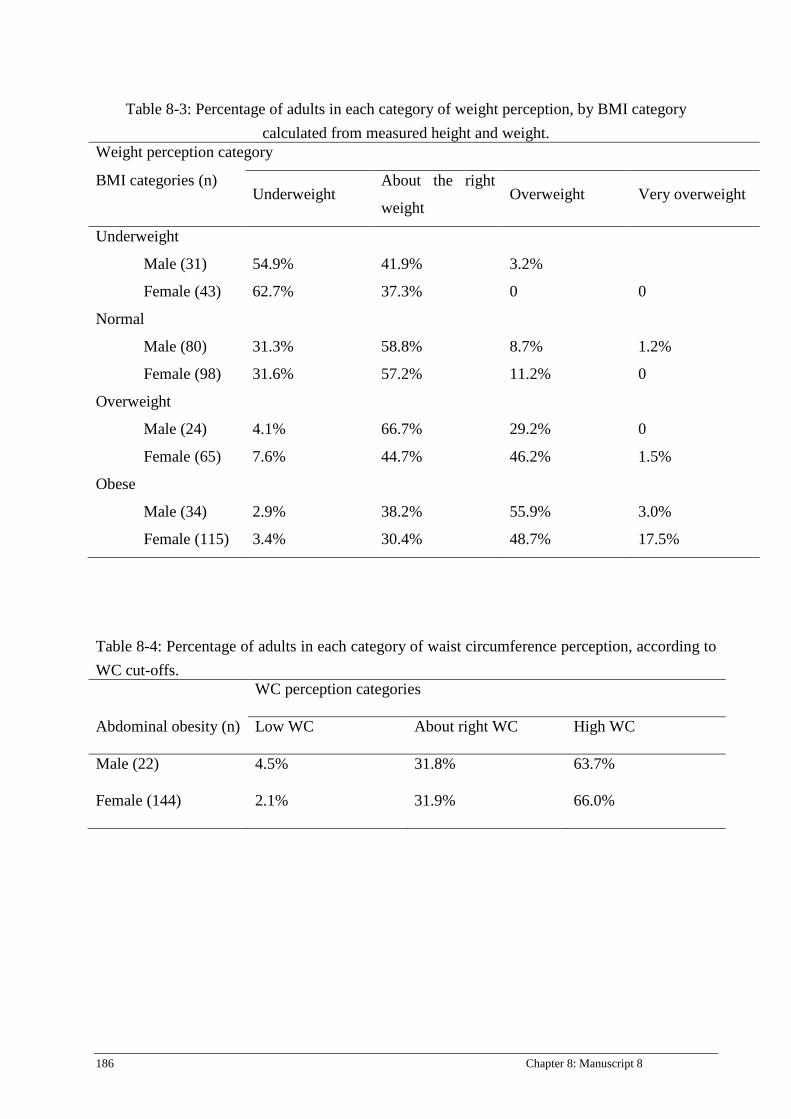
186 Chapter 8: Manuscript 8
Table 8-3: Percentage of adults in each category of weight perception, by BMI category calculated from measured height and weight.
Weight perception category
BMI categories (n) Underweight
About the right
weight Overweight Very overweight
Underweight
Male (31)
Female (43)
54.9%
62.7%
41.9%
37.3%
3.2%
0
0
Normal
Male (80)
Female (98)
31.3%
31.6%
58.8%
57.2%
8.7%
11.2%
1.2%
0
Overweight
Male (24)
Female (65)
4.1%
7.6%
66.7%
44.7%
29.2%
46.2%
0
1.5%
Obese
Male (34)
Female (115)
2.9%
3.4%
38.2%
30.4%
55.9%
48.7%
3.0%
17.5%
Table 8-4: Percentage of adults in each category of waist circumference perception, according to WC cut-offs. WC perception categories
Abdominal obesity (n) Low WC About right WC High WC
Male (22)
Female (144)
4.5%
2.1%
31.8%
31.9%
63.7%
66.0%

Chapter 8: Manuscript 8 187
Table 8-5: Logistic regression model of under perception, correct perception and over perception of body weight.
Variables
Under perception Correct perception Over perception OR(95%CI) P value OR(95%CI) P
value OR(95%CI) P value
Age (years)
1.02 (1.01-1.03) 0.003 0.98(0.97 – 0.99) 0.002 1.00 (0.98 – 1.02)
0.98
Female (Ref.)
Male
1
0.77(0.53 – 1.12)
0.18
1
1.04(0.71 – 1.52)
0.85
1
1.85(1.00 – 3.40)
1
0.048
Urban(Ref.)
Rural
1
0.80(0.55 – 1.17)
0.25
1
1.03(0.70 – 1.51)
0.9
1
1.89(0.91 – 3.90)
0.086
Graduate(Ref.)
No Schooling
Up to 5 years
Upto O/L
Up to A/L
1
1.21(0.41 – 3.60)
2.29(0.92 – 5.68)
1.95(0.80 – 4.73)
0.95(0.38 – 2.36)
0.73
0.075
0.14
0.90
1
0.81(0.27 – 2.47)
0.75(0.30 – 1.88)
0.85(0.35 – 2.06)
2.00(0.80 – 5.00)
0.72
0.54
0.72
1.35
1
1.00(0.27 – 3.69)
0.31(0.09 – 1.00)
0.36(0.12 – 1.09)
0.22(0.06 – 0.79)
0.99
0.05
0.07
0.02
Sinhala (Ref.)
Others
1
1.02(0.67 – 1.56)
0.92
1
0.68(0.45 – 1.06)
0.09
1
2.36(1.25 – 4.45)
0.008
OR: odds ratio

188 Chapter 9: Manuscript 9
Chapter 9: Manuscript 9
Contribution of co-authors for thesis by published paper The authors listed below have certified that
1. They meet the criteria for authorship in that they have participated in the conception, execution, or interpretation, of at least that part of the publication in their field o expertise:
2. They take public responsibility for their part of the publication, except for the responsible author who accepts overall responsibility for the publication;
3. There are no other authors of the publication according to these criteria; 4. Potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or
publisher of journals or other publications, and (c) the head of the responsible academic unit, and 5. They agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
In the case of this chapter Paper: Validation of a Food Frequency Questionnaire to assess nutritional intake among
Sri Lankan adults.
Contributor Statement of contribution Ranil Jayawardena Study design, data collection, data analysis
and drafted the manuscript Nuala Byrne Study design, data interpretation and revision
of the draft and approved the final manuscript.
Mario Soares Study design, data interpretation and revision of the draft and approved the final manuscript.
Prasad Katulanda Study design, data interpretation and revision of the draft and approved the final manuscript.
Andrew Hills Study design, data interpretation and revision of the draft and approved the final manuscript.
Principal supervisor confirmation I have sighted email or other correspondence from all co-authors confirming their certifying authorship.
Nuala Byrne 18/04/2013
Name signature Date
Chapter 9: Manuscript 9 189
TITLE PAGE
Ranil Jayawardena1,2*, Nuala M. Byrne1, Mario J. Soares3, Prasad Katulanda2, Andrew P. Hills4
1Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of
Technology, Brisbane, Queensland, Australia.
2Diabetes Research Unit, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka.
3Curtin Health Innovation Research Institute, School of Public Health, Faculty of Health
Sciences, Curtin University, Perth, WA, Australia.
4Mater Mothers’ Hospital, Mater Medical Research Institute and Griffith Health Institute,
Griffith University, Brisbane, Queensland, Australia.
Citation
R Jayawardena, NM Byrne, MJ Soares, P Katulanda, AP Hills. Validation of Food Frequency
Questionnaire for Sri Lankan adults. Nutrition Journal (Under review): MS ID:
1813393429968846.
190 Chapter 9: Manuscript 9
ABSTRACT
Background
Sri Lanka is undergoing a nutritional transition and diet-related chronic diseases are emerging as
important health problems. Currently, no validated food frequency questionnaire (FFQ) exists to
measure the habitual dietary intake of Sri Lankan adults. The purpose of the study was to assess
the validity of a semi-quantitative FFQ against a 7-day weighed-intake dietary record (7DWR)
among Sri Lankan adults.
Methods
One hundred apparently healthy adults were randomly recruited from a community sample and
administrated the FFQ. All subjects also completed a 7DWFR. Paired sample t tests, Pearson's
correlation coefficients and Bland-Altman analysis were conducted to determine the validity and
the level of agreement between the two measures of food intake.
Results
Seventy-seven subjects completed the FFQ and 7-day WDR. Estimated mean energy intake (SD)
from FFQ (1794 ±398 kcal) and 7DWR (1698 ± 333 kcal, P < 0.001) was significantly different
due to a significant overestimation of carbohydrate (~10 g/d, P<0.05) and to some extent fat (~5
g/d, P<0.05). Significant positive correlations were found between the FFQ and 7DWR for
energy (r = 0.39), carbohydrate (r = 0.47), protein (r = 0.26), fat (r =0.17) and dietary fiber (r =
0.32). Bland-Altman analysis indicated fairly good agreement between methods with no
relationship between bias and average intake of each nutrient examined. Moreover, the FFQ
could correctly classify ~50% of subjects into their respective tertiles of macro and micro
nutrient intakes.
Conclusions
The developed FFQ appears to be an acceptable tool for assessing nutrient intake of Sri Lankans
adults and will assist proper categorization of individuals by tertiles of dietary exposure.
Chapter 9: Manuscript 9 191
INTRODUCTION
Sri Lanka is a low-middle-income country (LMIC) undergoing a nutritional transition. Although
under-nutrition and anemia are a cause for concern, a significant proportion of adults are
suffering from diet-related non-communicable diseases (NCDs). Specifically, a quarter of Sri
Lankan adults are suffering from the metabolic syndrome [1], the prevalence of obesity (BMI
>25 kg.m-2) is 20% among men and 25% among women [2], and nearly 11% adults have type 2
diabetes mellitus [3]. Not surprisingly, a recent priority area for the Sri Lankan health authorities
is to combat diet-related NCDs. However due to the absence of a valid nutrition assessment tool
[3], there is limited national information on eating patterns or dietary exposure to juxtapose
against national level prevalence data on diabetes and cardiovascular disease.
FFQs are designed to capture food habits over an extended period of time and so they are a
commonly accepted tool for assessing habitual dietary intake in epidemiological studies of diet
and chronic diseases [4]. In comparison to other dietary intake assessment methods, FFQs are
relatively inexpensive, easy for the volunteer to understand, and quick to administer [5]. FFQs
are used in both developed and developing countries to relate fruit and vegetable intake to risk of
cardiovascular disease [6], to study links between cancer and nutrition in several countries [7], as
part of national nutrition surveys [8], and to link maternal nutrition to pregnancy morbidity and
birth outcomes of South Indians [9].
Population-specific FFQs are important to assess the dietary intake of a particular group of
people. Sri Lanka has a multiethnic population. The relative validity of FFQs is usually assessed
by comparing their findings with a reference method and the 7-day weighed-intake dietary
record (7DWR) method is widely considered as the ‘gold standard’ approach to assess habitual

192 Chapter 9: Manuscript 9
diet [10]. The aim of this study was to assess the validity of a newly developed FFQ to estimate
nutrient intake compared to 7DWR among Sri Lankan adults.
METHODS
Background
In the Sri Lanka Diabetes and Cardiovascular Study (SLDCS) a multi-stage random-cluster
sampling method was used to select a nationally representative sample of non-institutionalized
adults aged ≥18 years [3]. A sub-sample of the SLDCS was used to develop a representative
FFQ for Sri Lankan adults. Details of the study design have been published elsewhere [11].
Ethical approval for the study was obtained from the Ethical Review Committee, University of
Colombo, Sri Lanka and written informed consent was obtained from each participant before
data collection.
Study sample
A total of 100 adults were randomly selected to participate in the validation study from the
SLDCS and stratified based on ethnicity and area of residence. Participants adhering to a
prescribed therapeutic diet or on weight reduction diet were excluded from the study. Of the 100
adults initially selected, 18 individuals failed to complete the 7DWR. A further five subjects
were excluded before statistical analyses were undertaken as their dietary records were unlikely
to represent habitual intake based on misreporting.
Dietary assessment
Food frequency questionnaire
The FFQ was developed from a country representative sample, the details of which have been
published previously [12]. Briefly, the FFQ contains colour photographs of 3 different portion
sizes of four commonly consumed foods and a list of food items (n=90) with their portion sizes
and frequencies. Food items were categorized to eight food groups namely 1) cereals; 2)
Chapter 9: Manuscript 9 193
vegetables; 3) pulses; 4) meat; 5) fruits; 6) drinks; 7) miscellaneous; and 8) alcohol. The FFQ
was interviewer-administrated in the local language (Sinhalese and Tamil) by two investigators.
The length of interview ranged from 15-20 minutes during which participants were asked to
recall the usual portion sizes and intake of foods comprising the FFQ over the past month.
Subjects were then instructed to complete a seven-day weighed food record.
Seven-day weighed intake
Subjects were requested to keep a weighed record of all food items and beverages consumed
both in and out of the home, over a period of seven consecutive days. Investigators provided
verbal instructions and demonstration on site and telephone instructions were also provided for
any specific queries. All subjects received a calibrated kitchen scale (Tanita KD-407) and a
recording diary, the ‘Home Record’ diary, to weigh and record home-cooked foods. A smaller
pocket sized ‘Eating and Drinking Away From Home’ diary (the ‘Eating Out’ diary) was also
provided for recording food intake when foods could not be weighed. Generally this was meant
to capture foods eaten away from home.
Analysis
Energy and nutrient intakes were calculated using NutriSurvey 2007 (EBISpro, Germany)
nutrient analysis software which was modified for Sri Lankan food items and recipes.
For statistical analysis, means and SDs of energy, macronutrient and micronutrient intakes were
determined for the FFQ and 7DWR methods. Differences and ratios between mean values
obtained with the FFQ and with the reference methods were calculated. Paired t test was used to
determine significant differences between means and correlation between intake amounts
obtained by the two methods evaluated by Pearson correlation analysis. Furthermore, the
agreement between the FFQ and the 7DWR was also examined by evaluating the proportion of
194 Chapter 9: Manuscript 9
participants who fell within the same tertile of the nutrient distribution for both the methods. To
assess agreement between the FFQ and reference methods, and to detect any bias with the test
method relative to the reference method, differences between the 2 respective methods were
plotted against the means, as suggested by Bland and Altman [13]. Minitab version 15.0 was
used for statistical analysis and P value < 0.05 was considered statistically significant.
RESULTS
Subjects were selected from different ethnic backgrounds and area of Sri Lanka. A total of 77
participants completed both 7DWR and FFQ accurately. Sixty-five of this group were women
and the majority were Sinhalese (n=69). Thirty-eight participants were from rural area, 31 from
urban areas and eight from estates.
Mean (SD) energy intake from 7DWR was 1697.9 (333.3) kcal/d and corresponding values from
FFQ was 1794.1 (397.6) kcal/d. Significantly higher energy values were recorded from FFQ
than the reference method (p<0.05). In both methods, over two-thirds of energy was derived
from carbohydrates, and fat provided 19.8% and 22.1% of energy from 7DWR and FFQ
respectively. Only 12.3% of energy was derived from protein in the 7DWR and the
corresponding value for FFQ was 11.1% (Table 9.1).
FFQ and 7DWR were significantly correlated for energy intake (r= 0.39; p<0.001), percentage
of calories from fat (r=0.34, P =0.002), protein (r=0.52, p<0.001) and carbohydrates (0.40,
p<0.001) dietary fiber (r=0.32, p=0.005), PUFA (r=0.37, <0.001), while dietary cholesterol just
reached significance (r= 0.23, p=0.05). Five out of eight vitamins showed significant correlation
and folic acid had the highest r value (r=0.48; p<0.001), whereas among six minerals, sodium
(r=0.17) and zinc (r=0.12) did not show significant correlation. Cross-tabulations of nutrient
intake assessed by the FFQ and 7DWR showed that FFQ was able to correctly classify most

Chapter 9: Manuscript 9 195
macro and micro nutrients into lowest and highest quintile. Notable exceptions were fat intake,
vitamin B1, B2, C, sodium, calcium and zinc (Table 9.2).
The Bland and Altman plot (Figure 9.1a), showing energy differences between 7DWR and FFQ
for each subject, did not indicate that the difference tended to increase as absolute energy intake
increased. Although FFQ reported higher mean energy values compared to reference method, the
spread around the mean reflected the variation is consistent across all levels of intake.
Carbohydrates, protein and fat also shared the same trends as energy (Figure 9.1). Overall, a few
subjects fell outside the limit of agreements (LOA). For all measurements the mean differences
(bias) were not associated with the average of the two methods. However, LOA were wide
(greater than ±2 SDs of the 7DWR) indicating poorer agreement between FFQ and 7DWR
across the range of intakes. On the other hand, although fat and protein showed low correlation,
the LOA for fat and protein were well within ±2 SDs of the 7DWR.
DISCUSSION
The main objective of this study was to examine the validity of our recently developed FFQ to
guage its relative validity and hence application at the next national level NCD survey. The
7DWR is considered the ‘gold standard’ but contributes considerable subject burden. Work
commitments either at office or working in the fields, places a distinct burden on the weighing of
all food eaten during a particular week. Not surprisingly, most men refused to participate or
discontinued the study. Hence our validation sample was mostly comprised of women. The
National Diet and Nutrition Survey in the UK received less than a 50% response rate for the
7DWR [10], a value much lower than this study.
A small survey suggested that a very high intake of starch foods among Sri Lankan adults may
be related to the epidemic of diabetes in the country [11]. Nearly 70 percent of calories were
196 Chapter 9: Manuscript 9
obtained from starch products in that study. Our FFQ showed a reasonable agreement in ranking
of subjects in their intake of energy, carbohydrate, protein and some micronutrients compared to
the reference method. This was evident in both the correlation analysis and Bland-Altman
analysis.
The Bland-Altman approach is considered the preferred statistical analysis to assess the
agreement between two methods [5]. Our FFQ did not show any systematic drift in bias between
the FFQ and 7DWR for macronutrients. Most importantly, it showed a level of agreement
between nutrients that is acceptable for comparison of such methods.
Previous studies using FFQs have reported correlation coefficients of 0.54-0.86 for nutrients
compared to dietary recalls [7]. A large epidemiological study to assess the risk factors of cancer
reported r values of 0.2 for energy between 12-day weight diet record and FFQ [14]. While an
FFQ administered during trimesters of pregnancy showed that correlation coefficients ranged
from 0.11 for vitamin A to 0.44 for protein intake against multiple 24-hour recalls [15]. Overall,
our FFQ showed a satisfactory range of correlations for energy and macronutrients (Table 9.1)
allowing some confidence in its use for studies on diet related NCDs. In addition, significant
correlation for several micronutrients such as iron, calcium and vitamin D indicate its usefulness
in studies on iron deficiency and osteoporosis in Sri Lanka.
The study of diet and chronic disease requires proper classification of subjects to relate the
exposure variable to its putative disease or outcome. Our analysis in Table 9.2 suggests that the
percentage of subjects correctly classified by tertile categories ranged from good to excellent for
many nutrients. A surprising outcome was the poor categorization of dietary fat intake despite no
significant difference in %fat intake between methods and a significant correlation between the
two intakes (Table 9.1). Sodium intake from the FFQ also suffered from a similar poor
classification. It is possible that from a Sri Lankan context both these dietary components have
much day-to-day variability within each person. While coconut oil is the main edible oil, the

Chapter 9: Manuscript 9 197
FFQ may have missed hidden fat and sodium sources. For example, use of coconut milk in
curries is common, but the precise amount used in home recipes may vary. Perhaps additional
probing questions on fat products and sources need to be included to better capture fat intake.
On the other hand, the FFQ is meant to capture usual intake over a prolonged period and so
minimizes day to day variations. Our 7DWFR captured one random week’s intake with a
limitation that food eaten out of home was estimated and recorded, not weighed. The latter
aspect of the method would have also contributed to the poorer categorization of subjects for fat
and sodium. In the present group food eaten away from home included food purchased from
shops or on the streets, where potentially intakes of fat and sodium would have varied from the
recipes available in the database. Objective sodium intake measurement such as 24-hour urinary
analysis can be used for accurate sodium analysis.
Another limitation in this study is the lack of information on the reproducibility of the FFQ. As
the FFQ captures long-term intake, a judgment of what time interval is appropriate becomes
difficult. However, we readministered the same FFQ (FFQ2) 7-10 days after the first FFQ and
found significant correlations between the two administrations (Table: 9.3; online
supplementary) but accept that to some extent, respondents may recall their previous responses
due to this short time interval [5]. Poor male representation (non-responders) in the study sample
may limit the acceptability of its usage among men. Different ethnic groups may have varied
cooking and dietary patterns, however smaller sample sizes may limit the sub-analysis for each
ethnic groups.
CONCLUSION
The validation of this FFQ was the first attempt to create a practical dietary intake instrument
targeted at a national level nutrition and health survey. This population-specific FFQ provides a
reasonable measure of energy and major nutrients intake in Sri Lankan adults. With some

198 Chapter 9: Manuscript 9
improvements, this FFQ could be a useful tool to examine the role of diet in the etiology of
chronic diseases in this population.
Chapter 9: Manuscript 9 199
REFERENCE LIST
1. Katulanda P, Ranasinghe P, Jayawardena R, Sheriff R, Matthews D: Metabolic
syndrome among Sri Lankan adults: prevalence, patterns and correlates.
Diabetology & Metabolic Syndrome 2012, 4:24.
2. Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Hills AP: The Obesity Epidemic
in Sri Lanka Revisited. Asia Pac J Public Health 2012.
3. Katulanda P, Constantine GR, Mahesh JG, Sheriff R, Seneviratne RD, Wijeratne S,
Wijesuriya M, McCarthy MI, Adler AI, Matthews DR: Prevalence and projections of
diabetes and pre-diabetes in adults in Sri Lanka--Sri Lanka Diabetes,
Cardiovascular Study (SLDCS). Diabet Med 2008, 25:1062-1069.
4. Willett WC, Sampson L, Browne ML, Stampfer MJ, Rosner B, Hennekens CH, Speizer
FE: the use of a self-administered questionnaire to assess diet four years in the past.
American Journal of Epidemiology 1988, 127:188-199.
5. Cade J, Thompson R, Burley V, Warm D: Development, validation and utilisation of
food-frequency questionnaires – a review. Public Health Nutrition 2002, 5:567-587.
6. Bazzano LA, He J, Ogden LG, Loria CM, Vupputuri S, Myers L, Whelton PK: Fruit
and vegetable intake and risk of cardiovascular disease in US adults: the first
National Health and Nutrition Examination Survey Epidemiologic Follow-up Study.
The American Journal Of Clinical Nutrition 2002, 76:93-99.
7. Kroke A, Klipstein-Grobusch K, Voss S, Möseneder J, Thielecke F, Noack R, Boeing H:
Validation of a self-administered food-frequency questionnaire administered in the
European Prospective Investigation into Cancer and Nutrition (EPIC) Study:
comparison of energy, protein, and macronutrient intakes estimated with the
doubly labeled water, urinary nitrogen, and repeated 24-h dietary recall methods.
The American Journal Of Clinical Nutrition 1999, 70:439-447.
8. Mishra G BK, Arbuckle J, Crawford D. : Dietary patterns of Australian adults and
their association with socioeconomic status: results from the 1995 National
Nutrition Survey. European Journal of Clinical Nutrition 2002, 56:687-693.
9. Dwarkanath P, Soares MJ, Thomas T, Vaz M, Swaminathan S, Kurpad AV: Food
Frequency Questionnaire Is a Valid Tool for the Assessment of Dietary Habits of
South Indian Pregnant Women. Asia-Pacific Journal of Public Health 2012.
200 Chapter 9: Manuscript 9
10. Swan G: Findings from the latest National Diet and Nutrition Survey. Proc Nutr Soc
2004, 63:505-512.
11. Jayawardena R, Byrne N, Soares M, Katulanda P, Hills A: Consumption of Sri Lankan
adults: an appraisal of serving characteristics. Public Health Nutr 2012, First View:1
- 6.
12. Jayawardena R, Swaminathan S, Byrne N, Soares M, Katulanda P, Hills A:
Development of a food frequency questionnaire for Sri Lankan adults. Nutrition
Journal 2012, 11:63.
13. Martin Bland J, Altman D: statistical methods for assessing agreement between two
methods of clinical measurement. The Lancet 1986, 327:307-310.
14. Date C, Fukui M, Yamamoto A, Wakai K, Ozeki A, Motohashi Y, Adachi C, Okamoto
N, Kurosawa M, Tokudome Y, et al: Reproducibility and Validity of a Self-
administered Food Frequency Questionnaire Used in the JACC Study. Journal of
Epidemiology 2005, 15:S9-S23.
15. Iqbal R, Ajayan K, Bharathi AV, Zhang X, Islam S, Soman CR, Merchant AT:
Refinement and validation of an FFQ developed to estimate macro- and
micronutrient intakes in a south Indian population. Public Health Nutrition 2009,
12:12-18.
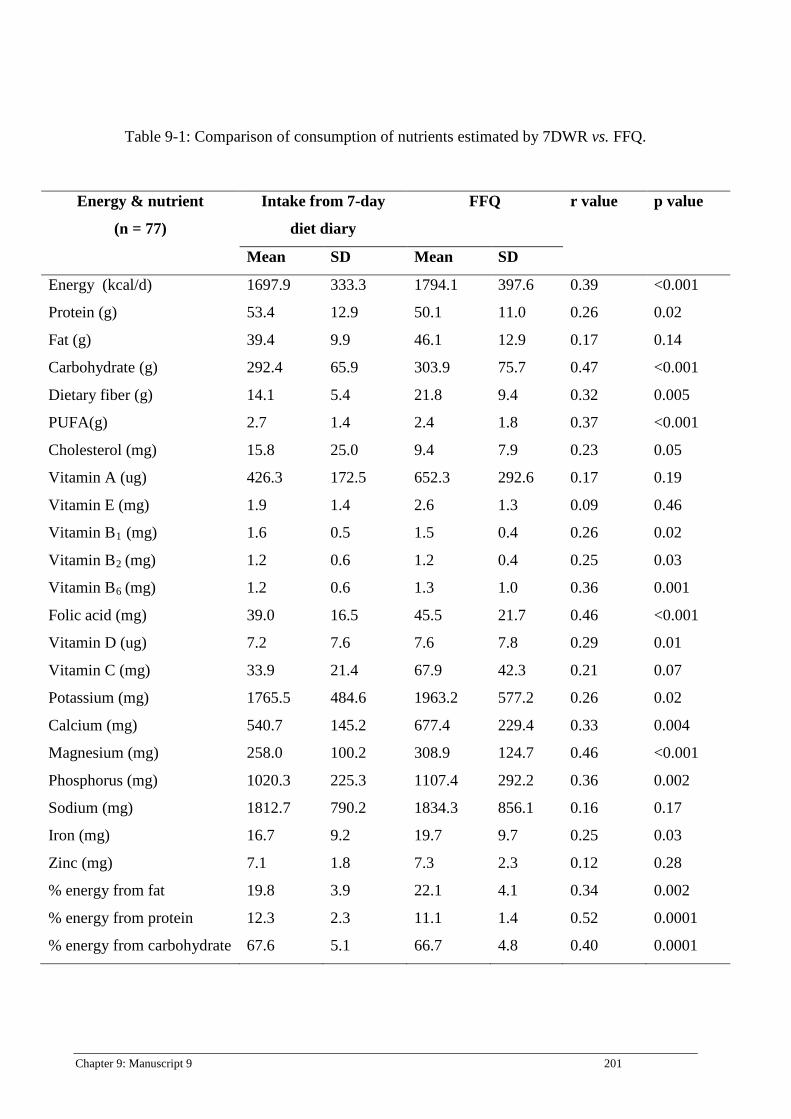
Chapter 9: Manuscript 9 201
Table 9-1: Comparison of consumption of nutrients estimated by 7DWR vs. FFQ.
Energy & nutrient
(n = 77)
Intake from 7-day
diet diary
FFQ r value p value
Mean SD Mean SD
Energy (kcal/d) 1697.9 333.3 1794.1 397.6 0.39 <0.001
Protein (g) 53.4 12.9 50.1 11.0 0.26 0.02
Fat (g) 39.4 9.9 46.1 12.9 0.17 0.14
Carbohydrate (g) 292.4 65.9 303.9 75.7 0.47 <0.001
Dietary fiber (g) 14.1 5.4 21.8 9.4 0.32 0.005
PUFA(g) 2.7 1.4 2.4 1.8 0.37 <0.001
Cholesterol (mg) 15.8 25.0 9.4 7.9 0.23 0.05
Vitamin A (ug) 426.3 172.5 652.3 292.6 0.17 0.19
Vitamin E (mg) 1.9 1.4 2.6 1.3 0.09 0.46
Vitamin B1 (mg) 1.6 0.5 1.5 0.4 0.26 0.02
Vitamin B2 (mg) 1.2 0.6 1.2 0.4 0.25 0.03
Vitamin B6 (mg) 1.2 0.6 1.3 1.0 0.36 0.001
Folic acid (mg) 39.0 16.5 45.5 21.7 0.46 <0.001
Vitamin D (ug) 7.2 7.6 7.6 7.8 0.29 0.01
Vitamin C (mg) 33.9 21.4 67.9 42.3 0.21 0.07
Potassium (mg) 1765.5 484.6 1963.2 577.2 0.26 0.02
Calcium (mg) 540.7 145.2 677.4 229.4 0.33 0.004
Magnesium (mg) 258.0 100.2 308.9 124.7 0.46 <0.001
Phosphorus (mg) 1020.3 225.3 1107.4 292.2 0.36 0.002
Sodium (mg) 1812.7 790.2 1834.3 856.1 0.16 0.17
Iron (mg) 16.7 9.2 19.7 9.7 0.25 0.03
Zinc (mg) 7.1 1.8 7.3 2.3 0.12 0.28
% energy from fat 19.8 3.9 22.1 4.1 0.34 0.002
% energy from protein 12.3 2.3 11.1 1.4 0.52 0.0001
% energy from carbohydrate 67.6 5.1 66.7 4.8 0.40 0.0001
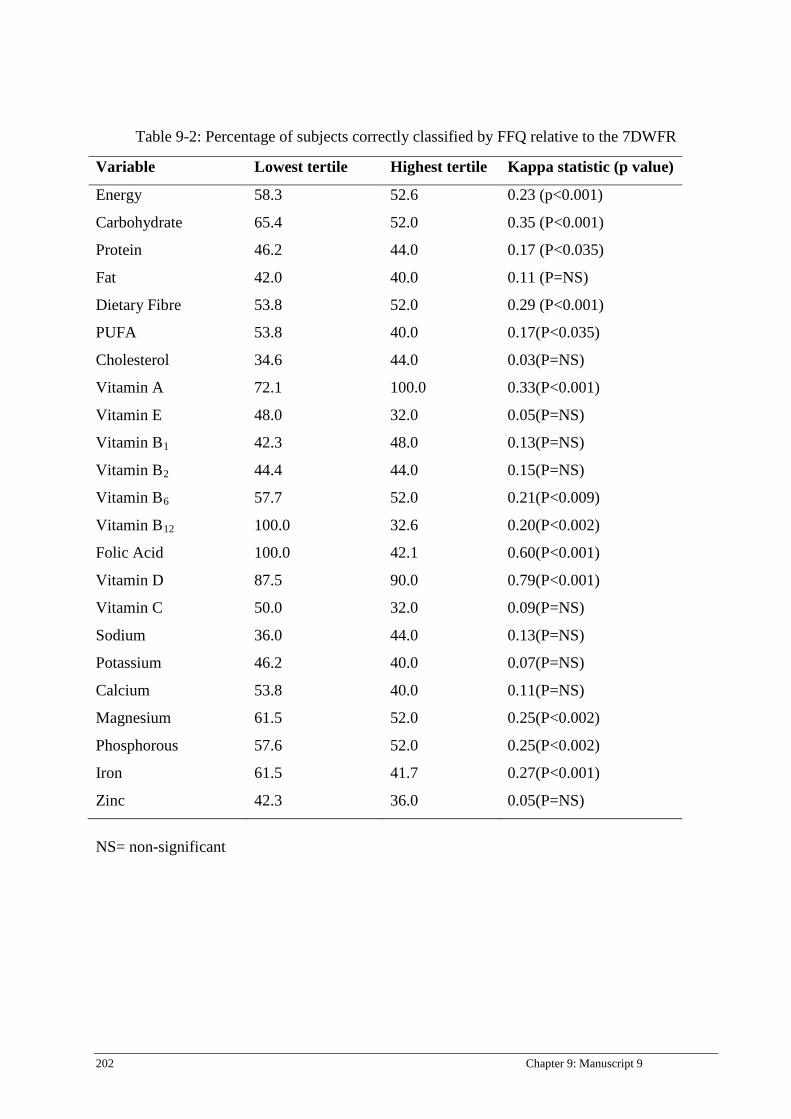
202 Chapter 9: Manuscript 9
Table 9-2: Percentage of subjects correctly classified by FFQ relative to the 7DWFR
NS= non-significant
Variable Lowest tertile Highest tertile Kappa statistic (p value)
Energy 58.3 52.6 0.23 (p<0.001)
Carbohydrate 65.4 52.0 0.35 (P<0.001)
Protein 46.2 44.0 0.17 (P<0.035)
Fat 42.0 40.0 0.11 (P=NS)
Dietary Fibre 53.8 52.0 0.29 (P<0.001)
PUFA 53.8 40.0 0.17(P<0.035)
Cholesterol 34.6 44.0 0.03(P=NS)
Vitamin A 72.1 100.0 0.33(P<0.001)
Vitamin E 48.0 32.0 0.05(P=NS)
Vitamin B1 42.3 48.0 0.13(P=NS)
Vitamin B2 44.4 44.0 0.15(P=NS)
Vitamin B6 57.7 52.0 0.21(P<0.009)
Vitamin B12 100.0 32.6 0.20(P<0.002)
Folic Acid 100.0 42.1 0.60(P<0.001)
Vitamin D 87.5 90.0 0.79(P<0.001)
Vitamin C 50.0 32.0 0.09(P=NS)
Sodium 36.0 44.0 0.13(P=NS)
Potassium 46.2 40.0 0.07(P=NS)
Calcium 53.8 40.0 0.11(P=NS)
Magnesium 61.5 52.0 0.25(P<0.002)
Phosphorous 57.6 52.0 0.25(P<0.002)
Iron 61.5 41.7 0.27(P<0.001)
Zinc 42.3 36.0 0.05(P=NS)
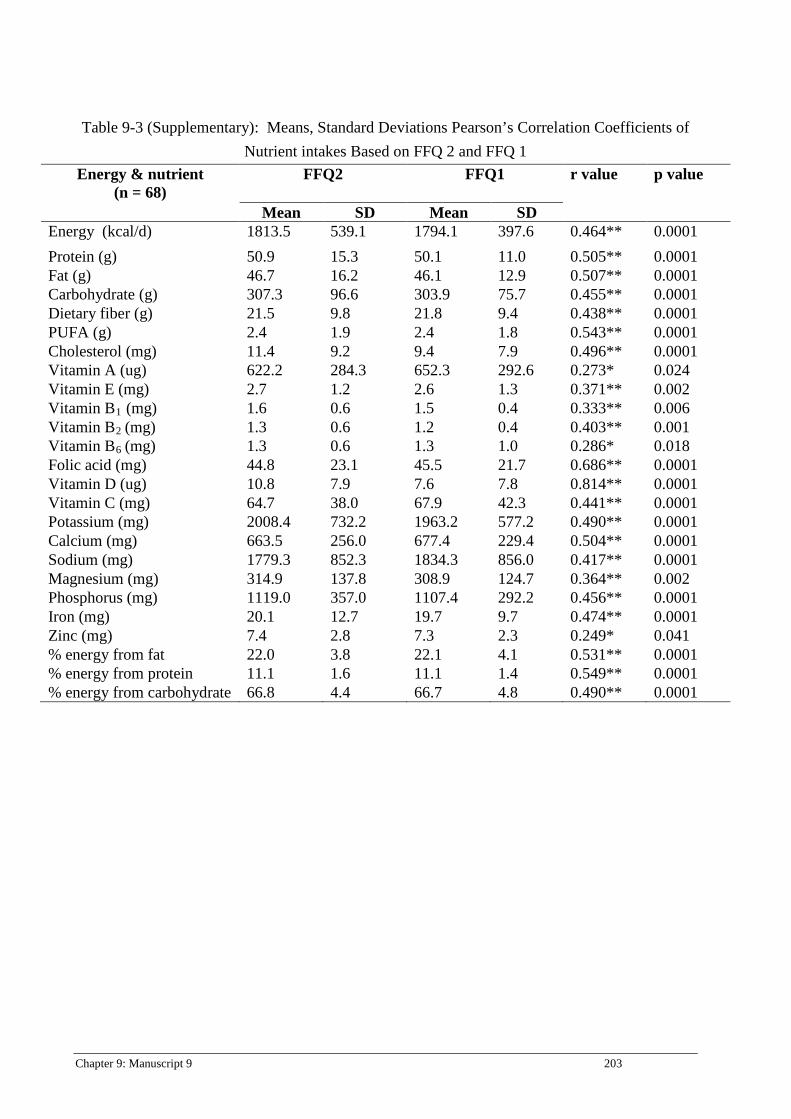
Chapter 9: Manuscript 9 203
Table 9-3 (Supplementary): Means, Standard Deviations Pearson’s Correlation Coefficients of
Nutrient intakes Based on FFQ 2 and FFQ 1
Energy & nutrient (n = 68)
FFQ2 FFQ1 r value p value
Mean SD Mean SD Energy (kcal/d) 1813.5 539.1 1794.1 397.6 0.464** 0.0001 Protein (g) 50.9 15.3 50.1 11.0 0.505** 0.0001 Fat (g) 46.7 16.2 46.1 12.9 0.507** 0.0001 Carbohydrate (g) 307.3 96.6 303.9 75.7 0.455** 0.0001 Dietary fiber (g) 21.5 9.8 21.8 9.4 0.438** 0.0001 PUFA (g) 2.4 1.9 2.4 1.8 0.543** 0.0001 Cholesterol (mg) 11.4 9.2 9.4 7.9 0.496** 0.0001 Vitamin A (ug) 622.2 284.3 652.3 292.6 0.273* 0.024 Vitamin E (mg) 2.7 1.2 2.6 1.3 0.371** 0.002 Vitamin B1 (mg) 1.6 0.6 1.5 0.4 0.333** 0.006 Vitamin B2 (mg) 1.3 0.6 1.2 0.4 0.403** 0.001 Vitamin B6 (mg) 1.3 0.6 1.3 1.0 0.286* 0.018 Folic acid (mg) 44.8 23.1 45.5 21.7 0.686** 0.0001 Vitamin D (ug) 10.8 7.9 7.6 7.8 0.814** 0.0001 Vitamin C (mg) 64.7 38.0 67.9 42.3 0.441** 0.0001 Potassium (mg) 2008.4 732.2 1963.2 577.2 0.490** 0.0001 Calcium (mg) 663.5 256.0 677.4 229.4 0.504** 0.0001 Sodium (mg) 1779.3 852.3 1834.3 856.0 0.417** 0.0001 Magnesium (mg) 314.9 137.8 308.9 124.7 0.364** 0.002 Phosphorus (mg) 1119.0 357.0 1107.4 292.2 0.456** 0.0001 Iron (mg) 20.1 12.7 19.7 9.7 0.474** 0.0001 Zinc (mg) 7.4 2.8 7.3 2.3 0.249* 0.041 % energy from fat 22.0 3.8 22.1 4.1 0.531** 0.0001 % energy from protein 11.1 1.6 11.1 1.4 0.549** 0.0001 % energy from carbohydrate 66.8 4.4 66.7 4.8 0.490** 0.0001

204 Chapter 9: Manuscript 9
2800260024002200200018001600140012001000
1000
500
0
-500
-1000
Averages
Diff
eren
ces
LLA = -897.05
ULA = 704.64
Mean = -96.20
Bland-Altman Plot
Figure 9-1: Bland and Altman plots for energy with the mean difference and limits of
agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of agreements in red line.
807060504030
50
40
30
20
10
0
-10
-20
-30
Averages
Diff
eren
ces
LLA = -24.95
ULA = 32.06
Mean = 3.55
Bland-Altman Plot
Figure 9-2: Bland and Altman plots for protein with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95%
limits of agreements in red line.

Chapter 9: Manuscript 9 205
706050403020
30
20
10
0
-10
-20
-30
-40
-50
Averages
Diff
eren
ces
LLA = -35.34
ULA = 22.42
Mean = -6.46
Bland-Altman Plot
Figure 9-3: Bland and Altman plots for fat with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95% limits of
agreements in red line.
450400350300250200150
200
100
0
-100
-200
Averages
Diff
eren
ces
LLA = -180.09
ULA = 98.25
Mean = -40.92
Bland-Altman Plot
Figure 9-4: Bland and Altman plots for carbohydrates with the mean difference and limits of agreements. Averages = FFQ+&DWR/2. Mean difference (FFQ-7DWR) is green line and 95%
limits of agreements in red line.
206 Chapter 10: General discussion
Chapter 10: General discussion
Chapters two to nine have incorporated separate discussion sections in which a specific
commentary of respective research findings in relation to the local, regional and global literature
have been provided. Further, each chapter has provided an interpretation of factors that may
have contributed to the research findings, the strengths and limitations of each study, and the
implications of the results for health promotion, education and further research. This final
chapter provides an overall discussion of the findings of the three major studies and the nine
manuscripts which collectively address the applicability of different nutritional assessment tools
and nutritional issues in South Asia in relation to current diabetic epidemic. The significance of
the research is discussed in light of its contribution to the current body of knowledge. Moreover,
this chapter discusses the strengths and limitations of the project as a whole. Finally, an overall
conclusion is provided along with a discussion of the application of findings for both clinical and
public health settings, and recommendations for future research.
Chapter 10: General discussion 207
COMPARISON OF DIFFERENT DIETARY ASSESSMENT TOOLS
Many different methods have been developed for the purpose of assessing dietary intake (1).
These range from detailed individual weighed records collected over a certain time period to
food frequency questionnaires, dietary recalls, household survey methods and dietary histories.
The most appropriate dietary assessment tool will depend on the purpose for which it is needed
e.g. to measure nutrients, foods or eating habits and diet-related health risks. It is important to
understand that each method has merits, associated errors and practical difficulties to be
considered when making a choice (2). While the 7-day weighed record is widely considered as
the reference method (3) for large epidemiological surveys, the FFQ is a more appropriate
method (1).
Dietary records
The respondent records the identity and amounts of all foods and beverages at the time of
consumption for a period of time (usually 1-7 days). Food and beverages are quantified by
estimating portion sizes using household measurements, or weighing the food or beverage on
scales. There are two types of food records 1) estimated food records and 2) weighed food
records (2).
For the estimated food record approach, the respondent records the foods and beverages and the
amounts of each consumed over one or more days. The amounts consumed may be measured,
using a scale or household measure (such as cups, tablespoons), or estimated, using models,
pictures, or no particular aid (2). Typically, if multiple days are recorded, they are consecutive
and no more than 3 or 4 days are included. Recording periods of more than 4 consecutive days
are usually unsatisfactory, as reported intakes decrease because of respondent fatigue (4).
The weighed record involves an individual or an investigator weighing every item of food and
drink prior to consumption. A detailed description of the food and its weight is recorded in a
specially designed booklet. Usually a space is left to record any leftovers so that the precise
weight of food eaten can be calculated. The 7-day weighed record has often been referred to as
the ‘gold standard’ against which less detailed and demanding methods can be compared (3). In

208 Chapter 10: General discussion
this thesis, a 7-day weighed record was used to validate the newly developed food frequency
questionnaire. However for collecting the food list, a 24-hour dietary recall was administrated.
24-hour dietary recall
For the 24-hour dietary recall, the respondent is asked to remember and report all the foods and
beverages consumed in the preceding 24 hours or in the preceding day. The recall is typically
conducted by interview, in person or by telephone - either computer-assisted or using a paper-
and-pencil form (5). Well-trained interviewers are crucial to administer a 24-hour recall as much
of the information is collected by asking probe questions. Ideally, the interviewer should be a
nutritionist; however, non-nutritionists who have been trained in the use of a standardized
instrument can also be effective. All interviewers should be knowledgeable about foods
available in the marketplace and about preparation practices, including prevalent regional and
ethnic foods or need to perform face validity (1). The interview is often structured, usually with
specific probes to help the respondent remember all foods consumed throughout the day.
Probing is especially useful in collecting necessary details, such as how foods were prepared. It
is also useful in recovering many items not originally reported, such as common additions to
foods (e.g., curry on rice) and eating occasions not originally reported (e.g., snacks and beverage
breaks). This is particularly important for elderly groups (2). However, interviewers should be
provided with standardized neutral probing questions so as to avoid leading the respondent to
specific answers when the respondent really does not know or remember (1).
Dietary history
Particularly in clinical settings a dietary history is used to assess eating habits and nutrition
levels. A dietary history is a structured interview method consisting of questions about habitual
intake of foods from the core (e.g., meat and alternatives, cereals, fruit and vegetables, dairy and
‘extras’) food groups in the last seven days (1). This is followed by a ‘cross check’ to clarify
information about usual intake in the past 3, 6, or 12 months, depending on the aims of the
assessment. This can be used as an alternative to the 24-hour dietary history or food recall. Usual
portion sizes are generally obtained in household measures and/or with the use of photographic
aids (5).
Chapter 10: General discussion 209
Food Frequency Questionnaire (FFQ)
The FFQ is one of the most commonly used methods in epidemiological studies to assess
individual long-term dietary intake of foods and nutrients (2). The questionnaires are typically
self-administered, asking the respondents to report the usual frequency of consumption of items
from a list of foods for a specified time period. The method is sufficiently simple to be used in
large epidemiological studies. Even though the absolute intake is an estimate, using this method
can rank individuals by levels of past nutrient intake in epidemiological studies (1). The
questionnaire is able to rank the population into levels of exposure which are used in the
calculation of relative risk for the development of the disease in question. Therefore, the FFQ is
the most suitable method for measuring dietary factors for nutrition-related NCDs in a large
survey. Moreover, the FFQ can be used to represent different ethnic groups as well as to
discriminate between people’s intake for nutrients known to be associated with the nutritional
related disease (6). For example, Liu et al. found a FFQ was able to assess dietary glycaemic
load in relation to metabolic risk factors (7).
At its simplest, the FFQ consists of a list of foods and a selection of options relating to the
frequency of consumption of each of the foods listed (e.g., times per day, daily, weekly,
monthly)(1). FFQs are designed to collect dietary information from large numbers of individuals
and are normally self-administered, though interviewer-administered and telephone interview are
possible modifications. Levels of education and facilities will determine the mode of
administration. For example, interviewer-administrated methods have been used in India where a
considerable proportion of the population is illiterate whereas in developed countries, an
internet-based FFQ is widely used (8). FFQs normally ask about intake within a given time
frame (e.g., in the past 1-2 months or 1 year) and therefore aim to capture habitual intake. The
length of the food list can vary depending on the nutrients or foods of interest. The number of
food items varies from few to several hundred (1). Many FFQs also attempt to collect
information about portion size in addition to frequency of consumption (9). These may be
referred to as semi-quantitative FFQs. Although there are difficulties implicit in calculating the
absolute nutrient intake of individuals from food frequency questionnaires, they are useful for
gathering information on groups of individuals as well as for looking at habitual intake of a
range of foods.
210 Chapter 10: General discussion
The appropriateness of the food list is crucial in the food frequency method (10). The full
variability of an individual’s diet, which includes many foods, brands, and preparation practices,
cannot be fully captured with a finite food list. Obtaining accurate reports for foods eaten both as
single items and in mixtures is particularly problematic especially in Asian countries where
many mixed dishes and curries eaten. FFQs can ask the respondent to report either a combined
frequency for a particular food eaten both alone and in mixtures or separate frequencies for each
food used. All FFQs must be associated with a food database to allow for the estimation of
nutrient intakes for an assumed or reported portion size of each food queried (8).
In pursuit of improving the validity of the FFQ, investigators have addressed a variety of
frequency questionnaire design issues such as length, closed versus open-ended response
categories, portion size, seasonality, and time frame (1,10). Frequency instruments designed to
assess total diet generally list more than 100 individual line items, many with additional portion
size questions, requiring 30 to 60 minutes to complete. This raises concern about length and its
effect on response rates.
Accuracy of nutrient estimates
Accuracy of energy and nutrient is extremely important in any nutrition survey. The accuracy of
nutrient estimates depends on two factors: the accuracy of dietary information provided by the
participants and the accuracy of the food composition data. Key considerations related to these
two potential sources of error are outlined below.
Any technique used to measure food intake should not interfere with the subject's dietary habits
as this may alter the parameter being measured. Both under-reporting and over-reporting of food
intake are well-known problems in all types of dietary surveys, regardless of the dietary
assessment method used. If food intake is under-reported, energy and nutrient intakes may also
be underestimated, and estimates of inadequate intake may be overestimated. It is difficult to
quantify under-reporting, but research shows that the degree of under-reporting varies according
to personal characteristics and across types of foods (11,12). For example, under-reporting is
more common in those with a high BMI, and in females. Certain foods are more likely to be
under-reported, especially those perceived as less healthy (e.g., cakes, biscuits, desserts, fats).
On the other hand, over-reporting of fruit and vegetable intake can be seen amongst more
educated groups (11). Moreover, it is widely observed that culturally preferred foods tend to be
over-reported and vice versa (13). Apart from the type of foods, an accurate detail of the amount
of food is equally important. In all dietary assessment methods where food is not weighed,

Chapter 10: General discussion 211
portion sizes must be determined before nutrient output can be calculated. There are a number of
methods by which portion sizes may be obtained. These may include field workers weighing
certain food items on the individual’s behalf, the use of photographic atlases (14, 15) showing
portion sizes of commonly eaten foods to an individual, using data from manufacturers, portion
sizes collected from previous weighed food records, and household measures.
Unlike most developed countries, there is no centrally managed nutrient database in Sri Lanka.
We therefore compiled information from the food composition tables of Sri Lanka (16), the
United States Department of Agriculture nutrient database (USDA) (17), the Indian Food
Composition Tables (18), and McCance and Widdowson’s food composition tables (19) to
develop a comprehensive and new nutrient composition database as follows. a) Nutrition values
for single food items were taken mainly from the USDA nutrient database; b) Nutrition
information leaflets or details from direct contact with producers were used for locally available
food products (e.g., biscuits); c) For mixed dishes and cooked foods, local recipes were taken
from popular cookery books (20), and by interviewing participants. All recipes were accepted
after checking for face validity by consulting local housewives and nutritionists. According to
the recipes, ingredients were weighed to the nearest 1 g for edible portions of the foods, and the
food items were cooked and weighed. Nutritional composition of the final recipe was calculated
by entering nutritional values and weights of individual ingredients into a spreadsheet. The sum
of each nutrient was computed and standardized to 100 g of the final product. Data on weight
loss associated with cooking (e.g., due to water evaporation) was recorded to ensure accurate
nutrient density of the portion size consumed. However, nutrient losses (e.g., vitamins) during
food preparation were not considered. However in ideal circumstances, all food items should be
chemically analysis for their nutrient ingredients.
212 Chapter 10: General discussion
NUTRITIONAL ISSUES IN SOUTH ASIA IN RELATION TO THE CURRENT DIABETES EPIDEMIC
Diet is an important factor in preventing diabetes, managing existing diabetes, and preventing, or
delaying the development of its complications (21). Eating habits are one of the main
determinants of diabetes among South Asians. Although the published data on dietary habits and
development of diabetes in this region is limited, it is believed that dietary habits play an
important role in the epidemic of diabetes among South Asians.
Carbohydrates
Compared to Europeans, the diet of South Asians is predominantly based on starchy foods (22).
Similarly, Indian vegetarians have a higher percentage of carbohydrates in their diet when
compared to American vegetarians and non-vegetarians (23). Our data shows a majority of Sri
Lankan adults consume starchy foods above the upper limit of recommendations (24). Elevated
2-h insulin concentrations have been shown to be positively associated with the proportion of
energy intake from carbohydrate (22). Others have shown that compared with a low-
carbohydrate diet (35% of total energy from carbohydrates), an iso-caloric high-carbohydrate
diet (60% of total energy from carbohydrates) caused a 27.5% increase in plasma triglycerides, a
similar increase in VLDL-cholesterol levels, and an 11% reduction in HDL cholesterol levels
(25). A typical South Asian diet consists of over 60% of carbohydrates which may lead to
undesirable glycaemic and lipid changes. The quality of carbohydrates is also an important
factor in diabetes and a diet with high glycaemic index foods has been shown to increase
postprandial plasma glucose levels in subjects with impaired glucose tolerance (26). Mohan et
al. argued that increased consumption of refined cereals may be more detrimental than the
amount of carbohydrates among Indians (27). Higher intake of white rice was associated with an
increased risk of type 2 diabetes (28). Added sugar consumption is also high in India (29). Sri
Lankans consume over 3.5 portions of sugar day (24) and as sugary foods and refined starch
digest rapidly and are converted to glucose, this increases insulin demand and may lead to
pancreatic b-cell exhaustion in the long run (30).
Dietary fats
In a 14-year follow-up of 84,204 non-diabetic women, total fat and SFA and MUFA intake were
not associated with risk of type 2 diabetes (31). Similarly, another large prospective study on
Chapter 10: General discussion 213
men (n=42,504) found total fat and SFA were not associated with type 2 diabetes incidence
when adjusted for BMI (32). According to the National Sample Survey Organization (2004-
2005), the consumption of fat among Indians was 44 g/d in rural areas and 58.2 g/d in urban
areas (33). In the studies conducted in this thesis, we found that fat intake among men and
women in Sri Lanka was 40.5 g/d and 31.9 g/d, respectively (34). Most South Asians are getting
less than 20% of total calories from fat. According to the ranges of population nutrient intake
goals recommended by WHO, the percentage of energy from total carbohydrates, fats and
proteins should be 55-75%, 15-30% and 10-15%, respectively (35). Total fat consumption as an
energy source is under the safe limits among South Asians. However, type of fats may be
significant in this population. India and other South Asian countries often use ghee for cooking
which contains high TFA (36) whereas Sri Lankans and South Indians often consume coconut
products which contain SFA (37). Full cream milk and dairy products also provide SFA and
cholesterols. Although there is no evidence to suggest fat consumption and diabetes are
associated among South Asians, unhealthy fat consumption might increase the complications of
diabetes, especially cardiovascular complications. Ghee and dairy products also provide SFA
and cholesterols. On the other hand, MUFA and PUFA consumption is low among this
population (38).
Dietary fiber
Large prospective studies support a protective role of dietary fiber for the development of
diabetes (39, 40). A randomized, cross-over study showed that a high fiber diet (total, 50 g; 25 g
of soluble fiber and 25 g of insoluble fiber) compared to the recommended amount (total, 24 g; 8
g of soluble fiber and 16 g of insoluble fiber), significantly improved glycaemic control,
decreased hyperinsulinaemia, and lowered plasma lipid concentrations in patients with type 2
diabetes (41). These benefits most likely occur by slowing the digestion and absorption of food
and by regulating several metabolic hormones (40). Limited available data showed that daily
intake of dietary fiber is low among South Asians (34, 38).
Vitamin and minerals
Zinc is an important structural and functional molecule for insulin. Zinc supplementation in
patients with diabetes demonstrates that zinc supplementation has beneficial effects on
glycaemic control and promotes healthy lipid parameters (42). A meta-analysis of randomized
double-blind controlled trials regarding the effect of magnesium supplementation on glycaemic
control in type 2 DM showed significant reduction of fasting glucose level in the treatment

214 Chapter 10: General discussion
group (43). Mean daily intake of manganese and zinc is lower in Indian vegetarians (23). A
systematic review and meta-analysis of observational studies and clinical trials in adults with
outcomes related to glucose homeostasis showed vitamin D and calcium insufficiency may
negatively influence glycaemia (44). Several studies reported a high prevalence of
hypovitaminosis D and low dietary calcium level among Indians (45, 46). Our data showed low
calcium and vitamin D intakes among Sri Lanka adults. Indians consumed high amounts of salt,
Indian (Ladakh) men showed >200 mmol/day sodium excretion (47). In a Finnish prospective
study, the hazard ratio for diabetes for the highest (>200 mmol/24 h) versus combined lower
quartiles of 24-h urinary sodium excretion was 2.05 (95% CI, 1.43-2.96) after adjusting several
known risk factors. In contrast, potassium may have a protective effect against diabetes (48).
Fruit and vegetables are good sources of potassium.
Fruit and vegetables
Fruit and vegetables contain several nutrients, which may have a number of health benefits. The
effect is beyond the cumulative effects of individual nutrients such as dietary fiber, vitamins and
antioxidants. Although fruit and vegetables are not nutrients, we elaborate separately. Fruit and
vegetable intake is inversely associated with diabetes incidence (49). The EPIC-Norfolk Study
reported that subjects with unknown diabetes that consumed higher intakes of fruits and
vegetables had significantly lower levels of HbA1c (50). In a multivariate analysis, a significant
inverse trend was observed between fruit intake and the probability of having the glycaemic
component (plasma glucose ≥110 mg/dl) of metabolic syndrome features (51). Fruit and
vegetables reduce diabetes-associated complications, especially heart disease and stroke (52).
Fruit and vegetables are widely available in the South Asian countries but consumption is very
low. Average fruit consumption of four cities from Bangladesh was 1.7 servings/day and 1.6
servings/day among men and women, respectively. Corresponding values for vegetable
consumption were 3.4 and 3.0, for men and women (53). Fruit and vegetable intake among
Indian men and women were 1.2 servings/day for fruit and 1.3 servings/day for vegetables.
According to the World Health Survey 2002-2003, Pakistan and Nepal have the highest
prevalence of low fruit and vegetable consumption among 52 countries. Less than 1% of
Pakistani and less than 2% of Nepalese consume a minimum of five fruits and vegetables daily
(54). In Sri Lanka, we found that mean dietary intake of fruit and vegetables was 2.16
portions/day and only 3.5% of adults consumed according to the recommendations (24).
Similarly, only 2.7% of Maldives adults had five or more portions of fruits and vegetables daily
Chapter 10: General discussion 215
(55). The vegetable consumption pattern is very unique among South Asians. Although there is a
considerable variation among different ethnic groups, most of the vegetables are consumed in
the form of a curry, with cooking oils, curd, coconut milk and dairy fats. Moreover, adding
strong spices prevents consumption of vegetables in a large quantity. The cooking methods used
are boiling, steaming, grilling, baking and roasting as opposed to the South Asian countries
where frying is mostly the preferred method.
Occurrence and progression of diabetes and other metabolic diseases are associated with dietary
habits however assessment of dietary factors for chronic diseases is inherently difficult due to
several confounding factors. There is limited published data available on nutrient composition
and dietary habits of native South Asians. Lifestyle factors of immigrant South Asians could also
be different to their native counterparts. Furthermore, dietary habits are considerably
heterogeneous among ethnic groups. Culturally specific and sensitive dietary interventions are
required to identify nutritional risk factors for diabetes among South Asians.
216 Chapter 10: General discussion
STRENGTHS OF THE STUDY
There are several strengths of this research work including the sampling, data collection and
reporting methods. Firstly, studies were based on a sub-sample of the Sri Lanka Diabetes and
Cardiovascular Study (SLDCS). The SLDCS included a nationally representative sample of
5000 adults aged ≥18 years selected using a multi-stage random cluster sampling technique. The
response rate for the first study was over 80% and for the validation study approached 70%.
Having a representative sample is a key strength for any population-based study.
Secondly, although data collection was undertaken in different community settings, all
anthropometric data were collected using standardised equipment and techniques. Similarly, as
discussed in Chapter 2, robust data collection techniques were applied to collect the 24-hour
recall data. The seven-day weighed intake (7DWI) is considered the “gold standard” method to
retrieve dietary data. A satisfactory validation against 7DWI demonstrated the appropriateness of
the FFQ for this population.
Finally, it is extremely difficult to categorize mixed dishes to food groups therefore complex
dishes were disaggregated before ingredients were categorized into appropriate food groups.
This scientifically sound method helped to categorize dishes into the main food groups.
Moreover, defining portion sizes for many local fruit and vegetable, protein and starch items is
based on sound nutrition concepts.
LIMITATIONS OF THE STUDY
Due to the scope and various constraints such as time and funding associated with the
completion of the PhD project within a three-year period, several limitations of this research
Chapter 10: General discussion 217
project must be acknowledged. These relate to sampling, selection and confounding bias, and
limitations of some of the measurement tools used.
The accuracy of cross-sectional studies is based on the selection of a representative sample.
However, participation rate is a significant factor to assess the quality of the sampling. Study 1
had an 82% response rate but male participation was considerably lower. Moreover,
participation of young adults was limited. Although data collection was undertaken with prior
notice, few men and young working people participated due to other commitments. Having a
large proportion of over 40 year-old adults may limit the interpretation for young adults with
diverse eating patterns. Similarly, Study 2 was dominated by middle-aged women. Weighing
their own food was also not practical for many busy individuals.
Sri Lanka is a multi-cultural country with four sub-ethnic groups, namely Sinhalese, Indian
Tamil, Sri Lankan Tamils and Muslims. Each sub-ethnic group has different dietary and
behaviour patterns. Due to the small sample size, the representation of dietary intakes of
minority ethnic groups may not be adequate. The lower number of subjects in minority groups
may have affected an accurate determination of the prevalence of obesity. For example, there
was a high non-response rate from Sri Lankan Tamils in the previously war-affected areas.
Another shortcoming of this study was the limited accuracy of the nutrient values of some of the
food items. Due to highly diverse food items, many local food items were not available in any of
the food composition databases. Furthermore, there is a significant difference in the list of
ingredients in the ‘same’ dishes due to differences in cultural background. Therefore, due to the
absence of accurate nutritional composition of the food items, energy and nutrient values of
similar food items were used.

218 Chapter 10: General discussion
Obesity perception is very subjective. Measurement of obesity using an objective scale is not the
ideal. Self-perception of body weight is associated with additional parameters such as perception
of body shape and associated health risk. Qualitative details of misperception of body weight
would provide a more complete picture and help to better understand misperception of body
weight among this population. Lack of qualitative data with regards to obesity perception may
therefore be a limitation of the studies presented in this thesis.
RECOMMENDATIONS
Recommendations for future research
It is evident that Sri Lanka has a serious diet-related non-communicable diseases burden. A lack
of local data on eating habits and nutrient intake are evident. Our findings showed high intakes
of starchy foods and low fruit and vegetable intake. However, we collected only quantitative
data therefore we do not know the reasons for these less healthy eating habits which may be
associated with several cultural, economic and behavioural factors. Therefore, qualitative studies
among a representative group of adults would be essential to determine the underlying reasons
and causes at the grass root level. Similarly, qualitative data are necessary for a better
understanding of the misperception of body weight among many Sri Lankan adults.
Analytical research is important to obtain accurate nutrient values of local fruits, vegetables,
green leaves and locally made sweets. These foods play an important role in the Sri Lankan diet
but a lack of nutrition composition data hinders the provision of culturally acceptable nutritional
advice. In particular, research on micronutrients such as vitamin, mineral and anti-oxidant levels
is essential. Moreover, as Sri Lankans often consume foods which are cooked under extreme
heat and for a long time, it is hard to predict the nutrient composition of the end meal. Food
science research is therefore important to accurately document nutrient values of Sri Lankan
meals.

Chapter 10: General discussion 219
Children’s dietary patterns are equally important in the prevention of diet-related NCDs.
However, currently there is no country-specific FFQ for children. Dietary habits and portion
sizes in children are very different to adults. In particular, take-away foods are the main choices
in schools. Adolescents also have distinctive eating habits during a life transition period that can
be both physically and mentally taxing. Further research is therefore important to document the
food habits of children and adolescents and associated health risks in Sri Lanka.
Recommendations for public health and clinical initiatives and interventions
Translation of theory to practice is essential in health-related studies. This thesis is the first
nutritional survey undertaken in Sri Lanka and reports several unhealthy eating habits among
adults. However, cross-sectional studies are not adequate to establish the causative relationship
between dietary habits and high NCD levels. With the current findings, it is possible to start
public health intervention studies to encourage the reduction of high starchy food consumption
and increase intake of fruit and vegetables. Furthermore, dairy consumption of Sri Lankans is
also extremely low which may be due to the unavailability of fresh milk. Government policies
should give higher priority to increased milk and dairy food production and consumption.
The number of people suffering from obesity and diabetes has reached epidemic levels.
However, dietary changes and weight reduction are challenging for clinicians. Our data showed
an association between dietary habits and obesity level among Sri Lankan adults. A significant
amount of nutrition knowledge is important to provide a balanced diet with limited food items.
One of the main objectives of this thesis was to develop and validate a country-specific FFQ for
Sri Lankan adults. Researchers and government bodies should utilize this FFQ for the next
national health survey and other dietary intervention studies. The Sri Lankan government should
provide the technical support to improve the practicality of this FFQ for large-scale studies.

220 Chapter 10: General discussion
Firstly, optical scanning facilities are needed to obtain selected food items and secondly,
software development for the analysis of nutrients values and reporting is needed.
Chapter 10: General discussion 221
CONCLUSIONS
This thesis fills the significant research gap regarding dietary habits and obesity in Sri Lankan
adults. Findings from the nutrition survey showed on average, Sri Lankan adults consumed over
14 portions of starch/d; moreover, males consumed 5 more portions of cereal than females. Sri
Lankan adults consumed on average of 3.56 portions of added sugars/d with mean daily intake
of fruits and vegetables well below minimum dietary recommendations. As expected, over 70%
of energy was derived from carbohydrates. Moreover, high dietary diversity was associated with
high obesity levels among Sri Lankan adults. The success of a weight reduction intervention is
dependent upon an individual’s awareness of their own body weight and their motivation to
change. Self-perception of body weight is a strong determinant of nutritional habits and weight
management and misperception of body weight may be a barrier to successful weight loss and
healthy weight management in this population. The development and validation of this country-
specific FFQ will boost nutritional research in the country however more effective collaborations
of clinicians, public health experts and policy makers are needed to improve the health and
wellbeing of Sri Lankan adults.
222 Chapter 10: General discussion
REFERENCE LIST
1. Walter Willett EL. Nutritional epidemiology. In: Willett W, editor. Monographs in
Epidemiology and Biostatistics: Oxford University Press; 1998. p. 101-47.
2. Wendy Wrieden. A short review of dietary assessment methods used in National and
Scottish Research Studies. Dundee2003.
3. Henderson L, Gregory J, Swan G. The national diet & nutrition survey: Adults aged 19 to
64 years: Stationery Office; 2003.
4. Gersovitz M, Madden JP, Smiciklas-Wright H. Validity of the 24-hr. dietary recall and
seven-day record for group comparisons. Journal of the American Dietetic Association.
1978;73(1):48.
5. Buzzard I, Faucett CL, Jeffery RW, McBANE L, McGOVERN P, Baxter JS, et al.
Monitoring Dietary Change in a Low-Fat Diet Intervention Study:: Advantages of Using 24-
Hour Dietary Recalls vs Food Records. Journal of the American Dietetic Association.
1996;96(6):574-9.
6. Shahar D, Shai I, Vardi H, Brener-Azrad A, Fraser D. Development of a semi-
quantitative Food Frequency Questionnaire (FFQ) to assess dietary intake of multiethnic
populations. European journal of epidemiology. 2003;18(9):855-61.
7. Liu S, Manson JE, Stampfer MJ, Holmes MD, Hu FB, Hankinson SE, et al. Dietary
glycemic load assessed by food-frequency questionnaire in relation to plasma high-density-
lipoprotein cholesterol and fasting plasma triacylglycerols in postmenopausal women. Am J Clin
Nutr. 2001 Mar;73(3):560-6.
8. Bharathi AV, Kurpad AV, Thomas T, Yusuf S, Saraswathi G, Vaz M. Development of
food frequency questionnaires and a nutrient database for the Prospective Urban and Rural
Epidemiological (PURE) pilot study in South India: methodological issues. Asia Pac J Clin Nutr.
2008;17(1):178-85.
9. Victoria CC. Dietary questionnaires. 2010; Available from:
http://www.cancervic.org.au/about-our-research/epidemiology/nutritional_assessment_services.
10. Bharathi A, Kurpad A, Thomas T, Yusuf S, Saraswathi G, Vaz M. Development of food
frequency questionnaires and a nutrient database for the Prospective Urban and Rural
Epidemiological (PURE) pilot study in South India: Methodological issues. Asia Pacific Journal
of Clinical Nutrition. 2008;17(1):178-85.

Chapter 10: General discussion 223
11. Mendez MA, Wynter S, Wilks R, Forrester T. Under- and overreporting of energy is
related to obesity, lifestyle factors and food group intakes in Jamaican adults. Public Health
Nutr. 2004 Feb;7(1):9-19.
12. Azizi F, Esmaillzadeh A, Mirmiran P. Correlates of under- and over-reporting of energy
intake in Tehranians: body mass index and lifestyle-related factors. Asia Pac J Clin Nutr.
2005;14(1):54-9.
13. Mattisson I, Wirfalt E, Aronsson CA, Wallstrom P, Sonestedt E, Gullberg B, et al.
Misreporting of energy: prevalence, characteristics of misreporters and influence on observed
risk estimates in the Malmo Diet and Cancer cohort. British Journal of Nutrition.
2005;94(5):832-42.
14. Michael Nelson MA, James Meyer. A Photographic Atlas of Food Portion Sizes. UK:
MAFF publications; 1997.
15. Suzana Shahar NAMY, Nik Shamita Safii, Rafidah Ghazau, Roslina Ahmad. Atlas of
Food Exchanges & Portion Sizes. Kuala Lampur: MDC Publishers; 2009.
16. Perera WDA JP, Thaha SZ, . Tables of food composition for use in Sri Lanka.
Colombo1979.
17. National Agricultural Library. USDA: Foods List. . 2013.
18. Gopalan C RB, Balasubramanian SC, . Nutritive value of Indian foods. Hyderabad:
National Institute of Nutrition; 1989.
19. Welch AA UI, Buss DH, Paul AA, Southgate DAT, . McCance and Widdowson’s The
Composition of Foods. Cambridge: Royal Society of Chemistry; 1995.
20. Dissanayake C. Ceylon Cookery: Stamford Lake (pvt) Ltd. ; 2010.
21. Association AD. Nutrition Recommendations and Interventions for Diabetes: A position
statement of the American Diabetes Association. Diabetes Care. 2008 January 1,
2008;31(Supplement 1):S61-S78.
22. Sevak L, McKeigue PM, Marmot MG. Relationship of hyperinsulinemia to dietary intake
in south Asian and European men. The American Journal of Clinical Nutrition. 1994 May 1,
1994;59(5):1069-74.
23. Kelsay JL, Frazier CW, Prather ES, Canary JJ, Clark WM, Powell AS. Impact of
variation in carbohydrate intake on mineral utilization by vegetarians. Am J Clin Nutr. 1988
Sep;48(3 Suppl):875-9.
24. Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Hills AP. Food consumption of Sri
Lankan adults: an appraisal of serving characteristics. Public Health Nutrition. 2013;16(04):653-
8.

224 Chapter 10: General discussion
25. Garg A, Grundy SM, Unger RH. Comparison of Effects of High and Low Carbohydrate
Diets on Plasma Lipoproteins and Insulin Sensitivity in Patients With Mild NIDDM. Diabetes.
1992 October 1, 1992;41(10):1278-85.
26. Wolever TM, Mehling C. Long-term effect of varying the source or amount of dietary
carbohydrate on postprandial plasma glucose, insulin, triacylglycerol, and free fatty acid
concentrations in subjects with impaired glucose tolerance. Am J Clin Nutr. 2003
Mar;77(3):612-21.
27. Mohan V, Radhika G, Vijayalakshmi P, Sudha V. Can the diabetes/cardiovascular
disease epidemic in India be explained, at least in part, by excess refined grain (rice) intake?
Indian J Med Res. 2010 Mar;131:369-72.
28. Sun Q, Spiegelman D, van Dam RM, Holmes MD, Malik VS, Willett WC, et al. White
rice, brown rice, and risk of type 2 diabetes in US men and women. Arch Intern Med. 2010 Jun
14;170(11):961-9.
29. Popkin BM, Horton S, Kim S, Mahal A, Shuigao J. Trends in diet, nutritional status, and
diet-related noncommunicable diseases in China and India: the economic costs of the nutrition
transition. Nutr Rev. 2001 Dec;59(12):379-90.
30. Hu FB. Globalization of diabetes: the role of diet, lifestyle, and genes. Diabetes Care.
2011 Jun;34(6):1249-57.
31. Salmeron J, Hu FB, Manson JE, Stampfer MJ, Colditz GA, Rimm EB, et al. Dietary fat
intake and risk of type 2 diabetes in women. Am J Clin Nutr. 2001 Jun;73(6):1019-26.
32. van Dam RM, Willett WC, Rimm EB, Stampfer MJ, Hu FB. Dietary fat and meat intake
in relation to risk of type 2 diabetes in men. Diabetes Care. 2002 Mar;25(3):417-24.
33. Ministry of Statistics & Programme Implementation Government of India.
NUTRITIONAL INTAKE IN INDIA 2004-2005. New Delhi 2007 Contract No.: Report No.
513(61/1.0/6).
34. Jayawardena R, Swaminathan S, Byrne N, Soares M, Katulanda P, Hills A. Development
of a food frequency questionnaire for Sri Lankan adults. Nutrition Journal. 2012;11(1):63.
35. Report of a Joint WHO/FAO Expert Consultation. Diet, Nutrition and the prevention of
Chronic Diseases. Geneva 2003.
36. Ismail J, Jafar TH, Jafary FH, White F, Faruqui AM, Chaturvedi N. Risk factors for non-
fatal myocardial infarction in young South Asian adults. Heart. 2004 Mar;90(3):259-63.
37. Amarasiri WA, Dissanayake AS. Coconut fats. Ceylon Med J. 2006 Jun;51(2):47-51.
38. Misra A, Khurana L, Isharwal S, Bhardwaj S. South Asian diets and insulin resistance.
Br J Nutr. 2009 Feb;101(4):465-73.
Chapter 10: General discussion 225
39. Hodge AM, English DR, O’Dea K, Giles GG. Glycemic Index and Dietary Fiber and the
Risk of Type 2 Diabetes. Diabetes Care. 2004 November 1, 2004;27(11):2701-6.
40. Meyer KA, Kushi LH, Jacobs DR, Slavin J, Sellers TA, Folsom AR. Carbohydrates,
dietary fiber, and incident type 2 diabetes in older women. The American Journal of Clinical
Nutrition. 2000 April 1, 2000;71(4):921-30.
41. Chandalia M, Garg A, Lutjohann D, von Bergmann K, Grundy SM, Brinkley LJ.
Beneficial Effects of High Dietary Fiber Intake in Patients with Type 2 Diabetes Mellitus. New
England Journal of Medicine. 2000;342(19):1392-8.
42. Jayawardena R, Ranasinghe P, Galappatthy P, Malkanthi R, Constantine G, Katulanda P.
Effects of zinc supplementation on diabetes mellitus: a systematic review and meta-analysis.
Diabetol Metab Syndr. 2012;4(1):13.
43. Song Y, He K, Levitan EB, Manson JE, Liu S. Effects of oral magnesium
supplementation on glycaemic control in Type 2 diabetes: a meta-analysis of randomized
double-blind controlled trials. Diabet Med. 2006 Oct;23(10):1050-6.
44. Pittas AG, Lau J, Hu FB, Dawson-Hughes B. The role of vitamin D and calcium in type
2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab. 2007
Jun;92(6):2017-29.
45. Harinarayan CV, Ramalakshmi T, Prasad UV, Sudhakar D, Srinivasarao PV, Sarma KV,
et al. High prevalence of low dietary calcium, high phytate consumption, and vitamin D
deficiency in healthy south Indians. Am J Clin Nutr. 2007 Apr;85(4):1062-7.
46. Shivane VK, Sarathi V, Bandgar T, Menon P, Shah NS. High prevalence of
hypovitaminosis D in young healthy adults from the western part of India. Postgrad Med J. 2011
Aug;87(1030):514-8.
47. Brown IJ, Tzoulaki I, Candeias V, Elliott P. Salt intakes around the world: implications
for public health. Int J Epidemiol. 2009 Jun;38(3):791-813.
48. Colditz GA, Manson JE, Stampfer MJ, Rosner B, Willett WC, Speizer FE. Diet and risk
of clinical diabetes in women. Am J Clin Nutr. 1992 May;55(5):1018-23.
49. Ford ES, Mokdad AH. Fruit and vegetable consumption and diabetes mellitus incidence
among U.S. adults. Prev Med. 2001 Jan;32(1):33-9.
50. Sargeant LA, Khaw KT, Bingham S, Day NE, Luben RN, Oakes S, et al. Fruit and
vegetable intake and population glycosylated haemoglobin levels: the EPIC-Norfolk Study. Eur
J Clin Nutr. 2001 May;55(5):342-8.
226 Chapter 10: General discussion
51. Esmaillzadeh A, Kimiagar M, Mehrabi Y, Azadbakht L, Hu FB, Willett WC. Fruit and
vegetable intakes, C-reactive protein, and the metabolic syndrome. Am J Clin Nutr. 2006
Dec;84(6):1489-97.
52. Van Duyn MA, Pivonka E. Overview of the health benefits of fruit and vegetable
consumption for the dietetics professional: selected literature. J Am Diet Assoc. 2000
Dec;100(12):1511-21.
53. Kanungsukkasem U, Ng N, Van Minh H, Razzaque A, Ashraf A, Juvekar S, et al. Fruit
and vegetable consumption in rural adults population in INDEPTH HDSS sites in Asia. Glob
Health Action. 2009;2.
54. Hall JN, Moore S, Harper SB, Lynch JW. Global variability in fruit and vegetable
consumption. Am J Prev Med. 2009 May;36(5):402-9 e5.
55. Aboobakur M, Latheef A, Mohamed AJ, Moosa S, Pandey RM, Krishnan A, et al.
Surveillance for non-communicable disease risk factors in Maldives: results from the first
STEPS survey in Male. Int J Public Health. 2010 Oct;55(5):489-96.
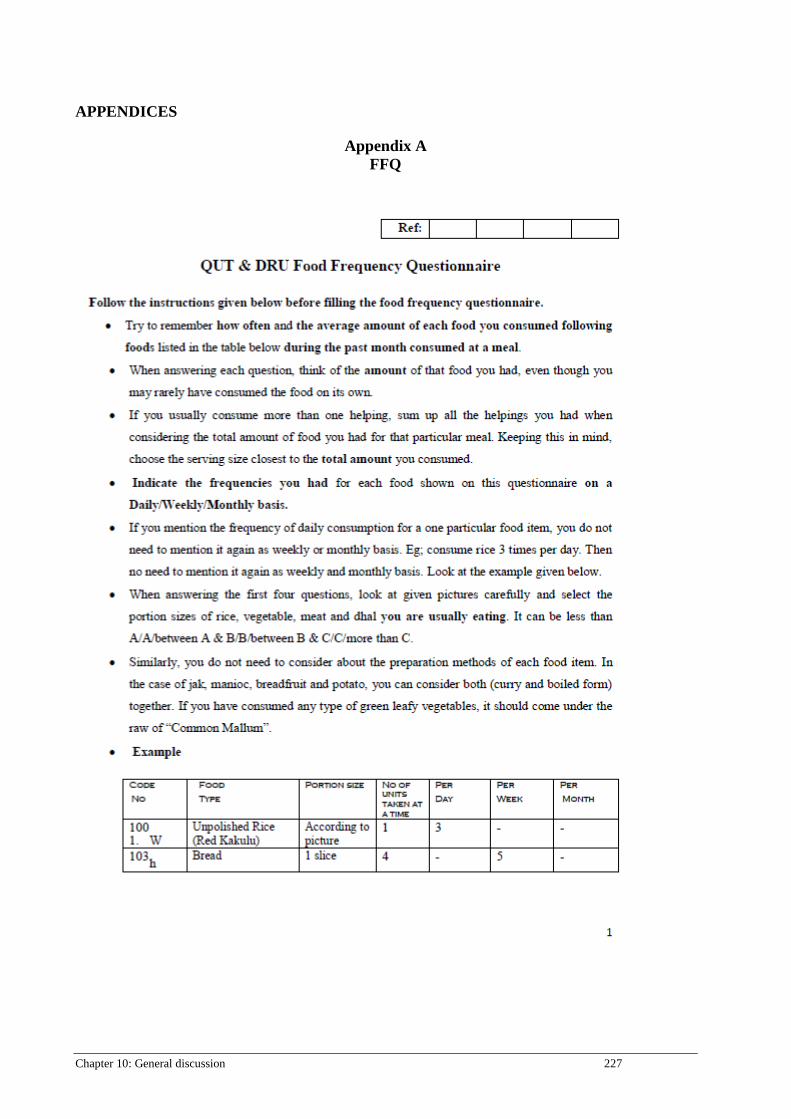
Chapter 10: General discussion 227
APPENDICES
Appendix A FFQ
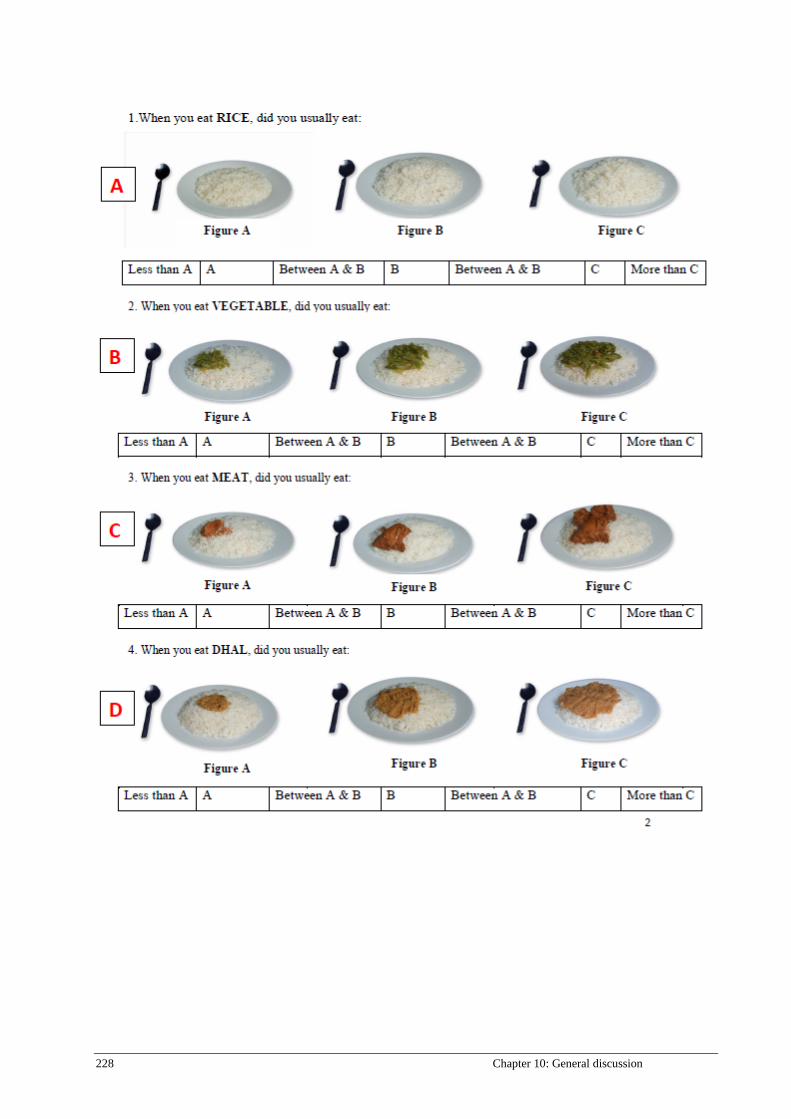
228 Chapter 10: General discussion
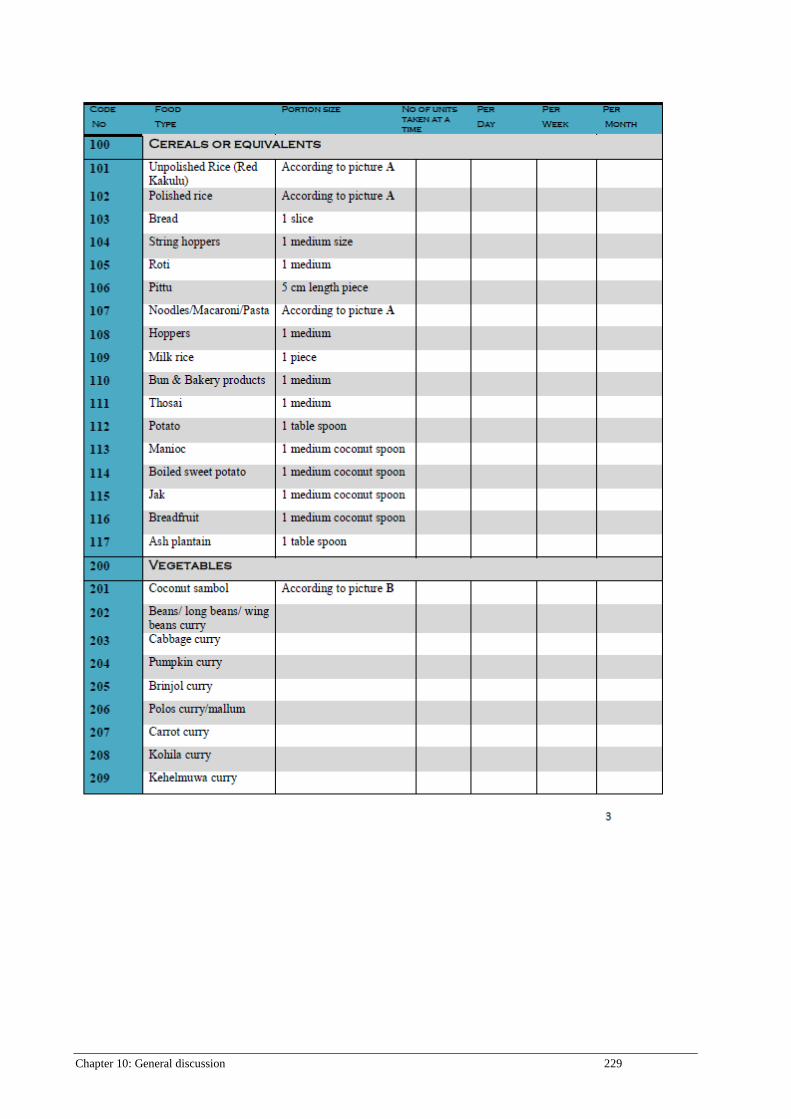
Chapter 10: General discussion 229
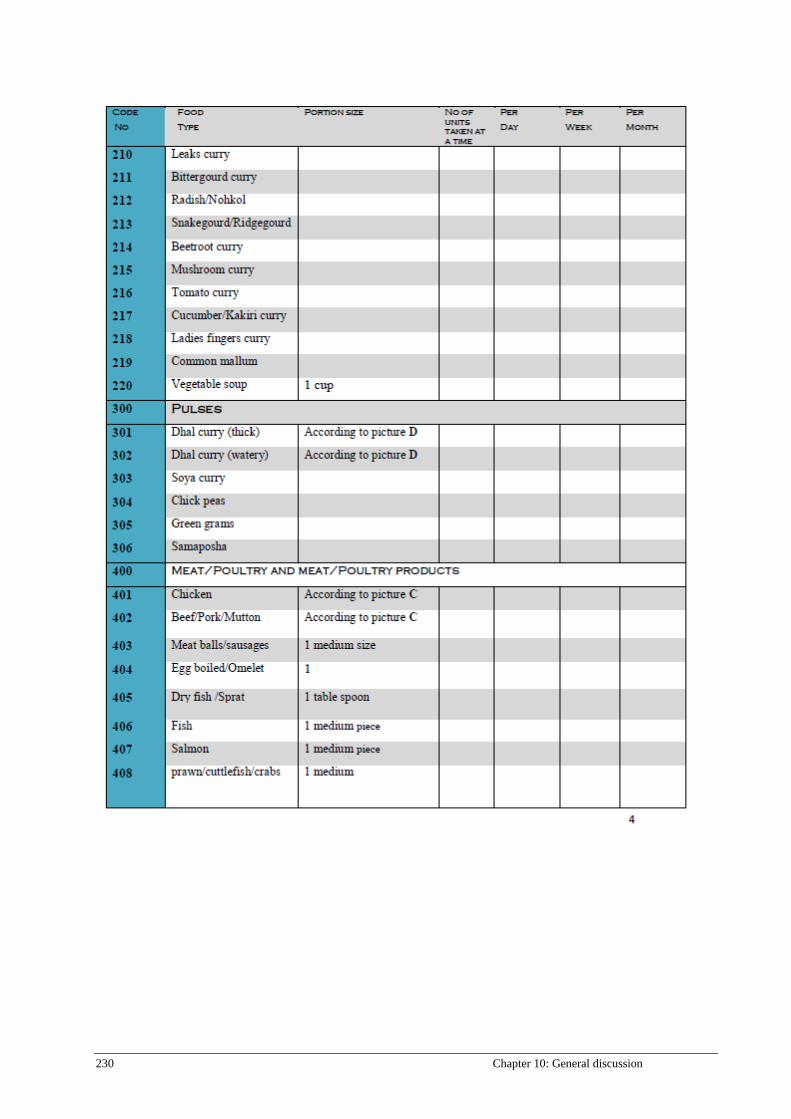
230 Chapter 10: General discussion
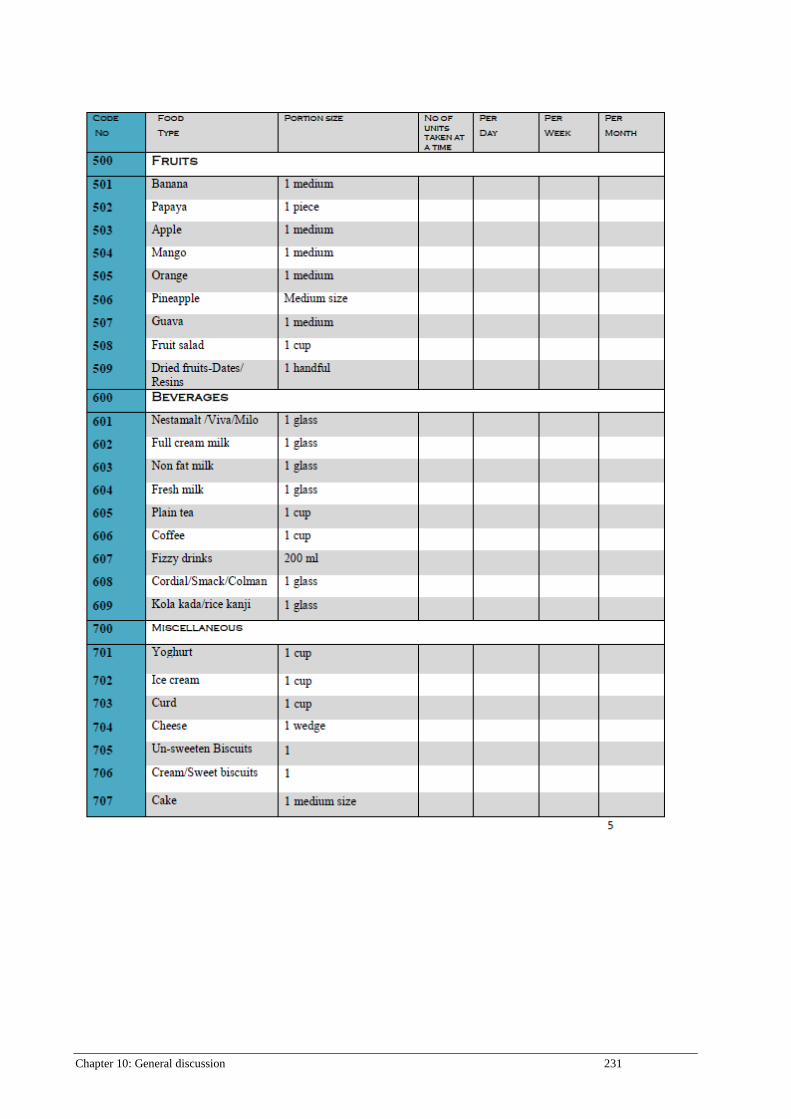
Chapter 10: General discussion 231
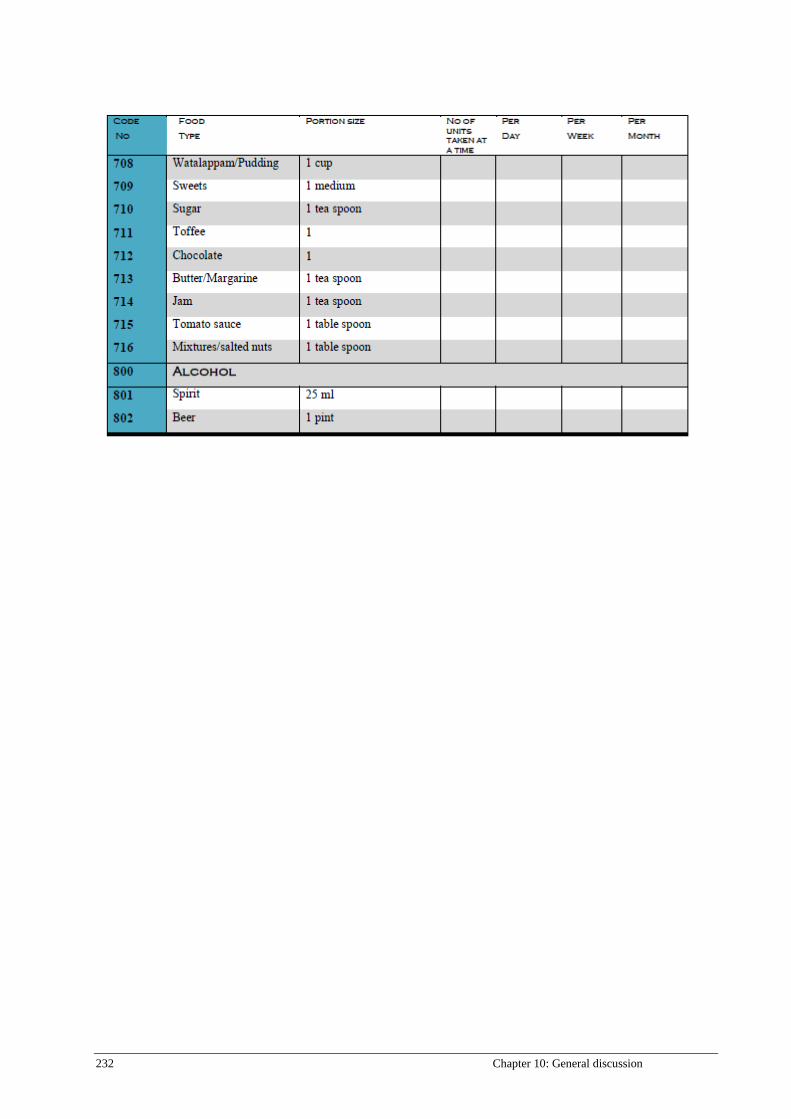
232 Chapter 10: General discussion























![[Guest Editor, Chandana Jayawardena.] Tourism and (BookFi.org)](https://img.pdfslide.net/doc/110x75/55cf8e8b550346703b933cde/guest-editor-chandana-jayawardena-tourism-and-bookfiorg.jpg)





