Embed Size (px)
Citation preview

Rapid and Continuous Magnetic Resonance
Imaging Using Compressed Sensing
by
Li Feng
A Dissertation Submitted in Partial Fulfillment
of The Requirements for The Degree of
Doctor of Philosophy
Department of Basic Medical Science
Program in Biomedical Imaging
New York University
May, 2015
____________________
Daniel K. Sodickson, MD, PhD
____________________
Ricardo Otazo, PhD

All rights reserved
INFORMATION TO ALL USERSThe quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a complete manuscriptand there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
Microform Edition © ProQuest LLC.All rights reserved. This work is protected against
unauthorized copying under Title 17, United States Code
ProQuest LLC.789 East Eisenhower Parkway
P.O. Box 1346Ann Arbor, MI 48106 - 1346
UMI 3716516
Published by ProQuest LLC (2015). Copyright in the Dissertation held by the Author.
UMI Number: 3716516

© Li Feng
All Rights Reserved, 2015

iii
DEDICATION
To my whole family, for their infinite love and support.

iv
ACKNOWLEDGMENTS
I started my MRI journey at NYU School of Medicine in May 2008
when I was a Master student. The past seven years that I spent here gave
me lots of memories and I owe my gratitude to many people who both
helped me in my studies and research and enriched my life in New York
City. The support, generosity and love from those people have made the
past many years a wonderful part of my life and will be deeply embedded in
my memory forever.
The first two people I would like to thank are Dr. Daniel Sodickson
and Dr. Ricardo Otazo. I am very grateful to have advising from both of
them in my PhD study. Dan’s enthusiasm for research and his passion in
both teaching and presentation are very impressive and encouraging to
inspire me throughout my whole PhD study. Dan gave me tremendous
freedom and kept encouraging me to actively think and test my own ideas
for research. He always gave me great feedback to guide my research
towards the direction that could solve practical problems. All of these
enabled me to grow rapidly and helped me develop good research
independence. Moreover, Dan welcomes any questions and critiques from
the students, and of course always gives excellent advices and answers
whenever we need. He is such a wonderful advisor and role model that all

v
the students can rely upon. On the other hand, Ricardo is really a wonderful
mentor who taught me lots of hands-on skills and helped me with all the
details in my research. My PhD study in the past many years would not
have been so productive without the support from Ricardo and it was such
a fabulous experience working with him. Ricardo was always available
whenever I needed his help. I could knock at his office door directly without
an appointment for discussions and he always welcomed me without any
hesitation. I enjoyed all the discussion with him, in which his critical thinking
and depth of knowledge were extremely helpful in my research. Meanwhile,
Ricardo is such an excellent presenter in giving a talk, and I have learnt a
lot from him in how to make good slides and how to tell a good story in a
presentation.
Dr. Daniel Kim deserves lots of my gratitude. Dan was my first
mentor in the MRI world and he is the person who brought me into this field
when I was still a Master student. I am so grateful and feel so lucky that he
accepted me as a summer intern in 2008 to work with him on a cardiac MRI
project. Dan taught me many things that all beginners need to learn,
including how to use the MRI scanners, how to perform a cardiac MRI
exam, how to efficiently debug a program and how to make good figures for
a paper. His patience and step-by-step guidance in my first MRI project
helped me grow up quickly from a “raw” novice and led to my first lead-

vi
author paper published in Magnetic Resonance in Medicine (MRM) and first
oral presentation acceptance at the 2009 Annual Meeting of the
International Society for Magnetic Resonance in Medicine (ISMRM), even
before I started the PhD study. Although he moved to Utah in the summer
of 2011 and it is hard to meet and talk to him now, I will never forget those
days that we worked together in his office and the scanner rooms in the
later evenings.
I would like to also thank Jian Xu from Siemens Healthcare USA for
his infinite support in both research and living. Jian was the first few people
I met when I came to the US in 2007. He was the first person I have known
in the MRI field and was the person who introduced me to NYU School of
Medicine. I enjoyed those countless weekends I spent with him in the MRI
scanner room. He taught me many things about sequences and cardiac
MRI, and gave me tremendous support in cardiac MRI sequences for my
research. I feel very lucky to be good friends with him.
I am grateful for Drs. Leon Axel and Hersh Chandarana, who gave
me clinical advising in my PhD study. They always pointed out practical
clinical needs for me and guided me to find good solutions for them. I also
appreciate their great support for clinical patient studies in both cardiac and
abdominal MRI.

vii
Special thanks go to Drs. Tobias Block and Florian Knoll from NYU,
Robert Grimm from University of Erlangen, and Dr. Jing Liu from UCSF. I
started working with Tobias in 2011 and I was happy that he joined NYU in
the end of 2011 and brought his radial imaging sequence here. My
dissertation could not have been finished without his support on radial
sequences. Meanwhile, I also learnt a lot from Tobias’ critical thinking and
attitude in research. Robert is Tobias’s PhD student and I enjoyed the time
we spent together here at NYU in 2012. His great effort led to successful
application of our compressed sensing approaches for clinical studies.
Florian shared his GPU implementation of 3D non-Cartesian gridding with
me and this was extremely helpful for the 3D radial imaging reconstructions
in my research. I was very lucky that I could be always the first person who
has access to his latest version of 3D non-Cartesian gridding code. Jing is
an expert in both cardiac imaging and radial imaging at UCSF. She gave
me lots of help, suggestions in both my research projects and career
planning.
We started the collaboration with Dr. Matthias Stuber’s research
group at the University of Lausanne in Switzerland in 2014. I am very
grateful to the whole team at Lausanne, including Dr. Matthias Stuber, Dr.
Davide Piccini, Simone Coppo, Gabriele Bonanno and many others, for the
opportunity to have this wonderful collaboration. Davide provided me with

viii
support for the 3D golden-angle spiral phyllotaxis sequence; Simone and
Gabriele were always willing to share so many coronary MRA datasets with
me without any hesitation and gave me great help with coronary artery MR
image post-processing. All of these valuable supports helped me finish the
last part of my dissertation very quickly. I believe our collaboration will
continue to be fruitful and can keep moving forward successfully in the
future.
I want to thank Dr. Ruth Lim for her help in the evaluation of MRI
image quality in many of my projects. Her response was always very fast,
and she gave me very helpful comments from a clinical point of view. I hope
we would have more opportunities in the future to work together on more
projects.
I would like to thank rest of my Committee members, including Dr.
Christopher Collins, Dr. Riccardo Lattanzi and Dr. Reza Nezafat. It is my
great honor to have Dr. Reza Nezafat from Beth Israel Deaconess Medical
Center at Harvard Medical School joins my Committee team as my external
dissertation reviewer.
In additional to the people who gave me direct support in research, I
need to express my gratitude to many lab mates and friends at NYU School
of Medicine, including Ding Xia, Cem Deniz, Leeor Alon, Gene Cho, Gang
Chen, Manushka Vaidya, Gillian Haemer, Alicia Yang, Nicole Wake,

ix
Gregory Lemberskiy Ke Zhang, Hong-Hsi Lee, Harikrishna Rallapalli and
Yuan Wang. These friends enriched my life in the lab and always gave me
great suggestions, help, positive energy and encouragement whenever I
needed them. I would like to specially thank Alicia, Nicole and Gillian, who
gave me great help in proofreading of the dissertation and language editing
in general. I also need to thank many friends in the Chinese Student and
Scholar Association (CSSA) of NYU Medical Center. I will never forget the
times we spent together for karaoke and poker games.
Finally, my greatest gratitude goes to my wife, my parents and all my
other family members. I would not have been able to finish my study without
their infinite support, encouragement and love.

x
ABSTRACT
Magnetic Resonance Imaging (MRI) is a powerful and multifaceted
imaging modality widely used for routine clinical practice. However, the
stringent constraints on MR imaging speed have resulted in comparatively
long examination times, and/or in limited spatial resolution, temporal
resolution and volumetric coverage. Meanwhile, slow image acquisitions
also lead to increased sensitivity to motion, particularly in abdominal and
cardiovascular exams, which require patient- or anatomy-specific scan
planning and reliable motion compensation strategies. The cost of these
complex and cumbersome imaging acquisitions is substantial “dead time”
between successive imaging protocols, as well as the potential discomfort
for patient during prolonged imaging examinations.
Rapid imaging approaches have the potential to shift the balance
from complex and tailored acquisitions to a continuous process that leads to
a simple and efficient imaging paradigm. Compressed sensing is such an
approach that can be applied to accelerate data acquisitions, and that could
further change the imaging paradigm in MRI. In this dissertation, novel
imaging techniques are developed using compressed sensing to enable
rapid and continuous MRI. In particular, golden-angle radial sampling is
combined with compressed sensing and parallel imaging to enable

xi
continuous data acquisitions. Moreover, a new use of sparsity to handle
physiological motion is also proposed for improved rapid and continuous
free-breathing MRI using compressed sensing ideas. The performance of
the proposed techniques is demonstrated for a wide range of clinical
applications in MRI.
The contributions presented in this dissertation enable rapid and
continuously updated image acquisitions, which eliminate “dead time” and
complex anatomy-specific scan planning, and which are also compatible
with flexible reconstructions that can be tailored retrospectively for various
clinical needs.

xii
TABLE OF CONTENTS
DEDICATION ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙iii
ACKNOWLEDGMENT ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙iv
ABSTRACT ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙x
LIST OF FIGURES ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙xix
LIST OF TABLES ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙xxxviii
1. Chapter1 ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙1
1.1. Overview and Motivation ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙1
1.2. Thesis Contributions and Outline ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙9
2. Background ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙12
2.1. MR Signal ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙12
2.1.1. NMR Phenomenon ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙12
2.1.2. Signal Excitation ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙14
2.1.3. Relaxation ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙16
2.2. Signal Localization ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙17
2.2.1. Slice Selection ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙19
2.2.2. Spatial Encoding and k-Space Formalism ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙19

xiii
2.3. MR Image Acquisition ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙21
2.4. Imaging Requirements ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙23
2.4.1. Field of View and Spatial Resolution ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙23
2.4.2. Signal to Noise Ratio ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙26
2.5. MR Image Reconstruction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙28
2.5.1. Generalized Image Reconstruction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙28
2.5.2. Reconstruction of Non-Cartesian k-Space Data ∙∙∙∙∙∙∙∙∙∙∙∙∙30
2.6. Parallel MRI ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙34
2.6.1. The Need for Speed in MRI ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙34
2.6.2. Spatial Encoding Using Coil Arrays ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙35
2.6.3. Generalized Parallel MRI Reconstruction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙36
2.6.4. Estimation of Coil Sensitivities ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙38
2.6.5. SNR in Parallel MRI ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙39
2.7. Compressed Sensing MRI ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙41
2.7.1. Introduction to Compressed Sensing ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙41
2.7.2. The Sensing Problem ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙43
2.7.3. Sparsity ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙45
2.7.4. Conditions for Sparse Signal Recovery ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙46

xiv
2.7.5. Sampling and Incoherence ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙47
2.7.6. Image Reconstruction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙51
2.7.7. Combination of Compressed Sensing and Parallel Imaging
∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙54
2.7.8. Low Rank Matrix Completion ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙57
2.8. Motion in MRI ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙59
2.8.1. Influence of Motion in MRI ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙59
2.8.2. Free-Breathing MRI Techniques ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙61
3. Accelerated T2 Measurement of the Heart Using k-t
SPARSE-SENSE ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙64
3.1. Prologue ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙64
3.2. Introduction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙65
3.3. Low Rank Property in MR T2 Mapping ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙67
3.4. Imaging Studies ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙70
3.4.1. k-Space Undersampling and Pulse Sequence ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙71
3.4.2. Phantom Validation ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙74
3.4.3. T2 Mapping of the Heart ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙74
3.4.4. Improving Sparsity Using Preconditioning RF Pulses ∙∙∙∙∙74

xv
3.5. Image Reconstruction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙77
3.6. Image Analysis and Statistics ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙77
3.7. Results ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙78
3.8. Discussion ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙84
3.9. Conclusion ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙86
4. Accelerated Real-Time Cardiac Cine MRI Using k-t
SPARSE-SENSE ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙88
4.1. Prologue ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙88
4.2. Introduction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙89
4.3. Imaging Strategies ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙91
4.3.1. k-Space Undersampling: Incoherence and Self-Calibration
of Coil Sensitivities ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙91
4.3.2. Comparison of Sparsifying Transforms ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙92
4.3.3. Comparison of Acceleration Rates ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙98
4.4. Imaging Studies ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙99
4.4.1. Pulse Sequence ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙99
4.4.2. Cardiac Imaging ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙99
4.5. Image Reconstruction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙102

xvi
4.6. Image Analysis and Statistics ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙103
4.7. Results ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙106
4.8. Discussion ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙110
4.9. Conclusion ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙115
5. GRASP: Golden-Angle Radial Sparse Parallel MRI ∙∙∙∙117
5.1. Prologue ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙117
5.2. Introduction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙116
5.3. Golden-Angle Radial Sampling ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙121
5.4. GRASP Reconstruction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙122
5.5. Reconstruction Implementation ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙123
5.6. Imaging Applications ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙126
5.7. Image Reconstruction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙129
5.8. Image Analysis and Statistics ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙130
5.9. Results ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙133
5.10. Discussion ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙139
5.11. Conclusion ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙144
6. XD-GRASP: Extra-Dimensional Golden-Angle Radial
Sparse Parallel MRI ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙146

xvii
6.1. Prologue ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙146
6.2. Introduction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙147
6.3. A Simple Example of XD-GRASP ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙152
6.4. Motion Estimation and Data Sorting ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙154
6.5. Image Reconstruction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙160
6.6. Imaging Applications ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙163
6.7. Results ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙170
6.8. Discussion ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙176
6.9. Conclusion ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙182
7. Towards Five-Dimensional Cardiac and Respiratory
Motion-Resolved Whole-Heart MRI Using XD-GRASP
∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙184
7.1. Prologue ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙184
7.2. Introduction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙186
7.3. 3D Phyllotaxis Golden-Angle Radial Sampling ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙188
7.4. Free-Breathing Whole-Heart MRI ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙190
7.4.1. ECG-Triggered Whole-Heart Coronary MRA ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙190
7.4.2. Free-Breathing Continuous Whole-Heart MRI ∙∙∙∙∙∙∙∙∙∙∙∙∙191

xviii
7.5. Motion Estimation ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙192
7.6. Data Sorting ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙194
7.7. Image Reconstruction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙195
7.8. Image Quality Comparison ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙198
7.9. Results ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙199
7.10. Discussion ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙203
7.11. Conclusion ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙207
8. Summary and Future Work ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙209
8.1. Chapter Summaries ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙210
8.2. An Outlook for the Future ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙214
9. List of Publications ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙219
9.1. Journal Papers ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙219
9.2. Conference Contributions ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙221
Bibliography ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙230

xix
LIST OF FIGURES
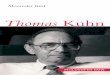
Figure 2.1. (a) Without a strong external magnetic field (B0), the spins are
randomly oriented and the total magnetic moments have a vector sum of
zero. (b) Alignment of spins either parallel or anti-parallel to the direction of
B0 when exposed to an external magnetic field. (c) A net magnetization
vector Mz (also known as M0) is generated as the vector sum of all the spin
angular momenta at the thermal equilibrium state. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙13
Figure 2.2. Excitation of the spins. Following the excitation, the excess z-
population is at least partially converted into a transverse magnetization
component (Mxy), and the ensemble of spins retain their relative alignment,
or phase coherence. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙16
Figure 2.3. Comparison of Cartesian sampling and radial sampling
schemes. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙22
Figure 2.4. In Cartesian, the sampling intervals (∆kx and ∆ky) must be
smaller than the reciprocal the object size in the corresponding spatial
dimensions in order to avoid aliasing. In radial sampling, the maximum
interval between two adjacent radial lines (∆d) has to be small than or equal
to ∆k in order to reconstruct an image without aliasing artifacts .
∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙24

xx
Figure 2.5. An example of multicoil brain images with corresponding coil
sensitivity maps with 8 coil elements. Each individual coil element has a
different spatially-varying sensitivity pattern. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙35
Figure 2.6. Sparse representation of a brain image in wavelet transform
domain. By keeping only the largest 10% coefficients and discarding the
rest, the image can still be recovered without loss of important information
but with 10-folder smaller size. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙44
Figure 2.7. A cardiac cine image series has temporal correlation because
dynamic region is limited in only a small region, while the background is
static. An FFT can be employed along the temporal dimension to sparsify
the dataset. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙46
Figure 2.8. Sampling matrix and the corresponding Gram matrix HA A . Ψ
is set as the identity matrix and Φ is the fully sampling Fourier matrix (a)
and partial Fourier matrices with regular (b) and random (c) undersampling
schemes. The off-diagonal entries in (c) are very small, suggesting that
random undersampling is good for compressed sensing∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙49
Figure 2.9. An example of one dimensional variable density undersampling
pattern and the corresponding incoherence, represented by the point
spread function (PSF) of the undersampling pattern. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙51

xxi
Figure. 2.10. Combination of compressed sensing and parallel imaging
enables reduced incoherent artifact level when compared with a single coil
model. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙54
Figure 3.1. Low rank property of T2 mapping. (a): An example of cardiac
T2 mapping image series, in which images at different echo times have
similar anatomical structures but with different T2-weighted contrast. (b):
The Casorati matrix generated from the image series. The Casorati matrix
can be represented by a few dominant singular values and the
corresponding singular vectors. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙68
Figure 3.2. Schematics details of estimating a PCA basis. By concatenating
each time signal vector along column direction, a matrix V is constructed. A
basis set for PCA is then estimated by conducting eigen-decomposition of
the covariance matrix C of V. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙69
Figure 3.3. (a): A simulated monoexponential decay curve. (b): FFT
representation of (a). (c): PCA representation of (a). These plots clearly
show that a monoexponential decay curve is sparser in PCA domain than in
FFT domain. To further validate this finding, a reference cardiac T2
mapping image series is displayed in both (d) FFT and (e) PCA domains.
The results were consistent with the ideal curves shown (a–c). ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙71

xxii
Figure 3.4. (a): Six-fold accelerated ky-t undersampling pattern with 16
dynamic frames. (b) Corresponding PSF in the sparse y-PCA space using
PCA as the sparsifying transform. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙72
Figure 3.5. Schematic diagram of the proposed accelerated T2 mapping
pulse sequence with preconditioning RF pulses. ECG triggering was used
to image at mid to late diastole, to image at a cardiac phase where there is
minimal cardiac motion. Three presaturation RF modules and a single fat
suppression module were applied before ME-FSE readout. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙75
Figure 3.6. (a): Representative short-axis scout image displaying positions
and thicknesses of three presaturation RF pulses (displayed as meshed-
strip lines). Resulting images with none (b), fat suppression (c), three
spatial presaturation RF pulses (d), and fat suppression plus three spatial
presaturation RF pulses (e). The combined use of fat suppression and
spatial presaturation RF pulses produced the best suppression of bright
signals unrelated to the heart. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙76
Figure 3.7. Representative T2 mapping images acquired using the
reference and accelerated T2 mapping pulse sequences: (top row)
GRAPPA and (bottom row) k-t FOCUSS. When compared with GRAPPA,
k-t FOCUSS consistently yielded higher spatial resolution in the phase-
encoding direction (1.7 x 1.7 mm2 vs. 1.7 x 4.2 mm2; accelerated vs.
reference, respectively). ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙80

xxiii
Figure 3.8. Zoomed cardiac T2 mapping images and the T2 maps
corresponding to Figure 3.7: (top row) GRAPPA and (bottom row) k-t
FOCUSS. When compared with GRAPPA image, k-t FOCUSS image
produced higher spatial resolution in the phase-encoding direction, as
shown by the intensity profiles of the muscle–blood border. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙81
Figure 3.9. Example cardiac T2 mapping image and the corresponding T2
maps with and without preconditioning RF pulses. For the latter case, note
the signal heterogeneity in the k-t FOCUSS reconstruction, particularly in
the lateral wall, as well as the corresponding T2 error. These results are
corroborated with zero-filled FFT reconstruction images which show more
residual aliasing artifacts for the latter case. The results clearly demonstrate
the usefulness of increasing sparsity in cardiac T2 mapping through the use
of preconditioning RF pulses. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙85
Figure 4.1. (a): Eight-fold accelerated ky–t sampling pattern varied along
time. (b): A schematic illustrating how the kx–ky–t sampling pattern is
averaged over time to produce the resulting kx–ky sampling pattern. This
kx–ky pattern represents the sampling used to perform self-calibration of
coil sensitivities. White lines represent acquired samples. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙92
Figure 4.2. Simulation results comparing the fully sampled reference
cardiac cine data to retrospectively eight -fold accelerated k– t
SPARSESENSE results with different sparsi fying transforms with

xxiv
regularization weight 0.01: temporal FFT, temporal PCA, and temporal TV.
(a): In the zoomed view of the heart, temporal TV yielded the lowest RMSE.
(b): In the chest wall, temporal FFT yielded the lowest RMSE. (c) and (d):
Corresponding plots of RMSE for the heart and chest wall regions,
respectively, as a function of regularization weight ranging from 0.005 to
0.05. These results show that temporal TV is superior to the other two
sparsifying transforms for the dynamic region, whereas temporal FFT is
superior to the other two transforms for the static region. Based on these
results, we elected to use temporal TV as the primary sparsifying transform
with regularization weight 0.01 and temporal FFT as the secondary
transform with regularization weight 0.001. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙94
Figure 4.3. Numerical simulation results comparing the (a) fully sampled
data (R = 1) to the retrospectively eight-fold undersampled reconstruction
results using four different sparsifying transforms: (b) temporal FFT, (c)
temporal PCA, (d) temporal TV, and (e) temporal TV + FFT. (First row) end-
systolic SAX image, (second row) spatial-temporal profile from the SAX
image, (third row) end-systolic LAX image, and (fourth row) spatial-temporal
profile from the LAX image. Both temporal FFT and temporal PCA yielded
more temporal blurring artifacts within the wall (arrows) than temporal TV
and temporal TV + FFT. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙96

xxv
Figure 4.4. Numerical simulation results (top row: end-diastolic images,
middle row: end-systolic images, bottom row: spatial-temporal plots through
the blood-myocardium boundary) comparing different R values using
temporal TV with weight 0.01 and temporal FFT with weight 0.001: (first
column) R = 1, (second column) R = 2, (third column) R = 4, (fourth column)
R = 6, (fifth column) R = 8, and (sixth column) R = 10. These results show
good results can be obtained up to R = 8. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙98
Figure 4.5. (a): Coil sensitivities calculated using an (left column) external
reference acquisition (pre-scan) and (right column) self-calibration method.
(b): The resulting k–t SPARSE-SENSE images using externally and self-
calibrated coil sensitivities. Note that two sets of data are very similar,
suggesting that our self-calibration of coil sensitivities was robust. ∙∙∙∙∙∙∙∙∙102
Figure 4.6. Schematic flowchart of the image reconstruction method. (a):
Coil sensitivity maps were self-calibrated by averaging undersampled k-
space data over time and computed using the adaptive array combination
method. (b): Multicoil, zero-filled k-space data, along with the corresponding
coil sensitivity maps, were reconstructed using both temporal TV and
temporal FFT as the sparsifying transforms, where regularization weight of
temporal TV is 10 times larger than that for temporal FFT. 104
Figure 4.7. (Rows 1–2) End-diastolic and (rows 3–4) end-systolic images at
multiple cardiac phases comparing (rows 1 and 3) breath-hold cine MRI and

xxvi
(rows 2 and 4) real-time cine MRI. Both image sets were acquired from a
29-year-old (male) healthy subject. Note that the breath-hold cine MR
images had higher spatial resolution than the real-time cine MR images (1.6
mm2 vs. 2.3 mm2, respectively). ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙106
Figure 4.8. Bland–Altman plots illustrating good agreement between
breath-hold cine MRI and real-time cine MRI for the following LV function
measurements: (top, left) EDV (mean difference = 15.2 mL [solid line];
lower and upper 95% limits of agreement = 27.6 and 2.8 mL [dashed lines],
respectively), (top, right) ESV (mean difference = 2.1 mL [solid line]; lower
and upper 95% limits of agreement = 4.7 and 8.9 mL [dashed lines],
respectively), (bottom, left) SV (mean difference = 17.3 mL [solid line]; lower
and upper 95% limits of agreement = 31.3 and 3.3 mL [dashed lines],
respectively), and (bottom, right) EF (mean difference = 5.7% [solid line];
lower and upper 95% limits of agreement = 11.3% and 0.1% [dashed lines],
respectively). ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙107
Figure 4.9. Proposed real-time cine MRI protocol with prospective ECG
triggering to capture true end diastole, where images are continuously
acquired through the second R-wave to visually identify true end diastole.
This proposed approach produced global function measurements in
excellent agreement with breath-hold cine MRI with retrospective ECG
gating. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙110

xxvii
Figure 4.10. Representative end-diastolic and end-systolic real-time cine
images: (top row) SAX view of a 26-year-old (female) patient and (bottom
row) LAX view of a 36-year-old (male) patient. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙111
Figure 5.1. (a) Continuous acquisition of radial lines with stack-of-stars
golden-angle scheme in GRASP. (b) Point spread function (PSF) of an
undersampled radial trajectory with 21 golden-angle spokes and 256
sampling points in each readout spoke for a single element coil (top) and for
a sensitivity-weighted combination of 8 RF coil elements (bottom). The
Nyquist sampling requirement is 256*π/2≈402. The standard deviation of
the PSF side lobes was used to quantify the power of the resulting
incoherent artifacts (pseudo-noise) and incoherence was computed using
the main-lobe to pseudo-noise ratio of the PSF. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙120
Figure 5.2. GRASP reconstruction pipeline. (a) Estimation of coil sensitivity
maps in the image domain, where the multicoil reference image (x-y-coil) is
given by the coil-by-coil NUFFT reconstruction of the composite k-space
data set that results from grouping all the acquired spokes. (b)
Reconstruction of the image time-series, where the continuously acquired
data are first re-sorted into undersampled dynamic time series by grouping
a number of consecutive spokes. The GRASP reconstruction algorithm is
then applied to the re-sorted multicoil radial data, using the NUFFT and the
coil sensitivities to produce the unaliased image time-series (x-y-t). ∙∙∙∙∙∙∙123

xxviii
Figure 5.3. Reconstruction of one representative partition from the contrast-
enhanced volumetric liver dataset acquired with golden-angle radial
sampling scheme using NUFFT (a) and GRASP with three different
weighting parameters (b-d) by grouping 21 consecutive spokes in each
temporal frame. Results with λ = M0*0.05 achieved an appropriate
compromise between image quality and temporal fidelity. This value was
therefore chosen for GRASP reconstruction with temporal resolutions of 21
spokes per frame. The weighting parameter was adjusted for different
temporal resolutions according to the level of incoherent aliasing artifacts or
pseudo-noise in the PSF. M0 was the maximal magnitude value of the
NUFFT images that were also used to initialize the GRASP reconstruction.
∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙132
Figure 5.4. Comparison of GRASP (top) reconstruction with coil-by-coil
compressed sensing (middle) and iterative SENSE (bottom) reconstructions
in the liver dataset with the same acceleration rate and temporal resolution
of 21 spokes/frame = 3 seconds/volume. GRASP showed superior image
quality compared to both coil-by-coil compressed sensing and iterative
SENSE reconstructions. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙134
Figure 5.5. (a) GRASP reconstruction of free-breathing contrast-enhanced
volumetric abdominal imaging of a 10-year old patient referred for tuberous
sclerosis. Representative images with three different temporal resolutions

xxix
are shown, including (top) 34 spokes/frame = 8 seconds/volume, (middle)
21 spokes/frame = 5 seconds/volume and (bottom) 13 spokes/frame = 3
seconds/volume. The reconstructed image matrix size was 256 x 256 in
each dynamic frame, with in-plane spatial resolution of 1 mm and the
weighting parameters of different temporal resolutions were adjusted
according to the acceleration rate. b) Signal-intensity time courses for the
aorta and portal vein, which do not show significant temporal blurring as
compared with the corresponding NUFFT results. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙136
Figure 5.6. (a) GRASP reconstruction of free-breathing contrast-enhanced
volumetric unilateral breast imaging in an adult patient referred for
fibroadenoma with fibrocystic changes. Temporal resolution is 21
spokes/frame = 3 seconds/volume. The reconstructed image matrix size is
256 x 256 for each dynamic frame, with in-plane spatial resolution of 1.1
mm. b) Signal-intensity time courses for the breast lesion, which is a
fibroadenoma with fibrocystic changes (white arrow), for the heart cavity
(white ROI), and for a blood vessel and breast tissue (white arrows),
showing no significant temporal blurring. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙137
Figure 5.7. (a) GRASP reconstruction of contrast-enhanced volumetric
neck imaging in an adult patient referred for neck mass and squamous cell
cancer. Temporal resolution is 21 spokes/frame = 7 seconds/volume. The
reconstructed image matrix size is 256 x 256 for each dynamic frame, with

xxx
in-plane spatial resolution of 1 mm. b) Signal-intensity time courses
evaluated for the carotid arteries show no significant temporal blurring.
∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙138
Figure 6.1. Schematic illustration of the XD-GRASP method: (a)
Continuously acquired radial k-space data are sorted into respiratory states
from expiration (top) to inspiration (bottom), using a respiratory motion
signal extracted directly from the data. Different colors indicate different
motion states. The number of spokes grouped in each motion state is the
same. (b) Approximately uniform coverage of k-space, with distinct
sampling patterns in each respiratory motion state, is achieved using the
golden-angle acquisition scheme. (c) Data sorting removes blurring and
clearly resolves respiratory motion, at the expense of introducing
undersampling artifacts. The purple dashed line shows the distinct
respiratory motion states after data sorting. (d) Sparsity is exploited along
the extra dimension to remove aliasing artifacts due to undersampling.
∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙151
Figure 6.2. Data sorting procedure for XD-GRASP in abdominal MRI
without contrast ejection. Respiratory motion was first sorted from end-
expiration to end-inspiration and the corresponding set of spokes were
evenly distributed into multiple respiratory states so that the number of
spokes is the same in each motion state. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙153

xxxi
Figure 6.3. XD-GRASP motion estimation and data sorting for cardiac cine
imaging. (a) 2D golden-angle radial trajectory. Motion signals are estimated
from the central k-space position of each radial line (gray dot). (b-c)
Estimation of cardiac and respiratory motion signals using information from
multiple coils. The signals with the highest peaks in the frequency range of
0.1-0.5Hz and 0.5-2.5Hz are automatically selected for respiratory and
cardiac motion signals, respectively. (d) Conventional GRASP sorting of
cardiac phases, given by grouping consecutive spokes in each frame. (e)
XD-GRASP sorting, in which all the cardiac cycles are concatenated into an
expanded dataset with one cardiac dimension (tC) and an extra respiratory
dimension (tR), so that sparsity along tC and tR can be exploited in the
multidimensional compressed sensing reconstruction. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙155
Figure 6.4. Selection of cardiac and respiratory motion signals from
multiple coils. (a) 2D golden-angle radial trajectory for free-breathing 2D
cardiac cine MRI and (b) estimation of cardiac and respiratory motion
signals using information from multiple coils. The motion signal in the coil-
element with the highest peak in the frequency range of 0.1-0.5Hz was
automatically selected to represent respiratory motion; and the motion
signal in the coil-element with the highest peak in the frequency range of
0.5-2.5Hz was automatically selected to represent cardiac motion. A

xxxii
filtering procedure can be performed on the detected motion signals for
denoising. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙156
Figure 6.5. XD-GRASP motion estimation and data sorting for DCE-MRI
imaging. (a) 3D stack-of-stars radial trajectory with golden-angle rotation,
where all spokes along kz for a given rotation angle are acquired before
rotating the sampling direction to the next angle. (b) A 1D Fourier transform
along the series of k-space central points of each slice is performed to
obtain a projection profile of the entire volume for each angle and all the
projection profiles from all coils are concatenated into a large two-
dimensional matrix, followed by principal component analysis (PCA) along
the z+coil dimension. (c-d) The principal component with the highest peak
in the frequency range of 0.1-0.5Hz is selected to represent respiratory
motion. (e-g) Contrast-enhancement effect is approximately removed by
estimating and subtracting the envelope of the composite signal. (h-i)
Processed respiratory motion signals are shown superimposed on the z-
projection profiles for normal breathing (left) and heavy breathing (right),
demonstrating reliable motion estimation. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙158
Figure 6.6. For DCE-MRI, the respiratory motion sorting procedure
described in Figure 6.2 is performed in each contrast-enhancement phase
separately. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙160

xxxiii
Figure 6.7. Conventional NUFFT reconstruction without respiratory sorting
(motion average) and XD-GRASP reconstruction with 6 respiratory states
for datasets acquired in transverse, coronal and sagittal orientations. XD-
GRASP significantly reduces motion-blurring, as indicated by the white
arrows. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙169
Figure 6.8. XD-GRASP reconstruction results for four representative
respiratory sparsity regularization parameters ( 2 ) in cardiac imaging and
liver DCE-MRI. Utilization of a sparsity constraint along the extra
respiratory-state dimension improved the removal of undersampling
artifacts, when compared with the non-regularized case ( 2 =0). Very low
values of 2 resulted in residual aliasing artifacts, while very high values of
2 introduced blurring. A 2
of 0.01 in cardiac cine imaging and 0.015 in
liver DCE-MRI provided a good tradeoff between residual aliasing artifacts
and temporal fidelity. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙171
Figure 6.9. Comparison of XD-GRASP against the standard breath-hold
approach used in routine clinical studies (i.e., with retrospective ECG-
gating) at end-diastolic and end-systolic cardiac phases in the volunteer
scan. XD-GRASP provided similar performance to the routine clinical
breath-hold method. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙172

xxxiv
Figure 6.10. (a) XD-GRASP provides access to respiratory motion
information for each cardiac phase, where respiratory-related motion of the
interventricular septum, especially at diastolic cardiac phases (top row) can
be seen, indicating left-right ventricular interaction during respiration. Gray
arrows indicate different respiratory motion states. (b) Comparison of XD-
GRASP reconstruction exploiting sparsity along two dynamic dimensions
(right-hand column) with GRASP reconstruction exploiting sparsity along a
single dynamic dimension only (left-hand column), using the same data set
acquired during free breathing. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙174
Figure 6.11. (a) Comparison of XD-GRASP and the standard breath-hold
approach with retrospective ECG-gating for the patients. Conventional
breath-hold scans achieved good image quality in a patient with normal
sinus rhythm, but it produced poor image quality for patients with
arrhythmia. XD-GRASP achieved consistent image quality by separating
the cardiac phases with arrhythmia. (b) In the patient with 2nd degree AV
block, the arrhythmic cardiac cycles were further sorted for a separate XD-
GRASP reconstruction to provide additional physiological information. (c)
Corresponding cardiac motion signals for three patients with varying length
of the cardiac cycle indicated by gray arrows. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙176
Figure 6.12. Comparison of GRASP with XD-GRASP in both aortic and
portal-venous enhancement phases in two representative partitions each

xxxv
from two volunteer datasets. XD-GRASP improved delineation of the liver
and vessels with enhanced vessel-tissue contrast. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙177
Figure 6.13. Comparison of GRASP with XD-GRASP in a total of five
representative partitions from two volunteers and one patient. Volunteer 4
was asked to breathe deeply. XD-GRASP achieved superior overall image
quality, with reduced motion-blurring. The white arrow indicates a
suspected liver tumor, which is better delineated in XD-GRASP. ∙∙∙∙∙∙∙∙∙∙∙∙179
Figure 6.14. Comparison of XD-GRASP reconstructions with different
number of respiratory motion states in abdominal DCE-MRI (end-expiratory
motion state only). 4 and 6 respiratory states achieved better resolved
respiratory motion than 2 states and 1 state. 6 respiratory states resulted in
slightly lower performance than 4 respiratory states. White arrows indicate
motional blurring for a choice of 1 motion state, and residual blurring for a
choice of 2 motion states. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙182
Figure 7.1. Comparison of golden-angle radial sampling schemes that are
based on stack-of-stars pattern (a) and spiral phyllotaxis pattern (b),
respectively. When compared with the stack-of-stars scheme, radial
sampling is also employed along the kz dimension in the 3D phyllotaxis
sampling trajectory, so that each k-space line passes through the center of
k-space and an image can be reconstructed with isotropic spatial resolution.
The 3D radial sampling pattern in (b) can be segmented into multiple

xxxvi
heartbeats for cardiac MRI, with golden-angle rotation along the z-axis
between every two successive data interleaves. An additional spoke
oriented along the superior-inferior (SI) direction (red lines) can be acquired
at the beginning of each data interleave for respiratory motion detection and
self-navigation. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙189
Figure 7.2. (a) Data sorting procedure in XD-GRASP reconstruction for
ECG-triggered whole-heart coronary MRA, in which the 3D golden-angle
radial k-space data are sorted into 4 respiratory motion states spanning
from expiration (top) to inspiration (bottom) (x-y-z-respiratory) using the
respiratory motion signals drived from the acquired data. The sorting
procedure is performed so that the number of spokes grouped in each
motion state is the same. Approximately uniform coverage of k-space with
distinct sampling patterns in each motion state can be achieved, as shown
in (b)&(c)∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙193
Figure 7.3. Five-dimensional data sorting in free running continuous whole-
heart imaging, with one cardiac motion dimension (20 cardiac phases) and
one respiratory motion-state dimension (4 respiratory states). ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙195
Figure 7.4. Comparison of XD-GRASP reconstruction (end-expiratory
motion states) with the 1D respiratory motion correction reconstruction in
two representative datasets. XD-GRASP improves the delineation of

xxxvii
coronary arteries and removes the blurring effects by resolving the
respiratory motion. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙200
Figure 7.5. End-expiratory myocardial wall (SAX and 4CH), proximal
coronary arteries, right coronary artery (RCA) and left anterior descending
coronary artery (LAD) in diastolic (top) and systolic (bottom) phases. All the
images are reformatted from a single continuous data acquisition with 5D
XD-GRASP reconstruction. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙201
Figure 7.6. 5D XD-GRASP reconstruction achieved reduced blurring,
improved sharpness and better visualization of myocardium and the RCA
compared with 4D reconstruction with respiratory motion correction (MC) in
one representative volunteer with irregular respiratory pattern. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙202

xxxviii
LIST OF TABLES
Table 3.1. Mean Segmental and Whole Myocardial T2 Measurements
Obtained Using GRAPPA and k-t SPARSE-SENSE Datasets. Not that
these values represent results analyzed by observer 1 and analysis 1.
∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙82
Table 3.2. Bland–Altman Statistics of T2 Measurements Obtained Using
GRAPPA and k-t SPARSE-SENSE Datasets. Note that these values
represent results analyzed by observer 1 and analysis 1. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙83
Table 3.3. Intraobserver and Interobserver Agreements for T2 Calculations
Based on Manual Segmentation of LV Contours. Intraobserver difference
was defined as T2 (analysis 1)-T2 (analysis 2), and interobserver difference
was defined as T2 (observer 1)-T2 (observer 2). ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙84
Table 4.1. Mean scores of image quality, temporal fidelity of wall motion
and artifact, produced by Breath-Hold cine MRI and Real-Time cine MRI.
∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙108
Table 4.2. Bland–Altman and CV analyses of four global function
measurements between Real-Time and Breath-Hold cine MRI pulse
sequences. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙109
Table 4.3. ICC analysis of interobserver variability of EDV, ESV, SV, and
EF within each pulse sequence type. ICC scale: 0-0.2 indicates poor

xxxix
agreement, 0.3-0.4 indicates fair agreement, 0.5-0.6 indicates moderate
agreement, 0.7-0.8 indicates strong agreement, and >0.8 indicates almost
perfect agreement. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙109
Table 5.1. Representative imaging parameters of dynamic volumetric MRI
in different applications. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙128
Table 5.2. Image quality assessment scores represent mean ± standard
deviation for each reconstruction category for different applications. ∙∙∙∙∙∙139
Table 7.1. Readers’ scores for comparison of 1D self-navigation motion
correction reconstruction v.s. XD-GRASP reconstruction (end-expiration
only) in visualization/sharpness of RCA, LAD and left main coronary artery.
0-4: non-diastolic to excellent. * Indicates statistical significance. LM: Left
Main Coronary Artery. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙203
Table 7.2. Readers’ scores for comparison of 1D self-navigation motion
correction reconstruction v.s. XD-GRASP reconstruction (end-expiration
only) in diastolic quality of RCA, LAD and left main coronary artery. 0 = not
visible, 1 = visible, and 2 = diagnostic. * Indicates statistical significance.
LM: Left Main Coronary Artery. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙204
Table 7.3. Reader’s scores for comparison of 4D reconstruction with motion
correction v.s. 5D XD-GRASP reconstruction (end-expiration only) in
visualization/sharpness of myocardium, the proximal segment of RCA, LAD

xl
and left main coronary artery. 1-5: non-diastolic to excellent. * Indicates
statistical significance. LM: Left Main Coronary Artery. ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙204

1
Chapter 1
Introduction
1.1. Overview and Motivation
Magnetic Resonance Imaging (MRI) is a multifaceted, non-invasive
and powerful imaging modality, with a broad range of applications in both
clinical diagnosis and basic scientific research. Comparing to other medical
imaging modalities, MRI does not use ionizing radiation and provides
superior soft-tissue characterization with high resolution and flexible image
contrast parameters. Moreover, MRI allows good visualization of anatomical
structure, physiological function, blood flow, and metabolic information,
making it compelling in a variety of clinical applications.
MRI is based on the phenomenon of nuclear magnetic resonance
(NMR) that was discovered in the 1940s (1,2) and has been applied in a
variety of research experiments in chemistry, biology, physics and medicine.

2
In a simple NMR experiment, the signal is generated by applying a resonant
radiofrequency (RF) pulse to excite the spin of the atomic nucleus in an
object that is placed inside a strong static magnetic field (B0). Following the
excitation, the object being studied emits a decaying RF signal that can be
detected in the form of radiofrequency voltage in a receiver coil. In order to
distinguish the received signals from different spatial positions, additional
magnetic field gradients are superimposed on the main magnetic field, so
that the field strength varies linearly with spatial position, allowing the exact
origins of NMR signal emitted from the object to be localized (3). Based
upon the idea of gradient encoding, Fourier imaging was proposed (4), in
which measurements representing the spatial frequency of the object,
termed k-space, can be acquired using a specific trajectory (5,6). The most
common acquisition scheme is Cartesian sampling, where k-space points
are acquired on a uniform rectangular grid and image reconstruction is
performed in a robust and efficient fashion by applying an inverse Fast
Fourier Transform (FFT).
Fourier imaging led to revolutionary progress in MRI and formed the
basis of most variants of MRI techniques that are used today. However, the
major limitation of Fourier imaging is the relatively slow data acquisition
process, in which only one k-space position can be encoded per unit time
and this process has to be sequentially repeated until the entire k-space

3
region for the target spatial resolution is covered. Low imaging speed
increases patient discomfort and imposes strict limits in spatiotemporal
resolution and volumetric coverage. Meanwhile, in order to make the best
use of precious scan time, data acquisitions are often planned in oblique
image planes adjusted to the target anatomy, which results in complex and
cumbersome scan planning and also requires extensive training for scan
operators. Furthermore, because of the wide range of contrasts that MR is
capable of producing, the acquisition planning is often repeated multiple
times for different imaging sequences and protocols, which results in
substantial “dead time” between successive data acquisitions. The exam
workflow is even more complicated and tedious in the imaging of moving
organs, such as liver, kidney or heart. For example, in a typical cardiac MRI
exam, the data acquisition has to be synchronized with the contraction of
the heart and is usually performed during multiple breath-holds in order to
avoid respiratory-motion induced artifacts (7). Since breath-hold capabilities
are subject dependent and can be significantly limited in patients, repeated
data acquisitions are often required in the case of failed breath-holds, or in
the presence of different types of arrhythmias, which further increase
patient discomfort and prolong the examination times, making MRI more
challenging in some applications such as cardiac imaging or abdominal
imaging.

4
Rapid imaging approaches can help shift the balance from complex
tailored acquisitions to a simple and continuous acquisition paradigm in MRI.
Since the introduction of MRI, researchers have devoted tremendous effort
to the acceleration of MR scans, and the speed with which data can be
acquired has already increased dramatically with a combination of
advances in MR hardware and innovations in imaging techniques. For
example, fast switching magnetic field gradients have allowed the intervals
between data collections to be reduced substantially. The invention of fast
imaging strategies, such as Echo-Planar Imaging (EPI) (8), Fast Spin-Echo
(FSE) imaging (9), Fast Low Angle SHot (FLASH) imaging (10), balanced
Steady-State Free Precession (bSSFP) imaging (11), and spiral imaging
sequences (12,13) all significantly increased imaging efficiency. However,
the nature of sequential data acquisition in conventional Fourier imaging still
limits achievable imaging speed.
An alternative approach to increase imaging speed in MRI is to
reduce the quantities of phase-encoding measurements while maintaining
the target resolution. The idea of partial Fourier imaging was proposed in
the 1980s and early 1990s for accelerated MRI exams, in which the
conjugate symmetry of k-space is exploited to reduce scan times by
acquiring approximately half of the k-space data (14-16). Although partial
Fourier imaging is still used in clinical exams today, the maximum

5
acceleration factor that can be achieved is only close to two. Beginning in
the late 1990s, a variety of parallel imaging techniques, such as
Simultaneous Acquisition of Spatial Harmonics (SMASH) (17), Sensitivity
Encoding (SENSE) (18), and Generalized Autocalibrating Partially Parallel
Acquisition (GRAPPA) (19), were proposed to accelerate the data
acquisition in MRI using an array of receive coils with spatially-varying
sensitivities. The knowledge of coil sensitivities, which is usually estimated
using additional reference data, can be employed to perform some portion
of spatial encoding that is normally accomplished via gradients, thus
enabling reconstruction of an image without aliasing from only a subset of
k-space data (20). Temporal parallel imaging techniques, such as TSENSE
(21) or TGRAPPA (22), further eliminate the need to acquire extra
reference data for coil sensitivity calibration in dynamic imaging exams,
estimating the coil sensitivities by combining different temporal frames
acquired with shifted lattice undersampling patterns, under the assumption
that the sensitivity maps are smooth and do not change significantly over
time. However, the acceleration in parallel imaging is fundamentally limited
by noise amplification in the reconstruction (also known as g-factor), which
increases non-linearly with increasing acceleration factor (18,20). The
presence of extensive spatial and temporal correlations in dynamic MRI can
be also exploited to accelerate data acquisition, and these methods are

6
usually combined with parallel imaging for better performance. For example,
k-t acceleration methods, such as k-t BLAST/k-t SENSE (23), k-t GRAPPA
(24) and k-t PCA (25), are based on the fact that the representation of
dynamic images in the combined spatial and temporal Fourier domain (x-f
space) is typically sparse, which reduces the signal overlap in x-f space due
to regular k-t undersampling and thus enables higher accelerations. K-t
techniques represented the first attempt to exploit compressibility or
sparsity to reconstruct undersampled data. However, one potential
drawback of k-t techniques is the need to explicitly compute the signal
distribution in x-f space, which is usually performed by acquiring a low
spatial resolution reference image. Therefore, it can be challenging to
recover some detailed features using k-t techniques, and their use may
introduce residual aliasing artifacts at edges.
The idea of compressed sensing (26,27), proposed in the 2000s,
represents another powerful approach for increasing imaging speed in MRI
by exploiting the compressibility or sparsity of an image (28). Since its
introduction, compressed sensing has already generated great excitement
and enabled significant advances in coding and information theory.
According to the Nyquist theorem, the sampling rate in a conventional
sampling scheme must be at least twice the maximum bandwidth presented
in the signal. Unfortunately, in many applications, Nyquist sampling is time-

7
consuming and data-intensive, posing a challenge for sampling system
design, data storage and transmission. In order to address this logistical
and computational challenge, high-dimensional data are often compressed
after acquisition by transforming to a basis that provides a sparse or
compressible representation for the signal, and discarding insignificant
components. This transform coding framework has been widely used in the
JPEG, JPEG2000 and MPEG image/video compression standards. The
ability to compress images so effectively raises an interesting question, one
which underlies compressed sensing: instead of first sampling a signal at a
high sampling rate and then discarding most of the sampled measurements
in the compression process, why not directly acquire the data in a
compressed form at a lower sampling rate? In other words, can we build the
compression process directly into the acquisition or sensing step, so that
one does not have to perform so many measurements only to discard most
of them afterwards? Candes, Romberg, Tao and Donoho proved the
feasibility of this hypothesis (26,27) and proposed the compressed sensing
framework by which a sparse or compressible signal could be successfully
recovered from undersampled measurements that are far below the Nyquist
limit (26,27).
After rapid development in the past decade, compressed sensing
has already achieved notable impact in a wide range of application areas,

8
including medical imaging, sensor design in high-resolution cameras,
geophysical data analysis, computational biology, radar analysis and many
others. One of the applications that can substantially benefit from
compressed sensing is MRI, in which the imaging speed can be
dramatically improved by reconstructing the sparse representation of an
image from undersampled measurements without loss of important
information (28). Meanwhile, since multicoil data acquisition is widely used
in MRI nowadays, compressed sensing can be combined with parallel
imaging to further increase imaging speed and improve reconstruction
performance exploiting the idea of joint multicoil sparsity (29-31). These two
reconstruction approaches can be synergistically combined, because image
sparsity and coil sensitivity encoding are complementary sources of
information. On one hand, compressed sensing can serve as a regularizer
for the inverse problem in parallel imaging, and can thus prevent heavy
noise amplification due to high accelerations. On the other hand, parallel
imaging can reduce the level of incoherent aliasing artifact in compressed
sensing, by exploiting joint sparsity in sensitivity-weighted combinations of
multicoil images (30).
Remarkable advances in rapid MRI have been achieved over the last
two decades, improving the performance of existing techniques and
enabling new imaging methods that were not feasible before due to limited

9
imaging speed. However, the paradigm of routine clinical imaging still
remains complex, given the rich diversity of acquisition choices and the
adjustments needed to reduce the influence of unwanted effects, such as
respiratory motion, cardiac motion, relaxation effects, and others. Therefore,
it is desirable to shift the day-to-day clinical workflow from time-consuming,
inefficient, and tailored acquisitions to rapid, continuous and comprehensive
acquisitions with user-defined reconstructions adapted retrospectively for
different clinical needs. The combination of compressed sensing and
parallel imaging has the potential to enable such an efficient imaging
paradigm. The overall goal of this dissertation is to develop novel imaging
techniques that support simple and efficient MRI protocols, and begin to
enable a rapid continuous data acquisition paradigm for clinical and
research MRI exams.
1.2. Thesis Contributions and Outline
Chapter 1 (current chapter) gives an introductory overview and
motivation for this dissertation.
Chapter 2 presents a brief overview of fundamental principles of
MRI, parallel MRI and compressed sensing.
Chapter 3 and Chapter 4 present highly-accelerated MR parameter
(T2) mapping and real-time cardiac cine MRI using k-t SPARSE-SENSE,
which is a framework combining compressed sensing and parallel imaging

10
using Cartesian k-space sampling. The purpose and contribution of these
two chapters are to demonstrate the performance of k-t SPARSE-SENSE
for different clinical applications and also compare the performance of
different sparsifying transforms that can be used in the subsequent
chapters.
Chapter 5 presents a highly-accelerated dynamic imaging technique
called Golden-angle RAdial Sparse Parallel MRI (GRASP), which
synergistically combines compressed sensing and parallel imaging
reconstruction with golden-angle radial sampling. Golden-angle radial
sampling provides a continuous data acquisition scheme that is robust to
motion and well-suited for compressed sensing acceleration. GRASP
represents a promising imaging paradigm for clinical workflow, based on
rapid continuous data acquisition with flexible spatiotemporal resolution
tailored retrospectively to different clinical needs. The performance of
GRASP is demonstrated in a wide range of clinical applications, including
dynamic contrast-enhanced imaging of the liver, kidney, breast, neck,
prostate, etc.
Chapter 6 presents a novel framework for free-breathing MRI called
eXtral-Dimensional Golden-angle RAdial Sparse Parallel MRI (XD-GRASP),
which uses the same continuous data acquisition as GRASP, but
reconstructs additional motion dimensions using compressed sensing.

11
Instead of explicitly removing or correcting for motion, XD-GRASP takes a
different approach to handling various types of periodic motion by sorting
and reconstructing the acquired data with multiple resolved motion states.
Besides motion compensation, XD-GRASP also provides access to new
physiological information that could be of potential clinical value.
Chapter 7 presents an extension of XD-GRASP to 3D golden-angle
radial sampling based on the spiral phyllotaxis sampling pattern. 3D radial
sampling not only enables volumetric isotropic spatial coverage, but also
provides increased motion robustness and allows exploitation of
incoherence along all spatial dimensions. The performance of the technique
is first demonstrated for free-breathing ECG-triggered whole-heart coronary
MR angiography (MRA) with improved motion compensation. It is then
applied for continuous five-dimensional cardiac and respiratory motion-
resolved whole-heart MRI that enables simultaneous assessment of
myocardial function in arbitrary planes and visualization of whole-heart
arterial anatomy (including aorta and coronary arteries, etc).
Chapter 8 summarizes the contributions presented in this
dissertation and discusses an outlook for the future.
Chapter 9 is a list of publications.

12
Chapter 2
Background
This chapter presents a brief overview of basic principles of MRI,
parallel imaging and compressed sensing. The discussion is focused on the
aspects that are relevant to the subsequent chapters of the dissertation.
2.1. MRI Signal
2.1.1. NMR Phenomenon
The physical phenomenon behind MRI is nuclear magnetic
resonance (NMR), which was first discovered in the 1940s (1,2). An atomic
nucleus with an odd number of protons possesses an angular momentum J
called spin, which generates a tiny magnetic moment μ . The magnetic
moment is directly proportional to the angular moment as
γμ J (2.1)

13
Figure. 2.1: (a) Without a strong external magnetic field (B0), the spins are randomly oriented and the total magnetic moments have a vector sum of zero. (b) Alignment of spins either parallel or anti-parallel to the direction of B0 when exposed to an external magnetic field. (c) A net magnetization vector Mz (also known as M0) is generated as the vector sum of all the spin angular momenta at the thermal equilibrium state.
Here γ is a constant called the gyromagnetic ratio. The proton in hydrogen
(1H) is particularly interesting because it is abundant in water and other
molecules in the human body. At room temperature and without a strong
external magnetic field (B0), the spins are randomly oriented and their
magnetic moments have a vector sum of zero, as shown in Figure 2.1a.
When the spins are placed in a strong external magnetic field, they
align themselves with B0, as shown in Figure 2.1b. In fact, in the so-called
thermal equilibrium state, proton spins are divided among two populations,
one population (n+) oriented parallel and the other (n-) oriented anti-parallel
to B0. (In general, at thermal equilibrium, spins populate their quantized
energy states according to a Boltzmann distribution; for spin-1/2 species

14
such as 1H, there are two such states corresponding to oppositely oriented
angular momenta.) The n+ spin population is at a relatively lower energy
state and thus has a slightly larger number of spins than the n- spin
population. This results in a net magnetization vector 0M , which is the
vector sum of all the spin angular momenta and is aligned in the direction of
B0, known as the z direction or longitudinal direction, as shown in Figure
2.1c. The magnitude of 0M can be calculated as
2 2
0
04
h B NM
KT
(2.2)
Here h is Planck’s constant, K is the Boltzmann’s constant and T is the
absolute temperature. Equation 2.2 suggests that the net magnetization
that can be measured in MRI is proportional to the magnetic field B0.
When spins are perturbed away from the axis of the applied B0 field,
they precess around the direction of B0 at a frequency that is proportional to
the strength of B0, as given by the Larmor equation
γ 0ω B (2.3)
Now let us consider how such perturbations are accomplished.
2.1.2. Signal Excitation
In order to generate MR signal that can be measured by a detector,
the net magnetization 0M needs to be tipped towards the direction

15
perpendicular to B0, which is known as the x-y plane or transverse plane.
This process is known as “excitation” and is achieved by applying a
radiofrequency (RF) pulse that creates a magnetic field (B1) perpendicular
to B0 and rotating at the Larmor frequency. The RF pulse causes 0M to
move away from the z direction into the transverse plane until the pulse is
switched off. The nutation angle through which 0M moves, or the “flip angle”
of the pulse, is given by
1
0( )
T
B t dtt (2.4)
Here B1 is the strength of the RF magnetic field and T is the duration of the
pulse. Following the excitation, the excess z-population 0M is at least
partially converted into a transverse magnetization component ( xyM ), as
shown in Figure 2.2, and the ensemble of spins retain their relative
alignment, or phase coherence. The precession of xyM generates an
oscillating magnetic field, and the changing magnetic flux associated with
this field can then induce a voltage in a suitably configured receive coil. This
voltage constitutes the MR signal, which can subsequently be demodulated
or manipulated otherwise as desired.

16
Figure. 2.2: Following the excitation, the excess z-population is at least partially converted into a transverse magnetization component (Mxy), and the ensemble of spins retain their relative alignment, or phase coherence.
2.1.3. Relaxation
After the RF pulse is switched off, the precessing spins gradually
lose their coherence and return to the z-directed equilibrium state, in
processes known collectively as relaxation. The loss of spin coherence
results from differences in local field strength and precession frequency, or
else from other interactions between spins and their environment, and it is
characterized by a time constant T2. The return to longitudinal equilibrium is
associated with loss of the energy the spins absorbed from the RF pulse,
and is characterized by a time constant T1.
These two relaxation mechanisms, together with the behavior of the
magnetization vector when exposed to an external magnetic field, can be
described by the Bloch equation:

17
0
2 1
( )γ
i j kMM B
x y zM M M Md
dt T T
(2.5)
Here ( )M x y zM ,M ,M , and i , j , and k are unit vectors along x, y, and z
directions respectively. The cross-product term describes the precession
behavior and the relaxation terms describe the exponential behavior of
transverse dephasing and longitudinal recovery. For a flip angle of 90o, the
solution to Equation 2.5 is given by
1
2 0
-t /Tz 0
-iω t-t /Txy 0
M (t)= M (1- e )
M (t)= M e e (2.6)
2.2. Signal Localization
In a hypothetical uniform-sensitivity receiver coil, the MR signal
following an RF pulse contains contributions from all the transverse
magnetization within the entire volume of interest (VOI). This signal can be
expressed as
( )
( ) ( ) ( ) 02 -i t-t /T
vol volS t = M ,t dr= M e e dr
rr r
(2.7)
Here M is the object to be imaged and r is a vector indicating spatial
position. For the purposes of simplicity, the transverse relaxation term
exp( )2-t /T may be ignored for the time being, and the exp( )0-i t term
can be also removed via demodulation in the process of signal detection.

18
Therefore, the MR signal that is detected immediately after RF excitation
can be simplified as
( )vol
S = M drr (2.8)
Equation 2.8 suggests that the detected signal arises from the entire
sample volume and thus the spatial information in the acquired signal
cannot be differentiated. In order to obtain the spatial positions of the signal,
additional magnetic field gradients must be used to generate spatially
varying longitudinal field strength (3).
In general, the field gradients applied in MRI are time-varying and
can be expressed as a vector:
( ) ( ) ( ) ( )G i j kx y z
t G t G t G t (2.9)
Thus, the total magnetic field with all three gradients turned on is
0( ) ( )B r, G rt B t (2.10)
where r is the spatial position in the sample. Since the magnetic field now
varies as a function of position, spins at different positions have different
precession frequencies, with the differences given by
( ) γr G r (2.11)
Therefore, when gradients are turned on, Equation 2.8 can be expressed as
γ( ) ( ) exp( γ ( ) )
ti t
vol volS = M e dr M i d drG r
0r r G r (2.12)

19
where t is the duration of the applied gradients. The orientation of the
gradient fields is parallel to B0 and thus the Larmor frequency, which is
proportional to the field strength, becomes dependent on signal location.
2.2.1. Slice Selection
An RF pulse is usually designed at the resonance condition, with a
bandwidth centered at the Larmor frequency. Thus, without the presence of
gradients, the RF pulse excites all the spins in the object being imaged
since they are all rotating at the same frequency. In order to excite a slice in
2D MR imaging, a slice-selective gradient ( zG ) needs to be first imposed
along an axis perpendicular to the imaging slice to be excited, so that the
Larmor frequency of the spins varies along that axis. Besides, a specially
tailored RF pulse needs to be applied simultaneously with the gradient, with
its frequency bandwidth matching the range of frequencies contained in the
desired slice. This slice-selective excitation ensures that only spins within a
slice or slab of interest can be excited, while leaving other spins
unperturbed. Accordingly, the relationship between slice thickness and RF
bandwidth or gradient strength can be given by
RF bandwidth
slice thisknesszG
(2.13)
2.2.2. Spatial Encoding and k-Space Formalism

20
Following slice selection, the in-plane spatial information now can be
further encoded with two additional gradients, known as frequency-
encoding and phase-encoding gradients.
In 2D imaging, the received MRI signal in Equation 2.12 can be
described as
0
γ( ) ( , )exp( ( ) )t
x ys t m x y i d dxdy G r (2.14)
Here ( )m x,y represents the spin density in the 2D object to be imaged.
Considering only the x and y gradient fields ( )xG t and ( )yG t , Equation 2.14
becomes
0 0( ) ( , )exp γ ( ) exp γ ( )
t t
x yx y
s t m x y i G d x i G d y dxdy (2.15)
Setting
0
0
γ( ) ( )
2
γ( ) ( )
2
t
x x
t
y y
k t G d
k t G d
(2.16)
Equations 2.15 can be rewritten as
2 [ ( ) ( ) ]
( , ) ( , )x y
x yx y
i k t x k t ys k k m x y e dxdy
(2.17)
Here xk and yk are the spatial-frequency variables in a two-dimensional
space that is known as k-space. Equation 2.17 is usually referred as the
signal equation, which suggests that the MRI signal represents the spatial

21
Fourier transform of the object being imaged. The signal equation can be
extended into three dimensions as
2 [ ( ) ( ) ( ) ]
( , , ) ( )x y
x y zx y z
zi k t x k t y k t zs k k k m x,y,z e dxdydz
(2.18)
Here additional phase-encoding is employed along the partition dimension.
2.3. MR Image Acquisition
It can be seen from Equation 2.15 that the position in k-space at a
given time t depends on the area of the gradient waveform at that time
point. Therefore, theoretically an MR image can be acquired by traversing
k-space using any trajectory designed by altering the gradients in an
appropriate way according to Equation 2.16. A variety of sampling
trajectories (i.e., Cartesian, radial, spiral, and many other variants) have
been proposed since the introduction of MRI.
In Cartesian sampling, k-space data is acquired in a sequential line-
by-line fashion on a Cartesian grid until sufficient data are acquired to form
an image, as shown in Figure 2.3a.
Instead of sampling parallel lines, k-space data can be also acquired
in a radial scheme, as shown in Figure 2.3b, where each radial line is
acquired with a combination of gradients in both x and y directions. This
combination can be altered to enable rotated sampling of k-space lines at
different angles according to

22
Figure. 2.3: Comparison of Cartesian sampling and radial sampling schemes.
0
0
cos( )
sin( )
x
y
G G
G G
(2.19)
Here is the acquisition angle of a given radial line and 0G denotes the
gradient amplitude needed to sample the central k-space line.
It is straightforward to extend two-dimensional acquisitions, including
both Cartesian and radial sampling, into three dimensions by adding an
additional phase-encoding step along the slice dimension. In particular,
radial and Cartesian sampling can be combined in a hybrid three-
dimensional acquisition scheme known as stack-of-stars sampling, where
radial sampling is employed in the kx-ky plane and Cartesian sampling is

23
employed along the kz dimension. Alternatively, radial sampling can be also
employed in all three dimensions, with isotropic volumetric coverage.
The distinct acquisition geometry in radial sampling offers some
unique imaging properties, such as higher inherent incoherence, improved
robustness to motion, self-navigation and readout oversampling in multiple
spatial dimensions. Those features are exploited in Chapters 5-7.
2.4. Imaging Requirements
2.4.1. Field of View and Spatial Resolution
Although the discussion so far has been focused on continuous time
signals, k-space is always sampled discretely in practice, with the sampling
intervals defined as ∆kx and ∆ky in the frequency-encoding and phase-
encoding dimensions in the case of Cartesian sampling. Considering the
one-dimensional case first, the discrete sampling of each k-space line
represents multiplication of the continuous signal by a comb function with
interval width ∆k. This corresponds to a convolution of the 1D object being
imaged with the Fourier transform of the comb-function, which is also a
comb function with reciprocal interval width 1/∆k. Therefore, the discrete
sampling leads to periodic replication of the imaged object at a distance of
1/∆k. According to the Nyquist sampling theorem, a band-limited signal with
given bandwidth B must be sampled at an interval (∆k) no larger than 1/2B

24
Figure. 2.4: In Cartesian, the sampling intervals (∆kx and ∆ky) must be smaller than the reciprocal the object size in the corresponding spatial dimensions in order to avoid alishing. In radial sampling, the maximum interval between two adjacent radial lines (∆d) has to be small than or equal to ∆k in order to reconstruct an image without aliasing artifacts.
in order to reconstruct it without aliasing. Generalized to the two-
dimensional case in MRI, and considering the case of Cartesian sampling,
the following requirements must be satisfied:
1
1
x
x
y
y
kW
kW
(2.20)
Here xW and
yW are the size, in the x and y dimensions, respectively, of the
object being imaged. Since the field of view (FOV), which indicates the
extent of the region to be imaged, can be defined as

25
1
1
x
x
y
y
FOVk
FOVk
(2.21)
it suggests that the FOV must be greater than the size of the object in order
to avoid aliasing.
The relationship in Equation 2.21 can also be applied in non-
Cartesian imaging. In the case of radial sampling, for example, the
maximum interval between two adjacent radial lines, as denoted by ∆d in
Figure 2.4b, must be less than or equal to ∆k, which can be satisfied when
2
sn n
(2.22)
Here sn is the number of radial lines and n is the number of sampling
points in each readout line. Equation 2.22 suggests that radial sampling
requires more measurements than Cartesian sampling in order to
reconstruct an image without aliasing artifacts.
Theoretically, an image can be reconstructed unambiguously from
infinite k-space sampling. However, k-space sampling in practice is always
finite, with the highest spatial frequency sampled represented by kxmax and
kymax in two spatial dimensions. This can be described as a multiplication of
infinite k-space sampling by a rectangular function with width 2×kmax (from –
kmax to +kmax) in each dimension. Therefore, the reconstructed image

26
always represents the convolution of the true object with a point spread
function (PSF), which is the Fourier transform of the rectangular truncation
window (a sinc function). The sinc function limits the ability to resolve
detailed structures and thus the spatial resolution is limited to the effective
width, often measured as the full-width at half maximum (FWHM), of the
PSF. The spatial resolution in MRI, denoted as x and y in two
dimensions, can be calculated as
1
1
x
x x x
y
y y y
FOVx
N k N
FOVy
N k N
(2.23)
Since max2x x xk N k and
max2y y yk N k , we also have
max
max
1
2
1
2
x
y
xk
yk
(2.24)
2.4.2. Signal to Noise Ratio
The intensity values of an MR image represent combinations of the
true signal intensity and the noise. Therefore, another practical
consideration for MRI is signal to noise ratio (SNR). The noise in an image
can result from a number of factors, including noise in the body due to
movement of charged particles and other similar mechanisms, and noise

27
from the measurement electronics. Although SNR is usually expressed as a
function of various parameters including voxel size, number of averages,
number of sampling points, and receiver bandwidth, it can be simplified as
follows (32):
( )( )( ) sSNR x y z T (2.25)
Here sT indicates the total readout duration in a scan. This equation
indicates that the SNR is in general proportional to the voxel size and to the
square root of the total acquisition time. Proportionality to the voxel size
imposes a trade-off between spatial resolution and SNR in MRI. Meanwhile,
factors that change the Ts also tend to change the SNR. For example, the
SNR decreases in the case of undersampling (see parallel imaging in
section 2.6) and higher readout bandwidth (decreased sampling dwelltime
in each readout line and thus shorter TR). On the other hand, SNR can be
increased by acquiring the same image multiple times and averaging.
Meanwhile, we can double the sampling rate in each readout line to
increase FOV in order to avoid aliasing without SNR penalty, because it
neither changes the voxel size nor the sampling time Ts.
2.5. MR Image Reconstruction
2.5.1. Generalized Image Reconstruction

28
As shown in Equation 2.17, MR signal from a two-dimensional plane
is a spatial integration of the spin density against the sinusoidal spatial
modulation generated by encoding gradients. In other words, the MR signal
comprises projections of the spin density against Nx×Ny distinct functions,
in which a total number of Nx×Ny measurements are obtained in the
presence of frequency- and phase-encoding gradients. As discussed in the
previous sections, appropriate discretization is needed in practical MRI
acquisition and thus the integration in Equation 2.17 can be approximated
as
,
( , ) ( )exp( 2 [ ])yx
x y
yxx y
kks k k m x,y i x y
N N (2.26)
Equation 2.26 represents the Fourier transform of the spin density in the
two-dimensional plane with appropriate discretization of the continuous
positions. Therefore, the reconstruction of the image can be formulated as
the inverse discrete Fourier transform (DFT) of the MR measurements
,
1( ) ( , )exp( 2 [ ])
yxx y
yx x ykx ky
kkm x,y s k k i x y
N N N N (2.27)
The spatial encoding part in Equation 2.27 can be written as
( ) exp( 2 )exp( 2 )yx
x y
yx
kkE x, y,k ,k i x i y
N N (2.28)
Equation 2.28 is usually referred as “encoding function”, because it

29
represents the way that spatial encoding is performed. Thus, Equation 2.26
can be rewritten in matrix notation as
s = Em (2.29)
Here s is the measured MR signal vector in k-space (with size Nk×1), m is
the image vector to be reconstructed (with size N𝜌×1) and E is the
encoding matrix that transforms the image vector into the signal vector (with
size Nk×N𝜌). Reconstruction of the image m is given by inverting Equation
2.29
-1m=E s (2.30)
Supposing the measurement matrix E is full rank, the reconstruction
described in Equation 2.30 is discussed in three different situations.
i) When Nk=N𝜌, the system is well-determined and then s can be uniquely
reconstructed from Nk linearly independent measurements.
ii) When Nk>N𝜌, the system is over-determined and, strictly speaking, there
is no solution. In general, a good guess for the solution can be found by
minimizing the mean square error
2
2s
ˆmin E m-s (2.31)
Here 2 is the L2-norm to quantify the energy or power of the difference
between the measurements and the estimated solution. The solution of
Equation 2.31 is given by the Moore-Penrose pseudoinverse

30
H H
m̂ = (E E)E s (2.32)
Here H defines the Hermitian conjugate and m̂ represents the
approximate solution.
iii) When Nk<N𝜌, the system is under-determined. This is usually the case
for undersampling in MRI, and the solution is not unique. In this case,
one classic way of arriving at a solution is to solve the following
optimization problem:
2
2s
s t 2
ˆmin m
ˆ. . E m-s (2.33)
Here is the estimated noise level. Based on the isometric property of
the Fourier transform, minimization of energy in the image domain is
equivalent to minimization of energy in k-space, and thus the solution to
Equation 2.33 is the zero-padded reconstruction, which can lead to
aliasing artifacts in the result. Additional regularizations can be applied
to reconstruct a better solution, which will be discussed more in the
section on compressed sensing.
2.5.2. Reconstruction of Non-Cartesian k-Space Data
As mentioned above, MRI reconstruction can be performed by
applying an inverse DFT on the measured k-space data as shown in
Equation 2.27. For Cartesian sampling, where all the k-space points are

31
sampled on an equidistant grid, the image reconstruction can be efficiently
implemented with an inverse Fast Fourier Transform (FFT) instead of
inverse DFT, which reduces the computational problem from N2 to N∙logN
and thus enables faster reconstruction.
In the case of non-Cartesian sampling, k-space data is not located
on a conventional Cartesian grid, and thus the use of inverse FFT for
reconstruction is not valid anymore. A straightforward approach for non-
Cartesian image reconstruction would be direct evaluation of Equation 2.27.
However, this approach is computationally expensive and is impractical for
clinical use.
A generalized and efficient approach for non-Cartesian image
reconstruction is the use of non-uniform FFT, which is also known as
gridding (33,34). The reason this works is because the image support is
finite and thus each point in k‐space can be estimated by convolution with a
sinc function, which corresponds to the multiplication of the image by a
rectangular function in the image domain. In a standard gridding
reconstruction, the measured k-space points on an arbitrary trajectory (i.e.,
radial or spiral) are first interpolated onto a Cartesian grid, and then
subjected to the inverse FFT to reconstruct the final images. In actual
practice, gridding reconstruction typically requires multiple steps.

32
The sampling density of a non-Cartesian trajectory is typically not
uniform, with denser sampling usually performed in the center of k-space
than in the outer regions. This leads to significant image blurring in the
reconstructed image, because signal from the dense sampling regions
accumulates and thus results in overestimation of the central k-space
regions. Therefore, a density compensation process is usually needed
before the interpolation. This compensation can be achieved by weighting
each k-space point with the inverse density of the corresponding sampling
positions in k-space, which is called a density compensation function
(DCF). The DCF can be estimated by computing a Voronoi diagram of the
trajectory (35), or in the case of radial sampling, the DCF can be simplified
as a Ram-Lak filter (also known as an M filter) because the sampling
density of each k-space point is inversely proportional to its distance to the
k-space center.
The interpolation process in a gridding reconstruction can be
achieved by convolving the measured k-space data with a pre-defined
kernel at the desired k-space positions
( ) ( )ii
i
s k s K k k ˆ (2.34)
Here ik k is the distance between the ith k-space point and the desired
position in Cartesian grid, and K is the kernel used for convolution. The

33
convolution with a kernel in k-space leads to a multiplication of the image
with the Fourier transform of the kernel, thus it would in a sense be ideal to
choose the sinc function because it can preserve the original image
information. However, it is generally impractical to compute the convolution
with a full sinc function, and thus a compact kernel has to be used to
approximate the properties of the sinc function. The Kaiser-Bessel kernel
has been shown to provide good image quality (33) and thus it is commonly
used in gridding reconstruction. Moreover, in order to avoid aliasing effects
due to the interpolation with a finite kernel, the convolution is usually
evaluated on a two-fold oversampled Cartesian grid with half of the
sampling distance. This leads to doubled FOV in the final results, and the
reconstructed image can be cropped back to the original FOV at the end of
the reconstruction.
After the interpolation process, a two-dimensional inverse FFT can
be directly applied to reconstruct the image. However, due to the
convolution with a finite kernel in k-space, the reconstructed image is
modulated by the Fourier transform of the kernel. This undesired
modulation, which is called apodization or roll-off effect, can be
compensated by dividing the image by the Fourier transform of the kernel,
which is known as deapodization or roll-off correction.
2.6. Parallel MRI

34
2.6.1. The Need for Speed in MRI
MR imaging speed is of critical importance in many clinical
applications. However, the imaging speed with which gradient-encoded MR
images can be acquired is fundamentally limited by the sequential nature of
gradient-based MR acquisitions, in which only one k-space line can be
acquired per unit time. In order to accelerate data acquisition, conventional
MRI requires stronger field gradients, faster gradient switching rates, and/or
more frequent RF excitations. Faster gradient switching can lead to
peripheral nerve stimulation, and more frequent RF pulses can result in
increased RF power deposition, with an increased risk of damaging
biological tissues.
Another way of accelerating MR imaging is to acquire reduced
quantities of measurements without compromising image information or
spatiotemporal resolution. Partial Fourier imaging is one of the simplest
approaches for accelerated data acquisition in MRI. In this approach,
approximately half of the k-space lines are acquired and the rest are
estimated by exploiting the conjugate symmetry property of the Fourier
transform for real-valued objects (14-16). However, the maximum
acceleration factor in Partial Fourier imaging is limited to less than two.
Parallel MRI, introduced in earnest in the late 1990s (17-19), is a more
popular and more flexible approach for increasing imaging speed. Parallel

35
Figure. 2.5: An example of multicoil brain images with corresponding coil sensitivity maps with 8 coil elements. Each individual coil element has a different spatially-varying sensitivity pattern.
MRI uses spatial information from an array of RF receive coils to perform
some portion of the spatial encoding that is normally accomplished via field
gradients. Since signals in multiple receive coil elements may be acquired
simultaneously, coil-based encoding enables acquisition of multiple lines of
image data at the same time (20). Over the past two decades, parallel MRI
has evolved rapidly, and it is implemented on most clinical MR scanners in
use today. A generalized formulation of parallel MRI is briefly reviewed in
this section.
2.6.2. Spatial Encoding Using Coil Arrays
In parallel MRI, an array of RF receiver coils is used for data
acquisition. Each individual coil element has different spatially-varying
sensitivities, as shown in Figure 2.5. In the case of two-dimensional
imaging, the k-space data acquired in each coil-element can be described
by adapting Equation 2.17 as follows:

36
2 [ ( ) ( ) ]
( , ) ( , ) ( , )x y
x yl lx y
i k t x k t ys k k c x y m x y e dxdy
(2.35)
Here, cl 1,2,3, ,N is the coil index ( cN is the total number of coil
elements) and ( )lc x, y is the coil sensitivity map for the l th coil element. A
hybrid encoding function can then be formulated as
( ) ( )exp( 2 )exp( 2 )x y x yl lE x,y,k ,k c x, y i k x i k y (2.36)
Equations 2.35 and 2.36 suggest that as long as the combination of
different coil sensitivities can imitate the gradient encoding, some k-space
lines that are traditionally acquired using gradient encoding can be
generated retrospectively using the coil sensitivities. In other words, the use
of multiple receiver coils with different spatial sensitivities allows for
acquisition of multiple k-space lines simultaneously.
2.6.3. Generalized Parallel MRI Reconstruction
The hybrid encoding function formulated in Equation 2.36 does not
form a pure Fourier basis, and thus reconstruction is more involved than an
inverse Fourier transform. Combining Equation 2.35 and 2.36, we have
( , ) ( , ) ( , , , )x yx ylx y
s k k m x y E x y k k dxdy (2.37)
Or, with appropriate discretization
,
( , ) ( , ) ( , , , )x yx yl
x y
s k k m x y E x y k k (2.38)
Equation 2.38 can be rewritten in matrix notation as

37
s =Ε m (2.39)
Here vector s contains the measured multicoil MR signal (with size
NcNk×1), m is the image vector to be reconstructed (with size N𝜌×1), and
E is the hybrid encoding matrix (with size NcNk×N𝜌). It can be seen from
Equation 2.39 that theoretically the encoding matrix E remains invertible as
long as gradient encoding steps are reduced by no more than a maximum
factor of Nc. In general, the reconstruction problem is over-determined, and
thus reconstruction of image m̂may be performed by minimizing the mean
square error
2
2m
ˆmin E m-s (2.40)
As is the case for Equation 2.32, the solution of Equation 2.40 can be found
by computing the Moore-Penrose pseudoinverse
1 1 H H
m̂ = (E E)E s (2.41)
Here, the pseudoinverse has been generalized by including a noise
covariance matrix , which accounts for correlations in noise contributions
from distinct array elements, and which can be computed from
measurements in the absence of RF excitation (i.e. with a flip angle of
zero). The noise covariance matrix is a practical tool to evaluate the noise
distribution in different coil elements in the measurement system. The best
reconstruction result can be obtained when any noise shared by more than

38
one coil is removed from the problem. This step is commonly known as
noise decorrelation or noise whitening.
Practical parallel MRI reconstruction methods are usually
implemented based on particular sampling patterns (i.e., regular
undersampling), or else using iterative reconstructions in the case of non-
Cartesian sampling. Different parallel imaging techniques, such as SMASH,
SENSE, and GRAPPA, have been extensively developed and broadly
implemented for day-to-day clinical exams. The discussion of specific
parallel imaging algorithms can be found in many classic papers and
textbooks (36-39).
2.6.4. Estimation of Coil Sensitivities
In parallel MRI, accurate coil sensitivity information is required in
order to reconstruct the image from undersampled k-space data. Since the
sensitivities can depend not only on the geometry of the coil array, but also
on the object be imaged, estimation of coil sensitivities is required for each
individual scan. Additional reference data, which can be either acquired
separately or self-calibrated, is used for coil sensitive estimation.
In parallel image reconstruction methods like SENSE, coil sensitivity
maps must be calculated explicitly and then used to compute the encoding
matrix so that the aliased image can be unfolded from undersampled
measurements. In parallel image reconstruction methods like GRAPPA (19)

39
or SPIRiT (31), on the other hand, the coil sensitivity maps do not need to
be calculated explicitly and the missing k-space lines are estimated using
autocalibrated measurements acquired as an integral part of the data
measurements. Autocalibration has the advantage that reconstructions are
less sensitive to temporal changes such as motion. In dynamic imaging, the
sampling pattern in different temporal frames can be specifically designed,
so that the coil sensitivities can be estimated from the averaging of all the
dynamic frames. In these methods, additional reference data is not
necessary for coil sensitivities estimation.
The raw sensitivity maps are generally corrupted by noise, and many
approaches have been proposed to produce smooth sensitivity maps, such
as the adaptive array combination (40).
2.6.5. SNR in Parallel MRI
Although parallel imaging has already enabled significant progress in
rapid MRI, it has been found that acceleration in parallel imaging is limited
by noise amplification in the reconstructed images, whose extent is
ultimately determined by RF receiver coil design (41). The classic SNR
equation for parallel imaging was proposed by Pruessmann (18) as
0SNR
SNRg R
(2.42)

40
It can be seen from Equation 2.42 that the SNR in parallel imaging is
determined by three terms, including:
i) The baseline SNR0 of the system or the acquisition protocol, which is
related to many factors such as echo time (TE), repetition time (TR), and
other sequence parameters.
ii) The undersampling factor R , which is related to the parallel imaging
acceleration. This is consistent with the SNR Equation described in
section 2.4.2, which indicates that the SNR drops whenever the
sampling time Ts is decreased.
iii) The geometry-factor, or simply g-factor, g , which is related to the coil
design or coil geometry. The g-factor results from the nonunitarity of the
combined coil-sensitivity- and gradient-based encoding functions, and
the corresponding ill-conditioning of the encoding matrix inverse.
Intuitively speaking, high degrees of overlap in coil sensitivities results in
amplification of noise out of proportion to signal, especially in the case of
excessive accelerations.
It has been demonstrated that there is a fundamental upper limit to
acceleration for a given level of acceptable noise amplification (41,42). This
limit arises from the smoothness of physically realizable electromagnetic
fields, as described by Maxwell’s equations. Generally speaking,
accelerations beyond a factor of 3 or 4 for 2D imaging or a factor of 6 to 10

41
for 3D imaging are starved for SNR, even when arrays with very large
numbers of elements are used.
2.7. Compressed Sensing MRI
Parallel imaging has led to revolutionary progress in the field of rapid
MRI in the past two decades. However, as discussed in the previous
section, the maximum acceleration that can be achieved in parallel imaging
is limited by the number and the design of coils, and ultimately by
fundamental electrodynamic principles. Compressed sensing (26,27) is
another powerful approach that can be applied to accelerate data
acquisitions in MRI (28), and has attracted enormous attention since its
introduction. Compressed sensing can be combined with parallel imaging in
MRI to further increase imaging speed by exploiting joint sparsity in multicoil
images (29-31). In this section, the basics of compressed sensing, its
application for MRI, and its combination with parallel imaging, are briefly
reviewed.
2.7.1. Introduction to Compressed Sensing
Conventional schemes for sampling a signal must satisfy the
requirements of the Nyquist theorem: namely, that the sampling rate must
be at least twice the maximum bandwidth presented in the signal.
Unfortunately, in many applications, Nyquist sampling is time-consuming

42
and data-intensive, posing a challenge for sampling system design, data
storage, and transmission. In order to address this logistical and
computational challenge, high-dimensional data are usually compressed
after acquisition by transforming to a basis that provides a sparse or
compressible representation for the signal and discarding insignificant
components. This transform coding framework has been widely used in the
JPEG, JPEG2000, and MPEG standards.
The ability to compress images so effectively raises an interesting
question, one which underlies compressed sensing: instead of first
sampling a signal at a high sampling rate and then discarding most of the
sampled measurements in the compression process, why not directly
acquire the data in a compressed form at a lower sampling rate? In other
words, can we build the compression process directly into the acquisition or
sensing step, so that one does not have to perform so many measurements
and discard most of them afterwards? Candes, Romberg, Tao, and Donoho
proved the feasibility of this hypothesis and proposed a framework by which
a sparse or compressible signal could be successfully recovered from
undersampled measurements that are far below the Nyquist limit (26,27).
After rapid development in the past decade, compressed sensing
has already achieved notable impact in a wide range of application areas,
such as sensor design in high-resolution cameras and medical imaging.

43
One of the applications that can substantially benefit from compressed
sensing is MRI, in which the imaging speed can be dramatically improved if
three requirements can be satisfied, including: i) the image is sparse or has
a sparse representation in some transform domain; ii) incoherent sampling,
seen in the structural preservation of image content and the structural
disintegration of artifacts in the sparse domain; iii) a non-linear
reconstruction to recover the image by removing the incoherent artifact. The
discussions in the following sections will focus on these aspects.
2.7.2. The Sensing Problem
The sampling of a signal vector mwith size N×1 can be interpreted
as a projection of the signal onto the sampling waveforms i
,i is i 1,2,3,...,M m (2.43)
Here s is a measurement vector with size M×1. In matrix notation, we have
s =Φm (2.44)
Here the waveforms form the sampling matrix Φ with size of M×N.
In the case of undersampling, the number of measurements is
smaller than the dimensionality of the signal (M<N) and therefore the
system is under-determined, assuming that the sampling matrix Φ has full
rank. As shown in section 2.5, the solution to Equation 2.44 is not unique.
However, if the signal m is known to be sparse and the sampling matrix Φ

44
Figure. 2.6: Sparse representation of a brain image in wavelet transform domain. By keeping only the largest 10% coefficients and discarding the rest, the image can still be recovered without loss of important information but with 10-folder smaller size.
satisfies certain specific requirements, it is possible to recover the signal
from an incomplete set of measurements. For example, supposing a signal
is K-sparse with K<M, which means that there are at most K nonzero
components in the signal vector, and the locations of the nonzero
components are also known. In this case, the measurement matrix Φ can
be reduced to KΦ , with size M×K, by keeping only the K columns
corresponding to nonzero locations. The signal m can be similarly reduced
to Km with only the nonzero coefficients. Therefore, the system becomes
K Ks =Φ m (2.45)
In this situation, only K measurements are sufficient to recover the signal.
2.7.3. Sparsity
From the previous subsection, we know that the first requirement in
compressed sensing is sparsity of the signal. A signal is said to be sparse if

45
most of its coefficients are zero or close to zero, and the relatively few large
coefficients can capture most of the information. In other words, sparsity
implies that one can discard the small coefficients without significant
perceptual loss. The signal can be sparse itself, or it can be compressible,
which means that the signal has a sparse representation in some
appropriate transform domains. Mathematically speaking, a compressible
signal m can be expanded in a transform basis (such as a wavelet basis)
Ψ as follows:
m=Ψx (2.46)
Here, x is the sparse representation of signal m in the basis defined by Ψ .
In Figure 2.6 we can see how a dataset that is not sparse in the
image domain, a brain MR image, may have a sparse representation in a
different domain, the wavelet transform domain. By keeping only the largest
10% of coefficients and discarding the rest in the transform domain, the
image can still be recovered without losing important information, but with
10-folder smaller size. Dynamic images have much higher sparsity than
static images because of the the presence of significant temporal
correlations associated with periodic motion or gradual evolution.
Therefore, a dynamic image series can have sparse representation with an
appropriate transform applied along the dynamic dimension. Figure 2.7

46
Figure. 2.7: A cardiac cine image series has temporal correlation because dynamic region is limited in only a small region, while the background is static. An FFT can be employed along the temporal dimension to sparsify the dataset.
shows an example of sparse representation of a cardiac cine image series,
in which a temporal FFT is employed as the sparsifying transform.
2.7.4. Conditions for Sparse Signal Recovery
In order to reconstruct the sparse signal from undersampled
measurements, the measurement matrix must be designed properly so that
it can preserve the information of the sparse signal. Equations 2.44 and
2.46 can be combined as
s =ΦΨx Ax (2.47)

47
Here the measurement matrix Φ and the sparse representation matrix Ψ
are combined as a single matrixA . We can define the isometry constant
K of A as the smallest number such that
2 2 2
2 2 2(1 ) (1 )K K x Ax x (2.48)
holds for all K-sparse vectors x (26). A is said to obey the restricted
isometry property with a constant K if Equation 2.48 is satisfied. Good
performance of compressed sensing can be ensured when K is close to
zero. Equation 2.48 implies that the matrix A can preserve at least part the
energy of a K-sparse vector. In other words, it suggests that any K-sparse
vectors cannot be in the null space of matrix A and all subsets of K
columns taken from A must be linearly independent or even nearly
orthogonal. Note that in the case of undersampling, all of the columns of
matrix A cannot be exactly orthogonal, because A is a wide matrix, with
more columns than rows. As proposed by Candes (26), a sufficient
condition to ensure stable recovery of a K-sparse signal is that A satisfies
2 2 2
2 22 2 2(1 ) (1 )K K x Ax x (2.49)
with an isometry constant 2 2 1K for any 2K-sparse vectors.
2.7.5. Sampling and Incoherence

48
Although restricted isometry property guarantees sparse signal
recovery, it is computationally expensive to verify in practice. Therefore, it is
preferable to exploit some properties of A that can be easily evaluated. The
mutual coherence of a matrix, which is defined as the largest absolute inner
product between any two columns, is one such property, and can be
formulated as follows:
2 2
,μ( ) max
i j
i ji j
A A
A AA (2.50)
The mutual coherence can be estimated by calculating the Gram matrix
HA A . When A is very close to the identity matrix, the off diagonal entries
in matrix HA A are small, suggesting high incoherence and therefore
ensuring good performance in compressed sensing. One can relate the
mutual coherence to the restricted isometry property because μ must be
small when Equation 2.48 is satisfied.
The restricted isometry property also implies that the measurement
basis Φ must be incoherent with sparse representation basisΨ . In other
words, a signal having a sparse representation in a given transform domain
Ψ must spread out in the sampling domain Φ , thus ensuring sparse signal
recovery from only a small subset of measurements. Supposing Φ and Ψ

49
Figure. 2.8: Sampling matrix and the corresponding Gram matrix HA A . Ψ is set as
the identity matrix and Φ is the fully sampling Fourier matrix (a) and partial Fourier matrices with regular (b) and random (c) undersampling schemes. The off-diagonal entries in (c) are very small, suggesting that random undersampling is good for compressed sensing.
are both orthonormal bases, incoherence can be measured by calculating
the coherence between two bases as
1 ,
( , ) max ,jkk j N
N
Φ Ψ (2.51)
Herek
and j
are normalized to 1, and [ ]1, N . Equation 2.47
calculates the largest correlation between any two elements of Φ and Ψ .
Small coherence indicates that Φ and Ψ do not contain correlated
elements, and thus are paired well for compressed sensing.
Since MRI k-space data are acquired in the spatial frequency
domain, the measurement matrix is the partial Fourier matrix in the case of

50
undersampling. Therefore, the mutual coherence can be used as a metric
to evaluate different undersampling schemes. Figure 2.8 shows the Gram
matrix HA A , where Ψ is set as the identity matrix and Φ is the full Fourier
matrix (a) and partial Fourier matrices that were taken from (a) in a regular
(b) and random (c) fashion. It can be seen from Figure 2.8 that regular
undersampling leads to aliasing artifacts, while random undersampling
produces high incoherence (small off-diagonal coefficients) that is preferred
in compressed sensing. In fact, random undersampling is broadly employed
for Cartesian sampling in compressed sensing MRI, and a more common
way of measuring incoherence is to evaluate the point spread function
(PSF) of the undersampling mask, as proposed by Lustig (28). Moreover,
some practical restrictions have to be considered when designing an
undersampling pattern. For example, since most of the energy is
concentrated in the low-frequency region of k-space, taking more
measurements from the k-space center is preferred. Because
undersampling along the frequency-encoding dimension does not save
acquisition time in Cartesian MRI, undersampling is only performed along
the phase-encoding dimensions. Therefore, the ability to exploit
incoherence in conventional Cartesian imaging is limited to the phase-
encoding dimensions only. Figure 2.9 shows an example of a 1-dimensional
variable density undersampling pattern and the corresponding PSF along

51
Figure. 2.9: An example of one dimensional variable density undersampling pattern and the corresponding incoherence, represented by the point spread function (PSF) of the undersampling pattern.
the phase-encoding dimension. More freedom can be achieved by
extending the sampling scheme into three-dimensional or non-Cartesian
sampling, in which undersampling can be performed along more than one
dimension. Moreover, dynamic MRI is particularly interesting for
compressed sensing, because different undersampling patterns can be
applied in different dynamic frames, providing the possibility of exploiting
incoherence along the temporal dimension.
2.7.6. Image Reconstruction
The compressed sensing theory states that as long as the signal is
sparse and the requirement for the restricted isometry property or
incoherence is satisfied, the sparse solution is unique and guaranteed (26).

52
The measurement of sparsity in a signal vector can be performed by
calculating the zero-norm (L0-norm), which is defined as:
0
0x i
i
x (2.52)
The L0-norm simply counts the number of nonzero coefficients in a vector.
Therefore, the reconstruction of the sparse signal x in compressed sensing
can be formulated by minimizing the L0-norm problem
0arg min
. .s txx
s =ΦΨx (2.53)
or
0arg min
. .s txx
s = xA (2.54)
Because the measurements are usually contaminated by noise, Equation
2.54 is modified as follows:
0
2
2
arg min
. .s t
xx
s - Ax (2.55)
Here is the estimated noise level and the L2-norm is applied to quantify
the power or energy in the difference between the measurements and the
estimated solution. A more general formulation for solving the problem is to
find the signal m that has a minimized L0-norm in the sparse domain

53
0
2
2
arg min
. .s t
H
fΨ m
s -Φm (2.56)
Here H is defined as the Hermitian conjugate. While the L0-norm can
exactly determine the sparsest solution, minimizing the L0-norm is an NP-
hard problem, which is computationally intensive. Therefore, different
approaches that can be applied to solve the compressed sensing problem
more efficiently have attracted lots of attention. Currently the main type of
sparse recovery algorithms is related to the basis pursuit (BP), in which a
L1-norm minimization is used to replace the L0-norm minimization as
follows:
1
2
2
arg min
. .s t
H
fΨ m
s -Φm (2.57)
Here the L1-norm is defined as the summation of the absolute values of all
the coefficients in a signal vector
1
x i
i
x (2.58)
The L1-norm minimization problem in Equation 2.58 is a convex problem
and thus guarantees a global minimum over all the possible solutions. It has
been demonstrated that as long as certain conditions can be satisfied (e.g.,
the restricted isometry property), the solution of minimizing the L1-norm can
be equivalent to the solution of minimizing the L0-norm (26). The

54
Figure. 2.10: Combination of compressed sensing and parallel imaging enables reduced incoherent artifact level when compared with a single coil model.
constrained minimization problem in Equation 2.57 can be alternatively
formulated as an unconstrained problem using Lagrange multipliers
(Equation 2.59), so that it can be efficiently solved using algorithms like
gradient descent or conjugate gradient methods.
2
2 1arg min H
ms -Φm Ψ m (2.59)
The regularization parameter in Equation 2.52 controls the trade-off
between the data consistency (L2-norm) and the promotion of sparsity (L1-
norm).
2.7.7. Combination of Compressed Sensing and Parallel Imaging
Compressed sensing can be combined with parallel imaging to
further increase imaging speed by exploiting the idea of joint multicoil
sparsity. These two approaches can be synergistically combined as image

55
sparsity and coil sensitivity encoding are complementary sources of
information. On one hand, compressed sensing can serve a regularizer for
the inverse problem in parallel imaging and prevent noise amplification. On
the other hand, the additional spatial encoding capabilities of multiple
receiver coils in parallel imaging enable exploitation of joint sparsity in
multicoil images, and thus higher acceleration rates. In this section, a
reconstruction framework called k-t SPARSE-SENSE (30), which combines
compressed sensing and parallel imaging using a SENSE-type
reconstruction scheme, is briefly reviewed.
Instead of performing compressed sensing reconstructions for each
individual coil separately, a joint compressed sensing reconstruction that
enforces joint sparsity in the multicoil model is applied in k-t SPARSE-
SENSE. With this approach, the additional spatial encoding capabilities of
multiple receive coils can be exploited to reduce the incoherent aliasing
artifacts in the multicoil combination, thus enabling higher acceleration
rates. Figure 2.10 shows the reduction of incoherent artifact when
comparing a joint 8-coil array model to a single coil model.
The reconstruction of k-t SPARSE-SENSE can be formulated as
2
2 1arg min H
m-ΦCm s Ψ m (2.60)

56
Here Φ is the same measurement matrix as before and 21, ,... nC C CC
are the coil sensitivities in n coil elements. When compared with Equation
2.59, the L1-norm term in 2.60 enforces joint multicoil sparsity, since m
represents the combined multicoil image and is comprised of contributions
from all coils. The coil sensitivity maps can be self-calibrated or estimated
from reference data acquired separately. Reconstruction algorithms that
solve the compressed sensing problem in Equation 2.59 can be applied for
the joint compressed sensing problem with the incorporation of coil
sensitivities.
In addition to the combination with parallel imaging in a SENSE-type
framework, compressed sensing can be also combined with
GRASP/SPIRiT-type parallel imaging methods, such as L1-SPIRiT
proposed in (31). The performances of different combinations would
achieve similar performance though the coil sensitivities are used in
different ways, e.g., autocalibrated or explicitly calibrated. The differences
between SENSE and GRAPPA, however, will affect the corresponding
combination. For example, because GRAPPA or SPIRiT use a kernel with a
pre-defined kernel size to estimate the missing k-space points, standard
variable density random undersampling patterns may fail to achieve good
performance because there are larger gaps in the outer part of k-space
than the central part, and thus the estimation of high-frequency k-space

57
points can be challenging. Therefore, different random undersampling
strategies (e.g., poisson-disc undersampling) are required. On the other
hand, variable density random undersampling would achieve good
performance in the combination of compressed sensing with a SENSE-type
framework because SENSE effectively uses all of the k-space point to
estimate the missing k-space points (20).
2.7.8. Low Rank Matrix Completion
The undersampled dataset in MRI can be described in terms of a
matrix with missing entries, and correspondingly, the reconstruction of an
image from undersampled data can be formulated as a procedure to fill the
missing k-space lines. If a matrix is in low-rank condition, it can be
represented by only a few dominant singular values, and their
corresponding singular vectors, without loss of important information. In
other words, an image can have a sparse representation in the singular
value decomposition (SVD) domain if it has low rank. Therefore, the low
rank property of a matrix can be applied to enforce sparsity and exploit the
correlation in MRI images (43). Since dynamic image series usually have
much higher correlation with much lower rank along the temporal
dimension, the low rank constraint is often applied in the reconstruction of
undersampled dynamic MRI.

58
As shown in Equation 2.46, the measurement of an image can be
described as
s =Φm (2.61)
Here m is the image to be reconstructed and s are the measurements. In
the case of undersampling, the system is underdetermined and the solution
is not unique. However, if the image to be reconstructed is known to have
low rank, and if the requirement for incoherent sampling, as described in
section 2.7.5, is satisfied, a natural way to complete the missing entries in a
matrix is to search for the solution that has the lowest rank:
2
2
min rank( )
. .s t
m
s -Φm (2.62)
Unfortunately, similar to minimization of the L0-norm, rank-minimization is
also an NP-hard problem and there is no efficient way to solve this problem.
Usually the nuclear norm is used to replace the rank function in Equation in
2.57 as follows:
*
2
2
min
. .s t
m
s -Φm (2.63)
Here * is the nuclear norm of a matrix, given by the sum of its singular
values. In dynamic MRI, the nuclear norm is enforced on the corresponding
Casorati matrix of the image series, in which each image frame is
concatenated into an individual column in the Casorati matrix.

59
The major difference between standard compressed sensing
reconstruction with L1-norm minimization (Equation 2.63) and low rank
completion with nuclear norm minimization (Equations 2.57) is that SVD is
performed as the sparsifying transform to exploit the sparsity of images,
and therefore, it does not require an explicit sparsifying transform. Image
series in specific applications, such as MR parameter mapping, have very
low rank, and thus reconstruction with nuclear norm minimization can
achieve superior performance to standard compressed sensing
reconstructions that use a temporal sparsifying transform such as temporal
FFT, as will be seen in Chapter 3. The exploitation of the low rank property
can be further combined with a sparsity constraint to enable reconstruction
with improved performance (44).
2.8. Motion in MRI
2.8.1. Influence of Motion in MRI
As discussed in the previous sections, MRI data acquisition is
comparatively slow, which leads to sensitivity to subject motion (45).
Loosely speaking, motion in MRI can be divided into three major categories:
rigid body motion (or bulk motion), blood flow, and elastic motion (i.e.,
cardiac motion, respiratory motion, and gastrointestinal peristalsis) (46).
According to the shift property of the Fourier transform, any motion of the
object being imaged generates a phase modulation in k-space, which

60
results in ghosting artifacts in conventional Cartesian imaging. Ghosting
artifacts appear as replicated copies of the moving object exclusively along
the phase-encoding direction. Since the ghosting artifacts are generally
overlaid with the true image representation, they also lead to blurring in the
image.
Although the sensitivity to motion in MRI can sometimes be used to
produce useful information (e.g., velocity mapping of blood flow), they
usually degrade image quality and can result in diagnostic
misinterpretations. Since the introduction of MRI, tremendous efforts have
been made to mitigate or correct for motion artifacts. There are various
strategies to handle different types of motion in MRI. For example, the
subjects being imaged can be immobilized. Specific strategies in sequence
design (e.g., gradient moment nulling) can be used to compensate artifacts
induced by blood flow. Cardiac motion can be eliminated by synchronizing
and gating the data acquisition with the cardiac contraction of the subjects,
so that the data acquisitions are only performed in specific quiescent period
(e.g., mid-diastole). Among various types of motion, respiratory motion is
one of the most frequent sources of artifacts. Although it can be avoided
with suspension of breathing during scans, breath-hold capabilities are
subject-dependent and can be significantly limited in some patients.
Meanwhile, typical breath-hold durations (10-15 seconds) also limit spatial

61
resolution and volumetric coverage. Therefore, free-breathing MRI is
desirable and attractive. Different techniques that can be used for free-
breathing MRI exams are surveyed in the following subsection.
2.8.2. Free-Breathing MRI Techniques
The most popular free-breathing approach is to use either navigator
signals (47) or respiratory bellows (48) to monitor respiratory motion, so that
data are only acquired at a specific respiratory state (e.g., end-expiration).
This approach is widely used in cardiovascular MR exams. However, this
gated data acquisition significantly reduces imaging efficiency and further
prolongs the total examination times. Real-time MRI is another approach
that can be used for free-breathing cardiac cine imaging (49), but the
acquisitions usually comprise only a single slice with limited spatial and
temporal resolution. Therefore, advanced image reconstruction techniques,
such as temporal parallel imaging or dynamic compressed sensing imaging,
are needed. Non-Cartesian k-space sampling schemes, such as radial or
spiral sampling, are substantially less sensitive to motion, and thus enable
free-breathing imaging, sometimes at the expense of increased scan times
(50-52). For example, radial imaging eliminates k-space gaps due to
motion-related phase shifts, by repeated sampling of the k-space center.
However, substantial motion is still a challenge for non-Cartesian imaging
and can result in blurring and undersampling artifacts, e.g. streaks in radial

62
imaging. Non-Cartesian imaging also offers the potential benefit of
retrospective self-gating, owing to the continuous passage of the radial lines
through the center of k-space, and can therefore eliminate the need to use
navigator signals or other external gating devices (53,54). However, the
self-gating approaches are still inefficient, since typically only data within a
predefined motion state (e.g., close to expiration) is used for reconstruction.
Another type of approach has also been proposed to correct for
respiratory motion by integrating an image registration framework into the
reconstructions. For example, a rigid-body motion registration framework
can be applied for respiratory motion correction in coronary MR
angiography (MRA) or cardiac perfusion imaging (55). More complex
deformable registration techniques that account for non-rigid body motion
can be also employed for reconstruction of cardiac cine images, cardiac
perfusion images, and abdominal DCE-MRI images (56-58). Moreover,
some approaches are even able to learn the motion fields to guide image
reconstruction, which, in addition to performing motion correction, can also
provide access to specific motion information (59). These motion correction
schemes, however, require the use of specific motion models, which may
be insufficient to account for the complex movement of the organs during
respiration, especially for patients with pronounced respiration or irregular
respiratory patterns. A novel free-breathing technique is proposed in this

63
dissertation to perform motion sorting and the reconstruction of additional
respiratory motion dimension in place of conventional motion correction.
The technique is called XD-GRASP (eXtra-Dimensional Golden-angle
RAdial Sparse Parallel imaging) and will be described in Chapters 6 and 7,
with demonstration of applications to both abdominal and cardiovascular
imaging.

64
Chapter 3
Accelerated T2 Measurement of the Heart Using k-t
SPARSE-SENSE
3.1. Prologue
As briefly reviewed in Chapter 2, compressed sensing can be
combined with parallel imaging (e.g. with approaches like k-t SPARSE-
SENSE) to further increase imaging speed and improve reconstruction
performance by exploiting joint sparsity in multicoil images. In this chapter,
we investigate the feasibility of applying a tailored k-t SPARSE-SENSE
reconstruction framework for accelerated parameter mapping by exploiting
the low rank property of the dynamic image series. Specifically, we focus on
rapid T2 measurement in the heart, which is particularly interesting but
challenging due to the influence of both cardiac motion and respiratory
motion.

65
The contents presented in this chapter were published in the journal
Magnetic Resonance in Medicine (MRM 2011 Jun; 65(6):1661-9) (60).
3.2. Introduction
T2-weighted MRI is a valuable method for detecting T2 changes that
are induced by a variety of diseases in the liver (61-64), heart (65-68), and
other organs. The most widely exploited contrast mechanism in T2-weighted
MRI is the alteration of water content by diseases, with edematous tissue
exhibiting increased T2-weighted signal and excessive iron accumulation
resulting in decreased T2-weighted signal. However, the resulting clinical
interpretation in T2-weighted images is often hindered by surface coil effects,
which can yield non-uniform MR signals unrelated to pathology.
Quantitative tissue characterization with T2 measurement or T2
mapping can overcome the limitations associated with T2-weighted MRI and
thus can improve the accuracy of assessing the severity of diseases.
Multiple single spin-echo pulse sequence with different echo times is
currently considered the reference technique for T2 quantification. However,
this technique is substantially inefficient for clinical application because
sufficient time is needed for spin relaxation after acquisition of each k-space
measurement. An alternative approach for T2 quantification is multiecho fast
spin echo (ME-FSE) pulse sequence (9), which accelerates the data
acquisition with the echo train length. While the ME-FSE sequence

66
considerably reduces the total acquisition time comparing to multiple single
spin-echo acquisitions, the imaging efficiency is still relatively low,
especially for abdominal or cardiac imaging that are affected by cardiac
motion and respiratory motion. Moreover, in the presence of radio
frequency field (B1) inhomogeneity, the flip angle variation can produce
indirect echoes and thus result in systemically error in T2 quantification. The
use of phase-cycling in Carr-Purcell-Meiboom-Gill (CPMG) sequence
(69,70) has been used to correct the flip angle variation for even echoes
and thus only even echoes can be kept to form the images with improved
accuracy in T2 quantification at the expense of reduced imaging efficiency.
In order to overcome the limitations associated with the ME-FSE
sequence, the sequence has been modified previously with “reverse centric”
k-space reordering, in which two successive echoes are used to form an
image with the odd and even echoes acquired at the outer and inner halves
of k-space, respectively (71). Therefore, this new ME-FSE sequence can
characteristically behave like an even-echo CPMG sequence with two-fold
acceleration. The accuracy of this sequence has been validated in vivo
against the even-echo only CPMG sequence, as described in (71).
Combining the two-fold acceleration in this new ME-FSE sequence with
conventional parallel imaging enables data acquisition within single breath-
hold for abdominal and cardiac imaging with spatial resolution on the order

67
of 2.7 x 3.8 mm2 (71). However, this spatial resolution may still not be
adequate, particularly in cardiac imaging, which is sensitive to partial
volume effects, especially in patients with thinned myocardial wall. Thus,
faster imaging speed is desirable for further accelerating T2 measurements.
T2 mapping is a good candidate for compressed sensing, because
the transverse magnetization (e.g., signal) as a function of time is
approximately mono-exponential and thus can be sparsely represented with
an appropriate transform basis along the echo dimension. In this work, we
propose to accelerate the ME-FSE pulse sequence described above for
cardiac T2 mapping with increased spatial resolution, using a tailored k-t
SPARSE-SENSE reconstruction framework adapted from (30). The results
were validated against that obtained from a reference approach using the
ME-FSE pulse sequence with parallel imaging only.
3.3. Low Rank Property in MR T2 Mapping
In MR T2 mapping, a dataset consists of a series of images that are
acquired at the same position but at different echo times and the signal
decay in each image pixel across the dynamic series is a function of T2
value to be estimated. Thus, the images along the echo dimension usually
have similar anatomical structures but with different T2-weighted contrast,
resulting substantial redundancy along the dynamic dimension. The data
redundancy in a T2 mapping dataset can be expressed as the low rank

68
Figure. 3.1: Low rank property of MRPM. (a): An example of cardiac T2 mapping image series, in which images at different echo times have similar anatomical structures but with different T2-weighted contrast. (b): The Casorati matrix generated from the image series. The Casorati matrix can be represented by a few dominant singular values and the corresponding singular vectors.
property of the corresponding Casorati matrix (Figure 3.1), in which each
image frame is concatenated into an individual column. Due to the low rank
property, the Casorati matrix can be represented by a few dominant
singular values and their corresponding singular vectors, suggesting that a
T2 mapping dataset is sparse and accordingly, the low rank constraint can
be used to reconstruct an accelerated T2 mapping dataset. This is known
as low rank matrix completion as reviewed in Chapter 2. The low rank
constraint can be enforced by performing a principal component analysis
(PCA) along the echo dimension as the sparsifying transform. Figure 3.2
shows the schematic details of performing a PCA on a reference cardiac T2

69
Figure. 3.2: Schematics details of estimating a PCA basis. By concatenating each time signal vector along column direction, a matrix V is constructed. A basis set for PCA is then estimated by conducting eigen-decomposition of the covariance matrix C of V.
mapping dataset. By concatenating each time signal vector along column
direction, a matrix V is constructed. Then, by conducting eigen-
decomposition of the covariance matrix C of V, a basis set for PCA can be
estimated.
In order to further demonstrate the low rank property of a T2 mapping
dataset, numerical simulation was performed to compare two different
sparsifying transforms, fast Fourier transform (FFT) and PCA along echo
dimension for a representative T2 mapping dataset. Using the
corresponding sequence parameters used in this study (see Pulse
Sequence section) and assuming T2 = 50 msec, an ideal monoexponential
curve representing the transverse magnetization was generated and plotted

70
in Figure 3.3a. The same monoexponential time curve was replicated for
each point on the image plane (x-y) to emulate the spatial resolution studied
in vivo, where x and y are two spatial dimension in an image. The temporal
FFT and PCA representations of this curve are shown in Figure 3.3b&c.
These plots clearly show that a monoexponential decay curve is sparser in
temporal PCA domain than in temporal FFT domain. To further validate this
finding, both temporal FFT and PCA representations of a reference cardiac
T2 mapping dataset are shown in Figure 3.3d&e. These preliminary results
prove that temporal PCA enables sparser representation than temporal FFT
for T2 mapping datasets, and confirms the rationale behind the exploitation
of low rank property in T2 mapping studies with compressed sensing.
3.4. Imaging Studies
The aim of the work was to achieve relatively high spatial resolution
(less than 2 x 2 mm2) for cardiac T2 mapping within clinically acceptable
breath-hold duration (less than 20 sec) using the ME-FSE sequence
developed in (71) and k-t SPARSE-SENSE reconstruction. An acceleration
rate (R) of 6, was needed to acquire a 192 x 192 x 16 (echoes) data matrix
within single breath-hold duration of less than 20 heart beats. For a field of
view of 320 x 320 mm2 and an inter-echo spacing of 5 ms, the acquisition
matrix corresponds to a scan time of 18 heart beats (one heart beat to
acquire the coil sensitivity data; one heart beat to acquire dummy scans to

71
Figure. 3.3: (a): A simulated monoexponential decay curve. (b): FFT representation of (a). (c): PCA representation of (a). These plots clearly show that a monoexponential decay curve is sparser in PCA domain than in FFT domain. To further validate this finding, a reference cardiac T2 mapping image series is displayed in both (d) FFT and (e) PCA domains. The results were consistent with the ideal curves shown (a–c).
approach steady-state of magnetization; and 16 heart beats to acquire the
image data) and an echo-train duration of ~160 ms.
3.4.1. k-Space Undersampling and Pulse Sequence
A different pseudo-random undersampling pattern with higher
density at the center of k-space for each time point was proposed for
applications of compressed sensing to dynamic imaging, in order to
maximize incoherence and reduce the resulting aliasing artifacts by
distributing them along two dimensions (72). We generated a similar 6-fold
accelerated variable-density random undersampling pattern along ky for

72
Figure. 3.4: (a): Six-fold accelerated ky-t undersampling pattern with 16 dynamic frames. (b) Corresponding PSF in the sparse y-PCA space using PCA as the sparsifying transform.
each t, where ky is the spatial frequency in the phase-encoding direction
and t is the echo dimension (Figure 3.4a). Figure 3.4b shows the resulting
point-spread-function (PSF) after applying fast Fourier transform (FFT)
along ky and PCA along t, where ky is the phase-encoding direction. The
ratio of the peak and standard deviation of PSF, which has been proposed
as a measure of incoherence (28), was 31.7.
For the purposes of this work, the ME-FSE pulse sequence with
parallel imaging alone is defined as the reference T2 mapping pulse
sequence, and the ME-FSE pulse sequence with k-t SPARSE-SENSE is
defined as the accelerated T2 mapping sequence. The details of the
reference T2 mapping pulse sequence can be found in (71).
Both the reference and accelerated T2 mapping pulse sequences
were implemented on a whole-body 3T MRI scanner (MAGNETOM

73
TimTrio, Siemens AG, Healthcare Sector, Erlangen, Germany) equipped
with a gradient system capable of achieving a maximum gradient strength
of 45 mT/m and a slew rate of 200 T/m/s. The RF excitation was performed
using the body coil, and a 32-element cardiac coil array (Invivo, Orlando,
FL) was employed for signal reception. Relevant imaging parameters for
both pulse sequences were: field of view = 320 x 320 mm2, slice thickness
= 10 mm, inter-echo spacing = 5 ms, number of images = 16, echo train
length per shot = 32, echo train duration = 163 ms, receiver bandwidth =
531 Hz/pixel, and double-inversion black-blood preparation pulses. As
mentioned previously, the sequence was employed with “reverse centric” k-
space reordering, in which two successive echoes form an image with the
odd and even echoes acquired at the outer and inner halves of k-space,
respectively.
The accelerated T2 mapping pulse sequence used R = 6, acquisition
matrix = 192 x 192 x 16, breath-hold duration = 18 heartbeats (one
heartbeat to acquire the coil sensitivity maps, one heartbeat to acquire
dummy scans to approach steady-state of magnetization, and 16
heartbeats to acquire the image data). The reference T2 mapping pulse
sequence used GRAPPA with R = 1.8, acquisition matrix = 192 x 76, and
breath-hold duration = 21 heat beats (one heart beat to acquire dummy
scans to approach steady-state of magnetization and 20 heart beats to

74
acquire the image data). Note that in order to maintain single breath-hold
duration on the order of 20s, the spatial resolution in the phase-encoding
direction in the reference T2 mapping pulse sequence was set at only 40%
of the resolution achieved in the accelerated T2 mapping pulse sequence.
3.4.2. Phantom Validation
For in vitro validation, we imaged a phantom consisting of five tubes
containing different concentrations of manganese chloride (MnCl2) in
distilled water: 0.135, 0.270, 0.405, 0.540, and 0.675 mM. MnCl2 was
chosen because it has T1/T2 on the order of 10, and these concentrations
were chosen to emulate clinically relevant T2 values in the myocardium.
3.4.3. T2 Mapping of the Heart
Twelve adult volunteers (seven men and five women; mean age =
26.1 ± 1.8 years) were imaged in a middle ventricular short-axis plane.
Electrocardiogram triggering was used to acquire image at middle to late
diastole, where cardiac motion is minimal. Human imaging was performed
in accordance with protocols approved by the New York University School
of Medicine Institutional Review Board and was found to comply with the
HIPAA. All subjects provided written informed consent before the imaging.
3.4.4. Improving Sparsity Using Preconditioning RF Pulses

75
Figure. 3.5: Schematic diagram of the proposed accelerated T2 mapping pulse sequence with preconditioning RF pulses. ECG triggering was used to image at mid to late diastole, to image at a cardiac phase where there is minimal cardiac motion. Three presaturation RF modules and a single fat suppression module were applied before ME-FSE readout.
As discussed in Chapter 2, the performance of compressed sensing
is determined by image sparsity. We hypothesize that suppression of bright
signals (e.g., fat signal) unrelated to the heart increases the sparsity of T2
mapping datasets and thus improve the performance of reconstruction.
Given that the proposed ME-FSE echo train is acquired at middle to late
diastole (~163 ms) per heartbeat, the pulse sequence permits the use of
multiple preconditioning RF pulses before ME-FSE readout (Figure 3.5),
without exceeding clinically acceptable specific absorption rate limit. We
explored the use of fat suppression and spatial pre-saturation RF pulses to
suppress bright signals unrelated to the heart (e.g., chest wall and back).
Note that pulse duration of a spatial pre-saturation module is ~4.8 ms and
that pulse duration of a fat suppression module is ~12.2 ms. Figure 3.6
shows a short-axis scout image to illustrate how preconditioning RF pulses
were utilized to increase the sparsity for cardiac T2 mapping imaging, as
well as the resulting four cases of results with GRAPPA (see Pulse

76
Figure. 3.6: (a): Representative short-axis scout image displaying positions and thicknesses of three presaturation RF pulses (displayed as meshed-strip lines). Resulting images with none (b), fat suppression (c), three spatial presaturation RF pulses (d), and fat suppression plus three spatial presaturation RF pulses (e). The combined use of fat suppression and spatial presaturation RF pulses produced the best suppression of bright signals unrelated to the heart.
Sequence section for the relevant imaging parameters) using different
preconditioning RF pulses: (i) none, (ii) fat suppression only, (iii) three
spatial pre-saturation pulses only, and (iv) fat suppression plus three
spatial pre-saturation RF pulses. The slice thickness of the pre-saturation
bands was graphically adjusted between 50 and 100 mm. Among the four
cases of preliminary results, the combined use of fat suppression and
spatial pre-saturation RF pulses produced the best suppression of bright
signals unrelated to the heart (Figure 3.6). Given the lack of consequential
penalty associated with the combined use of fat saturation and three spatial
pre-saturation pulses, we acquired accelerated T2 mapping images with fat
saturation plus the preconditioning RF pulses. To validate the usefulness of
increasing sparsity with preconditioning RF pulses, we compared both the

77
image quality and T2 accuracy of accelerated data with and without
preconditioning RF pulses.
3.5. Image Reconstruction
The GRAPPA image reconstruction was performed online, using
commercially available reconstruction algorithm. The k-t SPARSE-SENSE
reconstruction was performed offline using customized software developed
in a graphics processing unit (GPU) platform with Compute Unified Device
Architecture programming. The compressed sensing optimization problem
was solved using focal underdetermined system solver (FOCUSS) (73,74).
Temporal PCA was used as the sparsifying transform in k-t SPARSE-
SENSE reconstruction and the PCA basis was calculated and updated in
each iteration of the reconstruction. Using a NVIDIA Tesla GPU with 4 GB
global memory, the total reconstruction time of each dynamic image series
using k-t SPARSE-SENSE was ~1 min.
3.6. Image Analysis and Statistics
3.6.1. Image Analysis
Image analysis was performed using software developed in MATLAB
(MATLAB Statistics ToolboxTM). For each MnCl2 phantom bottle, a mask
covering the whole bottle was manually generated and the corresponding
pixel-by-pixel T2 map was calculated. For in vivo data, both reference and

78
accelerated T2 mapping datasets of all subjects were pooled and
randomized for independent blinded analysis. The left ventricle (LV)
endocardial and epicardial contours were manually drawn to mask the
whole LV. The corresponding pixel-by-pixel T2 map was calculated by
nonlinear least square fitting for three parameters of the monoexponential
signal relaxation equation:
2/2 2 1/2
0( ) ( ) ;
t T
ideal idealS t S S S e
[3.1]
where S(t) is the signal amplitude at time t, Sideal is the ideal signal, and the
three unknown parameters are: the initial signal amplitude (S0), the mean
background noise (σ), and T2. This approximate estimation procedure is
similar to the method of McGibney and Smith (75).
3.6.2. Statistical Analysis
For each bottle of the phantom, the mean transverse relaxation rate
(R2 = 1/T2) was calculated. The five mean R2 measurements were plotted
as a function of MnCl2 concentration, and the transverse relaxivity of MnCl2
was calculated by performing linear regression analysis.
According to the 16-segment model recommended by American
Heart Association, the middle ventricular short-axis view of the myocardium
was divided into six segments including: anterior, anteroseptal, inferoseptal,
inferior, inferolateral, and anterolateral. Statistical analysis was performed

79
using SPSS version 18 (SPSS, Chicago, IL). The mean T2 and segmental
T2 measurements were compared using the paired-sample t-test (two-
tailed). A P < 0.05 was considered to be statistically significant. Reported
values represent mean ± standard deviation. Bland–Altman analysis was
performed to compare T2 measurements obtained using the accelerated T2
mapping pulse sequence and the reference T2 mapping pulse sequence.
To assess the influence of manual segmentation of LV contours on
T2 calculation, we assessed the intra-observer and inter-observer variability
of T2 calculation using the Bland–Altman analysis. For intra-observer
variability assessment, one blinded observer repeated the image analysis
(i.e., contour segmentation and T2 calculation) with 2 weeks of separation
from the first analysis, and Bland–Altman analysis was performed on the
resulting two sets of T2 measurements (analysis 1 vs. analysis 2). Intra-
observer difference was defined as T2 (analysis 1) – T2 (analysis 2). For
inter-observer variability assessment, the second blinded observer
independently analyzed the datasets, and Bland–Altman analysis was
performed on the resulting two sets of T2 measurements (observer 1,
analysis 1 vs. observer 2). Inter-observer difference was defined as T2
(observer 1, analysis 1) – T2 (observer 2).
3.7. Results

80
Figure. 3.7: Representative T2 mapping images acquired using the reference and accelerated T2 mapping pulse sequences: (top row) GRAPPA and (bottom row) k-t SPARSE-SENSE. When compared with GRAPPA, k-t FOCUSS consistently yielded higher spatial resolution in the phase-encoding direction (1.7 x 1.7 mm
2 vs. 1.7 x 4.2
mm2; accelerated vs. reference, respectively).
The two sets of in vitro T2 maps calculated from the reference and
accelerated ME-FSE data sets were in good agreement. The reference and
accelerated T2 maps yielded transverse relaxivities of 88.6 ± 1.2 and 88.3 ±
1.4 s–1/ mM, respectively.
Figure 3.7 shows representative cardiac T2 mapping images
acquired using the reference and accelerated T2 mapping pulse sequences.
The accelerated T2 mapping pulse sequence consistently yielded higher
spatial resolution in the phase-encoding direction (1.7 x 1.7 mm2 vs. 1.7 x
4.2 mm2; accelerated vs. reference, respectively). In all subjects, k-t
SPARSE-SENSE yielded good image quality. Figure 3.8 shows the
corresponding zoomed images and the resulting T2 maps. Mean T2 values

81
Figure. 3.8: Zoomed cardiac T2 mapping images and the T2 maps corresponding to Figure 3.7: (top row) GRAPPA and (bottom row) k-t FOCUSS. When compared with GRAPPA image, k-t FOCUSS image produced higher spatial resolution in the phase-encoding direction, as shown by the intensity profiles of the muscle–blood border.
of this subject calculated from GRAPPA and k-t SPARSE-SENSE images
were 51.7 ± 3.6 and 51.6 ± 4.0, respectively. When compared with the
GRAPPA image, k-t SPARSE-SENSE image yielded higher spatial
resolution, as highlighted by the intensity profiles at the edge of the muscle–
blood border.
For the pool of 12 subjects, mean myocardial T2 values measured by
observer 1 (analysis 1) using the GRAPPA and k-t SPARSE-SENSE data
were 49.9 ± 1.5 and 50.0 ± 1.5, respectively, and they were not significantly
different (P > 0.05). The corresponding mean segmental T2 values are
summarized in Table 3.1, and mean T2 values for every segment were not
significantly different (P > 0.05). These findings are consistent with

82
Myocardium GRAPPA (msec) k-t SPARSE-SENSE (msec)
Anterior 49.1±3.2 48.7±2.6
Anteroseptal 52.0±3.0 51.5±2.8
Inferoseptal 51.4±2.6 51.6±2.9
Inferior 50.3±1.8 49.9±1.9
Inferolateral 50.2±1.5 49.6±2.7
Anterolateral 47.1±1.9 49.1±2.6
Whole Myocardium 49.9±1.5 50.0±1.5
Table. 3.1: Mean Segmental and Whole Myocardial T2 Measurements Obtained Using GRAPPA and k-t SPARSE-SENSE Datasets. Not that these values represent results analyzed by observer 1 and analysis 1.
previously reported T2 measurements of healthy subjects at 3T. These
mean T2 values between GRAPPA and k-t SPARSE-SENSE were not
significantly different (P > 0.05).
According to the Bland–Altman analysis, T2 measurements obtained
from k-t SPARSE-SENSE and GRAPPA images were in excellent
agreement (mean difference = 0.04 ms; upper/lower 95% limits of
agreement were 2.26/-2.19 ms), suggesting that the corresponding T2
measurements are quantitatively equivalent. The corresponding Bland–
Altman statistics for the segmental T2 measurements are summarized in
Table 3.2.
The intra-observer agreements for T2 calculations using the same
set of GRAPPA and k-t SPARSE-SENSE data were -0.18 and 0.04, the
upper 95% limits of agreements were 0.99 and 0.91, and the lower 95%
limits of agreements were -1.34 and -0.83, respectively. The inter-observer

83
Myocardium Difference (msec) Upper 95%
Limit (msec) Lower 95%
Limit (msec)
Anterior -0.40 5.43 -6.23
Anteroseptal -0.52 5.69 -6.72
Inferoseptal 0.21 4.01 -3.60
Inferior -0.36 3.29 -4.00
Inferolateral -0.59 5.31 -6.49
Anterolateral 1.99 8.14 -4.17
Whole Myocardium 0.04 2.26 -2.19
Table. 3.2: Bland–Altman Statistics of T2 Measurements Obtained Using GRAPPA and k-t SPARSE-SENSE Datasets. Note that these values represent results analyzed by observer 1 and analysis 1.
agreements for T2 calculations using the same set of GRAPPA and k-t
SPARSE-SENSE data were 0.36 and 0.35, the upper 95% limits of
agreements were 1.56 and 1.37, and the lower 95% limits of agreements
were -0.83 and -0.68, respectively. These Bland–Altman statistics (Table
3.3) suggest that T2 calculations from a given set of data are highly
repeatable and reproducible.
Figure 3.9 shows examples of cardiac T2 mapping images and the
corresponding T2 map with and without preconditioning RF pulses. For the
latter case, signal heterogeneity was found in the k-t SPARSE-SENSE
reconstruction, particularly in the lateral wall, and the corresponding T2 error
was produced. In this subject, the mean T2 measurements within the
segmented myocardium were 50.0 ± 4.0 ms and 60.8 ± 12.9 ms for with
and without preconditioning RF pulses, respectively. These results are
corroborated with zero-filled FFT reconstruction images which show more

84
Agreement Type Difference (msec) Upper 95%
Limit (msec) Lower 95%
Limit (msec)
Intra (GRAPPA) -0.18 0.99 -1.34
Intra (k-t SPARSE-SENSE) 0.04 0.91 -0.83
Inter (GRAPPA) 0.36 1.56 -83
Inter (k-t SPARSE-SENSE) 0.35 1.37 -0.68
Table. 3.3: Intraobserver and Interobserver Agreements for T2 Calculations Based on Manual Segmentation of LV Contours. Intraobserver difference was defined as T2 (analysis 1)-T2 (analysis 2), and interobserver difference was defined as T2 (observer 1)-T2 (observer 2).
aliasing artifacts for the latter case. These findings clearly demonstrate that
the use of preconditioning RF pulses for k-t SPARSE-SENSE
reconstruction increases sparsity in T2 mapping datasets and thus improve
the accuracy of T2 measurement.
3.8. Discussion
Our results demonstrate the feasibility of performing a 6-fold
accelerated breath-hold cardiac T2 mapping acquisition using k-t SPARSE-
SENSE. When compared with the reference T2 mapping pulse sequence
with GRAPPA, the accelerated T2 mapping pulse sequence with k-t
SPARSE-SENSE produced in vivo results of comparable accuracy. In all
the subjects, k-t SPARSE-SENSE reconstruction consistently produced
good image quality. The intra-observer and inter-observer agreements for
T2 calculations from a given set of images were excellent.
This study demonstrates that the proposed method is a promising

85
Figure. 3.9: Example cardiac T2 mapping image and the corresponding T2 maps with and without preconditioning RF pulses. For the latter case, note the signal heterogeneity in the k-t FOCUSS reconstruction, particularly in the lateral wall, as well as the corresponding T2 error. These results are corroborated with zero-filled FFT reconstruction images which show more residual aliasing artifacts for the latter case. The results clearly demonstrate the usefulness of increasing sparsity in cardiac T2 mapping through the use of preconditioning RF pulses.
investigational tool for myocardial T2 measurement with relatively high
spatial resolution (1.7 x 1.7 mm2). The reconstruction approaches can be
also applied in other application other than cardiac imaging. Preliminary
results for accelerated parameter mapping in musculoskeletal MRI using
the proposed approach have been reported in (76).
Our initial studies also have limitations that warrant discussion. First,
commercially available fat suppression pulse did not completely suppress
the undesirable fat signals. The use of improved fat suppression pulse,
such as chemically selective inversion recovery, should further suppress

86
the fat signal and, subsequently, increase sparsity of cardiac T2 mapping
datasets. Second, we used three spatial pre-saturation pulses before ME-
FSE readout to suppress bright signals outside the heart. More work is
needed to explore the optimal use of spatial pre-saturation pulses (e.g.,
quantity, width, location, and orientation, etc) for maximal suppression of
undesirable background signal. Third, our accelerated T2 mapping pulse
sequence acquired an echo train for ~160 ms during middle to late diastole,
and our data analysis was performed assuming no cardiac motion.
However, even with a perfectly still breath hold, gradual ventricular
relaxation occurs during 160 ms of data acquisition. Advanced image
registration methods could be further used to eliminate this potential source
of error in data fitting for T2 calculation. Fourth, our study was carried out in
a small number of healthy subjects at 3T, without edema or iron overload.
Further studies in a larger number of patients with the whole spectrum of T2
encountered in clinical practice are necessary to fully evaluate the clinical
utility of the accelerated T2 mapping pulse sequence. Fifth, the breath-hold
duration of 18 heartbeats could be still too long for some patients with
impaired breath-hold capacity. In such patients, it may be necessary to
sacrifice some spatial resolution to reduce the breath-hold duration.
3.9. Conclusion

87
In conclusion, the proposed accelerated breath-hold T2 mapping
approach can be used to perform rapid T2 mapping of the heart with
relatively high spatial resolution. The proposed technique is a promising
investigational method for quantitative assessment of myocardial edema
and iron overload, and can be also applied in other organs such as liver, hip
or knee.

88
Chapter 4
Accelerated Real-Time Cardiac Cine MRI Using k-t
SPARSE-SENSE
4.1. Prologue
In the previous chapter, we have demonstrated that k-t SPARSE-
SENSE can be applied for accelerated MR T2 mapping. In this chapter, we
extend the applications of k-t SPARSE-SENSE to cardiac cine imaging,
which is a very important tool for evaluating myocardial function. We
demonstrate that k-t SPARSE-SENSE can be used to achieve 8-fold
accelerated real-time cardiac cine imaging, which allows cardiac exams
during free-breathing.
The contents presented in this chapter were published in the journal
Magnetic Resonance in Medicine (MRM 2013 Jul; 70(1): 64-74) (77).

89
4.2. Introduction
Non-invasive assessment of myocardial function plays an important
role in the management of various cardiac diseases (78-85). Breath-hold
cine MRI with balanced steady-state free precession (bSSFP) readout,
which is now considered the gold standard for imaging myocardial function,
offers good spatial resolution, high blood-to-myocardium contrast, and
exquisite image quality (86). However, in patients with impaired breath-hold
capacity and/or arrhythmias, breath-hold cine MRI may yield non-diagnostic
image quality. In these patients, real-time cine MRI may be more clinically
useful than breath-hold cine MRI (87-97).
Commercially available real-time cine MRI methods using dynamic
parallel imaging, such as TSENSE (21) or TGRAPPA (22), typically yield
relatively low spatio-temporal resolution, due to their poor image acquisition
speed. For example, our clinical real-time cine MRI protocol using
TGRAPPA with acceleration factor (R) = 3 produces 2.5 x 2.5 mm2 spatial
resolution and 114 ms temporal resolution. For patients with tachycardia
(heart rate > 100 bpm) or imaging during stress testing, higher temporal
resolution is desirable.
Many investigational image processing methods, in conjunction with
parallel imaging, have been reported to further accelerate real-time cine
MRI. For example, one method utilizes a Karhunen-Loeve transform filter to

90
improve the performance of TSENSE or TGRAPPA (98). Deformable
registration has been incorporated into the image reconstruction framework
to perform motion compensation (99). Besides, real-time cine MRI can be
also performed with retrospective reconstruction to improve spatio-temporal
resolution, in which multiple cardiac cycles are synchronized and averaged
with motion correction techniques (88,92). However, such retrospective
reconstruction method may not perform well in patients with arrhythmias,
because of its need for averaging results over multiple heart beats.
More advanced investigational image acquisition methods have also
been reported to further accelerate real-time cine MRI. The presence of
spatial and temporal correlations in cardiac cine datasets can be exploited
to further accelerate data acquisition, due to the sparsity in the spatial-
temporal Fourier domain. One such method is the partially separable
function model (100), which has been shown to produce high spatio-
temporal resolution for imaging rat hearts (101). Another method is radial k-
t SENSE (102), which has been shown to yield 8-fold accelerated real-time
cine MR images with 2.3 x 2.3 mm2 spatial resolution and 40 ms temporal
resolution.
An alternative method to further accelerate real-time cine MRI is
compressed sensing (26-28), which has been applied to accelerate breath-
hold cardiac cine MRI (73,74,103). These pioneering works have been

91
important developments but have not been applied for real-time cardiac
cine MRI yet. Real-time cardiac cine MRI is a good candidate for
compressed sensing, because the background is static (due to steady state
of magnetization) and the dynamic region (e.g., heart) is relatively small.
This condition produces a high degree of spatio-temporal correlation, which
could be exploited with an appropriate transform, such as temporal fast
Fourier transform (FFT), temporal principal component analysis (PCA) or
temporal finite differences (also known as temporal total-variation or
temporal TV).
Based on our clinical experiences, we are aiming to achieve spatial
resolution on the order of 2.5 x 2.5 mm2 and temporal resolution on the
order of 40 ms, to produce high-quality real-time cine MR images that could
be applied clinically for wall motion assessment and measurement of global
LV function. In this chapter, k-t SPARSE-SENSE is used to highly
accelerate real-time cine MRI with 8-fold acceleration. The resulting image
quality and global function measurements is compared and validated
against the reference approaches.
4.3. Imaging Strategies
4.3.1. k-Space Undersampling: Incoherence and Self-Calibration of
Coil Sensitivities

92
Figure. 4.1: (a): Eight-fold accelerated ky–t sampling pattern varied along time. (b): A schematic illustrating how the kx–ky–t sampling pattern is averaged over time to produce the resulting kx–ky sampling pattern. This kx–ky pattern represents the sampling used to perform self-calibration of coil sensitivities. White lines represent acquired samples.
The first major component in compressed sensing is incoherent
aliasing artifact due to k-space undersampling. Similar to the studies in
Chapter 3, a random k-space undersampling pattern with higher density at
the center of k-space was applied to achieve a high degree of incoherence
in time-series data, with different undersampling pattern at each time frame,
in order to distribute the resulting aliasing artifacts along both ky, the spatial
frequency in the phase-encoding dimension, and t, the temporal dimension.
An 8-fold accelerated ky-t undersampling pattern, as shown in Figure 4.1a,
was applied in this study. Note that temporal average of the sampling
pattern, kx-ky, represents the sampling used to perform self-calibration of
coil sensitivities, as shown in Figure 4.1b.
4.3.2. Comparison of Sparsifying Transforms

93
The second major component in compessed sensing is sparse
representation of the image with a known transform basis. We performed
retrospective undersampling experiments on fully sampled, breath-held cine
MR datasets (one short-axis (SAX) and one long-axis (LAX)) in order to
determine the optimal sparsifying transform and the corresponding
regularization parameter. The relevant imaging parameters (e.g., spatial
resolution, temporal resolution, receiver bandwidth, and flip angle) were
similar to the proposed real-time cine MRI protocol (see Pulse Sequence
section below). The k-t SPARSE-SENSE reconstruction was performed
using the steps described in the Image Reconstruction section below. This
subsection describes the methods and results of the preliminary
retrospective simulation experiment which was needed for the prospective
acceleration strategies.
4.3.2.1. Primary Sparsifying Transform: Dynamic Region
k-t SPARSE-SENSE reconstruction was first performed on
retrospectively 8-fold undersampled datasets using three different
sparsifying transforms, including temporal FFT, temporal PCA and temporal
TV (see Figure 4.1a for the sampling pattern). The regularization parameter
was determined empirically by comparing between k-t SPARSE-SENSE
images and fully-sampled cine MR images. Our prior cardiovascular MRI
applications of k-t SPARSE-SENSE reported regularization parameter

94
Figure. 4.2: Simulation results comparing the fully sampled reference cardiac cine data to retrospectively eight-fold accelerated k–t SPARSESENSE results with different sparsifying transforms with regularization weight 0.01: temporal FFT, temporal PCA, and temporal TV. (a): In the zoomed view of the heart, temporal TV yielded the lowest RMSE. (b): In the chest wall, temporal FFT yielded the lowest RMSE. (c) and (d): Corresponding plots of RMSE for the heart and chest wall regions, respectively, as a function of regularization weight ranging from 0.005 to 0.05. These results show that temporal TV is superior to the other two sparsifying transforms for the dynamic region, whereas temporal FFT is superior to the other two transforms for the static region. Based on these results, we elected to use temporal TV as the primary sparsifying transform with regularization weight 0.01 and temporal FFT as the secondary transform with regularization weight 0.001.
values ranging from 0.01 to 0.05. Thus, we repeated the experiment with
regularization weight ranging from 0.005 – 0.05 (0.005 increment) and
calculated the root-mean-square-error (RMSE) between k-t SPARSE-

95
SENSE and fully-sampled results. Note that, for each sparsifying transform
per regularization weight, RMSE was calculated for a cropped region
containing mainly the heart. Figure 4.2c shows the plot of RMSE as a
function of regularization parameter for the heart region. Compared with
temporal FFT and temporal PCA, temporal TV yielded lower RMSE, and
regularization weight = 0.01 yielded the minimal RMSE for temporal TV
(see Figure 4.2a). We also performed visual inspection to confirm high
temporal fidelity of myocardial wall motion at weight 0.01. Given these
results, we elected to use temporal TV as our sparsifying transform with
regularization weight 0.01.
4.3.2.2. Secondary Sparsifying Transform: Static Region
We also performed the same analysis on the static region (e.g.,
chest wall). Figure 4.2d shows the plot of RMSE as a function of
regularization parameter. Compared with temporal PCA and temporal TV,
temporal FFT yielded lower RMSE, suggesting that it is superior for
suppression of residual aliasing artifacts arising from the static region.
Therefore, to further suppress residual incoherent aliasing artifacts arising
from the background, we elected to add temporal FFT as a secondary
orthogonal sparsifying transform. The resultant reconstruction algorithm is a
combination of temporal TV and temporal FFT (temporal TV+FFT)), where
the regularization weight for temporal FFT was empirically chosen to be ten

96
Figure. 4.3: Numerical simulation results comparing the (a) fully sampled data (R = 1) to the retrospectively eight-fold undersampled reconstruction results using four different sparsifying transforms: (b) temporal FFT, (c) temporal PCA, (d) temporal TV, and (e) temporal TV + FFT. (First row) end-systolic SAX image, (second row) spatial-temporal profile from the SAX image, (third row) end-systolic LAX image, and (fourth row) spatial-temporal profile from the LAX image. Both temporal FFT and temporal PCA yielded more temporal blurring artifacts within the wall (arrows) than temporal TV and temporal TV + FFT.
times lower than that for temporal TV - small enough to not introduce
temporal blurring artifacts but large enough to help suppress residual
aliasing artifacts arising from the static regions. Given that the regularization
weight for temporal FFT is small (0.001), we did not perform a systematic
search for the optimum value. Note that both temporal TV and temporal
FFT terms were solved simultaneously during image reconstruction.
4.3.2.3. Preliminary Evaluation

97
For completeness, we also performed simulation experiments
comparing the performances of temporal FFT, temporal PCA, temporal TV,
and temporal TV + FFT, using both fully-sampled SAX and LAX datasets as
references. Both temporal FFT and temporal PCA, as shown in Figure
4.3b&c (x-y plane), produced temporal blurring artifact in the myocardial
wall (white arrows). In contrast, both temporal TV and temporal TV + FFT
(Figure 4.3d&e) did not produce the specific temporal blurring artifact. The
signal intensity profiles, through the blood-myocardium boundary, along y-t
were also evaluated for all datasets along the white dotted lines drawn on
Figure 4.3a. These spatial-temporal profiles also show more temporal
blurring artifacts for the temporal FFT and temporal PCA than temporal TV
and temporal TV+FFT. To further evaluate the temporal fidelity, the
reconstructed SAX (4 cases) and LAX (4 cases) datasets were randomized
for blind evaluation by 4 readers: two cardiologists, one pediatric
cardiologist, and one radiologist. Each reader independently ranked the
temporal fidelity of myocardial wall motion (1-4: highest-lowest). The
results, averaged over 4 readers, showed that both temporal TV+FFT (1.9)
and temporal TV (2.0) produced better temporal fidelity of myocardial wall
motion than temporal FFT (2.9) and temporal PCA (3.0). Based on these
preliminary results, we elected to use temporal TV + FFT as the sparsifying
transform for accelerated real-time cine MR data reconstruction.

98
Figure. 4.4: Numerical simulation results (top row: end-diastolic images, middle row: end-systolic images, bottom row: spatial-temporal plots through the blood-myocardium boundary) comparing different R values using temporal TV with weight 0.01 and temporal FFT with weight 0.001: (first column) R = 1, (second column) R = 2, (third column) R = 4, (fourth column) R = 6, (fifth column) R = 8, and (sixth column) R = 10. These results suggest that good results can be obtained up to R = 8.
4.3.3. Comparison of Acceleration Rates
To determine the maximal acceleration with acceptable image
quality, we performed repeated undersampling simulation with different
acceleration rates ranging from 2-10, where temporal TV with regularization
parameter 0.01 and temporal FFT with regularization parameter 0.001 were
used for k-t SPARSE-SENSE reconstruction. Figure 4.4 shows the end-
diastolic and end-systolic images for the different accelerations, as well as
their corresponding spatial-temporal plots through the blood-myocardium
boundary. These results show that good results can be obtained up to R =
8. Based on this preliminary experiment, we elected to use R =8 for
prospective accelerated acquisitions.

99
4.4. Imaging Studies
4.4.1. Pulse Sequence
Our proposed 8-fold accelerated, real-time cine MRI sequence was
implemented on a whole-body 3T MRI scanner (MAGNETOM TimTrio,
Siemens AG, Healthcare Sector, Erlangen, Germany). A 6-element body
matrix coil array and a spine coil array (with only 6 elements on) were
employed for signal reception.
The relevant imaging parameters for real-time cine were: field of
view = 300 x 300 mm2, acquisition matrix size = 128 x 128, spatial
resolution = 2.3 x 2.3 mm2, slice thickness = 8 mm, flip angle = 40o,
repetition time / echo time = 2.7/1.37 ms, receiver bandwidth = 1184
Hz/pixel, and temporal resolution = 43.2 ms. The total scan time was 2
heart beats per slice, with 1 heart beat to achieve steady-state of
magnetization, and another heart beat to acquire the cine data.
The relevant imaging parameters for breath-hold cine MRI were: field
of view = 300 x 300 mm2, acquisition image matrix = 192 x 192, spatial
resolution = 1.6 x 1.6 mm2, slice thickness = 8 mm, flip angle = 40o,
retrospective electrocardiogram (ECG) gating with 25 reconstructed cardiac
phases, receiver bandwidth = 1300 Hz/pixel, and 1.6-fold acceleration with
GRAPPA.
4.4.2. Cardiac Imaging

100
Twelve healthy human volunteers with no known cardiac disease (11
males and 1 female; mean age = 26.2 ± 2.7 years) and one male patient
(age = 45 years) with history of heart transplantation were imaged using
both real-time cine and breath-hold cine MRI sequences, to perform pre-
clinical testing and confirmation of comparability of global function
measurements with breath-hold cine MRI. Fifteen consecutive clinical
patients (7 males and 8 females; mean age = 49 ± 21 years) were recruited
for image quality assessment of real-cine MRI in a clinical setting. Human
imaging was performed in accordance with protocols approved by the New
York University School of Medicine Institutional Review Board and was
found to comply with the HIPAA. All subjects provided written informed
consent before the imaging.
4.4.2.1. Experiment I: Image Quality and Global Function
Measurement Comparison (real-time vs. breath-hold cine MRI)
In the first experiment, twelve healthy human volunteers were
imaged using both pulse sequences in a stack of 12 short-axis planes
covering the entire LV, in order to compare their resulting image quality
(only three views; base, mid, and apex) and global function measurements
including end diastolic volume (EDV), end systolic volume (ESV), stroke
volume (SV), and ejection fraction (EF). Real-time cine imaging of the entire
LV was performed during free breathing with prospective ECG triggering,

101
and breath-hold cine imaging was performed with 6 separate breath-holds
(2 slices per breath-hold) with retrospective ECG gating.
4.4.2.2. Experiment II: Comparison of LV Function by Real-time Cine
MRI with prospective ECG triggering vs. Breath-hold Cine MRI with
Retrospective ECG gating
In the second experiment, one male patient with history of heart
transplantation was imaged to compare global function measurements
between two different end-diastolic frames for real-time cine MRI with
prospective ECG triggering. We note that in prospective ECG triggering, it
may be difficult to capture true end diastole, which may lead to
underestimation of EDV, SV and EF when compared with retrospective
ECG gated acquisitions. In this patient, we imaged a stack of 14 short-axis
planes covering the entire LV, for 2 heart beats, in order to capture true end
diastole between the first and second heart beats with prospectively ECG
triggered real-time cine MRI. We calculated two sets of global function
measurements from this data set: i) first frame defined as end-diastole and
ii) visually identified end-diastolic frame, acquired between the first and
second heart beats. For reference, another stack of 14 short-axis slices
were acquired using breath-hold cine MRI with retrospective ECG gating.
4.4.2.3. Experiment III: Clinical application of real-time Cine MRI

102
Figure. 4.5: (a): Coil sensitivities calculated using an (left column) external reference acquisition (pre-scan) and (right column) self-calibration method. (b): The resulting k–t SPARSE-SENSE images using externally and self-calibrated coil sensitivities. Note that two sets of data are very similar, suggesting that our self-calibration of coil sensitivities was robust.
Fifteen patients (7 males and 8 females; mean age = 49 ± 21 years)
were recruited to evaluate the performance (e.g., image quality, wall
motion, artifacts) of our proposed real-time cine MRI pulse sequence. For
patient recruitment, the only inclusion criterion was normal sinus rhythm,
and our patient population included different cardiac disease conditions.
Given that our study was not aimed at a particular clinical indication, only
one cardiac view was acquired per patient (12 patients had SAX, 3 patients
had LAX).
4.5. Image Reconstruction
K-t SPARSE-SENSE reconstruction was performed off-line in
MATLAB (R2011b software; Mathworks, Natick, MA). The coil sensitivity

103
maps were self-calibrated by averaging undersampled k-space data over
time (see Figure 4.1b, Figure 4.6a) and computed using the adaptive array-
combination technique (40). This subsection describes the results of the
preliminary experiment to demonstrate that the self-calibration of coil
sensitivities is robust. We acquired a data set with external coil calibration
data, and compared the results using external and self-calibrated coil
sensitivities. Figure 4.5 shows a comparison between self-calibrated and
externally acquired (as a pre-scan) coil sensitivities, as well as their
resulting k-t SPARSE-SENSE images. Note that the two sets of data are
similar. The benefits of self-calibrated coil sensitivities are that they are
intrinsically registered with the undersampled data and do not require
additional time for acquisition.
For the k-t SPARSE-SENSE reconstruction, the optimization
problem (Figure 4.6b) was solved iteratively using a non-linear conjugate
gradient algorithm originally proposed in (28). The overall flowchart of the
image reconstruction is illustrated in Figure 4.6. Reconstruction time per
slice was about 4.6 min in a server equipped with an Intel Xeon CPU at
2.27 GHz with 24 GB RAM.
4.6. Image Analysis and Statistics
4.6.1. Image Analysis

104
Figure. 4.6: Schematic flowchart of the image reconstruction method. (a): Coil sensitivity maps were self-calibrated by averaging undersampled k-space data over time and computed using the adaptive array combination method. (b): Multicoil, zero-filled k-space data, along with the corresponding coil sensitivity maps, were reconstructed using both temporal TV and temporal FFT as the sparsifying transforms, where regularization weight of temporal TV is 10 times larger than that for temporal FFT.
For each subject, three slices (apex, mid, base) were selected from
both real-time and breath-hold cine sets for image quality assessment. A
total of 72 (36 real-time cine; 36 breath-hold cine) datasets were pooled and
randomized for blinded qualitative evaluation by four readers described
previously. Readers independently scored the image quality (1=non-
diagnostic, 2=poor, 3=adequate, 4=good, 5=excellent), temporal fidelity of
myocardial wall motion (1=non-diagnostic, 2=poor, 3=adequate, 4=good,
5=excellent), and artifact level (1=none, 2=mild, 3=moderate, 4=severe,
5=non-diagnostic).

105
For global function assessment, 24 (12 real-time cine; 12 breath-hold
cine) short-axis stacks of cine datasets were pooled and randomized for
blinded quantitative evaluation. The same 4 readers independently
calculated the EDV, ESV, SV, and EF for each data set.
For comparison of prospective ECG triggered real-time cine MRI and
retrospective ECG gated breath-hold cine MRI, one cardiologist analyzed a
short-axis stack of real-time cine MRI data with prospective ECG triggering
using two different end diastolic frames (1 and 16, where frame 16 was
visually defined as the true end diastole) and compared their global function
measurements with those obtained using a stack of breath-hold cine MR
data with retrospective ECG gating.
For evaluation of real-time cine MRI in patients, 15 cine datasets
were pooled and randomized for blinded evaluation. The same four readers
independently scored the image quality, temporal fidelity of myocardial wall
motion and artifact for each data set.
4.6.2. Statistical Analysis
For image quality comparison, the reported scores, which were
averaged over four readers, represent mean ± standard deviation.
Statistical analysis was performed using Excel (Microsoft Corporation,
Redmond, WA). Wilcoxon signed-rank sum test was used to compare the

106
Figure. 4.7: (Rows 1–2) End-diastolic and (rows 3–4) end-systolic images at multiple cardiac phases comparing (rows 1 and 3) breath-hold cine MRI and (rows 2 and 4) real-time cine MRI. Both image sets were acquired from a 29-year-old (male) healthy subject. Note that the breath-hold cine MR images had higher spatial resolution than the real-time cine MR images (1.6 mm
2 vs. 2.3 mm
2, respectively).
mean scores between two groups, where P < 0.05 was considered to be
statistically significant.
For global function comparison, Bland-Altman and coefficient of
variation (CV) analysis were performed. In addition, inter-observer
variability within each pulse sequence was also assessed by inter-class
correlation (ICC).
4.7. Results
4.7.1. Experiment I

107
Figure. 4.8: Bland–Altman plots illustrating good agreement between breath-hold cine MRI and real-time cine MRI for the following LV function measurements: (top, left) EDV (mean difference = 15.2 mL [solid line]; lower and upper 95% limits of agreement = 27.6 and 2.8 mL [dashed lines], respectively), (top, right) ESV (mean difference = 2.1 mL [solid line]; lower and upper 95% limits of agreement = 4.7 and 8.9 mL [dashed lines], respectively), (bottom, left) SV (mean difference = 17.3 mL [solid line]; lower and upper 95% limits of agreement = 31.3 and 3.3 mL [dashed lines], respectively), and (bottom, right) EF (mean difference = 5.7% [solid line]; lower and upper 95% limits of agreement = 11.3% and 0.1% [dashed lines], respectively).
Figure 4.7 shows representative sets of real-time cine MR images
and breath-hold cine MR images, in five short axis slices from one healthy
subject. Both breath-hold and real-time images produced good diagnostic
overall image quality. Table 4.1 shows the mean scores of image quality,
temporal fidelity of wall motion and artifact level for breath-hold cine and
real-time cine results (n=36). Compared with breath-hold cine, real-time

108
Sequence Image Quality Temporal Fidelity
of Wall Motion Artifact
Breath-Hold 4.6±0.5 4.7±0.4 1.4±0.6
Real-Time 3.5±0.5 4.5±0.4 2.3±0.5
Table. 4.1: Mean scores of image quality, temporal fidelity of wall motion and artifact, produced by Breath-Hold cine MRI and Real-Time cine MRI.
cine yielded significantly (P < 0.05) worse scores for all four categories.
However, for real-time cine MRI, the image quality and temporal fidelity of
wall motion scores were above 3.0 (adequate) and artifacts and noise
scores were below 3.0 (moderate), suggesting that acceptable diagnostic
image quality can be achieved. According to the Bland-Altman (Figure 4.8)
and CV analysis (Table 4.2), all four global function measurements,
averaged over 4 readers, were in good agreement, with CV less than 10%.
The inter-class correlation (Table 4.3) shows that the inter-observer
variability in calculating global function measurements ranged from
moderate to strong for real-time cine MRI and moderate to near perfect for
breath-hold cine MRI.
4.7.2. Experiment II
Figure 4.9 shows two potential candidates for an end-diastolic frame
from the same series of mid-ventricular short-axis images acquired with
prospective ECG triggering. In this example, the first candidate is cardiac
frame 1, and the second candidate is cardiac frame 16 (denoted as frame N
in the Figure). Note that cardiac frame 16 shows larger LV cavity than

109
Measurement Mean Mean
Difference Upper
95% Limit Low 95%
Limit CV(%)
EDV 143 mL -15.2 mL -2.8 mL -27.6 mL 6.22
ESV 55.7 mL 2.1 mL 8.9 mL -4.7 mL 4.42
SV 87.3 mL -17.3 mL -3.3 mL -31.3 mL 8.79
EF 0.61 -5.7% -0.1% -11.3% 4.68
Table. 4.2: Bland–Altman and CV analyses of four global function measurements between Real-Time and Breath-Hold cine MRI pulse sequences.
Measurement ICC (BH) ICC (RT)
EDV 0.88 0.78
ESV 0.76 0.77
SV 0.76 0.64
EF 0.64 0.64
Table. 4.3: ICC analysis of interobserver variability of EDV, ESV, SV, and EF within each pulse sequence type. ICC scale: 0-0.2 indicates poor agreement, 0.3-0.4 indicates fair agreement, 0.5-0.6 indicates moderate agreement, 0.7-0.8 indicates strong agreement, and >0.8 indicates almost perfect agreement.
cardiac frame 1. In the male patient with heart transplantation, defining
cardiac frame 1 as end diastole produced EDV = 86ml, ESV = 44ml, SV =
42ml, and EF = 49%. Defining cardiac frame 16 as end diastole produced
EDV = 94ml, ESV = 44ml, SV = 49ml, and EF = 53%. The reference breath-
held cine MRI with retrospective ECG gating yielded EDV = 99ml, ESV =
44ml, SV = 55ml, and EF = 56%. This comparison shows that the proposed
prospective ECG triggered approach of acquiring real-time cine MR data
through 2 heart beats would ensure capture of true end diastole.
4.7.3. Experiment III

110
Figure. 4.9: Proposed real-time cine MRI protocol with prospective ECG triggering to capture true end diastole, where images are continuously acquired through the second R-wave to visually identify true end diastole. This proposed approach produced global function measurements in excellent agreement with breath-hold cine MRI with retrospective ECG gating.
Figure 4.10 shows representative real-time cine MR images in two
different patients in different cardiac imaging planes. Real-time cine MRI
with k-t SPARSE-SENSE consistently yielded high-quality images in all
patients. The mean scores of image quality, temporal fidelity and artifact
were 3.7 ± 0.6, 4.3 ± 0.7 and 1.7 ± 0.7, which are similar to the
corresponding scores from volunteer data. Again, the image quality and
temporal fidelity of wall motion scores were above 3.0 (adequate) and the
artifact scores was below 3.0 (moderate).
4.8. Discussion

111
Figure. 4.10: Representative end-diastolic and end-systolic real-time cine images: (top row) SAX view of a 26-year-old (female) patient and (bottom row) LAX view of a 36-year-old (male) patient.
This work demonstrates the feasibility of performing 8-fold
accelerated real-time cine MRI using k-t SPARSE-SENSE, by exploiting a
high degree of spatiotemporal correlation in cardiac cine MRI data. Our 8-
fold accelerated real-time cine MRI protocol can achieve adequate spatial
resolution of 2.3 x 2.3 mm2 and relatively high temporal resolution of 43.2
ms for global cardiac function assessment, with diagnostically acceptable
image quality and high temporal fidelity. This work also demonstrates an
approach to capture end diastole with prospective ECG triggering, by

112
continuously performing real-time cine MRI through the second heart beat
and visually identifying the end-diastolic frame.
While real-time cine MRI yielded significantly worse image quality,
temporal fidelity and artifact scores compared with breath-hold cine MRI,
the image quality and temporal fidelity scores were above 3.0 (adequate),
and artifact score was below 3.0 (moderate). This trend was also true in 15
patients examined. Meanwhile, the temporal fidelity scores were above 4.0
(good) in both healthy subjects and patients. Temporal fidelity of myocardial
wall motion is particularly important to assess regional wall motion
abnormalities in the context of coronary artery diseases.
Previously reported k-t acceleration methods, such as k-t GRAPPA
(24), k-t SENSE (23), and PEAK-GRAPPA (104), also exploit
spatiotemporal correlations in the time series in combination with coil
sensitivities. However, sparsity and coil sensitivity encoding are exploited in
a different way than in k-t SPARSE-SENSE. These k-t acceleration
methods take advantage of sparsity to reduce signal overlap in the sparse
domain due to regularly undersampled data and perform a linear
reconstruction to reconstruct the sparse representation of the images using
prior information on this sparse representation and coil sensitivity
information. These linear algorithms are computationally less demanding.
Acceleration is achieved at the expense of signal-to-noise ratio and residual

113
coherent aliasing artifacts, and additional training data are usually needed
to learn the sparse representation. In contrast, a non-linear reconstruction is
used in k-t SPARSE-SENSE to recover the sparse signal coefficients
contaminated by incoherent aliasing artifacts produced by an irregular
(pseudo-random) undersampling pattern. This non-linear reconstruction is
computationally more demanding. Acceleration is achieved at the expense
of residual incoherent aliasing artifacts and loss of low signal coefficients in
the sparse domain, and it does not require training data.
The proposed 8-fold accelerated real-time cardiac cine method is a
promising investigational tool for rapid imaging of myocardial function,
particularly for patients with impaired breath-hold capacity, arrhythmias
and/or tachycardia. While this new pulse sequence may be clinically useful,
we describe several issues that warrant discussion below.
First, a combination of temporal TV and temporal FFT was utilized as
sparsifying transforms in this work, where the regularization weight for
temporal TV was empirically set to be ten times larger than that for the
temporal FFT. We note that the use of temporal FFT as a secondary
sparsifying transform with a low regularization weight reduces residual
incoherent aliasing artifacts. Temporal FFT and temporal PCA are good
sparsifying transforms to reduce aliasing artifacts because artifacts are
spread incoherently over the entire y-f space and y-PCA space,

114
respectively. They also exploit the correlation and redundancy over the
whole dynamic series. However, some signal coefficients with small signal
intensity are also suppressed along with incoherent aliasing artifacts, and
this leads to temporal blurring artifacts, as shown in Figure 4.3b&c.
Temporal TV, on the other hand, exploits temporal correlation by taking the
gradient of two adjacent temporal frames, producing less temporal blurring
than temporal FFT and temporal PCA, as shown in Figure 4.3d&e.
Second, we observed that regularization parameters in k-t SPARSE-
SENSE are crucial. For example, larger parameters produce less residual
artifacts at the expense of temporal blurring, and vice versa. In the current
implementation, we did not apply any rigorous mathematical criteria to
systematically select the regularization parameter. Instead, they were
determined empirically based on numerical analysis. This empirical
approach is based on our prior compressed sensing work in cardiovascular
MRI applications, where a fully sampled dataset was retrospectively
undersampled and reconstructed to “fine tune” the regularization parameter.
Third, compared with breath-hold cine MRI using retrospective ECG
gating, our accelerated real-time cine MRI with prospective ECG triggering
with cardiac frame 1 defined as end diastole underestimated EDV, SV, and
EF, because of the finite time needed to detect the ECG trigger and acquire
an image. We have proposed an alternative approach to overcome this

115
limitation in the future studies, by acquiring real-time cine data with
prospective ECG triggering for 2 heart beats and visually identifying a frame
that best represents end diastole (Figure 4.9).
Fourth, our study was carried out in a small number of healthy
volunteers and patients with cardiac disease and no arrhythmias. Further
studies in a larger cohort of patients with a variety of heart disease
encountered in clinical practice are necessary to fully evaluate the clinical
utility of the proposed accelerated real-time cine MRI. Sixth, we performed
real-time cine MRI during free breathing. As such, our LV function
measurements may be contaminated with respiratory motion. We note that
this is an issue for all other real-time cine MRI methods performed during
free breathing as well. One possible solution to minimize this problem is to
perform imaging with breath-hold. Lastly, the current implementation of k-t
SPARSE-SENSE performs the reconstruction of each slice series serially.
Parallel computing could be used to reduce the reconstruction time in
further works.
4.9. Conclusion
In conclusion, 8-fold real-time cine MRI with k-t SPARSE-SENSE
can be used to achieve adequate spatial resolution (2.3 x 2.3 mm2) and
relatively high temporal resolution (43 ms), with good image quality and
relatively accurate global function measurements. This 8-fold accelerated

116
real-time cine MRI method may be useful for patients with reduced breath-
hold capacity, arrhythmia, and/or tachycardia for qualitative assessment of
wall motion and quantitative assessment of LV function.

117
Chapter 5
Golden-Angle Radial Sparse Parallel MRI: Combination of
Compressed Sensing, Parallel Imaging, and Golden-Angle
Radial Sampling for Fast and Flexible Dynamic Volumetric
MRI
5.1. Prologue
In the previous two chapters, we have demonstrated the
performance of k-t SPARSE-SENSE for accelerated cardiac T2 mapping
and real-time cardiac cine MRI with Cartesian sampling. The required
incoherence was achieved using variable density random undersampling.
K-t SPARSE-SENSE has also been successfully implemented for several
additional applications (105,106). However, the performance of compressed
sensing using Cartesian sampling is fundamentally limited, since the
frequency-encoding dimension is usually fully sampled and thus

118
incoherence can only be exploited along the phase-encoding dimension.
Cartesian sampling, moreover, is sensitive to respiratory motion and the
results can be corrupted by ghosting artifacts or blurring. In this chapter, we
extend the reconstruction framework of k-t SPARSE-SENSE into radial
sampling and develop a new reconstruction approach called Golden-angle
RAdial Sparse Parallel MRI (GRASP), which combines compressed
sensing and parallel imaging with golden-angle radial sampling. We will
demonstrate that GRASP allows a simple and flexible means of performing
rapid dynamic MRI for a variety of clinical applications.
The contents presented in this chapter were published in the journal
Magnetic Resonance in Medicine (MRM 2014 Sep;72(3):707-17) (107), In
addition, Applications of GRASP were published in 1 paper in the Journal
Investigative Radiology (108) and 1 paper in the journal of Magnetic
Resonance Imaging (JMRI) (109) .
5.2. Introduction
Dynamic MRI requires rapid data acquisition to provide an
appropriate combination of spatial resolution, temporal resolution, and
volumetric coverage for clinical studies. For example, rapid imaging speed
is needed for dynamic contrast-enhanced (DCE) examinations, in which
fast signal-intensity changes must be monitored during the passage of the
contrast agent (110,111). As discussed in Chapter 1, a variety of fast MRI

119
techniques have been developed over the last two decades to accelerate
the data acquisition. These methods include various parallel imaging
techniques, k-t acceleration techniques, and many others.
Compressed sensing is becoming as a powerful approach to
accelerate data acquisition in dynamic MRI. Compressed sensing methods
exploit spatial and temporal correlations by employing irregular
undersampling schemes to create incoherent aliasing artifacts and using a
non-linear reconstruction to enforce sparsity in a suitable transform domain.
As seen in previous two chapters, incoherent aliasing artifacts are often
created using Cartesian k-space trajectories with random undersampling
patterns. However, because undersampling is only performed along the
phase-encoding dimension, the incoherence achievable in this way is
relatively low, which limits the performance of compressed sensing. Radial
k-space trajectories are an interesting alternative due to the inherent
presence of incoherent aliasing in multiple dimensions, even for regular
(non-random) undersampling. Moreover, radial sampling is known to have
less sensitive to motion, which improves capturing dynamic information
(50,112). When acquiring radial data according to the golden-angle ordering
scheme (113), where the angle of the radial lines is increased continuously
by 111.25°, a rather uniform coverage of k-space with high temporal
incoherence is obtained for any arbitrary number of consecutive lines. This

120
Figure. 5.1: (a) Continuous acquisition of radial lines with stack-of-stars golden-angle scheme in GRASP. (b) Point spread function (PSF) of an undersampled radial trajectory with 21 golden-angle spokes and 256 sampling points in each readout spoke for a single element coil (top) and for a sensitivity-weighted combination of 8 RF coil elements (bottom). The Nyquist sampling requirement is 256*π/2≈402. The standard deviation of the PSF side lobes was used to quantify the power of the resulting incoherent artifacts (pseudo-noise) and incoherence was computed using the main-lobe to pseudo-noise ratio of the PSF.
enables dynamic imaging studies using continuous data acquisition and
retrospective reconstruction of image series with arbitrary temporal
resolution by grouping different numbers of consecutive radial lines into
temporal frames.
In this work, the framework of k-t SPARSE-SENSE is extended to
golden-angle radial acquisitions and demonstrated for various clinical

121
dynamic imaging applications, including free-breathing liver DCE MRI,
pediatric body MRI, breast and neck imaging. The performance of the
proposed approach, entitled Golden-angle RAdial Sparse Parallel MRI
(GRASP), is compared to reconstructions with coil-by-coil compressed
sensing and parallel imaging alone.
5.3. Golden-Angle Radial Sampling
Continuous 3D data acquisition was implemented using a stack-of-
stars k-space trajectory, where Cartesian sampling is employed along the
partition dimension (kz) and golden-angle radial sampling is employed in the
kx-ky plane, as summarized in Figure 5.1a. The golden-angle acquisition
scheme (113), which has previously been applied for accelerated dynamic
imaging, ensures approximately uniform coverage of k-space for any
arbitrary number of consecutive spokes, in particular if the number belongs
to the Fibonacci series (defined as F(k+2) = F(k) + F(k+1), where k ≥ 0, and
F(0) = 0 and F(1) = 1, e.g. 1,2,3,5,8,13,21,34,…). Figure 5.1b shows the
point spread function (PSF) for a golden-angle radial acquisition with 21
spokes using a single element receiver coil (top) and a sensitivity-weighted
combination of 8 RF coil elements (bottom). The PSF for the single coil is
calculated by performing gridding on a simulated k-space matrix with ones
along an undersampled radial trajectory with 21 golden-angle spokes and
256 sampling points along each spoke, followed by an inverse nonuniform

122
fast Fourier transform (NUFFT) operation. The Nyquist sampling
requirement for this case is 256*π/2≈402, corresponding to a simulated
acceleration rate of 19.1. As mentioned in previously chapters, the PSF is
indicative of the degree of incoherence associated with particular
undersampling prior to the compressed-sensing reconstruction. The PSF of
the 8-coil acquisition with identical acceleration was computed using the
multicoil SENSE model, which performs a sensitivity-weighted combination
of individual PSFs using simulated sensitivity maps. The resulting
incoherence, which was computed as the ratio of the main-lobe to the
standard deviation of the side-lobes in the PSF, was 83.1 for the single-coil
case and 106.9 for the 8-coil case. As shown in the Figure 5.1b, the use of
the multicoil SENSE model reduces the side-lobes, which correspond to
aliasing artifacts due to undersampling. The higher encoding capabilities
provided by the coil array therefore are expected to improve the
performance of compressed sensing.
5.4. GRASP Reconstruction
Figure 5.2 shows the GRASP reconstruction pipeline. Since the kz
dimension is uniformly sampled, a fast Fourier transform (FFT) is applied
along this dimension to enable slice-by-slice reconstructions, which reduces
the computational burden and enables straightforward parallelization of the
reconstruction. Coil sensitivity maps are computed with the adaptive array-

123
Figure. 5.2: GRASP reconstruction pipeline. (a) Estimation of coil sensitivity maps in the image domain, where the multicoil reference image (x-y-coil) is given by the coil-by-coil NUFFT reconstruction of the composite k-space data set that results from grouping all the acquired spokes. (b) Reconstruction of the image time-series, where the continuously acquired data are first re-sorted into undersampled dynamic time series by grouping a number of consecutive spokes. The GRASP reconstruction algorithm is then applied to the re-sorted multicoil radial data, using the NUFFT and the coil sensitivities to produce the unaliased image time-series (x-y-t).
combination technique (40) using coil-reference data from the temporal
average of all acquired spokes, which is usually fully sampled as shown in
Figure 5.2a. Afterwards, the continuously acquired radial spokes are re-
sorted by grouping a Fibonacci number (e.g., 34, 21, or 13) of consecutive
spokes to form each temporal frame with the desired temporal resolution.
The GRASP reconstruction is formulated as follows:
2
2 1argmin
x
x F C x y S x [5.1]
where x is the image series to be reconstructed in x-y-t space, S is the
sparsifying transform (temporal finite differences, also known as temporal

124
total-variation or temporal TV in this work) imposed on the L1 norm,
1
n
y
y
y
are the acquired multicoil radial k-space data with n coils, F is the
NUFFT operator defined on the radial acquisition pattern,
1
n
c
c
c
are the
coil sensitivity maps in x-y space, and is the regularization weight that
controls the tradeoff between parallel imaging data consistency and
sparsity. A ramp filter in the kx-ky plane was applied to each spoke to
compensate for variable density sampling.
5.5. Reconstruction Implementation
5.5.1. Implementation of the Reconstruction Algorithm
The GRASP reconstruction was initially implemented in customized
software developed in MATLAB (Mathworks, MA), using a tailored version
of the non-linear conjugate gradient algorithm originally proposed in (28).
In order to achieve reconstruction times that allow for more practical
evaluation in clinical settings, the reconstruction was also implemented as a
stand-alone application using the C++ language. Several algorithmic
optimizations were incorporated to achieve high reconstruction speed. First,
a channel-compression procedure was applied to reduce the amount of k-

125
space data, which combined the receiver channels into eigenmodes based
on a principal component analysis and discarded higher-order modes such
that 95% of the signal power was preserved (114). Second, the
reconstruction was parallelized across slices using the OpenMP framework
(115), yielding an almost linear reduction of the reconstruction time with the
number of processor cores. The NUFFT was implemented via convolution
with a Kaiser-Bessel kernel. Interpolation coefficients were pre-calculated
and shared across threads. Corner rounding was applied to allow for
differentiation of the TV L1 norm.
5.5.2. Selection of Reconstruction Parameters
To determine the optimal weighting parameter , the performance of
several values was first evaluated on one representative dataset for one
temporal resolution and then adjusted for other temporal resolutions
according to the difference in aliasing artifacts (pseudo-noise). First,
GRASP reconstructions were performed using different weights ranging
from 0.01* M0 to 0.1* M0 (step size 0.01), where M0 was the maximal
magnitude value of the NUFFT images that are also used to initialize the
GRASP reconstruction, for the case of 21 spokes per temporal frame. An
adequate value for was selected by an experienced radiologist, who
identified the appropriate value corresponding to the adequate balance
between preservation of fine detail and residual noise or pseudo-noise

126
level, and also evaluated the signal intensity of regions of interest (ROI)
along time. The parameter for different temporal resolutions was then
obtained with 21 21/ *
tA A , where t
A is the pseudo-noise at the target
temporal resolution and 21A is the pseudo-noise at 21 spokes per frame.
The pseudo-noise was computed as described before. In this way, higher
temporal resolutions (or equivalently, use of fewer spokes for each temporal
frame) will be regularized more strongly, proportionally to the higher level of
pseudo-noise. This parameter estimation procedure needs to be performed
only once for a certain target temporal resolution and application, and the
value can then be used for different temporal resolutions and applications.
5.6. Imaging Applications
GRASP dynamic imaging was clinically implemented and evaluated
for a variety of representative imaging applications, as described in the
subsequent subsections. Human imaging was performed in accordance
with protocols approved by the New York University School of Medicine
Institutional Review Board and was found to comply with the HIPAA. All
subjects provided written informed consent before the imaging.
5.6.1. Dynamic Contrast-Enhanced Liver Imaging
DCE liver MRI was performed in six healthy volunteers (age
34.5±5.2 years) and seven patients (age 51±8.4 years) in axial orientation

127
during free breathing using whole-body 3T or 1.5T scanners (MAGNETOM
Verio / Avanto, Siemens AG, Healthcare Sector, Erlangen, Germany) with a
combination of body-matrix and spine coil elements with 12 channels in
total. Data acquisition was initiated simultaneously with intravenous
injection of 10 ml of gadopentate dimeglumine (Gd-DTPA) (Magnevist,
Bayer Healthcare, Leverkusen) followed by a 20-ml saline flush, both
injected at a rate of 2 ml/second. A radial stack-of-stars 3D Fast Low Angle
SHot (FLASH) pulse sequence with golden-angle ordering was employed
for the data acquisitions. Two-fold readout oversampling was applied to
avoid spurious aliasing along the spokes. All partitions corresponding to
one radial angle were acquired sequentially before moving to the next
angle. The ordering scheme along kz was switched between linear (from
kz=-kxmax/2 to kz=+kmax/2) and centric out (starting at kz=0) depending
on the number of slices, as done in most of the modern 3D gradient echo
(GRE) sequences. Frequency-selective fat suppression was used and 60
initial calibration lines were acquired to correct system-dependent gradient-
delay errors as described in (116). Relevant imaging parameters are listed
in Table 5.1.
5.6.2. Dynamic Contrast-Enhanced Pediatric Body Imaging
Abdominal DCE MRI was performed in five pediatric patients (age
4.8±4.1 years) in axial orientation on a 1.5T scanner (MAGNETOM Avanto,

128
DCE Liver DCE Pediatrics DCE Breast DCE Neck
#Sampling in Each Readout (2x)
512~768 512 512 512
#Partitions 29~40 48 35 69
#Spokes in Each Partition
600~800 800 2280 800
Slice Thickness (mm)
3 3 2 2
FOV (mm2) 370x370 250x250 270x270 256x256
TR/TE (ms) 3.83/1.71 4.24/2.07 3.6/1.47 4.57/2.06
Flip Angle (Degree) 12 12 12 12
Acquisition Time (s) 90 193 331 283
Table. 5.1: Representative imaging parameters of dynamic volumetric MRI in different applications.
Siemens AG, Healthcare Sector, Erlangen, Germany) using a body/spine
coil array with 12 elements. Acquisitions were performed during free
breathing because the patients were sedated during the exam. The imaging
and contrast-injection protocols were comparable to the liver example
described above. Relevant parameters are listed in Table 5.1.
5.6.3. Dynamic Contrast-Enhanced Breast Imaging
Free-breathing unilateral breast DCE MRI was performed in six
patients (age 55.3±6.7 years) in sagittal orientation prior to MRI-guided
biopsy using the radial 3D FLASH protocol on a 3T scanner (MAGNETOM
TimTrio, Siemens AG, Healthcare Sector, Erlangen, Germany), equipped
with a 7-element breast-coil array (InVivo Corporation, Gainesville, FL). A
single dose of Gd-DTPA with concentration of 0.1 mM/kg body weight was

129
injected at 3 ml/second into an antecubital vein. Relevant imaging
parameters are listed in Table 5.1.
5.6.4. Dynamic Contrast-Enhanced Neck Imaging
DCE MRI of the neck was performed in ten patients (age 66.2±19.9
years) in axial orientation using the radial 3D FLASH protocol on a 1.5T
scanner (MAGNETOM Avanto, Siemens AG, Healthcare Sector, Erlangen,
Germany), using a head/spine coil with 15 elements. The contrast-injection
protocol was identical to the liver example. Relevant imaging parameters
are listed in Table 5.1.
5.7. Image Reconstruction
Iterative SENSE, coil-by-coil compressed sensing, and GRASP
reconstructions were performed on all the datasets using 21 spokes for
each temporal frame. The reconstructed in-plane matrix size was 256x256
or 384x384, depending on the number of readout samples. The achieved
temporal resolution was about 3 seconds/volume for the liver application, 5
seconds/volume for the pediatric application, 3 seconds/volume for breast
imaging and 7 seconds/volume for neck imaging. Compared to the Nyquist
sampling rate, the reconstructions correspond to an acceleration rate of
19.1 or 28.7.

130
The iterative SENSE reconstruction was performed using the
GRASP implementation with a regularization weight of =0. In coil-by-coil
compressed sensing reconstruction, image reconstruction was performed
for each coil element separately, followed by sum of square combination.
The regularization parameter was selected only once, as described for
GRASP.
In order to demonstrate the flexibility of GRASP, reconstructions
were also performed with different temporal resolutions for one of the
pediatric datasets (13 and 34 spokes, corresponding to 3 and 8
seconds/volume).
Image reconstruction was performed using the C++ implementation
on a Linux server equipped with four Intel Xeon E5520 quad core CPUs at
2.27 GHz and 96 GB of RAM. The reconstruction time ranged between 30 -
45 minutes for a complete 3D data set, depending on the size of datasets.
5.8. Image Analysis and Statistics
In order to evaluate the image quality and temporal fidelity achieved
with GRASP, one representative partition was selected from each
reconstructed dataset for image quality assessment. Images were
compared between GRASP vs. iterative SENSE, GRASP vs. coil-by-coil
compressed sensing, and temporal fidelity assessment was compared
between GRASP vs. NUFFT.

131
5.8.1. Image Quality Assessment
A total of 39 liver datasets (13 iterative SENSE, 13 coil-by-coil
compressed sensing and 13 GRASP), 15 pediatrics datasets (5 iterative
SENSE, 5 coil-by-coil compressed sensing and 5 GRASP), 18 breast
datasets (6 iterative SENSE, 6 coil-by-coil compressed sensing and 6
GRASP) and 30 neck datasets (10 iterative SENSE, 10 coil-by-coil
compressed sensing and 10 GRASP) were pooled and randomized for
blinded qualitative evaluation by 3 radiologists with expertise on abdominal
imaging, breast imaging and neuroimaging respectively. The score levels
for all the image quality assessments were: 1 = non-diagnostic, 2 = poor, 3
= adequate, 4 = good and 5 = excellent.
The reported scores in each reconstruction category from all five
applications were pooled together to represent mean ± standard deviation.
Wilcoxon signed-rank sum test was chosen to compare the scores between
GRASP vs. iterative SENSE and GRASP vs. coil-by-coil compressed
sensing (n=34), using Excel (Microsoft, Redmond, WA), where P < 0.05
was considered to be statistically significant different.
5.8.2. Temporal Fidelity Assessment
For each of the GRASP datasets, a ROI was manually drawn to
evaluate the signal-intensity time courses. The upslope was computed
using a linear fit of the curve points selected between 10% and 90% of the

132
Figure. 5.3: Reconstruction of one representative partition from the contrast-enhanced volumetric liver dataset acquired with golden-angle radial sampling scheme using NUFFT (a) and iGRASP with three different weighting parameters (b-d) by grouping 21 consecutive spokes in each temporal frame. Results with λ = M0*0.05 achieved an appropriate compromise between image quality and temporal fidelity. This value was therefore chosen for iGRASP reconstruction with temporal resolutions of 21 spokes per frame. The weighting parameter was adjusted for different temporal resolutions according to the level of incoherent aliasing artifacts or pseudo-noise in the PSF. M0 was the maximal magnitude value of the NUFFT images that were also used to initialize the iGRASP reconstruction.
relative peak enhancement, which usually corresponded to the first pass of
contrast agent. The corresponding NUFFT data set was evaluated using
the same ROI, and the upslope was calculated using the same length of
curve points as reference. The analysis was performed on all GRASP

133
datasets (n=34) and the corresponding NUFFT results. The upslope of
NUFFT and GRASP reconstructions were pooled separately and the
relative accuracy was evaluated by performing linear correlation and
Intraclass correlation (ICC) in Excel (Microsoft, Redmond, WA).
5.9. Results
5.9.1. Selection of Reconstruction Parameters
Figure 5.3 shows the results from the NUFFT reconstruction of one
DCE liver data set (a) and the GRASP reconstructions with three
representative values of the weighting parameter (b-d). It should be
noted that although the dynamic curves from the NUFFT reconstruction are
contaminated by streaking artifacts, they still preserve good contrast-time
evolution due to the fact that intensities were averaged over a relatively
large ROI. Therefore, it can be used as a first rough measure to assess
temporal fidelity. The results suggest that = M0*0.05 yields a good
balance between image quality and temporal fidelity (Figure 5.3c). Higher
weighting (Figure 5.3d, = M0*0.09) produces lower residual artifact and
slightly better image quality but also stronger temporal blurring, and vice
versa for a lower weight (Figure 5.3b, = M0*0.01). Based upon these
results, = M0*0.05 was selected by the radiologist for GRASP

134
Figure. 5.4: Comparison of GRASP (top) reconstruction with coil-by-coil compressed sensing (middle) and iterative SENSE (bottom) reconstructions in the liver dataset with the same acceleration rate and temporal resolution of 21 spokes/frame = 3 seconds/volume. GRASP showed superior image quality compared to both coil-by-coil compressed sensing and iterative SENSE reconstructions.
reconstructions with 21 spokes. As shown in the following sections, this
weight led to similarly good results in other applications.
5.9.2. GRASP vs. Coil-by-Coil Compressed Sensing and Iterative
SENSE
Figure 5.4 shows the comparison of GRASP with coil-by-coil
compressed sensing and iterative SENSE reconstructions for a liver dataset
with in-plane matrix size of 384x384. GRASP showed better image quality
than coil-by-coil compressed sensing reconstruction, largely as a result of

135
the incorporation of coil sensitivities in the reconstruction and the reduction
of aliasing artifacts provided by the parallel-imaging component (Figure
5.1b). The reduction of aliasing artifacts enabled recovery of more signal
coefficients, particularly those corresponding to high resolution features,
which generally have lower values. GRASP also outperformed iterative
SENSE and showed significantly lower residual aliasing artifacts due to the
temporal TV constraint, which exploits additional temporal correlation and
sparsity.
5.9.3. Dynamic Pediatric Body Imaging
Figure 5.5a shows one representative partition of DCE-MRI from a
10-year old patient. The reconstructed images clearly show distinct aorta,
portal vein, and liver contrast enhancement over time. Note that the same
data set was used to reconstruct dynamic images with different temporal
resolutions by grouping 34 (top), 21 (middle), and 13 (bottom) spokes.
Figure 5.5b evaluates the corresponding signal intensity changes over time
for the aorta (AO) and portal vein (PV). For comparison, the signal intensity-
time curves of the NUFFT reconstruction are included as reference.
5.9.4. Dynamic Breast Imaging
Figure 5.6a shows unilateral breast DCE-MRI of a patient referred for
fibroadenoma with fibrocystic changes. The images reconstructed with

136
Figure. 5.5: (a) GRASP reconstruction of free-breathing contrast-enhanced volumetric abdominal imaging of a 10-year old patient referred for tuberous sclerosis. Representative images with three different temporal resolutions are shown, including (top) 34 spokes/frame = 8 seconds/volume, (middle) 21 spokes/frame = 5 seconds/volume and (bottom) 13 spokes/frame = 3 seconds/volume. The reconstructed image matrix size was 256 x 256 in each dynamic frame, with in-plane spatial resolution of 1 mm and the weighting parameters of different temporal resolutions were adjusted according to the acceleration rate. b) Signal-intensity time courses for the aorta and portal vein, which do not show significant temporal blurring as compared with the corresponding NUFFT results.
GRASP show appropriate contrast enhancement over time in the normal
breast tissue and in a suspicious breast lesion indicated by the white arrow.
GRASP also provided good image quality and depiction of relevant
morphological features, such as fibroglandular tissue, skin layer, and the
suspicious lesion. Figure 5.6b shows the corresponding signal intensity
changes over time of the breast lesion, heart cavity, vessel and breast

137
Figure. 5.6: (a) GRASP reconstruction of free-breathing contrast-enhanced volumetric unilateral breast imaging in an adult patient referred for fibroadenoma with fibrocystic changes. Temporal resolution is 21 spokes/frame = 3 seconds/volume. The reconstructed image matrix size is 256 x 256 for each dynamic frame, with in-plane spatial resolution of 1.1 mm. b) Signal-intensity time courses for the breast lesion, which is a fibroadenoma with fibrocystic changes (white arrow), for the heart cavity (white ROI), and for a blood vessel and breast tissue (white arrows), showing no significant temporal blurring.
tissue (white arrows and ROI). The GRASP reconstruction did not introduce
significant notable temporal blurring.
5.9.5. Dynamic Neck Imaging
Figure 5.7 shows representative images of two partitions from a
patient referred for neck mass and squamous cell cancer, together with the
corresponding signal-intensity changes for the carotid artery (white arrows).
The reconstruction shows good image quality in different phases and
similar contrast enhancement to the NUFFT curves.

138
Figure. 5.7: (a) GRASP reconstruction of contrast-enhanced volumetric neck imaging in an adult patient referred for neck mass and squamous cell cancer. Temporal resolution is 21 spokes/frame = 7 seconds/volume. The reconstructed image matrix size is 256 x 256 for each dynamic frame, with in-plane spatial resolution of 1 mm. b) Signal-intensity time courses evaluated for the carotid arteries show no significant temporal blurring.
5.9.6. Image Quality Comparison
Table 5.2 summarizes the mean scores and standard deviations for
different reconstruction strategies in each application. GRASP yielded
significantly better scores (P < 0.05) when compared with both iterative
SENSE and coil-by-coil compressed sensing reconstructions. The score of
GRASP was above 3.0 in all applications, suggesting that good image
quality can be achieved with the proposed acceleration rate and temporal
resolution.

139
DCE Liver DCE Pediatrics DCE Breast DCE Neck
GRASP 3.38±0.65 4.20±0.84 4.67±0.52 3.80±0.79
Coil-by-Coil CS 1.62±0.77 1.80±0.45 2.33±1.03 2.10±0.74
Iterative SENSE 1.38±0.65 1.40±0.55 2.17±1.17 1.00±0.00
Table. 5.2: Image quality assessment scores represent mean ± standard deviation for each reconstruction category for different applications.
5.9.7. Temporal Fidelity Comparison
For the upslope calculated from the data pairs (n=34, GRASP vs.
NUFFT), the linear regression coefficient was 0.99 and ICC was 0.99,
indicating strong agreement between the upslope obtained from GRASP
and NUFFT. This result suggests that GRASP does not introduce
significant temporal blurring.
5.10. Discussion
This chapter introduces a robust imaging approach for rapid dynamic
volumetric MRI named GRASP, which is applicable for a broad spectrum of
clinical applications. Even though individual components of the method
have been proposed before, the synergistic combination of compressed
sensing, parallel imaging, and golden-angle radial sampling results in a
technique that is particularly well-suited to obtain high spatial resolution,
high temporal resolution, and large volumetric coverage at the same time.
GRASP achieved significantly better performance than either parallel
imaging or compressed sensing alone and demonstrated high value for

140
clinical studies that require robustness to patient motion and simultaneous
high spatial and temporal resolution. GRASP can be also used in other
applications such as cardiac cine imaging.
The motion robustness can be mainly attributed to the use of radial
k-space sampling. Radial sampling is well-known for being less susceptible
than Cartesian sampling due to (i) lower sensitivity to motion-induced phase
shifts and (ii) signal averaging at the center of k-space. Moreover, it is well-
suited for compressed sensing because radial undersampling creates
incoherent low-intensity streaking artifacts. The golden-angle ordering
scheme additionally introduces temporal incoherence of the k-space
acquisition.
In radial sampling, the image contrast corresponds to the average
over the acquisition window because all lines cover k-space center. In this
regard, radial sampling introduces a certain amount of temporal blurring,
which manifests as slightly lower vessel-tissue contrast compared to
Cartesian acquisitions that use a narrow time window for the acquisition of
the k-space center. However, as opposed to other radial approaches that
use a broad temporal view-sharing filter to extract different temporal phases
without streaking artifacts, GRASP enforces data fidelity only within a
relatively small temporal window (e.g., 21 spokes), which enables to
preserve high temporal sharpness.

141
GRASP reconstruction removes streaking artifacts in the
undersampled time-series of images at the expense of suppressing small
coefficients in the temporal TV domain, which can compromise temporal
fidelity for high acceleration factors because rapidly oscillating intensity
changes may be dampened in this case while the temporal onset of sharp
intensity changes remains unaffected due to the use of the L1 norm.
However, unlike reconstruction approaches that employ TV constrains in
the spatial domain, GRASP does not lead to spatial image blurring or
synthetic appearance. In cases where there is motion between temporal
frames, temporal blurring artifacts might under certain circumstances
appear as spatial blurring artifacts, but these artifacts originate in the
temporal dimension. This penalty, which is common to all compressed
sensing methods, is due to the fact that MR images are compressible rather
than truly sparse, presenting a few high coefficients and many small
coefficients. If the small coefficients fall below the pseudo-noise level
created by the undersampling artifacts, they may not be robustly
recoverable. For the particular case of temporal TV, abrupt temporal
variations usually result in high coefficients that are well recovered by the
reconstruction. However, moderate or smooth signal variations might result
in low-value coefficients below the pseudo-noise level, which could be
suppressed by the reconstruction. Although minor compromises in the

142
temporal fidelity may result, it is unclear whether these effects are clinically
relevant. Future studies are planned to assess the impact on the diagnostic
performance of dynamic imaging, although the preliminary results obtained
so far indicate that the technique does not introduce clinically significant
temporal distortions. From a clinical perspective, it is presumably of higher
relevance that GRASP enables dynamic abdominal imaging in patients who
have difficulty in suspending their respiration, including severely sick,
pediatric, or sedated patients, and thus it is infeasible to perform dynamic
imaging with adequate diagnostic quality using established conventional
techniques.
GRASP provides a simple and flexible way of performing dynamic
MRI studies in these patients and can help to improve clinical workflow by
enabling data acquisition without the need for synchronization with breath-
hold commands or for selection of a predefined rigid temporal resolution.
While a typical clinical use case does not require reconstruction and
evaluation of image series at multiple temporal resolutions, which would
increase the workload of radiologists if used indiscriminately, the flexibility
of reconstructing different temporal resolutions without the need to re-
acquire data can be another advantage for specific clinical questions or in
the event of a suggestive finding. Formal studies are currently in progress
using a prototypic workflow integration to investigate the clinical potential of

143
multi-resolution reconstructions and to determine the range of effectively
achievable temporal resolutions.
The current implementation of GRASP has some limitations that will
be addressed in future work. First, a stack-of-stars k-space sampling
pattern is employed to enable parallelized slice-by-slice reconstructions.
This reduces the computational burden of GRASP reconstructions, but
prevents employing compressed sensing along the slice dimension. The
use of full 3D golden-angle radial sampling along with a volumetric
reconstruction are expected to further increase the performance, at the
expense of higher computational demand. Second, although temporal TV
has been used before for different dynamic MRI reconstructions (77,117-
119) and was shown to be better in some specific applications, it may be
not optimal to use it as the only sparsifying transform for all cases and
applications. Other advanced temporal sparsifying transforms, such as
dictionary learning, might be also useful to increase temporal fidelity for
high undersampling factors. Third, the current work did not use rigorous
mathematical criteria to select the weighting parameter , which controls
the tradeoff between removal of streaking aliasing artifacts and temporal
fidelity. The empirical rule to make proportional to the pseudo-noise level
in the PSF produced reasonable performance for different undersampling
factors. The same was also used in different applications for a given

144
temporal resolution, which suggests that the reconstruction can be
automated without intervention. However, evaluation on a larger set of
patients comparing with standard clinical techniques is required to test the
robustness of this new approach. Finally, because it is impossible in
practice to acquire a fully-sampled volumetric DCE dataset with the target
spatial and temporal resolution, the current study employed NUFFT
reconstructions as temporal reference. While NUFFT reconstructions
provide time curves without artificial temporal blurring effects, they can be
affected by strong streaking artifacts at high accelerations that limit their
value for assessing the ground-truth signal evolution. A comprehensive
analysis of the temporal fidelity achieved with GRASP using numerical
simulations and dynamic phantom scans is currently in progress.
5.11. Conclusion
The combination of compressed sensing, parallel imaging, and
golden-angle radial sampling employed in GRASP enables rapid dynamic
volumetric MRI studies with high spatial resolution, temporal resolution, and
motion robustness. Because of the continuous data acquisition and the
flexibility to reconstruct images retrospectively at different temporal
resolutions, dynamic imaging with GRASP can be integrated easily into
clinical workflow. GRASP can be used for a wide range of clinical

145
applications and demonstrated particular value for examinations of patients
that are unable to suspend respiration.

146
Chapter 6
XD-GRASP: Golden-Angle Radial MRI with Reconstruction
of an Extra Motion-State Dimensions Using Compressed
Sensing
6.1. Prologue
The GRASP technique presented in Chapter 5 has been
successfully demonstrated in a variety of clinical applications and it is
currently being tested in a wide range of routine clinical studies. However,
despite its robustness to respiratory motion, initial clinical studies suggest
that GRASP still suffers from residual respiratory blurring, which may
reduce the vessel-tissue contrast and thus hinder the clinical interpretation
of the images. In this chapter, we develop a novel framework for free-
breathing MRI called XD-GRASP, which exploits the self-navigation
properties of radial imaging and reconstructs an extra respiratory-state

147
dimension using compressed sensing. The proposed method represents a
novel way to handle respiratory motion using compressed sensing ideas.
Instead of seeking to remove motion, an additional respiratory-state
dimension is reconstructed, which improves image quality and also offers
new physiological information that could be of potential clinical value.
The contents presented in this chapter were published in the journal
Magnetic Resonance in Medicine (MRM 2015 Mar 25. doi:
10.1002/mrm.25665. [Epub ahead of print]) (120).
6.2. Introduction
Respiratory motion remains a major challenge in MRI, particularly for
abdominal and cardiovascular imaging. Due to the limited encoding speed
of conventional MRI, k-space lines may be acquired in different respiratory
motion states during free breathing, resulting in ghosting artifacts and
image blurring (45,121). As reviewed in Chapter 2, the simplest approach to
avoid respiratory motion effects is to suspend respiration during data
acquisition (7) – an approach that is currently widely used in routine clinical
MRI exams. However, breath-hold capabilities are subject-dependent and
can be significantly limited in some patients. In addition, typical breath-hold
durations (10-15 seconds) also limit achievable spatial resolution and
volumetric coverage. An alternative approach is to use either navigator
signals (47) or respiratory bellows (48) to monitor respiratory motion and

148
acquire data only at a specific respiratory state (e.g., end-expiration).
However, such gated data acquisition significantly reduces imaging
efficiency and further prolongs the total examination times. Real-time MRI
can be used for free-breathing cardiac cine imaging (77,101,122,123), but
the acquisitions usually comprise only a single slice with limited spatial and
temporal resolution. Non-Cartesian k-space sampling schemes, such as
radial or spiral, are substantially less sensitive to respiratory motion and
enable free-breathing imaging at the expense of increased scan times (50-
52). For example, radial imaging eliminates k-space gaps due to motion-
related phase shifts, by repeated sampling of the k-space center. However,
substantial motion is still a challenge for non-Cartesian imaging and can
result in blurring and aliasing artifacts, e.g., streaks for radial trajectories
(124,125). Non-Cartesian acquisitions also offer the potential benefit of
retrospective self-gating, owing to the continuous passage of the radial lines
through the center of k-space, and thus can eliminate the need to use
navigator signals or external devices (53,54). For example, Liu et al. have
proposed an image reconstruction approach for free-breathing cardiac cine
MRI, in which the cardiac and respiratory motion signals retrospectively
obtained from the data are used for self-gating and view-sharing
reconstruction with less motion blurring (53). However, these approaches

149
are still time-inefficient, since typically only data within a predefined motion
state (e.g., close to expiration) are used for the image reconstruction.
Compressed sensing with temporal sparsifying transforms has
enabled high accelerations in dynamic MRI studies (30,72,126). However,
respiratory motion generally leads to inter-frame misalignments, which
reduce temporal sparsity and result in temporal blurring. Several
approaches have been proposed to integrate an image registration
framework into the reconstruction problem, to correct for respiratory motion.
For example, rigid-body motion registration techniques have been applied
to compressed sensing cardiac perfusion imaging (127) and more complex
deformable registration techniques that account for non-rigid body motion
were employed in compressed sensing reconstruction of cardiac cine (58),
cardiac perfusion (56), and abdominal DCE-MRI examinations (57). A more
advanced method, which learns the motion fields from the data itself to
guide image reconstruction, was recently introduced, which, in addition to
performing motion compensation, can also provide access to specific
motion information (59).
With the goal of combining the motion-robustness of radial imaging
and the acceleration capabilities of compressed sensing, the Golden-angle
RAdial Sparse Parallel (GRASP) technique (107) has been proposed in
Chapter 5 for highly-accelerated motion-robust DCE-MRI. Successful

150
applications of GRASP for free-breathing imaging have been demonstrated
in various organs affected by respiratory motion, such as liver (108),
prostate (109) and small bowel (128). However, our clinical evaluation
suggests that GRASP still suffers from some degree of respiratory motion
blurring, especially in sick or elderly patients, who tend to be less
cooperative in following a shallow breathing pattern during data acquisition.
The resulting motion-blurring effects reduce vessel-tissue contrast and may
prevent the detection of small lesions.
In this work, we propose a novel image reconstruction framework,
called eXtra-Dimensional GRASP (XD-GRASP), which combines GRASP
with the self-navigation property of radial imaging and uses motion
detection schemes adapted from previous work (129,130). Instead of
removing or correcting the motion in question, XD-GRASP reconstructs
extra motion dimensions, where continuously acquired k-space data are
sorted into multiple sets of undersampled datasets with distinct motion
states, using motion signals extracted directly from the data (131,132). This
approach may also be generalized to account for multiple sources of motion
or dynamic signal change simultaneously, such as cardiac motion and
contrast enhancement in addition to respiratory motion, by sorting the data
into multiple additional motion-state dimensions. A compressed sensing
algorithm is employed to reconstruct the motion-sorted datasets by

151
Figure. 6.1: Schematic illustration of the XD-GRASP method: (a) Continuously acquired radial k-space data are sorted into respiratory states from expiration (top) to inspiration (bottom), using a respiratory motion signal extracted directly from the data. Different colors indicate different motion states. The number of spokes grouped in each motion state is the same. (b) Approximately uniform coverage of k-space, with distinct sampling patterns in each respiratory motion state, is achieved using the golden-angle acquisition scheme. (c) Data sorting removes blurring and clearly resolves respiratory motion, at the expense of introducing undersampling artifacts. The purple dashed line shows the distinct respiratory motion states after data sorting. (d) Sparsity is exploited along the extra dimension to remove aliasing artifacts due to undersampling.
exploiting sparsity along the corresponding motion-state dimensions. From
a clinical perspective, the extra dimensions may also provide new
physiological information, since images of different kinds of motion states

152
may be disentangled during reconstruction. The performance of XD-
GRASP is demonstrated by comparing against reconstructions without
motion sorting in representative free breathing imaging applications,
including: i) 3D abdominal imaging with respiratory motion only; ii) 2D
cardiac cine imaging with cardiac and respiratory motion, and iii) 3D liver
DCE-MRI with respiratory motion and time-dependent contrast-
enhancement.
6.3. A Simple Example of XD-GRASP
Successful implementation of XD-GRASP has two principal
requirements: (a) reliable physiological (e.g., respiratory and/or cardiac)
motion signals and (b) preservation of approximately uniform k-space
coverage in each motion state after data sorting. Golden-angle radial
sampling (113), which uses ~111.25o angular increment between
consecutive spokes, is employed for data acquisition, since the repeated
sampling of the k-space center enables extraction of motion-state signals,
and it allows the possibility of arbitrary data sorting with approximately
uniform k-space coverage in each motion state while maintaining sufficient
incoherence in the sampling pattern along the new motion-state dimension
for robust compressed sensing reconstruction.
Figure 6.1 illustrates the basic concept of XD-GRASP, in which the
continuously acquired radial k-space data are sorted into a specific number

153
Figure. 6.2: Data sorting procedure for XD-GRASP in abdominal MRI without contrast ejection. Respiratory motion was first sorted from end-expiration to end-inspiration and the corresponding set of spokes were evenly distributed into multiple respiratory states so that the number of spokes is the same in each motion state.
of respiratory states spanning from expiration (top) to inspiration (bottom)
using a respiratory motion signal derived from the acquired data (Figure
6.1a). The sorting procedure is performed so that the number of spokes
grouped in each motion state is the same (as shown in Figure 6.2).
Approximately uniform coverage of k-space with distinct sampling patterns
in each motion state is achieved by using the golden-angle acquisition
scheme (Figure 6.1b). Data sorting removes blurring and clearly resolves
respiratory motion (indicated by the purple dashed line), at the expense of
generating undersampling artifacts (Figure 6.1c). A compressed sensing
reconstruction that exploits sparsity along the new respiratory-state

154
dimension can be employed to remove undersampling artifacts (Figure
6.1d).
6.4. Motion Estimation and Data Sorting
Estimation of motion signals and data sorting were performed in a
slightly different way for each target application (e.g., cardiac vs. abdominal
imaging) and k-space trajectory (2D golden-angle radial vs. 3D stack-of-
stars golden-angle radial).
6.4.1. Motion Estimation and Data Sorting in 2D Cardiac Cine MRI
For cardiac cine imaging, the center of k-space (DC component) in
each spoke (Figure 6.3a), which reflects the change in average signal level
due to changes of the volume of lung and heart in the excited slab, was
used to extract information about physiological motion over time (54).
Information from multiple coils was used to obtain separate signals
representing respiratory or cardiac motion, as shown in Figure 6.4.
Conceptually, the motion signal from the coil nearest to the heart provides
predominantly cardiac motion information, and the motion signal from the
coil nearest to the diaphragm provides predominantly respiratory motion
information. Since these motions are known to have different frequency
contents, the motion signal in the coil-element with the highest peak in the
frequency range of 0.1-0.5Hz was automatically selected to represent

155
Figure. 6.3: XD-GRASP motion estimation and data sorting for cardiac cine imaging. (a) 2D golden-angle radial trajectory. Motion signals are estimated from the central k-space position of each radial line (gray dot). (b-c) Estimation of cardiac and respiratory motion signals using information from multiple coils. The signals with the highest peaks in the frequency range of 0.1-0.5Hz and 0.5-2.5Hz are automatically selected for respiratory and cardiac motion signals, respectively. (d) Conventional iGRASP sorting of cardiac phases, given by grouping consecutive spokes in each frame. (e) XD-GRASP sorting, in which all the cardiac cycles are concatenated into an expanded dataset with one cardiac dimension (tC) and an extra respiratory dimension (tR), so that sparsity along tC and tR can be exploited in the multidimensional compressed sensing reconstruction.
respiratory motion; and the motion signal in the coil-element with the

156
Figure. 6.4: Selection of cardiac and respiratory motion signals from multiple coils. (a) 2D golden-angle radial trajectory for free-breathing 2D cardiac cine MRI and (b) estimation of cardiac and respiratory motion signals using information from multiple coils. The motion signal in the coil-element with the highest peak in the frequency range of 0.1-0.5Hz was automatically selected to represent respiratory motion; and the motion signal in the coil-element with the highest peak in the frequency range of 0.5-2.5Hz was automatically selected to represent cardiac motion. A filtering procedure can be performed on the detected motion signals for denoising.
highest peak in the frequency range of 0.5-2.5Hz was automatically
selected to represent cardiac motion. A filtering procedure can be
performed on the detected motion signals for denoising (129). Figure 6.3b
shows an example of detected motion signals and Figure 6.3c shows the
corresponding frequency information. End-systolic motion-states were

157
identified as the valleys in the cardiac motion signal and thus any abnormal
cardiac cycles, in case of arrhythmias, can be identified according to the
difference between cycle lengths for rejection or a separate reconstruction.
Given the selected motion signals, the continuously acquired 2D cardiac
dataset can be sorted into an expanded dataset containing two dynamic
dimensions, representing predominantly cardiac and respiratory motions,
respectively. Specifically, the continuously acquired golden-angle radial
dataset were first sorted into a dynamic cardiac series by grouping a
number of consecutive spokes (e.g., 15 spokes) as one cardiac phase
(Figure 6.3d). All the cardiac cycles, identified using the cardiac motion
signal, were then sorted into an expanded dataset to generate an extra
respiratory state dimension tR (Figure 6.3e), so that sparsity along both
cardiac and respiratory dimensions can be exploited in the compressed
sensing reconstruction.
6.4.2. Motion Estimation and Data Sorting in 3D Abdominal MRI
The 3D stack-of-stars sampling scheme (Figure 6.5a), in which
golden angle radial sampling is employed in the kx-ky plane and Cartesian
sampling is employed along the kz dimension, acquires all spokes along kz
for a given rotation angle and then repeats the procedure for the next
rotation angle, i.e., an inner loop is defined along kz and an outer loop along
the rotation angle. A straightforward approach for motion detection would

158
Figure. 6.5: XD-GRASP motion estimation and data sorting for DCE-MRI imaging. (a) 3D stack-of-stars radial trajectory with golden-angle rotation, where all spokes along kz for a given rotation angle are acquired before rotating the sampling direction to the next angle. (b) A 1D Fourier transform along the series of k-space central points of each slice is performed to obtain a projection profile of the entire volume for each angle and all the projection profiles from all coils are concatenated into a large two-dimensional matrix, followed by principal component analysis (PCA) along the z+coil dimension. (c-d) The principal component with the highest peak in the frequency range of 0.1-0.5Hz is selected to represent respiratory motion. (e-g) Contrast-enhancement effect is approximately removed by estimating and subtracting the envelope of the composite signal. (h-i) Processed respiratory motion signals are shown superimposed on the z-projection profiles for normal breathing (left) and heavy breathing (right), demonstrating reliable motion estimation.
be to use the DC component of central spokes along the kz dimension (133)
and perform the same procedure as was just described for 2D imaging.

159
However, prior study has shown that motion detection is more robust using
the projections along the slice dimension for 3D stack-of stars imaging
(134). In this work, an adapted version of the projection approach was
employed for respiratory motion detection in 3D liver imaging. Specifically, a
projection profile of the entire volume was computed for each acquisition
angle by taking a 1D partition-direction Fourier transform of the series of
kx=ky=0 central points (gray lines in Figure 6.5a). Respiratory motion
detection was performed by first concatenating the projection profiles from
all coils into a large two-dimensional matrix, followed by principal
component analysis (PCA) along the concatenated z+coil dimension
(Figure 6.5b). As proposed in (130), PCA can be interpreted as a procedure
to determine the most common signal variation mode among all coils, and
the principal component with the highest peak in the frequency range of
0.1-0.5Hz was selected to represent respiratory motion (Figure 6.5c&d),
since respiratory motion is known to occur within this frequency range. For
DCE-MRI, contrast-enhancement has to be separated from respiratory
motion. In this work, the envelope of the detected motion signal was
estimated using a spline data fitting procedure and then subtracted to
generate the respiratory motion signal (Figure 6.5e-g). Figure 3h&i show
two representative examples of respiratory motion in both normal breathing
(left) and deep breathing (right) detected using the proposed approach,

160
Figure. 6.6: For DCE-MRI, the respiratory motion sorting procedure described in Figure 6.2 is performed in each contrast-enhancement phase separately
where motion signals were superimposed on the slice projection profiles.
Given the respiratory motion signal, the continuously acquired golden-angle
radial dataset was first divided into successive contrast-enhancement
phases (dynamic dimension tcontrast) and each phase was then further
sorted into multiple respiratory states (dynamic dimension tR), in which the
number of spokes is the same in each motion state, as shown in Figure 6.6.
6.5. Image Reconstruction
XD-GRASP reconstruction extends the GRASP pipeline by enforcing
a different sparsity constraint along each dynamic dimension. Specifically

161
for 2D free-breathing cardiac imaging, reconstruction was performed by
solving the following optimization problem:
2
1 1 2 22 1 1argmin
d
d F C d m S d S R d (6.1)
Here F is the non-uniform fast Fourier transform (NUFFT) operator (135)
defined for the radial sampling pattern, represents the n-elements
coil sensitivity maps with dimensionality of x-y-coil, where x and y represent
two spatial dimensions. d is the 2D dynamic image-series with one cardiac
motion dimension and one respiratory-state dimension (x-y-tC-tR), and
1
2
n
m
mm
m
are the corresponding multicoil radial k-space data sorted
according to the new dimensions (x-y-tC-tR-coil). 1S is the sparsifying
transform applied in the cardiac motion dimension with regularization
parameter 1 and 2
S is the sparsifying transform applied along the extra
respiratory-state dimension with regularization parameter 2 . R is a
reordering operator along the tR dimension that sorts all the respiratory
phases at a given cardiac position from expiratory state to inspiratory state.

162
This sorting procedure will ensure a smooth transition between adjacent
motion states, which improves the performance of total-variation
minimization along the dynamic dimensions as suggested in (136).
For 3D liver imaging, reconstruction was performed by solving the
following optimization problem:
2
1 1 2 22 1 1argmin
d
d F C d m S d S d (6.2)
Here F is the same as before,
1
2
n
C
CC
C
represents the n-elements coil
sensitivity maps with dimensionality of x-y-z-coil, where z is the partition
dimension. d is the 3D dynamic image- series with one contrast-
enhancement dimension and one respiratory-state dimension (x-y-z-tContrast-
tR), and
1
2
n
m
mm
m
are the corresponding multicoil radial k-space data
sorted according to the new dimensions (x-y-z-tContrast-tR-coil). 1S is the
sparsifying transform applied in the contrast-enhancement dimension with
regularization parameter 1 and 2
S is the sparsifying transform applied
along the extra respiratory-state dimension with regularization parameter

163
2 . For liver imaging without contrast injection, 1
is just set as zero. Since
each contrast enhancement phase is already sorted from end-expiratory
state to end-inspiratory state, which promotes a smooth transition between
respiratory motion states, the reordering operator R applied in Equation 6.1
is not needed for Equation 6.2.
In this work, temporal finite differences (also known as total-variation
minimization) along the dynamic dimensions was selected for both 1S and
2S based on the experiences in previous chapters, but with different
weights 1 and 2
tailored to reflect the different degrees of sparsity along
each dynamic dimension. For example, stronger regularization was applied
along the sparser dynamic dimension and vice versa.
6.6. Imaging Applications
The performance of XD-GRASP was tested in free-breathing 3D
abdominal imaging, 2D cardiac cine imaging and 3D liver DCE-MRI, on
both healthy volunteers and patients. Human imaging was performed in
accordance with protocols approved by the New York University School of
Medicine Institutional Review Board and was found to comply with the
HIPAA. All subjects provided written informed consent before the imaging.

164
6.6.1. Free-Breathing 3D Abdominal Imaging: Respiratory Motion
Only
3D abdominal imaging (without contrast injection) was performed on
one healthy volunteer (female, age=32) on a whole-body 3T scanner
(MAGNETOM TimTrio, Siemens AG, Healthcare Sector, Erlangen,
Germany) equipped with the standard 12-element body matrix coil array. A
3D stack-of-stars golden-angle radial FLASH pulse sequence with
frequency-selective fat suppression was employed and three scans were
performed in transverse, coronal and sagittal orientations, in order to test
the robustness to motion in different imaging planes. Relevant imaging
parameters included: TR/TE = 3.52/1.41 ms, FOV = 300 x 300 x 140 mm3,
number of points in each spoke = 192, number of partitions = 28 and spatial
resolution = 1.5 x 1.5 x 5 mm3. 510 spokes were acquired for each partition,
with a total scan time of ~57 seconds.
Six respiratory motion-states (84 spokes in each state) were
generated by sorting the continuously acquired data as described in Figure
6.1 and Figure 6.2. XD-GRASP was performed with one sparsifying
transform along the respiratory-state dimension ( 2S in Equation 6.2). The
results were compared with NUFFT reconstruction of the whole dataset
without motion sorting.

165
6.6.2. Free-Breathing 2D Cardiac Cine Imaging: Cardiac and
Respiratory Motions
2D cardiac cine data were acquired in one healthy volunteer (female,
age=32), one patient with normal sinus rhythm (male, age=46), one patient
with premature ventricular contractions (PVCs) (female, age=33) and
another patient with second-degree atrioventricular block (female, age=49).
Imaging was performed during normal free breathing on a whole-body 1.5T
scanner (MAGNETOM Avanto, Siemens AG, Healthcare Sector, Erlangen,
Germany) without any external triggering or gating, using a 2D radial
bSSFP pulse sequence with golden-angle acquisition scheme. Three short-
axis slices (SAX) in apical, middle, and basal ventricular positions, and one
slice in a four-chamber plane (4CH) were acquired in the volunteer scans.
Relevant imaging parameters included: TR/TE = 2.8/1.4 ms, FOV = 320 x
320 mm2, number of points in each spoke = 160, spatial resolution = 2 x 2
mm2, slice thickness = 8 mm, and the total acquisition time for each slice
was ~20 seconds. For comparison purposes, cardiac cine images with
similar imaging orientations and parameters were also acquired using the
routine clinical approach with breath-hold, Cartesian k-space sampling and
retrospective ECG gating. In the patient scans, one middle ventricular SAX
slice was acquired in each subject with the following imaging parameters:
TR/TE = 2.8/1.4 ms, FOV = 256 x 256 mm2, number of points in each

166
spoke = 128, spatial resolution = 2 x 2 mm2, slice thickness = 8 mm, and
the total acquisition time for each slice was ~15-20 seconds. For
comparison purposes, cardiac cine images with similar imaging orientations
but with relatively higher spatial resolution (~1.6 x 1.6 mm2) were also
acquired using the routine clinical approach with breath-hold, Cartesian k-
space sampling and retrospective ECG gating.
Cardiac cycles with arrhythmias were first detected and separated
using the cardiac motion signals in the patient datasets. Every 15
consecutive spokes were grouped to generate one dynamic phase,
achieving a temporal resolution of ~ 45 ms, as showing in Figure 6.3d. XD-
GRASP reconstruction was performed on an expanded time-series of
undersampled datasets (Figure 6.3e) with ~18-26 cardiac phases and ~10-
16 respiratory phases, depending on the heart rate of the subjects. The
cardiac cycles with arrhythmias in the patient with PVCs were rejected
because there were only 2 cardiac cycles with arrhythmias in the entire
acquisition. Thus the gain of performing XD-GRASP in arrhythmia cycles is
small because of the limited number of respiratory phases and limited
sparsity along the respiratory dimension. In the patient with second-degree
atrioventricular block, there were more arrhythmia cardiac cycles and thus a
separate XD-GRASP reconstruction was performed on the cardiac cycles
with arrhythmias. For comparison, GRASP reconstruction (without

167
respiratory sorting) was also performed on a time-series of undersampled
cardiac phases, where each cardiac phase was formed by grouping 15
consecutive spokes in the volunteer datasets. 1.5-fold zero-filling was
performed in all the results for visualization purposes, and a 5th-order
temporal medial filter was performed along the cardiac dimension after
image reconstructions, in order to further reduce the residual streaking
artifact (49).
6.6.3. Free Breathing 3D Liver DCE-MRI: Contrast Enhancement and
Respiratory Motion
3D liver DCE-MRI was performed on four volunteers (males, age =
32.5±1.3) as well as one patient (male, age=69) with a suspected liver
tumor on a whole-body 3T scanner (MAGNETOM Verio, Siemens AG,
Healthcare Sector, Erlangen, Germany) equipped with the standard 12-
element body matrix coil. Three volunteers and the patient were asked to
breathe normally and one volunteer was asked to breath heavily during the
scans. The 3D stack-of-stars pulse sequence was employed to acquire data
in transversal orientation and intravenous injection of 10 ml of
gadopentetate dimeglumine (Gd-DTPA) (Magnevist; Bayer Healthcare,
Leverkusen) was initialized simultaneously with the onset of data
acquisition, followed by a 20-ml saline flush, both injected at a rate of 2 ml /
second. Relevant imaging parameters for the volunteer scan included:

168
TR/TE ≈ 3.52/1.41 ms, FOV = 360 x 360 x 240 mm3, number of points in
each spoke = 256, spatial resolution = 1.4 x 1.4 x 3 mm3, number of
partitions = 80, with 60% slice resolution reduction and 6/8 partial Fourier
applied along the slice dimension. 600 spokes were continuously acquired
in each partition, for a total scan time of ~95 seconds. Imaging parameters
for the patient scans were similar, except that the number of points in each
spoke was 320, resulting in a spatial resolution of 1.1 x 1.1 x 3 mm3.
For comparison purposes, GRASP reconstruction (without
respiratory sorting) was first performed on a time-series of undersampled
contrast-enhancement phases, where each phase was formed by grouping
84 consecutive spokes (temporal resolution of ~13 seconds). XD-GRASP
reconstruction was then performed on a multidimensional undersampled
dataset, in which the 84 spokes in each contrast-enhancement phase were
further sorted into 4 respiratory states spanning from end-expiration to end-
inspiration. The sorting procedure was performed such that the number of
spokes in each motion state was the same, as shown in Figure 6.6.
6.6.4. Image Reconstruction Implementation
A tailored version of non-linear conjugate gradient optimization,
originally proposed in, was used to solve the optimization problem in both
Equations 6.1&6.2. Coil sensitivity maps were computed from a fully-
sampled reference given by NUFFT reconstruction of the whole dataset,

169
Figure. 6.7: Conventional NUFFT reconstruction without respiratory sorting (motion average) and XD-GRASP reconstruction with 6 respiratory states for datasets acquired in transverse, coronal and sagittal orientations. XD-GRASP significantly reduces motion-blurring, as indicated by the white arrows.
using the adaptive array combination method. Regularization parameters
1 and 2
were empirically selected by two experienced cardiac and body
radiologists. Specifically, the best value of 1 was selected first ( 2
was set
as zero) by testing different values and comparing image quality as well as
temporal fidelity, as previously performed in previous chapters. In the next
step, different values of 2 were then compared in combination with the 1
value selected in the first step and the radiologist selected the best value of

170
2 . According to our prior experience with compressed sensing MRI,
regularization parameters selected in this fashion can be used reliably in
the reconstruction of similar datasets. Image reconstruction was performed
in MATLAB (Mathworks, Natick, MA), using a workstation with a 16-core
Intel Xeon CPU and 96 GB RAM. XD-GRASP reconstruction time was ~5
minutes/slice for 3D abdominal imaging, ~40-60 minutes for 2D cardiac cine
imaging, and ~15 minutes/slice for 3D liver DCE-MRI.
6.7. Results
6.7.1. Free Breathing 3D Abdominal Imaging
Figure 6.7 compares the conventional NUFFT reconstruction of the
full dataset without respiratory sorting (corresponding to the motion
average) to XD-GRASP reconstruction with 6 respiratory motion states. XD-
GRASP improves the depiction of vessels and removes the blurring effects
at the edges of the liver (white arrows).
6.7.2. Comparison of Different Regularization Parameters for the
Extra Respiratory Dimension
Figure 6.8 shows XD-GRASP reconstruction results for four
representative respiratory sparsity regularization parameters ( 2 ) in cardiac
imaging and liver DCE-MRI. Utilization of a sparsity constraint along the
extra respiratory-state dimension improved the removal of undersampling

171
Figure. 6.8: XD-GRASP reconstruction results for four representative respiratory
sparsity regularization parameters ( 2 ) in cardiac imaging and liver DCE-MRI.
Utilization of a sparsity constraint along the extra respiratory-state dimension improved the removal of undersampling artifacts, when compared with the non-regularized case (
2 =0). Very low values of 2
resulted in residual aliasing artifacts, while very high
values of 2 introduced blurring. A 2
of 0.01 in cardiac cine imaging and 0.015 in
liver DCE-MRI provided a good tradeoff between residual aliasing artifacts and temporal fidelity.
artifacts, when compared to the non-regularized reconstruction ( 2 =0).

172
Figure. 6.9: Comparison of XD-GRASP against the standard breath-hold approach used in routine clinical studies (i.e., with retrospective ECG-gating) at end-diastolic and end-systolic cardiac phases in the volunteer scan. XD-GRASP provided similar performance to the routine clinical breath-hold method.
Very low values of 2 resulted in residual aliasing artifacts, while very high
values of 2 introduced blurring. A 2
on the order of 0.01 in cardiac cine
imaging and 0.015 in liver DCE-MRI provided a good tradeoff between
residual aliasing artifacts and temporal fidelity.

173
6.7.3. Free Breathing 2D Cardiac Cine Imaging
Figure 6.9 compares XD-GRASP with the standard breath-hold
approach using retrospective ECG-gating at end-diastolic and end-systolic
cardiac phases in the volunteer scans. Free-breathing XD-GRASP
achieved similar image quality to the conventional breath-hold approach but
also enabled the evaluation of the effects of respiratory motion at each
cardiac phase, which can be potentially valuable for examination of
conditions such as constrictive pericardial heart disease (137). Figure 6.10a
shows respiratory-related motion of the interventricular septum, especially
near end- diastolic cardiac phases, which indicates left-right ventricular
interaction during respiration.
Figure 6.10b show the comparison of XD-GRASP reconstruction
exploiting sparsity along two dynamic dimensions (right-hand column) with
GRASP reconstruction exploiting sparsity along a single dynamic dimension
only (left-hand column), using the same data set acquired during free
breathing. XD-GRASP reconstruction achieved superior image quality,
particularly in the removal of aliasing artifacts due to the separation of
cardiac and respiratory motion into different dimensions, which enables
exploitation of extra sparsity along the respiratory dimension.
Figure 6.11a compares XD-GRASP and the standard breath-hold
approach with retrospective ECG-gating for the patients. Although the

174
Figure. 6.10: (a) XD-GRASP provides access to respiratory motion information for each cardiac phase, where respiratory-related motion of the interventricular septum, especially at diastolic cardiac phases (top row) can be seen, indicating left-right ventricular interaction during respiration. Gray arrows indicate different respiratory motion states. (b) Comparison of XD-GRASP reconstruction exploiting sparsity along two dynamic dimensions (right-hand column) with GRASP reconstruction exploiting sparsity along a single dynamic dimension only (left-hand column), using the same data set acquired during free breathing.
conventional breath- hold approach produced good image quality in the
patient with normal sinus rhythm, it produced poor image quality for patients
with arrhythmia, due to the failure to properly synchronize cardiac cycles
with different length in the reconstruction. XD-GRASP, on the other hand,

175
achieved consistent image quality by enabling separation of cardiac cycles
with arrhythmia. In addition, the data from cardiac cycles with arrhythmia
can be used for a separate XD-GRASP reconstruction to provide additional
physiological information, as shown in the case of 2nd degree AV block
(Figure 6.11b). Figure 6.11c shows the corresponding cardiac motion
signals for three patients, where the cardiac cycle length is varying in the
patients with arrhythmia, indicated by gray arrows. The availability of these
signals offers the possibility to identify and separately reconstruct images of
the cardiac cycles affected by arrhythmia.
6.7.4. Free-Breathing 3D Liver DCE-MRI
Figure 6.12 shows the aortic and portal venous contrast-
enhancement phases in four representative partitions, for both GRASP and
XD-GRASP reconstruction of the first two volunteer datasets. The reduction
of respiratory motion blurring in XD-GRASP improved the delineation of
vessels and vessel-tissue contrast compared to GRASP.
The first four rows of Figure 6.13 show the portal vein
enhancement phase for two representative partitions each from volunteers
3 (normal breathing) and 4 (heavy breathing). GRASP suffered from
significant intra-frame respiratory motion blurring, especially in the dataset
acquired during heavy breathing. XD-GRASP improved the delineation of
vessels and borders in the liver, improved vessel-tissue contrast and

176
Figure. 6.11: (a) Comparison of XD-GRASP and the standard breath-hold approach with retrospective ECG-gating for the patients. Conventional breath-hold scans achieved good image quality in a patient with normal sinus rhythm, but it produced poor image quality for patients with arrhythmia. XD-GRASP achieved consistent image quality by separating the cardiac phases with arrhythmia. (b) In the patient with 2
nd
degree AV block, the arrhythmic cardiac cycles were further sorted for a separate XD-GRASP reconstruction to provide additional physiological information. (c) Corresponding cardiac motion signals for three patients with varying length of the cardiac cycle indicated by gray arrows.
enhanced the depiction of the kidney and bowel. The bottom row of Figure
6.13 shows the same comparison for one representative partition from the
patient dataset. The white arrow indicates a suspected liver lesion that can
be seen in GRASP but is better delineated in XD-GRASP.
6.8. Discussion
XD-GRASP provides a novel way to handle respiratory and other
types of motion in free-breathing MRI. Instead of removing motion, e.g.,

177
Figure. 6.12: Comparison of GRASP with XD-GRASP in both aortic and portal-venous enhancement phases in two representative partitions each from two volunteer datasets. XD-GRASP improved delineation of the liver and vessels with enhanced vessel-tissue contrast.
using self-gating, extra motion-state dimensions are reconstructed and a
compressed sensing approach is used to exploit compressibility in these
dynamic dimensions. XD-GRASP does not require the use of specific
motion models, and therefore it is immune to interpolation errors and offers
notable advantages as compared with previously proposed registration-
based compressed sensing reconstruction approaches (58,88), which co-

178
register images in different respiratory states to correct motion. In addition,
XD-GRASP also enables access to motion information that was not
available before, and thus it could potentially be used to study interesting
clinical problems, such as evaluation of the interaction of the left and right
ventricles during respiration, e.g., for the diagnosis of conditions such as
constrictive pericardial heart disease (137), and evaluation of the
respiration-dependent flow patterns in “Fontan physiology”. Furthermore,
there have been recent concerns about dyspnea caused by certain
hepatobiliary contrast agents, and the use of XD-GRASP for evaluation of
the impact of contrast injection on respiratory motion in abdominal DCE-
MRI is currently underway. Moreover, the ability to reconstruct images in
both inspiratory and expiratory phases from the same acquisition may also
be helpful, for example, in discriminating persistent stenosis of the celiac
artery from physiologic celiac artery narrowing during expiration.
The XD-GRASP approach is not limited to golden-angle radial
sampling, and it can be extended to other trajectories, as long as reliable
physiological motion information can be obtained (e.g., using external ECG
or respiration monitor devices) and arbitrary data sorting can be performed
with approximately uniform k-space coverage in each motion state. For
example, novel trajectories based on 3D Cartesian sampling with butterfly
navigators have been recently introduced for continuous data acquisition,

179
Figure. 6.13: Comparison of GRASP with XD-GRASP in a total of five representative partitions from two volunteers and one patient. Volunteer 4 was asked to breathe deeply. XD-GRASP achieved superior overall image quality, with reduced motion-blurring. The white arrow indicates a suspected liver tumor, which is better delineated in XD-GRASP.
following a golden-angle spiral pattern in the ky-kz plane (138). These
trajectories could be well-suited for XD-GRASP reconstruction (139).
In addition to cardiac cine imaging, other applications, such as
coronary MR angiography, can also benefit from simultaneous cardiac and
respiratory motion sorting. In these applications, data acquisition is usually

180
performed in a quiescent cardiac phase (e.g., mid-diastole) when cardiac
motion is minimal, and a navigator echo is employed to monitor the
movement of the diaphragm in order to minimize respiratory motion effects.
XD-GRASP can be used to reconstruct datasets acquired continuously
covering the entire cardiac cycles and cardiac phases with best delineation
of a particular artery can be retrospectively selected for visualization. The
application of XD-GRASP for coronary MRA will be exploited in next
chapter.
The temporal resolution demonstrated in this work for abdominal
DCE-MRI (11-12 seconds) may not be adequate for perfusion analysis,
which usually requires 2-3 second temporal resolution. Higher temporal
resolutions for DCE-MRI are restricted due to the fact that the contrast
enhancement is a non-periodic process, which limits the number of spokes
that can be combined for each respiratory state. One way to achieve higher
effective temporal resolutions would be to use a soft-gating approach,
which weights k-space data according to the respiratory motion signal, as
proposed in (140).
For abdominal DCE-MRI, the number of respiratory states was
selected such that they can adequately resolve respiratory motion without
introducing residual aliasing artifacts (As the number of motion states
increases, the number of radial spokes available for each state decreases,

181
resulting in increased undersampling). A small number of respiratory states
(e.g., 2) facilitate the removal of aliasing artifacts at the expense of limited
depiction of respiratory motion. A large number of respiratory states (e.g., 8
or 10), on the other hand, potentially enhances the visualization of
respiratory motion and reduces blurring at the expense of introducing
residual aliasing artifacts. As shown in Figure 6.14, we found empirically
that 4 respiratory motion states represent a good compromise between
removal of aliasing artifacts and motion-related blurring. Using more
respiratory states (e.g., 6) led to lower image quality due to increased
undersampling ratio and intrinsic limits in the performance of compressed
sensing reconstruction.
The reconstruction of the additional motion-state dimensions
increases the computational burden, particularly because one forward and
one backward NUFFT operation must be performed separately for each
motion state in each iteration. This issue can be addressed using parallel
computing, following the parallelization concept of the clinical
implementation of GRASP.
The stack-of-stars acquisition scheme employed in this work is still
sensitive to respiratory motion along the kz dimension (Cartesian sampling)
and limits the spatial resolution and slice coverage along z direction (i.e.,
only a limited number of partitions can be acquired, in order to maintain

182
Figure. 6.14: Comparison of XD-GRASP reconstructions with different number of respiratory motion states in abdominal DCE-MRI (end-expiratory motion state only). 4 and 6 respiratory states achieved better resolved respiratory motion than 2 states and 1 state. 6 respiratory states resulted in slightly lower performance than 4 respiratory states. White arrows indicate motional blurring for a choice of 1 motion state, and residual blurring for a choice of 2 motion states.
adequate temporal resolution). A true 3D golden-angle radial trajectory,
such as the spiral phyllotaxis sampling approach (141), can be helpful to
overcome these limitations which will be exploited in the next chapter.
6.9. Conclusion
XD-GRASP demonstrates a new use of sparsity for motion
compensation and offers a new way to handle respiratory or other types of
motion in free-breathing MRI. Instead of removing or correcting motion,
extra motion-state dimensions are reconstructed using a compressed
sensing approach that exploits sparsity along the new dimensions. XD-

183
GRASP reduces motion-induced blurring and allows separation of
respiratory motion from cardiac motion in cardiac cine MRI and from
contrast enhancement in DCE-MRI. Moreover, the reconstruction of
additional motion dimensions offers additional complementary information,
which can be of potential value for specific clinical applications.

184
Chapter 7
Towards Five-Dimensional Cardiac and Respiratory
Motion-Resolved Whole-Heart MRI Using XD-GRASP
7.1. Prologue
The stack-of-stars 3D radial sampling employed in Chapters 5 and 6
is relatively easy to implement and reconstruct. However, this sampling
scheme has several challenges. First of all, although radial sampling in the
kx-ky plane leads to reduced sensitivity to motion, the acquisition is still
sensitive to respiratory motion along the kz dimension, in which Cartesian
sampling is employed. In addition, stack-of-stars sampling also limits spatial
resolution in the partition dimension and the corresponding slice coverage.
In order to maintain adequate temporal resolution, only a limited number of
partitions can be acquired and interpolation is usually performed afterwards
to retrospectively increase the number of partitions. Accordingly, the

185
application of stack-of-star sampling to free-breathing 3D cardiac cine
imaging is challenging because the acquisition may fail to capture the
cardiac contraction when a large number of slices are needed. Moreover, in
the context of compressed sensing, the incoherence along the partition
dimension is also limited in stack-of-stars sampling and thus the overall
acceleration is limited. Although random undersampling could also be
implemented along the kz dimension, it would not be as efficient as in the
radial plane. The solution to address these challenges is to extend the
compressed sensing reconstruction into true 3D radial “kushball” sampling.
In this chapter, the XD-GRASP technique presented in Chapter 6 is
extended into a 3D golden-angle radial sampling scheme that is based on
the spiral phyllotaxis pattern. 3D radial sampling not only offers
reconstructions with volumetric isotropic resolution, but also allows
acceleration and exploitation of incoherence along all the spatial
dimensions. The proposed imaging framework is first applied for
electrocardiogram (ECG)-triggered respiratory motion-resolved whole-heart
coronary MR angiography (MRA), and then applied to demonstrate a
continuous five-dimensional whole-heart imaging framework with high
spatial and temporal resolutions, which allows simultaneous assessment of
myocardial function and visualization of cardiac and respiratory motion-
resolved whole-heart great vessels and coronary artery anatomy.

186
Some of the results presented in this chapter have been published in
an abstract at the 2015 Annual Meeting of the International Society for
Magnetic Resonance in Medicine (ISMRM 2015, page 27) (142).
7.2. Introduction
3D whole-heart MRI allows for a multifaceted assessment of the
cardiovascular system and is attractive due to the high SNR, large spatial
coverage, and simplified data acquisition. However, 3D imaging usually
requires prolonged data acquisition, and thus the sensitivity to motion,
particularly respiratory and cardiac motions during the scans, remains one
of the major challenges in this field. Conventional 3D cardiac MRI
acquisitions can be performed with ECG triggering, so that the effects of
cardiac motion can be minimized by acquiring data only within a short time
window (e.g., ~50-100 ms in mid-diastole or early-systole) in each cardiac
cycle. The influence of respiratory motion can also be minimized by
employing a navigator-gating (47), which tracks the movement of the right
diaphragm during the scan, so that only datasets at a consistent end-
expiratory phase are required. Although this image acquisition scheme has
been widely used in MR angiography (MRA) exams, it has several
challenges, including low scan efficiency, sensitivity to respiratory drifts, as
well as a relatively complicated measurement setup. In order to increase
the scan efficiency and thus imaging speed, various approaches have been

187
proposed to enable 3D free-breathing cardiac MRI by retrospectively
coregistering images at different respiratory states, so that nearly 100%
imaging efficiency can be achieved (55,143). However, the nature that data
acquisition is performed during a limited window in each cardiac cycle still
results in “deadtime” in the scan, and images can be only obtained at
specific cardiac phases. In order to make the best use of the scan time, a
number of 4D cardiac MRI methods have been proposed (144-146), either
employing navigator-gating/self-gating, or specific registration-based
respiratory motion correction, so that the anatomical and functional
information of the heart can be obtained simultaneously. Two self-navigated
4D cardiac MRI methods have recently been proposed for simultaneous
visualization of cardiac function and cardiac motion-resolved coronary
arteries with isotropic higher spatial resolution, in which respiratory motion
was corrected using either displacement-based or affine transform-based
registrations (130,147). Despite improved scan efficiency compared to the
navigator-gated acquisition, motion correction usually requires the use of
various registration algorithms that are based on specific motion models,
which may be insufficient to account for the complex 3D movement of the
heart during respiration, especially for patients with pronounced respiration
or irregular respiratory patterns.

188
Compressed sensing has become a powerful approach for fast
cardiac imaging, and in addition to enabling increased acquisition speed, it
has been shown that sparsity can be also used to resolve respiratory
motion by reconstructing an extra motion-state dimension (Chapter 6). A
corresponding technique called XD-GRASP was developed in Chapter 6 to
combine the self-navigation properties of radial sampling and the
acceleration capability of compressed sensing (120). XD-GRASP offers a
different way to handle various types of motion without performing motion
correction, while nearly 100% scan efficiency can be maintained. The
purpose of this work is to extend the XD-GRASP framework into 3D golden-
angle radial sampling and test the new imaging framework in 3D whole-
heart MRI. Specifically, XD-GRASP is first applied for ECG-triggered
respiratory motion-resolved whole-heart coronary MRA, and then applied to
demonstrate a continuous five-dimensional (x-y-z-cardiac-respiration)
whole-heart imaging framework with both high spatial and temporal
resolutions, which allows simultaneous evaluation of myocardial function
and cardiac and respiratory motion-resolved whole-heart arterial anatomy.
7.3. 3D Phyllotaxis Golden-Angle Radial Sampling
Figure 7.1 shows a comparison of golden-angle radial sampling
schemes that are based on stack-of-stars pattern (Figure 7.1a) and spiral
phyllotaxis pattern (141) (Figure 7.1b), respectively. When compared with

189
Figure. 7.1: Comparison of golden-angle radial sampling schemes that are based on stack-of-stars pattern (a) and spiral phyllotaxis pattern (b), respectively. When compared with the stack-of-stars scheme, radial sampling is also employed along the kz dimension in the 3D phyllotaxis sampling trajectory, so that each k-space line passes through the center of k-space and an image can be reconstructed with isotropic spatial resolution. The 3D radial sampling pattern in (b) can be segmented into multiple heartbeats for cardiac MRI, with golden-angle rotation along the z-axis between every two successive data interleaves. An additional spoke oriented along the superior-inferior (SI) direction (red lines) can be acquired at the beginning of each data interleave for respiratory motion detection and self-navigation.
the stack-of-stars scheme, radial sampling is also employed along the kz
dimension in the 3D phyllotaxis sampling trajectory, so that each k-space
line passes through the center of k-space and an image can be
reconstructed with isotropic spatial resolution. As described in (141), this 3D
radial sampling pattern can be segmented into multiple heartbeats for
cardiac MRI, with golden-angle rotation along the z-axis between every two
successive data interleaves. Besides, an additional spoke oriented along
the superior-inferior (SI) direction (red lines in Figure 7.1b) can be acquired

190
at the beginning of each data interleave for respiratory motion detection and
self-navigation. Similar to stack-of-stars golden-angle radial sampling, the
phyllotaxis 3D radial acquisition scheme also allows for sorting of all the
interleaves into different respiratory states according to their corresponding
respiratory phases, in which approximately uniform and distinct k-space
coverage can be achieved in each motion state.
7.4. Free-Breathing Whole-Heart MRI
The XD-GRASP framework with 3D golden-angle radial sampling
was implemented and tested for two whole-heart cardiac MRI studies, as
described in the following subsections. All the data were acquired at the
University of Lausanne. Human imaging was performed in accordance with
protocols approved by the University of Lausanne Institutional Review
Board and was found to comply with the HIPAA. All subjects provided
written informed consent before the imaging.
7.4.1. ECG-Triggered Free-Breathing Whole-Heart Coronary MRA
Free-breathing whole-heart coronary MRA was performed on 11
healthy volunteers on a 1.5T clinical MRI scanner (MAGNETOM Aera,
Siemens AG, Healthcare Sector, Erlangen, Germany) equipped with a total
number of 30 receiver coil elements (18 chest and 12 spine). Imaging was
performed with ECG-triggering and the acquisition window, which was set

191
around ~80-100ms, was placed in mid-diastole and adapted to the heart
rate of individual subject. The trigger delay time was set by visual inspection
of the most quiescent diastolic phase on a mid-ventricular short axis cine
image series acquired in free breathing with 3 averages, prior to the whole-
heart coronary MRA scan. k-Space data were acquired without any external
gating using a prototype 3D radial b-SSFP sequence with golden-angle
rotation scheme based on the spiral phyllotaxis pattern. The data
acquisition was employed with non-slice-selective pulses, T2 magnetization
preparation and fat-saturation. Relevant imaging parameters included:
TR/TE = 3.1/1.56ms, FOV = 220 x 220 x 220 mm3, matrix size = 192 x 192
x 192, voxel size = 1.15 x 1.15 x 1.15 mm3, RF excitation angle=90°, and
receiver bandwidth=898 Hz/Pixel. A total number of 12320 radial readouts
were acquired over 385 heartbeats in each subject, including 385 golden-
angle interleaves and 32 spokes in each of them. As described in the
previous section, each interleave started with a spoke oriented along the SI
direction for self-navigation
7.4.2. Free-Breathing Continuous Whole-Heart MRI
Continuous whole-heart MRI was performed on 9 healthy volunteers
during free-breathing without ECG triggering and any external gating on the
same 1.5T clinical scanner (MAGNETOM Aera, Siemens AG, Healthcare
Sector, Erlangen, Germany). k-Space data were continuously acquired

192
using the same prototype 3D radial b-SSFP sequence with golden-angle
rotation scheme. Imaging parameters included: TR/TE = 3.1/1.56 ms, FOV
= 220 x 220 x 220 mm3, matrix size = 192 x 192 x 192, voxel size = 1.15 x
1.15 x 1.15 mm3, and flip angle=90o. A total number of 126478 spokes were
acquired in each subject in 14 minutes and 17 seconds, including 5749
golden-angle interleaves and 22 spokes in each of them. Each interleave
started with a spoke oriented along the SI direction for self-navigation and
was preceded by CHESS fat saturation. More information on this
continuous whole-heart cardiac imaging sequence can be found in (147).
7.5. Motion Estimation
For ECG-triggered free-breathing whole-heart coronary MRA,
respiratory motion signal was detected using a technique recently proposed
by Bonanno (148). Specifically, the k-space center amplitude (KCA) in each
coil element was first obtained by averaging the absolute value of three
central points of the self-navigation readouts acquired at the beginning of
each data segment. Independent component analysis (ICA) (149) was then
performed on the KCA signals from all the coils to identify different
components. The one that can best represent respiration was selected and
used as the respiratory motion signal for subsequent data binning.
For continuous whole-heart imaging, the self-navigation spokes
acquired at the beginning of each interleave (red lines in Figure 7.1b) were

193
Figure. 7.2: (a) Data sorting procedure in XD-GRASP reconstruction for ECG-triggered whole-heart coronary MRA, in which the 3D golden-angle radial k-space data are sorted into 4 respiratory motion states spanning from expiration (top) to inspiration (bottom) (x-y-z-respiratory) using the respiratory motion signals drived from the acquired data. The sorting procedure is performed so that the number of spokes grouped in each motion state is the same. Approximately uniform coverage of k-space with distinct sampling patterns in each motion state can be achieved, as shown in (b)&(c).
used to extract respiratory motion signals of the acquired datasets. Similar
to the approach employed in Chapter 6 for abdominal imaging, a 1D
partition-direction FFT was performed on the self-navigation spokes and
principal component analysis was performed along the concatenated z+coil
dimension to determine the most common signal variation mode among all
the coil elements. The principal component with the highest peak in the
frequency range of 0.1-0.5Hz was selected to represent the respiratory
motion signal. Cardiac motion signal was obtained retrospectively from the
ECG trace.

194
7.6. Data Sorting
7.6.1. ECG-Triggered Free-Breathing Whole-Heart Coronary MRA
Figure 7.2a illustrates the data sorting procedure in XD-GRASP
reconstruction for ECG-triggered whole-heart coronary MRA, in which the
3D golden-angle radial k-space data are sorted into 4 respiratory motion
states spanning from expiration (top) to inspiration (bottom) (x-y-z-
respiratory) using the respiratory motion signals, so that respiratory motion
can be resolved and additional sparsity can be exploited along the new
dynamic dimension. Similar to the procedure described in Chapter 6, the
sorting procedure is performed such that the number of spokes grouped in
each motion state is the same. Due to the golden-angle acquisition scheme,
approximately uniform coverage of k-space with distinct sampling patterns
in each motion state can be achieved, as shown in Figure 7.2b. It has been
demonstrated in Chapter 6 that four respiratory states achieved a good
balance between the depiction of respiratory motion and residual streaking
artifact in abdominal imaging. Similarly, four respiratory states were also
found to provide a good balance in this study.
7.6.2. Free-Breathing Continuous Whole-Heart MRI
The continuously acquired whole-heart cardiac datasets were first
sorted into 20 cardiac phases (temporal resolution of ~40-50ms depending
on the heart rate) without any view sharing using the cardiac motion signal

195
Figure. 7.3: Five-dimensional data sorting in free running continuous whole-heart imaging, with one cardiac motion dimension (20 cardiac phases) and one respiratory motion-state dimension (4 respiratory states).
obtained from the ECG trace, and each cardiac phase was further sorted
into 4 respiratory motion states spanning from end-expiration to end-
inspiration using the estimated respiratory motion signal, thus generating a
5D image set (x-y-z-cardiac-respiratory), as shown in Figure 7.3.
7.7. Image Reconstruction
For ECG-triggered whole-heart coronary MRA, XD-GRASP
reconstruction was performed by employing a temporal sparsity constraint
along the new respiratory dimension by solving the following optimization
problem:
2
2 1min
dd F C d m S d (7.1)

196
Here, F is the non-uniform fast Fourier transform (NUFFT) operator (135)
defined for the 3D golden angle radial sampling pattern, C represents the
multiple-elements coil sensitivity maps with dimensionality of x-y-z-coil,
where x, y and z represent three spatial dimensions. d is the 4D dynamic
image-series with the sorted respiratory-state dimension
(size=192x192x192x4), and m is the corresponding multicoil radial k-space
data sorted according to the new dimensions. S is the sparsifying transform
applied in the respiratory motion dimension with regularization parameter .
For continuous whole-heart MRI, XD-GRASP reconstruction was
performed by solving:
2
1 1 2 22 1 1min
dd F C d m S d S d (7.2)
where F is the NUFFT operator as before, C represents the multiple-
elements coil sensitivity maps with dimensionality of x-y-z-coil, d is the 5D
image set to be reconstructed (size=192x192x192x20x4), and m is the
corresponding multicoil radial k-space data. S1 and S2 are the sparsifying
transforms applied along the cardiac and respiratory motion dimensions,
respectively, with regularization parameters 1 and 2 .
All the reconstructions were performed offline in MATLAB
(Mathworks, Natick, MA, USA) using a server equipped with two 16-core
Opteron CPUs, 256 GB RAM, and two NVIDIA graphics processing unit
(GPU) cards with 6 GB memory in each of them. In order to speed up the

197
reconstruction, the NUFFT operation was implemented using parallel
computing on GPUs, and was called in the main reconstruction program
implemented in MATLAB (150). Same as in Chapter 6, temporal finite
differences, also known as total-variation minimization, was used in the
reconstructions as the sparsifying transform. The non-linear conjugate
gradient optimization employed in the previous chapters was used to solve
the optimization problems. Coil sensitivity maps were computed from
reference multicoil images given by NUFFT reconstruction of the whole
dataset, using the adaptive array combination method (40). The averaged
XD-GRASP reconstruction time was ~20-30 minutes for each ECG-
triggered whole-heart coronary MRA dataset (size=192x192x192x4) and
was ~8 hours for each continuously acquired whole-heart dataset
(size=192x192x192x20x4).
For comparison purpose, all the ECG-triggered coronary MRA
datasets were also reconstructed using a 1D self-navigation motion
correction algorithm previously described in (143). Meanwhile, 4D
reconstruction with respiratory motion correction (MC), as described in
(147), was also performed on all the continuously acquired cardiac
datasets, in which 20 cardiac phases were generated without any view
sharing (size=192x192x192x20) and were reconstructed using compressed

198
sensing that exploits sparsity along the cardiac dimension only using a
total-variation constraint.
7.8. Image Quality Comparison
7.8.1. ECG-Triggered Free-Breathing Whole-Heart Coronary MRA
For ECG-triggered whole-heart coronary MRA, images at the end-
expiratory motion states were selected in XD-GRASP results for image
quality comparison. All the images, including XD-GRASP and 1D motion
correction reconstruction, were randomized for blinded evaluation. Two
coronary MRA experts scored the visualization/sharpness of the left main
coronary artery, the proximal segment of left circumflex coronary artery
(LCX), and the proximal, middle, distal segments of both right coronary
artery (RCA) and left anterior descending coronary artery (LAD) on a 5-
point scale classifying the definition of the vessel borders as follows: 0 = not
visible, 1 = markedly blurred, 2 = moderately blurred, 3 = mildly blurred and
4 = sharply defined. The reported scores represent mean ± standard
deviation, and a paired student's t-test was used for statistical analysis,
where P < 0.05 suggested statistical significance.
Additionally, the diagnostic quality and visibility of left main coronary
artery, the proximal segment of LCX, and each segment of RCA and LAD
were scored for all the coronary datasets on a 3-point scale (diagnostic
grading) by an experienced cardiovascular MR radiologist, who was

199
completely blinded to the type of reconstruction used. The scale used was:
0 = nonvisible, 1 = visible but non diagnostic and 2 = visible and diagnostic.
7.8.2. Free-Breathing Continuous Whole-Heart MRI
For continuously acquired whole-heart datasets, one end-systolic
frame and one mid-diastolic frame were manually selected from each
subject (in both the 4D reconstruction and the end-expiratory state of the
5D reconstruction) and all the images were randomized for blinded
evaluation. An experienced cardiovascular MR radiologist scored the
visualization/sharpness of myocardium, the LCX, and the proximal segment
of RCA and LAD on a 1-5 (non-diagnostic to excellent) scale. The reported
scores represent mean ± standard deviation, and a paired student's t-test
was used for statistical analysis, where P < 0.05 suggested statistical
significance.
7.9. Results
7.9.1. ECG-Triggered Free-Breathing Whole-Heart Coronary MRA

200
Figure. 7.4: Comparison of XD-GRASP reconstruction (end-expiratory motion states) with the 1D respiratory motion correction reconstruction in two representative datasets. XD-GRASP improves the delineation of coronary arteries and removes the blurring effects by resolving the respiratory motion.
Figure 7.4 compares the XD-GRASP reconstruction (end-expiratory
motion states) with the 1D respiratory motion correction reconstruction in
two representative ECG-triggered whole-heart coronary datasets. XD-
GRASP removes the blurring effects by resolving the respiratory motion,
and thus improves the delineation of coronary arteries, myocardium and the

201
Figure. 7.5: End-expiratory myocardial wall (SAX and 4CH), proximal coronary arteries, right coronary artery (RCA) and left anterior descending coronary artery (LAD) in diastolic (top) and systolic (bottom) phases. All the images are reformatted from a single continuous data acquisition with 5D XD-GRASP reconstruction.
papillary muscles. The readers’ scores for qualitative comparison of
different coronary arteries are summarizes in Table 7.1.
The comparison of diagnostic quality and visibility of different
coronary arteries are summarized in Table 7.2. The diagnostic scores for
XD-GRASP reconstructions were higher than the 1D respiratory motion
correction reconstructions in left main coronary artery, and different
segments of both LAD and RCA.
7.9.2. Free-Breathing Continuous Whole-Heart MRI
Figure 7.5 shows the ventricular chambers and the coronary arteries
at end-expiration in one representative continuously acquired whole-heart
dataset, in both systolic (top) and diastolic (bottom) phases, derived from
the 5D XD-GRASP reconstruction. Coronary arteries are reformatted using

202
Figure. 7.6: 5D XD-GRASP reconstruction achieved reduced blurring, improved sharpness and better visualization of myocardium and the RCA compared with 4D reconstruction with respiratory motion correction (MC) in one representative volunteer with irregular respiratory pattern.
“Soap-Bubble” software (Philips Healthcare, Netherlands). Good delineation
of both myocardial wall and coronary arteries was obtained without using
any explicit respiratory motion correction algorithm.
Figure 7.6 shows the results from another volunteer who had an
irregular respiratory pattern during data acquisition. In this subject, 5D XD-
GRASP reconstructions exhibited reduced motional blurring and achieved
improved visualization of both myocardial wall and RCA (red arrows) when

203
1D Self-
Navigation XD-
GRASP(Exp)
LM 1.8±0.8 2.0±0.5
LDA (Prox) 1.5±0.8 1.9±0.5
LDA (Mid) 1.0±0.8 1.5±0.4*
LDA (Dist) 0.8±0.6 1.1±0.6
LCX (Prox) 1.1±0.7 1.0±0.5
RCA (Prox) 1.9±0.7 2.2±0.4*
RCA (Mid) 1.7±0.6 2.0±0.4*
RCA (Dist) 1.2±0.8 1.5±0.4
Table. 7.1: Readers’ scores for comparison of 1D self-navigation motion correction reconstruction v.s. XD-GRASP reconstruction (end-expiration only) in visualization/sharpness of RCA, LAD and left main coronary artery. 0-4: non-diastolic to
excellent. * Indicates statistical significance. LM: Left Main Coronary Artery.
compared to the 4D reconstruction with 1D respiratory motion correction.
The readers’ scores for qualitative comparison of different coronary arteries
are summarizes in Table 7.3.
7.10. Discussion
This chapter extends the XD-GRASP reconstruction presented in
Chapter 6 into 3D phyllotaixs golden-angle radial sampling, which offers
volumetric data acquisitions with isotropic spatial resolution up to ~1.1mm3,
enabling acceleration and exploitation of incoherence along all the spatial
dimensions in compressed sensing reconstruction.
ECG-triggered acquisition scheme is still widely used in coronary
MRA and many other artery exams. Thus the new XD-GRASP framework
was first tested in ECG-triggered free-breathing whole-heart coronary MRA,
in which XD-GRASP combines the advantages of both conventional

204
Myocardium RCA (Prox) LAD (Prox) LM
4D 3.06±0.94 2.83±1.34 2.00±0.69 2.61±1.20
5D (Exp) 3.78±0.73* 3.44±1.20* 2.28±0.57* 3.22±1.17*
Table. 7.3: Reader’s scores for comparison of 4D reconstruction with motion correction v.s. 5D XD-GRASP reconstruction (end-expiration only) in visualization/sharpness of myocardium, the proximal segment of RCA, LAD and left main coronary artery. 1-5: non-diastolic to excellent. * Indicates statistical significance. LM: Left Main Coronary Artery
1D Self-
Navigation XD-
GRASP(Exp)
LM 1.8±0.4 2.0±0.0*
LDA (Prox) 1.6±0.5 2.0±0.0*
LDA (Mid) 1.3±0.6 1.4±0.5
LDA (Dist) 0.9±0.5 1.3±0.5
LCX (Prox) 1.4±0.7 1.4±0.7
RCA (Prox) 1.8±0.4 2.0±0.0
RCA (Mid) 1.3±0.5 1.7±0.5
RCA (Dist) 1.4±0.7 1.7±0.5
Table. 7.2: Readers’ scores for comparison of 1D self-navigation motion correction reconstruction v.s. XD-GRASP reconstruction (end-expiration only) in diastolic quality of RCA, LAD and left main coronary artery. 0 = not visible, 1 = visible, and 2 =
diagnostic. * Indicates statistical significance. LM: Left Main Coronary Artery.
navigator-gated acquisitions and self-navigation techniques. Coronary MRA
datasets are sorted into multiple respiratory motion states using the
respiratory motion signal derived from the acquired data. Instead of
performing registration-based motion correction, sparsity is exploited along
the new respiratory dimension. Therefore, it enables nearly 100% scan
efficiency and potentially avoids the interpolation errors that are typically
associated with the registration-based motion correction.
Compressed sensing has been previously applied for whole-heart

205
coronary MRA in many works (151-154). However, most of those
approaches were proposed to reduce the total acquisition time by exploiting
the spatial correlation. XD-GRASP works based on the fact that the
dynamic dimension usually has much higher correlation than the spatial
dimension, and thus the performance of compressed sensing
reconstruction can be substantially improved by exploiting temporal sparsity
instead of spatial sparsity only. Therefore, XD-GRASP represents a new
way of handling respiratory motion in coronary MRA.
Although good results have been achieved with the ECG-triggered
whole-heart coronary MRA, the data acquisition is only performed during
mid-diastole and thus the scan efficiency is not optimal. The reconstruction
performance can be largely improved if the acquisition is extended to cover
the entire cardiac cycles. Therefore, the XD-GRASP framework was also
applied for continuous whole-heart cardiac MRI, in which both ECG
triggering and external gating are not required during the scans and data
are acquired throughout the entire cardiac cycles. The continuously
acquired cardiac datasets are sorted into five dimensions, containing one
cardiac dimension and one respiratory dimension to resolve both cardiac
and respiratory motions. Compressed sensing is then employed to exploit
temporal sparsity along both dynamic dimensions. The proposed 5D XD-
GRASP reconstruction enables both high isotropic spatial resolution and

206
high temporal resolution for simultaneous assessment of myocardial
function in arbitrary orientations and visualization of coronary arteries at a
particular cardiac phase and respiratory motion-state.
In 5D whole-heart MRI, fat saturation is necessary to enable
visualization of arteries in small size, such as coronary arteries. Thus, the
steady state in the bSSFP sequence could be interrupted by the fat-
saturation modules. An alternative approach to solve this problem is to
switch the excitation pulses water-excitation pulses, which would maintain
the true steady state during the scans. For example, the image acquisition
proposed in (155) use FLASH sequence with water-excitation RF pulse at
3T scanners following slow contrast agent injection. However, FLASH
imaging may still suffers from reduced SNR when compared to bSSFP
imaging and the requirement for contract agent injection also exclude the
use of the techniques on patients with impaired kidney function.
Although ECG-triggering is not needed in the continuous 5D whole-
heart MRI, the ECG trace is still used to obtain cardiac motion signals.
Alternatively, cardiac motion signal can be also extracted directly from the
centers of k-space data or using the PCA approach as described in (130).
The possibility of extracting both cardiac and respiratory motion signals
simultaneously will be exploited in future works.

207
Additional works can be performed in the future to improve the
whole-heart MRI framework described in this chapter. First of all, the data
acquisition in 5D continuous whole-heart MRI is still very long (up to ~14
minutes). Additional experiments are needed in order to determine the
maximum acceleration so that the data acquisition can be shortened
accordingly. Besides, the image reconstruction time, especially in the 5D
image reconstruction, is very extensive and is not yet for clinical use. This
issue can be addressed by implementing the whole reconstruction steps in
GPUs or a workstation with clusters in the future. Moreover, the proposed
imaging framework can be also applied in other types of free-breathing
cardiac scans, such as 4D flowing imaging and late gadolinium
enhancement. Furthermore, these types of cardiac scans may be
potentially combined as a synergistic imaging framework that allows a push
button comprehensive examination of the cardiovascular system. Finally,
only qualitative comparison was performed in this study. Quantitative
comparison, in terms of the vessel sharpness, vessel length, could further
validate and strengthen the improvement and benefit of XD-GRASP
reconstruction compared to the existing reference approaches.
7.11. Conclusion
The extension of XD-GRASP framework into 3D golden-angle radial
sampling is a promising approach for whole-heart MRI. Challenges that are

208
associated with conventional navigator-gated acquisitions and self-
navigation approaches can be addressed and the advantages of both
techniques can be combined in XD-GRASP. The 5D whole-heart imaging
framework using XD-GRASP enables high isotropic spatial resolution and
high temporal resolution for assessment of myocardial function in arbitrary
orientations, and visualization of coronary arteries at particular cardiac
phases and respiratory motion-states.

209
Chapter 8
Summary and Future Work
The main contributions of this dissertation are the development of
novel MRI techniques that enable rapid and continuous data acquisition
during free breathing. Particularly, two techniques named GRASP and XD-
GRASP have been developed. GRASP represents an efficient and flexible
dynamic imaging framework, which enables continuous data acquisition
and user-defined reconstruction of temporal frames. GRASP offers notable
advantages for dynamic imaging, since the time dimension is defined
retrospectively and the same dataset can be reconstructed in different ways
according to the target application. The tools that enable this flexibility are
golden-angle radial sampling, which allows for quasi-arbitrary data sorting;
and the combination of compressed sensing and parallel imaging, which is
used to reconstruct the sorted undersampled dynamic image series. XD-
GRASP moves a step forward and proposes a new use of sparsity to

210
handle different types of motion in MRI. Instead of preventing or correcting
for motion, extra motion dimensions are explicitly reconstructed in XD-
GRASP using compressed sensing ideas. In this chapter, contributions of
this dissertation are summarized first and an outlook for the future is
discussed afterwards.
8.1. Chapter Summaries
k-t SPARSE-SENSE (30) is a reconstruction framework previously
developed in our group to combine compressed sensing and parallel
imaging using a SENSE-type formalism for accelerated Cartesian imaging.
Instead of performing compressed sensing reconstruction in each individual
coil separately, k-t SPARSE-SENSE proposes to exploit joint sparsity in the
multicoil images by taking advantage of the additional sensitivity encoding
capabilities provided by coil arrays, so that the imaging speed and the
reconstruction performance can be significantly improved. The dissertation
started with two applications of k-t SPARSE-SENSE for accelerated
dynamic imaging in Chapter 3 (MR parameter mapping) and Chapter 4
(real-time cardiac cine MRI). The performance of several temporal
sparsifying transforms, including temporal fast Fourier transform (FFT),
temporal principal component analysis (PCA) and temporal total-variation
(TV), were compared and tailored for compressed sensing reconstruction in
different clinical applications.

211
Although k-t SPARSE-SENSE has been applied to various clinical
applications with promising results, the performance of compressed sensing
is fundamentally limited in Cartesian imaging, since acceleration can only
be achieved along the phase-encoding dimension, limiting the use of
sparsity and incoherence. The ability to perform compressed sensing in
higher-dimensional datasets, e.g., in 3D datasets or in dynamic datasets
with both spatial and temporal dimensions, would improve the
reconstruction performance, since high-dimensional datasets are more
compressible and incoherent aliasing artifacts can be distributed over a
larger space with lower values. In addition, Cartesian imaging is sensitive to
motion, which usually results in ghosting artifacts in the reconstructed
image. Non-Cartesian imaging can effectively accelerate all spatial
dimensions and thus sparsity can be fully exploited. Furthermore, non-
Cartesian imaging (e.g., radial imaging) has reduced sensitivity to motion
due to the averaging effects associated with repeated sampling of the k-
space center, and thus ghosting artifacts can be avoided. In Chapter 5, the
reconstruction framework of k-t SPARSE-SENSE was applied to golden-
angle radial sampling and a new imaging technique, named Golden-angle
RAdial Sparse Parallel MRI (GRASP), was proposed. GRASP represents
an efficient and simplified imaging paradigm for clinical workflow, which
enables continuous data acquisitions during free breathing and image

212
reconstructions with retrospectively selected temporal information.
Meanwhile, the GRASP workflow can also maximize the amount of
information per unit time in a wide range of clinical applications and
facilitate the use of compressed sensing for clinical studies.
As presented in Chapter 5, GRASP allows rapid and continuous
free-breathing abdominal imaging, which is mainly attributed to the
combination of compressed sensing and parallel imaging, and also the
motion robustness of radial sampling. However, it only handles moderate
motion and it is not the ultimate solution for free-breathing imaging. Our
initial clinical evaluation also suggests that in certain patients, the image
quality is still suboptimal due to substantial respiration. The image blurring
introduced in these cases results in loss of vessel-tissue contrast and may
prevent the detection of suspected lesions with small size. Therefore, a
novel image reconstruction framework named eXtra Dimensional GRASP
(XD-GRASP) was developed, as described in Chapter 6. In XD-GRASP,
the continuously acquired data are first sorted into multiple motion states
(e.g., respiratory states) using a motion signal extracted directly from the
data, and a GRASP-type reconstruction is then applied to exploit sparsity in
the new dimension and remove undersampling artifacts. XD-GRASP
represents a novel use of sparsity to handle physiological motion, where
instead of removing or correcting for motion, extra respiratory-state

213
dimensions are reconstructed, which improves image quality and offers
access to new physiological information that was previously inaccessible
and could be of potential clinical value.
The GRASP and XD-GRASP techniques proposed in Chapters 5
and 6 employed stack-of-stars radial sampling for volumetric imaging. This
sampling scheme is relatively simple to implement and reconstruct, but the
fact that the kz dimension is sampled on a Cartesian grid introduces some
limitations. First, the incoherence along the slice dimension is limited and
thus the overall acceleration is reduced. Although random undersampling
could be implemented along the kz dimension as well, it would not be as
efficient as in the radial plane. Second, the number of slices that can be
acquired is limited and interpolation is usually required, which leads to
compromises in spatial resolution along the slice dimension. Third,
application of stack-of-stars sampling to 3D cardiac cine imaging is limited
because it may fail to capture the cardiac contraction when a large number
of slices are acquired. In order to increase the spatial coverage and extend
compressed sensing to a true 3D isotropic spatial coverage, a 3D golden-
angle radial sampling based on the spiral phyllotaxis pattern is employed for
XD-GRASP in Chapter 7. The proposed framework was first employed for
ECG-triggered whole-heart coronary MRA with improved respiratory motion
compensation and was then applied to continuous five-dimensional whole-

214
heart imaging with high spatial and temporal resolutions, which allows
simultaneous assessment of cardiac function in arbitrary planes and
visualization of cardiac and respiratory motion-resolved whole-heart arterial
anatomy.
8.2. An Outlook for the Future
Despite remarkable progress in imaging speed that has been
achieved over the past decades, the day-to-day practice of MRI is still
fundamentally limited due to the comparatively slow, complex, and
parameter-oriented imaging process compared with other imaging
modalities such as CT. This complexity results in part from the rich diversity
of acquisition approaches, reconstruction algorithms, and tissue contrast
mechanisms enabled by the magnetic resonance phenomenon. Therefore,
it is desirable to have an imaging paradigm that makes MRI simple and
information-rich, and shifts from time-consuming inefficient tailored
acquisitions to a push-button process that allows rapid and continuously
updated acquisitions with comprehensive information. This shift has the
capacity to change the paradigm of everyday clinical imaging, enabling
faster imaging with less operator-dependent planning, and to enhance
information content for research imaging as well.
While the paradigm of rapid, continuous and comprehensive imaging
described above has not been entirely achieved in this dissertation, the

215
work presented here can significantly improve the way that MRI exams are
performed every day. There are several directions that can be exploited in
the future to strengthen this work. For example, the GRASP or XD-GRASP
pipeline may be combined with MR Fingerprinting (MRF) (156), which
extracts various physical parameters such as T1, T2 and proton density from
a single MR scan. Currently the implementation of MRF is based on a pixel-
by-pixel pattern recognition using a dictionary database of signal evolution
time courses. However, the resulting images may be contaminated with
artifacts in cases of extreme undersampling, and thus the reliability of the
matching process can be reduced. GRASP can be applied to remove some
of the undersampling artifacts with a temporal sparsifying transform and
thus could potentially improve the pattern-matching performance. In
addition, most of the existing applications of MRF have been focused on
static organs such as the brain, because any physiological motion – and
most particularly through-plane motion – could introduce bias into the
observed spin dynamics. Therefore, it is challenging to extend MRF into
abdominal or chest wall exams. XD-GRASP may be a useful approach to
resolve cardiac, respiratory, and abdominal motion, and to provide reliable
signal evolution mapping in the presence of physiological motion. This
combination could have the potential to achieve rapid and continuous data

216
acquisitions with comprehensive information content for different clinical
needs.
The five-dimensional whole-heart imaging framework proposed in
Chapter 7 enables simultaneous evaluation of myocardial function and
whole-heart artery anatomy. The framework can be directly extended into
other scan types in cardiac MRI, such as perfusion imaging, late
gadolinium enhancement imaging, and multidimensional flow imaging.
Several different scan types may also be combined in a synergistic imaging
framework that allows a push-button comprehensive examination of the
cardiovascular system.
The advent of commercial MR-PET scanners has garnered
tremendous attention among researchers from both the MRI and the PET
community in the past few years. Although current state-of-the-art MR-PET
scanners are capable of performing simultaneous acquisition of both MRI
and PET data, the image reconstructions are usually performed separately
and the results are combined at the final stage for visualization. Since MRI
and PET images are acquired in the same organs, they share the same
anatomy and there are correlations between the images that can be
exploited to improve the reconstruction performance and image quality.
Preliminary results have already been reported for a new iterative joint
reconstruction framework based on the combination of compressed sensing

217
and parallel imaging that exploits the anatomical correlations between MR
and PET images using a joint sparsity constraint (157). However, most of
the current experiments are still performed in static organs, such as brain,
due to the easy alignment of images from two modalities. XD-GRASP could
be useful for joint MR-PET reconstruction in moving organs, such as liver,
kidney or heart. First, motion detected in the MRI data can be used to sort
both MRI and PET data into extra motion dimensions, so that physiological
motion, such as respiratory motion, can be resolved (158). Afterwards, the
sorted MRI and PET data can be effectively aligned, so that the correlation
between MRI and PET images in different motion states can be exploited
simultaneously for improved joint reconstruction.
One of the major limitations of compressed sensing reconstruction
for clinical studies is the long computation time for the non-linear iterative
reconstruction process. Moreover, large data size further imposes
challenges on computation time and requires adequate hardware and
software implementation. The GRASP and XD-GRASP reconstruction can
be implemented in graphical processor units (GPUs), which are expected to
provide good performance for computation of highly-parallel transforms
such as FFT and wavelets. However, the performance of GPUs may
decrease for the processing of large datasets due to limited GPU memory.
Clusters of multicore computers could offer better performance for

218
management of large datasets. Therefore, an appropriate combination of
both platforms is expected to provide faster reconstructions. In additional to
parallel implementation of the reconstruction algorithms, coil compression
methods and numerical optimization algorithms with faster convergence
could also be exploited to further increase the computation speed.

219
Chapter 9
List of Publications
9.1. Journal Papers
1. Feng L, Axel L, Chandarana H, Blick KT, Sodickson DK, Otazo R. “XD-GRASP: Golden-Angle Radial MRI with Reconstruction of Extra Motion-State imensions Using Compressed Sensing” Magn Reson Med. 2015 Mar 25. doi: 10.1002/mrm.25665. [Epub ahead of print]
2. Feng L, Grimm R, Block KT, Chandarana H, Kim S, Xu J, Axel L, Sodickson DK, Otazo R. “Golden-Angle Radial Sparse Parallel MRI: Combination of Compressed Sensing, Parallel Imaging, and Golden-Angle Radial Sampling for Fast and Flexible Dynamic Volumetric MRI” Magn Reson Med . 2014 Sep;72(3):707-17
3. Feng L, Srichai MB, Lim RP, Harrison A, King W, Adluru G, Dibella E,
Sodickson DK, Otazo R, Kim D. “Highly-Accelerated Real-Time Cardiac Cine MRI Using k-t SPARSE-SENSE” Magn Reson Med. 2013 Jul; 70(1): 64-74
4. Feng L, Otazo R, Jung H, Jensen JH, Ye JC, Sodickson DK, Kim D.
“Accelerated Cardiac T2 Mapping Using Breath-Hold Multiecho Fast Spin-Echo Pulse Sequence with k-t FOCUSS” Magn Reson Med. 2011 Jun; 65(6):1661-9

220
5. Feng L, Donnino R, Babb J, Axel L, Kim D. “Numerical and in vivo validation of fast cine displacement-encoded with stimulated echoes (DENSE) MRI for quantification of regional cardiac function” Magn Reson Med. 2009 Sep;62(3):682-90
6. Chandarana H, Feng L, Ream J, Wang Annie, Babb JS, Block KT,
Sodickson DK, Otazo R. “Respiratory Motion-Resolved Compressed Sensing Reconstruction of Free-Breathing Radial Acquisition for Dynamic Liver MRI” Accepted for publication in Investigative Radiology. May, 2015
7. Chandarana H, Feng L, Block KT, Rosenkrantz AB, Lim RP, Chu D,
Sodickson DK, Otazo R. “Free-Breathing Dynamic Contrast-Enhanced MRI of the Liver with Radial Golden-Angle Sampling Scheme and Advanced Compressed-Sensing Reconstruction” Investigative Radiology. 2013 Jan;48(1):10-6
8. Parasoglou P, Feng L, Xia D, Otazo R and Regatte RR. “Rapid 3D-
Imaging of Phosphocreatine Recovery Kinetics in the Human Lower Leg Muscles with Compressed Sensing” Magn Reson Med. 2012 Dec;68(6):1738-46
9. Rosenkrantz AB, Geppert C, Grimm R, Block TB, Glielmi C, Feng L,
Otazo R, Ream JM, Romolo MM, Taneja SS, Sodickson DK, Chandarana H. “Dynamic Contrast-Enhanced MRI of the Prostate with High Spatiotemporal Resolution using Compressed Sensing, Parallel Imaging, and Continuous Golden-Angle Radial Sampling: Preliminary Experience” Journal of Magnetic Resonance Imaging. 2015 May;41(5):1365-73
10. Kim D, Dyvorne HA, Otazo R, Feng L, Sodickson DK, Lee VS.
“Acelerated phase-contrast cine MRI using k-t SPARSE-SENSE” Magn Reson Med. 2012 Apr;67(4):1054-64
11. Kim D, Jensen JH, Wu EX, Feng L, Au WY, Cheung JS, Ha SY, Sheth
SS, Brittenham GM. “Rapid monitoring of iron-chelating therapy in thalassemia major by a new cardiovascular MR measure: the reduced transverse relaxation rate” NMR Biomed. 2011 Aug;24(7):771-7
12. Wu EX, Kim D, Tosti CL, Tang H, Jensen JH, Cheung JS, Feng L, Au WY, Ha SY, Sheth SS, Brown TR, Brittenham GM. “Magnetic resonance assessment of iron overload by separate measurement of

221
tissue ferritin and hemosiderin iron” Ann N Y Acad Sci. 2010 Aug;1202:115-22
9.2. Conference Contributions (First Author)
2015 1. Li Feng, Daniel K Sodickson, Ricardo Otazo “Rapid Free-
Breathing Dynamic Contrast-Enhanced MRI Using Motion-Resolved Compressed Sensing” (IEEE ISBI 2015, Brooklyn, NY, USA)
2. Li Feng, Simone Coppo, Davide Piccini, Ruth P Lim, Matthias Stuber, Daniel K Sodickson, and Ricardo Otazo “Five-Dimensional Cardiac and Respiratory Motion-Resolved Whole-Heart MRI” (ISMRM 2015, Toronto, Canada)
3. Li Feng, Hersh Chandarana, Davide Piccini, Justin Ream, Daniel K Sodickson, and Ricardo Otazo “Rapid Free-Breathing Dynamic Contrast-Enhanced MRI Using Motion-Resolved Compressed Sensing” (ISMRM 2015, Toronto, Canada)
2014 4. Li Feng, Leon Axel, Jian Xu, Daniel K Sodickson, Ricardo Otazo
“Rapid Real-Time Cardiac MRI Exploiting Synchronized Cardio-Respiratory Sparsity” (ISMRM 2014, Milan, Italy)
5. Li Feng, Leon Axel, Darragh Halpenny, Larry Latson, Jian Xu,
Daniel K Sodickson, Ricardo Otazo “Evaluating both “Normal” and “Ectopic” Cardiac Cycles in Patients with Arrhythmias Using Free-Breathing Compressed Sensing MRI with Physiological Motion Synchronization” (ISMRM 2014, Milan, Italy)
6. Li Feng, Daniel K Sodickson, Ricardo Otazo “A Robust and Automatic Cardiac and Respiratory Motion Detection Framework for Self-Navigated Radial MRI” (ISMRM 2014, Milan, Italy)
7. Li Feng, Leon Axel, Larry A Latson, Jian Xu, Daniel K Sodickson
and Ricardo Otazo “Compressed sensing with synchronized cardio-respiratory sparsity for free-breathing cine MRI: initial

222
comparative study on patients with arrhythmias” (SCMR 2014, New Orleans, LA, USA)
8. Li Feng, Leon Axel, Jian Xu, Daniel K Sodickson, Ricardo Otazo “Synchronized cardiac and respiratory sparsity for rapid free-breathing cardiac cine MRI” (SCMR 2014, New Orleans, LA, USA)
2013
9. Li Feng, Leon Axel, Jian Xu, Jing Liu, Daniel K Sodickson, Ricardo Otazo “Rapid Free-Breathing 4D Time-Resolved Non-Contrast Aorta MRA without Cardiac Triggering and External Gating” (2013 International Magnetic Resonance Angiography Workshop, New York, NY, USA)
10. Li Feng, Jing Liu, Kai Tobias Block, Jian Xu, Leon Axel, Daniel K Sodickson, and Ricardo Otazo “Compressed Sensing Reconstruction with an Additional Respiratory-Phase Dimension for Free-Breathing Imaging” (ISMRM 2013, Salt Lake City, USA)
2012
11. Li Feng, Hersh Chandarana, Jian Xu, Kai Tobias Block, Daniel
Sodickson, and Ricardo Otazo “K-t Radial SPARSE-SENSE: Combination of Compressed Sensing and Parallel Imaging with Golden Angle Radial Sampling for Highly Accelerated Volumetric Dynamic MRI” (ISMRM 2012, Melbourne, Australia)
12. Li Feng, Jian Xu, Leon Axel, Daniel Sodickson, and Ricardo Otazo “High Spatial and Temporal Resolution 2D Real Time and 3D Whole-Heart Cardiac Cine MRI Using Compressed Sensing and Parallel Imaging with Golden Angle Radial Trajectory” (ISMRM 2012, Melbourne, Australia)
13. Li Feng, Monvadi Barbara Srichai-Parsia, Ruth P Lim, Alexis Harrison, Wilson King, Ganesh Adluru, Edward Dibella, Daniel Sodickson, Ricardo Otazo, and Daniel Kim “Quantitative Assessment of Highly Accelerated Real Time Cardiac Cine MRI Using Compressed Sensing and Parallel Imaging” (ISMRM 2012, Melbourne, Australia)
2011

223
14. Li Feng, Jian Xu, Kim Dan, Axel Leon, Sodickson K Deniel, Otazo,
Ricardo “Combination of Compressed Sensing, Parallel Imaging and Partial Fourier for Highly-Accelerated 3D First-Pass Cardiac Perfusion MRI” (ISMRM, 2011, Montreal, Canada)
15. Li Feng, Ricardo Otazo, Monvadi B Srichai, Ruth P Lim, Daniel K. Sodickson, Daniel Kim “Highly-Accelerated Real-Time Cine MRI using Compressed Sensing and Parallel Imaging with Cardiac Motion Constrained Reconstruction” (ISMRM, 2011, Montreal, Canada)
16. Li Feng, Ricardo Otazo, Monvadi B Srichai, Ruth P Lim, Daniel K Sodickson, Daniel Kim “Highly-Accelerated Real-Time Cine MRI using Compressed Sensing and Parallel Imaging” (SCMR, 2011, Nice, France)
2010 17. Li Feng, Ricardo Otazo, Monvadi B. Srichai, Ruth P. Lim, Ding
Xia, Daniel K. Sodickson, Daniel Kim “Highly-Accelerated Real-Time Cine MRI Using Compressed Sensing and Parallel Imaging”, (ISMRM, 2010, Stockholm, Sweden)
18. Li Feng, Ricardo Otazo, Jens Jensen, Daniel K. Sodickson, Daniel Kim “Accelerated Breath-Hold Multi Echo FSE Pulse Sequence Using Compressed Sensing and Parallel Imaging for T2 Measurement in the Heart” (ISMRM, 2010, Stockholm, Sweden)
2009 19. Li Feng, Daniel Kim “Theoretical Validation of Fast Cine DENSE
MRI for Quantification of Regional Cardiac Function” (ISMRM, 2009, Honolulu, USA)
20. Li Feng, Robert M. Donnino, James Babb, Leon Axel, Daniel Kim
“In Vivo Validation of Fast Cine DENSE MRI for the Quantification of Regional Cardiac Function” (ISMRM, 2009, Honolulu, USA)
21. Li Feng, Donnino RM, Axel L, Kim D “Quantitative assessment of
intramyocardial function using Cine DENSE MRI: a validation study” (SCMR, 2009, Orlando, Florida, USA)

224
9.3. Conference Contributions (Co-Author)
2015
22. Simone Coppo, Li Feng, Davide Piccini, Jerome Chaptinel, Gabriele Bonanno, Gabriella Vincenti, Juerg Schwitter, Ricardo Otazo, Daniel Sodickson and Matthias Stuber “Improved free-running self-navigated 4D whole-heart MRI through combination of compressed sensing and parallel imaging” (ISMRM 2015, Toronto, Canada)
23. Hersh Chandarana, Li Feng, Justin Ream, Annie Wang, James Babb, Kai T. Block, Mary Bruno, Daniel K. Sodickson, Ricardo Otazo “Respiratory motion-resolved compressed sensing reconstruction of free-breathing radial acquisition for improved dynamic liver MRI with an hepatobiliary contrast agent” (ISMRM 2015, Toronto, Canada)
24. Ding Xia, Li Feng, Tiejun Zhao, and Ravinder R. Regatte “Highly-
Accelerated 3D T1rho Mapping of the Knee Using k-t SPARSE-SENSE” (ISMRM 2015, Toronto, Canada)
25. Daniel K Sodickson, Li Feng, Florian Knoll, Martijn Cloos, Noam Ben-
Eliezer, Leon Axel, Hersh Chandarana, Tobias Block, Ricardo Otazo “The rapid imaging renaissance: sparser samples, denser dimensions, and glimmerings of a grand unified tomography” (SPIE Medical Imaging 2015, Orlando FL, USA)
2014
26. Parisa Amiri Eliasi, Li Feng, Ricardo Otazo, Sundeep Rangan
“Fast Magnetic Resonance Parametric Imaging via Structured Low-Rank Matrix Reconstruction” (2014 48th Asilomar Conference on Signals, Systems and Computers)
27. Jian Xu, Li Feng, Davide Piccini, Ricardo Otazo, Gabriele Bonanno, Florian Knoll, Edward K. Wong, Daniel K Sodickson “Feasibility of Free-Breathing Whole Heart Coronary MRA in Less Than 3 Minutes Using Combination of Compressed Sensing,

225
Parallel Imaging and A 3D Radial Phyllotaxis Trajectory” (ISMRM 2014, Milan, Italy)
28. Jian Xu, Li Feng, Ricardo Otazo, Ruth P Lim, Davide Piccini, Gabriele Bonanno, Yi Wang, Edward K. Wong, Daniel K Sodickson “Free-Breathing 3D Isotropic Whole Chest Non-Contrast MRA Using a Combination of Compressed Sensing and Parallel Imaging with Phyllotaxis Radial Trajectories” (ISMRM 2014, Milan, Italy)
29. Alicia W Yang, Li Feng, Daniel K Sodickson, Ricardo Otazo “Fast
and Simple Patch-Based Sparse Reconstruction Exploiting Local Image Correlations” (ISMRM 2014, Milan, Italy)
30. Jing Liu, Li Feng, David Saloner “Highly Accelerated Free-breathing 4D Cardiac Imaging with CIRCUS Acquisition” (ISMRM 2014, Milan, Italy)
31. Noam Ben-Eliezer, Li Feng, Kai Tobias Block, Daniel K Sodickson, Ricardo Otazo “Accelerated in vivo mapping of T2 relaxation from radially undersampled datasets using compressed sensing and model-based reconstruction” (ISMRM 2014, Milan, Italy)
32. Thomas Koesters, Li Feng, Kai Tobias Block, Michael Fieseler, Klaus P Schafers, Daniel K Sodickson, Frenado Boada “Simultaneous Acquisition of MR and PET data for Motion-Free PET Reconstruction” (ISMRM 2014, Milan, Italy)
33. Jing Liu, Henrik Haraldsson, Li Feng, David Saloner “Free-Breathing Whole Heart CINE Imaging with Inversion Recovery Prepared SSFP Sequence: Feasibility for Myocardium Viability Assessment” (ISMRM 2014, Milan, Italy)
34. Florian Knoll, Thomas Koesters, Ricardo Otazo, Tobias Block, Li Feng, Kathleen Vunckx, David Faul, Johan Nuyts, Fernado Boada, Daniel Sodickson “Simultaneous MR-PET Reconstruction using Multi Sensor Compressed Sensing and Joint Sparsity” (ISMRM 2014, Milan, Italy)

226
35. Elwin Bassett, Ricardo Otazo, Li Feng, Ganesh Adluru, Edward Dibella, Daniel Kim “Highly Accelerated Cine DENSE MRI with k-t SPARSE SENSE” (ISMRM 2014, Milan, Italy)
36. Nathaniel E. Margolis, Linda Moy, Akshat Pujara, Alana Amarosa, Eric E. Sigmund, Christian Geppert, Christopher Glielmi, Melanie Freed, Li Feng, and Ricardo Otazo, Amy N. Melsaether, Sungheon Kim “Initial experience: combination of MR pharmacokinetic modeling and FDG uptake using simultaneous dynamic contrast enhanced MRI and PET imaging” (ISMRM 2014, Milan, Italy)
37. Rosenkrantz AB, Geppert C, Grimm R, Block TK, Glielmi C, Li Feng, Otazo R, Ream JM, Romolo MM, Taneja SS, Sodickson DK, Chandarana H “Combined Compressed Sensing, Parallel Imaging, and Golden-Angle Radial Sampling for High Spatiotemporal Dynamic Contrast-Enhanced MRI of the Prostate” (ISMRM 2014, Milan, Italy)
38. Espagnet, Camilla Rossi; Bangiyev, Lev; Block, Kai Tobias; Grimm, Robert; Feng, Li; Ruggiero, Vito; Babb, James; Davis, Adam; Sodickson, Daniel K.; Fatterpekar, Girish “High Resolution DCE MRI of the Pituitary Gland Using Radial K Space Aquisition with Compressed Sensing Reconstruction” (ISMRM 2014, Milan, Italy)
39. Ream, Justin; Doshi, Ankur M.; Block, Kai Tobias; Kim, Sungheon; Otazo, Ricardo; Feng, Li; Chandarana, Hersh “High Spatiotemporal Dynamic Contrast-Enhanced MRI of the Small Bowel in Active Crohn's Terminal Ileitis Using Compressed Sensing, Parallel Imaging, and Golden-Angle Radial Sampling” (ISMRM 2014, Milan, Italy)
40. Florian Knoll, Thomas Koesters, Ricardo Otazo, Tobias Block, Li
Feng, Kathleen Vunckx, David Faul, Johan Nuyts, Fernando Boada, Daniel K Sodickson “Joint reconstruction of simultaneously acquired MR-PET data with multi sensor compressed sensing based on a joint sparsity constraint” (EJNMMI Physics, July 2014, 1:A26)
41. Thomas Koesters, Florian Buether, Li Feng, Klaus Schafers, David Faul, Fernando Boada “Comparison of PET and MR based

227
data driven gating methods for simultaneous PET/MRI” (Society of Nuclear Medicine Annual Meeting 2014)
2013
42. Prodromos Parasoglou, Li Feng, Ding Xia, Ricardo Otazo, and
Ravinder R Regatte “Three Dimensional Mapping of Oxidative Capacity in Human Lower Leg Muscles Compressed Sensing 31P-MRI” (ISMRM 2013, Salt Lake City, Utah)
43. Hersh Chandarana, Kai Tobias Block, Henry Rusinek, Matthew B Greenberg, Li Feng, Daniel K Sodickson, and Ricardo Otazo “Free-Breathing Dynamic Contrast Enhanced Compressed-Sensing Imaging for Reliable Estimation of Liver Perfusion” (ISMRM 2013, Salt Lake City, Utah)
44. Riccardo Lattanzi, Alicia W Yang, Li Feng, Michael Recht, Daniel K Sodickson, and Ricardo Otazo “Feasibility of accelerating 3 T hip imaging using compressed sensing” (ISMRM 2013, Salt Lake City, Utah)
45. Robert Grimm, Li Feng, Christoph Forman, Jana Hutter, Berthold Kiefer, Joachim Hornegger, and Tobias Block “Automatic Bolus Analysis for DCE-MRI Using Radial Golden-Angle Stack-of-stars GRE Imaging” (ISMRM 2013, Salt Lake City, Utah)
46. Kai Tobias Block, Robert Grimm, Li Feng, Ricardo Otazo, Hersh Chandarana, Mary Bruno, Christian Geppert, and Daniel K. Sodickson “Bringing Compressed Sensing to Clinical Reality: Prototypic Setup for Evaluation in Routine Applications” (ISMRM 2013, Salt Lake City, Utah)
47. Kai Tobias Block, Robert Grimm, Li Feng, Ricardo Otazo, Hersh Chandarana, Daniel Sodickson, Ricardo Otazo “Prototypic Setup for Evaluation of a Compressed-Sensing Technique in Clinical Patient Studies” (ISMRM Workshop on Data Sampling and Image Reconstruction, Sedona, Arizona, 2013)
2012 48. Jian Xu, Li Feng, Ricardo Otazo, Alicia Yang, Kai Tobias Block,
Barbara Srichai, Ruth Lim, Kelly Anne Mcgorty, Joseph Reaume,

228
Leon Axel, Yao Wang, and Daniel Sodickson “Feasibility of 5-Minute Comprehensive Cardiac MR Examination Using Highly Accelerated Parallel Imaging and Compressed Sensing” (ISMRM 2012, Melbourne, Australia)
49. Jian Xu, Li Feng, Ricardo Otazo, Barbara Srichai, Ruth Lim, Bhat Himanshu, Kelly Anne Mcgorty, Joseph Reaume, and Daniel Sodickson “Feasibility of Dynamic 4D Whole Heart Viability Imaging Within a Single Breath-Hold Using Highly Accelerated Parallel Imaging and Compressed Sensing” (ISMRM 2012, Melbourne, Australia)
50. Hersh Chandarana, Li Feng, Tobias Kai Block, Andrew B Rosenkrantz, Ruth P Lim, Dewey Chu, Daniel K Sodickson, and Ricardo Otazo “Free-breathing dynamic contrast-enhanced MRI of the liver with radial golden-angle sampling scheme and advanced compressed-sensing reconstruction” (ISMRM 2012, Melbourne, Australia)
51. Hersh Chandarana, Li Feng, Tobias Kai Block, Joseph P Stepancic, Daniel K Sodickson, and Ricardo Otazo “Contrast-enhanced free-breathing perfusion weighted MR imaging of the whole-liver with high spatial and temporal resolution” (ISMRM 2012, Melbourne, Australia)
52. Sungheon Kim, Li Feng, Linda Moy, Melanie Moccaldi, Kai T. Block, Daniel K. Sodickson, and Ricardo Otazo “Highly-Accelerated Golden-Angle Radial Acquisition with Joint Compressed Sensing and Parallel Imaging Reconstruction for Breast DCE-MRI” (ISMRM 2012, Melbourne, Australia)
53. Alicia Yang, Li Feng, Jian Xu, Ivan Selesnick, Daniel K Sodickson, and Ricardo Otazo “Improved Compressed Sensing Reconstruction with Overcomplete Wavelet Transforms” (ISMRM 2012, Melbourne, Australia)
54. Daniel Kim, Alexis Harrison, Wilson King, Li Feng, Elwin Bassett, Christopher J McGann, Nassir F Marrouche, and Ricardo Otazo “Highly-accelerated, single breath-hold 3D Cine b-SSFP MRI with a combination of compressed sensing and parallel imaging” (ISMRM 2012, Melbourne, Australia)

229
55. Ricardo Otazo, Li Feng, Hersh Chandarana, Tobias Block, Leon Axel, Daniel Sodickson. “Combination of Compressed Sensing and Parallel Imaging for Highly-Accelerated Dynamic MRI” (IEEE ISBI 2012, Barcelona, Spain)
56. Kai Tobias Block, Martin Uecker, Shuo Zhang, Li Feng, Hersh Chandarana, Ricardo Otazo. “Iterative Reconstruction Techniques for Faster Scan Speed in Magnetic Resonance Imaging” (TOPIM 2012, Les Houches)
2010
57. Kim D, Wu EX, Jensen J, Au WY, Feng L, Cheung JS, Ha SY,
Sheth SS, Brittenham GM “A breath-hold R2 mapping pulse sequence detects a decrease in myocardial ferritin iron after one-week of iron chelation” (SCMR, 2010, Phoenix, Arizona, USA)
58. Otazo R, Feng L, Lim R, Duan Q, Wiggins G, Sodickson DK, Kim D “Accelerated 3D carotid MRI using compressed sensing and parallel imaging” (SCMR, 2010, Phoenix, Arizona, USA)
2009
59. Jian Xu, Ricardo Otazo, Sven Zuehlsdorff, Daniel Kim, Xiaoming
Bi, Qi Duan, Sonia Nielles-Vallespin, Monvadi Barbara Srichai, Thoralf Niendorf, Renate Jerecic, Bernd Stoeckel, Yao Wang, Li Feng, Kellyanne Mcgorty, Daniel K. Sodickson “Feasibility of Five-Minute Comprehensive Cardiac MR Examination Using Highly Accelerated Parallel Imaging with a 32-Element Coil Array” (ISMRM, 2009, Honolulu, USA)

230
Bibliography
1. Purcell EM, Torrey HC, Pound RV. Resonance Absorption by Nuclear Magnetic Moments in a Solid. Phys Rev 1946;69(1-2):37-38.
2. Bloch F. The Principle of Nuclear Induction. Science 1953;118(3068):425-430.
3. Lauterbur PC. Image Formation by Induced Local Interactions - Examples Employing Nuclear Magnetic-Resonance. Nature 1973;242(5394):190-191.
4. Kumar A, Welti D, Ernst RR. Nmr Fourier Zeugmatography. J Magn Reson 1975;18(1):69-83.
5. Ljunggren S. A Simple Graphical Representation of Fourier-Based Imaging Methods. J Magn Reson 1983;54(2):338-343.
6. Twieg DB. The K-Trajectory Formulation of the Nmr Imaging Process with Applications in Analysis and Synthesis of Imaging Methods. Medical Physics 1983;10(5):610-621.
7. Paling MR, Brookeman JR. Respiration artifacts in MR imaging: reduction by breath holding. Journal of computer assisted tomography 1986;10(6):1080-1082.
8. Mansfield P. Multi-Planar Image-Formation Using Nmr Spin Echoes. J Phys C Solid State 1977;10(3):L55-L58.
9. Hennig J, Nauerth A, Friedburg H. RARE imaging: a fast imaging method for clinical MR. Magn Reson Med 1986;3(6):823-833.
10. Frahm J, Haase A, Matthaei D. Rapid NMR imaging of dynamic processes using the FLASH technique. Magn Reson Med 1986;3(2):321-327.
11. Hawkes RC, Patz S. Rapid Fourier imaging using steady-state free precession. Magn Reson Med 1987;4(1):9-23.
12. Ahn CB, Kim JH, Cho ZH. High-Speed Spiral-Scan Echo Planar Nmr Imaging .1. Ieee T Med Imaging 1986;5(1):2-7.
13. Meyer CH, Hu BS, Nishimura DG, Macovski A. Fast Spiral Coronary-Artery Imaging. Magnetic Resonance in Medicine 1992;28(2):202-213.
14. J; C, Est A. Reducing MR imaging time by one-sided reconstruction. Magn Reson Imaging 1987;5:526.
15. Noll DC, Nishimura DG, Macovski A. Homodyne detection in magnetic resonance imaging. IEEE Trans Med Imaging 1991;10(2):154-163.
16. Amartur S, Liang ZP, Boada F, Haacke EM. Phase-constrained data extrapolation method for reduction of truncation artifacts. J Magn Reson Imaging 1991;1(6):721-724.

231
17. Sodickson DK, Manning WJ. Simultaneous acquisition of spatial harmonics (SMASH): fast imaging with radiofrequency coil arrays. Magn Reson Med 1997;38(4):591-603.
18. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: Sensitivity encoding for fast MRI. Magn Reson Med 1999;42(5):952-962.
19. Griswold MA, Jakob PM, Heidemann RM, Nittka M, Jellus V, Wang J, Kiefer B, Haase A. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn Reson Med 2002;47(6):1202-1210.
20. Sodickson DK, McKenzie CA. A generalized approach to parallel magnetic resonance imaging. Med Phys 2001;28(8):1629-1643.
21. Kellman P, Epstein FH, McVeigh ER. Adaptive sensitivity encoding incorporating temporal filtering (TSENSE). Magn Reson Med 2001;45(5):846-852.
22. Breuer FA, Kellman P, Griswold MA, Jakob PM. Dynamic autocalibrated parallel imaging using temporal GRAPPA (TGRAPPA). Magn Reson Med 2005;53(4):981-985.
23. Tsao J, Boesiger P, Pruessmann KP. k-t BLAST and k-t SENSE: dynamic MRI with high frame rate exploiting spatiotemporal correlations. Magn Reson Med 2003;50(5):1031-1042.
24. Huang F, Akao J, Vijayakumar S, Duensing GR, Limkeman M. k-t GRAPPA: a k-space implementation for dynamic MRI with high reduction factor. Magn Reson Med 2005;54(5):1172-1184.
25. Xu D, King KF, Liang ZP. Improving k-t SENSE by adaptive regularization. Magn Reson Med 2007;57(5):918-930.
26. Candes E, Romberg J, T. T. Robust uncertainty principles: Exact signal reconstruction from highly incomplete frequency information. IEEE Trans Inf Theory 2006;52:489-509.
27. Donoho D. Compressed sensing. IEEE Trans Inf Theory 2006;52:1289-1306.
28. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med 2007;58(6):1182-1195.
29. Liang D, Liu B, Wang J, Ying L. Accelerating SENSE using compressed sensing. Magn Reson Med 2009;62(6):1574-1584.
30. Otazo R, Kim D, Axel L, Sodickson DK. Combination of compressed sensing and parallel imaging for highly accelerated first-pass cardiac perfusion MRI. Magn Reson Med 2010;64(3):767-776.
31. Lustig M, Pauly JM. SPIRiT: Iterative self-consistent parallel imaging reconstruction from arbitrary k-space. Magn Reson Med 2010;64(2):457-471.
32. Macovski A. Noise in MRI. Magn Reson Med 1996;36(3):494-497.

232
33. Jackson JI, Meyer CH, Nishimura DG, Macovski A. Selection of a convolution function for Fourier inversion using gridding [computerised tomography application]. IEEE Trans Med Imaging 1991;10(3):473-478.
34. O'Sullivan JD. A fast sinc function gridding algorithm for fourier inversion in computer tomography. IEEE Trans Med Imaging 1985;4(4):200-207.
35. Rasche V, Proksa R, Sinkus R, Bornert P, Eggers H. Resampling of data between arbitrary grids using convolution interpolation. Ieee T Med Imaging 1999;18(5):385-392.
36. Schönberg SO, Dietrich O, Reiser MF. Parallel Imaging in Clinical MR Applications. Med Radiol Diagn Ima 2007:1-564.
37. Blaimer M, Breuer F, Mueller M, Heidemann RM, Griswold MA, Jakob PM. SMASH, SENSE, PILS, GRAPPA: how to choose the optimal method. Topics in magnetic resonance imaging : TMRI 2004;15(4):223-236.
38. Deshmane A, Gulani V, Griswold MA, Seiberlich N. Parallel MR imaging. J Magn Reson Imaging 2012;36(1):55-72.
39. Larkman DJ, Nunes RG. Parallel magnetic resonance imaging. Phys Med Biol 2007;52(7):R15-55.
40. Walsh DO, Gmitro AF, Marcellin MW. Adaptive reconstruction of phased array MR imagery. Magn Reson Med 2000;43(5):682-690.
41. Ohliger MA, Grant AK, Sodickson DK. Ultimate intrinsic signal-to-noise ratio for parallel MRI: electromagnetic field considerations. Magn Reson Med 2003;50(5):1018-1030.
42. Wiesinger F, Van de Moortele PF, Adriany G, De Zanche N, Ugurbil K, Pruessmann KP. Parallel imaging performance as a function of field strength--an experimental investigation using electrodynamic scaling. Magn Reson Med 2004;52(5):953-964.
43. Candes EJ, Recht B. Exact Matrix Completion via Convex Optimization. Found Comput Math 2009;9(6):717-772.
44. Otazo R, Candes E, Sodickson DK. Low-rank plus sparse matrix decomposition for accelerated dynamic MRI with separation of background and dynamic components. Magn Reson Med 2015;73(3):1125-1136.
45. Schultz CL, Alfidi RJ, Nelson AD, Kopiwoda SY, Clampitt ME. The effect of motion on two-dimensional Fourier transformation magnetic resonance images. Radiology 1984;152(1):117-121.
46. Zaitsev M, Maclaren J, Herbst M. Motion artifacts in MRI: A complex problem with many partial solutions. J Magn Reson Imaging 2015;Jan 28. doi: 10.1002/jmri.24850. [Epub ahead of print].

233
47. Wang Y, Rossman PJ, Grimm RC, Riederer SJ, Ehman RL. Navigator-echo-based real-time respiratory gating and triggering for reduction of respiration effects in three-dimensional coronary MR angiography. Radiology 1996;198(1):55-60.
48. Ehman RL, McNamara MT, Pallack M, Hricak H, Higgins CB. Magnetic resonance imaging with respiratory gating: techniques and advantages. AJR Am J Roentgenol 1984;143(6):1175-1182.
49. Uecker M, Zhang S, Voit D, Karaus A, Merboldt KD, Frahm J. Real-time MRI at a resolution of 20 ms. NMR Biomed 2010;23(8):986-994.
50. Glover GH, Pauly JM. Projection reconstruction techniques for reduction of motion effects in MRI. Magn Reson Med 1992;28(2):275-289.
51. Chandarana H, Block TK, Rosenkrantz AB, Lim RP, Kim D, Mossa DJ, Babb JS, Kiefer B, Lee VS. Free-breathing radial 3D fat-suppressed T1-weighted gradient echo sequence: a viable alternative for contrast-enhanced liver imaging in patients unable to suspend respiration. Invest Radiol 2011;46(10):648-653.
52. Liao JR, Pauly JM, Brosnan TJ, Pelc NJ. Reduction of motion artifacts in cine MRI using variable-density spiral trajectories. Magn Reson Med 1997;37(4):569-575.
53. Liu J, Spincemaille P, Codella NC, Nguyen TD, Prince MR, Wang Y. Respiratory and cardiac self-gated free-breathing cardiac CINE imaging with multiecho 3D hybrid radial SSFP acquisition. Magn Reson Med 2010;63(5):1230-1237.
54. Larson AC, White RD, Laub G, McVeigh ER, Li D, Simonetti OP. Self-gated cardiac cine MRI. Magn Reson Med 2004;51(1):93-102.
55. Bhat H, Ge L, Nielles-Vallespin S, Zuehlsdorff S, Li D. 3D radial sampling and 3D affine transform-based respiratory motion correction technique for free-breathing whole-heart coronary MRA with 100% imaging efficiency. Magn Reson Med 2011;65(5):1269-1277.
56. Likhite D AG, McGann CJ, and DiBella EV. Use of Deformable Registration for Quantification of Cardiac Perfusion in Patients with Arrhythmia Proceedings of the 21th Annual Meeting of ISMRM, Salt Lake City 2013. p 318.
57. Chen Y LG, Wright KL, Griswold MA, Seiberlich N, and Gulani V. 3D High Spatiotemporal Resolution Quantitative Liver Perfusion Imaging Using a Stack-Of-Spirals Acquisition and Through-Time Non-Cartesian GRAPPA Acceleration. Proceedings of the 21th Annual Meeting of ISMRM, Salt Lake City 2013. p 601.
58. Usman M, Atkinson D, Odille F, Kolbitsch C, Vaillant G, Schaeffter T, Batchelor PG, Prieto C. Motion corrected compressed sensing for

234
free-breathing dynamic cardiac MRI. Magn Reson Med 2013;70(2):504-516.
59. Otazo R, Koesters T, Candès E, DK S. Motion-guided low-rank plus sparse (L+S) reconstruction for free-breathing dynamic MRI. Proceedings of the 22th Annual Meeting of ISMRM, Milan, Italy, 2014. p742.
60. Feng L, Otazo R, Jung H, Jensen JH, Ye JC, Sodickson DK, Kim D. Accelerated cardiac T2 mapping using breath-hold multiecho fast spin-echo pulse sequence with k-t FOCUSS. Magn Reson Med 2011;65(6):1661-1669.
61. Ito K, Mitchell DG, Outwater EK, Szklaruk J, Sadek AG. Hepatic lesions: discrimination of nonsolid, benign lesions from solid, malignant lesions with heavily T2-weighted fast spin-echo MR imaging. Radiology 1997;204(3):729-737.
62. Li W, Nissenbaum MA, Stehling MK, Goldmann A, Edelman RR. Differentiation between hemangiomas and cysts of the liver with nonenhanced MR imaging: efficacy of T2 values at 1.5 T. J Magn Reson Imaging 1993;3(5):800-802.
63. McFarland EG, Mayo-Smith WW, Saini S, Hahn PF, Goldberg MA, Lee MJ. Hepatic hemangiomas and malignant tumors: improved differentiation with heavily T2-weighted conventional spin-echo MR imaging. Radiology 1994;193(1):43-47.
64. Ohtomo K, Itai Y, Yoshikawa K, Kokubo T, Iio M. Hepatocellular carcinoma and cavernous hemangioma: differentiation with MR imaging. Efficacy of T2 values at 0.35 and 1.5 T. Radiology 1988;168(3):621-623.
65. Higgins CB, Herfkens R, Lipton MJ, Sievers R, Sheldon P, Kaufman L, Crooks LE. Nuclear magnetic resonance imaging of acute myocardial infarction in dogs: alterations in magnetic relaxation times. The American journal of cardiology 1983;52(1):184-188.
66. Sekiguchi M, Yu ZX, Hasumi M, Hiroe M, Morimoto S, Nishikawa T. Histopathologic and ultrastructural observations of acute and convalescent myocarditis: a serial endomyocardial biopsy study. Heart and vessels Supplement 1985;1:143-153.
67. Sen-Chowdhry S, Prasad SK, McKenna WJ. Arrhythmogenic right ventricular cardiomyopathy with fibrofatty atrophy, myocardial oedema, and aneurysmal dilation. Heart 2005;91(6):784.
68. Willerson JT, Scales F, Mukherjee A, Platt M, Templeton GH, Fink GS, Buja LM. Abnormal myocardial fluid retention as an early manifestation of ischemic injury. The American journal of pathology 1977;87(1):159-188.

235
69. Carr HY, Purcell EM. Effects of Diffusion on Free Precession in Nuclear Magnetic Resonance Experiments. Phys Rev 1954;94(3):630-638.
70. Meiboom S, Gill D. Modified Spin-Echo Method for Measuring Nuclear Relaxation Times. Rev Sci Instrum 1958;29(8):688-691.
71. Kim D, Jensen JH, Wu EX, Sheth SS, Brittenham GM. Breathhold multiecho fast spin-echo pulse sequence for accurate R2 measurement in the heart and liver. Magn Reson Med 2009;62(2):300-306.
72. Lustig M, Santos J, Donoho D, Pauly J. k-t SPARSE: high frame rate dynamic MRI exploiting spatio-temporal sparsity. Proceedings of the 14th Annual Meeting of ISMRM, Seattle 2006. p 2420.
73. Jung H, Sung K, Nayak KS, Kim EY, Ye JC. k-t FOCUSS: a general compressed sensing framework for high resolution dynamic MRI. Magn Reson Med 2009;61(1):103-116.
74. Jung H, Ye JC, Kim EY. Improved k-t BLAST and k-t SENSE using FOCUSS. Phys Med Biol 2007;52(11):3201-3226.
75. McGibney G, Smith MR. An unbiased signal-to-noise ratio measure for magnetic resonance images. Med Phys 1993;20(4):1077-1078.
76. Lattanzi R, AW; Y, L; F, Recht M, DK; S, R O. Feasibility of Accelerating 3 T Hip Imaging Using Compressed Sensing. Proceedings of the 21th Annual Meeting of ISMRM, Salt Lake City 2013. p 3484.
77. Feng L, Otazo R, Srichai M, Lim P, Sodickson DK, Kim D. Highly-Accelerated Real-Time Cine MRI using Compressed Sensing and Parallel Imaging with Cardiac Motion Constrained Reconstruction. Proceedings of the 14th Annual Meeting of ISMRM, Montreal 2011. p 748.
78. Atkinson DJ, Edelman RR. Cineangiography of the heart in a single breath hold with a segmented turboFLASH sequence. Radiology 1991;178(2):357-360.
79. Barkhausen J, Goyen M, Ruhm SG, Eggebrecht H, Debatin JF, Ladd ME. Assessment of ventricular function with single breath-hold real-time steady-state free precession cine MR imaging. AJR Am J Roentgenol 2002;178(3):731-735.
80. Bellenger NG, Grothues F, Smith GC, Pennell DJ. Quantification of right and left ventricular function by cardiovascular magnetic resonance. Herz 2000;25(4):392-399.
81. Epstein FH, Wolff SD, Arai AE. Segmented k-space fast cardiac imaging using an echo-train readout. Magn Reson Med 1999;41(3):609-613.

236
82. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med 1990;322(22):1561-1566.
83. Sakuma H, Fujita N, Foo TK, Caputo GR, Nelson SJ, Hartiala J, Shimakawa A, Higgins CB. Evaluation of left ventricular volume and mass with breath-hold cine MR imaging. Radiology 1993;188(2):377-380.
84. Schulen V, Schick F, Loichat J, Helber U, Huppert PE, Laub G, Claussen CD. Evaluation of K-space segmented cine sequences for fast functional cardiac imaging. Invest Radiol 1996;31(8):512-522.
85. White HD, Norris RM, Brown MA, Brandt PW, Whitlock RM, Wild CJ. Left ventricular end-systolic volume as the major determinant of survival after recovery from myocardial infarction. Circulation 1987;76(1):44-51.
86. Carr JC, Simonetti O, Bundy J, Li D, Pereles S, Finn JP. Cine MR angiography of the heart with segmented true fast imaging with steady-state precession. Radiology 2001;219(3):828-834.
87. Beer M, Stamm H, Machann W, Weng A, Goltz JP, Breunig F, Weidemann F, Hahn D, Kostler H. Free breathing cardiac real-time cine MR without ECG triggering. Int J Cardiol 2010;145(2):380-382.
88. Hansen MS, Sorensen TS, Arai AE, Kellman P. Retrospective reconstruction of high temporal resolution cine images from real-time MRI using iterative motion correction. Magn Reson Med 2012;68(3):741-750.
89. Hori Y, Yamada N, Higashi M, Hirai N, Nakatani S. Rapid evaluation of right and left ventricular function and mass using real-time true-FISP cine MR imaging without breath-hold: comparison with segmented true-FISP cine MR imaging with breath-hold. J Cardiovasc Magn Reson 2003;5(3):439-450.
90. Kaji S, Yang PC, Kerr AB, Tang WH, Meyer CH, Macovski A, Pauly JM, Nishimura DG, Hu BS. Rapid evaluation of left ventricular volume and mass without breath-holding using real-time interactive cardiac magnetic resonance imaging system. J Am Coll Cardiol 2001;38(2):527-533.
91. Kellman P, Chefd'hotel C, Lorenz CH, Mancini C, Arai AE, McVeigh ER. Fully automatic, retrospective enhancement of real-time acquired cardiac cine MR images using image-based navigators and respiratory motion-corrected averaging. Magn Reson Med 2008;59(4):771-778.
92. Kellman P, Chefd'hotel C, Lorenz CH, Mancini C, Arai AE, McVeigh ER. High spatial and temporal resolution cardiac cine MRI from

237
retrospective reconstruction of data acquired in real time using motion correction and resorting. Magn Reson Med 2009;62(6):1557-1564.
93. Kerr AB, Pauly JM, Hu BS, Li KC, Hardy CJ, Meyer CH, Macovski A, Nishimura DG. Real-time interactive MRI on a conventional scanner. Magn Reson Med 1997;38(3):355-367.
94. Nagel E, Schneider U, Schalla S, Ibrahim T, Schnackenburg B, Bornstedt A, Klein C, Lehmkuhl HB, Fleck E. Magnetic resonance real-time imaging for the evaluation of left ventricular function. J Cardiovasc Magn Reson 2000;2(1):7-14.
95. Plein S, Smith WH, Ridgway JP, Kassner A, Beacock DJ, Bloomer TN, Sivananthan MU. Qualitative and quantitative analysis of regional left ventricular wall dynamics using real-time magnetic resonance imaging: comparison with conventional breath-hold gradient echo acquisition in volunteers and patients. J Magn Reson Imaging 2001;14(1):23-30.
96. Setser RM, Fischer SE, Lorenz CH. Quantification of left ventricular function with magnetic resonance images acquired in real time. J Magn Reson Imaging 2000;12(3):430-438.
97. Yang PC, Kerr AB, Liu AC, Liang DH, Hardy C, Meyer CH, Macovski A, Pauly JM, Hu BS. New real-time interactive cardiac magnetic resonance imaging system complements echocardiography. J Am Coll Cardiol 1998;32(7):2049-2056.
98. Ding Y, Chung YC, Jekic M, Simonetti OP. A new approach to autocalibrated dynamic parallel imaging based on the Karhunen-Loeve transform: KL-TSENSE and KL-TGRAPPA. Magn Reson Med 2011;65(6):1786-1792.
99. Xue H, Ding Y, Guetter C, Jolly MP, Guehring J, Zuehlsdorff S, Simonetti OP. Motion compensated magnetic resonance reconstruction using inverse-consistent deformable registration: application to real-time cine imaging. Med Image Comput Comput Assist Interv 2011;14(Pt 1):564-572.
100. Liang Z-P. Spatiotemporal imaging with partially separable functions. 2007. in Proc. IEEE Int. Symp. Biomed. Imaging. p 988-991.
101. Brinegar C, Wu YJ, Foley LM, Hitchens T, Ye Q, Ho C, ZP L. Real-time cardiac MRI without triggering, gating, or breath holding. 2008; Conf Proc IEEE Eng Med Biol Soc. p 3381-3384.
102. Muthurangu V, Lurz P, Critchely JD, Deanfield JE, Taylor AM, Hansen MS. Real-time assessment of right and left ventricular volumes and function in patients with congenital heart disease by using high spatiotemporal resolution radial k-t SENSE. Radiology 2008;248(3):782-791.

238
103. Jung H, Park J, Yoo J, Ye JC. Radial k-t FOCUSS for high-resolution cardiac cine MRI. Magn Reson Med 2010;63(1):68-78.
104. Jung B, Ullmann P, Honal M, Bauer S, Hennig J, Markl M. Parallel MRI with extended and averaged GRAPPA kernels (PEAK-GRAPPA): optimized spatiotemporal dynamic imaging. J Magn Reson Imaging 2008;28(5):1226-1232.
105. Kim D, Dyvorne HA, Otazo R, Feng L, Sodickson DK, Lee VS. Accelerated phase-contrast cine MRI using k-t SPARSE-SENSE. Magn Reson Med 2012;67(4):1054-1064.
106. Parasoglou P, Feng L, Xia D, Otazo R, Regatte RR. Rapid 3D-imaging of phosphocreatine recovery kinetics in the human lower leg muscles with compressed sensing. Magn Reson Med 2012;68(6):1738-1746.
107. Feng L, Grimm R, Block KT, Chandarana H, Kim S, Xu J, Axel L, Sodickson DK, Otazo R. Golden-angle radial sparse parallel MRI: Combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med 2014;72(3):707-717.
108. Chandarana H, Feng L, Block KT, Rosenkrantz AB, Lim P, Babb J, Sodickson DK, Otazo R. Free-Breathing Contrast-Enhanced Multiphase MRI of the Liver Using a Combination of Compressed Sensing, Parallel Imaging, and Golden-Angle Radial Sampling. Investigative Radiology: 2013;48(1):10-16.
109. Rosenkrantz AB, Geppert C, Grimm R, Block TK, Glielmi C, Feng L, Otazo R, Ream JM, Romolo MM, Taneja SS, Sodickson DK, Chandarana H. Dynamic contrast-enhanced MRI of the prostate with high spatiotemporal resolution using compressed sensing, parallel imaging, and continuous golden-angle radial sampling: Preliminary experience. J Magn Reson Imaging 2015;41(5):1365-1373.
110. Padhani AR. Dynamic contrast-enhanced MRI in clinical oncology: current status and future directions. J Magn Reson Imaging 2002;16(4):407-422.
111. Xu B, Spincemaille P, Chen G, Agrawal M, Nguyen TD, Prince MR, Wang Y. Fast 3D contrast enhanced MRI of the liver using temporal resolution acceleration with constrained evolution reconstruction. Magn Reson Med 2013;69(2):370-381.
112. Gai N, Axel L. Correction of motion artifacts in linogram and projection reconstruction MRI using geometry and consistency constraints. Med Phys 1996;23(2):251-262.
113. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An optimal radial profile order based on the Golden Ratio for time-resolved MRI. IEEE Trans Med Imaging 2007;26(1):68-76.

239
114. Buehrer M, Pruessmann KP, Boesiger P, Kozerke S. Array compression for MRI with large coil arrays. Magn Reson Med 2007;57(6):1131-1139.
115. Dagum L, OpenMP RM. An industry standard API for shared-memory programming. IEEE Computational Science and Engineering 1998;5(1):46-55.
116. Block KT, Uecker M. Simple Method for Adaptive Gradient-Delay Compensation in Radial MRI. Proceedings of the 19th Annual Meeting of ISMRM, Montreal 2011;p2816.
117. Feng L, Xu J, Axel L, Sodickson DK, Otazo R. High spatial and Temporal Resolution 2D Real Time and 3D Whole-Heart Cardiac Cine MRI Using Compressed Sensing and Parallel Imaging with Golden Angle Radial Trajectory. Proceedings of the 20th Annual Meeting of ISMRM, Melbourne, Australia, 2012. p 225.
118. Adluru G, Awate SP, Tasdizen T, Whitaker RT, Dibella EV. Temporally constrained reconstruction of dynamic cardiac perfusion MRI. Magn Reson Med 2007;57(6):1027-1036.
119. Adluru G, McGann C, Speier P, Kholmovski EG, Shaaban A, Dibella EV. Acquisition and reconstruction of undersampled radial data for myocardial perfusion magnetic resonance imaging. J Magn Reson Imaging 2009;29(2):466-473.
120. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med 2015;Mar 25. doi: 10.1002/mrm.25665. [Epub ahead of print].
121. Axel L, Summers RM, Kressel HY, Charles C. Respiratory effects in two-dimensional Fourier transform MR imaging. Radiology 1986;160(3):795-801.
122. Uecker M, Zhang S, Frahm J. Nonlinear inverse reconstruction for real-time MRI of the human heart using undersampled radial FLASH. Magn Reson Med 2010;63(6):1456-1462.
123. Zhao B, Haldar JP, Liang ZP. PSF model-based reconstruction with sparsity constraint: algorithm and application to real-time cardiac MRI. Conference proceedings : Annual International Conference of the IEEE Engineering in Medicine and Biology Society IEEE Engineering in Medicine and Biology Society Annual Conference 2010:3390-3393.
124. Lauzon ML, Rutt BK. Effects of polar sampling in k-space. Magn Reson Med 1996;36(6):940-949.
125. Lauzon ML, Rutt BK. Polar sampling in k-space: reconstruction effects. Magn Reson Med 1998;40(5):769-782.

240
126. Gamper U, Boesiger P, Kozerke S. Compressed sensing in dynamic MRI. Magn Reson Med 2008;59(2):365-373.
127. Otazo R KD, Axel L, and Sodickson DK. Combination of Compressed Sensing and Parallel Imaging with Respiratory Motion Correction for Highly-Accelerated First-Pass Cardiac Perfusion MRI. Proceedings of the 19th Annual Meeting of ISMRM, Montreal, Canada 2011. p 66.
128. Ream J, Doshi AM, Block KT, Kim S, Otazo R, Feng L, H C. High Spatiotemporal Dynamic Contrast-Enhanced MRI of the Small Bowel in Active Crohn's Terminal Ileitis Using Compressed Sensing, Parallel Imaging, and Golden-Angle Radial Sampling. Proceedings of the 22th Annual Meeting of ISMRM, Milan, Italy, 2014. p 2122.
129. Liu J, Spincemaille P, Codella NC, Nguyen TD, Prince MR, Wang Y. Respiratory and cardiac self-gated free-breathing cardiac CINE imaging with multiecho 3D hybrid radial SSFP acquisition. Magn Reson Med;63(5):1230-1237.
130. Pang J, Sharif B, Fan Z, Bi X, Arsanjani R, Berman DS, Li D. ECG and navigator-free four-dimensional whole-heart coronary MRA for simultaneous visualization of cardiac anatomy and function. Magn Reson Med 2014;72(5):1208-1217.
131. Feng L, Axel L, Latson L, Xu J, Sodickson DK, R O. Compressed sensing with synchronized cardio-respiratory sparsity for free-breathing cine MRI: initial comparative study on patients with arrhythmias. 2014/1/16. p O17.
132. Feng L, Liu J, Block K, Xu J, Axel L, Sodickson DK, Otazo R. Compressed Sensing Reconstruction with an Additional Respiratory-Phase Dimension for Free-Breathing Imaging. 2013. Proceedings of the 21th Annual Meeting of ISMRM, Salt Lake City 2013. p 606.
133. Grimm R, KT B, J H, C F, C H, B K, J H. Self-Gating Reconstructions of Motion & Perfusion for Free-Breathing T1-Weighted DCE-MRI of the Thorax Using 3D Stack-Of-Stars GRE Imaging. Proceedings of the 20th Annual Meeting of ISMRM, Melbourne, Australia, 2012. p 598.
134. Spincemaille P, Liu J, Nguyen T, Prince MR, Wang Y. Z intensity-weighted position self-respiratory gating method for free-breathing 3D cardiac CINE imaging. Magnetic resonance imaging 2011;29(6):861-868.
135. Fessler J, A, Sutton B, P. Nonuniform Fast Fourier Transforms Using Min-Max Interpolation. IEEE Transactions on Signal Processing, 2003;51(2):560-574.

241
136. Adluru G, Dibella EV. Reordering for improved constrained reconstruction from undersampled k-space data. Int J Biomed Imaging 2008:Article ID 341684.
137. McConnell MV, Wu HH. Respiratory-mode display of echocardiographic images highlights effects of pericardial disease. JACC Cardiovascular imaging 2013;6(8):917-919.
138. Cheng JY ZT, Alley MT, Lustig M, Vasanawala SS, Pauly JM. Variable-density radial view-ordering and sampling for time-optimized 3D Cartesian imaging. Proceedings of the ISMRM Workshop on Data Sampling and Image Reconstruction, Sedona, Arizona, USA, 2013.
139. Cheng JY ZT, Pauly JM, Vasanawala SS, Lustig M. Free Breathing Dynamic Contrast Enhanced 3D MRI with Resolved Respiratory Motion Proceedings of the 22th Annual Meeting of ISMRM, Milan, Italy, 2014. p 330.
140. Zhang T CJ, Alley MT, Uecker M, Lustig M, Pauly JM, and Vasanawala SS. Fast 3D Free-breathing Abdominal Dynamic Contrast Enhanced MRI with High Spatiotemporal Resolution. Proceedings of the 22th Annual Meeting of ISMRM, Milan, Italy, 2014. p 332.
141. Piccini D, Littmann A, Nielles-Vallespin S, Zenge MO. Spiral phyllotaxis: the natural way to construct a 3D radial trajectory in MRI. Magn Reson Med;66(4):1049-1056.
142. Feng L, Coppo S, Piccini D, Lim P, Stuber M, Sodickson DK, Otazo R. Five-Dimensional Cardiac and Respiratory Motion-Resolved Whole-Heart MRI. In: Proceedings of the 23rd Annual Meeting of ISMRM, Toronto, Canada, 2015. p27.
143. Piccini D, Littmann A, Nielles-Vallespin S, Zenge MO. Respiratory self-navigation for whole-heart bright-blood coronary MRI: methods for robust isolation and automatic segmentation of the blood pool. Magn Reson Med 2012;68(2):571-579.
144. Lai P, Huang F, Larson AC, Li D. Fast four-dimensional coronary MR angiography with k-t GRAPPA. J Magn Reson Imaging 2008;27(3):659-665.
145. Lai P, Larson AC, Park J, Carr JC, Li D. Respiratory self-gated four-dimensional coronary MR angiography: a feasibility study. Magn Reson Med 2008;59(6):1378-1385.
146. Wu HH, Gurney PT, Hu BS, Nishimura DG, McConnell MV. Free-breathing multiphase whole-heart coronary MR angiography using image-based navigators and three-dimensional cones imaging. Magn Reson Med 2013;69(4):1083-1093.

242
147. Coppo S, Piccini D, Bonanno G, Chaptinel J, Vincenti G, Feliciano H, van Heeswijk RB, Schwitter J, Stuber M. Free-running 4D whole-heart self-navigated golden angle MRI: Initial results. Magn Reson Med 2014;Nov 5. doi: 10.1002/mrm.25523. [Epub ahead of print].
148. Bonanno B, Piccini D, Maréchal B, Zenge MO, Stuber M. A New Binning Approach for 3D Motion Corrected Self-Navigated Whole-Heart Coronary MRA Using Independent Component Analysis of Individual Coils. Proceedings of the 22th Annual Meeting of ISMRM, Milan, Italy, 2014. p 936.
149. Hyvarinen A. Fast and robust fixed-point algorithms for independent component analysis. IEEE Trans Neural Netw 1999;10(3):626-634.
150. Knoll F, Schwarzl A, Diwoky C, Sodickson DK. gpuNUFFT - An Open Source GPU Library for 3D Regridding with Direct Matlab Interface. Proceedings of the 22nd Annual Meeting of ISMRM, Milan, Italy, 2014. p 4297.
151. Akcakaya M, Basha TA, Chan RH, Manning WJ, Nezafat R. Accelerated isotropic sub-millimeter whole-heart coronary MRI: Compressed sensing versus parallel imaging. Magn Reson Med 2014;71(2):815-822.
152. Akcakaya M, Basha TA, Chan RH, Rayatzadeh H, Kissinger KV, Goddu B, Goepfert LA, Manning WJ, Nezafat R. Accelerated contrast-enhanced whole-heart coronary MRI using low-dimensional-structure self-learning and thresholding. Magn Reson Med 2012;67(5):1434-1443.
153. Moghari MH, Akcakaya M, O'Connor A, Basha TA, Casanova M, Stanton D, Goepfert L, Kissinger KV, Goddu B, Chuang ML, Tarokh V, Manning WJ, Nezafat R. Compressed-sensing motion compensation (CosMo): a joint prospective-retrospective respiratory navigator for coronary MRI. Magn Reson Med 2011;66(6):1674-1681.
154. Nam S, Akcakaya M, Basha T, Stehning C, Manning WJ, Tarokh V, Nezafat R. Compressed sensing reconstruction for whole-heart imaging with 3D radial trajectories: a graphics processing unit implementation. Magn Reson Med 2013;69(1):91-102.
155. Pang J, Sharif B, Fan Z, Bi X, Arsanjani R, Berman DS, Li D. ECG and navigator-free four-dimensional whole-heart coronary MRA for simultaneous visualization of cardiac anatomy and function. Magn Reson Med 2014;Epub; DOI 10.1002/mrm.25450.
156. Ma D, Gulani V, Seiberlich N, Liu K, Sunshine JL, Duerk JL, Griswold MA. Magnetic resonance fingerprinting. Nature 2013;495(7440):187-192.

243
157. Knoll F, Koesters T, Otazo R, Block KT, Feng L, Vunckx K, Faul D, Nuyts J, Boada F, Sodickson DK. Simultaneous MR-PET Reconstruction Using Multi Sensor Compressed Sensing and Joint Sparsity. Proceedings of the 22nd Annual Meeting of ISMRM, Milan, Italy, 2014. p 82.
158. Koesters T, Feng L, Block KT, Fieseler M, Schäfers KP, Faul D, Sodickson DK, Boada F. Motion-Compensated EM PET Reconstruction for Simultaneous PET/MR Exams. Proceedings of the 22th Annual Meeting of ISMRM, Milan, Italy, 2014. p 789.