Embed Size (px)
Citation preview

Rarity of PIT1 Involvement in Children FromRussia With Combined PituitaryHormone Deficiency
Olga V. Fofanova,1,2 Noboru Takamura,4 Ei-ichi Kinoshita,5 Masaaki Yoshimoto,5 Yoshiro Tsuji,5Valentina A. Peterkova,1,2 Oleg V. Evgrafov,3 Ivan I. Dedov,2 Nikolai P. Goncharov,2 andShunichi Yamashita4,6*1Department of Pediatrics, Research Center for Medical Genetics, Moscow, Russia2Endocrinology Research Center, Research Center for Medical Genetics, Moscow, Russia3DNA-Diagnostics Laboratory, Research Center for Medical Genetics, Moscow, Russia4Department of International Health and Radiation Research, Nagasaki University School of Medicine,Nagasaki, Japan
5Department of Pediatrics, Nagasaki University School of Medicine, Nagasaki, Japan6Department of Nature Medicine, Nagasaki University School of Medicine, Nagasaki, Japan
To ascertain the molecular background ofcombined pituitary hormone deficiency,screening for mutations in the pituitary-specific transcription factor (Pit-1/GHF-1)gene (PIT1) was performed on a cohort of 15children from Russia with combined growthhormone (GH)/prolactin (Prl)/thyroid-stimulating hormone (TSH) deficiency. Thegroup of patients, suspected of PIT1 muta-tions, consisted of four familial cases (sevenpatients) and eight sporadic cases. All hadcomplete GH deficiency and complete orpartial Prl and TSH deficiency. Direct se-quencing of all six exons of PIT1 and its pro-moter region showed a C to T transition mu-tation at codon 14 of exon 1 in a 3 8/12-year-old girl. This novel PIT1 mutation results ina proline to leucine substitution (P14L). Thepatient was heterozygous for mutant andnormal alleles. The heterozygous P14L mu-tation was also present in her mother aswell as in her maternal aunt and grand-mother, all of whom were phenotypicallynormal. There was no mutation in the fa-ther’s DNA, suggesting the need for re-evaluation of genomic imprinting. In otherchildren of our series, no mutation in PIT1or in its promotor region was identified.
This is the first report on the analysis ofPIT1 and its promoter region in Russianchildren with GH/Prl/TSH deficiency. How-ever, as the involvement of PIT1 mutation israre in Russia, the other negative casesneed to be analyzed for another candidategene responsible for combined GH/Prl/TSHdeficiency. Am. J. Med. Genet. 77:360–365,1998. © 1998 Wiley-Liss, Inc.
KEY WORDS: mutation; Pit-1; GHF-1; com-bined pituitary hormone de-ficiency; genomic imprinting
INTRODUCTION
The first molecular searches for Pit-1 gene (PIT1)abnormalities were performed in 1990 on three modelsof hypopituitary mice. These dwarf strains are charac-terized by complete lack [Snell (dw), Jackson (dw8)], orincomplete lack [Ames (df)] of growth hormone (GH),prolactin (Prl), and thyroid-stimulating hormone(TSH)–producing cells and their corresponding hor-mones, and pituitary hypoplasia. Mutations in theSnell (W261C) and in the Jackson (Pit1 rearrange-ments) are located on mouse chromosome 16, and thatin the Ames on mouse chromosome 11 [Ingraham et al.,1990; Li et al., 1990; Pfaffle et al., 1992]. The humanPit-1 gene (PIT1) encodes the Pit-1 protein, consistingof 291 amino acids and belonging to the POU-family oftranscription factors. PIT1 consists of three functionaldomains; i.e., the transcriptional activation, POU-specific (POU-S), and POU-homeo (POU-H) domains.Both POU-S and POU-H are DNA-binding domains.Pit-1 is known to be the main stimulator of GH gene
Contract grant sponsor: Ministry of Education, Culture andScience of Japan; Contract grant number: 06042009.
*Correspondence to: Professor Shunichi Yamashita, M.D.,D.N.M., D.I.H.R.R., Atomic Bomb Disease Institute, NagasakiUniversity School of Medicine, 1-12-4 Sakamoto, Nagasaki 852-8523, Japan.
Received 14 August 1997; Accepted 16 March 1998
American Journal of Medical Genetics 77:360–365 (1998)
© 1998 Wiley-Liss, Inc.

transcription. It is also involved in the activatingexpression of Prl and TSH-b genes, by means of bind-ing to cell-specific cis-acting elements of these genes[Herr et al., 1988; Ingraham et al., 1990; Rosenfeld,1991; Ruvkin and Finney, 1991; Tuggle and Trenkle,1996]. Transcription factor, GATA-2, which is presentin thyrotrophs, is also believed to cooperate with Pit-1to activate the mouse TSH-b gene promoter [Diamondand Gutierrez-Hartmann, 1996]. Experimental studieson animal models found PIT1 expression in somato-trophs, lactotrophs, and thyrotrophs early in ontogeny,and showed that it is necessary for the differentiation,proliferation, survival, and specialized function ofthese types of adenopituitary cells during the embry-onic period [Ingraham et al., 1990; Li et al., 1990;Rosenfeld, 1991; Tuggle and Trenkle, 1996]. In addi-tion, Prl itself is demonstrated to be an activator of thePIT1 transcription in somatotrophs and lactotrophs,being mediated by the pituitary STAT-like factor [De-vost et al., 1996]. Recent data also pointed to the spe-cific interactions between Pit-1 and nucleic receptors,such as thyroid hormone, retinoic acid, and estrogenreceptors [Sanno et al., 1996; Tuggle and Trenkle,1996].
Children with combined GH/Prl/TSH deficiencyhave appeared since 1976 [Rogol and Kahn, 1976;Yoshimoto et al., 1988; Miyai et al., 1988; Wit et al.,1989]. Tatsumi et al. [1992] found a nonsense muta-tion, R172X, in PIT1 in a Japanese girl with combinedGH/Prl/TSH deficiency. Since then, different typesof molecular defects in PIT1 have been identified;i.e., whole gene deletion, eliminating binding tothe promoter region, and loss or inhibition of activa-tion [Ohta et al., 1992; Pfaffle et al., 1992; Radovick etal., 1992; Brown et al., 1996; Pernasetti et al., 1996].This work deals with a PIT1 mutation analysis amongRussian children with combined GH/Prl/TSH defi-ciency.
CLINICAL STUDY AND HORMONAL ANALYSIS
Fifteen Russian dwarf children (4 boys and 11 girls)with complete GH and complete or partial Prl/TSH de-ficiency were investigated. Of these 15, 4 were familialcases consisting of 7 patients (patients 1, 5, 6, 9, 10, 11,and 12) (Fig. 1) and 8 sporadic cases. The ethnic originof 14 patients is Russian, while patient 1 is a Chuvash,patient 3 is an Azerbaijani, patient 8 is a Tadjik-Russian, and patient 15 is a Tatar. Four patients live inMoscow, three in the Moscow region, two in the Volgaregion, two in the Ural region, two in Siberia, and onein the Caucasus. Diagnostic criteria were as follows: 1)severe growth retardation with −4 standard deviationscore (SD) or less from the mean of height for chrono-logical age (CA) and sex, 2) early onset of growth re-tardation (before age one year), 3) retarded bone age(BA) with a BA/CA ratio of 0.9 or less, 4) complete GHdeficiency with a peak GH level of 2 ng/ml or less in twoGH stimulation tests, 5) clinical symptoms of hypothy-roidism, 6) low basal serum levels of Prl, 7) low (orcloser to lower normal limits) basal serum levels ofTSH (free T4), 8) lack of response (or closer to lowernormal limits of response) of Prl and TSH to a TRHstimulation test, 9) normal basal serum levels of corti-sol; and 10) good response to recombinant GH treat-ment.
The patients were evaluated clinically and diagnostictests were performed in the Department of Pediatrics,Endocrinology Research Center, Moscow. Clinical dataon the 15 children are summarized in Table I. Deliveryconditions of the children were all normal except forfour patients with asphyxia (patients 1, 2, 5, and 8).Their CA ranged from 1.58 to 17.7 years (10.4–4.5years), BA from 0.8 to 11 years (5.1–3.2 years), and theBA/CA ratio from 0.30 to 0.79 (0.45–0.15). Most (13)children had a height of −4 SD or less, ranging from−8.72 to −4.43 SD, while SD in 2 patients was −3.67(patient 6) and −1.47 (patient 9), both having had
Fig 1. Four Russian families with con-genital combined pituitary hormone defi-ciency.
PIT1 Mutation Analysis in Russian Dwarf Children 361

affected sibs with −5.42 SD (patient 5) and −4.44 SD(patient 10).
At first examination, 12 patients had already re-ceived treatment with recombinant (or extracted) GH.Results of the TRH test on Prl and TSH secretion aresummarized in Table II. All patients had complete orincomplete Prl/TSH deficiency and complete GH defi-ciency. At the first examination, 12 of the 15 patientshad clinical symptoms of hypothyroidism and weretreated with L-thyroxine (Table III). In the patients ofpubertal age, bone age maturation was significantlydelayed, and they have not reached puberty.
PIT1 MUTATION ANALYSIS
Genomic DNA was extracted from peripheral bloodleukocytes of patients and their parents and relativesusing the standard method. DNA fragments coveringall six PIT1 exons, their respective exon-intron bound-aries, and the PIT1 promoter region were amplifiedwith polymerase chain reaction (PCR) using a ThermalCycler 2400TM (Perkin Elmer, ). Sets of primers were
as follows: Forward 1 (for exon 1), ATCGGCCCTTT-GA(G/T)ACAGTAA; Reverse 1, CCCGTCATATG-TAAACTG; Forward 2 (exon 2), TTTCTCGGTGACA-ACGTTG; Reverse 2, GTGTCCCCAAATTCAATA-AC; Forward 3 (exon 3), AAGGAGAATGACAAATG-GTC; Reverse 3, AAGTTCTTTTTCCTGTTGCC; For-ward 4 (exon 4), AAAGTTGGAGCTGATGGTC; Re-verse 4, CACAGCCTTCAGAGACAC; Forward 5 (exon5), TTTGTAATTATCTCTCTTTTCC; Reverse 5,TACACTCAAATGCTCATTCC; Forward 6 (exon 6),AATTTCACCCCCTATGTCC; Reverse 6, GAAACGG-GAGAAAAAGGCT; Forward 7 (for promotor region),CATTTGCAATTGTGTTAGTAGC; Reverse 7 (promo-tor region), CATTCCCACAAGAGAGT. PCR amplifica-tion was performed for 35 cycles at 94°C for 30 sec(denaturation), 58°C (for exons 1–3, 4, 6, and the pro-moter region) or 55°C (for exon 5) for one min (anneal-ing), and 72°C for 30 sec (extension), with an initialdenaturation step at 95°C for 5 min and final annealingstep at 72°C for 5 min (4°C storage). PCR productswere purified with an QIAEX II Gel Extraction kit(QIAGEN, ) and SUPREC-02 columns (Takara Shuzo,
TABLE I. Manifestations in Russian Children With Congenital Combined Pituitary Hormone Deficiency
PatientSex(m/f)
CA(yrs)
HeightSD
Height(cm)
Weight(kg)
Bodymassindex
BA(yrs)
BA:CAratio
Height velocitybefore treatment
(cm/yr)
Height velocity afterGH treatment
(cm/yr)
1a f 3.87 −6.50 72.1 7.6 14.6 1.0 0.39 4.0 13.7 (Genotropin)2 f 6.60 −4.88 92.1 11.5 13.5 2.0 0.30 3.0 —3 f 1.58 −5.63 64.3 5.0 12.2 0.8 0.50 — —4 f 12.78 −7.08 104.6 17.0 17.7 6.0 0.47 1.0 9.2 (Somatogen)5a m 11.48 −5.42 107.1 17.0 14.7 5.0 0.44 1.0 15.8 (Norditropin)6a f 17.47 −3.67 140.2 44.0 22.4 11.0 0.63 1.0 12.9 (Norditropin)7 f 14.50 −8.72 107 20.0 17.5 5.0 0.34 2.0 —8 f 10.39 −4.5 109.6 18.4 15.3 3.5 0.34 2.0 —9a m 8.80 −1.47 121.8 33.8 22.8 7.0 0.79 1.0 12.0 (Somatotropin)
10a f 11.60 −4.44 113.5 21.6 16.7 6.5 0.56 1.0 12.0 (Somatotropin)11a m 9.93 −5.78 100.4 16.3 16.3 3.5 0.35 — 19.8 (Norditropin)12a f 13.2 −6.97 109.2 19.0 15.9 8.5 0.64 — 18.3 (Norditropin)13 m 7.62 −6.19 89.1 12.0 15.2 2.5 0.33 1.0 16.0 (Humatrope)14 f 17.7 −4.43 135.6 37.0 20.1 11.0 0.62 — —15 f 9.06 −4.47 103.8 15.2 14.1 3.0 0.33 2.0 16.9 (Norditropin)
aFamilial cases.
TABLE II. Results of TRH Test in Children With Congenital Combined Pituitary Hormone Deficiency*
Patient
Prlb (mU/l) TSHc (mU/l)
0 min 15 min 30 min 60 min 90 min 0 min 15 min 30 min 60 min 90 min
1a 25 31 50 37 32 0.98 2.5 2.5 2.1 1.42 65 113 106 98 75 0.04 0.05 0.07 0.07 0.084 53 50 84 84 81 0.04 0.03 0.04 0.03 0.035a 144 168 171 202 168 0.48 0.70 0.79 0.78 0.706a 46 67 79 88 84 0.06 0.03 0.03 0.02 0.028 113 210 193 213 209 0.04 0.04 0.03 0.02 0.019a 216 213 241 298 228 0.15 0.17 0.24 0.42 0.57
10a 119 205 263 276 180 0.35 0.51 0.75 0.84 0.7511a 90 99 136 117 103 0.05 0.05 0.06 0.08 0.0912a 85 148 144 153 163 0.16 0.29 0.50 0.40 0.3913 81 107 114 84 77 1.8 2.5 2.9 3.0 3.014 58 38 77 63 66 0.03 0.11 0.01 0.02 0.0215 169 157 189 186 175 0.10 0.15 0.09 0.10 0.13
*TRH test was not conducted for patients 3 and 7.aFamilial cases.bNormal range: boys, 100–280 mU/l; girls, 129–340 mU/l.cNormal range: 0.17–2.9 mU/l.
362 Fofanova et al.

Japan). Purified PCR products were amplified againusing an ABI PRISM Dye Terminator Cycle Sequenc-ing Ready Reaction kit (Perkin Elmer). A reaction mix-ture (20 ml) contained 3 mL of PCR products (10 ng/ml),8 ml of Terminator Ready Reaction mixture, 1 ml ofprimer (3.2 pmol), and H2O. PCR was performed for 25cycles at 96°C for 10 sec, 50°C for 5 sec, and at 60°C for4 min. After excess dye terminators were removed byCENTRI-SEP Columns (Princeton Separation Inc.),loading buffer was prepared by combining deionizedformamide and a mixture containing 25 mM of EDTA(pH 8.0) and 50 mg/ml blue dextran in a ratio of 5:1,and the buffer (6 ml) was resuspended with each DNAsample. After vortexing and spinning down, thesamples were heated at 90°C for 2 min to denature inhot dry bath and placed on ice until loading. DirectDNA sequencing of both strands of the end-purifiedPCR products was performed using an ABI PRISM 377DNA Sequencer (Perkin Elmer).
A mutation in PIT1 was detected in only one patient(patient 1). The mutation was a heterozygous C-T sub-stitution at codon 14 of exon 1, resulting in proline toleucine substitution (P14L; Fig. 2). The same heterozy-gous mutation was observed in her mother, maternalaunt, and maternal grandmother (Fig. 3). However, noevidence for dwarfism in the parents’ relatives wasdemonstrated by their medical records. There was no
consanguinity between the parents. No mutations weredetected in any exons or the promoter region amongthe remaining 14 children studied.
DISCUSSION
Our study demonstrated a novel PIT1 mutation,P14L, in one Russian child with congenital combinedGH/Prl/TSH deficiency. It is interesting that the P14Lidentified here is close to the position of a previouslyreported P24L mutation in a 5-year-old Japanese boy[Ohta et al., 1992]. Both patients had total GH/Prl andpartial TSH deficiency without mental retardation,and each of them was heterozygous for the mutant al-lele. Mutations in the two patients were located in thesame, highly conserved region of the main transactiva-tion domain in PIT1 [Ingraham et al., 1990]. However,in neither family was there any evidence of inheriteddwarfism, although several maternal relatives had theidentical heterozygous mutation. Since an abnormalityin other regions of PIT1, such as in introns, could not beexcluded in our patient, which might be inherited fromthe father’s pedigree, further expression studies suchas in vitro expression studies are needed to confirm thefunctional defect of the P14L mutation. Okamoto et al.[1994] described a family where a patient and his ap-parently healthy father, grandmother, and aunts were
Fig. 2. DNA sequence analysis of patient 1. Partial sequences of PIT1-exon 1 show a C to T transition at codon 14 (arrows).
Fig. 3. Pedigree analysis of the family of patient 1 (closed circle). Half-closed circles show heterozygosity for P14L mutation.
TABLE III. Thyroid Status of Children With Congenital Combined Pituitary Hormone Deficiency
PatientTSH
(mU/l)Free T4(pmol/l)
T3(nmol/l)
T4(nmol/l)
Clinical symptoms of hypothyroidism attime of GH deficiency diagnosis
1a 1.6 (0.98) 10.6 (4.6) NA NA −d
2 1.3 (0.04) 13.1 (4.2) NA NA −d
3 1.2 12.2 NA NA −4 0.60 2.7 0.3 36.1 +5a 0.03 4.8 1.52c 63.9c +6a 0.10 6.2 1.47 43.5 +7 NAb NA NA NA +8 0.03 12.6c 0.9c 62.5c +9a 0.10 4.6 NA NA +
10a 0.03 11.1c 0.56c 106.0c +11a NA 4.3 1.6 41.2 +12a 1.26 4.2 1.5 51.2 +13 1.57 4.3 1.35 51.4 +14 0.1 3.4 NA 28.0 +15 0.70 4.01 NA 52.7 +
aFamilial cases.bNA, data not available.cData on L-thyroxine treatment.dLater, low TSH and thyroid hormone levels were detected and L-thyroxine treatment was begun.
PIT1 Mutation Analysis in Russian Dwarf Children 363
all heterozygous for an R271W mutation. They deter-mined which allele was expressed in lymphocytes inthe family members. As a result, a skewed pattern ofbiallelic expression was observed in the patient,whereas only the normal allele was expressed in otherrelatives with the mutation [Okamoto et al., 1994].Thus, the monoallelic expression in the patient wouldhave occurred through a genomic imprinting mecha-nism in which the maternally derived allele is silentand only the paternally derived allele is expressed[Okamoto et al., 1994]. However, the pedigree of ourpatient (patient 1) is unfavorable to the hypothesis,because both her mother and maternal grandmotherhad the identical PIT1 mutation.
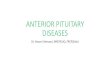
A total of nine different types of PIT1 mutations hasbeen reported in children with combined pituitary hor-mone deficiency [Li et al., 1990; Ohta et al., 1992;Radovick et al., 1992; Tatsumi et al., 1992; Parks et al.,1993; Yoshimoto et al., 1995; Brown et al., 1996] (TableIV). The mutations were found in exons 1, 3, 4, and 6that cover 4 of 6 exons of PIT1. A single mutation wasobserved in exon 1 (P24L) and two in exon 3 (R143Qand F135C). Exons 4 and 6 are believed to be the mu-tational hot spots for PIT1 mutations. Indeed, three ofthe nine mutations were located in exon 4 (R172X,A158P, and E174G) and three in exon 6 (R271W,P239S, and E250X). The 9 patients were Japanese,Dutch, German, Swiss, Saudi Arab, Thai, Tunisian andAmerican.
Mechanisms by which heterozygous mutations real-ize their dominant-negative effect on transactivationare widely discussed. Three alternative explanationsproposed included: 1) blockade of accessing the Pit-1
protein to the promoter by mutant Pit-1 homodimers,2) inhibition of wild-type Pit-1 action through ho-modimer formation with mutant Pit-1, and 3) interac-tion of mutant Pit-1 with limiting transcription factorand inhibition of its function when bound to DNA[Radovick et al., 1992; Parks et al., 1993; Phillips andCogan, 1994]. The mutations identified so far are clas-sified into several groups, according to the mutationsites (POU-S, POU-HD, or transactivation domains),type, and mechanism of action [Parks et al., 1995].Elimination of entire Pit-1 protein arises from a dele-tion involving the whole part of the gene [Pfaffle et al.,1992], and this sort of mutation was found in twoDutch children [Wit et al., 1989], each of them beingheterozygous for the PIT1 deletion and for an A158Pmissense mutation. Nonsense mutations, such as a ho-mozygous R172X mutation [Tatsumi et al., 1992] andcompound heterozygous for R172X/E174G mutations[Brown et al., 1996] result in the elimination of theentire POU-H domain and production of severely trun-cated Pit-1 protein that lacks the binding activity topromoter region. Missense mutations (e.g., homozy-gous mutations for A158P [Pfaffle et al., 1992], R143Q[Ohta et al., 1992], and for F135C [Pellegrini-Bouilleret al., 1996]) lead to loss of transcriptional activation,and result in essential reduction in DNA-binding ac-tivity. Transcriptional inactivation of mutant Pit-1 pro-tein due to P239S and E250X mutations was also de-scribed in seven children from three Saudi Arabianfamilies [Pernasetti et al., 1996] and in a Thai girl [Irieet al., 1995], respectively. R271W [Yoshimoto et al.,1995; Ohta et al., 1992; Radovick et al., 1992; Zegher etal., 1995] as one of the most common PIT1 mutations
TABLE IV. Summary of Reported Cases of Pit-1 Gene Abnormalities in Children With GH/Prl/TSH Deficiency
PatientPit-1 genemutation
A single basesubstitution Exon
No. ofpatients
Origin/country Inheritance Reference
1 R172X/R172X CGA→TGA 4 1 Japanese Recessive Tatsumi et al., 1992(Arg→Stop)
2 A158P/A158P GCA→CCA 4 2 Dutch Recessive Pfaffle et al., 1992(Ala→Pro)
A158P/Del 4 2 Dutch Recessive Pfaffle et al., 1992; Wit et al., 19893 R271W/Wild CGG→TGG 6 1 USA Dominant- Radovick et al., 1992; Rogol and Kahn, 1976
(Arg→Thr) negative1 Japanese Dominant- Ohta et al., 19924 Dutch negative
German Dominant- Pfaffle et al., 1992Swiss negative
2 Belgian Dominant- Zegher et al., 1995negative
4 R143Q/R143Q CGA→CAA 3 1 Japanese Recessive Ohta et al., 1992(Arg→Gln)
5 P24L/Wild CCT→CTT 1 1 Japanese Dominant- Ohta et al., 1992(Pro→Leu) negative
6 E250X/E250X GAA→TAA 6 1 Thai Recessive Irie et al., 1995(Glu→Stop)
7 P239S/P239S CCT→CCC 6 7 Saudi Recessive Pernasetti et al., 1996(Pro→Ser) Arabian
8 E174G/R172X GAA→GGA 4 1 USA Recessive Brown et al., 1996(Glu→Gly)(CGA→TGA(Arg→Stop)
9 F135C/F135C TTT→TGT 3 4 Tunisian Recessive Pellegrini-Bouiller et al., 1996(Phe→Cys)
10 P14L/Wild CCT→CTT 1 1 Russian Dominant- Ours(Pro→Leu) negative
364 Fofanova et al.

had been attributed to dominant-negative mutationsthat may inhibit transcriptional activation. However,since all these patients [Yoshimoto et al., 1995; Ohta etal., 1992; Radovick et al., 1992] as well as a mother-child pair reported by Zegher et al. [1995] were hetero-zygous for mutant allele special attention must be paid,especially for an involvement of other mutation sites inthe gene, in order to know whether the disease occursthrough a dominant-negative effect or through simplerecessive mechanism.
Our study failed to demonstrate any PIT1 mutationsin the remaining 14 Russian children with combinedpituitary hormone deficiency. Further analysis is abso-lutely necessary. A newly cloned gene, the prophet ofPit-1 (Prop-1) that is the gene for a pituitary-specific,paired-like homeodomain factor may be a candidate,since its mutation has been identified in the Amesdwarf lines [Sornson et al., 1996].
ACKNOWLEDGMENTS
This work was supported in part by a Grant-in-Aid(No. 06042009) from the Ministry of Education, Cul-ture and Science of Japan.
REFERENCESBrown MR, Parks JS, Voss TC, Vander-Heyden TC, Rich B, Rosenthal I,
Hurley DL (1996): Compound heterozygosity for Pit-1 mutations. “Ab-stract for 10th International Congress of Endocrinology, San Fran-cisco,” p 176.
Devost D, Oble S, Boutin JM (1996): Prolactin stimulates Pit-1 gene tran-scription in GC cells. “Abstract for 10th International Congress of En-docrinology, San Francisco,” p 303.
Diamond SE, Gutierrez-Hartmann A (1996): A 26 amino acid insertiondomain defines a functional transcription switch motif in GHF-2/Pit-1.‘‘Abstract for 10th International Congress of Endocrinology, San Fran-cisco,” p 316.
Herr W, Sturm Ra, Clerc RG, Corcoran LM, Baltimore D, Sharp PA, In-graham HA, Rosenfeld MG, Finney M, Ruvkun G (1988): The POUdomain: A large conserved region in the mammalian pit-1, oct-1, oct-2,and Caenorhabditis elegans unc-86 gene products (letter). Genes Dev2:1513–1516.
Ingraham HA, Albert VR, Chen RP, Crenshaw EB 3rd, Elsholtz HP, He X,Kapiloff MS, Mangalam HJ, Swanson LW, Treacy MN (1990): A familyof POU-domain and Pit-1 tissue-specific transcription factors in pitu-itary and neuroendocrine development. Annu Rev Physiol 52:773–791.
Irie Y, Tatsumi K, Ogawa M, Kamijo T, Preeyasombat C, Suprasongsin C,Amino N (1995): A novel E250X Mutation of the Pit-1 Gene in a patientwith combined pituitary hormone deficiency. Endocr J 42:351–354.
Kinoshita E, Parks JS, Brown MR, DiMattia G, Baba T, Matsumoto T,Yoshimoto M (1994): Human splicing variation of Pit-1 mRNA in afamily with GH, PRL and TSH deficiency. Clin Pediatr Endocrinol3(suppl 4):77–82.
Li S, Crenshaw EB 3rd, Rawson EJ, Simmons DM, Swanson LW, Rosen-feld MG (1990): Dwarf locus mutants lacking three pituitary cell typesresult from mutations in the POU-domain gene pit-1. Nature 347:528–533.
Miyai K, Hayashizaki H, Hiraoka Y, Matsubara K, Endo Y, Nishijo K,Matsuura M, Kohno H, Labbe A (1988): Familial hypothyroidism dueto thyrotropin gene abnormality. In Imura H, Shizume K, Yoshida S(eds). “Progress in Endocrinology.” Amsterdam: Elsevier, pp 545–550.
Ohta K, Nobukuni Y, Mitsubuchi H, Fujimoto S, Matsuo N, Inagaki H,Endo F, Matsuda I (1992): Mutations in the Pit-1 gene in children withcombined pituitary hormone deficiency. Biochem Biophys Res Commun189:851–855.
Okamoto N, Wada Y, Ida S, Koga R, Ozono K, Chiyo H, Hayashi A, Tat-sumi K (1994): Monoallelic expression of normal mRNA in the PIT1mutation heterozygous with normal phenotype and biallelic expressionin the abnormal phenotype. Hum Mol Genet 3:1565–1568.
Parks JS, Pfaffle RW, Brown MR (1992): New genetic findings in old syn-dromes. Acta Paediatr (suppl) 383:73–77.
Parks JS, Abdul-Latif H, Kinoshita E, Meacham LR, Pfaffle RW, BrownMR (1993): Genetics of growth hormone gene expression. Horm Res40:54–61.
Parks JS, Kinoshita E, Pfaffle RW (1993): Pit-1 and hypopituitarism.Trends Endocrinol Metab 4:81–85.
Parks JS, Brown MB, Abdul-Latif H, Kinoshita E (1995): Abnormalities ofthe pituitary-specific transcription factor-1 gene and protein. Clin Pe-diatr Endocrinol 4(suppl) 6:33–39.
Pellegrini-Bouiller I, Belicar P, Barlier A, Gunz G, Charvet J-P, Jaquet P,Brue T, Vialettes B, Enjalbert A (1996): A new mutation of the geneencoding the transcription factor Pit-1 is responsible for combined pi-tuitary hormone deficiency. J Clin Endocrinol Metab 81:2790–2796.
Pernasetti F, Milner RDG, Ashwal AA, Milner RDG, Ashwal AA, Lacoq P,Marial JA (1996): Combined pituitary hormone deficiency caused by anew PIT-1 mutation. “Abstract for 10th International Congress of En-docrinology, San Francisco,” p 955.
Pfaffle RW, DiMattia GE, Parks JS, Brown MR, Wit JM, Jansen M, Vander Nat H, Van den Brande JL, Rosenfeld MG, Ingraham HA (1992):Mutation of the POU-specific domain of PIT-1 and hypopituitarismwithout pituitary hypoplasia. Science 257:1118–1121.
Phillips JA III, Cogan JD (1994): Genetic basis of endocrine disease 6:Molecular basis of familial human growth hormone deficiency. J ClinEndocrinol Metab 78:11–16.
Radovick S, Nations M, Du Y, Berg LA, Weintraub BD, Wondisford FE(1992): A mutation in the POU-homeodomain of Pit-1 responsible forcombined pituitary hormone deficiency. Science 257:1115–1118.
Rogol AD, Kahn CR (1976) Congenital hypothyroidism in a young manwith growth hormone, thyrotropin and prolactin deficiencies. J Pediatr88:953–958.
Rosenfeld MG (1991): POU-domain transcription factors: Pou-er-ful devel-opment regulators. Genes Dev 5:897–907.
Ruvkin G, Finney M (1991): Regulation of transcription and cell identity byPOU domain proteins. Cell 64:475–478.
Sanno N, Teramoto A, Matsuno A, Takekoshi S, Osamura RY, Lloyd RV(1996): Expression of Pit-1 and estrogen receptor messenger ribo-nucleic acids in prolactin producing pituitary adenomas. Nonradioiso-topic in situ hybridization analysis. “Abstract for 10th InternationalCongress of Endocrinology, San Francisco,” p 242.
Sornson MW, Wu W, Dasen JS, Flynn SE, Norman DJ, O’Connell SM,Gukovsky I, Carriere C, Ryan AK, Miller AP, Zuo L, Gleiberman AS,Andersen B, Beamer WG, Rosenfeld MG (1996): Pituitary lineage de-termination by the Prophet of Pit-1 homeodomain factor defective inAmes dwarfism. Nature 384:327–333.
Tatsumi K, Miyai K, Notomi T, Kaibe K, Amino N, Mizuno Y, Kohno H(1992): Cretinism with combined hormone deficiency caused by a mu-tation in the PIT-1 gene. Nature Genet 1:56–58.
Tuggle CK, Trenkle A (1996): Control of growth hormone synthesis. DomesAnim Endocrinol 13:1–33.
Wit JM, Drayer NM, Jansen M, Walenkamp MJ, Hackeng WH, ThijssenJH, Van den Brande JL (1989): Total deficiency of growth hormone andprolactin, and partial deficiency of thyroid-stimulating hormone in twoDutch families: A new variant of hereditary pituitary deficiency. HormRes 32:170–177.
Yoshimoto M, Aoki S, Baba T, Matsumoto T, Hayashi S, Tsuji Y, MatsudaI (1988): A severe case of pituitary dwarfism associated with prolactinand thyroid-stimulating hormone deficiencies. J Jpn Pediatr Soc92:136–142.
Yoshimoto M, Kinoshita E, Wit JM (1995): Characterization of clinicalfeatures in patients with growth hormone, prolactin and thyroid-stimulating hormone deficiencies due to a transcriptional factor “Pit-1”abnormality. Clin Pediatr Endocrinol 4(suppl):41–51.
Zegher F, Pernasetti F, Vanhole C, Devlieger H, Van der Berghe G, MartialJA (1995): The prenatal role of thyroid hormone evidenced by fetoma-ternal Pit-1 deficiency. J Clin Endocrinol Metab 80:3127–3130.
PIT1 Mutation Analysis in Russian Dwarf Children 365