Embed Size (px)
Citation preview
OXYPHILIC GRANULAR CELL ADENOMA OF THE PAROTIDGLAND (ONCOCYTOMA)
REPORT OF FIvE CASES AND STUDY OF OXYPHILIC GRANULARCELLS (ONCOCYTES) IN NORMAL PAROTID GLANDS *
Luis MEZA-CHAVEZ, M.D.t(From the Departments of Pathology of Memorial Hospital, New York, N.Y., and of the
University of Michigan, Ann Arbor, Mich.)
Although the parotid gland is the most common site of neoplasms ofthe salivary glands,1~a pure adenoma in this location is considered ararity.2"11 McFarland9 reported a "possible case," reviewed the litera-ture, and concluded that "nearly all, if not, indeed, all, of the describedadenomas are but mixed tumors of unusual appearance." This statementis now no longer valid since the literature contains several reports of trueadenomas of which McFarland's case is a good example. A study of thereported adenomas leads to the impression that some of them belong toa definite neoplastic entity, because of the similarity of their cellularcomponents. The characteristic cells have been variously designated.They are epithelial in origin and larger than the normal cells of theparotid gland; they have granular or reticulated oxyphilic cytoplasm,according to the stain employed. Their nuclei are dark-staining, fre-quently pyknotic, and with irregular contours.
Schaffer12 was the first to describe these cells as "granular swollencells." He found them in the ducts and acini of salivary glands of thetongue, uvula, pharynx, and esophagus. Pischinger13 described themin the sublingual gland. Zimmermann14 observed them in the trachea,floor of the mouth, and sublingual glands. Because of the characteristicsof their nuclei he called them pyknocytes. Hamperl 15 studied the uvular,sublingual, and submaxillary glands of 85 persons whose ages rangedfrom infancy to 96 years. He gave a very complete and detailed descrip-tion of the same cells and called them "onkocytes" because of theirincreased size. He found them occasionally in persons under the ageof 5o, but they occurred more frequently between 5o and 70, and werepresent practically always in those over 70 years of age. These peculiarcells sometimes formed tumor-like areas of hyperplasia disposed assolid or adenomatous foci.15'16 In addition he described transitional formsbetween both ductal and acinar cells and the "onkocytes." 15 Steinhardt1examined the sublingual, submaxillary, and parotid glands of 65 personsand found 8 examples of what he thought were the "transitional form"
* Received for publication, June 4, 1948.t Hubert E. Rogers' Fellow in Pathology.
523

MEZA-CHAVEZ
between normal cells and the "onkocytes" described by Hamperl15;these "transitional forms" were found in 5 persons over 8o years of ageand in 3 between 6o and 8o years. Steinhardt failed to mention specif-ically in which of the glands he found the cells. He also observed nodularhyperplasia in the submaxillary glands of 2 of his cases; one of thesewas of the solid and the other of the adenomatous papillary type. Ham-perl17 wrote that the cells of the "transitional form" of Steinhardt were"onkocytes." Skorpil'I mentioned that in ioo salivary glands he found5 exam-)les of "oncocytes" forming nodular hyperplasia. The areas ofhyperplasia were present in submaxillary, sublingual, and nasal mucosalglands. Stout18 found cells of the same type in the bronchi of adults anddiscussed their possible relationship to the cells of bronchial adenomas.Nohteri19 studied the mucous membrane of the nose and of the larynx of4I and 37 persons, respectively, and his results were similar to those ofHamperl.'5 He found "oncocytes" only in persons over 52 years of ageand regularly in those over 70. In addition, he described a cyst in thelarynx composed of "oncocytes."
"Oncocytes" have been found also in other organs. Hamperl20 listedthe following: Parotid, submaxillary, sublingual, and minor salivaryglands; thyroid gland, parathyroid gland, hypophysis (anterior andposterior lobes), testicle, fallopian tube, pancreas, liver, stomach, andthe glands of the pharynx, trachea, and esophagus. Hamperl17 alsomentioned that Veratti21 had noted similar cells in the salivary glandsof dogs.
McFarland9 reported what seems to be the first proved case of pureadenoma of the parotid gland composed of the oxyphilic granular cells.*At that time he was not convinced that the lesion was a true adenoma,but seemed inclined to consider it as a mixed tumor of unusual appear-ance as shown by his conclusion: "The occurrence of gland-like tumors(adenomas) and of tumors containing varying quantities of glandulartissue is no indication that such tumors arise from the glandular tissueproper, but simply goes to show that glandular tissue may sometimespreponderate over other tissue components of mixed tumors." Thisview was restated in I93622 when, on commenting about the recurrenceof the tumor after I2 years, he said: "Subsequent events fully justifiedits original classification as a mixed tumor."23 However, in 194224 and194325 he referred to this adenoma as a "Hiirthle cell tumor (onchocy-toma)" and placed it under the group of "tumors mistaken for mixedtumors."
* The term "oxyphilic granular cell" will be used as a synonym of "oncocyte" and ofother terms used to designate the cells under discussion.
524

OXYPHILIC ADENOMA OF PAROTID GLAND
Gruenfeld and Jorstad26 reported the second example. They were thefirst to point out the similarity of the "onkocytes" of Hamperl to thecells of the case reported by McFarland as well as to those of their own.Their case appeared to be of multicentric origin. They expressed theopinion that it had originated from the duct system, and they called theirlesion an "onkocyte tumor." Harris27 reported a case which seemed tobe of multicentric origin from the ducts. He objected to the name onko-cytoma and stated: "Inasmuch as the onkocyte has also been namedpyknocyte, this tumor could be called pyknocytoma, but the need forany such name is not apparent." Skorpil10 reported 4 cases of adenomaof which the fourth was another example of parotid tumor composed of"onkocytes." As did the two previous authors, Skorpil stated that thetumor arose from the ducts, and added that the name "onkocitares"adenoma or "onkocytoma" would be appropriate for such a tumor.Ackerman6 recorded another example of adenoma and tabulated thereported cases up to that date. He reported his case under the name"oncocytoma of the parotid gland." Lloyd8 reported the most recentcase of parotid adenoma of the type under review, which is case 8 of hispaper. He used the name "oncocytoma of the parotid" to designate histumor. The only other proved case of tumor of this type found in thesalivary glands is that of AhlbomI who reported an adenoma of the hardpalate which probably arose from the minor salivary glands of thatregion.
Besides these cases which can definitely be accepted as examples ofthe type of tumor composed of oxyphilic granular cells, there are someothers which may be considered as possibly belonging to the samegroup, and also a few which have been included by some authors withoutsufficient justification. One probable case is the first of the two adenomasreported by HUckel28 of which part of the description and one illustration(his Fig. i) have some resemblance to the tumors under discussion. An-other is one of the two parotid adenomas briefly described by Blair andOlch.3 The possible acceptance of one of these is based on the fact thatGruenfeld and Jorstad,26 who had an opportunity of examining the casesof Blair and Olch, stated that "one of the two specimens was found to bean exact replica" of the tumor they reported. McFarland 24,25 mentionedanother case that probably is a tumor of this type. He included it, to-gether with his case reported in I927, under the title "Hiirthle cell tumor(onchocytoma)." However, he mentioned only that the patient was afemale, 74 years old, who had had a tumor in the left parotid gland formany years. The tumor was excised, but he did not describe or illustrateit. Another possible case, because of the description given, is the one
525

5MEZA-CHAVEZ
reported by Duplay29 which was examined by M. Ravier, but was notillustrated. Of the cases included in the group without adequate justifica-tion are two adenomas reported by Stohr and Risak,30 another reportedby Franssen,31 and one more reported by Steinhardt."' The cases of St6hrand Risak should not be included for the reasons already mentioned byHarris27; Franssen's case, about which Lloyd8 said "there seems nogood reason for not including this tumor among the oncocytomas,"cannot be accepted because neither the description nor the illustrationsis characteristic of the tumors here discussed. Steinhardt's case cannotbe included because I believe that this case represents a different type, ofwhich I have had an opportunity to study a few examples that provedto be unlike the ones described in this communication.Tumors formed by "onkocytes" have been reported in some other
organs besides the salivary gland. Hamperl20 summarized those casesand listed the pancreas, thyroid and parathyroid glands, and hypophysisas sites in which they have been described.
OXYPHILIC GRANULAR CELLS IN NoRMAL PAROTID GLANDSFrom the review of the available literature, it is evident that despite
the statement20 that "onkocytes" have been found in the parotid gland,no definite proof has been given of their demonstration in normal parotidglands. This made apparent the necessity of finding out if they arepresent in the parotid gland and if they form foci of nodular hyperplasiasimilar to those described in the other salivary glands. Their demonstra-tion was considered especially important since, with one exception, allof the salivary gland tumors composed of "onkocytes" occurred in theparotid. It is the purpose of this comun ication to summarize the re-sults of the search for "onkocytes" in IOO parotid glands and to report5 new cases of parotid adenoma believed to correspond to the grouphere reviewed.The IOO parotid glands were obtained from 5I persons on whom
autopsy was performed in the University Hospital (Michigan). Thesewere unselected persons who died from various diseases or from accidentor violence. Their ages ranged from 7 months to 76 years. Twenty-ninewere under 50 years of age, I7 between 5o and 70 years, and 5 wereover 70 years.Most of the material was fixed in io per cent formalin, but absolute
alcohol also was used in some cases. The sections were stained routinelywith hematoxylin and eosin, and Mayer's mucicarmine stain was donein every case in which oxyphilic granular cells were found. Best's car-mine stain was used also in the few instances in which the alcohol-fixedmaterial showed the cells under study.
526
OXYPHILIC ADENOMA OF PAROTID GLAND
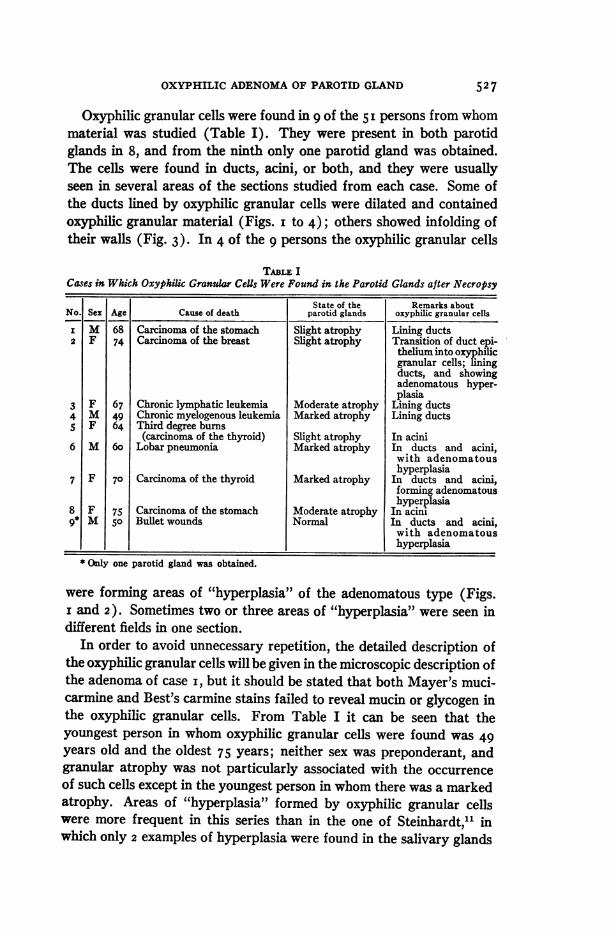
Oxyphilic granular cells were found in 9 of the 5 I persons from whommaterial was studied (Table I). They were present in both parotidglands in 8, and from the ninth only one parotid gland was obtained.The cells were found in ducts, acini, or both, and they were usuallyseen in several areas of the sections studied from each case. Some ofthe ducts lined by oxyphilic granular cells were dilated and containedoxyphilic granular material (Figs. I to 4); others showed infolding oftheir walls (Fig. 3). In 4 of the 9 persons the oxyphilic granular cells
TABLE ICases in Which Oxyphilic Granular CeUs Were Found in the Parotid Glands after Necropsy
State of the Remarks aboutNo. Sex Age Cause of death parotid glands oxyphilic granular cells
i M 68 Carcinoma of the stomach Slight atrophy Lining ducts2 F 74 Carcinoma of the breast Slight atrophy Transition of duct epi-
thelium into oxyphilicgranular cells; liningducts, and showingadenomatous hyper-plasia
3 F 67 Chronic lymphatic leukemia Moderate atrophy Lining ducts4 M 49 Chronic myelogenous leukemia Marked atrophy Lining ductsS F 64 Third degree burns
(carcinoma of the thyroid) Slight atrophy In acini6 M 6o Lobar pneumonia Marked atrophy In ducts and acini,
with adenomatoushyperplasia
7 F 70 Carcinoma of the thyroid Marked atrophy In ducts and acini,forming adenomatoushyperplasia
8 F 75 Carcinoma of the stomach Moderate atrophy In acini9* M 5o Bullet wounds Normal In ducts and acini,
with adenomatoushyperplasia
* Only one parotid gland was obtained.
were forming areas of "hyperplasia" of the adenomatous type (Figs.i and 2). Sometimes two or three areas of "hyperplasia" were seen indifferent fields in one section.
In order to avoid unnecessary repetition, the detailed description ofthe oxyphilic granular cells will be given in the microscopic description ofthe adenoma of case i, but it should be stated that both Mayer's muci-carmine and Best's carmine stains failed to reveal mucin or glycogen inthe oxyphilic granular cells. From Table I it can be seen that theyoungest person in whom oxyphilic granular cells were found was 49years old and the oldest 75 years; neither sex was preponderant, andgranular atrophy was not particularly associated with the occurrenceof such cells except in the youngest person in whom there was a markedatrophy. Areas of "hyperplasia" formed by oxyphilic granular cellswere more frequent in this series than in the one of Steinhardt,1l inwhich only 2 examples of hyperplasia were found in the salivary glands
527
MEZA-CHAVEZ
of 65 persons. The list of causes of death shows that with two exceptionsoxyphilic granular cells were present in persons with a neoplastic process.This relationship may not be significant since the cells occur in a periodof life when neoplasms are commonly found. Also, the necropsy servicefrom which this material was obtained is heavily weighted with casesof neoplastic disease. A study of a larger and more representative seriesis necessary to evaluate this relationship, which was not brought outin Hamperl's study.15
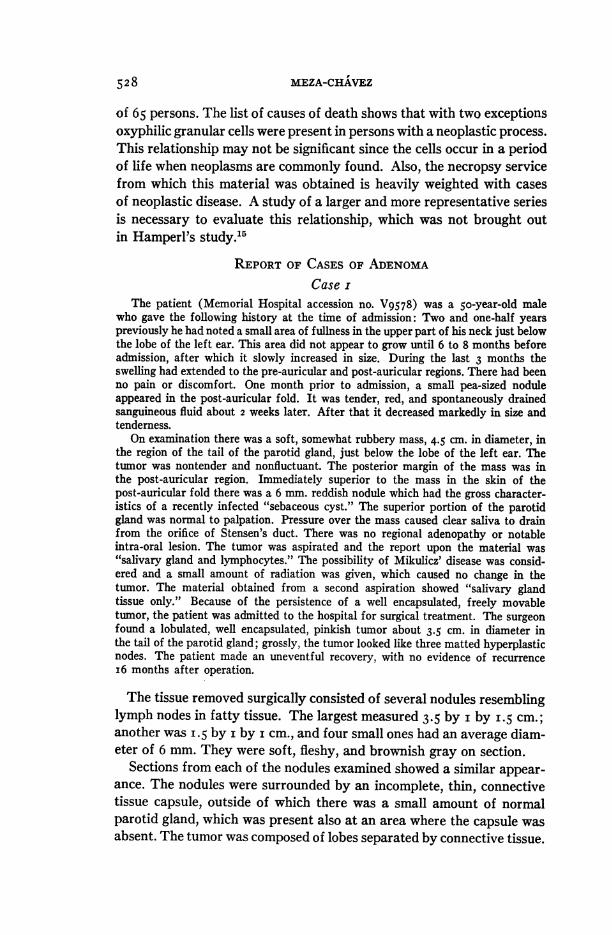
REPORT OF CASES OF ADENOMACase i
The patient (Memorial Hospital accession no. V9578) was a 5o-year-old malewho gave the following history at the time of admission: Two and one-half yearspreviously he had noted a small area of fullness in the upper part of his neck just belowthe lobe of the left ear. This area did not appear to grow until 6 to 8 months beforeadmission, after which it slowly increased in size. During the last 3 months theswelling had extended to the pre-auricular and post-auricular regions. There had beenno pain or discomfort. One month prior to admission, a small pea-sized noduleappeared in the post-auricular fold. It was tender, red, and spontaneously drainedsanguineous fluid about 2 weeks later. After that it decreased markedly in size andtenderness.
On examination there was a soft, somewhat rubbery mass, 4.5 cm. in diameter, inthe region of the tail of the parotid gland, just below the lobe of the left ear. Thetumor was nontender and nonfluctuant. The posterior margin of the mass was inthe post-auricular region. Immediately superior to the mass in the skin of thepost-auricular fold there was a 6 mm. reddish nodule which had the gross character-istics of a recently infected "sebaceous cyst." The superior portion of the parotidgland was normal to palpation. Pressure over the mass caused clear saliva to drainfrom the orifice of Stensen's duct. There was no regional adenopathy or notableintra-oral lesion. The tumor was aspirated and the report upon the material was"salivary gland and lymphocytes." The possibility of Mikulicz' disease was consid-ered and a small amount of radiation was given, which caused no change in thetumor. The material obtained from a second aspiration showed "salivary glandtissue only." Because of the persistence of a well encapsulated, freely movabletumor, the patient was admitted to the hospital for surgical treatment. The surgeonfound a lobulated, well encapsulated, pinkish tumor about 3.5 cm. in diameter inthe tail of the parotid gland; grossly, the tumor looked like three matted hyperplasticnodes. The patient made an uneventful recovery, with no evidence of recurrencei6 months after operation.
The tissue removed surgically consisted of several nodules resemblinglymph nodes in fatty tissue. The largest measured 3.5 by i by I.5 cm.;another was I.5 by i by i cm., and four small ones had an average diam-eter of 6 mm. They were soft, fleshy, and brownish gray on section.
Sections from each of the nodules examined showed a similar appear-ance. The nodules were surrounded by an incomplete, thin, connectivetissue capsule, outside of which there was a small amount of normalparotid gland, which was present also at an area where the capsule wasabsent. The tumor was composed of lobes separated by connective tissue.
528

OXYPHILIC ADENOMA OF PAROTID GLAND
The lobes were divided into irregular lobules by thin fibrous strands.There was some fatty tissue, particularly about the periphery of thetumor and within the normal parotid gland. Blood vessels of mediumsize were seen throughout. The lobules were formed by masses of epi-thelial cells arranged in a solid fashion, forming cords composed ofsingle or double rows of cells (Figs. 6 and ii ) or adopting a tubular oracinar pattern (Fig. io). The epithelial cells lay on a thin basementmembrane which in some cases was indistinguishable from the walls ofcapillary blood vessels running between the cords of cells (Fig. 6). Thecells were large, spherical, oval, columnar, pyramidal, or polyhedraldepending on the pattern which they formed. Their boundaries wereclearly seen when they formed cords, acini, or tubules, but were difficultto make out in the solid masses. The cytoplasm was abundant, granular,and stained intensely with eosin (Fig. 6). The granules were small,regular in size, and stained reddish with Masson's trichrome stain andpurplish blue with Mallory's aniline blue. A fine reticulated structurecould be made out in some of the cells in which the granules were in thespaces of the network. The nuclei were small, round or oval, with finegranular chromatin evenly distributed. They had a prominent nucleolus,and sometimes two nucleoli were seen. Some of the cells had two nucleior an elongated nucleus with a constricted area in its middle portion.Throughout the sections there were some cells which stained moreintensely. They were elongated, pyramidal, or irregular, with dark,irregularly indented nuclei in which no nucleoli could be seen. Their moreeosinophilic cytoplasm contained slightly larger granules. These cellsoften were in pairs or in small groups.The ducts were markedly reduced in number and only a few could be
considered normal. Some of the excretory ducts were distended withcoarsely granular substance in which a few leukocytes and desquamatedcells were seen (Fig. 7). A few ducts showed flattened epithelium whichprogressively changed into a cuboidal type with the characteristicoxyphilic cells. When studied in serial sections, one branched duct withthe features previously described showed the cells of its ramificationsto be continuous with cords of tumor cells (Fig. 7). In some instancesthe striated ducts, lined with eosinophilic cells, were seen also to forma unit with cords of tumor cells, all of them resting on a continuous basalmembrane.Some of the intercalated ducts were lined by stratified squamous
epithelium and ended in glandular structures. These glandular forma-tions had a basal membrane on which rested a row of low-cuboidal orflattened epithelial cells; toward the center the cells increased in sizeand became vacuolated. These cells had central nuclei; the cells closer to
529

MEZA-CHAVEZ
the lumina of the ducts had irregular pyknotic nuclei. They were seenalso in the lumina of some of the ducts as if forming a holocrine secretion.The structures were similar in all respects to sebaceous glands. Theseglands were observed also to arise from striated ducts in a few instances.
There was an area of parotid tissue in one section, between two lobulesof tumor, in which, in addition to the normal acini with cells containingbluish or purplish blue granular cytoplasm, there were other acini, thecells of which stained from light pink to a marked eosin red. Such aciniseemed to represent different stages of transformation from normalacini into those of the fully developed adenomatous type. The aciniwhich showed the earliest change were of normal size but the granules oftheir cells were eosinophilic. A narrow, clear halo could be seen aroundeach nucleus (Fig. 8). In a more advanced stage, cells and acini werelarger than is normal. The cells had a more eosinophilic granular cyto-plasm and the clear halos around the nuclei were still present in some ofthe cells (Fig. 9). When the changes were more advanced, the acini wereformed by cells with all of the characteristics of those in the tumor,except that they were slightly smaller (Fig. io). In this stage, a few ofthe cells showed a very fine, faint, perinuclear halo. In all of thesestages the nuclei showed no noticeable change. The different featuresdescribed in the acini were seen to occur also in the intercalated ducts,which in some cases contained a granular eosinophilic substance in theirlumina.
Throughout the sections there were lymphocytes forming irregulargroups but without follicle formation. They were frequently seen aroundducts and they were more numerous in these areas (Fig. 7). There wasno evidence of the presence of any of the components of the "mixedtumors." Careful search of the sections failed to reveal cells undergoingmitosis.
Case 2The patient was a female, 72 years old, who was admitted to the University Hos-
pital with the chief complaint of a swelling in the right side of the neck, present for7 to io years. When discovered it was the size of a small walnut, but it had increasedduring the last 4 to s years. There were no other symptoms.
On examination there was an elongated tumor, soft and uniform in consistency.It extended from the right mastoid and parotid regions downward for a distance ofabout 6 cm. The tumor was movable, nontender, and measured about 4 cm. in width.It was removed surgically and the surgeon stated that it was well encapsulated, lobu-lated, and soft. It extended from the level of the hyoid bone to a point 2 cm. aboveand behind the angle of the jaw. The tumor was easily stripped from its capsuleafter several large vessels passing through it had been clamped and divided. Therewas mild facial palsy after the operation. The patient recovered uneventfully andher palsy completely disappeared. She was without evidence of recurrence 12 yearsand 8 months after operation.
530
OXYPHILIC ADENOMA OF PAROTID GLAND
The tissue removed surgically (University of Michigan, no. W406-AN)was a flat, lobulated tumor measuring 8 by 5 by 2.5 cm. with a uniformlyfirm consistency. On section it showed a dark brown, lobulated surface.
Microscopic sections revealed a lobulated tumor surrounded by a thinfibrous capsule. The lobes were separated by septa which in some areasresembled those of a normal parotid gland. A small amount of non-neoplastic parotid gland was seen outside the capsule and also inside ofit about the periphery of the tumor (Fig. I4). The parotid tissue justinside the capsule was greatly compressed. There were many thin-walledblood vessels in all sections. This tumor was similar in appearance tothat of case i, with areas of solid and loose structure. There was fattytissue throughout the section, but it was more abundant in the less solidareas. Normal ducts were absent from all of the sections. The few ductspresent were seen in the interlobar septa. They were lined by stratifiedsquamous epithelium and one of them contained desquamated epitheliumin its lumen. There was lymphocytic infiltration around some of theducts; there were groups of lymphocytes in other areas of the tumoralso, but they never formed germinal centers. The tumor cells, like thosein case i, were arranged in cords, acini, tubules, and gland formation(Figs. I2 and I3). The cellular details were similar to those of the previ-ous case except for areas in which the granular appearance of the cyto-plasm was not so apparent. The granularity of the cytoplasm was bestobserved in sections stained with Mallory's aniline blue. The nuclei hadthe same characteristics as in case i, although pyknotic nuclei were notpresent in cells with the more eosinophilic cytoplasm, a type of cell rarelyseen in this case. Some cells were binucleate. At the periphery of thetumor there was an area of dilated ducts lined by cells of the same typeas those seen in the tumor. Some of the ducts contained an eosinophilicgranular material (Fig. 14). The same substance occasionally was seenin the lumina of duct-like structures throughout the tumor. The normalparotid tissue showed areas in which the acinar cells were slightly eosino-philic, suggesting the earliest state of transformation into tumor, asdescribed in case i. Study of numerous sections failed to show anymyxomatous, cartilaginous, or other tissues usually seen in the so-called"mixed tumors" of the parotid gland. Mitotic figures were not seen inany section.
Case 3There was no clinical history available for this case. Two slides (no. 75o7-LAV)
were sent to the Laboratory of Pathology of the University of Michigan with thestatement that they were "from an encapsulated, largely necrotic tumor of theparotid region."
53I

MEZA-CHAVEZ
The tumor might have been about 2 cm. in diameter, as judged by thesections submitted. The sections were stained with hematoxylin andeosin. One of them was restained with Weigert's iron hematoxylin.One of the sections showed a lobulated tumor rimmed by a fibrous
capsule. Outside the capsule there were some salivary gland acini andducts surrounded by proliferating fibroblastic tissue and inflammatorycells. The remainder of the section showed almost complete necrosisexcept in the interlobar septa which were infiltrated by leukocytes. Inthe other section the tumor was encapsulated. It showed a compactstructure with areas of necrosis. There were some thin-walled bloodvessels, more numerous in the center of the section. The cells of thetumor were spherical, oval, or polygonal; they formed a solid mass withsome suggestion of arrangement in cords and acini (Fig. I5). The cellsrested on a basement membrane and stained intensely with eosin. Ingeneral, cellular detail was not very clear, but there were some areasin which the cells showed the characteristic appearance described forcase i. Their nuclei were dark, small, round, or oval, with fine granularchromatin and a single nucleolus. As in the 2 previous cases, there werenone of the components usually found in "mixed tumors," and no evi-dence of mitotic division.
Case 4The patient was a female, 6o years old, who had an abscess in the left parotid
region in I927. She was told that it was due to infected tonsils, and tonsillectomy anddrainage of the abscess were done. In I943 she noted a small tumor at the angle ofthe left jaw. This tumor grew slowly and on one occasion it was excised and drained,but it never disappeared.
On physical examination there was a firm, irregular, oval-shaped mass, measuringabout 4.5 by 2.5 cm., just behind and slightly below the angle of the left jaw. Thetumor was excised. At operation it appeared to be fairly well encapsulated and wasthe size of a large walnut. The tumor was found in the inner prolongation of theparotid gland, and there was no evidence of infiltration.
The only material available from this case was a prepared slide stainedwith hematoxylin and eosin (University of Michigan, no. 8325-LAX).The two sections on the slide showed an encapsulated tumor with inter-lobular septa. Outside of the capsule there was a small amount of normalparotid gland in which two of the intercalated ducts showed glandularstructures indistinguishable from sebaceous glands and similar to thoseobserved in case i. In both sections there was an area of dense fibrousconnective tissue in which some salivary ducts, distended blood vessels,collections of lymphocytes, and a few macrophages containing bloodpigment were present. This area probably represented scar tissue result-ing from the previous excision and drainage. The tumor was formed by
532

OXYPHILIC ADENOMA OF PAROTID GLAND
solid masses of cells bounded by a basement membrane and arranged incords, lobules, and alveoli. The cells were round, oval, or polygonal andhad a finely granular eosinophilic cytoplasm. The nuclei were like thosein the cases previously described (Fig. i 6). No mitotic figures or indica-tions of a mixed tumor were seen.
Case 5This tumor (University of Michigan, no. 4856-LAO) was submitted on March 6,
I937, without clinical history except that it was from the parotid gland of a male.On January 20, I948, it was learned that the patient was without evidence of recur-rence and that he had been 32 years old at the time of operation in I937.
The size of the specimen was not recorded but it probably was aboutI.5 cm. in diameter, judging by the dimension of the sections. Micro-scopic examination showed that the tumor was lobulated and encapsu-lated, with a small amount of normal parotid gland attached to thecapsule. Septa of fibrous tissue separated the lobules. The tumor showedareas of compact structure, into some of which hemorrhage had occurred.In the solid areas the tumor mostly formed cords of cells arranged insingle or double rows. There also were areas of acinar or glandular forma-tion (Figs. i8 and I9). In the areas of hemorrhage the cords had beenbroken up, giving the tumor a pseudo-papillary appearance (Fig. i9).The tumor cells varied in shape from spherical to columnar. Other cel-lular details were the same as described for the other cases, except thatcells with two nuclei were seen more frequently (Fig. I7). Study ofmany sections failed to reveal a myxomatous or chondromatous com-ponent. A few mitotic figures were present.
DIsCUSSIONA definite answer to the question in respect to the significance of oxy-
philic granular cells cannot be given at the present time. Each investi-gator has advanced his opinion. Schaffer"2 considered them as a formof degeneration of the salivary gland epithellum. Pischinger13 inter-preted them as undifferentiated cells which, by amitotic division andfurther development, substituted for the destroyed glandular elements.Zimmermann14 considered them as anomalous cells because' they werenot present in all persons. He also expressed the opinion that they prob-ably were an abnormal form of cellular differentiation. Hamperl 1516'20interpreted them as a peculiar irreversible form of atrophy of the epi-thelium which also, in a broad sense, could be considered as degeneration.He emphasized the fact that the cells under discussion were associatedwith old age and glandular atrophy. Skorpil,'0 on Hamperl's findings
533
and his own, considered them to be normal in old persons and to representan irreversible transformation of the epithelial cells into a new type.However, it is still unknown why that change takes place, and what theactivities of this new type of cell may be. The presence of eosinophilicgranular material in the lumina of some of the ducts, resembling thegranules in the cytoplasm, suggests that they probably are able to secrete,or at least to extrude, part of their cytoplasmic content. This seems tobe true both in the cases in which the cells show "adenomatous" hyper-plasia and in neoplasms in which they assume a glandular structure.
Another problem with which one is confronted is to decide whether thetumors formed by these cells should be considered as true neoplasms oras a form of hyperplasia. The problem is made still more difficult by thefact that the cells involved in the process are not the normal cells of thegland, but result from the transformation of normal cells into cells ofan entirely new type. The best way to answer the question is to try toreconstruct the process that may take place. Normally, for unknownreasons, but probably in relation to advanced age and glandular atrophy,the cells of some ducts, acini, or both, undergo transformation into thenew type, forming isolated groups, or, in other cases, giving origin toareas of "nodular hyperplasia" which may be of solid, adenomatous,or adenomatous and papillary character.0'11'15'16 On the other hand,usually in old persons but not always so and again for unknown reasons,the transformation of the glandular epithellum does not remain localizedbut extends progressively to most of the elements around the originalarea of epithelial transformation, or it may spread from newly formedareas. At the same time, proliferation of the cells results in enlargementof the gland. This enlargement can be explained, first, by increase in sizeof all of the cells involved in the process, since they are larger than theones from which they arise, and secondly, by cellular proliferation, whichin many cases does not seem to be marked, since the evidence of cellulardivision is limited. The result is the formation of a new structure some-times presenting a glandular appearance, but which no longer is parotidgland or has any resemblance to it. In summary, the oxyphilic granularcells form a new and abnormal structure which arises from the glandby transformation of its cells into a new type and involves an increase insize of the area affected. Thus it seems reasonable to conclude that theprocess represents neoplasia rather than glandular hyperplasia.
Sometimes this tumor formation may originate in various areas of"adenomatous hyperplasia" in a single parotid gland. This occurrencemay take place simultaneously or at different times, which explains themulticentric origin of some of the tumors reported, such as those of
r
MEZA-CHAVEZ534
OXYPHILIC ADENOMA OF PAROTID GLAND
Gruenfeld and Jorstad,26 Harris,27 and case i of this communication, allof which were formed in several nodules. It also explains the "recur-rence" of the tumor reported by McFarland,9'22' 23'25 as has already beenpointed out by Ackerman.6 In trying to explain the origin of the tumor,Gruenfeld and Jorstad, Harris, and Skorpil 10 have already demonstratedthat the ducts take part. In their opinions, the tumor originates fromthem. This is true in some cases. However, it is also true that the trans-formation of the cells can occur first in the acini, and in such circum-stances, if a tumor develops, its origin should be considered as being fromthe acini. There seems to be enough evidence to substantiate the beliefthat all epithelial elements of the gland, with the possible exception ofthose of some of the excretory ducts, are liable to undergo transformationinto the new cells and therefore to form the tumor. Evidence that acinarcells take part in the formation of the tumor is found in the changesobserved in such cells in case i (Figs. 8 to io), and to a lesser degree incase 2 of this report. The participation of the acinar component in theformation of tumor seems not to have been observed before, althoughit could have been expected on the basis of the findings in normal glands.The presence of sebaceous glands, observed in ducts of cases i and 4,
will be discussed in another communication,32 but it should be statednow that such sebaceous glands form no part of the tumor. Their occur-rence was entirely incidental.
This tumor, although rare, has characteristic features by which it canbe easily recognized: It is composed of peculiar oxyphilic granular cells,which some authors have compared to the cells of the liver or adre-nal 920'26'27; normal ducts are absent or diminished; and there are groupsof lymphocytes which do not form follicles. This tumor may present anadenomatous form with acinar and tubular formations as in cases i and2, or it may adopt a more solid appearance with few areas of acinar ortubular structure, as in cases 3, 4, and 5 of this report. In the more solidform, the groups of lymphocytes may be few and small.
This tumor has been described or listed under different names, suchas "onkocyte tumor," "oncocytoma," "onkocitiires adenoma," and"Hiurthle cell tumor (onchocytoma)." In addition, the name "pykno-cytoma" has been proposed. The term most commonly used-"oncocy-toma" or "onkocytoma"-was first proposed by Jaffe33 to designate atumor of the parotid region more widely known by the names "papillarycystadenoma lymphomatosum" or "adenolymphoma." The term "onco-cytoma" obviously is based on the name "onkocyte," given by Hamperl 15to the cells herein described. This term "onkocyte," although probablyappropriate for the reasons advanced by Hamperl,' 520 has proved to be
535
536 MEZA-CHAVEZ
confusing since the Greek root Syxos has been used extensively to formother medical terms with the connotation "pertaining to tumor." Inter-pretation of "onkocyte" as "tumor cell" is entirely different from theidea of large size which Hamperl tried to convey by this word.
It is apparent that the term "oncocytoma" should not be used toname the tumor under discussion since it is not only an unfortunateterm, but it was originally devised to designate a different tumor. Theterm "pyknocytoma" suggested by Harris21 does not seem appropriatebecause it uses the word "pyknocyte" already discarded by Hamperl 'for reasons which he gave, and because it implies that the tumor is com-posed of pyknotic cells, which is not correct. Therefore, it is necessaryto devise new terms which will designate more accurately these cells andthe tumors formed by them, and which at the same time will not createfurther confusion. With this idea in mind I believe that a descriptiveterm such as "oxyphilic granular cells" should be used to designate thecells under discussion until future studies determine their exact natureand significance. For the same reasons a similar descriptive term shouldbe used to name the tumor formed by these cells. "Oxyphilic granularcell adenoma of the parotid gland" or "oxyphilic adenoma of the parotidgland" can be used to designate the neoplasms composed of these cellsand of the type described in this communication.
SUMMARYOne hundred parotid glands from 5I persons were investigated for
oxyphilic granular cells (oncocytes). These cells were found in 9 personswho ranged from 49 to 75 years of age. In 4 individuals the cells pro-duced nodular hyperplasia, and in the remaining 5 they were presentin the ducts or acini.
In connection with the description of 5 new cases of oxyphilic granularcell adenoma of the parotid gland (oncocytoma), their origin has beentraced to cells of both ducts and acini which undergo transformation intothe neoplastic type. The descriptive terms "oxyphilic granular cell" and"oxyphilic granular cell adenoma" are proposed to replace the confusingdesignations of "oncocytes" and "oncocytoma."
REFERENCESi. Ahlbom, H. E. Mucous- and salivary-gland tumours. Acta radiol., I935, suppI.
23, 452 pp-2. Bazzoli, L. Pathologia e clinica dei tumori delle ghiandole salivari. Arch. ital.
di chir., 1945, 67, 3-I04.3. Blair, V. P., and Olch, I. Y. Diseases of Salivary Glands. In: Lewis' Practice of
Surgery. W. F. Prior Co., Hagerstown, Md., I944, 4.4. Ewing, J. Neoplastic Diseases. W. B. Saunders Co., Philadelphia & London,
I940, ed. 4, p. 787.

OXYPHILIC ADENOMA OF PAROTID GLAND 537
S. Patey, D. H. The mixed tumours of the salivary glands. Brit. J. Surg., I930-3I,i8, 24I-258.
6. Ackerman, L. V. Oncocytoma of the parotid gland. Arch. Path., I943, 36,508-5 I I.
7. Benedict, E. B., and Meigs, J. V. Tumors of the parotid gland. Surg., Gynec.& Obst., I930, 5i, 626-647.
8. Lloyd, 0. C. Salivary adenoma and adenolymphoma. J. Path. & Bact., I946,58, 699-7Io.
9. McFarland, J. Adenoma of the salivary glands, with a report of a possible case., Am. J. M. Sc., I927, 174, 362-378.
io. Skorpil, F. tJber das Speicheldriusenadenom. Virchows Arch. f. path. Anat.,I940, 306, 714-736.
ii. Steinhardt, G. tYber besondere Zellen in den alternden Mundspeicheldriusen(Onkocyten) und ihre Beziehungen zu den Adenolymphomen und Adenomen.Virchows Arch. f. path. Anat., I933, 289, 624-635.
I 2. Schaffer, J. Beitrdge zur Histologie menschlicher Organe. IV. Zunge. V. Mund-h6hle-Schlundkopf. VI. Oesophagus. VII. Cardia. Sitzungsb. d. k. Akad. d.Wissensch. Math.-naturw. Cl., Wien, I897, io6, Pt. 3, 353-455.
I3. Pischinger, A. Beitrage zur Kenntnis der Speicheldriisen, besonders der Glandulasublingualis und submaxillaris des Menschen. Ztschr. f. mikr.-anat. Forsch.,1924, I, 437-489.
I4. Zimmermann, K. W. Die Speicheldrilsen der Mundh6hle und die Bauchspeichel-drilse. In: M6llendorff, W. v. Handbuch der mikroskopischen Anatomie desMenschen. J. Springer, Berlin, I927, 5, Pt. I, I28.
i5. Hamperl, H. Beitrage zur normalen und pathologischen Histologie menschlicherSpeicheldriusen. Ztschr. f. mikr.-anat. Forsch., I93I, 27, I-55.
i6. Hamperl, H. Onkocyten und Geschwiilste der Speicheldriusen. Virchows Arch. j.path. Anat., I93I, 282, 724-736.
I7. Hamperl, H. Ober besondere Zellen in altemden Mundspeicheldriisen (Onko-cyten) und ihre Beziehungen zu den Adenolymphomen und Adenomen. Vir-chows Arch. f. path. Anat., I933, 29I, 704-705.
i8. Stout, A. P. Cellular origin of bronchial adenoma. Arch. Path., I943, 35, 803-807.I9. Nohteri, H. A case of laryngeal cyst composed of oncocytes and the appearance
of oncocytes in mucous membrane of the nose and larynx. Acta path. etmicrobiol. Scandinav., I946, 23, 473-483.
20. Hamperl, H. Uber das Vorkommen von Onkocyten in verschiedenen Organenund ihren Geschwiulsten. Virchows Arch. f. path. Anat., I936-37, 298, 327-375-
2I. Veratti, E. Sui picnociti delle ghiandole salivali del cane. Monitore zool. ital.,I933, suppl. 43, I22. (Cited by Hamperl.17)
22. McFarland, J. Three hundred mixed tumors of the salivary glands, of whichsixty-nine recurred. Surg., Gynec. & Obst., I936, 63, 457-468.
23. McFarland, J. Ninety tumors of the parotid region, in all of which the post-operative history was traced. Am. J. M. Sc., I926, 172, 804-848.
24. McFarland, J. The histopathologic prognosis of salivary gland mixed tumors.Am. J. M. Sc., I942, 203, 502-5I9.
25. McFarland, J. The mysterious mixed tumors of the salivary glands. Surg.,Gynec. & Obst., I943, 76, 23-34.
26. Gruenfeld, G. E., and Jorstad, L. H. Adenoma of the parotid salivary gland:oncocyte tumor. Am. J. Cancer, I936, 26, 57I-575.
27. Harris, P. N. Adenoma of the salivary glands. Am. J. Cancer, I936, 27, 690-700.
28. Huckel, R. Eine ungewohnliche Adenomform der Parotis. Verhandl. d. deutsch.path. Gesellsch., 1930, 25, 342-347.
538 MEZA-CHAVEZ
29. Duplay, M. Ad6noma de la glande sous-maxillaire. Arch. gin. de m4d., I875,I, 60I-603.
30. Stbhr, F., and Risak, E. Zur Klinik und Anatomie der Parotisgeschwillste. Arch.f. klin. Chir., I926, 143, 609-648.
3I. Franssen, R. Eine Parathyreoidea- 1hnliche Geschwulst der Ohrspeicheldriisen.Zentralbi. f. aUg. Path. u. path. Anat., I932-33, 56, II3-II5.
32. Meza-ChAvez, L. Sebaceous glands in normal and neoplastic parotid glands.Possible significance of sebaceous glands in respect to the origin of tumors ofthe salivary glands. Am. J. Path. (In press.)
33. Jaffe, R. H. Adenolymphoma (onkocytoma) of the parotid gland. Am. J. Cancer,1932, I6, I4I5-I423.
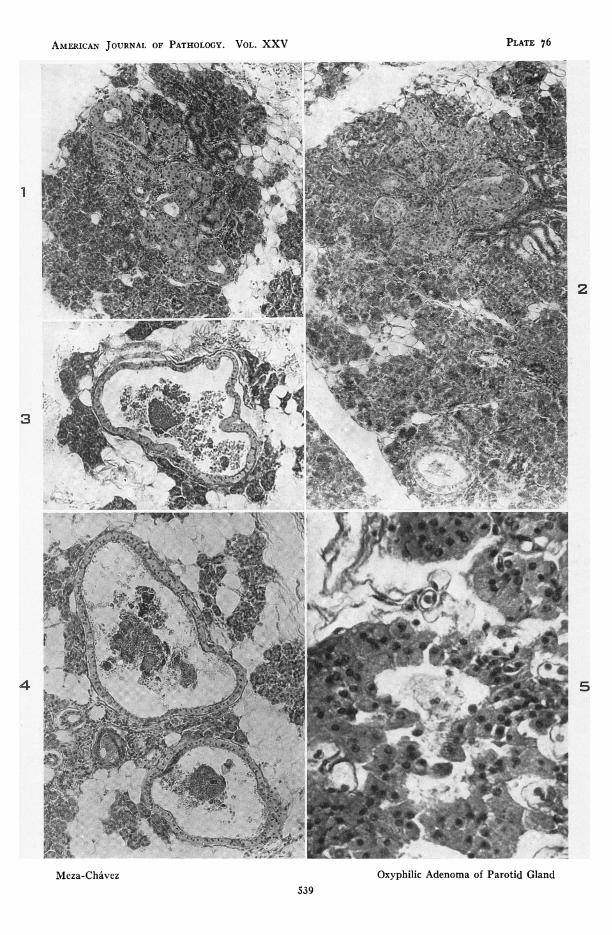
DESCRIPTION OF PLATESAll photomicrographs were obtained from slides stained with hematoxylin and
eosin, unless otherwise stated.
PLATE 76
FIGs. i and 2. Case 2, Table I. Oxyphilic granular cells forming "adenomatoushyperplasia" in a normal parotid gland. There is a dilated duct lined byoxyphilic granular cells in the lower portion of Figure 2. X II5.
FIGS. 3 and 4. Case 4, Table I. Normal parotid gland, showing dilated ducts lined byoxyphilic granular cells. Of note are the granular material in the lumina of theducts and the infolding of the wall of the duct in Figure 3. X 1I5.
FIG. S. Case 7, Table I. Oxyphilic granular cells from another area of hyperplasia inan otherwise normal parotid gland. X 375.
AMERICAN JOURNAL OF PATHOLOGY. VOL. XXV
2
.. ..6Z -k-4 i'
:,
F.:;
5
_----------
hl ar_i e .
Oxyphilic Adenoma of Parotid GlandMeza-Chavez539
at...::
..sj. I
:. ..
U.sg
PLATE 76
I
t IWIA

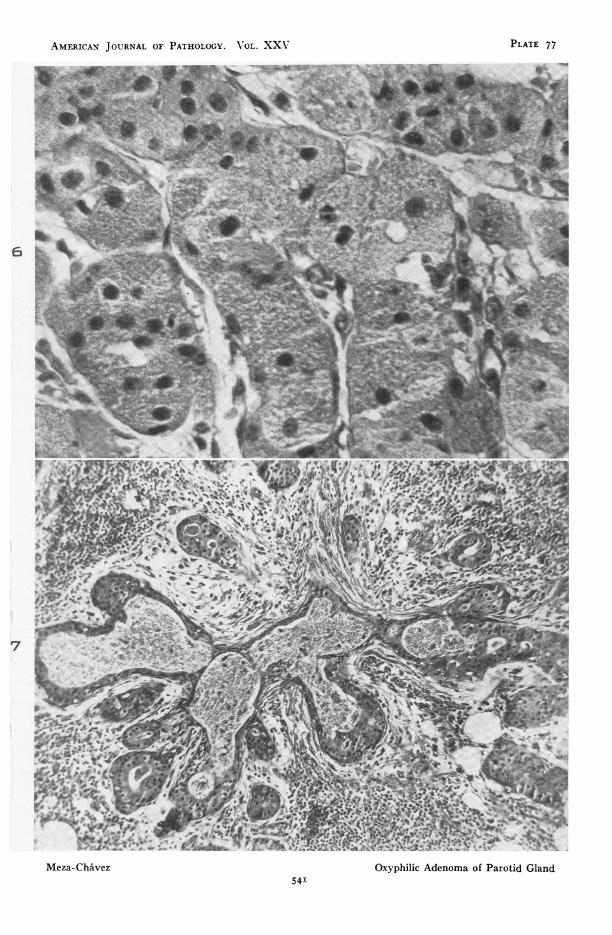
PLATE 77
FIG. 6. Case i. Area from the adenoma of the parotid gland in which cords of cellsare seen as well as the characteristic cellular structure of the oxyphilic granularcells. Trichrome stain. X 650.
FIG. 7. Case I. Distended duct containing oxyphilic granular material in its lumenand lined by oxyphilic granular cells in all its branches. Trichrome stain.X IOO.
540
AMERICAN JOURNAL OF PATHOLOGY. V OL. XXX PLATE 77
aw~~~~~~~~~a
AMIL~~~~~~~~~~~~~~~~~~~~~~~~~
N. ~ ~ ~ ~ ~ ~ ~ ~ ~ .
_a_I;1i._.... X -. X _ w ,^j
_.141ii- 21C t r.
^ l * E . g ~~~~~~~~~~- - -s*#s~~~~~.--e
rWN4~~~~~~~
Meza-CAvez xy hiicAeoa fPrtiGln
W~~/'_V-_~~,:^. j _w. o
.~~~~~~~~~~~_U...'¶Mea-hAe Oxni Anom of. PaotiGan
541-1., ,,' .1 - _,,,- -- .a_.

PLATE 78
FIGS. 8 to IO. Case i. Three stages of transformation of parotid epithelium intooxyphilic granular cells as described on page 530. X 375.
FIG. II. Case i. Area of the neoplasm in which the cells are forming cords composedof single and double rows of cells. X I25.
542
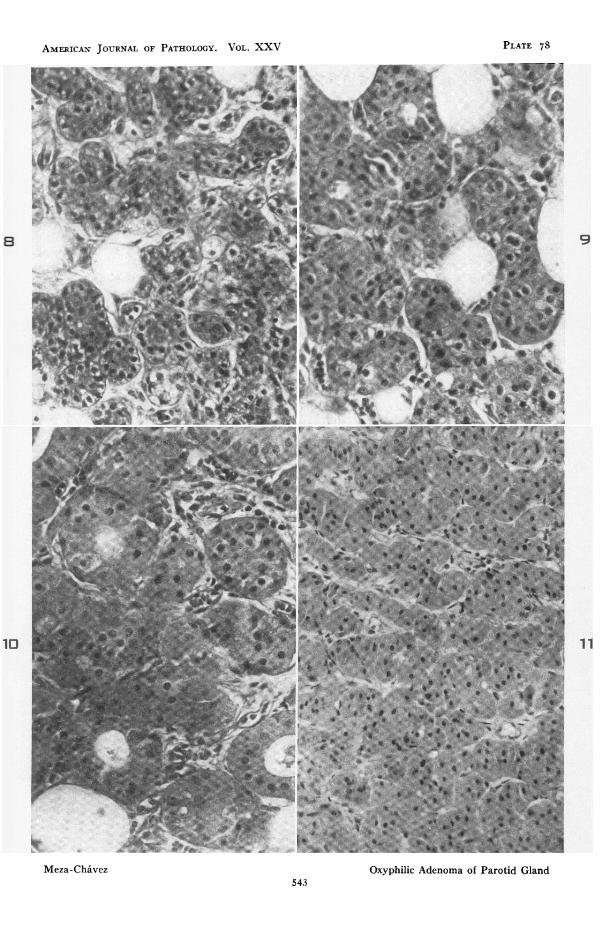
PLATE 78AMERICAN JOURNAL OF PATHOLOGY. VOL. XXV*-- -- @e b.0 _, | | s 9# - Xs l 1[ '^ .i s __. j - __ | _ X n5 w . r.. _.s _q_. si i__s ! E:_|Dl
...... g a. .. _2 _j. , !1W1 . * _l * t1 F ia 11i ...................................... i s_ L.4 . . 1|11_ 1n # 2 E : ._ . * iA *. .r .s S* | m _ _]---| | *.si:-*-2
::-e---* * --s-.--..}^x - i w w - r__F '1 w wOw--e-k , k w]* D'_UKiR *iv X go X .-
.."...._B":. r t.; ....^.,.*. K__ '_CU_i_;=<t.. . =tR-F__rF____r_t._____s _fffi.ff __
_,_.__' g.____ }|___ '_ s_ a__ _ __ 0t?'
_>-. B?jr rrr_z__ F i ................................................... .: _t_ R_J+ _ffi_ _ffi__ __ Z _4p__> '__ _|fi 11 r1'__:0'':: t m__L_ _2 'Wb:S_-,.s __
X B;J_Wz _ P_ s__s__z. _
A2-_.___sg 11
_meB_F_T_t __ f sj?f I_ , . -.................._ 'pF . : i .?ws wi .,. "
*_ 3| . -' *i?':,
* w y iiiiiiiL __ _ _
t_^;t3_ua.Ww,Sz
_ z t.sIE
w :¢ * '' R'. K
Meza-Chavez Oxyphilic Adenoma of Parotid Gland543
_ _- _2- _______________,_._

PLATE 79
FIG. I2. Case 2. Parotid adenoma. Area of the tumor showing a tubular and acinarstructure. X II5.
FIG. I3. Case 2. Parotid adenoma. Tubular and acinar structure seen at highermagnification. X 315.
FIG. I4. Case 2. Parotid adenoma. Of note are the distended ducts lined by oxy-philic granular cells, the infolding of the wall of one of the ducts, and the non-neoplastic parotid gland about the periphery of the tumor. X III.
FIG. I5. Case 3. Area from parotid adenoma. Weigert's iron hematoxylin and eosinstain. X II5.
544

AMERICAN JOURNAL OF PATHOLOGY. VOL. XXV PLATE 79
13
II
_* S
Meza-Chivez Oxyphilic Adenoma ofParotidGland 15
Meza-Chaivez Oxyphilic Adenoma of Parotid Gland545
_ -_,_ -v -- - - -

PLATE 8o
FIG. i6. Case 4. Area from adenoma of the parotid gland, showing the characteristicappearance of the oxyphilic granular cells. X 375.
FIG. I7. Case 5. Parotid adenoma. In this area the tumor has a solid appearance, andthere are several binucleated cells. X 375.
FIG. I8. Case 5. Normal parotid gland outside the tumor capsule. The neoplasmshows a mixed solid and acinar structure. X II5.
FIG. I9. Case 5. Portion of parotid adenoma showing a pseudo-papillary appearance.X II5.
546

AMERICAN JOURNAL OF PATHOLOGY. VOL. XXV PLATE 8o
AL~
I~~~~~~~~~~~~~~~~~~~~~~~~~
I.
Oft17
547Oxyphilic Adenoma of Parotid Gland


















![Litera art [by_mike_rt_scifi]](https://img.pdfslide.net/doc/110x75/5593631e1a28ab98478b4715/litera-art-bymikertscifi.jpg)