Embed Size (px)
Citation preview

Pergamon
0021-9630(95)0126-3
J. Child Psychol. Psyekial. Vol. 37, No. 4, pp IW -̂.'JT'*, 19%Elsevier Science Ud
© 1906 Associalion far Child Psychology anit PsychialryPrinled in Great Britain. All rights reserved
f](}2i-'it>y)m 115.00 + 0,00
Rating Child Psychiatric Caseness From Detailed Case Histories
Robert Goodman, Carole Yude, Hilary Richards and Eric Taylor
Department of Child and Adolescent Psychiatry, Institute of Psychiatry, London, U.K.
Novel operationalized criteria were used to rate detailed psychiatric case histories on 151schoolchildren with hemiplegia. Ratings of psychiatric caseness or non-caseness werereliable and valid; the method may be widely applicable. Caseness was defined bothnarrowly (in terms of social incapacity for the child) and broadly (in terms of disruption toothers and distress too). Both definitions could be applied reliably to children of normalintelligence but broadly defined caseness was more reliable for children with lowintelligence. Barely half of the psychiatric cases met operationalized criteria for one ormore DSM-IV or ICD-10 diagnosis. The others mostly had partial or mixed syndromesthat could, with clinical judgement, be assigned to 'not otherwise specified' diagnoses.Even with clinical judgement, however, a substantial minority of children with lowintelligence had clinically significant but undiagnosable abnormalities in socialrelated ness.
Copyright v(. 1996 Association for Child Psychology and Psychiatry.
Keywords: Child psychiatry, caseness, diagnostic criteria, classification
Introduction
In most child psychiatric studies of epidemiological orhigh-risk satnples, the prevalence of psychiatric disorder('caseness rate') is a key measure. When psychiatricdisorder is defined solely in terms of recognizedcotistellations of psychiatric symptoms, this cati resultin implausibly high caseness rates. For example, Bird etal. (1988) estimated from their epidemiological studythat 49.5% of Puerto Rican children aged between 4 and16 years met criteria for at least one DSM-III diagnosis.As Bird, Yager, Staghczza, Gould, Canino and Rubio-Stipec {1990} note, many of the children who wereeligible for DSM-III diagnoses were not significantlysocially impaired by their symptoms, did not seem inneed of treatment, and did not correspond to whatclinicians would normally recognize as 'cases'. For mostepidemiological purposes, children should not beclassified as psychiatric cases unless their psychiatricsymptoms have a significant impact (e.g. Rutter, Tizard& Whitmore, 197()b; Bird et al., 1990).
The impact of child psychiatric symptoms canpotentially be judged in one of several ways. Bird etal. (1990) suggest that the impact of symptoms should bejudged solely from the resultant social impairment, i.e.from the extent to which the symptoms compromise thechild's ability to fulfil normal role expectations ineveryday life. Though this unitary criterion is appea-lingly parsimonious, two other potential indices of
Requests for reprints to: Dr R. Goodman, Department of Childand Adolescent Psychiatry, Institute of Psychiatry, DeCrespigny Park, Umdon SE5 8AF, U.K.
symptom impact have considerable face validity, namelythe extent to which the symptoms cause disruption forothers or distress for the child.
Externalizing symptoms can sometimes lead tosubstantial disruption for others without resulting inmuch social impairment for the child. For example, theparents and siblings of children with severe physical orintellectual disabilities are sometimes remarkably stoicalin the face of marked opposition, tantrums anddestructiveness, having learned to circumvent or toleratethese behaviours at considerable cost to themselves. Itdoes not seem reasonable to say that such a child doesnot have a disorder simply because the family absorbsthe disruption without making the child 'pay for it'. Inkeeping with this, caseness in the Isle of Wight studieswas defined in terms of symptoms that resulted in socialimpairment for the child or that had a major impact onothers (Rutter et al., 1970b).
In some children, internalizing symptoms result insubstantial distress without much social impairment.Like their adult counterparts, anxious or depressedchildren are sometimes able to fulfil normal roleexpectations while experiencing considerable inneranguish. It does not make clinical sense to describesuch children as free from disorder for as long as theycontinue to 'go through the motions' of their ordinarylives; it is presumably for this reason that DSM-IVdiagnoses of anxiety and affective disorders can be madeif symptoms cause clinically significant distress even ifthey do not result in social impairment (AmericanPsychiatric Association, 1994). Perhaps all psychiatriccaseness should be defined broadly in terms ofsymptoms that result in significant distress for the child,significant social impairment of the child, or significant
369

370 R. GOODMAN el al.
disruption for others; this would correspond better withnormal clinical practice than a narrow definition ofcaseness solely in terms of the child being significantlysocially impaired.
The reported rate of caseness in any population willdepend not only on whether caseness is defined broadlyor narrowly but also on whether the investigators use abottom-up or top-down approach to the recognition ofpsychiatric disorder. Investigators using a bottom-upapproach determine whether their subjects meet thediagnostic criteria for any of the specific disordersrecognized by the current classifications (perhapsapplying additional impact' criteria to ensure thatchildren are only diagnosed as having a disorder if theirsymptoms have a significant impact). Following thisbottom-up approach, children need to meet the criteriafor at least one disorder to be considered a 'case'. Thepotential problem with this approach is that somechildren may fall between the cracks of our currentdiagnostic systems—a concern that may be particularlyrelevant to individuals of low intelligence (Sturmey,1993). A child with disparate symptoms might fail tomeet the diagnostic criteria for any currently recognizeddisorder even though the cumulative impact of thesymptoms is substantial. In order to include suchchildren, a top-down approach starts by classifyingchildren as cases or not according to whether they havepsychiatric symptoms that meet some chosen criterion ofimpact. How many of these children would also havebeen recognized by a bottom-up approach is then opento empirical investigation.
The caseness rates reported by different studies arecommonly contrasted with one another or combined inmeta-analyses. The value of doing this will depend onthe comparability and reliability of the casenessmeasures. Despite the existence of standardized psy-chiatric interviews for children and informants, there arestill major obstacles to generating reliable and validcaseness ratings that have the same meaning when usedby different investigators in different places or atdifferent times. In particular, there is no generallyaccepted method for integrating and reconciling thedifferent information obtained from different sourcesabout symptoms or impact. For instance, how should onejudge impairment in peer relations if a standardizedinterview with the child suggests good peer relationshipswhile standardized interviews with teachers and parentssuggest the opposite? Researchers may be tempted todefine a simple decision rule, e.g. that priority shouldalways be given to the child's report, or that the resultsof the three informants should be averaged. Cliniciansare likely to be suspicious of such simple rules,preferring to use multiple clues and clinical experienceto arrive at a decision. How convincing was the child'saccount of his friendships? Did the rest of what the childsaid suggest that he was a poor informant or prone togiving socially acceptable but inaccurate information?How long had the teacher known the child? Did theteacher appear to be an astute observer? Was that teacherever on playground duty? Having weighed up these andnumerous other factors, the clinician will arrive at ajudgement, sometimes prioritizing one informant, some-times another. If the final rating of caseness depends on
such clinical judgements, does this seriously underminereliability?
In the course of a study of the psychiatric complica-tions of childhood hemiplegia, we devised and used anoperationalized top-down method for determining thepresence or absence of psychiatric disorder. Casenesswas defined both narrowly and broadly, and clinicaljudgement was used in the interpretation of conflictinginformation. In this paper we address several questions.How reliable and valid was our method for ratingcaseness? What sorts of cases proved particularlydifficult to rate reliably? What difference did it makewhether caseness was defined narrowly or broadly?What proportion of cases identified using a top-downapproach would have been missed with a bottom-upapproach? What sorts of cases are particularly likely tobe missed by a bottom-up approach?
Method
The London Hemiplegia Register (LHR) used multipleascertainment techniques to recruit a large and representativesample of London children with a clinical diagnosis ofhemiplegia (Goodman & Yude, 1996). Individual assessmentswere carried out on a representative sub-sample of six- to ten-year-olds from the LHR, involving 150 children from GreaterLondon (Goodman & Yude, 1996), plus one hemiplegic childwho lived just outside the Greater London boundary but hadbeen included by error. These 151 children are the samesample described in Goodman (1994). Although the sampleincluded two children who did not appear to be hemiplegic onpersonal examination, these two nonhemiplegic children havebeen included in the analyses reported here since the focus ofthis paper is not on hemiplegia.
A research psychologist (CY) interviewed one or bothparents about their child's emotions, behaviour and relation-ships using a standardized semi-structured interview—theParental Account of Child Symptoms (PACS; Taylor,Schacher, Thorley & Wieselberg, 1986). The same assessorsubsequently administered the Wechsler Intelligence Scale forChildren—Revised (WISC-R, Wechsler, 1974) to subjects,obtaining meaningful scores on 139 subjects (92% of thesample). One of the remaining 12 subjects would not cooperatewith the testing despite repeated attempts (but clearly had mildlearning difficulties as judged by school and home observa-tion), while 11 subjects were functioning at or below the floorof the WISC-R. Overall, 98 subjects were of normalintelligence (10 ^ 70). 34 had mild intellectual impairment(IQ 50-69), and 19 had moderate, severe or profoundintellectual impairment (10 < 50).
Independently of the first assessor, a second assessor (RG)who had trained in paediatric neurology and child psychiatrysaw each child for a standard neurological examination andmental state examination (Rutter & Graham, 1968). Eachassessor was blind to the other's findings until all 151 childrenhad been seen, at which stage the two assessors pooled theirfindings and generated anonymized psychiatric case historieson each subject following a standard format.
Each case history included the child's age, gender andapproximate intelligence so that symptoms could be judged fordevelopmental appropriateness. Enough information on familycomposition and social circumstances was provided to makethe rest of the case history comprehensible. To reduce the riskof bias, no mention was made of the type or degree of physicaldisability unless the case history would have been uninterpre-table without this information. In no case was it necessary todisclose the degree or laterality of the motor disability. It was

CASENESS RATINGS 371
necessary, however, to mention the occurrence of seizures in 5of the 60 children who had current or resolved epilepsy (e.g. inthe case history of a boy whose marked worrying was largelyfocused on when he would next have a seizure). Similarly, itwas necessary in seven instances to mention visual or hearingimpairments, sickle cell disease or diabetes mellitus (e.g. in thecase history of a boy whose marked fear of falling or trippingwas related to his visual impairment).
The following parent-reported symptom domains werecovered in each case history: eating problems; sleep problems;anxieties; fears; misery and depressive symptoms; socialrelationships with parents, other adults, siblings and otherchildren; fidgetiness, restlessness, distractibility and impersis-tence in specified situations (watching television, reading,playing alone and with others, at meal times and on outings);irritability; noncompliance; tantrums; aggression; destructive-ness; lying; stealing; and other antisocial behaviours. If anypotentially autistic symptoms were reported, these wereincluded in the case history, along with an account of thepresence or absence of other potentially autistic symptoms.The following child-reported symptom domains were coveredin each case history: social relationships; anxieties; fears;misery and other depressive symptoms; obsessions andcompulsions; and aggressive and antisocial behaviours.Verbatim transcripts of the parents' and children's owndescriptions of symptoms were used where possible. Eachcase history also recorded the standardized observationalratings made by the assessors at the time of the neurological,psychiatric and psychometric assessment; these ratingscovered the child's attention, activity, oppositionality, affectand style of relating to the assessor. Finally, the case historysummarized which items from the Rutter (1967) and Conners(1969) questionnaires had been endorsed by the child's classteacher.
Using these standardized case histories, the two originalassessors—an experienced child psychiatrist (RG) and re-search psychologist (CY)—rated the 151 subjects on a novelcaseness scale (Appendix I), as well as on separate scales foremotional, conduct and hyperactivity disorders (Appendix 2).Two sample case histories, along with formulations andratings, constitute Appendix 3; a wider range of sample casehistories is available from the first author on request. Whenchildren met Appendix 1 criteria for psychiatric caseness(level 2 or above), the Appendix 2 ratings were used, wherepossible, to subclassify cases into emotional disorders,hyperkinesis (with or without a conduct disorder), or conductdisorders (including mixed disorders of conduct and emotionsbut excluding hyperkinetic conduct disorders). Children witheither hyperkinesis or significant situational hyperactivity werecombined to create a group with broadly defined hyperactivitydisorder [equivalent to Attention Deficit Disorder withHyperactivity (ADDH) in DSM-III; American PsychiatricAssociation, 1980|.
All the subjects were independently re-rated using the samecaseness criteria by an experienced child psychiatrist (HR)
who had had a period of training in the use of the novelcaseness criteria but who had no knowledge of the subjectsother than from the case histories, and who had never workedclinically with the other assessors. The assessors" rating ofcaseness and the independent rating of caseness were bothused in the reliability analyses; only the assessors' rating wasused in the other analyses.
The PACS interview with parents can be used to generateseparate symptom scores for hyperactivity, emotional symp-toms and conduct problems (Taylor et al., 1986; Taylor,Sandberg, Thorley & Giles, 1991). Using these scores, subjectswho did and did not meet our criteria for psychiatric casenesswere compared with community controls and psychiatric clinicattenders who had previously been assessed in other studiesusing the PACS interview (Taylor et al., 1986, 1991). Thiscomparison seemed justified since the researcher (CY) whoadministered and scored the PACS interview in this study hadbeen trained to do so by the team that studied the communitycontrols and psychiatric clinic attenders. When a member ofthat team and CY independently rated 11 audiotapes of PACSinterviews, the intraclass inter-rater reliabilities were 0.95 foremotional symptoms, 0.98 for conduct problems and 0.80 forhyperactivity (Heptinstall & Yude, unpublished data).
Results
Reliability
There was substantial agreement between the inde-pendent rater and the assessors on each subject'scaseness rating (Table I). The ratings were identicalfor 60% (91/151) of subjects. Furthermore, the dis-crepancy was relatively minor for most of the remainingsubjects, with 7% (10/151) of subjects being allocated todifferent subcategories of level 2, and with a one-pointdifference in caseness rating for 31% (47/151) ofsubjects. The inter-rater reliability was 0.81(p< 0.001), calculated as the Spearman intra-classcorrelation after combining both subcategories of level2.
There were major two-point discrepancies for justthree subjects (2% of sample), whose relevant char-acteristics are summarized in Table 2. All three had IQsunder 70 and two of the three had odd personalities withsome autistic features. Thus subject A had an odd socialmanner and she sometimes wandered away from home,being unperturbed when lost, even when taken to apolice station. Subject B was preoccupied with aero-planes and windows and tended to perseverate onfavourite themes. The primary cause of the disagreementbetween the two sets of raters was different in each ofthe three cases. For subject A, the existence of socialimpairment was uncertain because of a conflict of
Table 1Level of Caseness: Cross-Tabulation of Assessors' Rating and Independent Rating on Each Subject
Independent rating of caseness
Assessors' rating of caseness 0
268010
1
415281
2A
03960
2B
033
233
3
012
1419
0 = No disorder1 = Dubious disorder2A = Mild disorder (distress or disruption only)2B = Mild disorder (with social impairment)3 = Severe disorder

372 R. GOODMAN et al.
Table 2Subjects Occasioning Markedly Discrepant Rating
Subject A Subject B Subject C
Age10'Odd' personalityConflicting evidence on social impairmentUncertain if social impairment is due to psychiatric symptomsUncertain if 'symptoms' are developmentally appropriate
7 years59
9 years44
7 years20
Table 3Rates and Reliabitities of Broadly and Narrowly Defined Caseness
Whole sample(A'=151)
10 > 70(A' = 98)
IO<70(A'= 53)
Caseness rate(assesors
rating, %)
60
48
83
Broadly defined
Caseness rate(independent
rating, %)
57
48
74
caseness
K
0.74
0.75
0.62
(95%
(0.58,
(0.56,
(0.36,
Cl)
0.90)
0.95)
0.88)
Caseness rate(assesorsrating, %)
50
37
74
Narrowly defined
Caseness rate(independent
rating, %)
45
36
62
caseness
K (95%
0.67 (0.51,
0.76 (0.56,
0.35 (0.08,
Cl)
0.83)
0.96)
0.61)
evidence: parents and teachers were unequivocal that Awas isolated and had no special friends, whereas Aherself named friends readily and said she was neverisolated and lonely. There was no doubt that subject Bwas socially impaired—he was isolated from peers andfitted poorly into his own family—but it was uncertainwhether this rejection stemmed from his odd personalityrather than from his physical and intellectual disabilitiescombined with the prejudices of those around him. Forsubject C, the problem was knowing how muchallowance to make for his very low mental age. C wasmarkedly restless and inattentive but the two sets ofraters disagreed as to whether this amounted to anadditional hyperkinetic disorder or was simply oneaspect of C's profound learning difficulties. The factorscontributing to these marked but rare two-point dis-crepancies also contributed on a lesser scale to thecommoner one-point discrepancies.
The five-point scale of psychiatric caseness wasdichotomized in two ways to generate narrowly andbroadly defined caseness. As narrowly defined, casenesswas limited to children categorized as 2B or 3, i.e.children whose persistent psychiatric problems resultedin significant social impairment (handicap). The broaddefinition of caseness included children categorized as2A as well, i,e. all children whose persistent psychiatricproblems resulted in substantial handicap, distress ordisruption. Table 3 shows the kappa coefficients—ameasure of chance-corrected agreement—for each case-ness definition, both for the sample as a whole and forintellectually normal and learning disabled childrenseparately. Using Landis and Koch's (1977) bench-marks, all the kappa values indicate 'substantial'agreement (and were significant at ;7< 0.001), with the
exception of the 'fair' agreement for narrowly definedcaseness among children with an IQ under 70 (p< 0.01).With the narrow definition of caseness, agreement wassignificantly worse for children with IQs below 70 thanfor children with higher IQs (z = 2.44, p < 0.02). Thispoorer agreement was partly attributable to cases inwhich it was difficult to judge whether challengingbehaviour resulted just in disruption to others, orwhether it also resulted in significant handicap for thechild over and above the handicap already attributable tosevere learning difficulties.
Validity
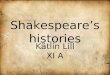
Our caseness criteria could be applied reliably, but didcaseness as defined by these criteria correspond to whatmost clinicians would recognize as a case? To examinethis, we compared the level of symptomatology in our'non-cases' and 'cases' with the levels found incommunity controls and psychiatric clinic attenders.To make the present sample more comparable with thecommunity and clinic groups, subjects with IQs below70 were excluded. For the comparisons presentedgraphically in Fig. 1, the broad definition of casenesswas used to dichotomize the present sample into casesand non-cases. The dimensional measures of hyperac-tivity, conduct problems and emotional symptoms usedin Fig. 1 are based on the number, frequency andseverity of symptoms. In Fig. l(a), the scores of our non-cases are compared with those of normal controls from aprevious epidemiological study (Taylor et al., 1991). InFig. l(b)-(e), the scores of our cases are compared withpsychiatric cases from a previous study of childrenattending a psychiatric clinic (Taylor et al., 1986)—

CASENESS RATINGS 373
(a) No psychiatric disorder
2.5i-
«; 2.0oo
6 ''^I. '0B
VI 0.5
0
This sampleN - 5 2
timmun. controlsN =42
ES(b) Emotional disorder
2.5
K 2.0ou
i"I. 1.0E
0.5Ui
This siimpleN= 15Psyctiiat. controlsN = 12
HA CP ES(c) Conduct disorder
Tliis sampleN= 13Psycliiat. controlsN - 3 9
This sampleN - 7Psychial. controls
HA
(e) ADDH
2.5
a 2.0
S. 10
^ 0.5
0
Cl'
This sampleN = 18Psychiat. controlsN -37
HA ES
Figure I. Mean symptom scores for cases and non-casesfrom this series compared with community controls andchildren attending a psychiatric clinic. HA = hyperactivity;
CP = conduct problem; ES = emotional symptoms.
having matched for diagnostic grouping. As can be seenfrom the profiles, our non-cases were as normal ascommunity controls, while our cases were as abnormalas clinic cases. Subjects and controls differed signifi-cantly on only 4 out of 15 comparisons (asterisked inFig. \,p < 0.05 in each case) without any clear pattern ofdifferences emerging.
Subjects Identified by Broad but not by NarrowDefinitions of Caseness
Of the 91 subjects who met our broad criteria forcaseness, there were 16 (18%) who did not meet ournarrow criteria because their psychiatric symptomsresulted in substantial distress to themselves or disrup-tion to others but not in substantial social impairment.The proportion of broadly defined cases who would nothave met a narrow definition of caseness was 23% (11/47) among children with IQs of 70 or more, as comparedwith 11% (5/44) among children with lower IQs—anonsignificant difference (continuity-adjusted /^=1 .5 ,1 df, p = 0.2).
The 16 subjects identified by broad but not by narrowcriteria comprised: 11 subjects whose emotional symp-toms resulted in substantial distress; three subjectswhose conduct problems resulted in substantial disrup-tion; one subject whose feeding and sleeping problemsresulted in substantial disruption; and one subject withmixed emotional and conduct problems that resulted inboth distress and disruption. The preponderance ofemotional disorders among the children with broadlybut not narrowly defined disorders applied both tochildren with normal and low IQs.
Cases that Might Have Been Missed with a Bottom-Up Approach
Of the 91 children who met our broad casenesscriteria, 56% (51) could be assigned to at least one ICD-10 (World Health Organization, 1993) or DSM-IV(American Psychiatric Association, 1994) diagnosticcategory defined by operationalized criteria, e.g. separa-tion anxiety disorder, oppositional defiant disorder,hyperkinesis, attention-deficit/hyperactivity disorder(ADHD). An additional 36% (33) could be assigned toat least one 'residual' diagnostic category of ICD-10 orDSM-IV, e.g. anxiety disorder, unspecified; disruptivebehaviour disorder, not otherwise specified; attention-deficit/hyperactivity disorder, not otherwise specified(ADHD-NOS). The remaining 8% (7) could not bediagnosed using any ICD-10 or DSM-IV category (apartfrom a 'catch-all" category such as 'Disorder of infancy,childhood or adolescence not otherwise specified'). Theproportion of cases falling into the three categories—having an operationalized diagnosis, having a residualdiagnosis, and being undiagnosable—was almost thesame when the analysis was restricted to the 75 childrenwith narrowly defined caseness (59%, 33% and 8%respectively). Though we report further analyses only forbroadly defined caseness, our findings were similar fornarrowly defined caseness.
Children who had to be assigned residual diagnosesfailed to meet the criteria for operationalized diagnosesfor two main reasons: in some cases, the children metsome but not enough of the criteria for one operationa-lized diagnosis ('partial syndromes'); in other cases, thechildren had some of the features of a variety of relateddiagnoses but did not meet full criteria for any one ofthem ('undifferentiated syndromes'). The commonestpartial syndrome in our series was ADHD-NOS—theonly DSM-IV diagnosis on 14 children. These children

374 R. GOODMAN et al.
had inattention and hyperactivity that resulted inimpairment in just one setting, usually school, therebyprecluding a diagnosis of ADHD. These children couldnot be assigned any diagnosis from the ICD-10 schemesince this scheme has no category for situationalhyperactivity. Another partial syndrome found in ninechildren in our series involved one or two veryprominent externalizing problems without a greatenough variety of problems to meet criteria for anoperationalizedl diagnosis of oppositional defiant dis-order or conduct disorder. For example, one seven-year-old boy's marked problems with irritability and frequenttemper tantrums overshadowed most aspects of hisfamily life and had led the family to seek treatment—buthe did not have enough associated problems to qualifyfor a diagnosis of oppositional defiant disorder. Suchchildren were classified under the rubric of 'disruptivebehaviour disorder not otherwise specified' in DSM-IVand 'conduct disorder, unspecified' in ICD-10. Twofurther children in this series had partial autisticsyndromes. The remaining eight children with residualdiagnoses all had undifferentiated emotional disorders,involving variable mixtures of generalized worrying,separation anxiety, specific and social fears, misery,obsessions and somatic complaints. They had some ofthe elements of many operationalized disorders but didnot meet the full criteria for any of them. The childrenwith residual diagnoses did not differ significantly fromchildren with operationalized diagnoses in terms of age,sex or IQ.
Whereas roughly half of the children with operatio-nalized or residual diagnoses were of normal intelli-gence, all seven undiagnosable children had an IQ of 70or less. One 10-year-old who was functioning at about an18-month-old level had a miscellany of nonorganicfeeding and sleeping problems that severely disruptedher mother's life. The primary problem in the remainingsix undiagnosable children, all of whom had IQsbetween 40 and 70, was an abnormal manner of relatingto other people that resulted in significant impairment inpeer relationships (and sometimes in wider handicapstoo). The assessors felt these children had 'oddpersonalities' but found it hard to characterize theoddness. Though these children did not meet fulldiagnostic criteria for autism, Asperger's syndrome,hyperkinesis or social phobia, their abnormalities ofsocial relatedness did involve elements found in thesedisorders. Thus the following elements were apparent tovarying degrees: lack of social interest, social gauche-ness, insensitivity to social cues, passivity, socialanxiety, disinhibition and a wheedling or pestering stylethat others found hard to tolerate. Impoverished pretendplay and rituals or preoccupations were evident in somebut not all cases. Borderline levels of conduct problemsor emotional symptoms were variable accompaniments.
Discussion
Reliability and Validity
Our operationalized criteria provided a reliablemethod for using detailed case histories in order todichotomize children into 'cases' who had a level of
symptomatology comparable to psychiatric clinic atten-ders, and 'non-cases' who had a level of psychiatricsymptomatology comparable to community controls.Though these findings suggest that our rating scheme isuseful, the subjects of this study all had a diagnosis ofchildhood hemiplegia. Would the criteria be as usefulwith other children? The question can only be answeredby empirical study, but we have no reason to doubt thegeneralizability of our findings; although children withcerebral palsy have a very high rate of psychiatricdisorders, these disorders are qualitatively similar tothose found in other children {Rutter, Graham & Yule,1970a). It is uncertain how far the reliability and validityof the method would be undermined if the criteria wereapplied without prior training or if the criteria wereapplied to less detailed case histories.
We identified three factors that made some casesdifficult to rate reliably. Firstly, when there wasconflicting evidence on social impairment, differentclinicians did not always agree on which source ofevidence to prioritize. In this study, using clinicaljudgement rather than a 'mechanical' decision rule(e.g. always to give precedence to the child's ownaccount) only resulted in one instance of a markeddiscrepancy between raters—a relatively small cost thatmay have been more than offset by increased validity.The second factor that impaired reliability was un-certainty about how much allowance to make for low IQwhen judging inattention and other psychiatric symp-toms that are closely related to developmental level.Once again, since we currently lack the empiricalevidence needed to formulate a valid decision rule onthis issue, there is little to gain by abandoning clinicaljudgement and adopting an arbitrary decision rule for thesake of a small increase in reliability.
The third factor reducing reliability was difficulty inpartitioning handicap. Our criteria specified that psy-chiatric problems only amounted to a psychiatricdisorder if they had a substantial impact in their ownright. For the narrow definition of caseness, thisinvolved determining not only that the child was sociallyimpaired but also that the psychiatric problems ac-counted for a substantial portion of this impairment. Thesecond task was often harder, particularly when the childalso had a learning disability. Consider, for example, ahemiplegic boy who is socially isolated in a mainstreamschool. It may not be easy to judge whether the isolationis due to the boy's irritability and social anxiety (makinghim a psychiatric 'case'), or if the isolation isattributable instead to his peers' responses to thecombination of physical disability, epilepsy, borderlineIQ and socially deprived background (making him a'non-case'). This was less of a problem when we used abroad definition of caseness, judging the impact ofsymptoms from distress and disruption as well as fromsocial incapacity; even in children with severe learningand physical disabilities, it was usually clear, forexample, whether separation anxiety resulted in sub-stantial distress or whether tantrums significantlyincreased the burden on carers^-even when it wasunclear whether the anxiety or tantrums resulted inadditional social impairment.
One possible solution to the difficulty in partitioning

CASENESS RATINGS 375
handicap between psychiatric and nonpsychiatric causesis to abandon the enterprise and consider a child as a'case' provided the child has psychiatric symptoms andis socially impaired (for whatever reason). In our view,this would create more problems than it solved. Manynormal children meet diagnostic criteria for specificpsychiatric disorders without being significantly im-paired by their symptoms—this is precisely whyadditional impairment criteria are used to reduce therate of 'false positive' cases (Bird et al., 1990). It wouldseem absurd, therefore, to label children with relativelylow levels of worrying or oppositionality as psychia-trically disordered simply because they had concurrentphysical or cognitive disabilities that did result inimpairment—the inevitable consequence would be afalsely inflated rate of psychiatric co-morbidity in allphysical and cognitive disabilities.
Using the disability scales of ICD-10 or DSM-IV todecide whether a child does or does not have apsychiatric disorder would potentially embody the worstof all worlds since these scales insist on somepartitioning of disability without separating out theimpact of psychiatric problems from the impact of otherproblems. The global assessment of psychosocialdisability that constitutes Axis VI of the multi-axialversion of ICD-10 (World Health Organization, 1991),for example, includes disability due to psychiatricproblems, specific learning problems or low intelligencebut specifically excludes disability due to physical orenvironmental limitations. The global assessment offunctioning (GAF) scale of DSM-IV is similar (Amer-ican Psychiatric Association, 1994). If either of thesescales were used to determine who did and did not havea psychiatric disorder, it would still be necessary topartition handicap. For example, did a child lack friendsbecause of her behavioural problems or because she wasobese and came from the 'wrong' social class? At thesame time, a child with low-level worrying mightwarrant an anxiety diagnosis if concurrent readingproblems led to appreciable social impairment. Givenall these difficulties, we conclude that when socialimpairment is used to determine who does and does nothave a psychiatric disorder, that measure will have toincorporate a clinical judgement on how far theimpairment is due to the psychiatric problems them-selves. Attempting to improve reliability by removingthis judgement is liable to undermine validity.
Broad or Narrow Criteria?
Among children with normal intelligence, bothbroadly and narrowly defined caseness could be ratedwith high reliability. Since the threshold for broadlydefined caseness identified a group of subjects with alevel of symptomatology equivalent to that of cliniccases, there is no particular reason to suppose that thebroad definition was so wide that a lot of false positiveswere included. For every three cases detected by thenarrow criteria, another case was detected by wideningthe criteria—with most of the extra cases havingemotional disorders. Whether the broad or the narrowdefinition was 'best' cannot be answered by this study.The empirical question that needs answering is how far
the 'core' cases detected by narrow criteria differ fromthe 'extra' cases detected only by the broad criteria—interms of aetiology, service need, treatment response andprognosis.
Sturmey (1993) has highlighted the uncertain relia-bility of applying DSM or ICD diagnoses to people withlearning difficulties. In our study, the reliability of ourcaseness ratings was relatively poor when narrow criteriawere applied to children with IQs under 70. By contrast,good reliability was obtained using broad criteria withthis group of children. We tentatively suggest, therefore,that a broad deflnition of caseness should be preferredwith this group unless there are compelling arguments tothe contrary.
Top-Down or Bottom-Up?
With DSM-III diagnostic criteria, many childrenqualify for at least one psychiatric diagnosis eventhough their symptoms do not have a significant impactand they do not correspond to what clinicians wouldnormally recognize as cases (Bird et al., 1988; 1990). Inother words, a bottom-up approach to case recognitioncan have an unacceptably high false positive rate. Toavoid this, the DSM-IV classification includes an impactcriterion in the definition of the common childpsychiatric diagnoses (American Psychiatric Associa-tion, 1994). As a result, a bottom-up approach to caserecognition using DSM-IV should not include childrenwho would not also have been recognized by a top-downapproach.
The converse does not necessarily apply, however.The top-down approach specifies that children are casesIf their psychiatric problems have a significant impac t -even if they do not meet the diagnostic criteria for anycurrently recognized disorder. How often would casesrecognized by this top-down approach be missed by abottom-up approach? Our findings suggest that theanswer depends both on diagnostic practice and on thenature of the sample.
Barely half of the cases detected with a top-downapproach would have been recognized by a bottom-upapproach that stuck rigidly to the operationalizeddiagnostic criteria of ICD-10 and DSM-IV. Most ofthe remaining children had partial or undifferentiatedversions of these well-defined syndromes; clinicaljudgement was needed to assign these children toresidual diagnoses such as 'disruptive behaviour dis-order, not otherwise specified'. Given a willingness touse clinical judgement in this way, our findings suggestthat a bottom-up approach functions as well as a top-down approach for children of normal intelligence. It isimportant to note, though, that epidemiologica! studiesthat use lay interviewers and a 'checklist' approach todiagnosis may miss a substantial number of clinicallysignificant cases of partial or undifferentiated disorders.
For children of low intelligence, a bottom-upapproach that used both operationalized and residualdiagnoses would still have missed roughly 20% ofchildren found by a top-down approach. Many research-ers have encountered problems applying unmodifiedDSM or ICD criteria to individuals with learningdisabilities (Sturmey, 1993). Our findings suggest that

376 R. GOODMAN et al.
ICD-10 and DSM-IV particularly lack the range ofdiagnostic categories needed for comprehensive cover-age of learning disabled children who are additionallyhandicapped by an abnormal manner of relating to otherpeople. Some but not all of these children couldpotentially be classified as having broadly definedautistic spectrum disorders, with 'aloof, 'passive' and'active but odd' subtypes (Wing, 1985). Other childrenhad rather different abnormalities of relatedness, morereminiscent of the social anxiety seen in the Fragile Xsyndrome (Maes, Fryns, van Walleghem & van denBerghe, 1993), or of the disinhibition seen in hyper-kinesis (Luk, Thorley & Taylor, 1987). There areimportant practical and theoretical reasons for wantingto identify these children as cases. Practically, identify-ing such children is important for service planning andprovision. Theoretically, these children may provide animportant window on brain-behaviour links. For boththese reasons, top-down approaches to case definitionare to be preferred when studying learning disabledchildren.
Acknowledgements—We are very grateful to the children,parents and teachers for their willing cooperation, and to BobAdak and Suzanne Pemberton for their invaluable assistance indata collection and coding. The study was generously fundedby the Wellcome Trust and Scope (formerly The SpasticsSociety).
References
American Psychiatric Association (1980). Diagnostic andStatistical Manual of Mentat Disorders, 3rd ed. Washing-ton, DC: American Psychiatric Association Press.
American Psychiatric Association (1994). Diagnostic andStatisticat Manuat of Mentat Disorders (4th ed), Washing-ton, DC: American Psychiatric Association.
Bird, H. B., Canino, G., Rubio-Stipec, M., Gould. M. S.,Ribera, J., Sesman, M., Woodbury, M., Huertas-Goldman,S., Pagan, A., Sanchez-Lacay, A. & Moscosco, M. (1988).Estimates of the prevalence of childhood maladjustment in acommunity survey in Puerto Rico. Archives of GeneratPsychiatry, 45, 1120-1126.
Bird, H. B., Yager, T. J., Staghezza, B., Gould, M. S., Canino,G. & Rubio-Stipec, M. (1990). Impairment in the epide-miological measurement of childhood psychopathology inthe community. Journal of the American Academy of Childand Adolescent Psychiatry, 29, 796-803.
Conners, C. K. (1969). A teacher rating scale for use in drugstudies with children. American Journal of Psychiatry, 126,884-888.
Goodman, R. (1994). Childhood hemiplegia: is the side of thelesion influenced by a family history of left handedness?
Developmental Medicine and Child Neurology, 36, 406-411.
Goodman, R. & Yude, C. (1996). Do incomplete ascertain-ment and recruitment matter? Developmental Medicine andChild Neurology, in press.
Landis, J. R. & Koch, G. G. (1977). The measurement ofobserver agreement for categorical data. Biometrics, 33,159-174.
Luk, S. L., Thorley, G. & Taylor, E. (1987). Gross over-activity: a direct study by direct observation. Journal ofPsychopathology and Behavioral Assessment, 9, 173-182.
Maes, B., Fryns, J. P., van Walieghem, M. & van den Berghe,H. (1993). Fragile-X syndrome and autism: a prevalentassociation or a misinterpreted connection? GeneticCounseling, 4, 245-263.
Rutter, M. (1967). A children's behaviour questionnaire forcompletion by teachers: preliminary findings. Journal ofChild Psychology and Psychiatry, 8, 1-11.
Rutter, M. & Graham, P. (1968). The reliability and validity ofthe psychiatric assessment of the child: I. Interview with thechild. British Journal of Psychiatry, 114, 563-579.
Rutter, M., Graham, P. & Yule, W. (1970a). A neuropsychia-tric study in chitdhood. Ctinics in developmental medicine,Nos 35136. London: S.I.M.P. with Heinemann.
Rutter, M., Tizard, J. & Whitmore, K. (1970b). Education,health and behaviour. London: Longman.
Sturmey, P. (1993). The use of DSM and ICD diagnosticcriteria in people with mental retardation. Journal ofNervous and Mental Disease, 181, 38-41.
Taylor, E., Schacher, R., Thorley, G. & Wieselberg, M.(1986). Conduct disorder and hyperactivity: I. Separation ofhyperactivity and antisocial conduct in British childpsychiatric patients. British Journal of Psychiatry, 149,760-767.
Taylor, E., Sandberg, S., Thorley, G. & Giles, S. (1991). Theepidemiology of chitdhood hyperactivity. Institute ofPsychiatry: Maudsley Monographs, Vol. 33. Oxford: OxfordUniversity Press.
Wechsler, D. (1974). The Wechsler inteltigence scate forchitdren (Revised Edn). New York: The PsychologicalCorporation.
Wing, L. (1985). Services for severely retarded children andadolescents. In M. Rutter and L. Hersov (Eds), Child andadotescent psychiatry: modern approaches (2nd Edn).London: Blackwell.
World Health Organization (1991). Draji multi-axial versionof ICD-10 prepared for use by clinicians deating with childand adolescent psychiatric disorders. Geneva: WorldHealth Organization.
World Health Organization (1993). The ICD-10 classificationof mental and behavioural disorders: diagnostic criteria forresearch. Geneva: World Health Organization.
Accepted manuscript received 14 August 1995
Appendix 1: Criteria for Psychiatric Caseness
Children should only be rated as psychiatric cases if theymeet all of the following three criteria:
Presence of psychiatric problems i.e. abnormalities ofbehaviour, emotions, or style of relating to others. Examples ofabnormal styles of relating to others include: aloofness, over-
friendliness and gaucheness. Not being popular, or beingactively disliked, are common consequences of psychiatricabnormalities, but peer neglect or rejection are not evidence inthemselves for an abnormal style of relating to others—theymay reflect prejudice about race, class, disability, etc. For'quantitative' symptoms, such as misery or oppositionality.

CASENESS RATINGS 377
distinguishing between problem behaviours and normalitydepends on severity, frequency, persistence, pervasiveness andassociated features. Enuresis, tics, specific learning problemsand low intelligence are not counted as psychiatric problems.
Persistence for at least six months Problems that haveunequivocally ceased by the time of assessment are not coded,but if problems wax and wane without entirely disappearing,the coding should be based on the average level of problemsover the preceding twelve months even if this average level ofproblems is higher than that at the time of assessment.
Substantial impact This is judged primarily by the socialimpairment (handicap) to the child, i.e. the extent to which thepsychiatric problems limit or prevent the fulfilment of normalchildhood roles. The key domains here are home life,friendships, class work, leisure activities and physical safety/wellbeing. In some cases, psychiatric problems result inmarked distress for the child without significant socialimpairment, e.g. the child reports persistent and severeworrying or misery (and parents or teachers may confirmthis), but the child continues to lead a full life, and classroomperformance is not substantially affected. In other cases, thepsychiatric problems result in significant disruption to otherswithout socially impairing the child, e.g. the child extortsmoney from younger children, steals from shops, andvandalizes telephone boxes—but gets on well with familymembers, friends and classroom work. Because it is uncertainwhether problems resulting in distress or disruption withoutsocial impairment should be coded as disorders, they are codedseparately here to allow either splitting or lumping.
On the basis of the information available, each subjectshould be assigned to one of the following caseness levels:
0= Normal: no psychiatric problems, or problems resultingin little or no distress, disruption or handicap.
1 = Dubious disorder: the child has symptoms that are not soclearly outside normal limits that they warrant a 2 or 3rating, but neither are they likely to be trivial as far as thechild, the family or the school are concemed.
2A = Mild disorder involving distress or disruption withouthandicap: psychiatric problems causing significant dis-tress or disruption (or both) but not causing significantsocial impairment.
2B = Mild disorder with handicap: psychiatric problemscausing significant social impairment (and often sig-nificant distress or disruption too).
3 = Severe disorder: psychiatric problems causing severesocial impairment—with marked social incapacity in atleast one key domain, or moderate social incapacity in atleast two domains.
(In principle, level 3 could also have been subdividedaccording to whether the psychiatric problems did or did notresult in handicap for the child. In practice, we did notencounter any child who had what we considered on clinicalgrounds to be a severe disorder that resulted in distress ordisruption without social impairment—so a level 3A categorywas unnecessary.)
Appendix 2: Criteria for Subtype Ratings: No Attempt is Made Here to Separate Mild and Severe Disorders
Hyperactivity Level0 = Not hyperactive. Code here if:
not restless (out of seat, fidgety) or inattentive;equivocal restlessness or inattentiveness (e.g. mini-
mal, or contradictory reports from the samesetting);
restless with normal attention;attention deficit without restlessness.
1 = Borderline: definite restlessness and inattentiveness in atleast one setting (allowing for chronological and mentalage) but not enough of a problem to result in significantsocial impairment in any setting.
2A = Significant situational hyperactivity: definite restlessnessand inattentiveness (allowing for chronological andmental age) that is prominent and handicapping eitherat home or at school—and neither prominent norsignificantly handicapping in the other setting.
2B = Significant pervasive hyperactivity: definite restlessnessand inattentiveness (allowing for chronological andmental age) that are prominent both at home and atschool, and that result in significant social impairment inat least one of those settings.
Emotional Disorder Level0= Normal: no problem/minimal problem.
1 = Borderline: the level of fears, worries, misery orobsessive-compulsive features is not trivial but neitheris it resulting in significant distress or social impairment.This level of symptoms can be thought of as the top endof the normal range.
2A = Significant distress without handicap: fears, worries,misery or obsessive-compulsive features are prominentand distressing for the child, but result in little or nosocial impairment.
2B = Significant handicap: fears, worries, misery or obsessive-compulsive features are prominent and result in sig-nificant social impairment (and usually significantdistress too).
Notes:
Irritability is not counted as an emotional disorder.Fears should only be coded if they are:
definite, e.g. reported both by the child and an adult,or reported by an adult with convincing details ofresultant avoidance or incapacity;
high impact—fears that are not prominent are notcoded (e.g. a child who has a definite but isolatedfear of snakes, who avoids going to the zoo, andwho does not think about snakes in their absence,is coded 0).
A definite and prominent fear (of a commonly encounteredstimulus) is coded 2B if the child avoids the situation leadingto significant social impairment, and is coded 2A if the childendures the stimulus with intense anxiety but is notsignificantly socially impaired by attempts to avoid thestimulus.
Conduct Disorder Level0= Normal: no problem/minimal problem.
1 = Borderline: the level of defiant, aggressive or antisocial

378 R. GOODMAN et al.
behaviours is not trivial but neither is it resulting insignificant disruption or social impairment. This level ofsymptoms can be thought of as the top end of the normalrange; most of these children will be thought of as'difficult' rather than disordered.
2A = Significant disruption without handicap: defiant, aggres-sive or antisocial behaviours are prominent and result insignificant disruption to others, but there is little or noresultant social impairment for the child.
2B = Significant handicap: defiant, aggressive or antisocial
behaviours result in significant social impairment for thechild. The behaviours (and the social impairment) maybe situational or pervasive—and usually result insignificant disruption too.
Note:Marked problems with just one behaviour (e.g. frequent
severe tantrums but nothing else) can be coded 2A or 2Bif they result in significant disruption or social impair-ment.
Appendix 3: Sample Case Histories, with Formulations and Ratings
Case 1
Teresa is a nine-year-old girl of low average intelligence.She lives with both her parents and a sister two years youngerthan her. Her mother does not work outside the home. Herparents have a warm marriage with many shared interests.
By her mother's account Teresa has no eating or sleepingproblems. She has a marked fear of heights (which hasincreased over the last two years) and the dark. She will not goout into the garden at night and keeps a light on in her room atnight. On most school days she worries about being teased andabout her difficulties with two-handed activities—with theworries being particularly prominent when sport or sciencepracticals are on the timetable. According to her mother, theseworries result in distress during term time (so that she isnoticeably more relaxed and happier during holidays) but donot result in any avoidance of school. Teresa is mildly shy, andsometimes feels that people are against her. She gets on wellwith her sister though there are some negative interactions onmost days. There are no problems with disinhibition. Hermother described her as a "grumpy, unenthusiastic child whois difficult to motivate at times".
She is able to watch TV for over 30 min without restlessnessor fidgetiness. She can read for up to 15 min withoutrestlessness or fidgetiness. She can play atone or with othersfor over 30 min without restlessness or fidgetiness. There areno problems at meal times or with running away outside thehome.
There are mild grumbles at bedtime on most days. Hertempers are mild and infrequent. She can be cheeky to hermother but only rarely. She will generally stall when asked tocomply with a request on most days. There are no problemswith lying, stealing or destructiveness. Her aggressive out-bursts are minimal and relate to episodes of rough play withher sister. There are no problems with conduct outside thehome.
Teresa needed a little encouragement at the start ofpsychometric testing, but was happy to work once she feltcomfortable with the demands of the situation. During thepsychiatric assessment, she was very restless and fidgety butshe persisted well with tasks and was not distractible. Thoughshe was able to name friends at school, she often played aloneeither because her 'friends' were playing with someone else orbecause she found them too bossy. She had two good friendswho lived near her but did not go to her school. She used toworry about her parents because they were old and might die,but she had stopped worrying about that. She was a bit worriedabout her teeth, fearing that they might fall out because she didnot brush them well enough. She said she was scared of thedark and was not able to sleep without a light on at night. Shewas never seriously miserable.
The Rutter questionnaire (Rutter, 1967) completed by her
teacher reported definite problems with worries, fear of newsituations, fussiness and somatic complaints, plus possibleproblems with settling to tasks, misery, apathy, solitariness andbeing disliked by others. The Conners questionnaire (Conners,1969) reported excessive demands for teachers attention, quitea lot of inattentiveness and just a little fidgetiness, restlessness,poor concentration and disruptiveness.
Assessors' formulation of Case 1 Teresa's fears andworries do result, according to her mother, in some distressduring term time, and this is corroborated by the teacher'sreport of definite fears and worries. Given Teresa's ownaccount, however, it is not clear that the level of distresswarrants more than a 'dubious' rating. Her peer relationshipsal school are impaired but the cause is uncertain—-teasing andlack of friends may be due to her physical problems rather thanto her emotional problems or shyness. Teresa's account thatshe does have some good friends out of school suggests thather problems in school may reflect ostracism rather than a lackof social competence on Teresa's part. The restlessness duringthe psychiatric assessment and the teacher's report of possibleinattentiveness are not enough for any hyperactivity rating(particularly given her low average IQ).
Psychiatric disorder: assessors' r a t ing-1 ; independent rat-ing = 1.
Hyperactivity rating: assessors' rating = 0; independent rat-ing = 0.
ED rating: assessors" rating = I; independent rating = 1.CD rating: assessors' rating = 0; independent rating = 0.
Case 2
Sandra is a eight-year-old girl of average intelligence. Shelives with both parents and a sister two years older than her.Her parents have a good marriage. They sometimes deal withher rather differently, but there is no direct countermanding.
By her mother's account, there are no problems with eatingor sleeping. Sandra has many worries. Will the boat she is onsink? Will the train she is on crash? Will she be able to get offthe bus in time at the bus stop? Will she be able to keep upwith school work? Will she get lost in a crowd? On outings,she is keen to hold on to someone's hand at all times. Shesometimes worries about friendships at school, about teasing,and about not being very good at sport. When a smoke alarmwas first installed in her home, she lay awake much of thenight worried about fire. She is somewhat worried beforeseparations (e.g. when going to stay with grandparents) andtakes several anxious farewells before finally leaving. Afterseeing a young child bowled over by a dog on a lead, she wasvery frightened of dogs for a couple of weeks, running and

CASENESS RATINGS 379
clinging to her mother if a dog was anywhere in the vicinity.This concern was less prominent at the time of the interview,but she still ran to her mother if a dog came quite near. She isalso frightened of thunder, leaping into her mother's lap.Subsequent reassurance does not prevent her being equallyfrightened by the next thunderclap. Sandra has wanted to beable to cook things and she and her mother have purchased avariety of one-handed aids, but progress with cookery isimpeded because of her marked concerns about lightingmatches and using the gas stove. Anxieties sometimes interferewith her falling asleep, or cause her to wake with nightmares.Her mother also attributed frequent stomach aches to anxietyand reassurance-seeking. These various problems do notprevent Sandra leading a very full life, attending schoolregularly and engaging in a wide variety of after-schoolactivities, either alone or with other children. Sandra fairlyoften seems down and miserable—mildly so two or three timesa week, and more profoundly so once a week or less. It is noteasy to jolly her out of these moods but she does usuallyrespond if her mother sits and reads to her. Sandra has dailypositive interactions with her older sister, but also squabbleswith her most days. She is appropriately reserved withstrangers.
She can watch TV, read a book and play alone or withothers for up to 30 min without restlessness, but with moderatefidgetiness. There arc no problems at meal times or withrunning away outside the home.
She sometimes grumbles at bed-time. She is generallycompliant, but resists getting ready for school in the mornings(because it interrupts her games). She is slightly cheeky to hermother most days. There is some lying, mostly related to herapparent difficulty in distinguishing between pretend andreality—but she sometimes sticks to false accounts even whenchallenged. She has deliberately spoiled some of her sister'sthings in the past, but not recently. She does not have tempertantrums and had been mildly aggressive only three times inthe previous year. There were no conduct problems outside thehome.
She was an easy child to work with during psychometrictesting. During the psychiatric interview, she was slightlyfidgety but was not restless, impersistent or distractible. Shewas not obviously anxious at any time during the interview butwas clearly sad when describing bullying at school. She has
good friends at school, but she is teased more than mostchildren, and is also frequently pushed around and bossed byboys in the playground. She said that this .spoiled quite a lot ofher time at school, and made her feel like crying much of thetime. She would worry both at school and at night about whatthe boys were going to get up to. She sometimes worries atnight about her parents dying or becoming ill the next day.When asked directly, she said that she did sometimes haveepisodes of unprovoked anxiety without any focus, but shedoes not tell any one about these and they are not very severe.She is scared of the dark, so that she is very reluctant to go tosleep without a light on. She is also scared of dogs, so that shetries hiding behind her mother when a dog is coming along—but she would not avoid going to the park even if she knowsthat there will be dogs there. "Sometimes, I am afraid ofeagles, but I have not seen any". She is a bit scared ofescalators but goes on them provided someone holds her hand.She no longer goes on the top floor of a bus since a scare whenshe almost got separated from her father because of the delayin getting off after sitting upstairs. There were no feelings ofworthlessness or definite obsessive-compulsive symptoms.
A Rutter questionnaire (Rutter, 1967) completed by herteacher reported no definite problems but possible problemswith worries.
Assessors' formulation of Case 2 Sandra has manyworries and fears, though she mostly keeps these to herselfand they are not very evident to her teacher. She also describessignificant misery and she did seem sad when describingbullying at school. Her mother's account puts less weight onthe misery, and the teacher questionnaire did not report it at all.Overall, it does seem likely that anxiety and depression are acause of significant distress to Sandra even though they do notresult in significant social incapacity (even if she does lesscooking than she would otherwise want to and is unusuallyclingy when out).
Psychiatric disorder: assessors' rating - 2A; independentrating = 2A.
Hyperactivity rating: assessors' rating = 0; independent rat-ing = 0.
ED rating: assessors' rating = 2A; independent rating = 2A.
CD rating: assessors" rating = 0; independent rating = (1.