Embed Size (px)
Citation preview

RATIONALE OF OVERDENTURE
PROSTHESIS

CONTENTS INTRODUCTION HISTORY DEFINITION SYNONYMS TYPES OF OVERDENTURE INDICATIONS CONTRAINDICATIONS RATIONALE OF OVERDENTURE ADVANTAGES DISADVANTAGES DISCUSSION CONCLUSION

INTRODUCTION
• Restoration and rehabilitation of loss of teeth and associated structures to maintain alveolar ridge morphology and proprioceptive sense presents a challenge to the prosthodontists.
• Overdenture is a removable prosthesis whose denture base
covers one or more natural teeth or tooth roots
• Its use dates back over 100 years.
• With increasing stress on preventive measures in
prosthodontics, overdentures have evolved to the point
where it is now a feasible alternative to most treatment plan.

• Overdenture has made it possible to prevent the patient from being completely edentulous even when the few remaining teeth are badly worn out or periodontally compromised.
• In overdenture, retention and stability are enhanced and residual ridge resorption is much less as compared to that in a conventional complete denture.
• However, it also has some disadvantages. The abutments which are covered by the denture base are more prone to caries and periodontal disease , etc.

HISTORY OF OVERDENTURES
• 1856- Ledger makes a prosthesis representing over dentures.
• 1861- Atkinson publishes a paper on ‘plates covering fangs’.
• 1861- American Dental Conference in Connecticut increases awareness of the importance roots might have in supporting dentures.
• 1896- Essig describes a telescopic like coping in a textbook
• 1970’s- Overdentures assume importance in popular dental literature.
• 1909- William Hunter proposed focal sepsis theory in which he described as “a box of gold over a mass of sepsis”
• 1955- Brill summarized the ideas of using root canal treated abutments, with attachments, to retain partial or complete dentures placed over the teeth.

DIFINITION
• Overdenture is a removable partial denture or complete denture that covers and rests on one or more remaining natural teeth, the roots of natural teeth, and /or dental implants. (Gpt-8)

HYBRID DENTURE

TELESCOPIC DENTURE
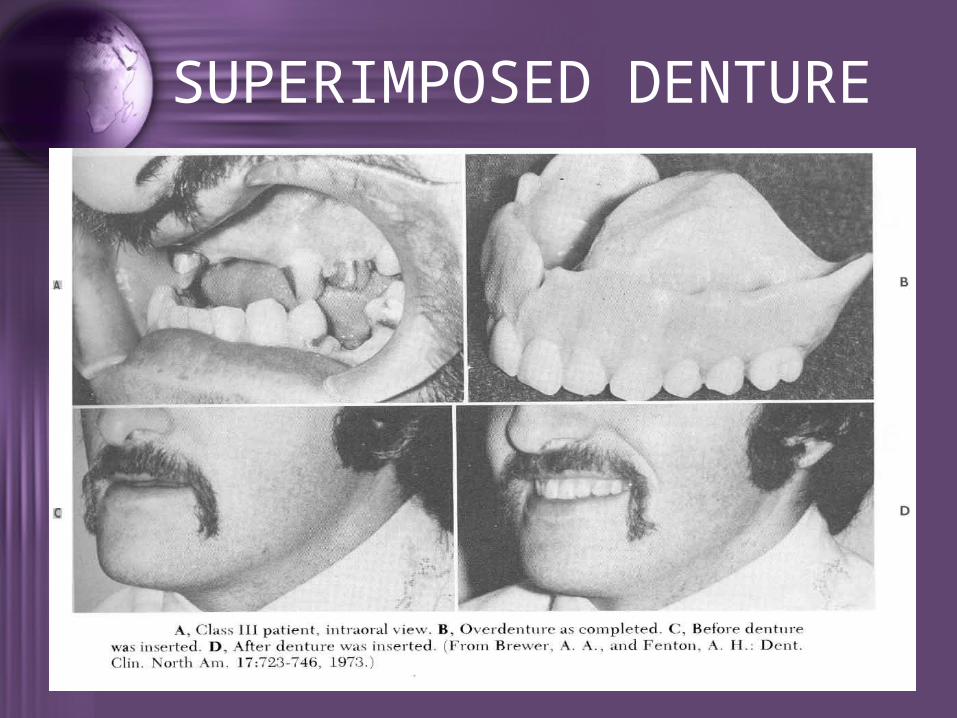
SUPERIMPOSED DENTURE

IMPLANT SUPPORTED OVERDENTURE

TYPES OF OVERDENTURE
• TRANSITIONAL OVERDENTURE
• TRAINING OVERDENTURE
• IMMEDIATE REPLACEMENT OVERDENTURE
• DIFINITIVE PROSTHESIS
TRANSITIONAL OVERDENTURE
• This particularly useful group has application when the patient is already wearing a partial denture. It consists of a modification of this partial denture to replace further lost teeth or to cover the roots of overdenture abutments once the teeth have been prepared.

TRAINING OVERDENTURE
• Strictly speaking, this is not an overdenture, but it do has many applications in overdenture techniques. It is commonly employed to replace hopeless posterior teeth once they have been removed. It serve as a replacement to allow the patient to accommodate to the replaced posterior teeth.

IMMEDIATE REPLACEMENT OVERDENTURE
• This is constructed before the last remaining teeth are extracted and the overdenture abutments prepared
DIFINITIVE PROSTHESIS
• This is usually constructed atleast 6 months following extraction of the last teeth and the preparation of the abutments. It should be planned to provide service for several years.
INDICATIONS
• Morphologically compromised dental arches.
• Patients with badly worn out teeth due to attrition.
• Presence of few remaining teeth.
• Patients with congenital defects like: Cleft palate, Oligodontia, Microdontia, Prognathic mandible.
• Patients with poor prognosis for complete denture.

• Patients with abnormal jaw size and position where orthognathic surgery is contraindicated.
• When the bone volume and anatomic obstacles do not enable to place the required number of implants for fixed prosthesis.
• Limited financial budget.
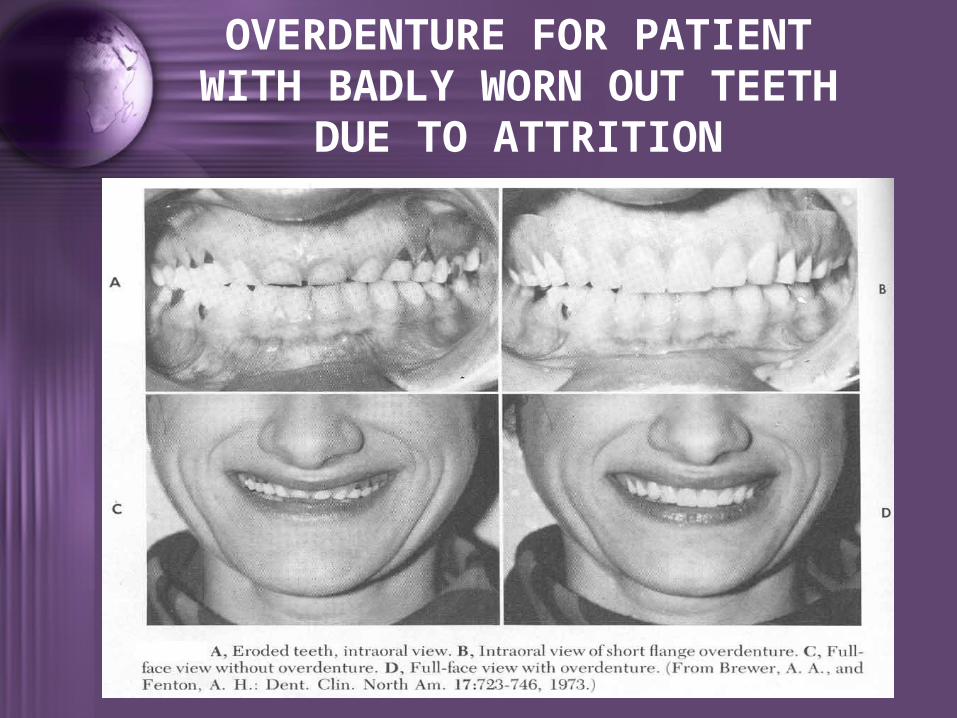
OVERDENTURE FOR PATIENT WITH BADLY WORN OUT TEETH
DUE TO ATTRITION

OVERDENTURE FOR PATIENT WITH OLIGODONTIA

OVERDENTURE FOR PATIENT WITH PROGNATHIC MANDIBLE-SUPERIMPOSED DENTURE

OVERDENTURE FOR PATIENT WITH ABNORMAL JAW SIZE

CONTRAINDICATIONS
• High caries index.• Poor oral hygiene.• Poor prognosis of abutment.• Uncontrolled metabolic diseases.• Where endodontics and periodontics
treatment cannot be performed satisfactorily.
• Reduced inter-arch space.

RATIONALE OF OVERDENTURE
• PSYCHOLOGICAL ADVANTAGE. For the partially edentulous patient, retention of teeth
provides great psychological comfort.
Retention of even a single root removes the patient’s ever present fear of being completely edentulous.
• PRESERVATION OF RESIDUAL ALVEOLAR RIDGE It has been shown by Tallgren that the bone loss around
mandibular natural teeth in patients with partial dentures was only 0.8mm, compared with a 6.6mm loss in those wearing complete dentures

Crum and Rooney have shown that with the retention of mandibular canines there is only 0.6mm ridge reduction in the anterior part of the mandible in patients with overdentures,whereas patients with complete dentures lost an average of 5mm.
This preservation of alveolar ridge occurrs because of the roots’ ability to express the compressive force of denture bearing into tensile force to the bone via the periodontal ligaments.
Occlusal forces generated during mastication are directed through the denture teeth and acrylic resin base to both abutment roots and the mucosa overlying the supporting residual ridge.

When abutment roots are properly contoured, this force is directed down their long axes through sharpeys’ fibers.
Excessive compressive force placed on the residual ridge by the prosthesis leads to compression of the mucosa against the bone and contributes to residual ridge reduction.The exact mechanism is not clearly known, but interference with venous drainage, increased accumulation of metabolites, and changes in calcium metabolism may all lead to a shift in bone homeostasis that favours osteoclastic activity over osteoblastic activity.
• INCREASED PATIENT’S MANIPULATIVE SKILLS IN HANDLING THE DENTURE.
The patient, although wearing a complete denture, retains that important sensitive ability to be aware of occlusal contact because of the proprioceptive impulse that has been preserved with the periodontal membrane along with the roots.
This enables the patient to controll the force of occlusion in very much the same manner as a person with natural teeth.

These factors greatly enhance the patient’s denture coordination and ability to control the denture in his/her physiologic environment.
Pacer and bowman found that the overdenture patient possessed more typical sensory functions, that is closer to natural dentitions than a conventional complete denture patient in discriminating between occlusal forces.
• PRESERVATION OF THE PROPRIOCEPTIVE IMPULSES.
In overdenture, as some teeth or roots are preserved, the proprioceptive impulse supplied by the periodontal membrane that surrounds the roots is preserved.
• IMPROVED TACTILE DISCRIMINATION.
Effective mastication which require tactile discrimination relies upon feedback.
The extraction of teeth result in loss of mechanoreceptors from associated periodontal ligaments.
Mericske stern has shown that the ability to perceive thin test foils placed between the artificial teeth of root supported overdentures was greater than those supported by implants.

• IMPROVED BASAL SUPPORT. This is because of the vertical stops provide by the
abutment roots.
• IMPROVED RETENTION. Retained teeth used in a removable overdenture can be
modified to provide varying types and degrees of retention. Some degree of retention can be obtained by merely
tapering a reduced clinical crown and thus providing frictional resistance.
When sufficient tooth structure remains, clinical crown can be prepared to receive cast copings so that added length and controlled taper will result in greater resistance to vertical displacement.
If remaining tooth structure is severely compromised, it may be possible to improve the coronal bulk with threaded pins and crown build up procedures.

• IMPROVED STABILITY. The vertical walls of the remaining roots will provide some
additional stabilization for the overlying prosthesis.
The greater the vertical space occupied by the root preparation, the greater the stabilization provided
.
• A SIMPLE APPROACH TO THE PROBLEM OF THE PATIENT.
In the past, patients with congenital defects, such as cleft palate, partial anodontia, microdontia, amelogenesis imperfecta, and so on, posed a rather detailed, lengthy, and expensive course of treatment. With the advent of overdenture, a reasonable, relatively fast, and inexpensive mode of treatment became possible.

• ESTHETIC CONSIDERATIONS. Partially edentulous arches may present with remaining
teeth that are spaced in such a manner that normal or esthetic arrangement of the teeth may be greatly enhanced if the offending teeth are endodontically treated, coronally amputated, and used as overdenture abutments.
An example of this could be a kennedy class iii maxillary edentulous arch in which a retained central incisor may be isolated, with other incisors being absent. The remaining incisor may be severely rotated, angled, or displaced mesially or distally to such an extent that replacement teeth cannot be esthetically arranged. A practical solution to this is to endodontically treat the central incisor, amputate the clinical coronal portion, and place a partial overdenture base over the retained tooth structure. Supplied teeth can then be arranged at will.

• HARMONY OF ARCH FORM. The construction of a complete denture for maxilla opposed by a
mandibular removable partial denture results in excessive resorption of bone that directly opposes the lower natural teeth. This is classically found on the anterior aspect of the maxillary arch when it has opposed lower anterior natural teeth.
This makes the maxillary arch no longer capable of supporting and retaining a complete denture.
This problem and others similar to it can be prevented by originally retaining some of the natural teeth on the arch and use them as abutments for an overdenture
ADVANTAGES
• Psychological benefits to the patient.• Preservation of alveolar bone.• Preservation of proprioceptive impulses.• Improved tactile discrimination.• Improved support, stability and retention.• Improved taste sensation.• Improved chewing capacity.• Reduced time and cost as compare to implants fixed
prosthesis.• Convertibility.

DISADVANTAGES
– Overdenture is bulkier than conventional complete denture.
– Overdenture is more susceptible to fracture as the denture base is trimmed very thin around the abutments.
– Abutments are more prone to dental caries and periodontal disease as they are covered by the denture.
• Caries-prone patients and patients with progressive periodontal diseases may be poor candidates for overdenture treatment.
• Contact between the denture base and the abutment , either by design or because of tooth eruption, can produce a fulcrum in the denture base where the contact occurs.
• It is more expensive than conventional complete denture.

CONCLUSION• Overdenture therapy constitute an essentially preventive
prosthodontic concept as it endeavors to preserve the few remaining teeth and supporting structures to maintain ridge contour and proprioception for enhanced sensory experience of the denture wearing patient, based on rational principles and proper clinical evidence.
• The prognosis of the overdenture prosthesis is influenced by numerous factors, including the selection of the patient, treatment planning, preparation of the mouth, execution of the prosthodontic therapy and also by maintenance therapy necessary to ensure a satisfactorily result.
• The preservation of alveolar bone around abutment teeth and in the adjoining area due to lowering of the compressive stresses by use of overdenture results in more stable and functionally superior retentive prosthesis.
CONCLUSIONThe rationale of overdenture therapy can be thoroughly summarized and after a proper evaluation of the literature published on the topic, it can be concluded that :-
• Overdenture therapy slows down residual ridge resorption around abutment teeth and also in adjoining tissues.
• Overdenture therapy reduces need for frequent relining of dentures.
• Overdentures are more stable and functionally more retentive.
• Patient satisfaction is superior to that of the conventional denture therapy.

BIBLIOGRAPHY1. Sheldon Winkler-Essentials of Complete Denture
Prosthodontics (2nd edition), 384-402, AITBS (India).
2. Harold W. Preiskel -Overdentures Made Easy- A Guide to Implant and Root Supported Prostheses, 11-13, Quintessence Publishing Co Ltd, 1996.
3. Dental Update-Implant Complications and failures: C. J. Watson, D. Tinsley and S. Sharma, June, 2001.
4. Dental Update- Mandibular Implant-retained Overdenture with Magnets: A Case Report by Angeline S.Y. Tan and A. Damien Walmsley, March, 2004.
5. The Journal of Prosthetic dentistry- Treatment outcomes with implant-supported overdentures: Clinical considerations-Regina Mericske-Stern, January, 1998, Vol-79.
6. The Journal of Indian Prosthodontic Society- Clinical assessment of the overdenture therapy- R.C. Dhir, December 2005, Vol-5, Issue 4

THANK YOU



![DENT...Porcelain and cast restorations; prosthodontics (fixed partial dentures [bridges], removable partial dentures, and complete dentures); implants; etc. CLASS IV: ORTHODONTICS](https://img.pdfslide.net/doc/110x75/5ed5609cf98bb3308d2fa371/dent-porcelain-and-cast-restorations-prosthodontics-fixed-partial-dentures.jpg)

























