Embed Size (px)
Citation preview

THE RED BLOOD CELL:
STRUCTURE AND
FUNCTION

Blood:Ave 70 kg 5 L of bld (7% by vol)

Erythrocytes
Structurally the simplest
cell in the body
Basic function: Create
& maintain an
environment for
physical integrity &
functionality of Hgb

Erythropoiesis
(Kinetics)

Substances necessary for RBC production:
Metals (iron, cobalt,
manganese)
Vitamins (B12, B6, C,
E, folate, riboflavin,
pantothenic, thiamine)
Amino acids
Regulatory substances:
Erythropoietin
Thyroid hormones
Androgens
Erythroid hyperplasia of BM in anemia

Reduced production
Deficiency of hematinics
Iron deficiency
Folate & B12 deficiency
Dyserythropoiesis
ACD
MDS
Sideroblastic a
Marrow infiltration
Failure of production
Aplastic anemia
Pure red cell aplasia
Increased destruction
Hemolytic anemia
Intrinsic causes
Membrane defects
Enzymopathy
Hemoglobinopathy
Extrinsic causes
Immune reactions
Microangiopathic
Parasitic
Hypersplenism
Bleeding
Classification of anemia

Anemia due to failure of
production: Aplastic anemia

Causes Of Aplastic Anemia
Idiopathic (70 % or >)
Inherited:
Fanconi anemia
Familial aplastic anemia
Dyskeratosis congenita
Shwachman Diamond Syndrome
Dubowitz syndrome

Causes Of Aplastic Anemia
Acquired:
Secondary
Drugs 6 –mecaptopurine
Methotrexate
Cyclophosphamide
Chloremphenicol
Chemicals: insecticides
Toxin (benzene ,carbon tetrachloride)
Irradiation
Infection: Viral hepatitis; HIV; IM; CMV
MDS

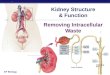
Aplastic anemia: hypocellular bone marrow is largely devoid
of hematopoietic cells; often only fat cells, fibrous stroma,
Aplastic anemia

CAUSES
DEPRESSION OR CESSATION OF ACTIVITY OF
ALL BLOOD PRODUCING ELEMENT
DAMAGE TO STEM CELL
LEUKOPENIA
THROMBOCYTOPENIA
DECREASE IN FORMATION OF RBC
PANCYTOPENIA
REPEATED
INFECTION;
FREQUENT
SICK DAY
BLEEDING
TENDENCY AEB
ECCHYMOSIS,
PURPURA,
PETICHIAE,
BLEEDING FROM NOSE,
MOUTH,
VAGINA, RECTUM
PALLOR OF SKIN & MUCOUS
MEMBRANE, CYANOSIS
APLASTIC ANEMIA

Aplastic Anemia: Clinical Features
Anemia: pallor, easy fatigability, weakness, loss of appetite
Thrombocytopenia: petechiae, easy bruising, severe nosebleeds, bleeding into GIT & renal tract
Leukopenia: increased susceptibility to infections & oral ulcer
Hepatosplenomegaly & LAD do not occur; their presence suggest underlying leukemia
Hyperplastic gingivitis
Special features
Skin: Hyperpigmentation, café –au-lait spots, erythematous rash
Head: Microcephaly, micro-ophthalmia
Mouth: cleft lip, leukoplakia
General: small stature

Erythrocytes: Normal mature RBC
Biconcave disc
Approximatly 8 um in
dia
2.5 um thick at the
periphery
1.0 um thick at center
Contains 27- 34 pg (10-
12 g) of hgb (about
95% of dry wt of RBC)

Areas of RBC metabolism
crucial for RBC survival &
function
RBC membrane
RBC metabolic pathways
Hemoglobin structure & function

RBC MEMBRANE:
Hereditary Membrane Dse.
Hereditary Spherocytosis
Hereditary Ovalocytosis / Elliptocytosis
Hereditary Stomatocytosis

RBC MEMBRANE:
3 Major Structural Proteins
Semi-permeable bilayer of
lipids (including cholesterol)
& proteins
Deformable to pass through
microvessels & permeable
to allow H2O & electrolytes
to exchange (inc surface
area)
Major protein is spectrin Cytoskeletal Proteins: Maintain
RBC Shape, Strength, Flexibility

Case

Hereditary Spherocytosis
Autosomal Dominant -
Most Common
Autosomal Recessive -
More Severe
MC in Northern
European ancestry
A spectrin def w/
principal defect in
abnormality of ankyrin
Vertical stabilization
defect of phospholipid
bilayer spectrin -
phospholipid bilayer
separates
Portions PL bilayer
forms vesicles (lost)
decreased surface
area spherocytosis

Hereditary Spherocytosis
Mutation of Ankyrin Gene
(Most Common Defect)
Abnormal Ankyrin Protein
Deficiency of Spectrin
Assembly

Hereditary Spherocytosis
Defects may be in:
Actin - spectrin - band 3 complex
Spectrin - 4.1 -glycophorin complex
Connection between bilayer & spectrin

Hereditary Spherocytosis: S/S:
Waxing / waning anemia, jaundice (hemolysis
accelerated by infection)
Splenomegaly (hyperplasia secondary to
increased workload), pigmented gallstones
(hx cholecystectomy), ankle ulcers
Family hx: (AD 1: 5000 people of European
descent)

Hereditary Spherocytosis Lab Dx:
PBS: Moderate Anemia;
Spherocytes; Reticulocytes
(polychromatophilia)
Inc retic ct, inc LDH, inc B1,
inc EOFT
Normal MCH w/ an inc
MCHC
BM - Erythroid Hyperplasia
Coomb’s Test - Negative
Inc Autohemolysis Test
corrected by glucose

Hereditary Spherocytosis
Tx: folate replacement, splenectomy in some
circumstances
Pearl: Parvovirus B19 infection in patients w/
hemolytic anemias in general aplastic crisis

Case
14 mon old African-
American child
presents w/ mild
anemia; Hx / PDx
obtained & when
reviewed showed these
cells
What are they?

Hereditary elliptocytosis &
Hereditary pyropoikilocytosis
Defects in horizontal
junctions:
Between a- & b-
spectrin dimers or
Between spectrin, actin
& band 4.1
RBC cytoskeleton loose
structural strength &
lateral integrity

Hereditary elliptocytosis
Autosomal dominant
Structural abnormality of spectrin or def of
RBC membrane protein 4.1
W/o anemia & usually w/o splenomegaly &
only mild hemolysis; Most patients
asymptomatic
EV hemolysis, thus splenectomy corrects
hemolysis, but not the RBC membrane defect

Hereditary elliptocytosis
PBS: large #s of elliptocytes &/or ovalocytes
# of elliptocytes does not correlate w/ severity of hemolysis
EOFT is usually normal
Reticulocytes mild inc (<5%)
Haptoglobin levels low

Hereditary pyropoikilocytosis
Rare AR
Severe hemolysis, bizarre poikilocytosis & RBC fragmentation (hallmarks)
Structural abnormality of spectrin, RBCs fragment when heated (45°C)
Normal RBCs fragment at 49°C

Case
Membrane permeability
defect in
stomatocytosis

Biochemical changes that can cause shape
change in RBC
Accumulation of cholesterol causes
increased membrane
Target cell
Acanthocyte
Decreased spectrin causes decreased
membrane
Spherocyte
Bite cell

RBC Metabolic Pathways
Essential for O2 transport & maintaining
physical characteristics of RBC


Red cell metabolic pathways
Generates 90% of energy
needs from Glucose 2
ATP molecules (energy)
90-95% of intracellular
glucose thru free-energy
diffusion
RBCs have no glycogen
Glucose (Na-K ATPase
pump & Ca-Mg ATPase
pump affected in PK Def

Case
5 y/o African-American
boy recently presented
w/ fever. Prescribed
Bactrim for presumed
otitis media. Brought
back in by mom due to
increased fatigue &
PBS showed

Red cell metabolic pathways
Metabolizes 5-10% of glucose
Protects RBC from oxidative injury
G6PD is rate-limiting enzyme
G6PD also produces NADPH (keeps glutathione reduced)
Glutathione protects via break down of H2O2 H2O + O
Most common defect is G-6PD def

G6PD Pathophysiology
Defect in HMP
G6PD def dec antioxidant GSHRBCs sensitive to oxidant stressesoxidized hgb (Heinz bodies) Macrophages of RES phagocytose bits of RBC membrane w/ underlying precipitated hgbpoikilocyte hemolysis

G6PD Pathophysiology
Actual def not due to
absence of enzyme,
but defective protein
folding protein w/
decrease half-life
later stages of RBCs
life (> 20 days),
functional levels of
enzyme decline

G6PD Pathophysiology
Mediterranean type:
Asso w/ fava bean
ingestion
More severe hemolysis
because all RBCs have
dec G6PD activity due
to dec synthesis &
stability
African American type:
Asso w/ intermittent
hemolysis since the
older RBCs have dec
levels of G6PD &
usually occurs in
response to oxidative
states (infections)

G6PD Def: Clin Dx
Jaundice in 1st 24 hrs of life (pathologic
jaundice)
X-linked common in African Americans &
Mediteraneans
Acute self-limited IV hemolytic a
Oxidative stress: infection, medication, fava
beans

G6PD Deficiency
Episodic hemolytic a
triggered by oxidant stress
(drugs, infection)
X-linked -10 – 14% males of
African descent carry an
unstable A variant of G6PD
More severe, chronic form
seen in men of
Mediterranean descent
(think fava beans in
Mediterranean pt)

G6PD Deficiency
PBS: Bite cells & blister cells
Dx: PBS, G6PD level, Heinz body prep
G6PD levels may be normal in acute setting due to selective removal of older RBCs w/ lower baseline G6PD levels
Tx: Get rid of offending oxidant stress (drug, infection)
Important drugs to know that may precipitate hemolysis: SULFA, anti-malarial drugs, dapsone, Vit K, fava beans

G6PD Deficiency
> 400 Variants
X Linked, M > F
African Americans (Males 10%)
Mediterranean Grps (inc severity)
Asymptomatic Unless Oxidative Stress
(Therapeutic Drugs, Fava Beans)
Denatured Hgb Precipitates RBCs
Removed by Spleen

G-6-PD def
> 200 M people (Mediterranean, West
African, Mid-East & SEA) due to chronic
hemolysis
Blacks often have an episodic variant in w/c
oxidant cmpds (antimalarials, sulfonamides,
or infections) cause hemolysis
Women heterozygotes (half the normal
amount of RBC) G6PD show increased
resistance to P falciparum

G-6-PD def:
Stressors of G6PD System
Antimalarials
Sulfonamides
Nitrofurans
Phenacetin
Synthetic vit K
Naphthalene (moth balls)
Fava beans
Infection
Diabetic ketoacidosis

Red cell metabolic pathways
Maintains iron in the
ferrous (Fe2) state
In the absence of the
enzyme (methgb
reductase), methgb
accumulates & it cannot
carry O2

Red cell metabolic pathways
Leubering-Rapaport
shunt
Allows RBC to regulate
O2 transport during
conditions of hypoxia or
acid-base imbalance
Permits accumulation
of 2,3-DPG essential
for maintaining normal
O2 tension


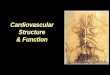
Hb-O2 Dissociation Curve
Sigmoid Shape
F8 Histidine & Porpyrin Ring
Alpha-Beta Dimer
Cooperative Binding

OxyHgb Dissociation Curve


CO2 Transportation

Breakdown of the RBC
Toward the end of 120 day life span, 1% of
RBC’s per day
Membrane becomes less flexible
Concentration of cellular hemoglobin increases
Enzyme activity (esp glycolysis) diminishes

Erthrocyte Destruction
Extravascular Hemolysis (major- 90% via RES)
Intravascular Hemolysis (minor- 5-10%)

Extravascular Hemolysis

Intravascular Hemolysis

References
Harmening, D.H., et al., Clinical hematology and fundamental of hemostasis, 3rd Ed, F.A.
Davis Company, Philadelphia, 1997.
McKenzie, S.B., et al., Text book of hematology, 2nd Ed, Williams & Wilkins, A
Waverly Company, Baltimore,1995.