Embed Size (px)
Citation preview
RCT����������
����2018/01/09���������ICU
���
•��RCT�• CONSORT����• CONSORT�� Introduction• CONSORT�� Method• RCT�•��

•��RCT�• CONSORT����• CONSORT�� Introduction• CONSORT�� Method• RCT�•��
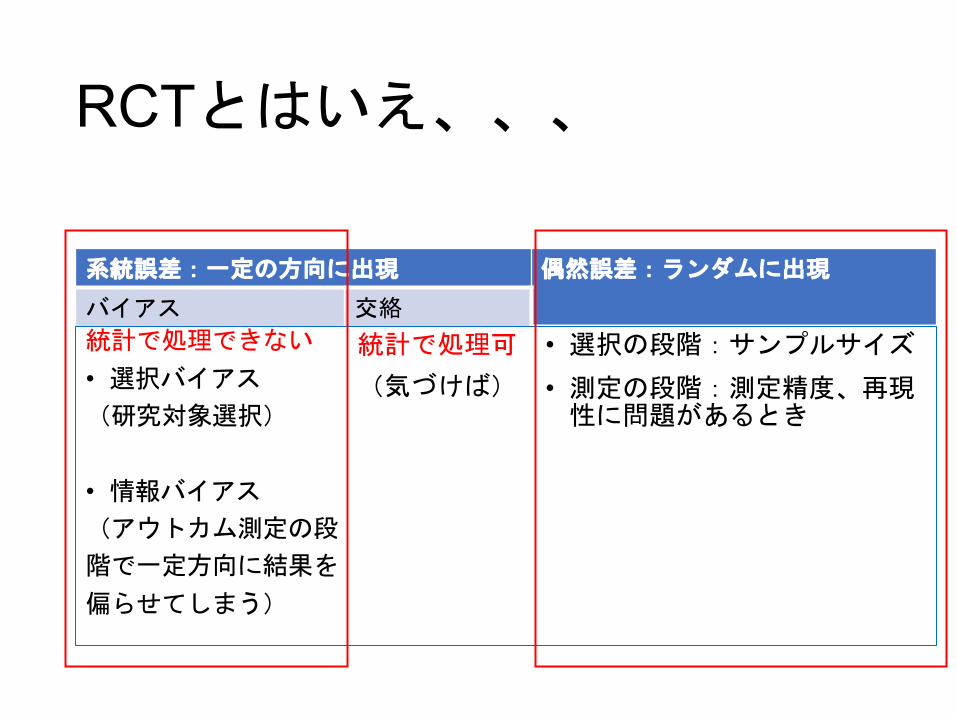
�������������
↓
�/��� ����
�����������
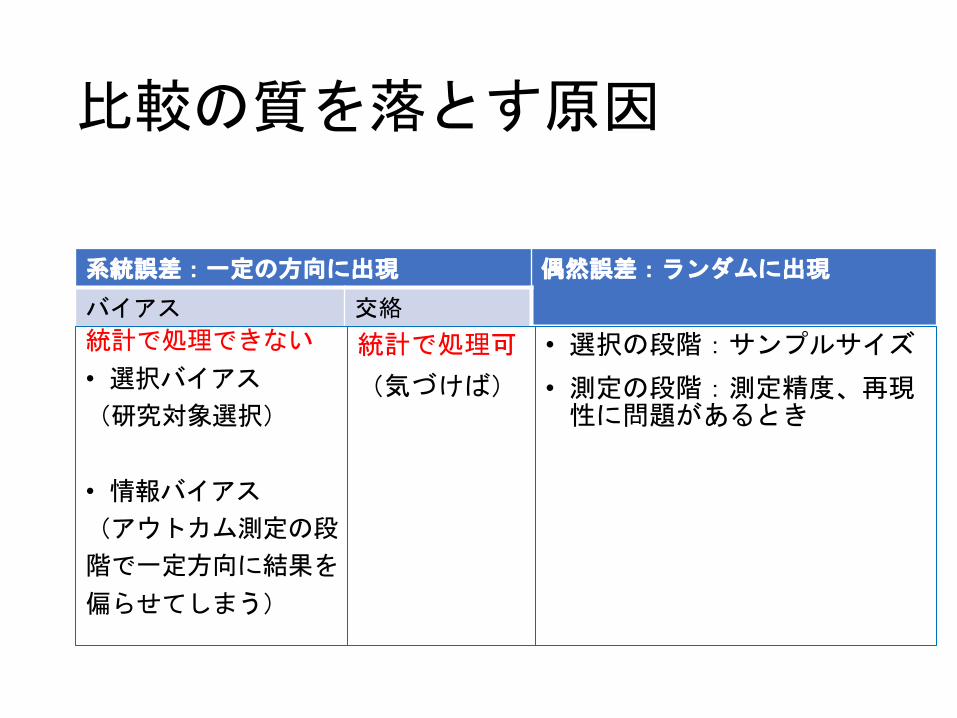
=O�N�J�-1
FIL5U&3�:/�,A )@L5U#%�"�,A
��� 'H
IK +B.
S>���T
IK +B ���
• P9 ���SCD4MP9T
• 82 ���S����"?3�<
Q &3:/�G;�
(�����T
• P9�<QU�%!$���• ?3�<QU?3E6�*A7�0R�����

=O�N�J�-1
FIL5U&3�:/�,A )@L5U#%�"�,A
��� 'H
IK +B.
S>���T
IK +B ���
• P9 ���SCD4MP9T
• 82 ���S����"?3�<
Q &3:/�G;�
(�����T
• P9�<QU�%!$���• ?3�<QU?3E6�*A7�0R�����
���
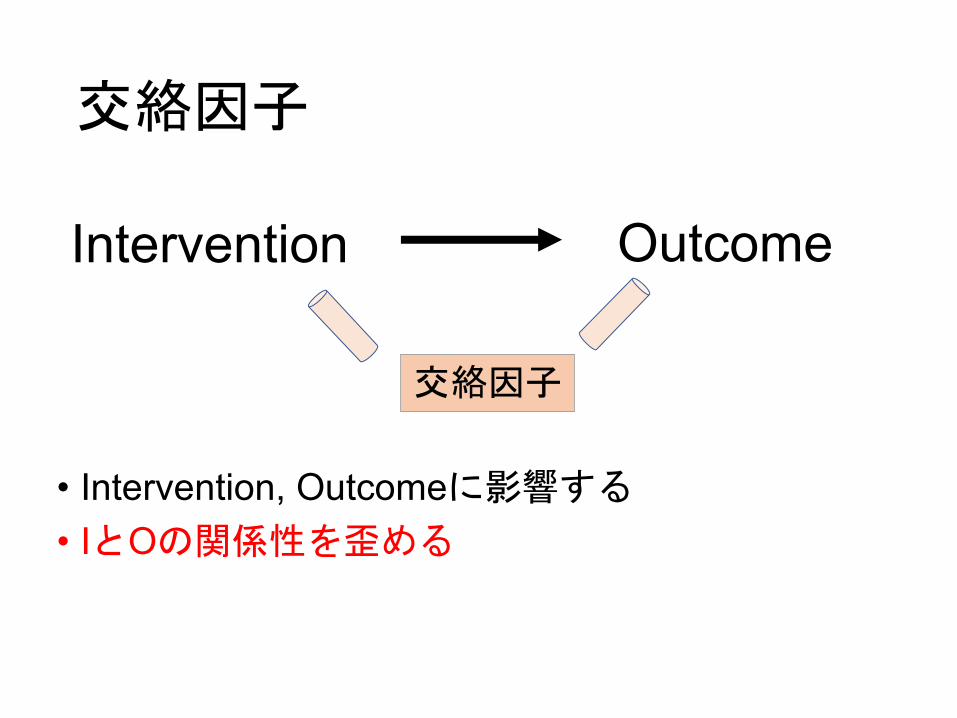
Intervention
���
Outcome
• Intervention, Outcome�����• I�O�� ����
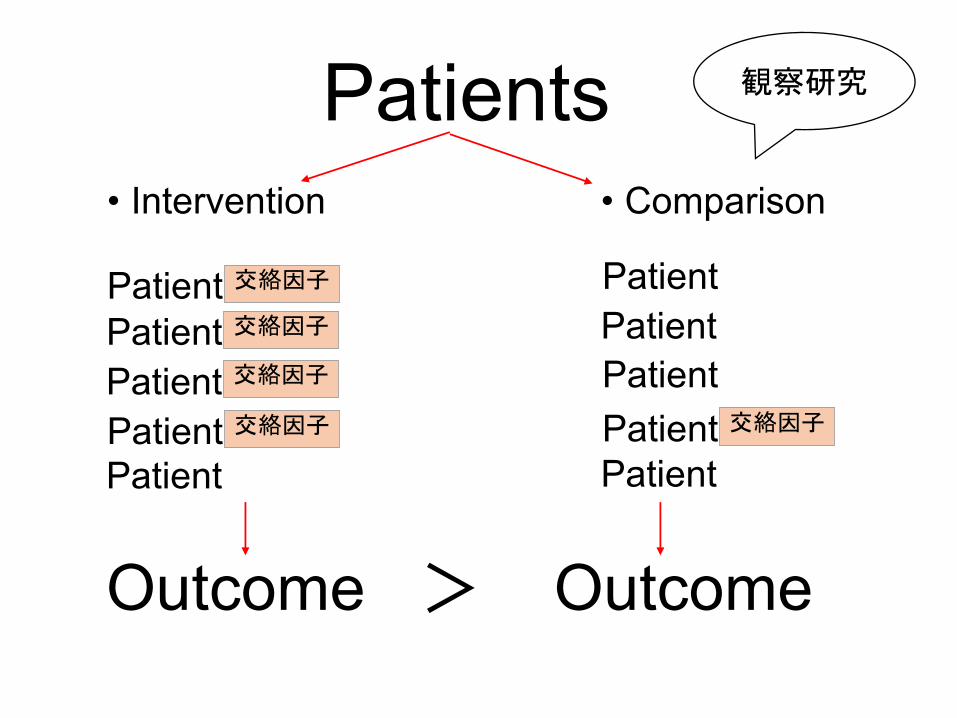
• Intervention • Comparison
Patients
PatientPatientPatientPatient ����
Patient ����Patient ����
Patient ����Patient ����PatientPatient
Outcome Outcome
����

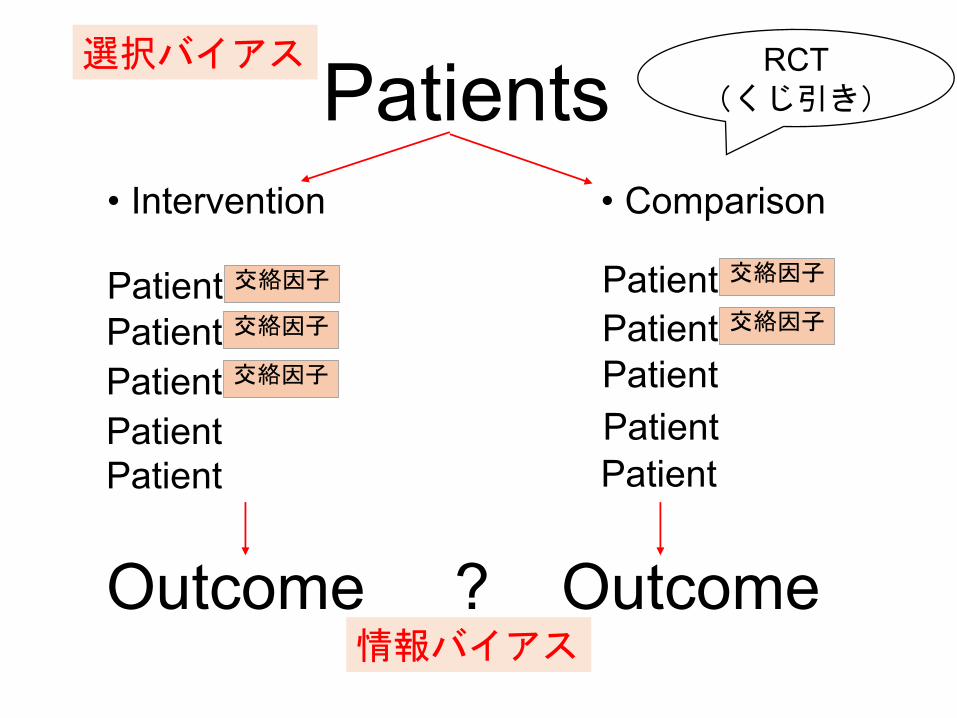
• Intervention • Comparison
Patients
PatientPatientPatient
Patient ����Patient ����Patient ����
Patient ����Patient ����
PatientPatient
Outcome ? Outcome
RCT����

#%�"-?PMU
HKN5X&2�;/�,C )BN5X#%�"�,C
��� 'J
KL�+D.
V@��W
KL�+D����
• Q: ���VEF3OQ:W
• 91 ���V����"A2�>
R�&2;/�I=�
(�����W
• Q:�>RX�%!$���• A2�>RXA2G6�*C8�0T��� �
'J�7S�<4����
• Intervention • Comparison
Patients
PatientPatientPatient
Patient ���Patient ���Patient ���
Patient ���Patient ���
PatientPatient
Outcome ? Outcome
RCT������
������
����
RCT�������
DGI4P'2�9/�-? *>I4P$&�#�-?
!��� (F
GH ,@.
N<���O
GH ,@ ���
• K8!���NAB3JK8O
• 71!���N�� �#=2�;
L '29/�E:�
)����O
• K8�;LP�&"%���• =2�;LP=2C5�+?6�0M�����

N Engl J Med 2017;377:465-75.
�����
�����
•��RCT�• CONSORT����• CONSORT�� Introduction• CONSORT�� Method• RCT�•��
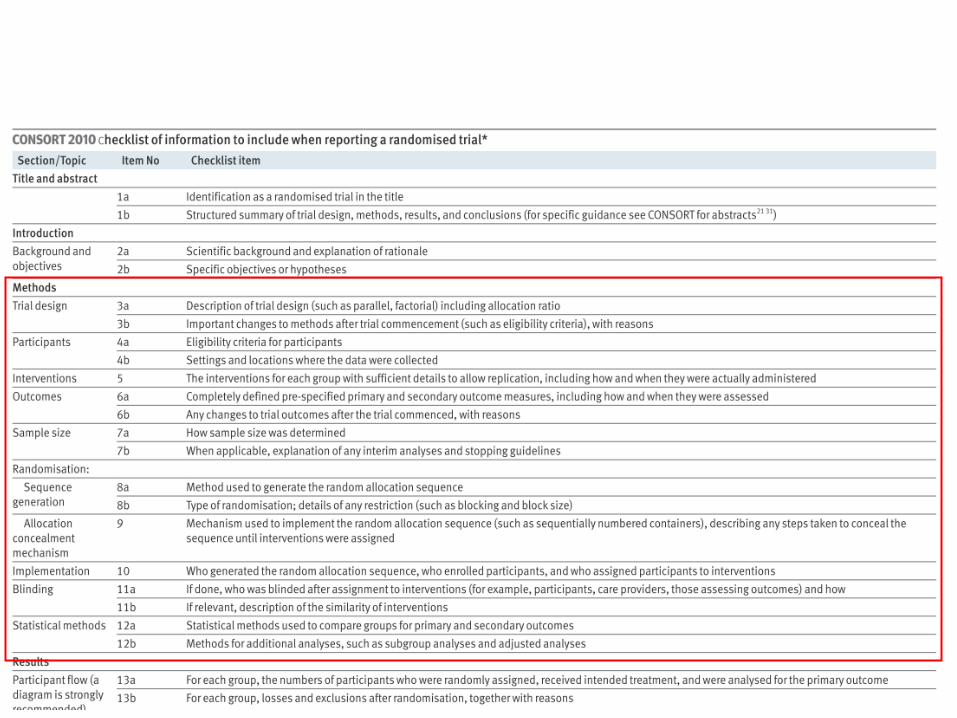
CONSORT (/�• 1996*�#6CONSORT(/�D7
Consolidated Standards of Reporting Trials: >+@I'%�F��<$&3
• 2001*-?↓↓ )� @I;1��C"
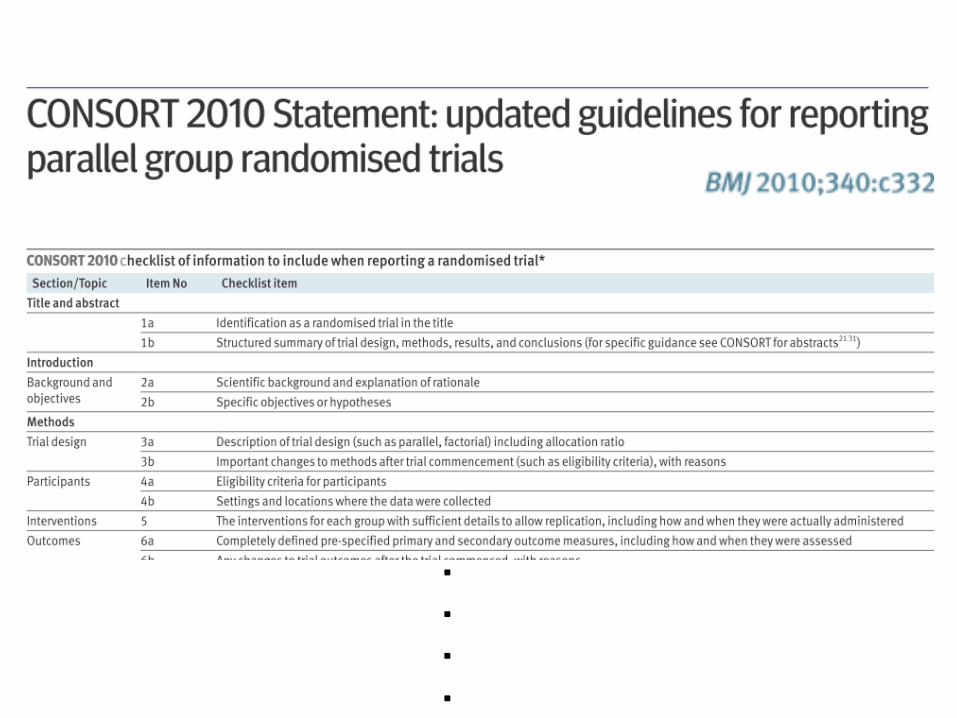
↓CONSORT2010�D7• C"�'% .2�B��� • �2=ERCT�54�,����• 25H8 ��������������• 9: .2A�������0!G &3
�
�
�
�
�
�
�

•��RCT�• CONSORT����• CONSORT�� Introduction• CONSORT�� Method• RCT�•��


����Introduction
�����
•���������rationale ����•���������hypothesis �
• Clinical Question↓
• Research Question�PICO �� ���↓
• Intervention vs. Comparison �� ����

��RQFINER����
• Feasible �����• Interesting ����• Novel������• Ethical ���• Relevant�����

������� ���OK ?• Feasible �����• Interesting ����• Novel������• Ethical����• Relevant���!
• RCTs are one of the possible experiments.
��
Premise��
Hypothesis��
Outcome

• RCTs are one of the possible experiments.
�����
���
��
Premise�
Hypothesis�
Outcome
• RCTs are one of the possible experiments.
��
��
Premise��
Hypothesis��
Outcome
Many other trials, in our opinion,failed either because ,,,,
• Wrong premises
• Premises that were too vague and generic.If too generic, the heterogeneity of thepopulation is an unavoidable consequence.

����� vs. �����• The trialists spent a lot of effort in improving their internal validity, by increasing the numberof rules and caveats to avoid possible biases in the conduct of the trials.
• This obviously makes the results valid only for the restricted patient population enrolled in the study and the generalization of the results(the external validity) is problematic.
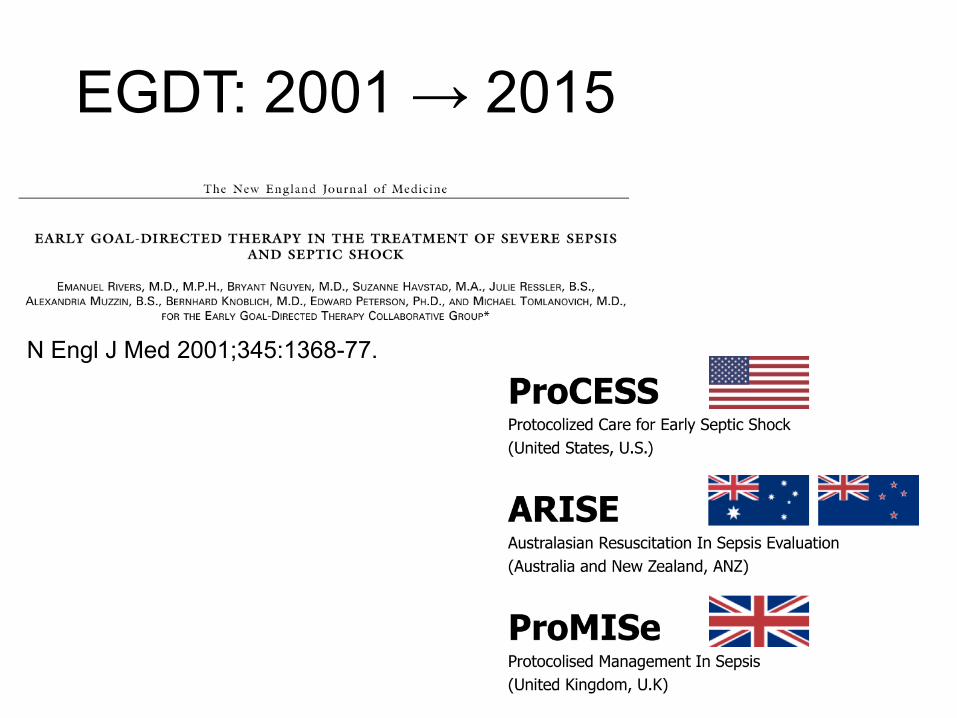
EGDT: 2001 → 2015
N Engl J Med 2001;345:1368-77.
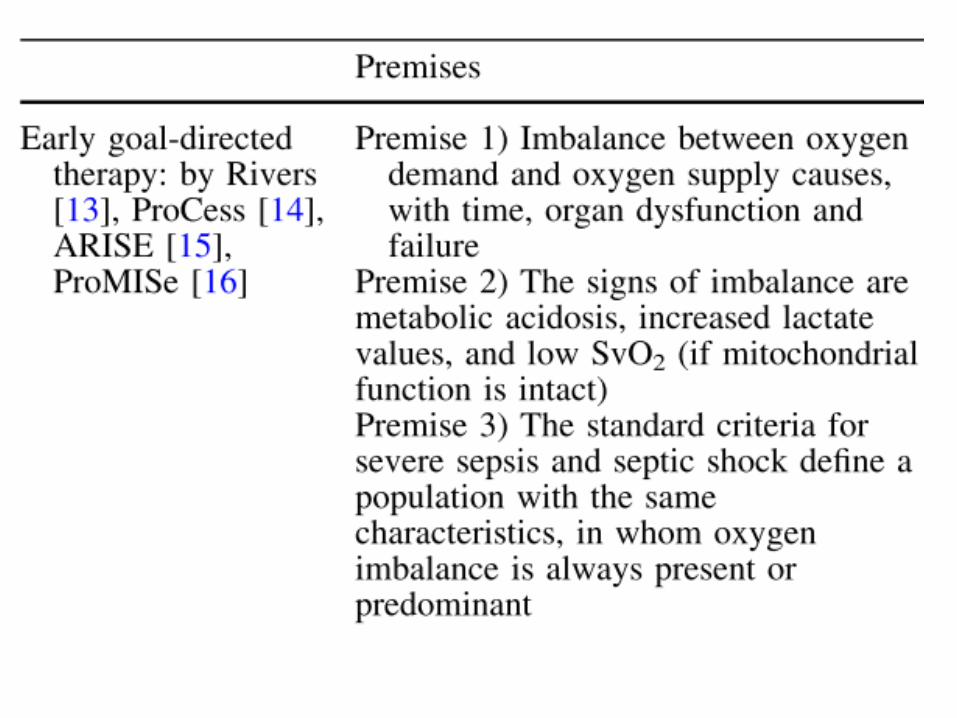

�� Hypothesis
• Severe sepsis, septic shock
↓ ��CVP�ABP�SvO2
•���������� �����

Outcome
N Engl J Med 2001;345:1368-77.
○
×××

?
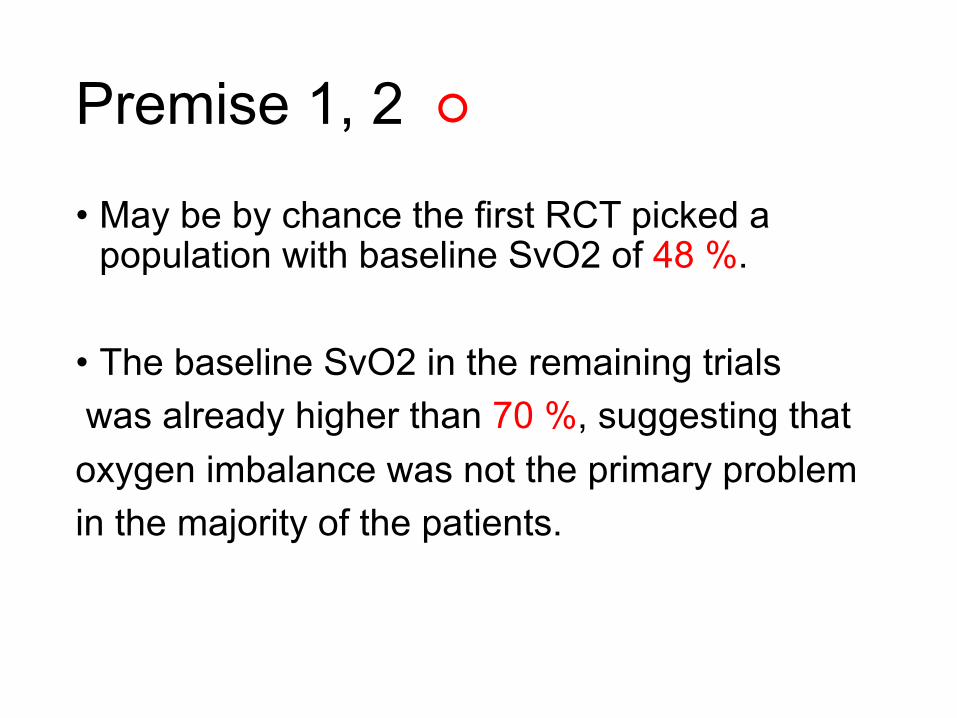
Premise 1, 2 ○
• May be by chance the first RCT picked a population with baseline SvO2 of 48 %.
• The baseline SvO2 in the remaining trialswas already higher than 70 %, suggesting that oxygen imbalance was not the primary problem in the majority of the patients.

?

Premise 3 Too generic and wrong

The pendulum effect• )�/����4��%�2�.0�!$����
• Single center→Multi center�&#��(���-+• EGDT65�.0����• %-�.0�������3�*,�'"����1)���� ��7����
Crit Care Med 2010; 38[Suppl.]:S534–S538

• Truly negative trials are valuable because they prevent the use of interventions that are either costly but nonbeneficial or even harmful (e.g.,intensive insulin therapy and hydroxyethyl starch).
• Understanding an evidence base requires the ability to distinguish among these reasons so as to differentiate trials that are truly negative from those that may be falsely negative.
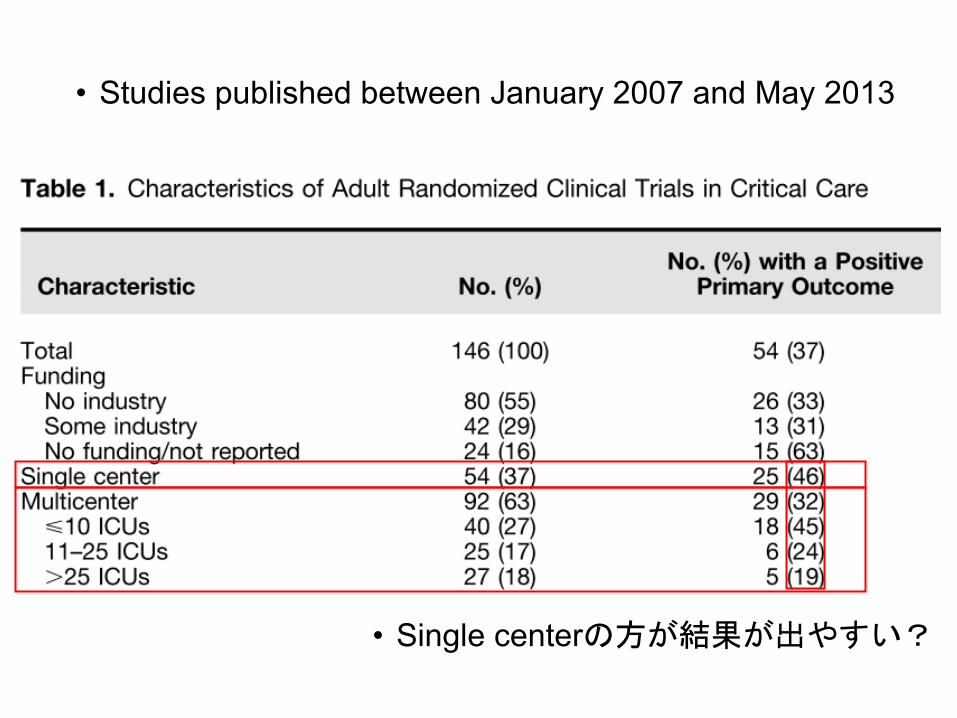
• Studies published between January 2007 and May 2013
• Single center���������

•��RCT�• CONSORT����• CONSORT�� Introduction• CONSORT�� Method• RCT�•��

'- ���
•'- ����&(.�$#,0%�����/�������
•'-+�������*%���.)�� eligibility criteria ��/���!"�

����Participant�
•���������eligibility criteria�
• ���������������
Was the right group of patients not identified?• ���" �� ���$�AMI�����%• �! ������������ICU�� �#�
Why have so many RCTs “failed?”
Crit Care Med 2010; 38[Suppl.]:S534–S538
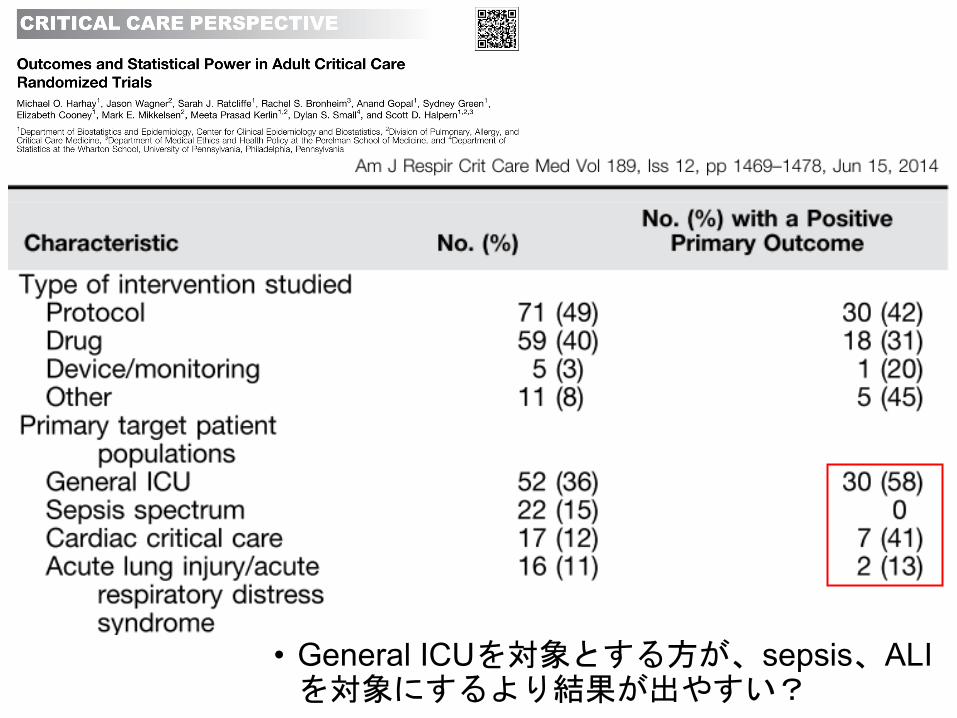
• General ICU� ������sepsis�ALI� ������������

High Exclusion Rates Lead to Limited Clinical Applicability
With such tight exclusion criteria limiting enrollment,,,,
• How can the patient population that is actually studied really be representative of the entire population initially considered eligible?
• How can the results be applicable to the general ICU population?
Crit Care Med 2010; 38[Suppl.]:S534–S538

TRICC study• Just 13% of 6451
patients screened were randomized.
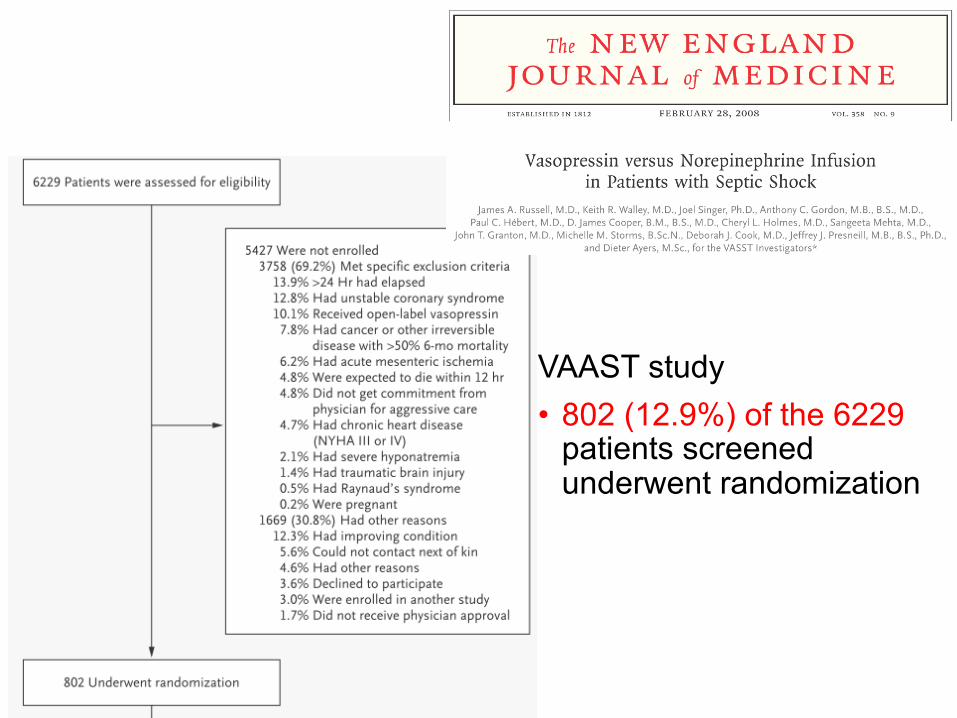
VAAST study• 802 (12.9%) of the 6229
patients screened underwent randomization

����������
• 1679 (84%) of 2011 patients were randomized.
N Engl J Med 2010;362:779-89.
�� Intervention!
•����������������•����������������� �
Were the interventions ineffective?�� �������� ��������
��
truly negative�������� ���������OK
Why have so many RCTs “failed?”
Crit Care Med 2010; 38[Suppl.]:S534–S538

Was it a question of severity?• 2*"!/�1�)+�( U shape���5)+�3�������� or ���4�� ���6
Is the timing of interventions correct?�%',*�&',*)+�(�0��-$��
�#�. ��
����7%',*8&',* Shock 2007; 28:636–643ARDS7%',*≑&',* Chest 2010; 137:81–87
Why have so many RCTs “failed?”
Crit Care Med 2010; 38[Suppl.]:S534–S538
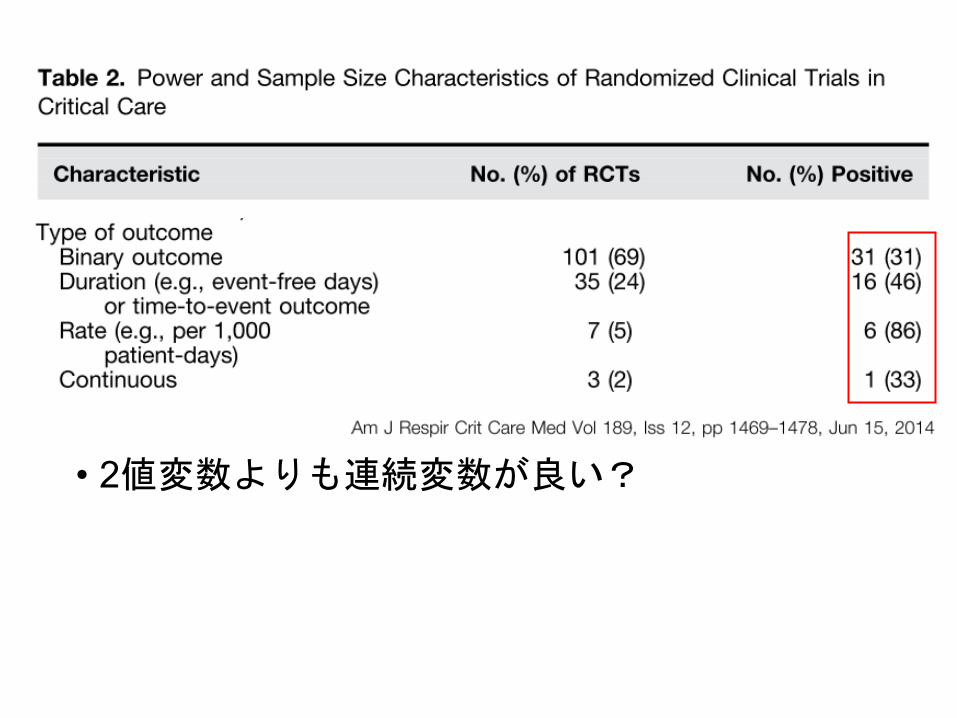
�����1Outcome2
•���$���!)��*����+��#'�����,�/(�������,������� �
•-0.� ��������"��%&�

G-;VSample sizeW
•�����JAG-;�D�����•*RN@�*B6E�Q>�
�*RN@
• I→?1*B�:→F1*B�=�0<��• N@�$ &("�5;�D���• 5;�7�����α!')�U��+�4T
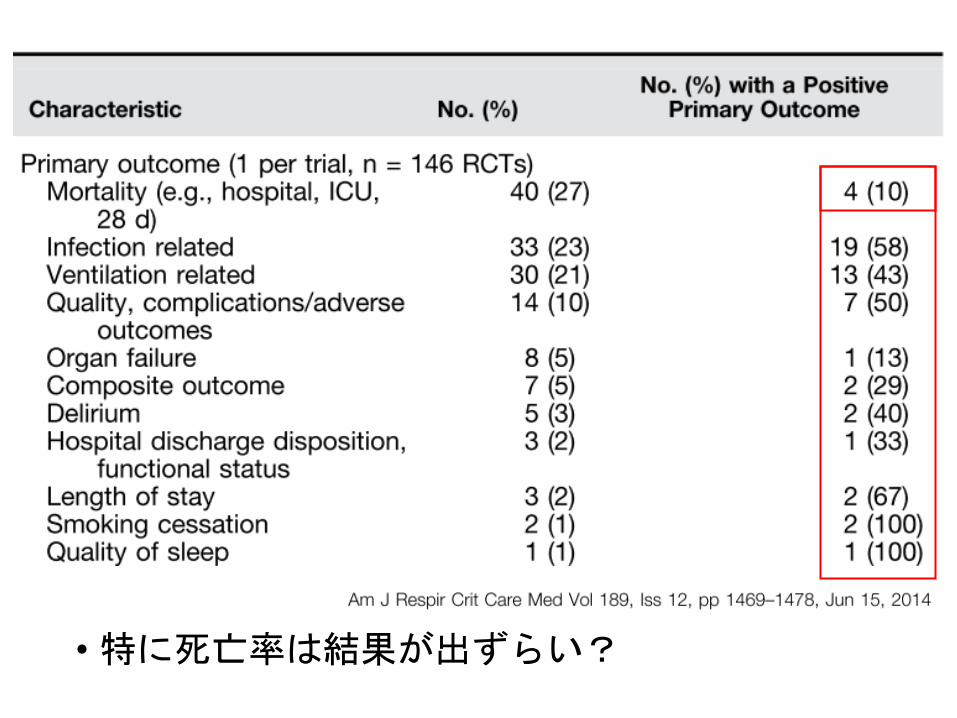
→=�CS�*RN@�������3 ��p.�P9���28H,/�KL%# (�MO�
Were the end points wrong?
• )�: 3'&�*0$7��9=:,�� ����;
• ��%"<��� !1��#��5.(�-+��9
• ��/<�4�8��
Was the power inadequate?
• �������62����
Why have so many RCTs “failed?”
Crit Care Med 2010; 38[Suppl.]:S534–S538
•����� ������
• 2������������

34��� ������������

47���������� �����������
(��10!(Allocation concealment) •���� (�2-�&)�,����+*4-"��'%��5�#/� ��.����� (�2-�10� �������
� �������$3
�����
•����allocation ����������•���� � : ����������,�������
• +9����&�$�(:)3
• ��������&�$� �ABAB AABB BABA ,,,,,,������ !:)3
:=�#3 +;�<����>��������.���
concealment�0, 72
• /'����&�$���������.���
58�"1*-�/%'�/������'
�����'�46
• �!��$!#� 2�+�-( �2�+�������
[< �2�+��
)/�BI�CK���
�$�!�#�>U�P�60��!��$G�EW
:F��2�+��D� �� �9T
��!��$,_AM��"����QZ�=?
• &>S!#� 2�+�>U�71�@���X\83�;%�
• *�.!#� 5],��LJ^�4R!#� 5]Y'�VN^��
�!#� 5�HO

���Implementation�
•�� ���������•�����������enrollment�•�������� ����assign�

• 9��������

Proper use of envelopes• Envelopes must be made opaque through use of a
cardboard or aluminium foil insert
• Envelopes must be numbered, opened sequentially
• Reporting the use of sequentially numbered opaque sealed envelopes (SNOSE) is accepted to be the minimum standard
0/&:Blinding;�masking )1
•�����&����*(�$ �,�5�����������������:'%2��#+.2�������4"2��;�
•87�*(��#�9!-�36�
Unblinded RCTs can be a problem because there is a risk that patients will receive different treatment according to the physician’s own beliefs.
Crit Care Med 2010; 38[Suppl.]:S534–S538
$(�#�!-Statistical method.•�&���#� ����%, *�"���$(�#�!�
•������'��)�'����+�#'���!�
���
•!)+Registration,•!) ��&*!)��• �����+Protocol,•�$��-��� ��������•'(��#+Funding,•'(��#�����#+%���"#��,-'(��#���

•��RCT�• CONSORT����• CONSORT�� Introduction• CONSORT�� Method• RCT�•��
•����Critical Care����RCT
JAMA. 2017;317(13):1321-1328.
?; Premise
•%��'&�#)$!�*( A��97GP�3����
•BQR ./•QI2>�,���5�OJ��M1�C6 ����5�C��4L8��
•DH�:0��-F���������S• MENDS study��"�(*#N=��)'� &K A��28<@+E�C��
�" Hypothesis
���������!��
↓↓ DEX�����#$� ��↓
•���������28���� %
• 28����ventilater-free days %
8$3 Investigator-initiatedChief investigator
• Yu Kawazoe (2003��) �)�-/�� #"�→'���
• Kyohei Miyamoto92006��:�)�-/�� #"�
Collaborater
• Takeshi Morimoto ���.� 2�+� �#!
• Hitoshi Yamamura �7�/� "�→��� �#!
• Akihiro Fuke �7�/� %1��,����
• Atsunori Hashimoto ���.� "�
• Makoto Ito ��-/1��,���� 86
• Nobuaki Shime 5�,���� "�
• Kohei Kato &��.� "�
• Kenji Yamauchi �(�
• Hiroyuki Koami 4�
�ESICM�������* https://www.esicm.org/ictv-presidents-session-desire-trial-results/
February 2013 ; January 201603�

Inclusion
• 20#��!-' +0�)��)1
•���� 24"/�������(&0NIV�1��.�*���� +
•��,$���%�%�'����
Exclusion
•+��(,�(Child-Pugh�-B or C)•���&!���+�����(NYHA �)•)"��� �� ��•'%#��+�*$,�•��� ��• Dexmedetomidine����� ��• Attending physician's decision
',#�!���
Attending physician�eligible ")�•',���',&*��%(
• Internet Data and Information Center for Medical Research (INDICE)�+-�����$
�INDICEUMIN��� ����������“electronic data capturing system”


• ��������"(����� �@→46:�����)
• ' "A8*;)�=>79.13�COPD
• �46:�ID��������/• (?�+ �0<�8*;)�-$��!• ,:ID�����"�2#5&��%

• "#%�(��)*� ���+����������)*��� ,����'�
• �����$!�)*&�

���
•�$��JSICM������%��•����������•"#�&���"#�&��� ���%��•�!�JSICM������%��
Primary Outcome0!Co - Primary Outcome• 28&)�*• 28&Ventilator Free Days (����.�)47+ &%�28&8-�"��(25
2015/5/2�Ventilator Free Days��'(Outcome data�������/1)• �"���(2���→)��#3���
�$,�5&�)�→�"���(2�5&�VFD�0&� ���26&$,�28&�)��6�4&$,�6&�)��4�-���VFD2&5
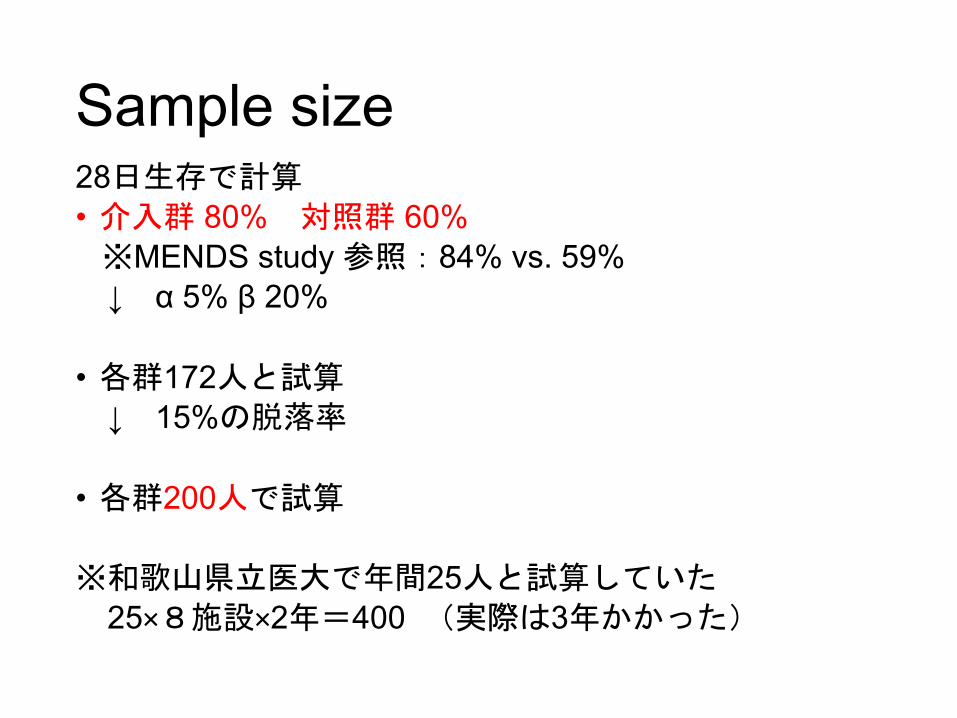
Sample size28����%!• �" 80% ��" 60%�MENDS study ��-84% vs. 59% ↓ α 5% β 20%
• �"172�'!↓ 15%#$�
• �"200��'!
����� ����(25�'!����25×,�&×2�.400 *�)�3�����+

$� �
28����(#• ��% 80%→80% ��% 60%→72%
↓ α 5% β 20%
• �%172 *#
↓ 15%�&'�
• �%200 �*#
����!"����+25 *#����25×/�)×2�0400 -�,�3�����.
Masking, Blinding
Open label•'- �)* �"���!#�+����•�����/�-35)*-4�"���!#�+����
→)*�/���������&������%2 ($1���limitation�,��.0

The main statistical analysis for efficacyComparison between groups of 28-day mortalityMeasure: Death until 28 days after the initiation of mechanical ventilation. Patients who were alive at 28 days were censored at 28 days. Aim: Comparison of the occurrence of the events between groupsTest: Log-rank test, Cox proportional hazard model Significance: Two-sided p values of less than 0.05 were considered statistically significant. Confidence interval: 95%confidence interval (CI) of the hazard ratio were calculated. Expression: The number of the occurrence of the events, Cumulative incidence, and hazard ratio.
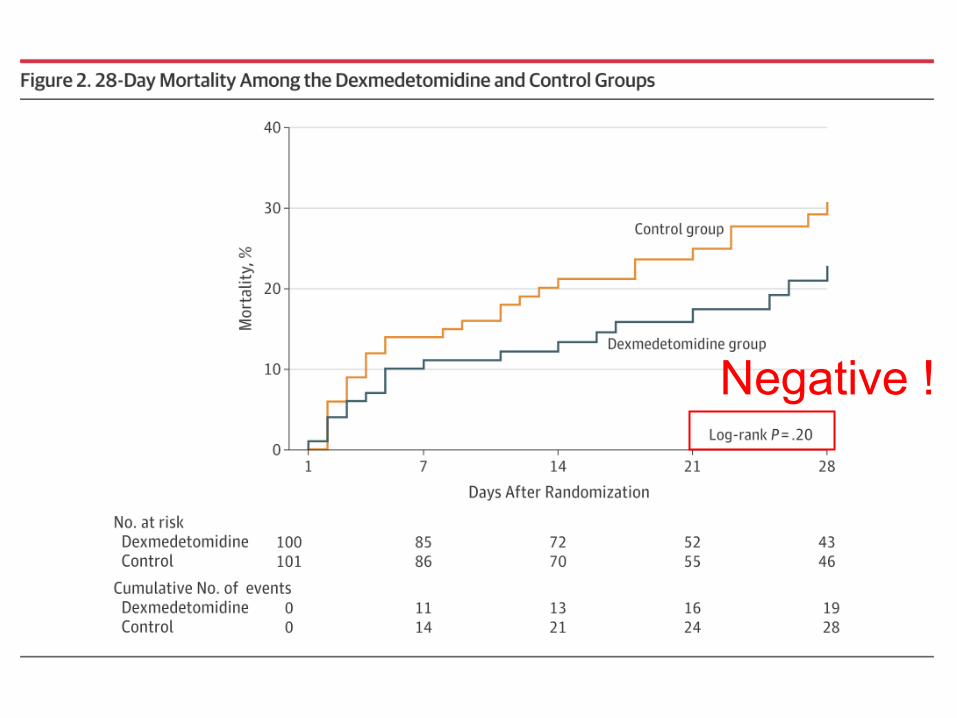
Negative !
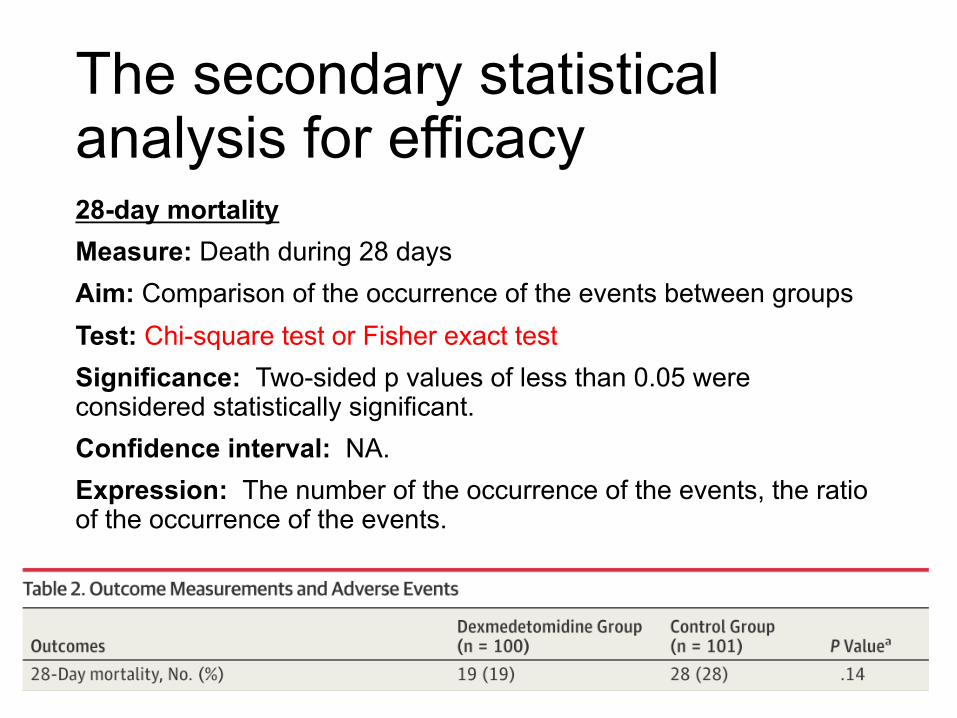
The secondary statistical analysis for efficacy28-day mortality Measure: Death during 28 days Aim: Comparison of the occurrence of the events between groups Test: Chi-square test or Fisher exact testSignificance: Two-sided p values of less than 0.05 wereconsidered statistically significant.Confidence interval: NA.Expression: The number of the occurrence of the events, the ratio of the occurrence of the events.

Data and safety monitoring board (DSMB) and interim analysis• Dr. Sadao Kawasaki (Department of Emergency
Medicine Minami Wakayama Medical Center, Japan) →���
• Dr. Takahiro Ashikawa (Department of emergency medicine, Minami Wakayama Medical Center, Japan) →���
• Dr. Yasuhiro Iwasaki (Department of Emergency and Critical Care Medicine, Wakayama Medical University, Japan) →���
The DSMB will independently perform����•�$ ����1����)%�•'+"#����&
• Emergent reporting system�������������*�����(!

Discussion
• The study may have identified a clinically important benefit of dexmedetomidine—an 8% reduction in 28-day mortality—that did not demonstrate statistical significance.
• Physicians may consider an 8% difference in 28-day mortality to be clinically significant but this study was underpowered to detect this difference.

Funding• Funding/Support: This study was supported in part by a noncontractual research grant to Wakayama Medical University provided by Hospira Japan.
• Role of the Funder/Sponsor: Hospira Japan participated in part of the design of this study;however, it had no role in the conduct of the study;collection, management, analysis, and interpretation of the data; preparation or approval of the manuscript; or decision to submit the manuscript for publication.
��
• No earlier multicenter RCTs have investigated the effects of ANP infusion in patients with cardiac surgery–associated AKI.
��
• We therefore decided to evaluate the effects of ANP on renal function and medical costs in patients with cardiac surgery–associated AKI.

• ��&"&�0+�/�0+�)#����ICU�!$��ICU��-��ICU
• (*���
• 11%.���• May 2012 - March 201511��,���2• '���� 90�������

����
• Double-blind
• ANP 0.02 μg /kg/min (2 mL/h) •��� (5% glucose, 2 mL/h�
• Preoperative level�����
•��������������
���������
•����Study coordinators�INDICE��• INDICE randomization system����

Inclusion
• Age of ≥20 years
• Recent elective cardiac surgery, namely, CABG, valve surgery, thoracic aortic aneurysm surgery, or a combination thereof.
• AKI within 48 hours after cardiac surgery
��������ANP����
Exclusion
• Severe hypotension or cardiogenic shock
• Right ventricular infarction
• Dehydration
• End-stage renal disease
• Administration of nonsteroidal anti-inflammatory drugs,
angiotensin-converting enzyme(ACE) inhibitor, or angiotensin
receptor blocker (ARB) within 24 hours before the operation
• Administration of contrast agent within 3 days before the operation
• Extracorporeal membrane oxygenation.
The primary end point
• Change in renal function over the 90-day follow-up measured by serum levels of creatinine and cystatin C, and creatinine clearance or eGFR.
• ������→ a difference in means of 74.25 � ���
↓↓↓ α 5% β 20%
• ��87���↓ 10%����
• ��97���
����������������
Sample size and power calculation

Reasons why,,,,• approval of ethics committees• difficulty in obtaining consent from patients• decisions by several hospitals to prioritize
patients with ventricular assist devices.
• many surgeons in trial sites insisted on using ANP in patients with high preoperative creatinine levels
→these patients were excluded before assessment for eligibility and were administered ANP during surgery.

• �!���#(+ � �
• ������%'("� )�� “��$&”�������������*

����������
Funding
• This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.

•��RCT�• CONSORT����• CONSORT�� Introduction• CONSORT�� Method• RCT�•��

49#�+�7!�� ;
• 1�.*�"�� ;����positive �negative �-)6• �����.*��� ;/:��positive��-)6?
'�+�7!�� ;
• 1�.*�"�� ;����positive ��-)6?• �����.*��� ;/:��positive��-)6?=$�������?>
.*� ;�%8(��3�5&������#�?
,2<���0?





























