Embed Size (px)
Citation preview

University of Nebraska Medical Center University of Nebraska Medical Center
DigitalCommons@UNMC DigitalCommons@UNMC
Capstone Experience Master of Public Health
8-2021
RE-AIM Evaluation of Workplace Weight Management RE-AIM Evaluation of Workplace Weight Management
Interventions: A Systematic Review Interventions: A Systematic Review
Adrienne Gothard University of Nebraska Medical Center
Follow this and additional works at: https://digitalcommons.unmc.edu/coph_slce
Part of the Public Health Commons
Recommended Citation Recommended Citation Gothard, Adrienne, "RE-AIM Evaluation of Workplace Weight Management Interventions: A Systematic Review" (2021). Capstone Experience. 156. https://digitalcommons.unmc.edu/coph_slce/156
This Capstone Experience is brought to you for free and open access by the Master of Public Health at DigitalCommons@UNMC. It has been accepted for inclusion in Capstone Experience by an authorized administrator of DigitalCommons@UNMC. For more information, please contact [email protected].

1
RE-AIM Evaluation of Workplace Weight Management Interventions: a Systematic
Review
Adrienne Gothard
Concentration: Health Promotion
Capstone Committee:
Paul Estabrooks, PhD (Chair)
Melissa Tibbits, PhD
Fabio Almeida, PhD, MSW
Abstract
Overweight/Obesity is a major public health concern that affects nearly a third of the world’s population. In addition to personal health effects such as cardiovascular disease, cancer, and diabetes, obesity can take a toll on an employer’s bottom line, specifically healthcare costs and absenteeism. Many employers promote intervention programs targeted at lifestyle and behavioral factors to improve workforce health. A 2016 systematic review by Weerasekara et al. compared several of these intervention programs based on the effectiveness of the program, measured in participant’s weight changes from baseline to post-intervention. While this information can be valuable to employers who are interested in implementing their own program, more information is needed on the cost, including implementation and continuing costs, the representativeness of the sample included in the program, and the ability to maintain effectiveness over time. Using the reach, effectiveness, adoption, implementation, and maintenance framework (RE-AIM), this project will expand on previous findings and provide much needed data to assist employers and identify best practices for workplace weight management intervention programs. This systematic literature review evaluates interventions published between August 2015 and June 2021. While most studies address several aspects of the reach dimension, very few effectively outline measures of adoption or the cost aspects of the effectiveness dimension.

2
CHAPTER 1- INTRODUCTION
Research Question & Objectives
The aim of this project, RE-AIM Evaluation of Workplace Weight Management
Interventions: a Systematic Review, is to evaluate existing workplace weight
management interventions through the lens of the RE-AIM framework. This project
expands on the findings of a 2016 systematic review titled “Effectiveness of Workplace
Weight Management Interventions: a Systematic Review” by Weerasekara et al. In
addition to the evaluation of intervention effectiveness, this project also evaluates
interventions based on their reach, adoption, implementation, and maintenance. The
original review included a search of literature from inception to August 2015. This
project uses the same search criteria used in the original systematic review to evaluate
recent literature based on studies published after August 2015.
The purpose of this review is to identify long-term (³6 month) workplace weight
management interventions and review the data across the measures of the reach,
effectiveness, adoption, implementation, and maintenance framework (RE-AIM). The
specific question to be answered by the review is: How many of the RE-AIM dimensions
are addressed by the current literature addressing workplace wellness interventions for
obesity? The primary aim of this project is to identify effective and long-lasting
interventions that may be implemented at workplace settings to give employers a place
to start when looking to invest in the health and well-being of their most valuable
resource, the workforce. Building off of the base information included in the
Weerasekara et al. review, the additional information included in this review, can help to
translate this important setting-based research into practice.

3
Rationale for Review
In recent decades, the workplace, where employed individuals spend a large
proportion of their waking hours, has become a setting of interest for health promotion
interventions. Interest in workplace wellness intervention programs from the perspective
of an employer often stems from the assumption that these programs will result in
increased employee health status, thus reducing health care costs and increasing
productivity in the workplace. In 2012, an estimated $8.65 billion dollars in lost
productive time was attributed to absenteeism related to obesity in the United States.
Additionally, annual health care spending per capita for obesity related expenses are
estimated at $1600 for men and $1525 for women (Yarborough et al., 2018).
Employer based programs generally target lifestyle and behavioral factors, such
as weight management, physical activity, stress reduction, and tobacco cessation
(Abraham, 2019). These programs are especially important in occupations that are
inherently sedentary, such as “desk jobs”. Excessive sitting and physical inactivity at
work have been associated with increased risk of obesity (Shrestha et al., 2018).
Over the years, studies have shown variable results for the desired outcomes,
and thus evaluation of programs based on gold standard randomized control trials
(RCTs) are needed. This systematic literature review will include only RCT studies and
will add a thorough review of workplace weight management interventions to the current
literature available to researchers and employers.
The RE-AIM framework was developed to help invested parties evaluate a
program through multiple lenses, thus broadening the scope of the evaluation (RE-AIM,
n.d.). The RE-AIM framework takes into account many of the factors that may affect

4
program success in a “real-world” situation. The RE-AIM acronym stands for reach,
effectiveness, adoption, implementation, and maintenance (RE-AIM, n.d.). “Reach”
shows the representativeness of individuals of a given program, while “adoption” shows
the representativeness of the setting. “Effectiveness” refers to the outcomes of the
intervention, both positive and negative. The “implementation” element of RE-AIM
evaluates the level of fidelity and consistency with which the intervention program
adheres to the outlined description or program plan. “Maintenance” refers to how the
intervention becomes engrained in the setting culture and the long-term effects in the
individual (RE-AIM, n.d.). Since this framework doesn’t focus only on the outcome of
an intervention (i.e. overall weight loss), this review will help to determine the overall
success of workplace weight management intervention programs.
CHAPTER 2- BACKGROUND
Description of the Health Problem
Overweight and obesity are described by the World Health Organization (WHO)
as “abnormal or excessive fat accumulation that may impair health” (World Health
Organization, 2020). Overweight range is defined by the Centers for Disease Control
and Prevention (CDC) as a body mass index (BMI) of 25 to <30 kg/m2, while obesity is
defined as a BMI of 30 kg/m2or higher (CDC, 2021). Obesity increases an individual’s
risk for a myriad of health conditions, such as diabetes mellitus, cardiovascular disease,
and certain types of cancers (Sandercock & Andrade, 2018).
Overweight/obesity is a global health problem, affecting nearly one-third of the
population worldwide. The number of individuals who fall into an overweight or obese

5
category has doubled since 1980 (Chooi et al, 2019). These staggering statistics speak
to the need for interventions, including setting-based approaches, to address weight
management.
The definition of clinically significant weight loss is a measure of weight reduction
of at least 5% of baseline weight (Swift et al., 2016). This is the level of weight loss that
has been shown to improve cardiometabolic risk factors, and as such the threshold of
>5% weight loss is an attractive goal for public health researchers when designing
weight loss interventions.
CHAPTER 3 - METHODS
Search Strategy
In June 2021, a systematic literature search was conducted using the following
literature databases: Medline, CINAHL, Scopus, and Cochrane Central Register of
Controlled Trials. The search strategy of the original review by Weerasekara et al. was
mimicked for the search (Appendix A). Due to limitations in the availability of databases
through University of Nebraska Medical Center library, not all of the databases used in
the original review were used for this search (e.g. Scopus, SportDiscus and LILACS
were not included in the search). An additional search criterion for publication date
(August 2015-current) was added to ensure no overlap in articles from the original
study.
Inclusion and Exclusion Criteria
As per the Weerasekara et al. protocol, study eligibility included the
following:

6
1. Intervention(s) was conducted in a workplace with a primary aim to promote
weight loss, prevent weight gain, or maintain weight status;
2. Study design included randomization of samples, such as randomized control
trials, cluster randomized trials, and crossover designs (pre-post and quasi
experimental designs were not included);
3. Study population of adults of both sexes, age greater than or equal to 18
years, and who were employed at the workplace with no exclusions based on
weight status, co-existing risk factors, or comorbidities;
4. Primary outcomes of intervention studies were change in weight, BMI (body
mass index), and/or body fat;
5. Intervention duration of ³ 6 months;
6. Intervention type including dietary, physical activity, financial incentives,
behavior change and goal setting, environmental workplace modification, and
health risk appraisal with feedback. Intervention types excluded were those
where food or meal replacements (³1 meal/day) were provided.
Data extraction & Quality Assessment
Once eligible studies were identified, data extraction for the dimensions of the
RE-AIM framework was completed using the coding methods described in the 2018
review titled “Understanding the impact of rural weight loss interventions: A systematic
review and meta-analysis” by Porter et al. The data abstraction tool used by the Porter
et al. study team was utilized to code the RE-AIM data and ensure a thorough review of
all dimensions (Porter et al., 2018). Prior to coding the eligible articles for this review,

7
the coder (AG) selected a sample study to review and code information for each of the
five dimensions of the RE-AIM framework: reach, effectiveness, adoption,
implementation, and maintenance. This sample coding was reviewed by a senior
scientist to ensure competence in data extraction. The list of RE-AIM indicators and
their corresponding definitions is presented in Appendix B. This assessment was
completed in lieu of a formal quality assessment tool, as relevant data was extracted
from all studies included for review.
CHAPTER 4 – RESULTS
Search Results & Selection Process
The literature database searches in Medline, CINAHL, Scopus, and Cochrane
Central Register of Controlled Trials originally yielded 625 potentially relevant articles.
Once duplicates were removed, remaining articles titles and abstracts were screened
for eligibility criteria. Final review of the full text of potentially eligible articles was then
performed to identify articles for inclusion. Ultimately, 21 articles from 13 unique
intervention studies were included for review and data abstraction. Figure 1 outlines the
study selection process in the Preferred Reporting Items for Systematic Reviews
(PRISMA) flow diagram (Page et al., 2021).

8
Figure 1. Preferred Reporting Items for Systematic Reviews (PRISMA) flow diagram.
Description of Studies
Interventions included in this review varied by geographic location, including the
United States (n=9), Denmark (n=1), Iran (n=1), Ireland (n=1), and Malaysia (n=1). By
design, all study settings were workplaces with a focus on employee study participants.
Intervention settings included government agencies, nursing home/health care facilities,
social service organizations and health centers, manufacturing workplaces,
transportation companies, and academic institutions. Study duration varied from 6-24
months. Table 1 summarizes the characteristics of each study, including the study goal,
design, and evaluation period.
Potentially relevant records identified from electronic databases search
(N=625)
Records screened (N=382)
Duplicates excluded (N=243)
Records excluded by title/abstract (N=346)
Full text articles assessed for eligibility
(N=36)
Records identified by secondary reference
(N=2)
Full text articles eligible and included in analysis (N=21 articles from 13 unique intervention studies)
Records excluded (N=17)
Does not apply to key question (n=8) Study design did not meet criteria (n=5) Study duration did not meet criteria (n=3) Not in a worksite (n=1) Article not in English (n=1)

9
10
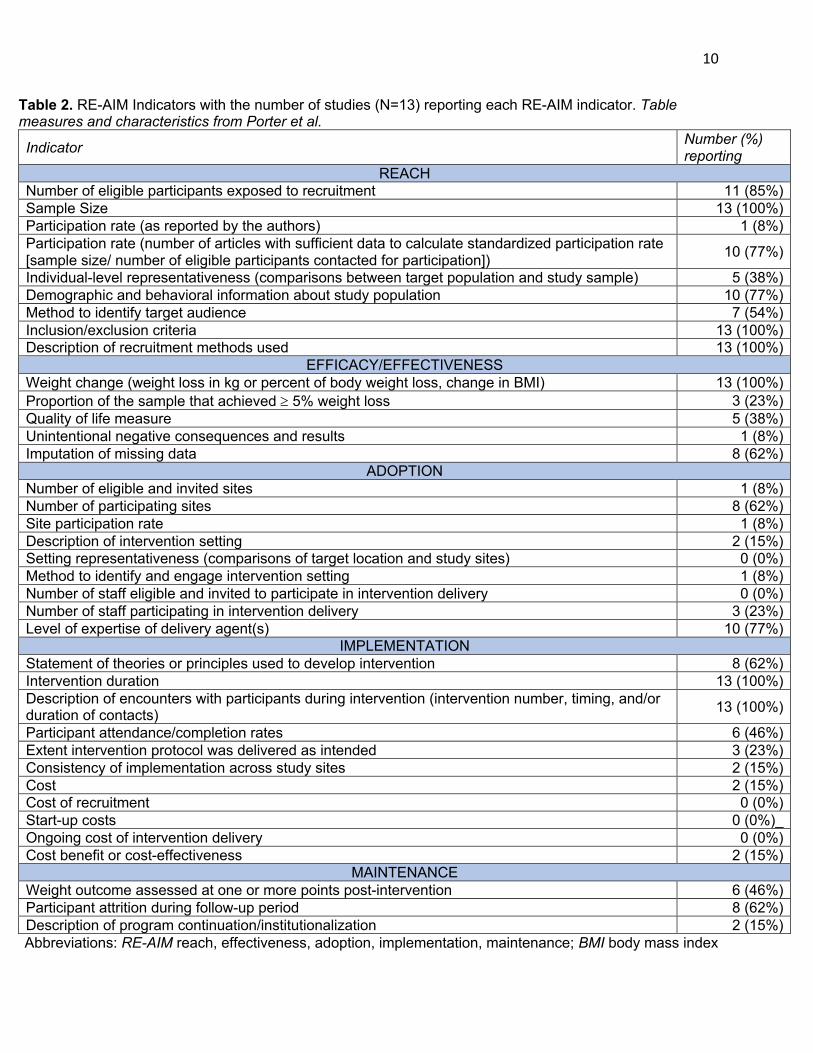
Table 2. RE-AIM Indicators with the number of studies (N=13) reporting each RE-AIM indicator. Table measures and characteristics from Porter et al.
Indicator Number (%) reporting
REACH Number of eligible participants exposed to recruitment 11 (85%) Sample Size 13 (100%) Participation rate (as reported by the authors) 1 (8%) Participation rate (number of articles with sufficient data to calculate standardized participation rate [sample size/ number of eligible participants contacted for participation]) 10 (77%)
Individual-level representativeness (comparisons between target population and study sample) 5 (38%) Demographic and behavioral information about study population 10 (77%) Method to identify target audience 7 (54%) Inclusion/exclusion criteria 13 (100%) Description of recruitment methods used 13 (100%)
EFFICACY/EFFECTIVENESS Weight change (weight loss in kg or percent of body weight loss, change in BMI) 13 (100%) Proportion of the sample that achieved ³ 5% weight loss 3 (23%) Quality of life measure 5 (38%) Unintentional negative consequences and results 1 (8%) Imputation of missing data 8 (62%)
ADOPTION Number of eligible and invited sites 1 (8%) Number of participating sites 8 (62%) Site participation rate 1 (8%) Description of intervention setting 2 (15%) Setting representativeness (comparisons of target location and study sites) 0 (0%) Method to identify and engage intervention setting 1 (8%) Number of staff eligible and invited to participate in intervention delivery 0 (0%) Number of staff participating in intervention delivery 3 (23%) Level of expertise of delivery agent(s) 10 (77%)
IMPLEMENTATION Statement of theories or principles used to develop intervention 8 (62%) Intervention duration 13 (100%) Description of encounters with participants during intervention (intervention number, timing, and/or duration of contacts) 13 (100%)
Participant attendance/completion rates 6 (46%) Extent intervention protocol was delivered as intended 3 (23%) Consistency of implementation across study sites 2 (15%) Cost 2 (15%) Cost of recruitment 0 (0%) Start-up costs 0 (0%)_ Ongoing cost of intervention delivery 0 (0%) Cost benefit or cost-effectiveness 2 (15%)
MAINTENANCE Weight outcome assessed at one or more points post-intervention 6 (46%) Participant attrition during follow-up period 8 (62%) Description of program continuation/institutionalization 2 (15%) Abbreviations: RE-AIM reach, effectiveness, adoption, implementation, maintenance; BMI body mass index

11
Summary of Findings
Table 2 summarizes the results of the coding and RE-AIM indicators
assessment.
REACH All studies included a description of the target population, and a majority of the
studies included the demographic and behavioral information about the study population
(e.g. participants’ sex, age range, education level, marital status, etc.). All studies also
included at least a brief description of the recruitment strategies used for participation in
the intervention program. Inclusion criteria was included for all studies, while 4 studies
listed exclusion criteria as “none”, as all employees were encouraged to participate in
the intervention. According to one study “…all employees at the sites were eligible to
participate. This is typical of worksite programs, which tend to be all-inclusive to avoid
issues related to fairness and access.” (Wilson et al., 2016b). Authors of another study
stated, “There were no exclusions by BMI category or other chronic conditions because
the interventions addressed small lifestyle changes that could be adopted regardless of
any underlying conditions.” (Fernandez et al., 2015).
All studies reported the sample size of the study population, with a majority in the
range from 42 to 850 participants with an outlier of 3799 participants. After removing the
outlier, the median sample size was 290 (± 560). Only one study explicitly stated the
participation rate (Ing et al., 2018), although 10 of the studies (77%) provided sufficient
data to calculate a standardized participation rate.

12
Five of the studies (38%) provided comparisons between the study sample and
the broader target population. One study noted that the financial component of the study
led to “higher income and more educated participants than the overall hospital
workforce” (Cleveland et al., 2020). Of note, one limitation noted by many of the studies
in this review is the potential for selection bias. Although these studies are randomized,
they rely on voluntary participation, which may lead to study samples having more
motivated participants compared to general workplace population.
EFFECTIVENESS
All 13 studies included a measure of weight change as an outcome of the
intervention. These measures included change in weight, BMI, or body weight (percent)
in comparison to an untreated control group, a comparison group, or other treatment
groups. All studies reported mean loss in weight, BMI, or % body weight compared to
baseline measures. Table 3 outlines the outcomes of the studies with an outcome of
weight change (studies with a goal of weight gain prevention and/or weight maintenance
excluded).
Interventions that focused on weight loss maintenance or weight gain prevention
reported mixed success. One study showed that a deposit contract led to more
participants meeting their weight loss maintenance goals than the control (Cleveland et
al., 2020), and another study with the goal of weight loss maintenance showed that a
larger proportion of participants in a DVD intervention were able to maintain weight loss
compared to a face-to-face intervention (Ing et al., 20148). One study showed that
minimizing environmental exposure to calorically dense foods may have an impact on

13
preventing weight gain (Fernandez et al., 2015), while another study showed no
difference in intervention and control groups for preventing weight gain (Thorndike et a.,
2021).
Only three studies (23%) reported the proportion of the sample that achieved
³5% weight loss (Jamal et al., 2016; Patel et al., 2016; Wilson et al., 2016). One
additional study gave participants a goal to lose 5-7% of their body weight but did not
report outcomes in terms of body weight percent loss (Ferrera et a., 2020).
Table 3. Impact of interventions on weight for those studies with a goal of weight loss
Study Weight Change from Baseline, Mean (kg) Evaluation
Period (month)
Abdi et al. -1.9 kg (telephone group) -1.08 kg (web group) 6
Balk-Møller et al. -1.04 kg (intervention group) 9.5
Geaney et al. -0.7 kg (education group) -0.04 kg (environmental group) -0.4 kg (combined intervention group)
7-9
Jamal et al. -2.24 kg (intervention) -0.69 kg (comparison) 6
Kullgren et al. -2.3 kg* (no match group) -1.6 kg* (1:1 match group) -1.3 kg* (2:1 match group)
6
Patel et al. -0.55 kg* (delayed premium adjustment group) -0.64 kg* (immediate premium adjustment group) -0.45 kg* (daily lottery group)
12
Wilson et al. -2.2 kg* (phone group) -1.5 kg* (small group) -1.2 kg* (self-study)
6
Study Weight Change from Baseline, Mean (BMI, kg/m2)
Evaluation Period
(month) Fernandez et al. -0.54 kg/m2 (intervention group) 24
Study Weight Change from Baseline, Mean (% body weight)
Evaluation Period
(month) Ferrera et al. -2.7% body weight (YMCA DPP group)
-2.41% body weight (VLM-DPP group) 6
*original measure of weight change listed in pounds, converted to kg [number in pounds/2.2]

14
ADOPTION
Of the five dimensions of RE-AIM, adoption was the dimension with the least
amount of reporting across the board for all studies. The number of participating sites
was described in eight (62%) of the studies, while the number of individuals participating
in the delivery of the intervention was only stated in three (23%) of the studies.
The level of expertise of the intervention delivery agent was described in a
majority of the studies (10 studies, 77%), although the detail provided varied greatly. For
instance, one study simply stated, “trained staff from the research group” (Balk-Møller et
al., 2017), while another study went into much more detail, describing the ideal peer
health coach as “outgoing, respected and a good communicator” and specifying that an
occupational health nurse would be on site at the workplace (Wilson et al., 2016b).
IMPLEMENTATION All 13 studies described intervention details (number of contacts, timing and/or
duration of contacts) to some extent. For several of the interventions, outlines of class
schedules and teaching points were provided in table form. Three studies (Jamal et al.,
2016; Wilson et al., 2016; Wilson et al., 2016b) were adaptations of previous protocols,
and as such described the extent to which the protocol was modified and the reasons
why the protocol was modified to fit the target worksite populations. Eight studies (62%)
described the public health theories or principles used to develop the intervention.
An important feature of the “Implementation” dimension of RE-AIM is cost. Very
few studies reported details on the costs of the interventions, specifically cost of
recruitment, start-up costs, ongoing costs, and cost-effectiveness. Only two studies

15
provided a description of intervention costs and cost effectiveness, and these numbers
were published in supplemental articles dedicated to the cost aspect of the studies
(Fitzgerald et al., 2018 & Corso et al., 2018). One of these studies (Corso et al., 2018)
described the cost of the intervention for each of the three treatment arms (ranging from
$143/employee for the self-study group to $601/employee for the phone treatment
group).
MAINTENANCE For the maintenance dimension, eight (62%) of the studies described the attrition
of the participants, including the reasons for loss to follow-up. Additionally, six (46%) of
the studies assessed a weight outcome at some point post intervention during the
study. Many of the reasons listed for loss to follow-up were financial, job change,
personal reasons, and workplace restructuring.
Quality Assessment
As outlined in the inclusion criteria for eligible studies, intervention types
including dietary, physical activity, financial incentives, behavior change and goal
setting, and environmental workplace modification were considered. Table 4 outlines
the intervention characteristics of each of the 13 intervention studies. An inclusion
criterion was a measure of weight to evaluate effectiveness of the intervention. Table 4
also shows the studies that had an additional dietary and or physical activity measure
included in their evaluation.

16

17
DISCUSSION
Summary
The RE-AIM framework is an effective assessment for identifying the necessary
program components that should be included not only in the report of an intervention
program, but also the planning and design of the program. By addressing the
dimensions of RE-AIM, program planners can help to ensure generalizability of studies,
therefore making them more available to be reproduced or adapted to other settings
(RE-AIM, n.d.).
The concept of reach (representativeness of individuals) is especially important
in workplace settings, as there can be many differences in population characteristics
and setting (RE-AIM, n.d.). In the same workplace, the population could have a large
difference in age, baseline health status, education level, etc., all of which could play a
role in how they respond to an intervention. Understanding the reach of an intervention
program will help employers to understand how the intervention may work with their
specific workplace population.
Effectiveness, of course, is important in the evaluation of any intervention
program, especially when able to be compared to cost. If a study is able to show
positive outcomes for employee health, employers may be more likely to employ a
program if they can justify the cost. In contrast, if a study does not show positive
impacts (e.g. clinically significant weight loss, weight gain prevention, or weight loss
maintenance), there is likely little incentive to invest resources into a program.
The findings of this study, specifically the categorical lack of information
regarding intervention program costs, show a need for transparency in this area,

18
especially if the program is to be replicated and translated to other settings. Additionally,
information on the adoption, both at the individual and setting levels, may be beneficial
for public health practitioners and researchers when creating similar programs.
Public Health Implications
Worksite weight management intervention programs have the potential to have
major public health implications on adults in the workforce. Interventions targeted at
weight management have the potential to not only increase the health of the individual,
through weight reduction, but also mental health. Improvements in workplace
environment and lifestyle interventions also have the potential to improve the health and
well-being of all employees, not just those who are overweight or obese.
Strengths and Limitations
One strength of this review is that techniques from other successful reviews were
able to be utilized. This created a strong foundation to build upon for this review of more
recent studies. The assessment tool used by Porter et al. provided and thorough review
of the dimensions of the RE-AIM framework.
One potential limitation of this review is the relatively small sample size. Since
the window for study publication was a little under seven years and many studies did
not meet the eligibility criteria, this systematic review only represented 13 studies from
21 published articles. Additionally, the effects of the COVID-19 pandemic over the past
year and a half have likely affected many studies that were in progress during the onset
of the pandemic, and delayed others that may have been planned.

19
In addition to the small sample size of studies, another limitation to this review is
the evaluation of study effectiveness. Since the studies did not all have the same
primary outcome measure, very few comparisons in terms of effectiveness could be
made in contrast to a review where all of the studies had the same measure (e.g. weight
loss measured in kg or pounds lost from baseline to post-intervention). Additionally,
there was a large range for intervention duration (ranging from 6 to 24 months), which
also makes comparisons in weight changes difficult. Future studies in this area could
potentially expand some of the other eligibility criteria, while honing in on only studies
with similar intervention durations and units of measure.
Gaps in Evidence
Many workplace weight management studies are currently evaluating the
potential of deposit contracts for weight loss, weight loss maintenance, or weight gain
prevention. Starting in 2014, the limit of the amount that employers may use to provide
wellness-inceptives increased from 20% to 30% of the total amount of an employee’s
health insurance premiums (Volpp et al., 2011). More studies evaluating the optimal
incentive type (e.g. deposit contracts vs. cost-sharing mechanisms) as well as the
optimal financial investment for the employer are needed to evaluate the prospective
success of financial incentives for weight management.
Another possible future area of study is the adaptation of successful health
promotion interventions to be specific to weight management in the workplace. Three of
the studies included in this review (Ferrara et al., 2020; Wilson et al., 2016; Wilson et
al., 2016b) derived interventions from the National Diabetes Prevention Program,

20
including the lifestyle change programs that are recognized by the CDC (Ferrara et al.,
2020). Employers may be able to utilize programs and resources that are already in
existence to implement successful and cost-effective weight management interventions.
Conclusions
The potential of workplace interventions for overweight/obesity has been seen as
an area of great potential over the past few decades. The importance of reaching
individuals where they spend a large proportion of their waking hours is essential to
promoting a healthy lifestyle. These of interventions can provide a mix of dietary and
physical activity instruction, behavioral modification, environmental changes, and
financial incentives. In program planning and evaluation, it is crucial to take into account
the dimensions of the RE-AIM framework to increase the validity and generalizability of
public health interventions.

21
BIBLIOGRAPHY
Abdi, J., Eftekhar, H., Mahmoodi, M., Shojayzadeh, D., Sadeghi, R., Saber, M. (2015). Effect of the intervention based on new communication technologies and the social-cognitive theory on the weight control of the employees with overweight and obesity. Journal of Research in Health Sciences, 15(4), 256-61. Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med12&NEWS=N&AN=26728913.
Abraham, J. M. (2019). Employer wellness programs—a work in progress. Journal of
the American Medical Association, 321(15):1462–1463. https://doi.org/10.1001/jama.2019.3376
Balk-Møller, N. C., Larsen, T. M., Holm, L. (2017). Experiences from a web- and app-
based workplace health promotion intervention among employees in the social and health care sector based on use-data and qualitative interviews. Journal of Medical Internet Research, 19 (10), e108. https://dx.doi.org/10.2196/jmir.7278
Balk-Møller, N. C., Poulsen, S. K., Larsen, T. M. (2017). Effect of a nine-month web-
and app-based workplace intervention to promote healthy lifestyle and weight loss for employees in the social welfare and health care sector: a randomized controlled trial. Journal of Medical Internet Research, 19, e108. https://dx.doi.org/10.2196/jmir.6196
Brace, A. M., Padilla, H. M., DeJoy, D. M., Wilson, M. G., Vandenberg, R. J., Davis, M.
(2015). Applying re-aim to the evaluation of fuel your life : a worksite translation of dpp. Health Promotion Practice, 16, 28-35. https://dx.doi.org/10.1177/1524839914539329
CDC (2021, June 7). Defining adult overweight & obesity.
https://www.cdc.gov/obesity/adult/defining.html Chooi, Y.C., Ding, C., & Magkos, F. (2019). The epidemiology of obesity. Metabolism,
92, 6-10. https://doi.org/10.1016/j.metabol.2018.09.005 Cleveland, L. P., Seward, M. W., Simon, D., Rifas-Shiman, S. L., Lewis, K. H., Bennett-
Rizzo, C., Halperin, F., McManus, K. D., Block, J. P. (2020). Bwhealthy weight pilot study: a randomized controlled trial to improve weight-loss maintenance using deposit contracts in the workplace. Preventive Medicine Reports, 17, 101061. https://dx.doi.org/10.1016/j.pmedr.2020.101061

22
Corso, P. S., Ingels, J. B., Padilla, H. M., Zuercher, H., DeJoy, D. M., Vandenberg, R. J., Wilson, M. G. (2018). Cost effectiveness of a weight management program implemented in the worksite: translation of fuel your life. Journal of Occupational & Environmental Medicine, 60, 683-687. https://dx.doi.org/10.1097/JOM.0000000000001343
Faghri, P. D., Simon, J., Huedo-Medina, T., Gorin, A. (2017). Perceived self-efficacy
and financial incentives: factors affecting health behaviors and weight loss in a workplace weight loss intervention. Journal of Occupational & Environmental Medicine, 59, 453-460. https://dx.doi.org/10.1097/JOM.0000000000000987
Fernandez, I. D., Chin, N. P., Devine, C. M., Dozier, A. M., Martina, C. A., McIntosh, S.,
Thevenet-Morrison, K., Hongmi, Y. (2015). Images of a healthy worksite: A group-randomized trial for worksite weight gain prevention with employee participation in intervention design. American Journal of Public Health, 105(10, 2167-2174.
Ferrara, A., McDonald, J. C., Brown, S. D., Alexander, J. G., Christian-Herman, J. L.,
Fisher, S., Quesenberry, C. P. (2020). Comparative effectiveness of 2 diabetes prevention lifestyle programs in the workplace: the city and county of san francisco diabetes prevention trial. Preventing Chronic Disease, 17, E38. https://dx.doi.org/10.5888/pcd17.190396
Fitzgerald, S., Murphy, A., Kirby, A., Geaney, F., Perry, I. J. (2018). Cost-effectiveness
of a complex workplace dietary intervention: an economic evaluation of the Food Choice at Work study. BMJ Open, 8(3):e019182. doi: 10.1136/bmjopen-2017-019182.
Geaney, F., Kelly, C., Di Marrazzo, J. S., Harrington, J. M., Fitzgerald, A. P., Greiner, B.
A., Perry, I. J. (2016). The effect of complex workplace dietary interventions on employees' dietary intakes, nutrition knowledge and health status: a cluster controlled trial. Preventive Medicine, 89, 76-83. https://dx.doi.org/10.1016/j.ypmed.2016.05.005
Geaney, F., Scotto Di Marrazzo, J., Kelly, C. et al. The food choice at work study:
effectiveness of complex workplace dietary interventions on dietary behaviours and diet-related disease risk - study protocol for a clustered controlled trial. Trials 14, 370 (2013). https://doi.org/10.1186/1745-6215-14-370
Kullgren, J. T., Troxel, A. B., Loewenstein, G., Norton, L. A., Gatto, D., Tao, Y., Zhu, J.,
Schofield, H., Shea, J. A., Asch, D. A., Pellathy, T., Driggers, J., Volpp, K. G. (2016). A randomized controlled trial of employer matching of employees' monetary contributions to deposit contracts to promote weight loss. American Journal of Health Promotion, 30, 441-52. https://dx.doi.org/10.1177/0890117116658210

23
Ing, C. T., Miyamoto, R. E. S., Fang, R., Antonio, M., Paloma, D., Braun, K. L., Kaholokula, J. K. (2018). Comparing weight loss-maintenance outcomes of a worksite-based lifestyle program delivered via dvd and face-to-face: a randomized trial. Health Education & Behavior, 45, 569-580. https://dx.doi.org/10.1177/1090198118757824
Jamal, S. N., Moy, F. M., Azmi Mohamed, M. N., Mukhtar, F. (2016). Effectiveness of a
group support lifestyle modification (gslim) programme among obese adults in workplace: a randomised controlled trial. PLoS ONE, 11, e0160343. https://dx.doi.org/10.1371/journal.pone.0160343
Levy, D. E., Gelsomin, E. D., Rimm, E. B., Pachucki, M., Sanford, J., Anderson, E.,
Johnson, C., Schutzberg, R., Thorndike, A. N. (2018). Design of choosewell 365: randomized controlled trial of an automated, personalized worksite intervention to promote healthy food choices and prevent weight gain. Contemporary Clinical Trials, 75, 78-86. https://dx.doi.org/10.1016/j.cct.2018.11.004
Padilla, H. M., Zuercher, H., Robertson, M., DeJoy, D. M., Wilson, M., Vandenberg, R. J., Corso, P. S. (2021). Reach, uptake, and satisfaction of three delivery modes of fuel your life. Health Promotion Practice, 22, 415-422. https://dx.doi.org/10.1177/1524839919869921
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffman, T.C., Mulrow, C. D.,
Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J.M., Hrobjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. The BMJ, 372, 71. https://doi.org/10.1136/bmj.n71
Patel, M. S., Asch, D. A., Troxel, A. B., Fletcher, M., Osman-Koss, R., Brady, J., Wesby,
L., Hilbert, V., Zhu, J., Wang, W., Volpp, K. G. (2016). Premium-based financial incentives did not promote workplace weight loss in a 2013-15 study. Health Affairs, 35, 71-9. https://dx.doi.org/10.1377/hlthaff.2015.0945
Porter, G. C., Laumb, K., Michaud, T., Brito, F., Petreca, D., Schwieger, G., Bartee, T.,
Yeary, K. H. K., & Estabrooks, P. (2018). Understanding the impact of rural weight loss interventions: A systematic review and meta-analysis. Obesity Reviews, 20, 713-724. https://doi.org/10.1111/obr.12825
RE-AIM. (n.d.). Frequently Asked Questions. https://www.re-aim.org/about/frequently-
asked-questions/ Sandercock, V. & Andrade, J. (2018 Dec 3). Evaluation of Worksite Wellness Nutrition
and Physical Activity Programs and Their Subsequent Impact on Participants’ Body Composition. Journal of Obesity. https://doi.org/10.1155/2018/1035871

24
Shrestha N., Kukkonen-Harjula K. T., Verbeek J. H., Ijaz S., Hermans V., Pedisic Z. (2018). Workplace Interventions for Reducing Sitting at Work. The Cochrane Database of Systematic Reviews, 6. https://doi.org/ 10.1002/14651858.CD010912.pub4
Stankevitz, K., Dement, J., Schoenfisch, A., Joyner, J., Clancy, S. M., Stroo, M.,
Ostbye, T. (2017). Perceived barriers to healthy eating and physical activity among participants in a workplace obesity intervention. Journal of Occupational & Environmental Medicine, 59, 746-751. https://dx.doi.org/10.1097/JOM.0000000000001092
Swift, D. L., Johannsen, N. M., Lavie, C. J., Earnest, C. P., Blair, S. N., & Church, T. S.
(2016). Effects of clinically significant weight loss with exercise training on insulin resistance and cardiometabolic adaptations. Obesity (Silver Spring, Md.), 24(4), 812–819. https://doi.org/10.1002/oby.21404
Thorndike, A. N., McCurley, J. L., Gelsomin, E. D., Anderson, E., Chang, Y., Porneala,
B., Johnson, C., Rimm, E. B., Levy, D. E. (2021). Automated behavioral workplace intervention to prevent weight gain and improve diet: the choosewell 365 randomized clinical trial. JAMA Network Open, 4, e2112528. https://dx.doi.org/10.1001/jamanetworkopen.2021.12528
Volpp, K. G., Asch, D. A., Galvin, R., & Loewenstein, G. (2011). Redesigning employee
health incentives--lessons from behavioral economics. The New England journal of medicine, 365(5), 388–390. https://doi.org/10.1056/NEJMp1105966
Weerasekara, Y.K., Roberts, S.B., Kahn, M.A. et al. (2016). Effectiveness of workplace
weight management interventions: a systematic review. Current Obesity Reports, 5, 298–306. https://doi.org/10.1007/s13679-016-0205-z
Wilson, M. G., DeJoy, D. M., Vandenberg, R. J., Corso, P., Padilla, H., Zuercher, H.
(2016). Effect of intensity and program delivery on the translation of diabetes prevention program to worksites. American College of Occupational and Environmental Medicine, 58, 1113-1120.
Wilson, M. G., DeJoy, D. M., Vandenberg, R. J., Padilla, H., Davis, M. (2016b). Fuel
your life: a translation of the diabetes prevention program to worksites. American Journal of Health Promotion, 30, 188-97. https://dx.doi.org/10.4278/ajhp.130411-QUAN-169
World Health Organization (2020, April 1). Obesity and Overweight.
https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight

25
Yarborough, C. M., Brethauer, S., Burton, W. N., Fabius, R. J., Hymel, P., Kothari, S., Kushner, R. F., Morton, J. M., Mueller, K., Pronk, N. P., Roslin, M. S., Sarwer, D. B., Svazas, B., Harris, J. S., Ash, G. I., Stark, J. T., Dreger, M., Ording, J. (2018). Obesity in the Workplace: Impact, Outcomes, and Recommendations. Journal of Occupational and Environmental Medicine, 60, 1, 97–107. https://doi.org/10.1097/JOM.0000000000001220

26
Appendix A: Literature Database Search Strategies
Database Search Strategy- OVID Medline
August 2015-Present Workplace ((work* or job* or employment*) adj2 (place* or site* or location* or setting*)).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] OR (workplace* or workplace* or work setting* or work-place* or work-site* or work-setting*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] OR exp Workplace/ OR (employer* adj2 (sponsor* or support* or based)).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept] AND Weight loss/ Primary outcome body constitution/ or exp "body weights and measures"/ or anthropometry/ OR (body adj2 (fat or composition or weight or measure* or constitution)).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] OR (bmi or "body mass index").mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] OR (skinfold* adj2 thick*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] OR (waist adj2 (hip or circumference)).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] OR exp Body Composition/ OR (body adj2 (fat or composition or weight or measure* or constitution)).mp. [mp=title, abstract, original title,name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] OR exp Adipose Tissue/ OR (adipos* or anthro*).mp. OR body weight/ or weight gain/ or weight loss/ or exp overweight/ OR (weight adj2 (loss* or reduc* or lower* or control* or prevent* or gain* or over)).mp.

27
AND Randomized Controlled Trial (randomized controlled trial or controlled clinical trial).pt. or randomized.ab.or placebo.ab. or clinical trials as topic.sh. or randomly.ab. or trial.ti OR (random* or RCT*).mp. or exp Randomized Controlled Trials/ or exp Clinical Trials as Topic/ Limit to: Clinical trial, all or comparative study or controlled clinical trial or evaluation studies or meta-analysis or multicenter study or systematic reviews)
Database Search Strategy - CINAHL Workplace ( (work* OR job* OR employment*) N2 (place* OR site* OR location* OR setting*) ) OR ( (workplace* OR workplace* OR worksetting* OR workplace* OR workplace* OR worksetting*)) OR (MH "Work Environment") OR ( employer* N2 (sponsor* OR support* OR based) ) AND Weight loss/ Primary outcome ( body mass index or bmi ) OR (MH "Body Weights and Measures" OR MH "Body Weight Changes" OR MH "Body Mass Index" OR MH "Waist Circumference" OR MH "WaistHip Ratio" OR MH "Anthropometry" ) OR (weightloss or overweight or obes*) OR ( MH "Body Weight" OR MH "Obesity+" OR MH "Weight Loss" OR MH "Body Constitution" ) OR ( weight N2 (change* OR loss* or reduc* or lower* or control* or prevent* or gain* or over) ) OR ((MH "Adipose Tissue Distribution") OR (MH "Adipose Tissue+") OR adipos* OR anthropomet* ) OR ( waist N2 (hip or circumference) ) OR skinfold* N2 thick* OR body N2 (fat or composition or weight or measure* or constitution) AND Randomized Controlled Trial ( (MH "Clinical Trials") OR (MH "Randomized Controlled Trials") ) OR TI trial* Limiters – Publication Type: Randomized Controlled Trial; Published Date: August 2015- June 2021
Database Search Strategy – Cochrane Clinical Trial Registry (Title Abstract Keyword search) Workplace ((work* or job* or employment* or occupation*) adj2 (place* or site* or location* or setting*)).mp. (mp=title, original title, abstract, mesh headings, heading words, keyword) OR (workplace* or workplace* or worksetting* or work-place* or work-site* or worksetting*). mp. (mp=title, original title, abstract, mesh headings, heading words,

28
keyword) OR Workplace OR (employer* adj2 (sponsor* or support* or based)).mp. (mp=title, original title, abstract, mesh headings, heading words, and keyword) AND Weight loss/ Primary outcome body constitution or "body weights and measures" or anthropometry OR (body adj2 (fat or composition or weight or measure* or constitution)).mp. (mp=title, original title, abstract, mesh headings, heading words, keyword) OR (bmi or "body mass index").mp. (mp=title, original title, abstract, mesh headings, heading words, keyword) OR (skinfold* adj2 thick*).mp. (mp=title, original title, abstract, mesh headings, heading words, keyword) OR (waist adj2 (hip or circumference)).mp. (mp=title, original title, abstract, mesh headings, heading words, keyword) OR Body Composition OR (body adj2 (fat or composition or weight or measure* or constitution)).mp. (mp=title, original title, abstract, mesh headings, heading words, keyword) OR Adipose Tissue OR (adipos* or anthro*).mp. (mp=title, original title, abstract, mesh headings, heading words, keyword) OR “body weight” or “weight gain” or “weight loss” or “overweight” OR (weight adj2 (loss* or reduc* or lower* or control* or prevent* or gain* or over or change*)).mp. AND Randomized Controlled Trial (randomized control trial or controlled clinical trial) or clinical trials Limit to Content Type: Trials, Original Publication Year: Between 2015-2021
Database Search Strategy – Scopus Workplace ( TITLEABSKEY ( ( work* OR job* OR employment* ) W/2 ( place* OR site* OR location* OR setting* ) ) OR ( TITLEABSKEY ( workplace* OR workplace* OR worksetting* OR workplace* OR workplace* OR worksetting* ) ) OR TITLEABSKEY ( employer* W/2 ( sponsor* OR support* OR based ) ) ) This was combined with the following search strategy using AND: Weight loss/ Primary outcome ( ( TITLEABSKEY ( body W/2 ( fat OR composition OR weight OR measure* OR constitution ) ) ) OR ( TITLEABSKEY( bmi OR "body mass index" ) ) OR ( TITLEABSKEY ( skinfold* W/2 thick* ) ) OR ( TITLEABSKEY ( waist W/2 ( hip OR circumference ) ) ) OR ( TITLEABSKEY ( adipos* OR anthropomet* ) ) OR ( TITLEABSKEY ( weight W/2 ( loss* OR reduc* OR lower* OR control* ORchange* OR prevent* OR gain* OR over ) ) ) OR ( TITLEABSKEY ( "body weight" OR obes* OR "weightloss" OR "weight gain" OR "weight loss" OR overweight ) ) OR ( TITLEABSKEY ( "body composition" OR "body constitution" OR "body fat" ) ) ) )

29
This was combined with the following search strategy using AND: Randomized Controlled Trial ( ( TITLEABSKEY ( random* OR trial* ) ) ) A date range was added: Published from 2015 to Present

30
Appendix B- RE-AIM Indicators and Corresponding Definitions
REACH Number of Eligible and
invited (exposed) to recruitment
The total number of eligible participants contacted for participation.
Sample size The number of people who agree to participate (e.g. n= ).
Participation rate Sample size divided by the target population denominator.
Participation rate (calculated)
Sufficient data to calculate standardized participation rate [sample size/ number of eligible participants contacted for participation].
Individual-level representativeness
Comparisons made between target population and study sample with a description of what those comparisons were.
Description target audience A brief description of the broader target population (i.e., not simply of the study sample).
Method to identify target population
Describe the process by which the target population was identified for participation in the study.
Inclusion criteria/ Exclusion criteria
Explicit statement of characteristics of the target population that were used to determine if a potential participant is eligible to participate. Explicit statement of characteristics that would prevent a potential participant from being eligible to participate.
Description of recruitment strategies used Describe the methods used to recruit participants into the study.
EFFICACY/EFFECTIVENESS Weight change Weight loss in kg or percent of body weight loss, change in BMI
Proportion of the sample that achieved ³ 5% weight
loss
Proportion of the sample that achieved ³ 5% weight loss
Quality of life measure Includes a measure of quality of life with some latitude for coding articles that refer to well-being or satisfaction with life.
Unintentional negative consequences and results
To evaluate unanticipated consequences and results that may be a product of the intervention and may have caused unintended harm.
Imputation of missing data Substitution of some value for missing data. Specify imputation procedure.

31
ADOPTION
Number of eligible and invited sites
Total sites that met eligibility criteria and were approached for intervention delivery.
# Participating (sites) The total number of sites that agreed to participate. Participation rate (sites) The proportion of sites eligible and contacted that participated. Description of targeted
location Characteristics that would be considered an ideal location for the intervention.
Description of intervention location
The explicit statement of characteristics of the location of the intervention.
Method to identify setting Describe the process by which the location was identified for participation in the study.
Setting Representativeness (# of Comparisons)
Total number and type of comparisons of targeted intervention sites and those that participated, including a list: size, location, etc.
# eligible and invited(exposed)
Total staff that met eligibility criteria and were approached for intervention delivery.
# Participating in delivery The total staff members that agreed to participate.
Level of expertise of delivery agent
Training or educational background in relevant area; Degrees, certifications of delivery agents (such as PhD, Masters, Registered Dietitian, etc.)
IMPLEMENTATION
Theories Explicit statement of theories or principles used to develop the intervention
Intervention number of contacts
Total number of encounters with participants. Could include face-to-face meetings, telephone calls, newsletters etc.
Timing of contacts Describe when the intervention contacts occur over the course of the intervention.
Duration of contacts Length of each intervention contact.
Extent protocol delivered as intended (%) Description of fidelity to the intervention protocol.
Consistency of implementation across
setting and delivery agents
Description of the degree of similarities between multiple settings sites & delivery agents
Participant attendance/completion
rates
The proportion of the intervention that the participants received, on average.
Measure of cost The ongoing cost of delivery across all levels of the intervention

32
Cost of recruitment The cost of recruitment can reflect monetary and/or time units.
Cost effectiveness Code as reported if specific mention and amounts are provided for the cost of the intervention.
MAINTENANCE
Was individual behavior assessed at some duration following the completion of
the intervention? (give duration of follow-up)
Description of follow-up outcome measures of individuals available at some duration after intervention termination
Participant Attrition Describe the degree to which participants were lost to follow-up (and the reasons) during the period in time from the interventions completion to the follow-up.
Was the program institutionalized?
Description of the how the intervention was integrated into the delivery system through methods such as policy changes, job description changes.
Biography & CV
Adrienne Gothard is a Master of Public Health student at the University of Nebraska
Medical Center, with a concentration in health promotion. Ms. Gothard holds a
Bachelor’s degree in Nutrition and Dietetics from the University of Northern Colorado
and has been a Registered Dietitian since 2012. Her current professional public health
interests center around corporate wellness and improving the health of the workforce.
33
AdrienneGothard,RDN
RegisteredDietitianNutritionist
EDUCATIONMasterofPublicHealth:HealthPromotionconcentrationExpectedAugust2021UniversityofNebraskaMedicalCenterDieteticInternship July2011-March2012UniversityofNorthernColorado(UNC),Greeley,COBachelorofScience:Dietetics,Minor:PsychologyMay2010UniversityofNorthernColorado(UNC),Greeley,CO
RELEVANTWORKEXPERIENCE
FOOD SAFETY CONSULTANT National Environmental Health Association, Denver CO May 2021- Present
§ Execute tasks for project deliverables as directed within the food safety team § Develop thoroughly researched reports and content for the organization’s website § Communicate effectively and professionally with stakeholders, subject matter experts,
partner organizations, and other project participants
CLINICAL NUTRITION MANAGER Sodexo Inc., Good Samaritan Medical Center, Lafayette CO November 2019– April 2021
§ Directed daily operations of hospital clinical nutrition program § Managed team of 6 Registered Dietitian Nutritionists § Responsible for the training of new clinical dietitians and interns § Monitored staffing productivity and managed the clinical nutrition program budget § Completed audits of malnutrition program data to create action plans and report
financial outcomes to the client § Created and presented educational in-services for nutrition department staff, hospital
wide employee health classes, and client-facing presentations § Promoted health and wellness as a 6-year member of the hospital’s Employee Wellness
Committee § Implemented health and wellness initiatives in the hospital café
PATIENT FOOD SERVICES MANAGER Sodexo Inc., Good Samaritan Medical Center, Lafayette CO March 2019 – November 2019
§ Directed daily operations of patient meal services to ensure timely and accurate delivery of meals and nourishments to patients

34
§ Managed a team of twenty-five+ employees § Collaborated with clinical departments and hospital leaders to ensure exceptional
patient experience § Ensured that employees had appropriate equipment, inventory, and resources to
perform their jobs § Ensured compliance with all state, federal, and local regulations for quality assurance,
food safety, and workplace safety CLINICAL DIEITITAN Sodexo Inc., Good Samaritan Medical Center, Lafayette CO September 2012 – March 2019





























