Slide 1
Reaching Out Across the Miles:The Role of Telehealth in Maternal
and Child HealthLorie Wayne Chesnut, DrPH, MPHUniversity of
Kentucky College of Public Health
With special thanks to Rob Sprang, MBA, Director, Kentucky
TeleCareJanuary 2014Photo by Pat Richter, Colorado
It all started with a question from a State Title V leader ...I
wonder how other states are using telehealth systems to improve
maternal and child health?
January 2014
Telehealth and MCHExamples from the fieldJanuary 2014
Photo by Don Chesnut: Upper Peninsula, MI
MethodsData Source: Title V MCH Block Grant TVISSystem
(2012/2014) Annual Reports andApplications
Step 1: Narrative Text Search
Step 2: What telehealth project is associated with each National
or State Performance Measures ?
Step 3: Compile results for each performance measure.
Step 4: Calculate frequencies and conduct in-depth interviews
for particularly interesting or creative telehealth
applications
January 2014Search Terms Used
TelehealthTelemedicineTele-TeledentistryTelerehabilitationTelepsychiatryTeleaudiologyTelegeneticshttps://perfdata.hrsa.gov/mchb/TVISReports/Default.aspx
4LimitationsStates strive to include information in their annual
report about programs that improve access and care for disparate
populations. But space for narrative within the TVIS system is
limited.
This fact may result in a lack of information about telehealth
activities currently underway in communities around the state.
More may be going on then is reported in the Title V
narrative.January 2014
Photo: Don Chesnut. Seney Wildlife Refuge, Upper Peninsula, MI,
2013
Most Common Telehealth Applications by Title V NPMJanuary
2014NPM # and Description# of States Reporting Use of Telehealth
(12/14 Application/Annual Report)NPM #01: The percent of screen
positive newborns who received timely follow up to definitive
diagnosis and clinical management for condition(s) mandated by
their State sponsored newborn screening programs. 9 statesNPM #05:
The percent of children with special health care needs age 0 to 18
whose families report the community-based service systems are
organized so they can use them easily. 9 states NPM #12: The
percent of newborns who have been screened for hearing before
hospital discharge.7 states, 1 territoryNPM #17: The percent of
very low birth weight infants delivered at facilities for high-risk
deliveries and neonates.6 states
Additional Telehealth Applications by Title V NPMJanuary 2014NPM
# and Description# of States Reporting Use of Telehealth (12/14
Application/Annual Report)NPM #03: The percent of children with
special health care needs age 0 to 18 who receive coordinated,
ongoing, comprehensive care within a medical home.5 states, 1
territoryNPM #09: Percent of third grade children who have received
protective sealants on at least one permanent molar tooth.3 states
NPM #15: The rate (per 100,000) of suicide deaths among youths aged
15 through 19.2 states
January 2014Direct Health ServicesEnabling
ServicesPopulation-Based ServicesInfrastructure ServicesThe MCH
Pyramid Examples of Telehealth ApplicationsMedical consultations,
outreach clinics, follow-up services for patients with established
diagnoses. CYSHCN. School-based dental exams, cleanings, fluoride
varnish application, dental sealants. Mental health counseling,
telepsychiatry consults, family and individual therapy.Provider
training and continuing education, evidence-based guideline
development, evaluation, health care quality and standards, service
monitoring, billing systems, stress management and mental health
support for health professionals in rural areas. Health Screenings
including school-based dental and mental health screenings,
hospital-based audiology screenings. High-risk pregnancy
monitoringHealth education, individual and family support, case
management, translation support, rural outreach. Genetic
counseling. High-risk maternal and infant transport coordination.
Telehealth services bring access to rural populations by reducing
travel time to clinic sites.
Overview: Telehealth Activities to Address Select MCH
OutcomesJanuary 2014Newborn Metabolic ScreeningChildren/Youth with
Special Health Care NeedsNewborn Hearing ScreeningHigh Risk
DeliveryDental Services
Newborn Metabolic Screening/Genetic ServicesTelegenetics is
defined as the use of telemedicine for the provision of clinical
genetics services. Clinical genetics includes types of
sub-specialty areas including prenatal, pediatric, biochemical and
cancer.
Providers are often based in urban areas at tertiary centers,
thus out of the reach of infants, children and their families who
live in rural areas.
States set up genetic clinics on a rotating schedule based on
population need. While this improves access to care, needs of
children and families are often not met or only partially met.
In 2004, the Maternal and Child Health Bureau funded 7 regional
genetic collaboratives and a national coordinating center to
support genetic services for pregnant women, infants and children
in the U.S.
(National Coordinating Center for the Regional Genetic and
Newborn Screening Service Collaboratives @
http://www.nccrcg.org)
January 2014
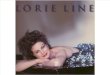
HRSA Regional Genetics and Newborn Screening
Collaboratives*January 2014Initial visits are usually done in
person. Telegenetics is typically used for genetic counseling and
follow-up care. Barriers specific to telegenetics practice:
Fewer clinical geneticists and genetic counselors are being
trained. While telehealth improves their ability to consult with
individuals in remote sites, their time may be even further
stretched with the acquisition of additional patients.
Interstate practice issues (such as licensing) are also a
problem. This is a particular issue for supersubspecialists who
might specialize in rare genetic disorders and who might be needed
to consult for only a few cases each year.
*Source: NNSGRC. Accessed 01-14-14 at
http://genes-r-us.uthscsa.edu/resources/genetics/StatePages/genetic_region_map.htm
11Children & Youth with Special Health Care Needs
(CYSHCN)Broad categories of services include clinical management
(endocrinology and diabetes care, neurology, dermatology,
cardiology, etc.), nutritional counseling, rehabilitation and
neurodevelopmental services, family case-management, etc.
Many states note telehealth services for the CYSHCN
population.
Children in rural communities often have difficulty accessing
medical specialists, rehabilitation services, neurodevelopmental
services.
January 2014Example: Telerehabilitation, defined as the delivery
of rehabilitation services via information and communication
technologies.
The delivery of these services may include a broad array of
providers including physical therapists, speech-language
pathologists, occupational therapists, audiologists, dieticians,
psychologists, assistive technologists. Source: ATA, A Blueprint
for Telerehabilitation Guidelines (2010)
Newborn Hearing Screening: Applications and Public Health
Implications Not yet widely used, first use about 15 years ago.
Few published articles regarding efficacy need for more
research.
Needed to provider/family access in rural areas
Loss-to-follow-up following after failure of hearing screening*
(HRSA estimates 40% of infants recommended to return never do )
HRSA funding a teleaudiology pilot project in North Dakota**.
January 2014For teleaudiology in general, two synchronous
models:
High-quality interactive video, remote (local) technician tests
under the supervision of the clinician located at the hub site.
Patient data obtained, clinician diagnoses, recommends
management.
Remote-control computer enables clinician at hub site to test
patient directly at remote site. No technician necessary at remote
site, however facilitator needed for some tasks. ** Rural
Assistance Center. Teleaudiology: Taking Diagnostics to the Infant
http://www.raconline.org/success/project-examples/641Resource:
Krumm M & Syms MJ. (2011). Telehealth in otolaryngology
Teleaudiology. Otolaryngologic Clinics of North America. Volume 44
(6):1297-1304
13TeleAudiology: Taking Diagnostics to the Infant (North Dakota,
Minot State University)Developed by Neil Scharpe, Steve Peterson
and Tom Froelich at Minot University and completed in August
2010.
Funded through a 2-year HRSA contract awarded to the North
Dakota Center for Persons with Disabilities at Minot State
University (one of about 60 Centers of Excellence for persons with
disabilities in the nation)
Charged with creating protocols to complete audiology
diagnostics with infants 0-6 months of age using the internet
Three deliverables:Management ProtocolTechnical ProtocolTool
Kit
January 2014For more information about North Dakotas
TeleAudiology Protocol and Tool Kit, contact: Neil Scharpe,
DirectorGreat Plains Center for Community Research and ServiceMinot
State University500 University Ave. WestMinot, ND
[email protected] 701-858-3596
Regionalization of Perinatal Care Level of Care and Volume of
Deliveries Matter!Why is the system breaking down?
Shortages of providers in rural areas (preference to practice in
urban locations)High cost of malpractice insurance driving OB/GYNS
and Pediatricians out of rural communitiesHigh-risk patients in
rural areasMedicaid reimbursement issuesFinancial competition among
hospitals for patients Patient choice they want to remain near
homeJanuary 2014Hall et al., 2010 ACOG Committee Recommendation:
Encourage and participate in efforts to utilize effective
telemedicine technologies to expand and improve services for rural
women.
- ACOG Committee Opinion Number 429, March 2009, Obstetrics
& Gynecology, 113(3):762-765.
ANGELS: Distant Obstetric Care Delivery in ArkansasANGELS =
Antenatal & Neonatal Guidelines, Education and Learning
System
Collaboration between Arkansas Medicaid Program and the
University of Arkansas for Medical Sciences. Link:
http://angels.uams.edu/
PurposeTo enhance primary obstetrical care in rural areas and
small communities across ArkansasTo increase appropriate referrals
of high-risk obstetric cases to board-certified maternal fetal
medicine specialists
To assure that all Medicaid obstetric recipients have access to
the highest quality perinatal care including genetic counseling
January 2014Lowery et al., 2007
ANGELS: Distant Obstetric Care Delivery in ArkansasEmpowering
the local providerthrough:
Telemedicine support ConsultationBest Practices development and
adoption
Fetal-Medicine Specialists (all located in Little Rock)
Promote interaction between providers statewideEnable earlier
recognition of high-risk pregnancies/birthsFacilitate transfer to
Level III hospitals when indicatedIncrease accessibility to FM
specialists.ANGELS ComponentsStatewide telemedicine and clinic
networkEducation and support program for obstetrical providersCase
management servicesA 24-hour call centerAn evidence-based
guidelines development and distribution network. January 2014Lowery
et al., 2007.
ANGELS: Distant Obstetric Care Delivery in ArkansasConnecting
...
Area Health Education Centers (AHEC)~ 40 hospitals and rural
health centers via telemedicine network
Enabling ...
Consultations with rural practitioners and patientsLive
examinations and ultrasounds over interactive videoMeetings with
hospital administrators and their staffDissemination of protocols,
best-practice information, etc.
Evaluating ANGELS
Volume of MFM consults to OB patientsVolume of case management
calls moving through the call center from OB patients and
providersVolume of high-risk maternal transports at UAMSVolume of
evidence-based guidelines distributed to OB providersVolume and
proportion of LBW and VLBW births delivered at Level III
facilities
January 2014Lowery et al., 2007
Why Do We Need Teledentistry?Shortage of dental providers in
rural areas
Shortage of dentists, dental hygienists and other dental
professionals nation-wide.
Graying of the nations dental workforce retirement, fewer days
worked for current practitioners and too few providers trained at
U.S. Schools of Dentistry
The cost of setting up a new dental practice is high providers
prefer to practice in urban or metropolitan areas
Dental Hygienists scope of practice independent or under the
supervision of a dentist (varies state-to-state and by service)
Advanced communication technologies may create new bridges among
dentists. Advances such as videoconferencing and real-time on-line
collaboration will make various forms of "teledentistry" possible
and practical. Legal, licensure, and political considerations may
prove more difficult to address than technical ones.
- The Future of Dentistry: Todays Vision: Tomorrows Reality,
ADA, 2001January 2014
Arizonas Oral Health Workforce Grant (Teledentistry)
2009Purpose:
To promote and develop enhanced dental teams utilizing
teledentistry practice and/or affiliated practice to improve
workforce capacity, diversity and flexibility for providing oral
health services to underserved populations and underserved
areas.
Objectives:
Build and expand regional/local program development
infrastructureTrain providers for enhanced dental teams and
increase provider understanding and competencies for teledentistry
practice and affiliated practiceEducate and increase awareness of
program administrators, policymakers and funders about enhanced
dental teams and how teledentistry practice and affiliated practice
can increase workforce capacity and flexibility in community
settingsIncrease the number of enhanced dental teams at the state,
regional and local levelsDevelop and gather resource materials,
tools and lessons to support development of practice models, making
this information accessible to providers, programs and
communities.Accessed 01/16/14 at
http://azdhs.gov/phs/owch/oral-health/azsmiles/documents/about/EDT_Grant-Program-Key-Points.pdf
20Arizonas Oral Health Workforce Grant (Teledentistry)
2009Benefits Realized Include ...
School-based preventive care for pre-school and school-aged
children. Kids dont have to miss school the services come to them.
Oral health evaluation collects data and triages children based
upon needs. Time-saving, child not lost-to-follow-up.
Allows for partnership with Head Start this group may be
difficult to reach. Families may live a long way from a dentist
Involves school nurses a great resource for children and
families
Provides preventive care to inner-city children.
Develops curricula for dental hygienists what is really needed
in the real world in partnership with North Arizona University.
Provides training for dentists on how to treat children/youth
with special health care needs.
Building partnerships throughout Arizona, between dental
providers, policy specialists and other stakeholders.
January 2014Source: Personal Communication Julia Wacloff, RDH,
MSPH 01/11/11. Note: In Arizona, registered dental hygienist s are
allowed to provide dental hygiene services under an affiliated
practice relationship with a licensed dentist.
Arizona TeleDentistry: Lessons LearnedStrong infrastructure
critical (advanced IT support, business model, administrative
support, encryption)
Equipment and technology continue to evolve. Equipment you
purchase today (whether technology or peripherals) is outdated in
just a few years.
As equipment and techniques change, so must people evolve.
Training needs are continuous and challenging.
Reimbursement continues to be a challenge. Not all children
involved are Medicaid enrollees. Few private insurance policies
support teledentistry. In Arizona, IHS insurance adds to the
mix.
For both patients and providers, teledentistry can be a GREAT
educational tool. Families and the child can see the decayed
tooth.
Oral cameras can also be used to teach youth about oral cancers
visual images make a difference.January 2014Source: Personal
Communication Julia Wacloff, RDH, MSPH 01/11/11More about
teledentistry in Arizona:
http://www.azdhs.gov/phs/owch/oral-health/documents/reports/teledentistry-arizona.pdf
Whats next? Watch our site for a special series of webinars
entitled Telehealth & You: All you need to know but just what
you need to know!
This series will have short presentations directed to Title V
MCH Leadership, Providers, and Technologists, as well as others. We
wont overwhelm you with all of the nuts and bolts of complete
telehealth systems you can pick and choose depending upon your
interests and needs.
Presentations and papers about the uses of telehealth technology
to improve MCH outcomes learn about teleaudiology, teledentistry
and how the field of mental health use telehealth systems to
improve access to care!
January 2014Consulting by Rob Sprang, MBA, Director, Kentucky
TeleCare for specific state needs regarding telehealth. Rob has a
long history of working in telehealth and has also served as
President of the Board of Directors for the Center for Telehealth
and e-Health Law (Washington DC) and is currently President of the
Board of Directors for CTeL Innovations. Rob is always pleased to
share his expertise about telehealth systems and how these can be
used to improve MCH outcomes.
Resources for Further InformationA Few Websites for Future
Interest
American Telehealth Association
http://www.americantelemed.org/i4a/pages/index.cfm?pageid=1
The Center for Telehealth and e-Health Law
http://www.telehealthlawcenter.org/
American Academy of Pediatrics
http://www2.aap.org/sections/telecare/
Health Resources and Services Administration: Telehealth.
http://www.hrsa.gov/telehealth/default.htm
The Telemedicine & Advanced Technology Research Center
(TATRC) (Department of Defense). http://www.tatrc.org/
January 2014
Resources for Further InformationA Sampling of MCH Programs
Utilizing Telehealth Technology
AFHCAN Telehealth Solutions http://www.afhcan.org/
TeleAudiology: Taking Diagnostics to the Infant
http://www.infanthearing.org/meeting/ehdi2010/ehdi_2010_presentations/TeleAudiology.pdf
The Antenatal and Neonatal Guidelines, Education and Learning
System (ANGELS) http://angels.uams.edu/ (Arkansas)
January 2014Resources for Further InformationSelected
Reports
Hein, MA. (2009) Telemedicine: An Important force in the
Transformation of Healthcare. U.S. Department of Commerce,
International Trade Administration.
Hersh, WR., Hickam, DH., Severance, SM., Dana, TL., Krages, KP,
Helfand, M. (2006) Telemedicine for the Medicare Population:
Update. Oregon Evidence-based Practice Center, Portland, OR.
(Prepared for the Agency for Healthcare Research and Quality,
HHS).
Clinical Diagnosis & Management Cluster (2006). Telegenetics
Summary Document. Region 4 Genetics Collaborative.
Center for Telemedicine Law (2003). Telemedicine Reimbursement
Report. Washington, DC.
Puskin, DS., Kumekawa, JK. (2001). 2001 Telemedicine Report to
Congress. Office for the Advancement of Telehealth, HRSA/HHSJanuary
2014Citations (page 1 of 2)Books:
Darkins, AW and Cary, MA. Telemedicine and Telehealth:
Principals, Policies, Performance, and Pitfalls. New York, NY;
Springer Publishing; 2000.Institute of Medicine. Telemedicine: A
Guide to Assessing Telecommunications in Health Care. Washington,
DC; National Academy Press; 1997.
Additional Reports and Publications
American Telemedicine Association (2010) A Blueprint for
Telerehabilitation Guidelines. Accessed 01/23/11 at
http://www.americantelemed.org/files/public/standards/ATA%20Telerehab%20Guidelines%20v1%20(2).pdfAu,
S., Hasegawa, L, Silvey, K., Stock, J. (2010) Regional Genetic
Services Practice Model Evaluation: Report on Delivering Genetic
Service via Outreach and Telehealth in Guam and the Western States.
Western States Genetic Services Collaborative. Bronstein JM,
Ounpraseuth S., Jonkman J, Fletcher D, Nugent RR, McGhee J, Lowery
CL. (2012). Use of speciality OB consults during high-risk
pregnancies in a Medicaid-covered population: initial impact of the
Arkansas ANGELS intervention. Med Care Res Rev. 69(6):699-720.Hall
RW, Hall-Barrow J, Garcia-Rill E. (2010) Neonatal regionalization
through telemedicine using a community-based research and education
core facility. Ethnicity and Disease. 20(1 Suppl 1): S1-136-40Kim
EW, Teatue-Ross TJ, Greenfield WW, Keith Williams D, Kuo D, Hall
RW. (2013) Telemedicine collaboration improves perinatal
regionalization and lowers statewide infant mortality. Journal of
Perinatology. 33(9):725-30.
Citations (page 2 of 2)Krumm, M., Ribera, J., Schmeidge, J.
(2005) Using a Telehealth Medium for Objective Hearing Testing:
Implications for Supporting Rural Universal Newborn Hearing
Screening Programs. Seminars in Hearing. 26(1):3-12. Krupinski, E.,
Dimmick S., Grigsby, J., Mogel G., Puskin D., Speedie, S., Stamm,
B., Wakerfield, B., Whited, J., Whitten P., Yellowlees, P. (2006).
Telemedicine and e-Health. 12(5):579-589. Lamar, R. (Ed.). (2004)
Evolution Summative Evaluation of the Alaska Federal Health Care
Access Network Telemedicine Project. Alaska Native Tribal Health
Consortium, University of Alaska, Alaska Telehealth Advisory
Council. Lowery C, Bronstein J, McGhee J, Ott R, Reece EA, Mays GP.
(2007). ANGELS and University of Arkansas for Medical Sciences
paradigm for distant obstetrical care delivery. Am J Obstet
Gynecol. 196(6):534.e1-9. Nemes, J. (2010). Tele-audiology, a
once-futuristic concept, Is growing into a worldwide reality. The
Hearing Journal. 63(2):19-24Novotney, A. (2011). A new emphasis on
telehealth How can psychologists stay ahead of the curve and keep
patients safe? Monitor on Pcyshology (APA). Accessed 01/16/14 at
https://www.apa.org/monitor/2011/06/telehealth.aspxPatricoski, C.
(2004) Alaska Telemedicine: Growth Through Collaboration.
International Journal of Circumpolar Health 63(4) 365-386Scharpe,
N., Peterson, S., Froelich, T. TeleAudiology: Taking Diagnostic to
the Infant. North Dakota Center for Persons with Disabilities and
Minot State University Center of Excellence. Accessed 01/24/11 at
http://www.infanthearing.org/meeting/ehdi2010/ehdi_2010_presentations/TeleAudiology.pdf